Embed Size (px)
Citation preview
UNIVERSITY OF MISSOURI-KANSAS CITY
SCHOOL OF DENTISTRY
UNDERGRADUATE
CLINIC FEE SCHEDULE
OCTOBER, 2007
1.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
INDEX
Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.02
Diagnostics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01-3.02
Emergency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01
Endodontics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.01
Miscellaneous Charges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.01
Operative Dentistry - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.01-5.02
Oral Surgery . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.01-6.02
Orthodontics - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.01-7.02
Payment Procedure:
Discount Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.03
Insurance Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.05
Missouri Medicaid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.05
Payment Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.01
Reduction or Waiver of Fees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.04
Pediatric Dentistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01, 5.01, 5.02, 7.02
Periodontics - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.01
Prosthodontics, Fixed . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9.01
Prosthodontics, Removable . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10.01-10.02
Radiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.02
THE ABBREVIATION, UCF, MEANS USUAL AND CUSTOMARY FEE.
1.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
INDEXConsultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.02
Diagnostics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01-3.02
Emergency . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01
Endodontics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.01
Endodontics - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.01B-1.03B
Miscellaneous Charges . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11.01, 8.01B
Operative Dentistry - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.01-5.02
Operative Dentistry - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.01B-2.02B
Oral Surgery - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.01-6.02
Oral Surgery - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01B-3.03B
Orthodontics - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.01-7.02
Orthodontics - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4.01B-4.02B
Payment Procedure:
Discount Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.03
Insurance Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.05
Missouri Medicaid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.05
Payment Policy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.01
Reduction or Waiver of Fees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2.04
Pediatric Dentistry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.01, 5.01, 5.02, 7.02
Periodontics - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.01
Periodontics - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5.01B-5.02B
Prosthodontics, Fixed - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9.01
Prosthodontics, Fixed - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.01B
Prosthodontics, Removable - Predoctoral Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10.01-10.02
Prosthodontics, Removable - Graduate Clinic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7.01B-7.02B
Radiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3.02
Student Fees . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1.01C-9.02C
THE ABBREVIATION, UCF, MEANS USUAL AND CUSTOMARY FEE.
2.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Payment Policy
It is the general policy of the School of Dentistry not to grant deferred payments for professionaldental treatment. This policy is based on the fact that the professional fee schedule of the Schoolof Dentistry is considerably lower than that found in private dental practices. Payment forbridges, crowns, full and partial removable prosthodontics must be made in full in advanceof any preparation of teeth. The fees for all other dental treatment will be collected during theclinic period in which treatment is performed. Any fee listed with a range, as “individualconsideration”, or any fee not listed should be established in advance of treatment with thedepartment chairperson.
Deferred payments may be extended, subject to the approval of the Dental School BusinessOffice, under the conditions listed below:
1. Clients of welfare and rehabilitation agencies will be extended deferred paymentsonly after the School of Dentistry has received written authorization from theappropriate agency.
2. Patients of the Orthodontics Department may be extended deferred paymentssubject to the approval of the Dental School Business Office.
3. Fees for treatment, other than Orthodontics, exceeding $500, may be consideredfor deferred payment. The deferred payment schedule will require a minimummonthly payment of $50.00 and a maximum of 12 months to pay the balance due. Deferred payment applications are initiated in the Patient Accounts Office and aresubject to approval. There will be a $10.00 credit analysis fee on each approvedDeferred Treatment Contract.
4. Approval of deferred payments for treatment plans under $500 will be consideredonly under circumstances of immediate emergency nature or under conditionswhere denial of credit would detract seriously from a student’s opportunity toreceive needed clinical experience. Such applications for deferred payments willbe considered only upon the recommendation of the student and the AssistantDean for Clinical Programs. Such recommendations for deferred payment willbe made on the forms provided for that purpose. Deferred payments foremergency treatment for the relief of pain or treatment of acute infection or injurymay be made upon the recommendation of the faculty member responsible for thearea of emergency treatment.
2.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Fee Policy Regarding Consultations
Patients seeking or referred for consultation in the area of a department chairperson’s expertisewill be treated in the following manner:
1. The patient will be referred directly to the appropriate Department Chairman.
2. It will be the Department Chairman’s individual prerogative to charge aconsultation fee of $58.00. If the chairperson provides the consultation as acourtesy to the patient, a fee waiver must be executed.
3. In all instances, a patient record must be completed and computer numberassigned. The consultation must be thoroughly documented in the patient record.
4. Customary fees must be charged if any treatment is rendered.

2.0310/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Discount Policy
Discounts will be allowed only if an approved form for the discount has been obtained from thedental school credit manager (Office of Patient Accounts). Such forms will carry an expirationdate and discounts for treatment after that date will require a new authorization form. Discountsapply only to the Predoctoral Dental and Dental Hygiene Clinic. Discounts do not apply inpostgraduate clinics to individuals (including the below descriptions under a and b) under anydiscount codes.
The discount is 50% (except for gold work and veneers as noted in the fee schedule). Discountsare available to the following patients:
a. Full-time academic and non-academic employees of the University of Missouri-Kansas City School of Dentistry, their spouses and dependent children under 21years of age. This also applies to retirees of the University of Missouri-KansasCity School of Dentistry.
b. Dental school students’ parents, spouses and dependent children under 21 years ofage. This is to include undergraduate and graduate dental students, dentalhygiene students, Master’s in Oral Biology and/or Interdisciplinary PhD studentswith the coordinating discipline of Oral Biology, and Truman Medical Centerresidents.
c. Full-time academic and non-academic employees of the University of Missouri-Kansas City School of Dentistry only will receive a 50% discount on Crown andBridge procedures that are performed in the predoctoral clinic and laboratorywork completed in School of Dentistry Laboratory. Outside laboratory casesshould be billed at full fee. Follow the same procedures you use to process allemployee discounts.
Undergraduate and graduate dental school students and dental hygiene student clinic fees will becollected on the basis of the Special Fee Schedule (1.01C to 9.02C) devised for the purpose (bluesection of the Clinic Fee Schedule).
Exceptions to the discount policy will be made only with the approval of the Dean.

2.0410/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Policy on Reduction or Waiver of Dental Feesfor Academic or Professional Reasons
A clinical faculty member may reduce or waive a clinic fee at his/her discretion when treatmentis to be provided as part of a research project; as a demonstration case for student teaching; or asan essential, not otherwise available, aspect of a student’s clinical teaching experience. He/shemay also authorize reduction of the fee to the extent that he/she considers professionally justifiedfor replacement of a restoration or appliance. The approval of the Assistant Dean for ClinicalPrograms will be required if the reduction or waiver exceed $300.00. Written approvalMUST be obtained BEFORE the start of the procedure. NO EXCEPTIONS.
The faculty member will approve the reduction or waiver in the patient record and on the formprovided for this purpose. These forms are available from Patients Accounts.
The following guidelines should be used as an aid to consistency in determining fee waivers forfixed and removable prosthodontics.
Failure from: 0-12 months no fee1-2 years 25% fee2-3 years 50% fee3-4 years 75% feebeyond 4 years total fee
These guidelines do no impose total inflexibility of judgement, but rather afford us the guidanceto be more consistent in our approval of fee waivers.
2.0510/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Clinic Insurance Policy
A. Patient must provide a Dental Insurance Claim Form which can be obtained from theinsured’s employer. The patient information section must be filled out and must besigned in the places where signatures are required. There may be circumstances wheremore than one claim form will be needed.
B. We do not accept “Assignment of Benefits”. Therefore, patients are expected to pay asservices are rendered.
C. Patient Accounts will file the insurance claims daily as treatment is completed. Patientswill be reimbursed by their individual insurance carrier.
Missouri Medicaid
Effective September 1, 2005, Missouri Medicaid for adults will not include dental coverage,except for trauma/disease and some assistance categories. Please continue to take medicaidpatients to Patient Accounts before every appointment since some “assistance” and“trauma/disease” cases may be covered.
Treatment Which Needs Prior Authorization for Payment
The request forms on this treatment with the necessary documents are completed by PatientAccounts, approved and signed by an authorized faculty member, and submitted to JeffersonCity for approval. The approved forms are returned to Patients Accounts. No treatment will berendered on any service requiring prior approval until the School of Dentistry has in theirpossession said approval. Upon receipt of approved predetermination forms the student doctorwill be notified of approval and the time limitations for completion of procedure (the patient’streatment plan must be entered in the computer and required pre-treatment rendered before thepredetermination forms can be filled out by Patient Accounts).

3.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Diagnostics
ADACode Description Fee UCF
EvaluationD0140 Limited Oral Evaluation(Emergency Visit) . . . . . . . . . . $39.00 . . . . . . . . . . . $65.00Examination, intra-oral x-rays (PA’s and BW”s as needed to diagnose specific concern) anddiagnosis.
Patients who are presently assigned to students and are under active treatment should be seen bytheir respective student or by another student in the team. If, in the judgement of facultymember, the emergency is the result of a failure attributable to our responsibility, a fee waivermay be authorized.
D0120 Diagnosis (periodic recall) - Adult . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 44.00D0120 Denture Recall . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 44.00D0150 Diagnosis (initial) - Adult (one time fee) . . . . . . . . . . . . . . 36.00 . . . . . . . . . . . . 76.00
Diagnosis and entry/interpretation of health history (medical and dental).D0150 Diagnosis (transfer) - Adult . . . . . . . . . . . . . . . . . . . . . .No chargeD0170 Re-evaluation/other - limited, problem-focused
(established patient; non-operative visit) . . . . . . . . . . . . . 13.00 . . . . . . . . . . . . 62.00D0180 Diagnosis with periodontal maintenance . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 82.00D0470 Diagnostic Casts . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.00 . . . . . . . . . . . . 95.00
D1120 Pediatric Diagnosis and Prophy . . . . . . . . . . . . . . . . . . . . . 36.00 . . . . . . . . . . . . 56.00Diagnosis, treatment prescription and preventive dentistry including diagnostic casts, patientcounseling, diagnostic tests with the exception of radiographs, recording of plaque scores,patient education and motivation, self-care instruction in toothbrushing, interproximal cleansingand cleansing of existing prosthodontic restorations, complete prophylaxis, topical fluorideapplication (3 or less visits).
D9999 Exit examination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . No charge
3.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
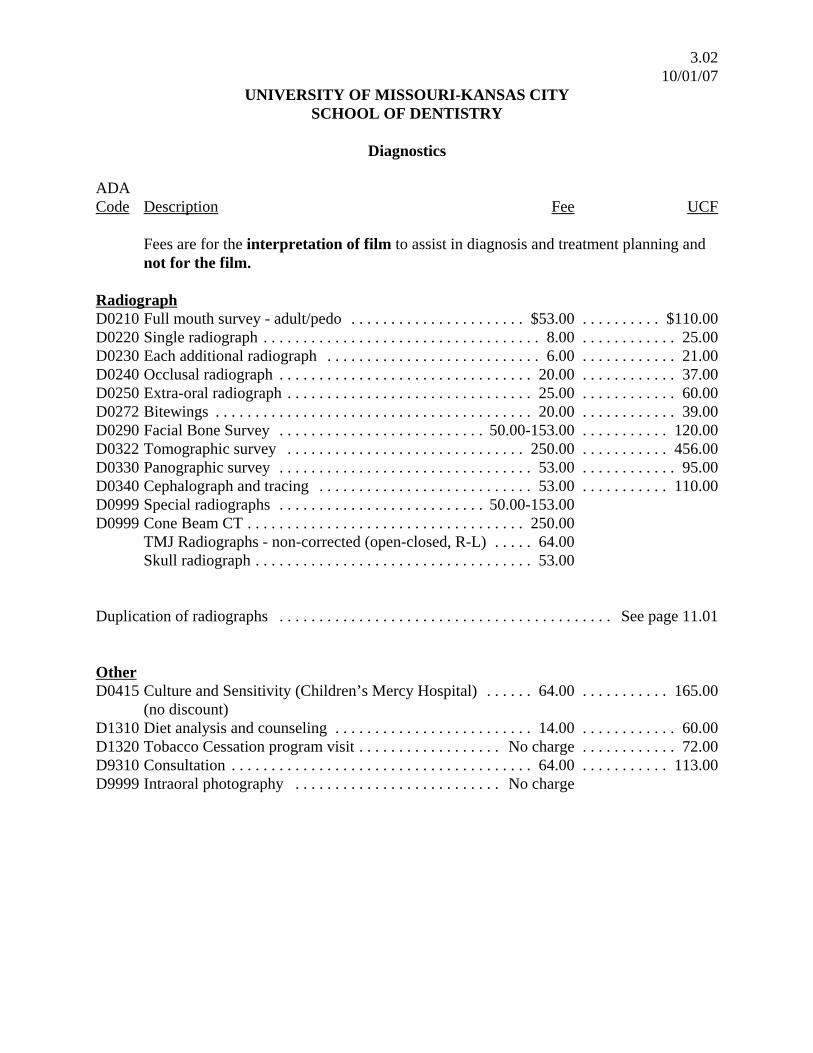
Diagnostics
ADACode Description Fee UCF
Fees are for the interpretation of film to assist in diagnosis and treatment planning andnot for the film.
RadiographD0210 Full mouth survey - adult/pedo . . . . . . . . . . . . . . . . . . . . . . $53.00 . . . . . . . . . . $110.00D0220 Single radiograph . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8.00 . . . . . . . . . . . . 25.00D0230 Each additional radiograph . . . . . . . . . . . . . . . . . . . . . . . . . . . 6.00 . . . . . . . . . . . . 21.00D0240 Occlusal radiograph . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20.00 . . . . . . . . . . . . 37.00D0250 Extra-oral radiograph . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25.00 . . . . . . . . . . . . 60.00D0272 Bitewings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20.00 . . . . . . . . . . . . 39.00D0290 Facial Bone Survey . . . . . . . . . . . . . . . . . . . . . . . . . . 50.00-153.00 . . . . . . . . . . . 120.00D0322 Tomographic survey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 250.00 . . . . . . . . . . . 456.00D0330 Panographic survey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.00 . . . . . . . . . . . . 95.00D0340 Cephalograph and tracing . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.00 . . . . . . . . . . . 110.00D0999 Special radiographs . . . . . . . . . . . . . . . . . . . . . . . . . . 50.00-153.00D0999 Cone Beam CT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 250.00
TMJ Radiographs - non-corrected (open-closed, R-L) . . . . . 64.00Skull radiograph . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.00
Duplication of radiographs . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . See page 11.01
OtherD0415 Culture and Sensitivity (Children’s Mercy Hospital) . . . . . . 64.00 . . . . . . . . . . . 165.00
(no discount)D1310 Diet analysis and counseling . . . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 60.00D1320 Tobacco Cessation program visit . . . . . . . . . . . . . . . . . . No charge . . . . . . . . . . . . 72.00D9310 Consultation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64.00 . . . . . . . . . . . 113.00D9999 Intraoral photography . . . . . . . . . . . . . . . . . . . . . . . . . . No charge
4.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
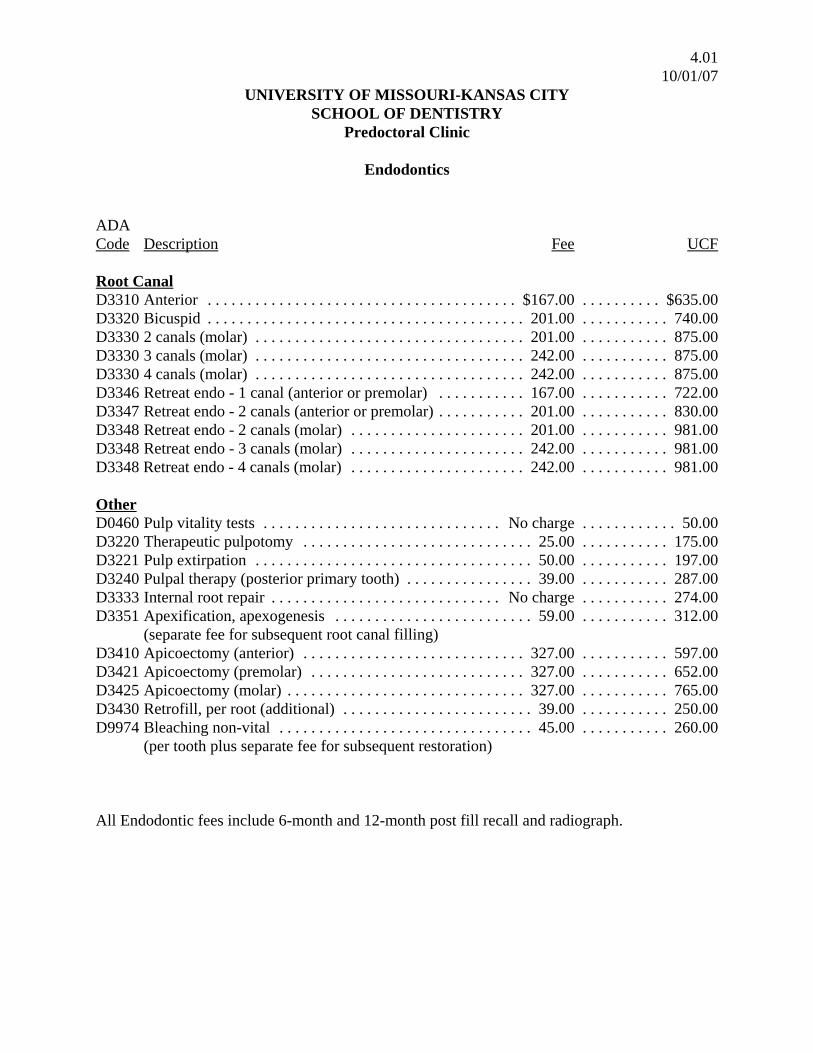
Endodontics
ADACode Description Fee UCF
Root CanalD3310 Anterior . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $167.00 . . . . . . . . . . $635.00D3320 Bicuspid . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201.00 . . . . . . . . . . . 740.00D3330 2 canals (molar) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201.00 . . . . . . . . . . . 875.00D3330 3 canals (molar) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242.00 . . . . . . . . . . . 875.00D3330 4 canals (molar) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 242.00 . . . . . . . . . . . 875.00D3346 Retreat endo - 1 canal (anterior or premolar) . . . . . . . . . . . 167.00 . . . . . . . . . . . 722.00D3347 Retreat endo - 2 canals (anterior or premolar) . . . . . . . . . . . 201.00 . . . . . . . . . . . 830.00D3348 Retreat endo - 2 canals (molar) . . . . . . . . . . . . . . . . . . . . . . 201.00 . . . . . . . . . . . 981.00D3348 Retreat endo - 3 canals (molar) . . . . . . . . . . . . . . . . . . . . . . 242.00 . . . . . . . . . . . 981.00D3348 Retreat endo - 4 canals (molar) . . . . . . . . . . . . . . . . . . . . . . 242.00 . . . . . . . . . . . 981.00
OtherD0460 Pulp vitality tests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . No charge . . . . . . . . . . . . 50.00D3220 Therapeutic pulpotomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25.00 . . . . . . . . . . . 175.00D3221 Pulp extirpation . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50.00 . . . . . . . . . . . 197.00D3240 Pulpal therapy (posterior primary tooth) . . . . . . . . . . . . . . . . 39.00 . . . . . . . . . . . 287.00D3333 Internal root repair . . . . . . . . . . . . . . . . . . . . . . . . . . . . . No charge . . . . . . . . . . . 274.00D3351 Apexification, apexogenesis . . . . . . . . . . . . . . . . . . . . . . . . . 59.00 . . . . . . . . . . . 312.00
(separate fee for subsequent root canal filling)D3410 Apicoectomy (anterior) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327.00 . . . . . . . . . . . 597.00D3421 Apicoectomy (premolar) . . . . . . . . . . . . . . . . . . . . . . . . . . . 327.00 . . . . . . . . . . . 652.00D3425 Apicoectomy (molar) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 327.00 . . . . . . . . . . . 765.00D3430 Retrofill, per root (additional) . . . . . . . . . . . . . . . . . . . . . . . . 39.00 . . . . . . . . . . . 250.00D9974 Bleaching non-vital . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 260.00
(per tooth plus separate fee for subsequent restoration)
All Endodontic fees include 6-month and 12-month post fill recall and radiograph.
5.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
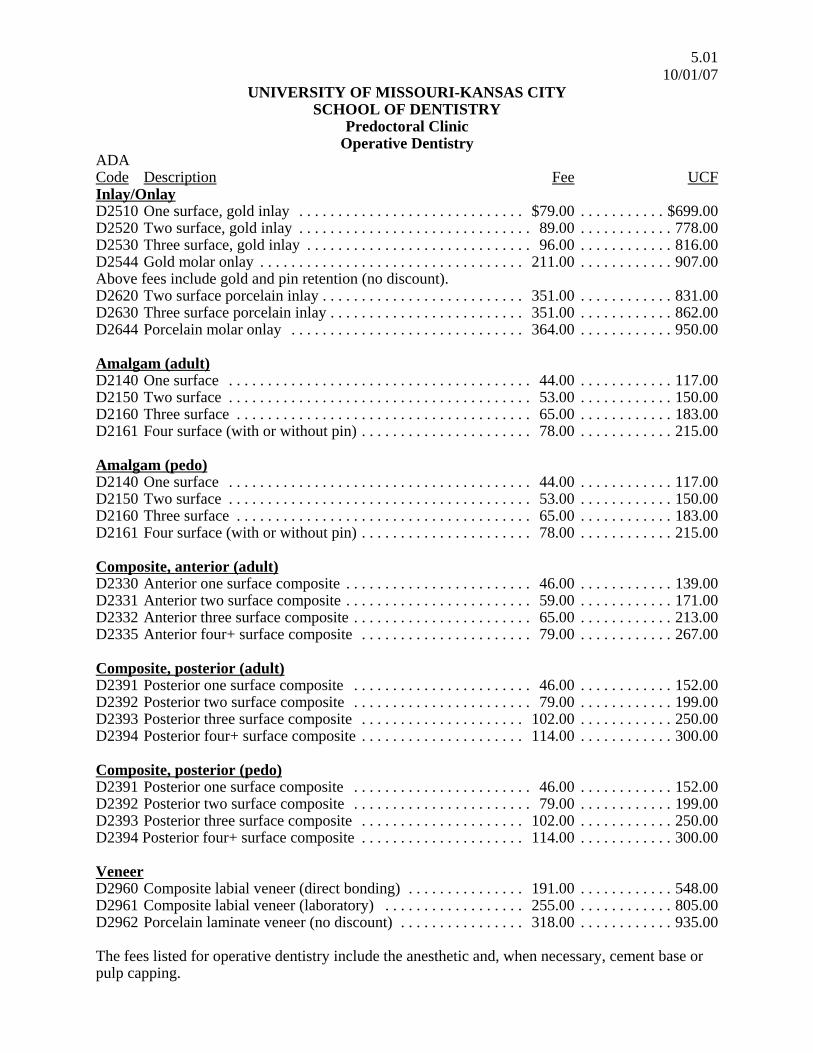
Predoctoral ClinicOperative Dentistry
ADACode Description Fee UCFInlay/OnlayD2510 One surface, gold inlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $79.00 . . . . . . . . . . . $699.00D2520 Two surface, gold inlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89.00 . . . . . . . . . . . . 778.00D2530 Three surface, gold inlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 96.00 . . . . . . . . . . . . 816.00D2544 Gold molar onlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 211.00 . . . . . . . . . . . . 907.00Above fees include gold and pin retention (no discount).D2620 Two surface porcelain inlay . . . . . . . . . . . . . . . . . . . . . . . . . . 351.00 . . . . . . . . . . . . 831.00D2630 Three surface porcelain inlay . . . . . . . . . . . . . . . . . . . . . . . . . 351.00 . . . . . . . . . . . . 862.00D2644 Porcelain molar onlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 364.00 . . . . . . . . . . . . 950.00
Amalgam (adult)D2140 One surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44.00 . . . . . . . . . . . . 117.00D2150 Two surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.00 . . . . . . . . . . . . 150.00D2160 Three surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65.00 . . . . . . . . . . . . 183.00D2161 Four surface (with or without pin) . . . . . . . . . . . . . . . . . . . . . . 78.00 . . . . . . . . . . . . 215.00
Amalgam (pedo)D2140 One surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44.00 . . . . . . . . . . . . 117.00D2150 Two surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.00 . . . . . . . . . . . . 150.00D2160 Three surface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 65.00 . . . . . . . . . . . . 183.00D2161 Four surface (with or without pin) . . . . . . . . . . . . . . . . . . . . . . 78.00 . . . . . . . . . . . . 215.00
Composite, anterior (adult)D2330 Anterior one surface composite . . . . . . . . . . . . . . . . . . . . . . . . 46.00 . . . . . . . . . . . . 139.00D2331 Anterior two surface composite . . . . . . . . . . . . . . . . . . . . . . . . 59.00 . . . . . . . . . . . . 171.00D2332 Anterior three surface composite . . . . . . . . . . . . . . . . . . . . . . . 65.00 . . . . . . . . . . . . 213.00D2335 Anterior four+ surface composite . . . . . . . . . . . . . . . . . . . . . . 79.00 . . . . . . . . . . . . 267.00
Composite, posterior (adult)D2391 Posterior one surface composite . . . . . . . . . . . . . . . . . . . . . . . 46.00 . . . . . . . . . . . . 152.00D2392 Posterior two surface composite . . . . . . . . . . . . . . . . . . . . . . . 79.00 . . . . . . . . . . . . 199.00D2393 Posterior three surface composite . . . . . . . . . . . . . . . . . . . . . 102.00 . . . . . . . . . . . . 250.00D2394 Posterior four+ surface composite . . . . . . . . . . . . . . . . . . . . . 114.00 . . . . . . . . . . . . 300.00
Composite, posterior (pedo)D2391 Posterior one surface composite . . . . . . . . . . . . . . . . . . . . . . . 46.00 . . . . . . . . . . . . 152.00D2392 Posterior two surface composite . . . . . . . . . . . . . . . . . . . . . . . 79.00 . . . . . . . . . . . . 199.00D2393 Posterior three surface composite . . . . . . . . . . . . . . . . . . . . . 102.00 . . . . . . . . . . . . 250.00D2394 Posterior four+ surface composite . . . . . . . . . . . . . . . . . . . . . 114.00 . . . . . . . . . . . . 300.00
VeneerD2960 Composite labial veneer (direct bonding) . . . . . . . . . . . . . . . 191.00 . . . . . . . . . . . . 548.00D2961 Composite labial veneer (laboratory) . . . . . . . . . . . . . . . . . . 255.00 . . . . . . . . . . . . 805.00D2962 Porcelain laminate veneer (no discount) . . . . . . . . . . . . . . . . 318.00 . . . . . . . . . . . . 935.00
The fees listed for operative dentistry include the anesthetic and, when necessary, cement base orpulp capping.
5.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
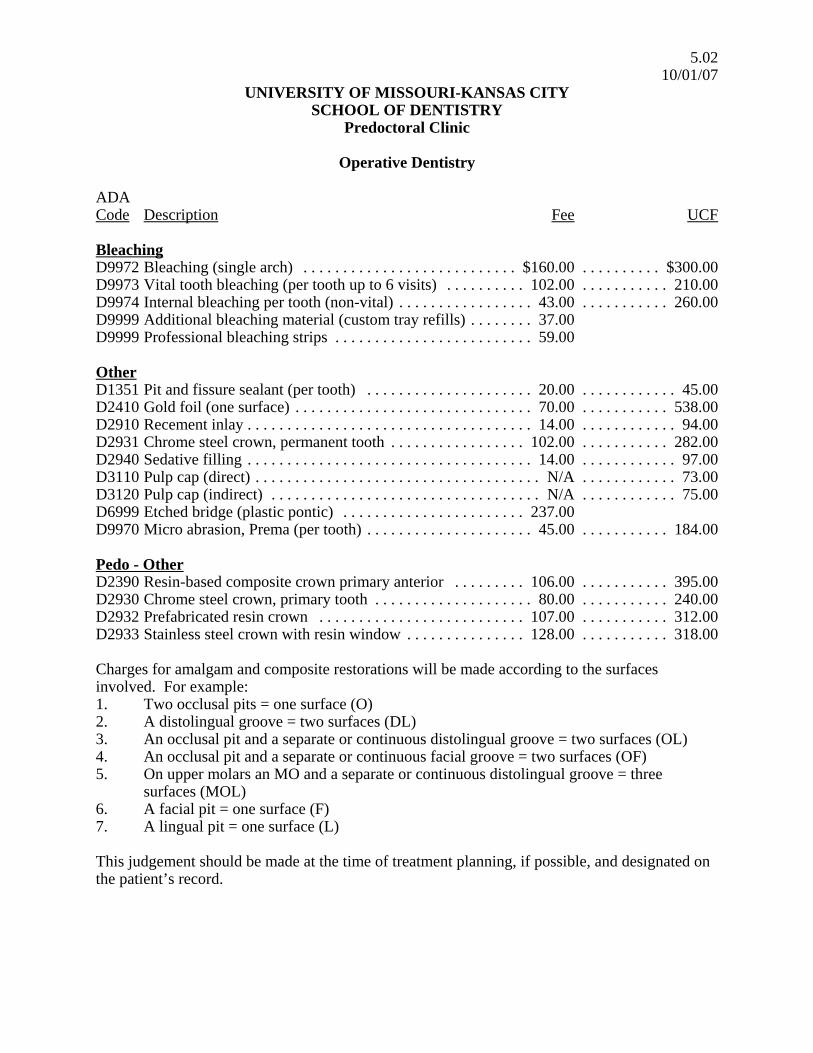
Operative Dentistry
ADACode Description Fee UCF
BleachingD9972 Bleaching (single arch) . . . . . . . . . . . . . . . . . . . . . . . . . . . $160.00 . . . . . . . . . . $300.00D9973 Vital tooth bleaching (per tooth up to 6 visits) . . . . . . . . . . 102.00 . . . . . . . . . . . 210.00D9974 Internal bleaching per tooth (non-vital) . . . . . . . . . . . . . . . . . 43.00 . . . . . . . . . . . 260.00D9999 Additional bleaching material (custom tray refills) . . . . . . . . 37.00D9999 Professional bleaching strips . . . . . . . . . . . . . . . . . . . . . . . . . 59.00
OtherD1351 Pit and fissure sealant (per tooth) . . . . . . . . . . . . . . . . . . . . . 20.00 . . . . . . . . . . . . 45.00D2410 Gold foil (one surface) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 70.00 . . . . . . . . . . . 538.00D2910 Recement inlay . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 94.00D2931 Chrome steel crown, permanent tooth . . . . . . . . . . . . . . . . . 102.00 . . . . . . . . . . . 282.00D2940 Sedative filling . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 97.00D3110 Pulp cap (direct) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . N/A . . . . . . . . . . . . 73.00D3120 Pulp cap (indirect) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . N/A . . . . . . . . . . . . 75.00D6999 Etched bridge (plastic pontic) . . . . . . . . . . . . . . . . . . . . . . . 237.00D9970 Micro abrasion, Prema (per tooth) . . . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 184.00
Pedo - OtherD2390 Resin-based composite crown primary anterior . . . . . . . . . 106.00 . . . . . . . . . . . 395.00D2930 Chrome steel crown, primary tooth . . . . . . . . . . . . . . . . . . . . 80.00 . . . . . . . . . . . 240.00D2932 Prefabricated resin crown . . . . . . . . . . . . . . . . . . . . . . . . . . 107.00 . . . . . . . . . . . 312.00D2933 Stainless steel crown with resin window . . . . . . . . . . . . . . . 128.00 . . . . . . . . . . . 318.00
Charges for amalgam and composite restorations will be made according to the surfacesinvolved. For example:1. Two occlusal pits = one surface (O)2. A distolingual groove = two surfaces (DL)3. An occlusal pit and a separate or continuous distolingual groove = two surfaces (OL)4. An occlusal pit and a separate or continuous facial groove = two surfaces (OF)5. On upper molars an MO and a separate or continuous distolingual groove = three
surfaces (MOL)6. A facial pit = one surface (F)7. A lingual pit = one surface (L)
This judgement should be made at the time of treatment planning, if possible, and designated onthe patient’s record.

6.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Oral Surgery
ADACode Description Fee UCF
Extraction/AlveoplastyD7111 Extraction, crown remnants of deciduous tooth . . . . . . . . . $25.00 . . . . . . . . . . $120.00D7140 Extraction, erupted/exposed teeth or roots . . . . . . . . . . . . . . 50.00 . . . . . . . . . . . 145.00D7210 Extraction, surgical or non-impacted third molars . . . . . . . . 64.00 . . . . . . . . . . . 243.00D7220 Soft tissue impaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89.00 . . . . . . . . . . . 275.00D7230 Partial bone impaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 100.00 . . . . . . . . . . . 350.00D7240 Full bone impaction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 128.00 . . . . . . . . . . . 430.00D7310 Alveoplasty with extractions (per quadrant) . . . . . . . . . . . . . 64.00 . . . . . . . . . . . 256.00D7320 Alveoplasty without extraction (per quadrant) . . . . . . . . . . . 76.00 . . . . . . . . . . . 387.00
Path ExcisionsD7285 Biopsy of oral tissue - hard . . . . . . . . . . . . . . . . . . . 102.00-153.00 . . . . . . . . . . . 362.00D7286 Biopsy of oral tissue - soft . . . . . . . . . . . . . . . . . . . . . 76.00-128.00 . . . . . . . . . . . 276.00D7410 Excision of benign soft tissue lesions up to 1.25 cm.
(including non-odontogenic cysts) . . . . . . . . . . . . . . . 76.00-140.00 . . . . . . . . . . . 365.00D7450 Removal of benign intraosseous odontogenic
cyst or tumor up to 1.25 cm. . . . . . . . . . . . . . . . . . . . 70.00-153.00 . . . . . . . . . . . 501.00D7460 Removal of benign intraosseous non-odontogenic
cyst or tumor up to 1.25 cm. . . . . . . . . . . . . . . . . . . . 70.00-153.00 . . . . . . . . . . . 500.00
Pre-ProstheticD7471 Removal of lateral exostosis (maxilla or mandible,
per quadrant) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 95.00 . . . . . . . . . . . 757.00D7472 Removal of torus palatinus . . . . . . . . . . . . . . . . . . . . 89.00-166.00 . . . . . . . . . . . 716.00D7473 Removal of torus mandibularis (per quadrant) . . . . . . 39.00-68.00 . . . . . . . . . . . 669.00D7485 Surgical reduction of osseous tuberosity . . . . . . . . . 128.00-166.00 . . . . . . . . . . . 609.00D7960 Frenectomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114.00 . . . . . . . . . . . 400.00D7970 Excision of hyperplastic tissue (per arch) . . . . . . . . . 89.00-166.00 . . . . . . . . . . . 467.00
(for epulis with tissue reattachments, see Vestibuloplasty, D7340/7350)D7972 Surgical reduction of fibrous tuberosity . . . . . . . . . . 89.00-128.00 . . . . . . . . . . . 735.00

6.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Oral Surgery
ADACode Description Fee UCF
Infections, Trauma, TMJD7270 Tooth reimplantation and/or stabilization accidentally
evulsed tooth (per tooth) . . . . . . . . . . . . . . . . . . . . . . . . . . . $45.00 . . . . . . . . . . . 495.00D7510 Incise and drain (intra-oral) . . . . . . . . . . . . . . . . . . . . . . . . . . 76.00 . . . . . . . . . . . 200.00D7520 Incise and drain (extra-oral) . . . . . . . . . . . . . . . . . . . . . . . . . 153.00 . . . . . . . . . . . 388.00D7530 Removal of foreign body from oral soft tissues . . . . . 39.00-128.00 . . . . . . . . . . . 320.00D7550 Sequestrectomy for removal of non-vital bone . . . . . 25.00-191.00 . . . . . . . . . . . 504.00D7560 Caldwell-Luc procedure . . . . . . . . . . . . . . . . . . . . . . . . . . . 224.00 . . . . . . . . . . 1,172.00D7771 Stabilize alveolar fracture . . . . . . . . . . . . . . . . . . . . . . . . . . 191.00 . . . . . . . . . . 1,513.00D7910 Suture of recent small wounds up to 5cm (superficial)89.00-198.00 . . . . . . . . . . . 275.00D7980 Sialolithotomy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 166.00 . . . . . . . . . . . 705.00D7995 Synthetic graft - mandible or facial bones . . . . . . . . . 89.00-445.00
OthersD9610 Medications (therapeutic drug injection) . . . . . . . Per prices below . . . . . . . . . . . . 77.00
Corticosteroid injection . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.00Vancomycin IV . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 191.00Ampicillin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39.00Gentamycin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 39.00
D9630 Other drugs and/or medicaments . . . . . . . . . . . . . Per prices below . . . . . . . . . . . . 35.00Oral antibiotics (no discount) . . . . . . . . . . . . . . . . . . . . . . . . . 9.00Oral steroids (no discount) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9.00
D9999 INR/protime blood study . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25.00
AnesthesiaD9230 Nitrous Oxide analgesia/sedation . . . . . . . . . . . . . . . . . . . . . 49.00 . . . . . . . . . . . . 67.00D9248 Non parenteral sedation/analgesia administration/
monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64.00 . . . . . . . . . . . 300.00
7.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
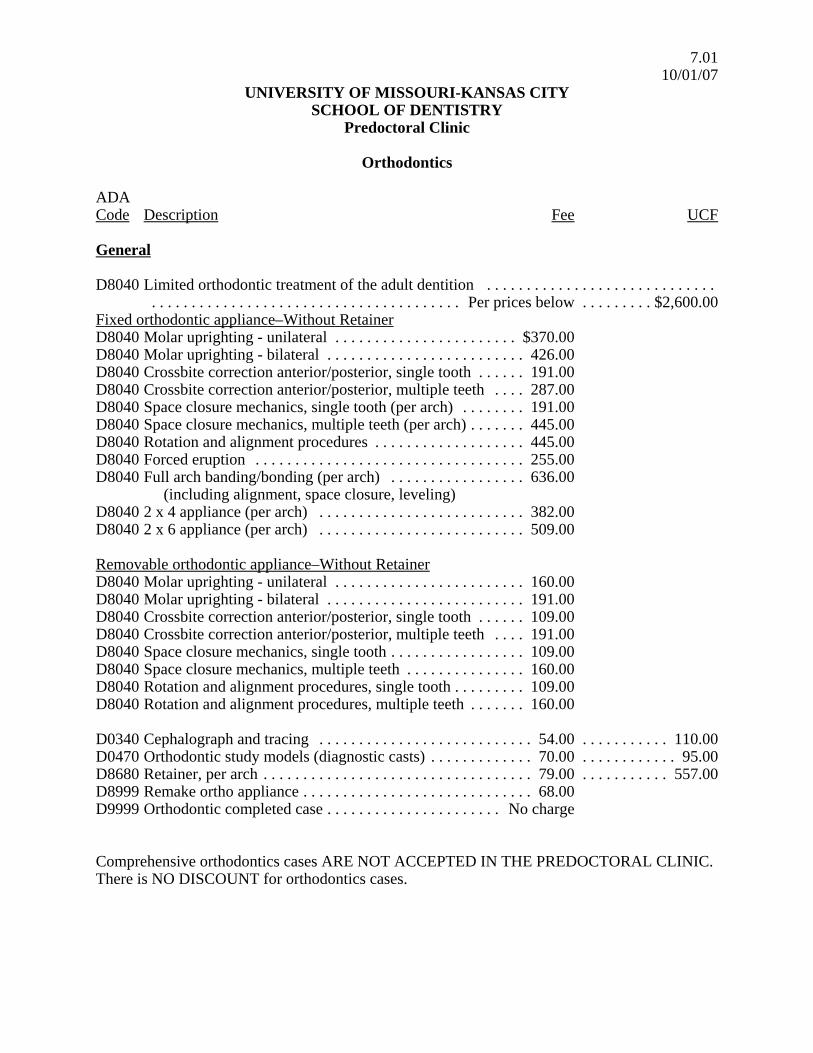
Orthodontics
ADACode Description Fee UCF
General
D8040 Limited orthodontic treatment of the adult dentition . . . . . . . . . . . . . . . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Per prices below . . . . . . . . . $2,600.00
Fixed orthodontic appliance–Without RetainerD8040 Molar uprighting - unilateral . . . . . . . . . . . . . . . . . . . . . . . $370.00D8040 Molar uprighting - bilateral . . . . . . . . . . . . . . . . . . . . . . . . . 426.00D8040 Crossbite correction anterior/posterior, single tooth . . . . . . 191.00D8040 Crossbite correction anterior/posterior, multiple teeth . . . . 287.00D8040 Space closure mechanics, single tooth (per arch) . . . . . . . . 191.00D8040 Space closure mechanics, multiple teeth (per arch) . . . . . . . 445.00D8040 Rotation and alignment procedures . . . . . . . . . . . . . . . . . . . 445.00D8040 Forced eruption . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 255.00D8040 Full arch banding/bonding (per arch) . . . . . . . . . . . . . . . . . 636.00
(including alignment, space closure, leveling)D8040 2 x 4 appliance (per arch) . . . . . . . . . . . . . . . . . . . . . . . . . . 382.00D8040 2 x 6 appliance (per arch) . . . . . . . . . . . . . . . . . . . . . . . . . . 509.00
Removable orthodontic appliance–Without RetainerD8040 Molar uprighting - unilateral . . . . . . . . . . . . . . . . . . . . . . . . 160.00D8040 Molar uprighting - bilateral . . . . . . . . . . . . . . . . . . . . . . . . . 191.00D8040 Crossbite correction anterior/posterior, single tooth . . . . . . 109.00D8040 Crossbite correction anterior/posterior, multiple teeth . . . . 191.00D8040 Space closure mechanics, single tooth . . . . . . . . . . . . . . . . . 109.00D8040 Space closure mechanics, multiple teeth . . . . . . . . . . . . . . . 160.00D8040 Rotation and alignment procedures, single tooth . . . . . . . . . 109.00D8040 Rotation and alignment procedures, multiple teeth . . . . . . . 160.00
D0340 Cephalograph and tracing . . . . . . . . . . . . . . . . . . . . . . . . . . . 54.00 . . . . . . . . . . . 110.00D0470 Orthodontic study models (diagnostic casts) . . . . . . . . . . . . . 70.00 . . . . . . . . . . . . 95.00D8680 Retainer, per arch . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 79.00 . . . . . . . . . . . 557.00D8999 Remake ortho appliance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 68.00D9999 Orthodontic completed case . . . . . . . . . . . . . . . . . . . . . . No charge
Comprehensive orthodontics cases ARE NOT ACCEPTED IN THE PREDOCTORAL CLINIC.There is NO DISCOUNT for orthodontics cases.

7.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Orthodontics
ADACode Description Fee UCF
Pedo ApplianceD1510 Unilateral space maintainer . . . . . . . . . . . . . . . . . . . . . . . . . $76.00 . . . . . . . . . . $275.00
(C.S.C. or bank and loop or bar)D1515 Bilateral space maintainer, fixed . . . . . . . . . . . . . . . . . . . . . . 98.00 . . . . . . . . . . . 375.00
(lingual or palatal arch)D1525 Bilateral space maintainer, removable . . . . . . . . . . . . . . . . . . 76.00 . . . . . . . . . . . 426.00
(acrylic saddles with CS bar)D1550 Recement space maintainer . . . . . . . . . . . . . . . . . . . . . . . . . . . N/A . . . . . . . . . . . . 70.00D8210 Hawley retainer (removable appliance therapy) . . . . . . . . . . 98.00 . . . . . . . . . . . 800.00D8220 Fixed appliance therapy . . . . . . . . . . . . . . . . . . . Per prices below . . . . . . . . . . . 925.00
(treatment to control harmful habits)D8220 Tongue thrust appliance (habit appliance) . . . . . . . . . . . . . . . 98.00D8220 Space regainer . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98.00D8220 Posterior crossbite appliance, bands and elastics . . . . . . . . . 76.00D8220 Ectopic molar movement . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.00
(deimpactor or brass ligature)Quadhelix (jackscrew appliance) . . . . . . . . . . . . . . . . . . . . . 128.00
D8999 Adjustment to quadhelix (each month after placement) . . . . 43.00 . . . . . . . . . . . . 50.00

8.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral ClinicPeriodontics
ADACode Description Fee UCFPreventive or MaintenanceD1110 Adult prophy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $50.00 . . . . . . . . . . . $76.00
10 teeth or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.00 . . . . . . . . . . . . 76.00D4910 Periodontal maintenance . . . . . . . . . . . . . . . . . . . . . . . . . . . . 50.00 . . . . . . . . . . . 122.00
10 teeth or less . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34.00 . . . . . . . . . . . 122.00
Therapeutic/GingivitisD1110 Adult prophy and gingivitis . . . . . . . . . . . . . . . . . . . . . . . . . . 64.00 . . . . . . . . . . . . 76.00D4999 Re-evaluation and deplaque . . . . . . . . . . . . . . . . . . . . . . . . . . 13.00 . . . . . . . . . . . . 45.00
Therapeutic/PeriodontitisD4341 Scaling/root planing (UR), 4-8 teeth per quadrant . . . . . . . . 65.00 . . . . . . . . . . . 220.00D4341 Scaling/root planing (LR), 4-8 teeth per quadrant . . . . . . . . . 65.00 . . . . . . . . . . . 220.00D4341 Scaling/root planing (UL), 4-8 teeth per quadrant . . . . . . . . . 65.00 . . . . . . . . . . . 220.00D4341 Scaling/root planing (LL), 4-8 teeth per quadrant . . . . . . . . . 65.00 . . . . . . . . . . . 220.00D4999 Scaling of non RP teeth per quad, UR, LR, UL, LL . . . . . . . . 6.00D4342 Scaling/root planing (UR), 1-3 teeth per quadrant . . . . . . . . 38.00 . . . . . . . . . . . 159.00D4342 Scaling/root planing (LR), 1-3 teeth per quadrant . . . . . . . . . 38.00 . . . . . . . . . . . 159.00D4342 Scaling/root planing (UL), 1-3 teeth per quadrant . . . . . . . . . 38.00 . . . . . . . . . . . 159.00D4342 Scaling/root planing (LL), 1-3 teeth per quadrant . . . . . . . . . 38.00 . . . . . . . . . . . 159.00D4999 Re-evaluation and deplaque . . . . . . . . . . . . . . . . . . . . . . . . . . 13.00 . . . . . . . . . . . . 45.00
OtherD1205 Topical application of fluoride (with prophy) . . . . . . . . . . . . 14.00 . . . . . . . . . . . . 97.00D4210 Gingivectomy/gingivoplasty per quadrant
(and their interproximal areas) . . 65.00+22.00 per additional tooth . . . . . . . . . . . 565.00D4240 Gingival flap . . . . . . . . . . . . . . . 90.00+15.00 per additional tooth . . . 654.00 quadrantD4249 Crown lengthening . . . . . . . . . . 90.00+15.00 per additional tooth . . . . . . . . . . . 675.00
(apically positioned flap)D4274 Distal or proximal wedge procedure . . . . . . . . . . . . . . . . . . . 90.00 . . . . . . . . . . . 615.00D4355 Full mouth debridement for comprehensive diagnosis . . . . . 26.00 . . . . . . . . . . . 164.00D4381 Atridox (per tube) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27.00 . . . . . . . . . . . 160.00D4381 Arestin (two syringes) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 27.00 . . . . . . . . . . . 160.00D5986 Custom fluoride trays (both arches) . . . . . . . . . . . . . . . . . . . . 34.00 . . . . . . . . . . . 194.00D9910 Finishing procedure following periodontal surgery,
fluoride treatment, desensitization, and polishing.Per tooth (maximum $20 per patient) . . . . . . . . . . . . . . . . . . 13.00 . . . . . . . . . . . . 57.00
D9940 Night guard/occlusal guard (TMJ splint completed by 4th
year only in the Special Patient Care area) . . . . . . . . . . . . . 160.00 . . . . . . . . . . . 545.00D9940 Night guard (completed by outside laboratory) . . . . . . . . . . 268.00 . . . . . . . . . . . 545.00D9951 Limited occlusal adjustment . . . . . . . . . . . . . . . . . . . . . . . . . 18.00 . . . . . . . . . . . 160.00D4381 OraQuix . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10.00
9.014/28/08
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
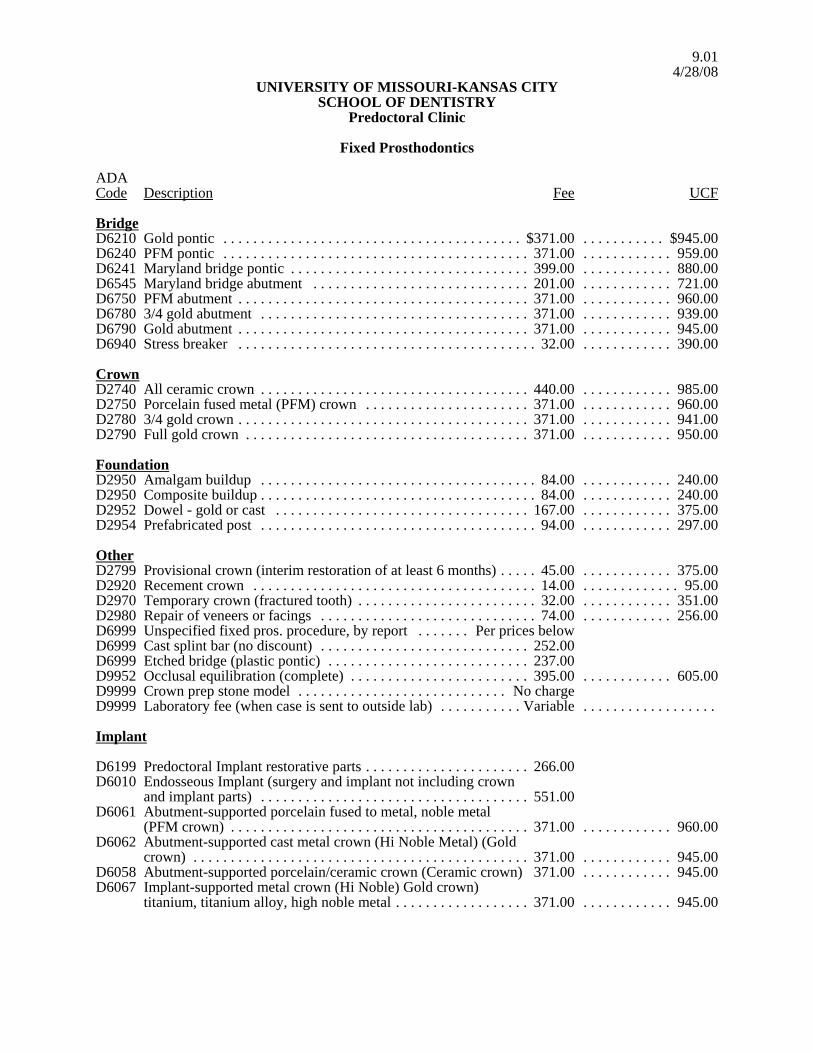
Fixed Prosthodontics
ADACode Description Fee UCF
BridgeD6210 Gold pontic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $371.00 . . . . . . . . . . . $945.00D6240 PFM pontic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 959.00D6241 Maryland bridge pontic . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 399.00 . . . . . . . . . . . . 880.00D6545 Maryland bridge abutment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 201.00 . . . . . . . . . . . . 721.00D6750 PFM abutment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 960.00D6780 3/4 gold abutment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 939.00D6790 Gold abutment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 945.00D6940 Stress breaker . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.00 . . . . . . . . . . . . 390.00
CrownD2740 All ceramic crown . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 440.00 . . . . . . . . . . . . 985.00D2750 Porcelain fused metal (PFM) crown . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 960.00D2780 3/4 gold crown . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 941.00D2790 Full gold crown . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 950.00
FoundationD2950 Amalgam buildup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84.00 . . . . . . . . . . . . 240.00D2950 Composite buildup . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84.00 . . . . . . . . . . . . 240.00D2952 Dowel - gold or cast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 167.00 . . . . . . . . . . . . 375.00D2954 Prefabricated post . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94.00 . . . . . . . . . . . . 297.00
OtherD2799 Provisional crown (interim restoration of at least 6 months) . . . . . 45.00 . . . . . . . . . . . . 375.00D2920 Recement crown . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . . . 95.00D2970 Temporary crown (fractured tooth) . . . . . . . . . . . . . . . . . . . . . . . . 32.00 . . . . . . . . . . . . 351.00D2980 Repair of veneers or facings . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.00 . . . . . . . . . . . . 256.00D6999 Unspecified fixed pros. procedure, by report . . . . . . . Per prices belowD6999 Cast splint bar (no discount) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 252.00D6999 Etched bridge (plastic pontic) . . . . . . . . . . . . . . . . . . . . . . . . . . . 237.00D9952 Occlusal equilibration (complete) . . . . . . . . . . . . . . . . . . . . . . . . 395.00 . . . . . . . . . . . . 605.00D9999 Crown prep stone model . . . . . . . . . . . . . . . . . . . . . . . . . . . . No chargeD9999 Laboratory fee (when case is sent to outside lab) . . . . . . . . . . . Variable . . . . . . . . . . . . . . . . . .
Implant
D6199 Predoctoral Implant restorative parts . . . . . . . . . . . . . . . . . . . . . . 266.00D6010 Endosseous Implant (surgery and implant not including crown
and implant parts) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 551.00D6061 Abutment-supported porcelain fused to metal, noble metal
(PFM crown) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 960.00D6062 Abutment-supported cast metal crown (Hi Noble Metal) (Gold
crown) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 945.00D6058 Abutment-supported porcelain/ceramic crown (Ceramic crown) 371.00 . . . . . . . . . . . . 945.00D6067 Implant-supported metal crown (Hi Noble) Gold crown)
titanium, titanium alloy, high noble metal . . . . . . . . . . . . . . . . . . 371.00 . . . . . . . . . . . . 945.00
9.024/28/08
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
ADACode Description Fee UCF
D6066 Implant supported porcelain fused to metal (PFM crown)titanium, titanium alloy, high noble metal 371.00 . . . . . . . . . . . . 960.00
D0605 Implant supported porcelain/ceramic crown (ceramic crown) 371.00 . . . . . . . . . . . . 960.00
Twins Program See Page 10.02.
All fees include gold alloy when applicable (no discount on crowns, dowels, porcelain laminateveneers).

10.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Removable Prosthodontics
ADACode Description Fee UCF
Full DentureD5110 Maxillary denture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . $399.00 . . . . . . . . . $1,485.00D5120 Mandibular denture . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 399.00 . . . . . . . . . . 1,485.00D5130 Immediate maxillary denture . . . . . . . . . . . . . . . . . . . . . . . . 532.00 . . . . . . . . . . 1,581.00
(including one rebase or one reline)D5140 Immediate mandibular denture . . . . . . . . . . . . . . . . . . . . . . 532.00 . . . . . . . . . . 1,581.00
(including one rebase or one reline)D5860 Tooth supported denture (overdenture) . . . . . . . . . . . . . . . . 399.00 . . . . . . . . . . 1,783.00
Partial DentureD5211 Maxillary partial (resin base) . . . . . . . . . . . . . . . . . . . . . . . . 344.00 . . . . . . . . . . 1,175.00D5212 Mandibular partial (resin base) . . . . . . . . . . . . . . . . . . . . . . 344.00 . . . . . . . . . . 1,116.00D5213 Maxillary partial (cast framework) . . . . . . . . . . . . . . . . . . . 466.00 . . . . . . . . . . 1,552.00D5214 Mandibular partial (cast framework) . . . . . . . . . . . . . . . . . . 466.00 . . . . . . . . . . 1,562.00D5820 Transitional partial - maxillary (flipper) . . . . . . . . . . . . . . . 166.00 . . . . . . . . . . . 608.00D5821 Transitional partial - mandibular (flipper) . . . . . . . . . . . . . . 166.00 . . . . . . . . . . . 610.00
Reline/RebaseD5710 Rebase - maxillary denture . . . . . . . . . . . . . . . . . . . . . . . . . 122.00 . . . . . . . . . . . 511.00D5711 Rebase - mandibular denture . . . . . . . . . . . . . . . . . . . . . . . . 122.00 . . . . . . . . . . . 509.00D5720 Rebase - maxillary partial . . . . . . . . . . . . . . . . . . . . . . . . . . 110.00 . . . . . . . . . . . 495.00D5721 Rebase - mandibular partial . . . . . . . . . . . . . . . . . . . . . . . . . 110.00 . . . . . . . . . . . 497.00D5730 Reline maxillary denture (chairside) . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 335.00D5731 Reline mandibular denture (chairside) . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 335.00D5750 Reline - maxillary denture . . . . . . . . . . . . . . . . . . . . . . . . . . . 88.00 . . . . . . . . . . . 415.00D5751 Reline - mandibular denture . . . . . . . . . . . . . . . . . . . . . . . . . 88.00 . . . . . . . . . . . 416.00D5760 Reline - maxillary partial . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.00 . . . . . . . . . . . 410.00D5761 Reline - mandibular partial . . . . . . . . . . . . . . . . . . . . . . . . . . 74.00 . . . . . . . . . . . 410.00
Twins Program See page 10.02.
If a denture is not satisfactory, please be sure patient understands they have an option - moneyrefunded or denture remade (with first denture returned). No third denture remakes. If remake ischosen, no money will be refunded. Original denture must be returned if refund requested.
10.0210/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Removable Prosthodontics
ADACode Description Fee UCF
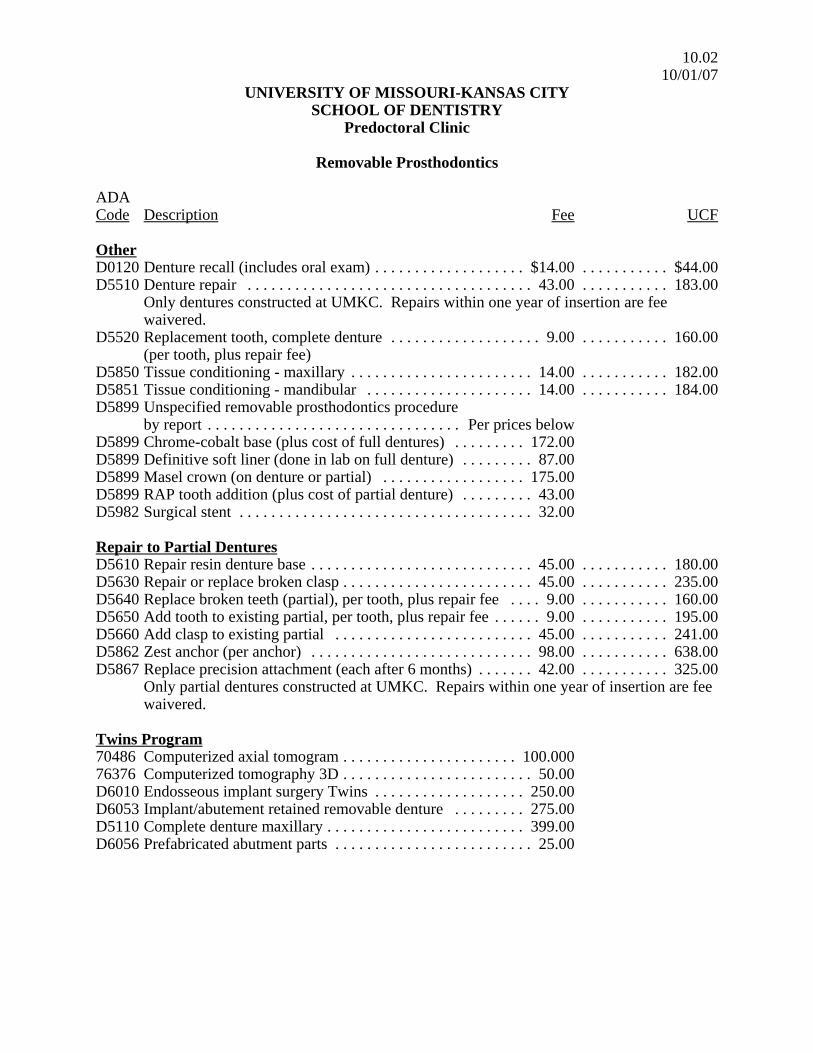
OtherD0120 Denture recall (includes oral exam) . . . . . . . . . . . . . . . . . . . $14.00 . . . . . . . . . . . $44.00D5510 Denture repair . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43.00 . . . . . . . . . . . 183.00
Only dentures constructed at UMKC. Repairs within one year of insertion are feewaivered.
D5520 Replacement tooth, complete denture . . . . . . . . . . . . . . . . . . . 9.00 . . . . . . . . . . . 160.00(per tooth, plus repair fee)
D5850 Tissue conditioning - maxillary . . . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . 182.00D5851 Tissue conditioning - mandibular . . . . . . . . . . . . . . . . . . . . . 14.00 . . . . . . . . . . . 184.00D5899 Unspecified removable prosthodontics procedure
by report . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Per prices belowD5899 Chrome-cobalt base (plus cost of full dentures) . . . . . . . . . 172.00D5899 Definitive soft liner (done in lab on full denture) . . . . . . . . . 87.00D5899 Masel crown (on denture or partial) . . . . . . . . . . . . . . . . . . 175.00D5899 RAP tooth addition (plus cost of partial denture) . . . . . . . . . 43.00D5982 Surgical stent . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 32.00
Repair to Partial DenturesD5610 Repair resin denture base . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 180.00D5630 Repair or replace broken clasp . . . . . . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 235.00D5640 Replace broken teeth (partial), per tooth, plus repair fee . . . . 9.00 . . . . . . . . . . . 160.00D5650 Add tooth to existing partial, per tooth, plus repair fee . . . . . . 9.00 . . . . . . . . . . . 195.00D5660 Add clasp to existing partial . . . . . . . . . . . . . . . . . . . . . . . . . 45.00 . . . . . . . . . . . 241.00D5862 Zest anchor (per anchor) . . . . . . . . . . . . . . . . . . . . . . . . . . . . 98.00 . . . . . . . . . . . 638.00D5867 Replace precision attachment (each after 6 months) . . . . . . . 42.00 . . . . . . . . . . . 325.00
Only partial dentures constructed at UMKC. Repairs within one year of insertion are feewaivered.
Twins Program70486 Computerized axial tomogram . . . . . . . . . . . . . . . . . . . . . . 100.00076376 Computerized tomography 3D . . . . . . . . . . . . . . . . . . . . . . . . 50.00D6010 Endosseous implant surgery Twins . . . . . . . . . . . . . . . . . . . 250.00D6053 Implant/abutement retained removable denture . . . . . . . . . 275.00D5110 Complete denture maxillary . . . . . . . . . . . . . . . . . . . . . . . . . 399.00D6056 Prefabricated abutment parts . . . . . . . . . . . . . . . . . . . . . . . . . 25.00

11.0110/01/07
UNIVERSITY OF MISSOURI-KANSAS CITYSCHOOL OF DENTISTRY
Predoctoral Clinic
Miscellaneous Charges
Duplication of X-ray FilmDuplicate full periapical survey . . . . . . . . . . . . . . . . . . . . . . $25.00Duplicate 5x12 panoramic . . . . . . . . . . . . . . . . . . . . . . . . . . . 17.00Duplicate occlusal film . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00Duplicate partial survey . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14.00Duplicate skull film . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17.00
Please note: The fees on this page are collected separately and are not included in the clinicmanagement software.





























