Embed Size (px)
Citation preview
University of MichiganDepartment of Radiology
Windows to the Acoustic World: A Review of Pathologies
Involving the Oval, Round, and ‘Third’ Windows.Authors: Rickin Shah, MD
Ashok Srinivasan, MD
DisclosuresNone
Special Thanks toDanielle Dobbs for illustrations
Objectives
To review physiology of hearing and the importance of the oval and round windows in this process
To discuss pathologies involving the oval andround windows
To describe the 'third window' phenomenon and present illustrated examples of different causative etiologies
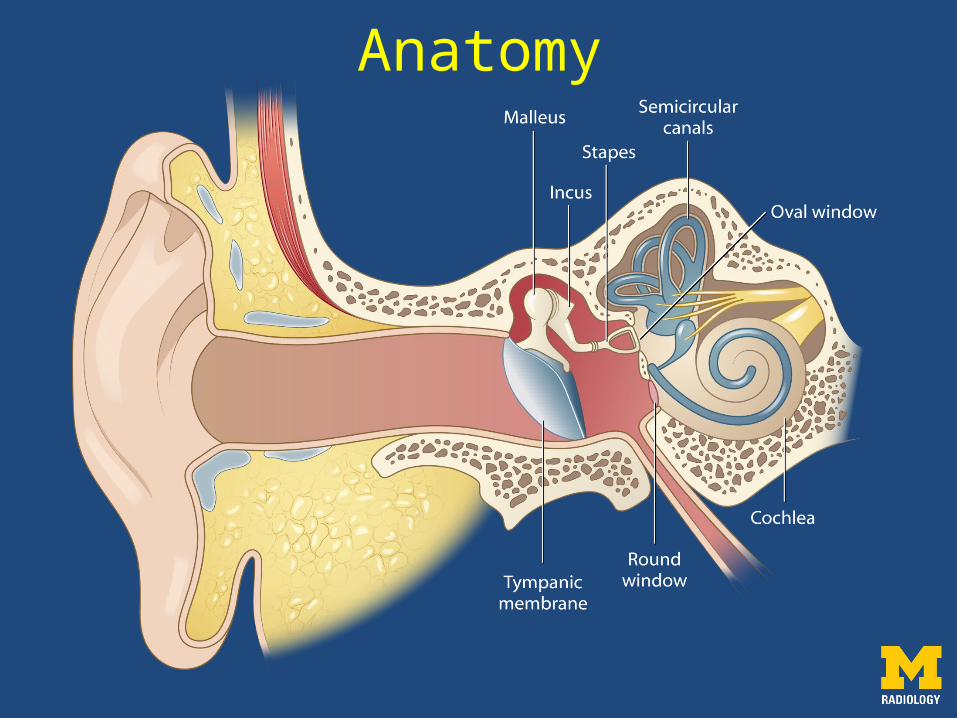
Anatomy
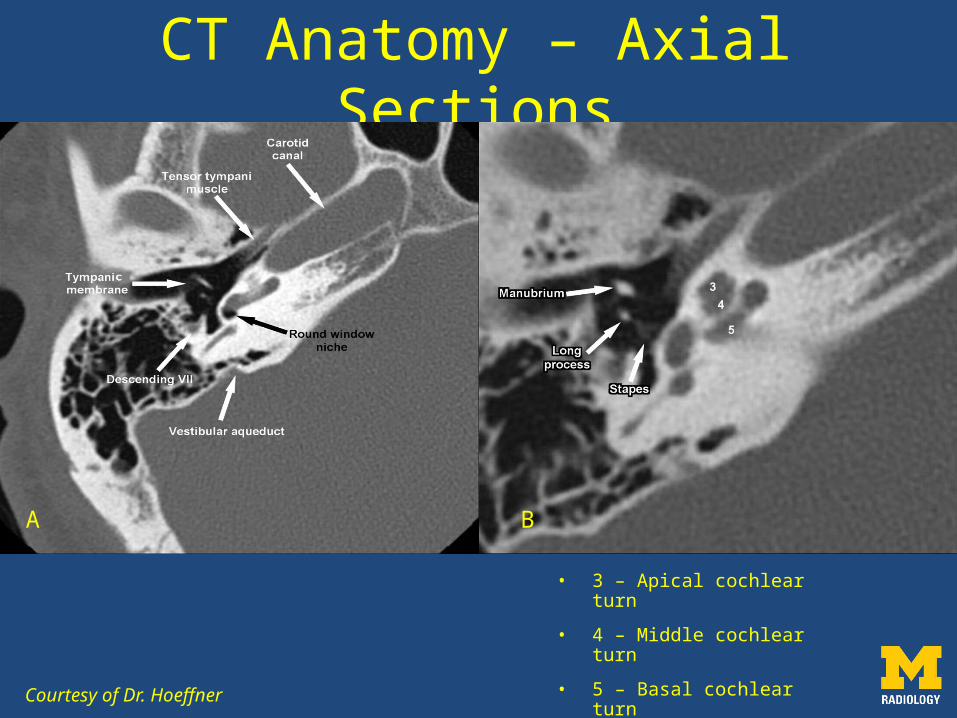
• 3 – Apical cochlear turn
• 4 – Middle cochlear turn
• 5 – Basal cochlear turn
CT Anatomy – Axial Sections
Courtesy of Dr. Hoeffner
BA
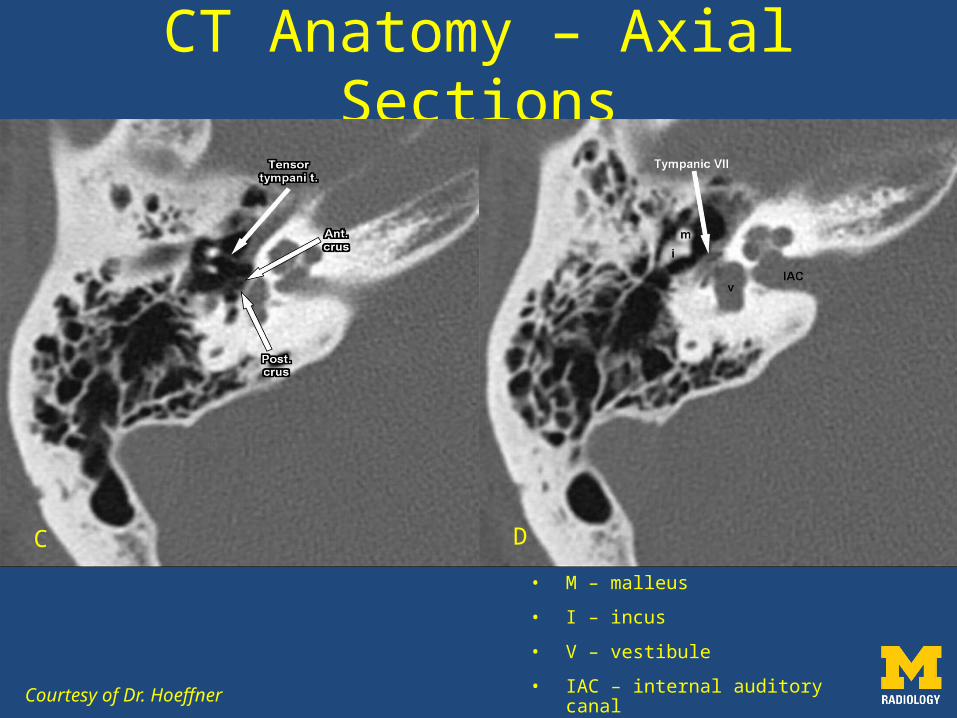
• M – malleus
• I – incus
• V – vestibule
• IAC – internal auditory canal
CT Anatomy – Axial Sections
Courtesy of Dr. Hoeffner
C D
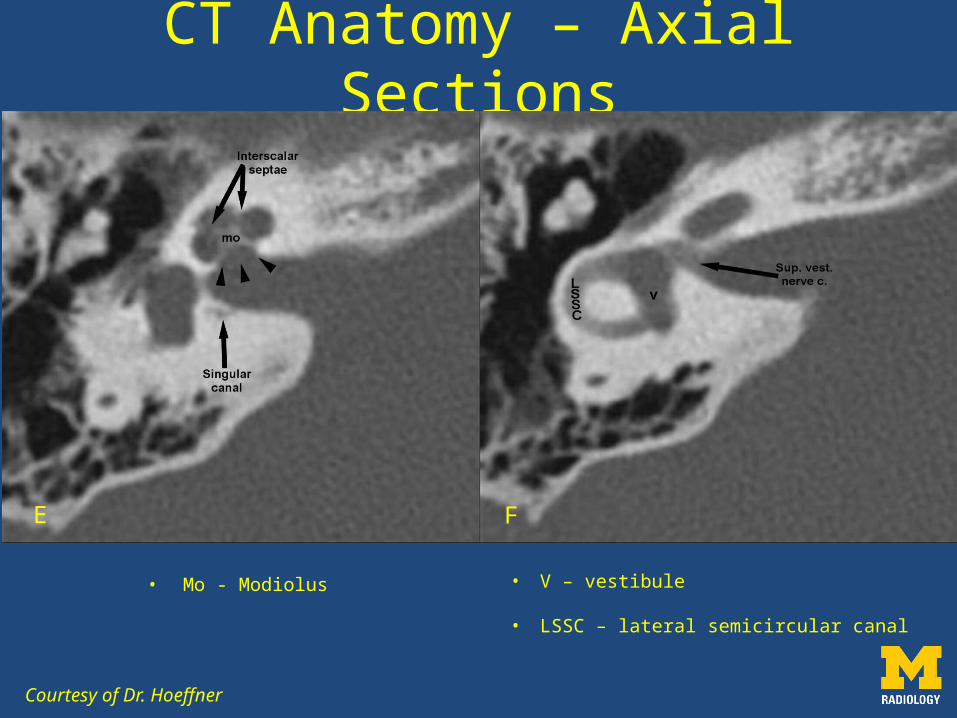
• Mo - Modiolus
CT Anatomy – Axial Sections
Courtesy of Dr. Hoeffner
E F
• V – vestibule
• LSSC – lateral semicircular canal
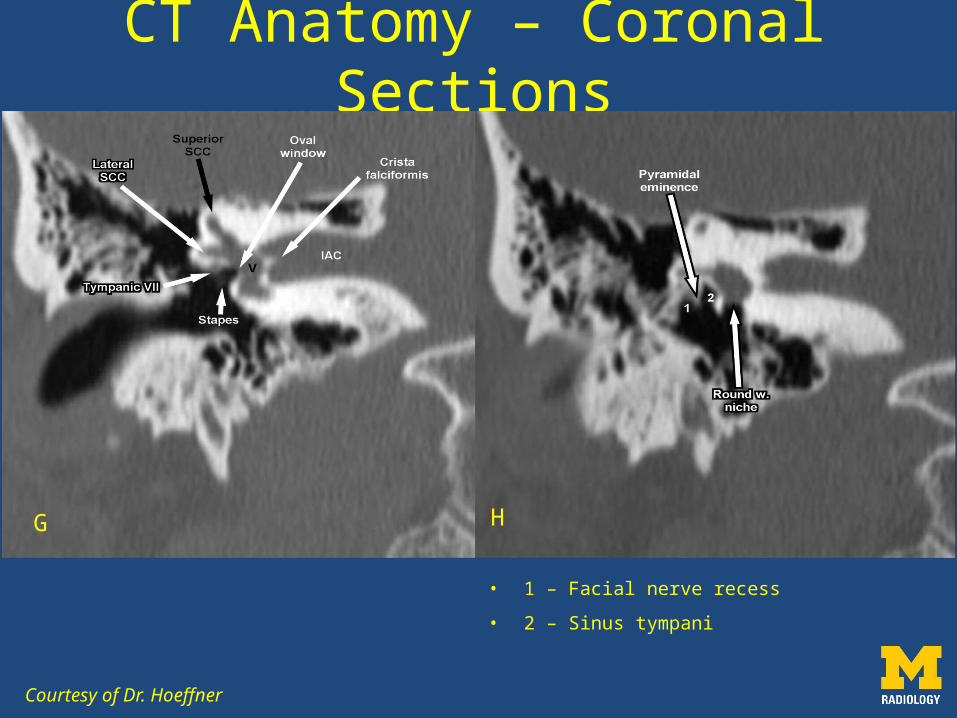
• 1 – Facial nerve recess
• 2 – Sinus tympani
Courtesy of Dr. Hoeffner
CT Anatomy – Coronal Sections
G H
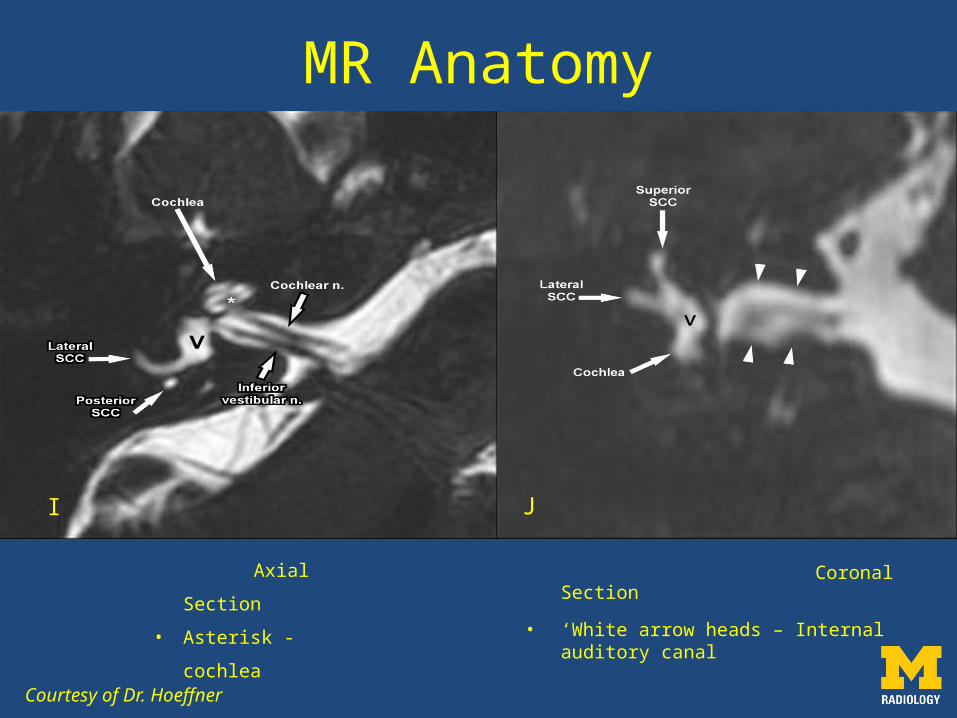
Coronal Section
• ‘White arrow heads – Internal auditory canal
Courtesy of Dr. Hoeffner
MR Anatomy
I J
Axial Section
• Asterisk -
cochlea
http://www.slideshare.net/schwartzcm/ch-10-senses-part-ii
Sound Transmission
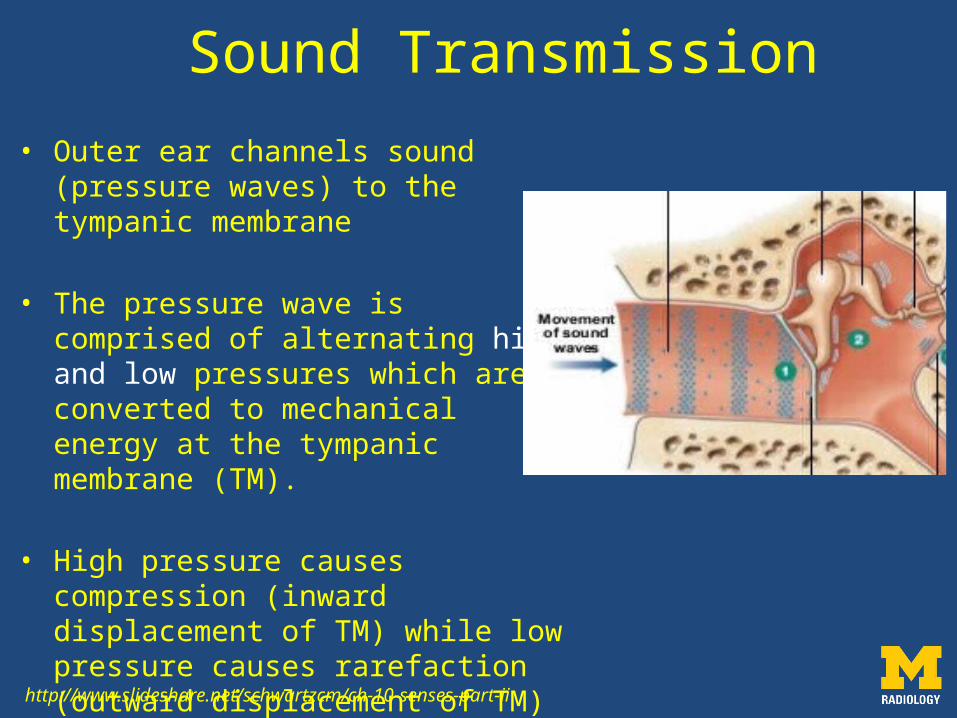
• Outer ear channels sound (pressure waves) to the tympanic membrane
• The pressure wave is comprised of alternating high and low pressures which are converted to mechanical energy at the tympanic membrane (TM).
• High pressure causes compression (inward displacement of TM) while low pressure causes rarefaction (outward displacement of TM)
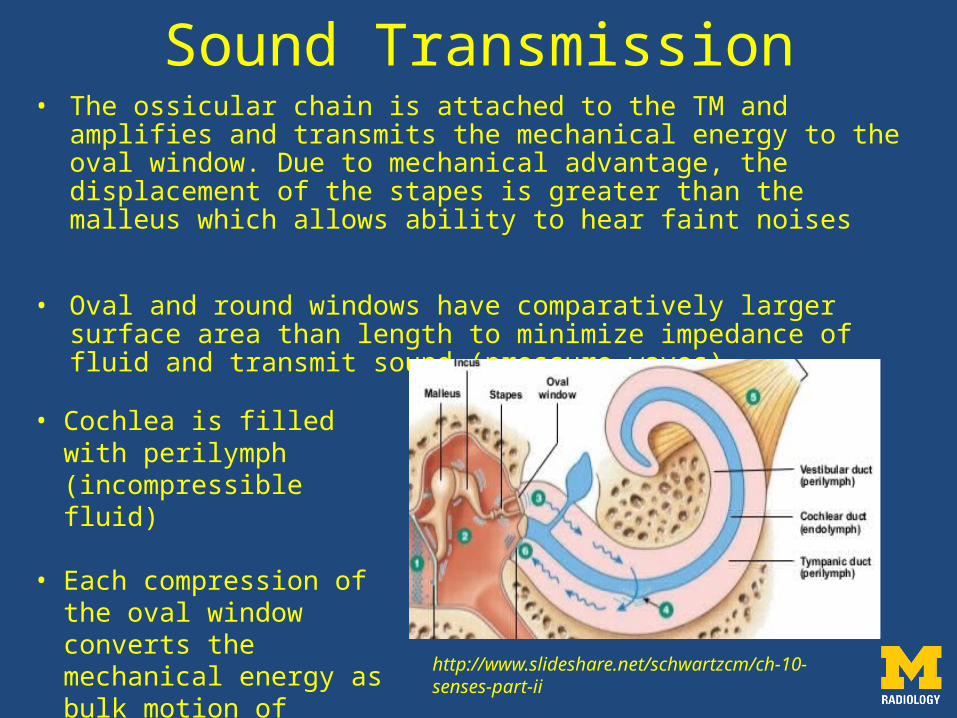
Sound Transmission• The ossicular chain is attached to the TM and amplifies and
transmits the mechanical energy to the oval window. Due to mechanical advantage, the displacement of the stapes is greater than the malleus which allows ability to hear faint noises
• Oval and round windows have comparatively larger surface area than length to minimize impedance of fluid and transmit sound (pressure waves)
• Cochlea is filled with perilymph (incompressible fluid)
• Each compression of the oval window converts the mechanical energy as bulk motion of perilymph fluid http://www.slideshare.net/schwartzcm/ch-
10-senses-part-ii
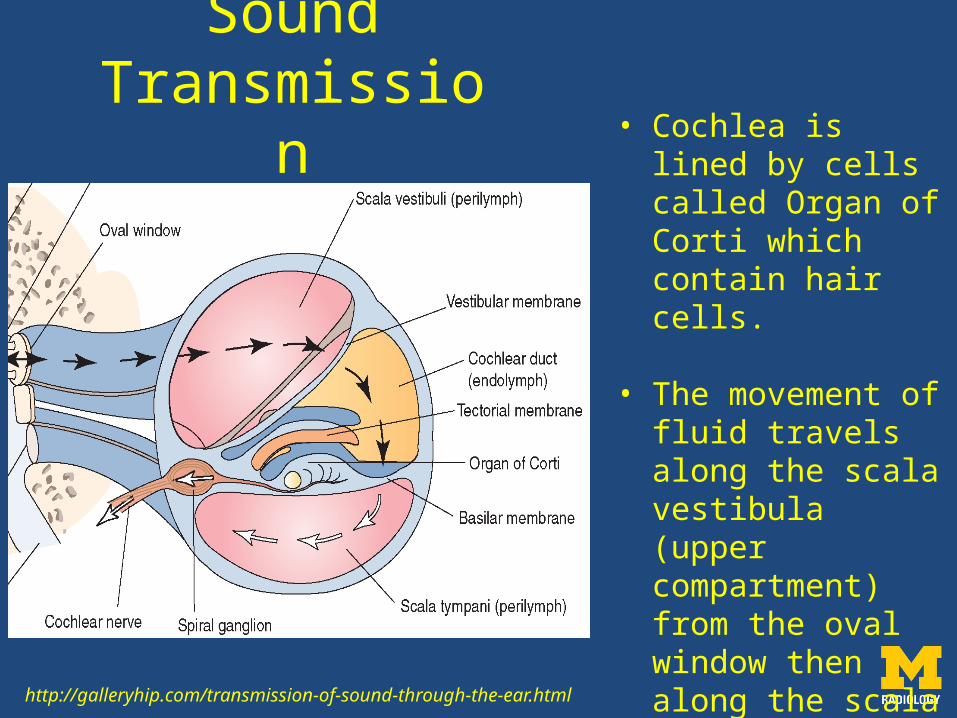
Sound Transmission
http://galleryhip.com/transmission-of-sound-through-the-ear.html
• Cochlea is lined by cells called Organ of Corti which contain hair cells.
• The movement of fluid travels along the scala vestibula (upper compartment) from the oval window then along the scala tympani to the round window.
Sound Transmission
Each sound wave bends certain hair cell projections based on their natural frequency
Each bend of the hair cells converts the mechanical energy into electric energy which is sent to the brain
Semicircular canals do not play a role in hearing but used to detect rotational acceleration in their planes

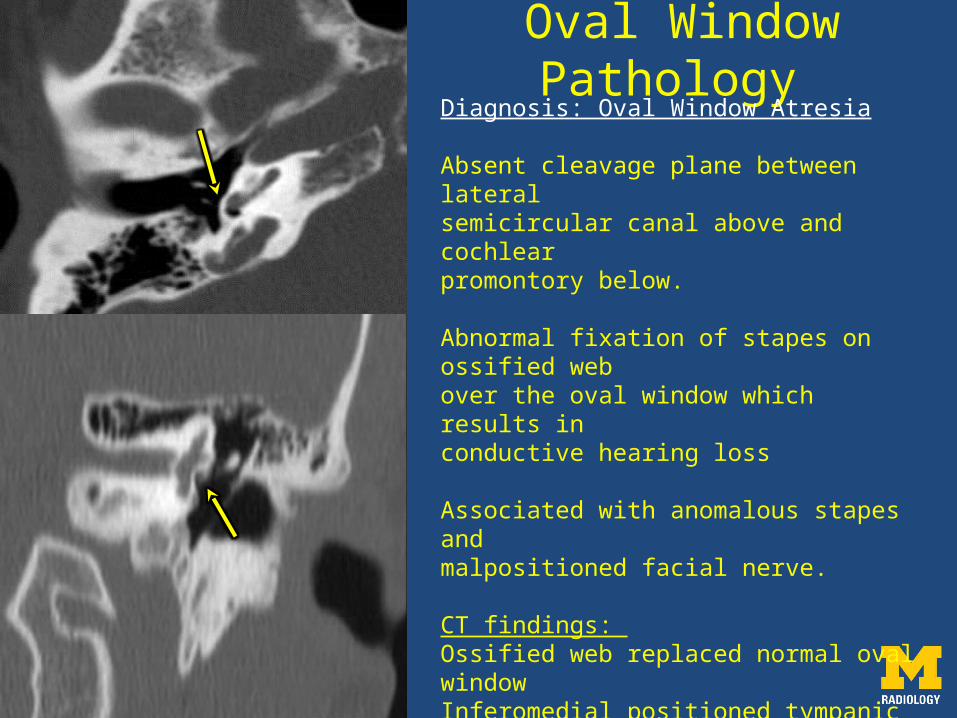
Oval Window Pathology
Diagnosis: Oval Window Atresia
Absent cleavage plane between lateralsemicircular canal above and cochlear promontory below.
Abnormal fixation of stapes on ossified web over the oval window which results in conductive hearing loss
Associated with anomalous stapes and malpositioned facial nerve.
CT findings: Ossified web replaced normal oval windowInferomedial positioned tympanic CN 7
Pearl: Must locate CN 7 for surgeon to ensure safecorrection
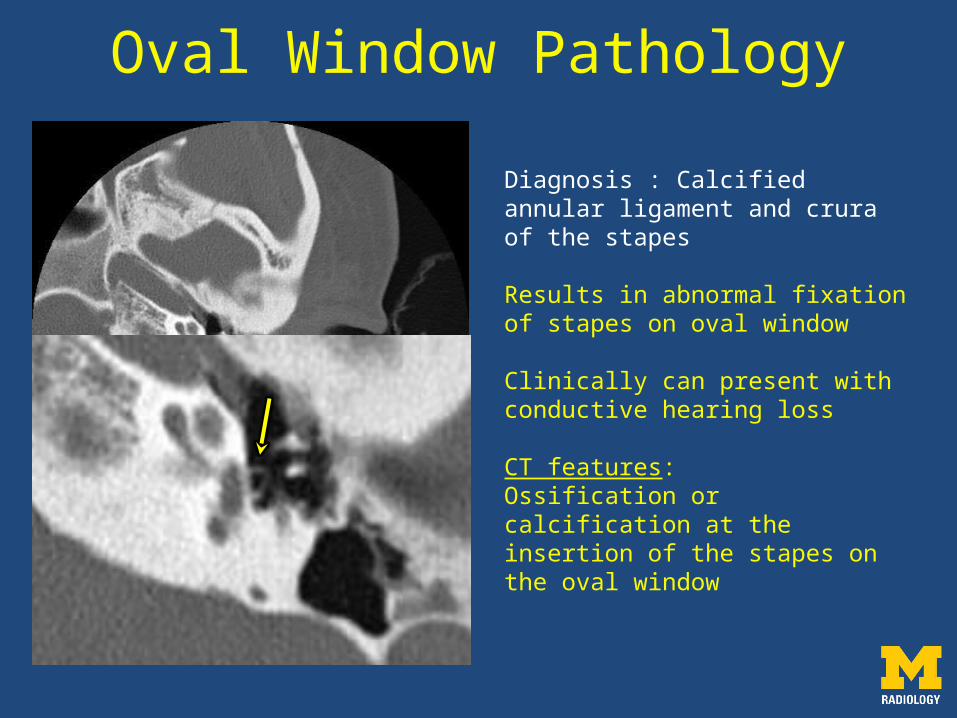
Oval Window Pathology
Diagnosis : Calcified annular ligament and crura of the stapes
Results in abnormal fixation of stapes on oval window
Clinically can present with conductive hearing loss
CT features:Ossification or calcification at the insertion of the stapes on the oval window
• Very rare
• Can have atresia of the round window
Round Window Pathology
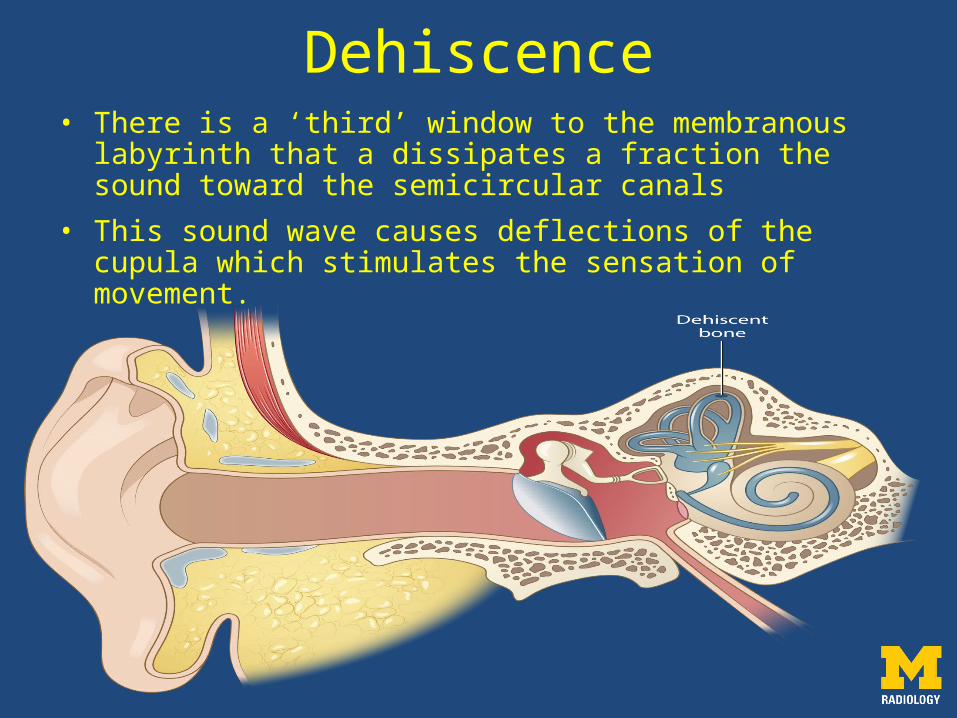
Dehiscence• There is a ‘third’ window to the membranous labyrinth
that a dissipates a fraction the sound toward the semicircular canals
• This sound wave causes deflections of the cupula which stimulates the sensation of movement.
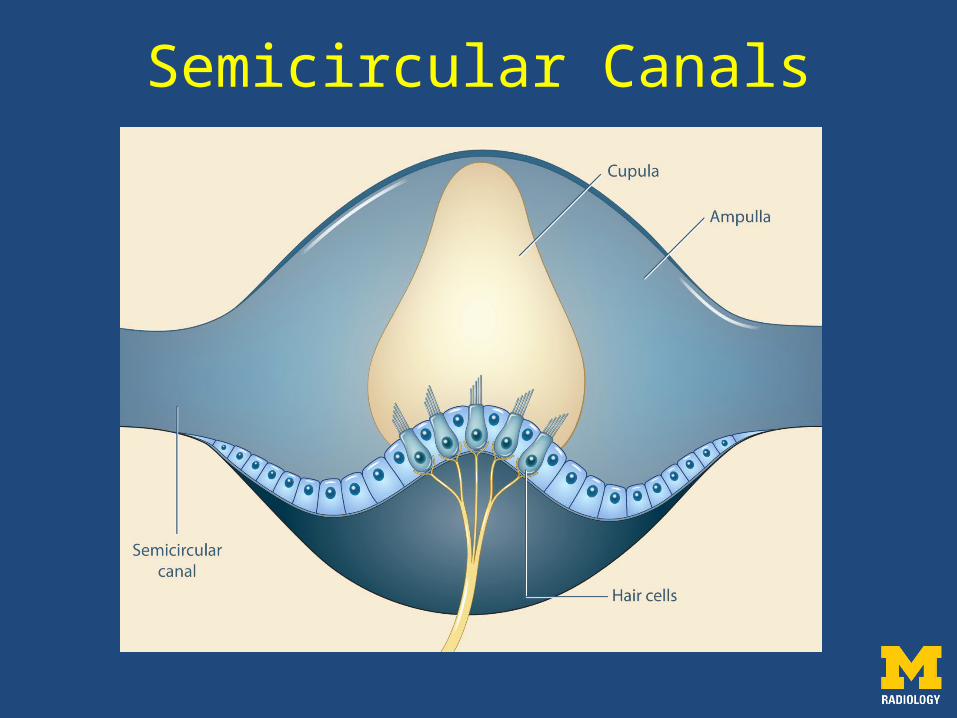
Semicircular Canals

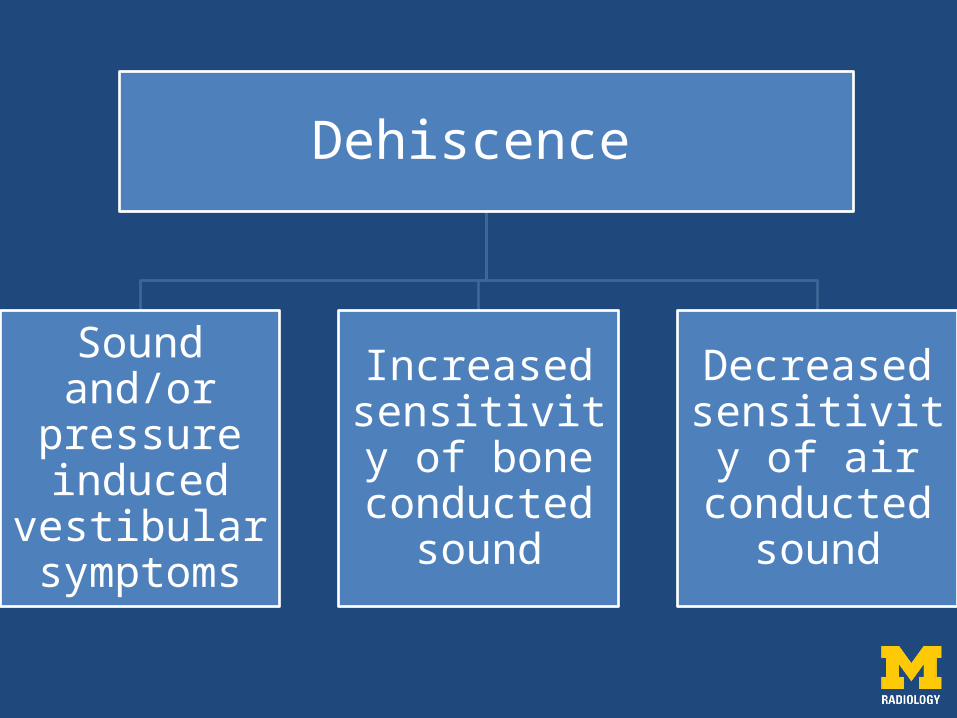
Dehiscence
Sound and/or
pressure induced
vestibular symptoms
Increased sensitivity of
bone conducted
sound
Decreased sensitivity of
air conducted
sound
and decrease sound conduction in cochlea
Sound induced vestibular symptoms
Flow of fluid pressure wave through the dehiscence and away from the vestibule and cochlea
There is excitation of the cupula resulting in motion sensation
Impact on Bone Conducted Hearing
Normally, there is pressure difference between the scala vestibula and scala tympani which allows for perception of bone conducted sound
A pathologic window on the scala vestibula side increases the pressure difference
This causes larger fluid movement of the vestibula side and improves the cochlear response to bone conducted sound
Impact on Air Conducted Hearing
Mechanical pressure wave transmitted onto oval window by stapes
Some perilymph fluid is displaced away from cochlea
This causes decreased response of cochlea to air conducted sound
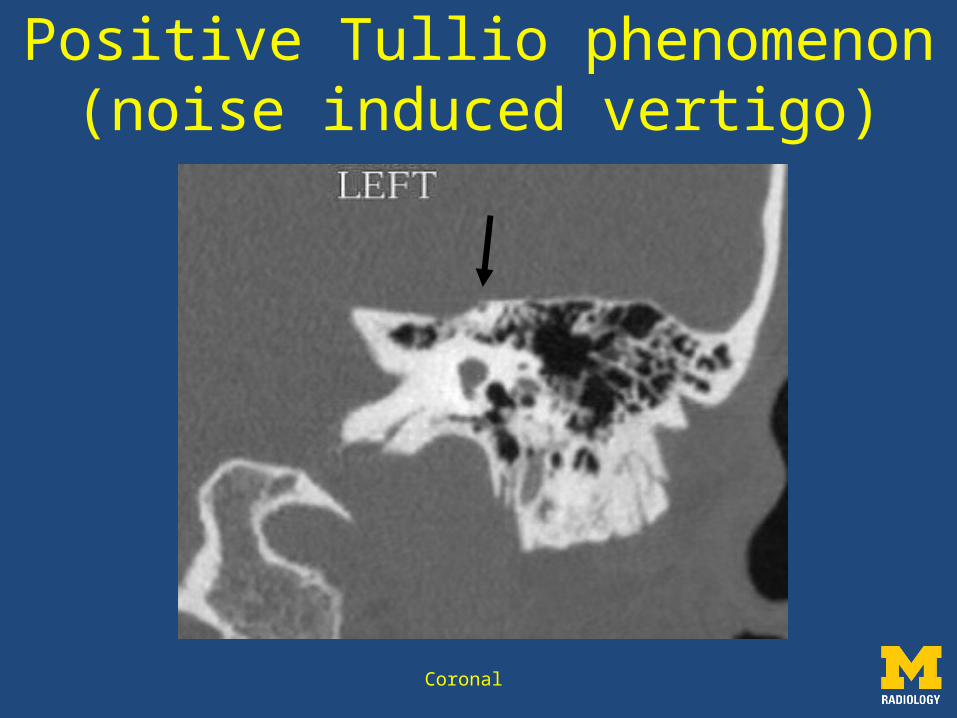
Coronal
Positive Tullio phenomenon(noise induced vertigo)
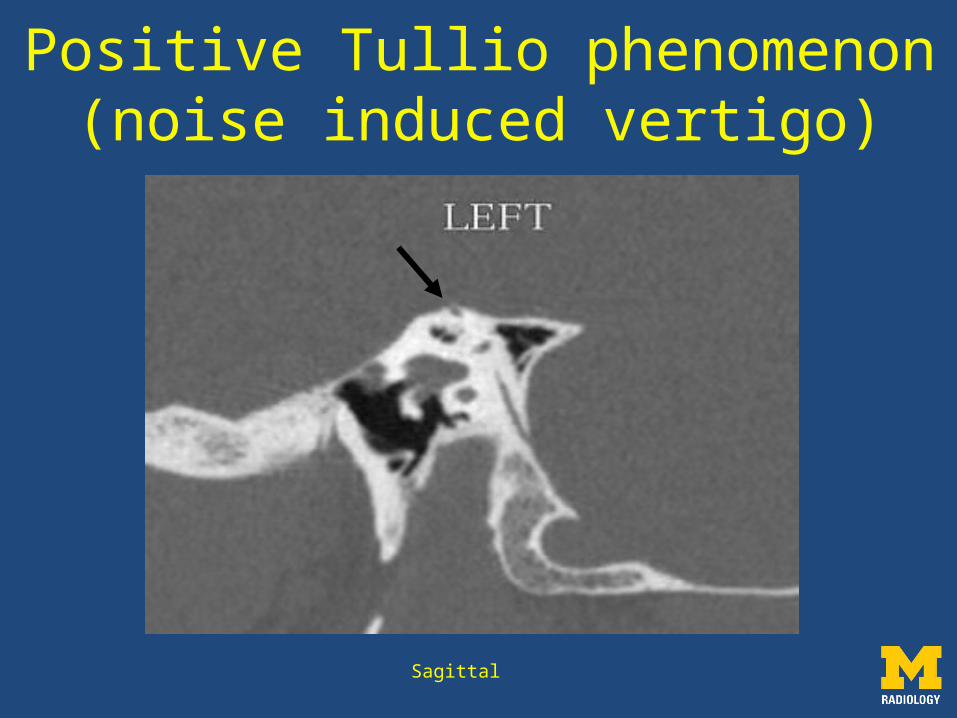
Sagittal
Positive Tullio phenomenon(noise induced vertigo)
• Absence of bony roof of the SSC of unclear etiology
• Thinning of tegmen tympani maybe associated
• Tullio phenomenon is a clinical manifestation with sound induced vertigo and/or nystagmus
• Should be considered in patients with suspected conductive hearing loss but intact TM and normal middle ears
• Pearl: asymptomatic thinning of SSC can occur and usually only seen on one coronal or axial section
Superior Semicircular Canal Dehiscence
• Fascia and/or bone chip plugging of dehiscence
• Resurfacing of the dehiscence with fascia and bone graft
Treatment
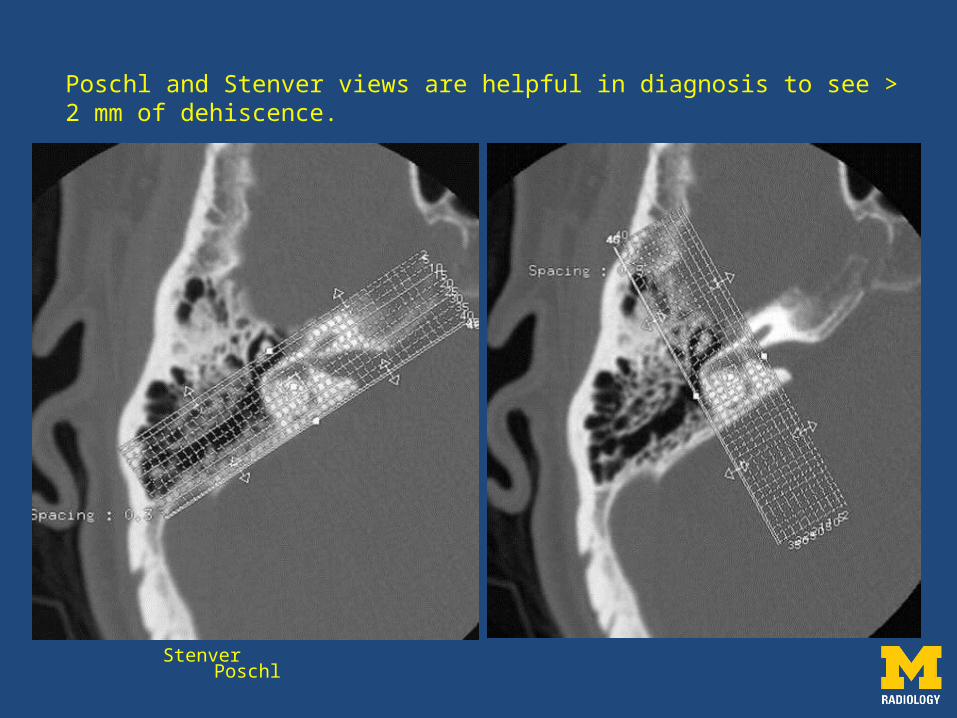
Stenver Poschl
Poschl and Stenver views are helpful in diagnosis to see > 2 mm of dehiscence.
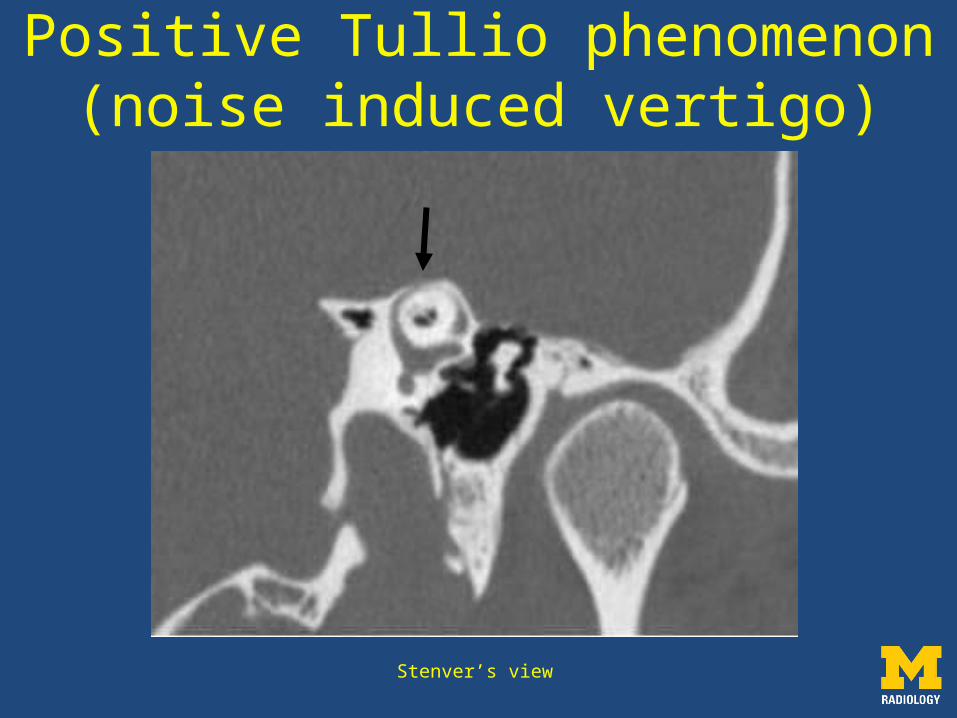
Stenver’s view
Positive Tullio phenomenon(noise induced vertigo)
Other Causes of the ‘Third Window’
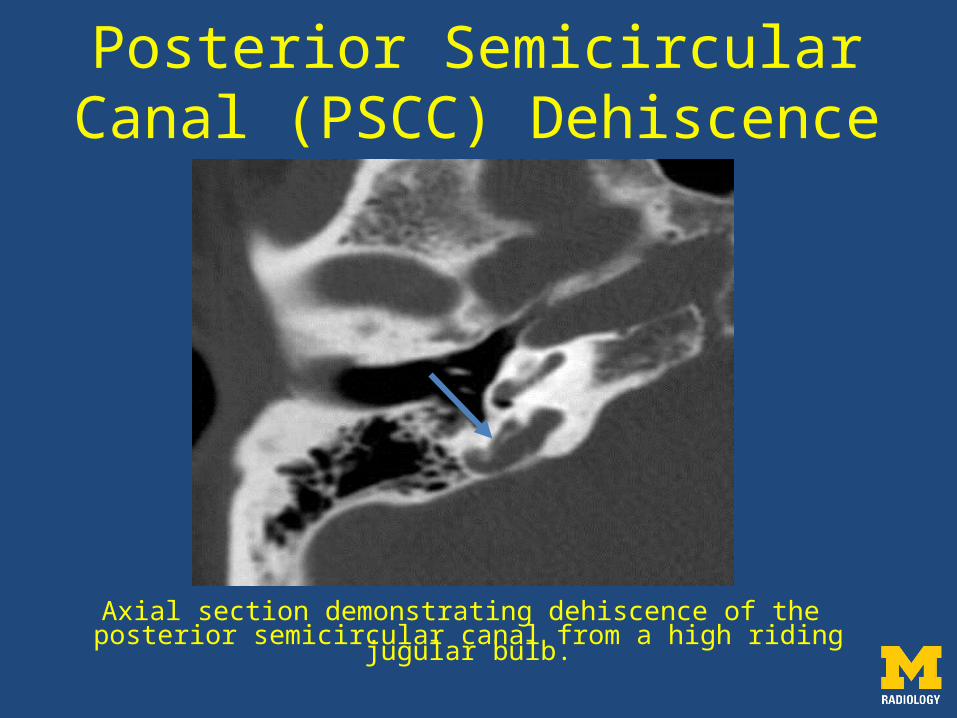
Axial section demonstrating dehiscence of the posterior semicircular canal from a high riding jugular bulb.
Posterior Semicircular Canal (PSCC) Dehiscence
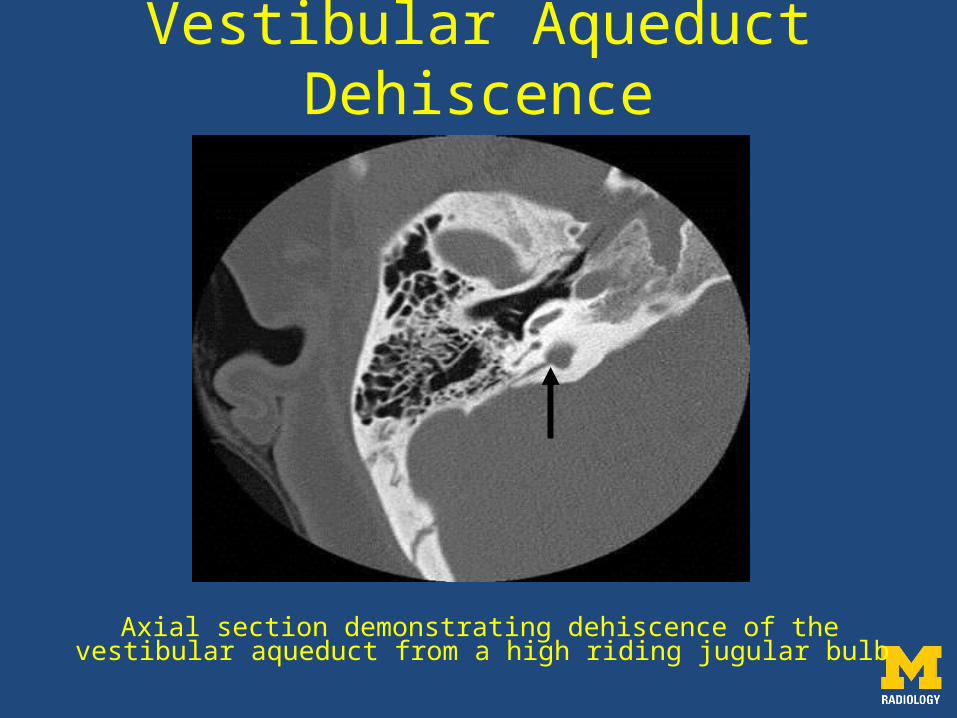
Axial section demonstrating dehiscence of the vestibular aqueduct from a high riding jugular bulb
Vestibular Aqueduct Dehiscence
• Reported incidence is lower than superior semicircular dehiscence
• Frequently due to a high riding jugular bulb
• Diagnosis must be made in conjunction with clinical exam and tests.
PSCC and Vestibular Aqueduct Dehiscence
• Lytic spongy bone of unclear etiology which starts just anterior to oval window (fissula ante fenestram)
• Can progress along medial wall of the middle ear and may involve the cochlear bony labyrinth
• It can cross the stapedial annular ligament and fixate the stapes to the oval window causing conductive hearing loss
Otosclerosis
• This can create a connection between the membranous labyrinth and middle ear results in a pathologic third window
• Fenestral and cochlear otosclerosis do not cause a ‘third’ window phenomenon
Cavitary otosclerosis
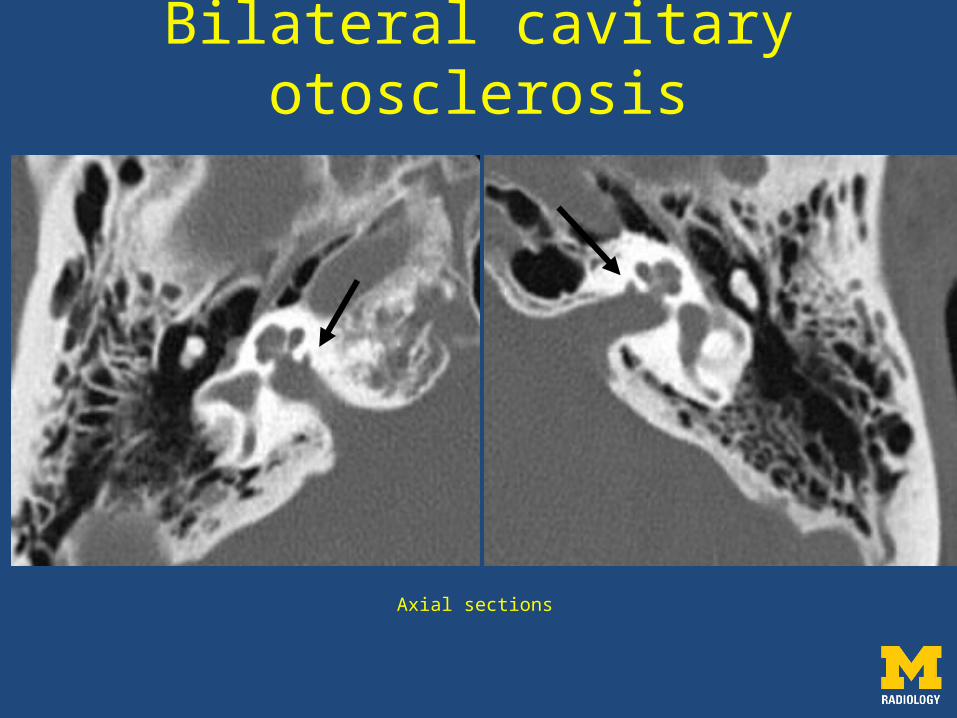
Axial sections
Bilateral cavitary otosclerosis
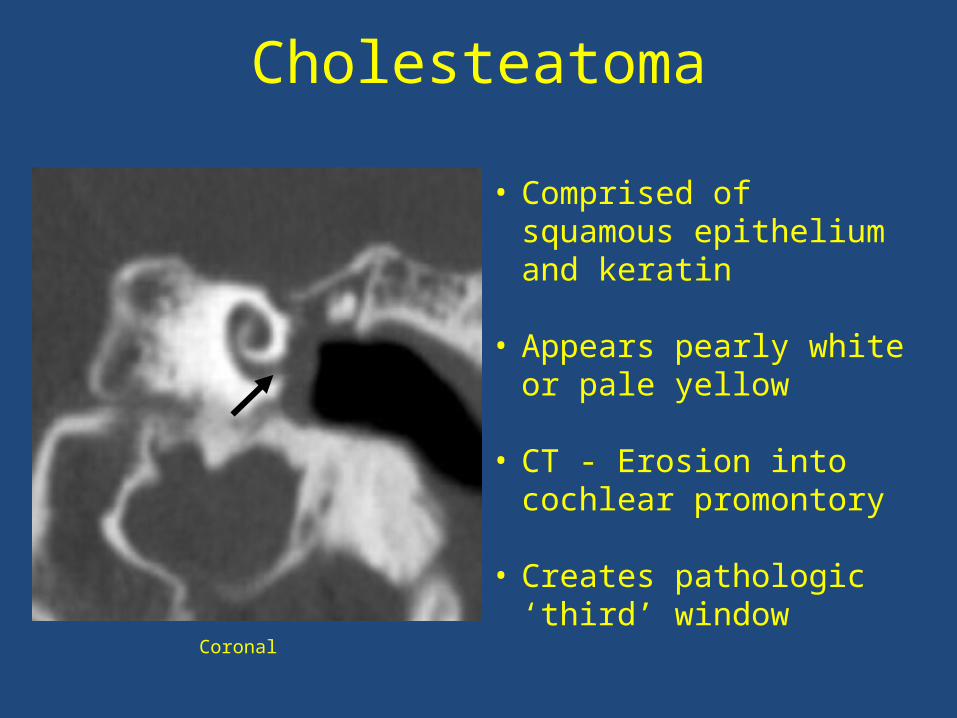
Cholesteatoma
• Comprised of squamous epithelium and keratin
• Appears pearly white or pale yellow
• CT - Erosion into cochlear promontory
• Creates pathologic ‘third’ window
Coronal
• Understanding the complex temporal anatomy is key for interpretation.
• There are many structural causes for conductive hearing loss and identifying the oval and round window pathologies is important.
• There are many causes for the ‘third window’ phenomenon and identifying the various entities is important for clinical management.
Summary
• Bou-Assaly W, Mukherji S, and Srinivasan A. Bilateral Cavitary Otosclerosis: A Rare Presentation of Otosclerosis and Cause of Hearing Loss. Clinical Imaging. 2013; 37:1116-1118. doi.org/10.1016/j.clinimag.2013.07.007
• Merchant S and Rosowski J. Conductive Hearing Loss Caused by Third Window Lesions of the Inner Ear. Otol Neurotol. April 2008; 29(3):282-289. doi:10.1097/mao.0b013e318161ab24.
• Alarcon A, Jahrsdoerfer R, and Kesser B. Congenital Absence of the Oval Window: Diagnosis, Surgery, and Audiometric Outcomes. Otol Neurotol. 2007; 29:23-28.
• Zeifer B, Sabini P, and Sonne J. Congenital Absence of the Oval Window: Radiologic Diagnosis and Associated Anomalies. Am J Neurorad. Feb. 2000; 21:322-327.
• Curtin H. Superior Semicircular Canal Dehiscence Syndrome and Multi-Detector Row CT. Radiol. 2003; 226:312-314.. doi:10.1148/radiol.2262021327.
• Nikkar-Esfahani A, Whelan D, and Banerjee A. Occlusion of the Round Window: A Novel Way to Treat Hyperacusis Symptoms in Superior Semicircular Canal Dehiscence Syndrome. J Laryngo Otol. 2013; 127:705-707. doi:10.1017/S0022215113001096
• Minor L, et al. Dehiscence of Bone Overlying the Superior Canal as a Cause of Apparent Conductive Hearing Loss. Otol Neurotol. 2003; 24:270-278.
• Russo J, et al. Posterior Semicircular Canal Dehiscence: CT Prevalence and Clinical Symptoms. Otol Neurtol. 2014; 35:310-314.
• Hourani R, Carey J, and Yousem D. Dehiscence of the Jugular Bulb and Vestibular Aqueduct: Findings on 200 Consecutive Temporal Bone Computed Tomography Scans. J Comput Assist Tomogr. 2005; 29(5):657-662.
References