Embed Size (px)
Citation preview

U2
NBa
b
c
d
e
a
ARRAA
KACRPV
1
mdcovs
0d
Transactions of the Royal Society of Tropical Medicine and Hygiene 105 (2011) 628– 636
Contents lists available at ScienceDirect
Transactions of the Royal Society ofTropical Medicine and Hygiene
j our na l ho me p age: ht t p: / /www.e lsev ier .com/ locate / t rs tmh
nnecessary antibiotic use for mild acute respiratory infections during8-day follow-up of 823 children under five in rural Vietnam
guyen Quynh Hoaa,b,∗, Nguyen Thi Kim Chucc, Ho Dang Phucd, Mattias Larssona,o Erikssone, Cecilia Stålsby Lundborga
Division of Global Health (IHCAR), Department of Public Health Sciences, Karolinska Institutet, Nobel väg 9, SE 171 77 Stockholm, SwedenVietnam Cuba Friendship Hospital, 37 Hai Ba Trung Street, Hanoi, VietnamDepartment of Public Health, Hanoi Medical University, 1 Ton That Tung Street, Hanoi, VietnamDepartment of Probability and Statistics, Institute of Mathematics, 18 Hoang Quoc Viet Road, Hanoi, VietnamNordic School of Public Health, Box 12133 SE-402 42 Gothenburg, Sweden
r t i c l e i n f o
rticle history:eceived 12 October 2010eceived in revised form 25 July 2011ccepted 25 July 2011vailable online 29 September 2011
eywords:ntibiotic usehildren under fiveespiratory infectionrospective studyietnam
a b s t r a c t
Few prospective studies regarding antibiotic use for mild acute respiratory infections (ARI)have been conducted in community settings. This paper aimed to assess knowledge of chil-dren’s caregivers and actual antibiotic use for children under five and to identify factorsassociated with antibiotic treatment for mild ARIs. Caregivers in 828 households in Bavi,Vietnam, were interviewed using a structured questionnaire assessing both knowledgeand practice. Subsequently, 823 children were followed for 28 days to collect informationregarding symptoms and drug use. For management of ARIs, only 13% of caregivers demon-strated correct overall knowledge in accordance with standard guidelines. The symptomsof the most recent illness were consistent with mild ARI in 79% of cases, and antibiotics wereused in 71% of these. During the 28-day period, 62% of children had been given antibioticsand 63% of antibiotic courses were used for mild ARIs. One-half of the mild ARI episodesand 63% of the children with mild ARIs were treated with antibiotics. Most of the unnec-
essary antibiotic treatment was recommended by healthcare providers (82%). Most of thechildren had been administered antibiotics for common colds, although most caregiversbelieved that antibiotics were not required. Antibiotics were unnecessarily recommendedat health facilities in the area.© 2011 Royal Society of Tropical Medicine and Hygiene. Published by Elsevier Ltd.
. Introduction
Few prospective studies regarding antibiotic use forild acute respiratory infections (ARI) have been con-
ucted in community settings. Mild ARI (the commonold) is defined as an acute inflammation of the nasal
r pharyngeal mucosa and is normally a self-limitingiral illness.1,2 Most respiratory infections present withymptoms such as rhinitis and sore throat, with or without∗ Corresponding author. Tel.: +46 76 281 1589; fax: +46 8 31 15 90.E-mail address: [email protected] (N.Q. Hoa).
035-9203/$ – see front matter © 2011 Royal Society of Tropical Medicine and Hoi:10.1016/j.trstmh.2011.07.015
All rights reserved.
fever or cough.2,3 A child with any of these symptoms,but not having any pneumonia signs such as fast breath-ing, chest in-drawing or general danger signs such asconvulsions, unconsciousness or persistent vomiting, isclassified as having a common cold.3 In children underfive, ARI is a common reason for seeking healthcare.4,5
Household members, particularly mothers, play a crucialrole in managing childhood illness. At home, caregiversundertake the primary diagnosis, assess the severity, and
make the decisions to seek or not to seek healthcare andadminister drugs. Treatment-seeking behaviour for illnessin children has been explored, but few studies specificallyfocus on healthcare-seeking for childhood ARIs.ygiene. Published by Elsevier Ltd. All rights reserved.

of Tropical Medicine and Hygiene 105 (2011) 628– 636 629
Box 1. Main questions used in the paper to assess knowledge ofcaregivers about antibiotic use for acute respiratory infection (ARI)among children. The full questionnaire is available in Vietnameseand English from the first author
In case of having respiratory infectious symptoms, when doesthe child need antibiotics?
1. Cough, stuffy nose or runny nose without fever (Yes/No)
2. Cough, stuffy nose or runny nose with fever (Yes/No)
3. Including one of the following symptoms: fast breathing, chestin-drawing or stridor (Yes/No)
4. Other respiratory symptoms (Yes/No). Respondents asked to
N.Q. Hoa et al. / Transactions of the Royal Society
Recommendations for the treatment of ARIs in childrenincluding rational antibiotic use have been formulatedinternationally and in the adapted Vietnamese Ministryof Health guidelines.3,6 Both guidelines recommend thatantibiotics should not be used for cough without anysign of difficult breathing. The Integrated Management ofChildhood Illness (IMCI) implementation strategies guidemothers on how to care for sick children as well as howto give drugs at home.3,6 Children who are classified ashaving a common cold do not require antibiotic treat-ment and can be managed at home.1,3,6 However, in manyplaces, especially rural areas such as Bavi District, Vietnam,the IMCI was not implemented. Frequent antibiotic usefor the common cold has been reported in Vietnam andmany other countries,7–10 accelerating the emergence andspread of resistant bacteria.11–13
It is important to investigate the actual situation ofantibiotic use for common colds in order to develop suit-able and contextualised intervention strategies to improveantibiotic use, particularly because mild ARIs are so com-mon. A better understanding of the knowledge and practiceof community members as well as healthcare providers willnot only facilitate communication between clinicians andcaregivers but also provide important input into interven-tion development processes.
This study is part of a larger project conducted in thepopulation of a rural area in northern Vietnam. Stud-ies of the perceptions of children’s caregivers regardingantibiotic use,14 the knowledge and practice of healthcareproviders,9 and the prevalence of antibiotic resistance havebeen conducted.13
The aim of this paper was to add to the above studiesby assessing the knowledge and practice of children’s care-givers regarding antibiotic use for mild ARIs in children aswell as the association between, on the one hand, knowl-edge and practice, and on the other hand, demographic,social and economic characteristics of the caregiver, thechild and the household.
2. Materials and methods
2.1. Study area and subjects
The study setting was Bavi District, Hanoi, wherean epidemiological field laboratory (FilaBavi) has beenimplemented since 1998.15 The district covers an area of410 km2, divided into lowland, highland and mountainousareas according to geographical characteristics. The sam-ple of FilaBavi was selected as a stratified random clustersample. A cluster was defined as a village or part of a largevillage. The sample of 847 children aged 6–60 months wasobtained from 847 households in 13 clusters within theFilaBavi framework.
2.2. Knowledge, reported practice and antibioticutilisation survey
The main caregiver for the selected child in eachhousehold was identified and interviewed using a ques-tionnaire with questions about antibiotic knowledge andperceptions in case the child gets an ARI (Box 1) as well as
present detail.
reported practice of drug- and healthcare-seeking in thechild’s most recent illness.
The caregiver was also requested to prospectively fillin a form about self-reported illness and drug use for thechild each day during a 28-day period (from March to June2007). Each week, FilaBavi interviewers came to interviewthe caregivers using a structured questionnaire. The infor-mation collected every day for 28 days included symptoms,type of healthcare sought, name of drugs administered,and information about who suggested or recommendedthe particular drug. All the self-reported forms, prescrip-tions and medicine containers were used to facilitate datacollection.
Healthcare-seeking behaviour was classified as: (i)self-treatment if the child had no treatment or was treatedwithout professional consultation; (ii) drug store if thecaregiver received advice and drugs in a drug outlet,drug store or pharmacy without clinical examination orprescription; (iii) private clinic if the caregiver soughtcare at a private health facility and then received either aprescription or drugs; and (iv) public clinic if the caregiversought care at a health commune station, hospital orregional polyclinic and received a prescription.
2.3. Data management and statistical analysis
To assess the appropriateness of antibiotic use forchildren, recommendations from the WHO3 and Viet-namese guidelines6 were used. Overall knowledge wasconsidered as correct if caregivers provided correctanswers to knowledge questions in accordance with theguidelines for all of the three stated ARI symptoms, i.e. ‘No’to questions 1, 2 and 4 and ‘Yes’ to question 3 (Box 1).
The illness of the child was classified based on theself-reported symptoms following the IMCI guidelines as:(i) mild ARI if any of following symptoms were present:cough, stuffy nose, runny nose, sore throat, but no fastbreathing or chest in-drawing; (ii) severe ARI if at least oneof the pneumonia symptoms were present: fast breathing,chest in-drawing or stridor; and (iii) other, for any othersymptom, e.g. watery faeces, bloody stools, vomit, earache,
injury, abdominal pain, skin rash or toothache.In the 28-day follow-up period, an episode of illnesswas defined as a period of consecutive days with the samesymptoms. A course of antibiotics was defined as a period
6 of Trop
oa
wCau(
akrapvsgidie
pcaau
TBc
a
b
c
*
†
30 N.Q. Hoa et al. / Transactions of the Royal Society
f consecutive days with use of the same or differentntibiotics.
Drugs recommended for the participating childrenere classified according to the Anatomical Therapeutichemical (ATC) classification system.16 This study includesntibiotics that are classified as antibacterials for systemicse and aggregated at the level of the active ingredientlevel 5 of the ATC class J01).16
Estimated proportions of correct overall knowledgend antibiotic use with a 95% CI were used to describe thenowledge and practice of children’s caregivers. Multipleegression models were used to examine the statisticalssociations between overall knowledge and antibiotic useercentage, respectively, and the following independentariables: sex of child; age of child; household’s economictatus; geographical region; sex of main caregiver; care-iver’s education; and caregiver’s occupation. The wealthndex, describing the household’s economic status, wasefined as a combination of information on household
ncome, expenditure and assets. This information wasxtracted from FilaBavi’s re-census survey 2007.
In the regression models using knowledge or reportedractice as a dependent variable, the unit of analysis is the
aregiver. Models with antibiotic use in a 28-day period asdependent variable have the illness episode as the unit ofnalysis. Here, two-level logistic regression models weresed with episode as the first level and child as the second.
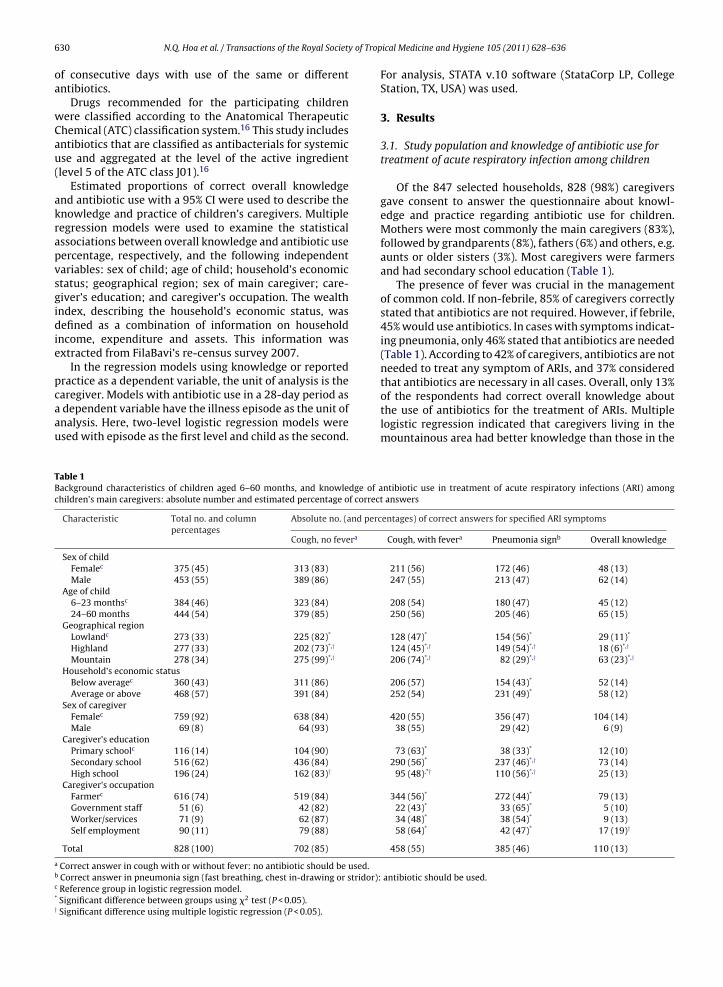
able 1ackground characteristics of children aged 6–60 months, and knowledge of ahildren’s main caregivers: absolute number and estimated percentage of correct
Characteristic Total no. and columnpercentages
Absolute no. (and perc
Cough, no fevera
Sex of childFemalec 375 (45) 313 (83)
Male 453 (55) 389 (86)
Age of child6–23 monthsc 384 (46) 323 (84)
24–60 months 444 (54) 379 (85)
Geographical regionLowlandc 273 (33) 225 (82)*
Highland 277 (33) 202 (73)*,†
Mountain 278 (34) 275 (99)*,†
Household’s economic statusBelow averagec 360 (43) 311 (86)
Average or above 468 (57) 391 (84)
Sex of caregiverFemalec 759 (92) 638 (84)
Male 69 (8) 64 (93)
Caregiver’s educationPrimary schoolc 116 (14) 104 (90)
Secondary school 516 (62) 436 (84)
High school 196 (24) 162 (83)†
Caregiver’s occupationFarmerc 616 (74) 519 (84)
Government staff 51 (6) 42 (82)
Worker/services 71 (9) 62 (87)
Self employment 90 (11) 79 (88)
Total 828 (100) 702 (85)
Correct answer in cough with or without fever: no antibiotic should be used.Correct answer in pneumonia sign (fast breathing, chest in-drawing or stridor):Reference group in logistic regression model.Significant difference between groups using �2 test (P < 0.05).Significant difference using multiple logistic regression (P < 0.05).
ical Medicine and Hygiene 105 (2011) 628– 636
For analysis, STATA v.10 software (StataCorp LP, CollegeStation, TX, USA) was used.
3. Results
3.1. Study population and knowledge of antibiotic use fortreatment of acute respiratory infection among children
Of the 847 selected households, 828 (98%) caregiversgave consent to answer the questionnaire about knowl-edge and practice regarding antibiotic use for children.Mothers were most commonly the main caregivers (83%),followed by grandparents (8%), fathers (6%) and others, e.g.aunts or older sisters (3%). Most caregivers were farmersand had secondary school education (Table 1).
The presence of fever was crucial in the managementof common cold. If non-febrile, 85% of caregivers correctlystated that antibiotics are not required. However, if febrile,45% would use antibiotics. In cases with symptoms indicat-ing pneumonia, only 46% stated that antibiotics are needed(Table 1). According to 42% of caregivers, antibiotics are notneeded to treat any symptom of ARIs, and 37% consideredthat antibiotics are necessary in all cases. Overall, only 13%
of the respondents had correct overall knowledge aboutthe use of antibiotics for the treatment of ARIs. Multiplelogistic regression indicated that caregivers living in themountainous area had better knowledge than those in thentibiotic use in treatment of acute respiratory infections (ARI) among answers
entages) of correct answers for specified ARI symptoms
Cough, with fevera Pneumonia signb Overall knowledge
211 (56) 172 (46) 48 (13)247 (55) 213 (47) 62 (14)
208 (54) 180 (47) 45 (12)250 (56) 205 (46) 65 (15)
128 (47)* 154 (56)* 29 (11)*
124 (45)*,† 149 (54)*,† 18 (6)*,†
206 (74)*,† 82 (29)*,† 63 (23)*,†
206 (57) 154 (43)* 52 (14)252 (54) 231 (49)* 58 (12)
420 (55) 356 (47) 104 (14)38 (55) 29 (42) 6 (9)
73 (63)* 38 (33)* 12 (10)290 (56)* 237 (46)*,† 73 (14)
95 (48),*† 110 (56)*,† 25 (13)
344 (56)* 272 (44)* 79 (13)22 (43)* 33 (65)* 5 (10)34 (48)* 38 (54)* 9 (13)58 (64)* 42 (47)* 17 (19)†
458 (55) 385 (46) 110 (13)
antibiotic should be used.
of Trop
N.Q. Hoa et al. / Transactions of the Royal Societyhighlands or lowlands. The highest proportion of correctoverall knowledge was obtained from a cluster in themountainous area (32%) and the lowest from a cluster inthe highland area (4%). There was some homogeneity inantibiotic knowledge among caregivers within clusters[intracluster correlation (ICC) = 0.16]. High-school-educated caregivers had better knowledge regardingantibiotic use in the case of pneumonia, but they hadpoorer knowledge in the case of cough with fever comparedwith primary- and secondary-school-educated caregivers(Table 1).
3.2. Antibiotic use and health-seeking behaviour forchildren during their most recent illness
Of the 828 respondents, 99% (821/828) providedinformation about their child’s most recent illness. Thereported symptoms were consistent with mild ARI (79%),severe ARI (11%) or other illness (9%). Antibiotics wereused in 69% of all cases. The percentage antibiotic usefor treatment of mild ARIs, severe ARIs and other ill-ness were 71% (464/654), 86% (79/92) and 33% (25/75),respectively.
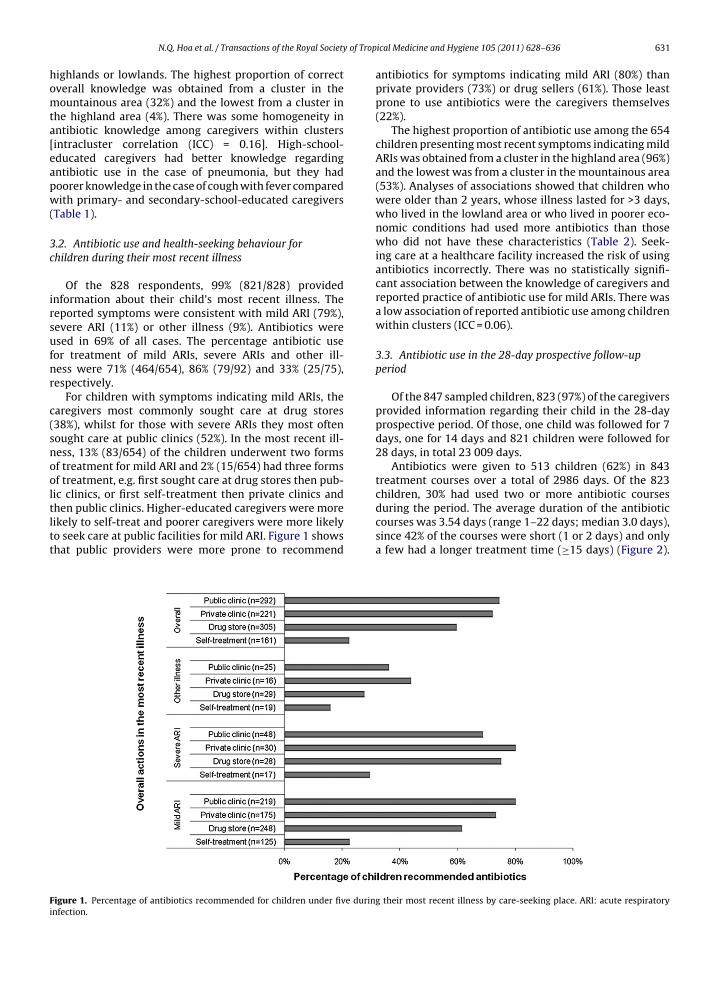
For children with symptoms indicating mild ARIs, thecaregivers most commonly sought care at drug stores(38%), whilst for those with severe ARIs they most oftensought care at public clinics (52%). In the most recent ill-ness, 13% (83/654) of the children underwent two formsof treatment for mild ARI and 2% (15/654) had three formsof treatment, e.g. first sought care at drug stores then pub-lic clinics, or first self-treatment then private clinics and
then public clinics. Higher-educated caregivers were morelikely to self-treat and poorer caregivers were more likelyto seek care at public facilities for mild ARI. Figure 1 showsthat public providers were more prone to recommendFigure 1. Percentage of antibiotics recommended for children under five durininfection.
ical Medicine and Hygiene 105 (2011) 628– 636 631
antibiotics for symptoms indicating mild ARI (80%) thanprivate providers (73%) or drug sellers (61%). Those leastprone to use antibiotics were the caregivers themselves(22%).
The highest proportion of antibiotic use among the 654children presenting most recent symptoms indicating mildARIs was obtained from a cluster in the highland area (96%)and the lowest was from a cluster in the mountainous area(53%). Analyses of associations showed that children whowere older than 2 years, whose illness lasted for >3 days,who lived in the lowland area or who lived in poorer eco-nomic conditions had used more antibiotics than thosewho did not have these characteristics (Table 2). Seek-ing care at a healthcare facility increased the risk of usingantibiotics incorrectly. There was no statistically signifi-cant association between the knowledge of caregivers andreported practice of antibiotic use for mild ARIs. There wasa low association of reported antibiotic use among childrenwithin clusters (ICC = 0.06).
3.3. Antibiotic use in the 28-day prospective follow-upperiod
Of the 847 sampled children, 823 (97%) of the caregiversprovided information regarding their child in the 28-dayprospective period. Of those, one child was followed for 7days, one for 14 days and 821 children were followed for28 days, in total 23 009 days.
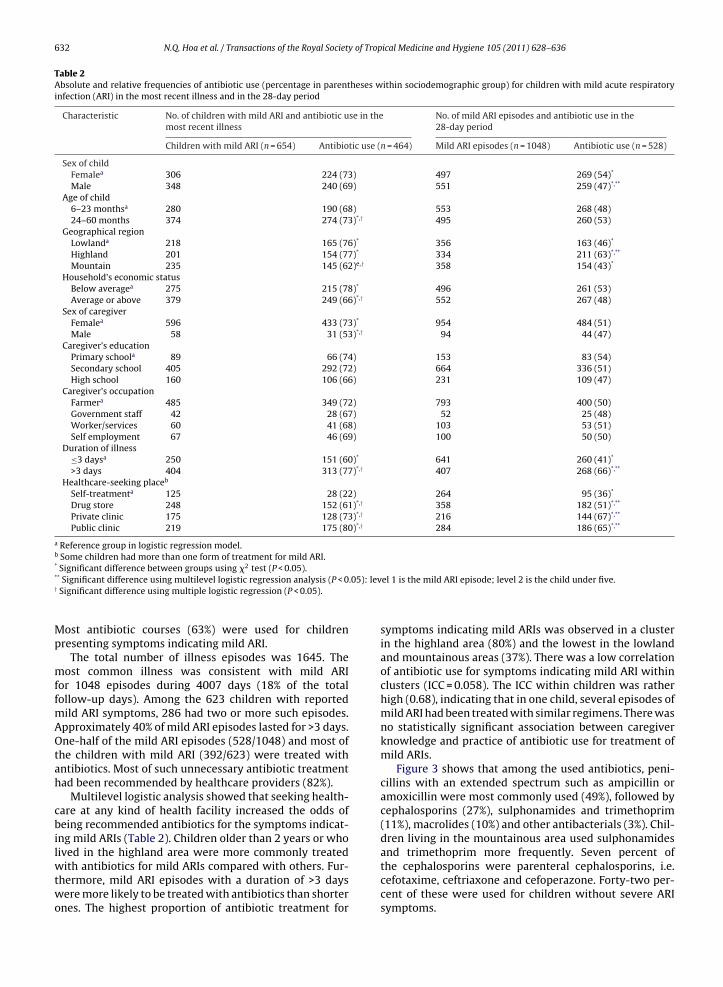
Antibiotics were given to 513 children (62%) in 843treatment courses over a total of 2986 days. Of the 823children, 30% had used two or more antibiotic courses
during the period. The average duration of the antibioticcourses was 3.54 days (range 1–22 days; median 3.0 days),since 42% of the courses were short (1 or 2 days) and onlya few had a longer treatment time (≥15 days) (Figure 2).g their most recent illness by care-seeking place. ARI: acute respiratory
632 N.Q. Hoa et al. / Transactions of the Royal Society of Tropical Medicine and Hygiene 105 (2011) 628– 636
Table 2Absolute and relative frequencies of antibiotic use (percentage in parentheses within sociodemographic group) for children with mild acute respiratoryinfection (ARI) in the most recent illness and in the 28-day period
Characteristic No. of children with mild ARI and antibiotic use in themost recent illness
No. of mild ARI episodes and antibiotic use in the28-day period
Children with mild ARI (n = 654) Antibiotic use (n = 464) Mild ARI episodes (n = 1048) Antibiotic use (n = 528)
Sex of childFemalea 306 224 (73) 497 269 (54)*
Male 348 240 (69) 551 259 (47)*,**
Age of child6–23 monthsa 280 190 (68) 553 268 (48)24–60 months 374 274 (73)*,† 495 260 (53)
Geographical regionLowlanda 218 165 (76)* 356 163 (46)*
Highland 201 154 (77)* 334 211 (63)*,**
Mountain 235 145 (62)e,† 358 154 (43)*
Household’s economic statusBelow averagea 275 215 (78)* 496 261 (53)Average or above 379 249 (66)*,† 552 267 (48)
Sex of caregiverFemalea 596 433 (73)* 954 484 (51)Male 58 31 (53)*,† 94 44 (47)
Caregiver’s educationPrimary schoola 89 66 (74) 153 83 (54)Secondary school 405 292 (72) 664 336 (51)High school 160 106 (66) 231 109 (47)
Caregiver’s occupationFarmera 485 349 (72) 793 400 (50)Government staff 42 28 (67) 52 25 (48)Worker/services 60 41 (68) 103 53 (51)Self employment 67 46 (69) 100 50 (50)
Duration of illness≤3 daysa 250 151 (60)* 641 260 (41)*
>3 days 404 313 (77)*,† 407 268 (66)*,**
Healthcare-seeking placeb
Self-treatmenta 125 28 (22) 264 95 (36)*
Drug store 248 152 (61)*,† 358 182 (51)*,**
Private clinic 175 128 (73)*,† 216 144 (67)*,**
Public clinic 219 175 (80)*,† 284 186 (65)*,**
a Reference group in logistic regression model.b Some children had more than one form of treatment for mild ARI.* Significant difference between groups using �2 test (P < 0.05).* .05): lev†
Mp
mffmAOtah
cbilwtwo
* Significant difference using multilevel logistic regression analysis (P < 0Significant difference using multiple logistic regression (P < 0.05).
ost antibiotic courses (63%) were used for childrenresenting symptoms indicating mild ARI.
The total number of illness episodes was 1645. Theost common illness was consistent with mild ARI
or 1048 episodes during 4007 days (18% of the totalollow-up days). Among the 623 children with reported
ild ARI symptoms, 286 had two or more such episodes.pproximately 40% of mild ARI episodes lasted for >3 days.ne-half of the mild ARI episodes (528/1048) and most of
he children with mild ARI (392/623) were treated withntibiotics. Most of such unnecessary antibiotic treatmentad been recommended by healthcare providers (82%).
Multilevel logistic analysis showed that seeking health-are at any kind of health facility increased the odds ofeing recommended antibiotics for the symptoms indicat-
ng mild ARIs (Table 2). Children older than 2 years or whoived in the highland area were more commonly treated
ith antibiotics for mild ARIs compared with others. Fur-hermore, mild ARI episodes with a duration of >3 daysere more likely to be treated with antibiotics than shorter
nes. The highest proportion of antibiotic treatment for
el 1 is the mild ARI episode; level 2 is the child under five.
symptoms indicating mild ARIs was observed in a clusterin the highland area (80%) and the lowest in the lowlandand mountainous areas (37%). There was a low correlationof antibiotic use for symptoms indicating mild ARI withinclusters (ICC = 0.058). The ICC within children was ratherhigh (0.68), indicating that in one child, several episodes ofmild ARI had been treated with similar regimens. There wasno statistically significant association between caregiverknowledge and practice of antibiotic use for treatment ofmild ARIs.
Figure 3 shows that among the used antibiotics, peni-cillins with an extended spectrum such as ampicillin oramoxicillin were most commonly used (49%), followed bycephalosporins (27%), sulphonamides and trimethoprim(11%), macrolides (10%) and other antibacterials (3%). Chil-dren living in the mountainous area used sulphonamidesand trimethoprim more frequently. Seven percent of
the cephalosporins were parenteral cephalosporins, i.e.cefotaxime, ceftriaxone and cefoperazone. Forty-two per-cent of these were used for children without severe ARIsymptoms.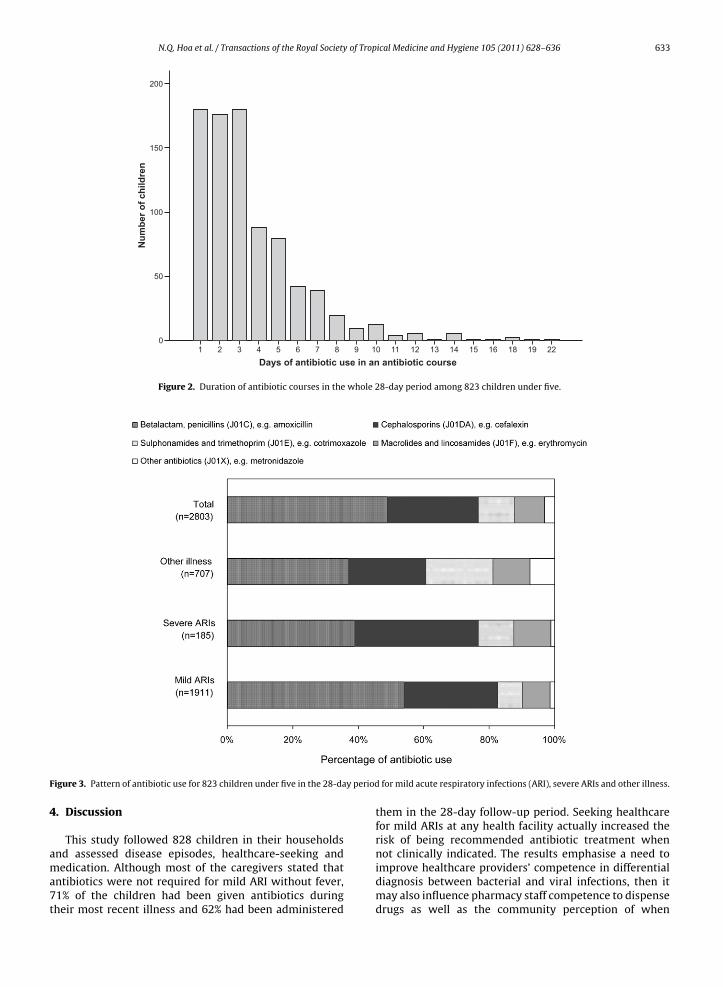
N.Q. Hoa et al. / Transactions of the Royal Society of Tropical Medicine and Hygiene 105 (2011) 628– 636 633
Days of antibiotic use in an antibiotic course22191816151413121110987654321
Num
ber o
f chi
ldre
n
200
150
100
50
0
Figure 2. Duration of antibiotic courses in the whole 28-day period among 823 children under five.
y period
Figure 3. Pattern of antibiotic use for 823 children under five in the 28-da4. Discussion
This study followed 828 children in their householdsand assessed disease episodes, healthcare-seeking and
medication. Although most of the caregivers stated thatantibiotics were not required for mild ARI without fever,71% of the children had been given antibiotics duringtheir most recent illness and 62% had been administeredfor mild acute respiratory infections (ARI), severe ARIs and other illness.
them in the 28-day follow-up period. Seeking healthcarefor mild ARIs at any health facility actually increased therisk of being recommended antibiotic treatment whennot clinically indicated. The results emphasise a need to
improve healthcare providers’ competence in differentialdiagnosis between bacterial and viral infections, then itmay also influence pharmacy staff competence to dispensedrugs as well as the community perception of when
6 of Trop
ad
wlriiabsbupottiariacpiukdib
uaiiThftfpsaOoavctsephoaeitp
e
34 N.Q. Hoa et al. / Transactions of the Royal Society
ntibiotics are needed and hence the expectations andemand from patients.
Most antibiotics were used for children presentingith symptoms indicating mild ARIs. Similarly high
evels of antibiotic use have been reported from someetrospective studies in Vietnam.7,17 The current find-ngs show more common irrational antibiotic use thans reported from other countries, which found 44–60%ntibiotic use for common cold.8,10 No evidence of theenefit of antibiotic treatment for ARIs without dangerigns such as rapid breathing and chest in-drawings haseen reported.18 As most children in the communitysed antibiotics incorrectly, there is a constant selectiveressure toward microbial resistance through eliminationf susceptible bacterial populations.19 In such a situation,he resistant bacteria adapt, replicate and spread ratherhan being killed, thus increasing the antibiotic resistancen the community.13 Previously, an association betweenntibiotic use, population density and increased antibioticesistance has been documented.20,21 The intense andndiscriminate use of the parenteral cephalosporins, whichre still effective to treat community-acquired pneumo-occal pneumonia and meningitis, might lead to resistanceroblems to these antibiotics in the near future. An effective
ntervention programme to reduce unnecessary antibioticse is urgently required. By focusing to improve caregivers’nowledge about the causes of colds and the normalevelopment of diseases as well as appropriate antibiotic
ndications, caregivers’ expectations on antibiotics mighte reduced.22
This study explored the association between antibioticse in the households and healthcare-seeking behaviourt healthcare facilities. Seeking healthcare at any facilityncluding drug stores, private clinics or public clinicsncreased the odds for antibiotic use to treat mild ARIs.his confirms the results of previous studies reporting thatealthcare providers often prescribe or dispense antibiotics
or common colds.9 Although the IMCI strategy with practi-ioner training has been implemented since 1999, it has soar only been fully implemented in one-third of Vietnam’srovinces. In addition, IMCI has not included providersuch as drug sellers or private practitioners although theyre of major importance for improving antibiotic use.ther explanations for unnecessary antibiotic prescribingr dispensing may be patients’ expectations, having doubtbout the effect of the oral antibiotics and a presumed pre-ention of serious secondary illness.23,24 The fear of seriousomplications might be due to the reported viral and bac-erial co-infectious pneumonia, especially in low-incomeettings.25 However, there is no evidence of the protectiveffect of antibiotics in such cases.26 Other factors thatossibly relate to inappropriate prescribing are physiciansaving inadequate time to explain to parents why antibi-tics are not necessary, lack of access to laboratory testing,nd misdiagnosis of viral infections. Studies reported thatven when physicians know that the use of antibioticss unnecessary, they are still used to maintain good rela-
ionships with patients.23 Other influence may be fromharmaceutical promotion, which is very difficult to assess.This study raises considerable concern about unnec-ssary health service utilisation for common colds. The
ical Medicine and Hygiene 105 (2011) 628– 636
Vietnamese policy of free treatment for children undersix is probably increasing health service utilisation forchildren. Evidence suggested that if fewer patients con-sulted doctors for mild infections, unnecessary antibioticprescribing would be reduced.27 Adopting more patient-centre consulting skills might be a tool to rationaliseprescribing of antibiotics. The implications for practice arethat antibiotics should not be given in the first instance, asthey would not decrease the symptoms of mild ARIs. Suchtraining should be offered to all community members aswell as to healthcare providers.
A positive correlation was found between high antibi-otic use and older age, lower economic status and longerduration of illness. Reported expenditure to diagnoseand treat communicable illness in poor households haspreviously been reported to be relatively higher comparedwith more affluent households.28 A worry among parentsof having to take several days off to take care for andspending more money to treat a severely sick child mightreinforce expectations of the antibiotics’ positive effect.14
The finding that children older than 2 years were morelikely to use antibiotics might reflect that parents protecttheir small children from adverse effects of antibiotics.14
The association with duration of illness might be due tothe perception that illness with fever and longer durationis more severe and requires antibiotics. As we separatedthe recommendation of drug sellers from those of care-givers themselves, the proportion of self-medication withantibiotics was lower in this study compared with resultspreviously reported in Vietnam,17 however it was morefrequent than reported in European countries.29
Higher-educated caregivers expressed poorer knowl-edge about antibiotic use and were more prone toself-medicate for mild ARI, which corresponds to previousstudies.29 We did not find a statistical association betweenpractice and caregiver’s knowledge regarding antibioticuse; the explanation might be that most caregivers justfollowed healthcare providers’ recommendations. It isimportant that parents recognise and seek care whenchildren have danger signs.3,6 Enhancing caregivers’ skillsto self-manage mild illness and to recognise danger signsmight decrease consultation rates for common colds in thelonger term.6
Generalisation of the results from this study outside thestudied clusters must be theoretical, that is based on thetheoretical propositions stating that important contextualfactors related to the risk of antibiotic use among children,e.g. with mild ARI, are not very different in the areas towhich generalisation is intended. The results can then bethe basis for theory-based judgements about the situationin other similar contexts.30
The strength of this community study is that it was aprospective study with a large sample size and collecteddetailed information on symptoms and drugs used eachday over 28 days. There was good co-operation withhouseholds regarding filling in the form about symptomsand drugs on a daily basis and answering the weekly
questionnaires. Data were collected by trained and expe-rienced interviewers who are familiar with the area. Wecarefully piloted and supervised work both in the fieldand regarding data entry in order to control the quality of
of Trop
N.Q. Hoa et al. / Transactions of the Royal Societythe data. There was a high response rate throughout thewhole study period.
The study has some limitations. Data based on struc-tured interviews with children’s caregivers were collectedwithout clinical examination. Also, information aboutthe expectations of the parents on receiving antibioticswhen seeking care was not collected, although this mightinfluence the prescribing pattern of health providers.
5. Conclusion
Most of the children had been given antibiotics forcommon colds despite most of the caregivers believingthat antibiotics were not required, pointing to a conflictbetween knowledge and practice. Seeking care at healthfacilities, public as well as private, increased unnecessaryuse of antibiotics for mild ARIs. The problem of inappropri-ate antibiotic use must be minimised by influencing bothpeoples’ health-seeking behaviour and health providers’prescribing and dispensing behaviour. Educational inter-ventions in the community about the causes of colds, theirnatural progress and appropriate antibiotic indicationscould help to improve antibiotic use in the community.
Authors’ contributions: All of the authors participatedin the conception and design of the study and revised thepaper critically for substantial intellectual content; NQHsupervised the data collection, performed data analysisand drafted the manuscript; NTKC and CSL supportedthe data collection and helped draft the manuscript; BEand HDP contributed to statistical analysis. All authorsread and approved the final manuscript. NQH and CSL areguarantors of the paper.
Acknowledgements: The authors would like to thank thehouseholds from the Bavi District who gave their time toreport drug use information and answer questions as wellas share their experiences. They gratefully acknowledgethe field staff, supervisors and officials of FilaBavi for theirskill in collecting and inputting data.
Funding: This study was supported by the Health SystemsResearch Project in Vietnam, funded by the Swedish Inter-national Development Cooperation Agency (SIDA)—SAREC(Sweden) and the Ministry of Science and Technology(Vietnam).
Conflicts of interest: None declared.
Ethical approval: The Ethical Review Board of HanoiMedical University (Hanoi, Vietnam) approved this study(No. 28/HMURB, 2006). Interviewers obtained verbalconsent from all caregivers before administering the ques-tionnaire. Confidentiality was assured and the participantswere informed that they had the right to withdraw fromthe study at any time without explanation.
References
1. Rosenstein N, Phillips WR, Gerber MA, Marcy SM, SchwartzB, Dowell SF. The common cold—principles of judicious use ofantimicrobial agents. Pediatrics 1998;101:181–4.
ical Medicine and Hygiene 105 (2011) 628– 636 635
2. Regamey N, Kaiser L, Roiha HL, Deffernez C, Kuehni CE, Latzin P,et al. Viral etiology of acute respiratory infections with cough ininfancy: a community-based birth cohort study. Pediatr Infect Dis J2008;27:100–5.
3. Gove S. Integrated management of childhood illness by outpatienthealth workers: technical basis and overview. The WHO WorkingGroup on Guidelines for Integrated Management of the Sick Child.Bull World Health Organ 1997;75(Suppl 1):7–24.
4. UNICEF. The state of the world’s children 2005: childhood underthreat. New York, NY: UNICEF; 2004. http://www.childinfo.org/publications smsbytheme.html [accessed 3 November 2009].
5. Ministry of Health. Vietnam national health survey 2001–2002. Hanoi,Vietnam: Ministry of Health, Vietnam; 2003.
6. Ministry of Health. Handbook of integrated management for commonchildhood illness. Hanoi, Vietnam: Ministry of Health, Vietnam; 2006.
7. Chuc NT, Larsson M, Falkenberg T, Do NT, Binh NT, Tom-son GB. Management of childhood acute respiratory infectionsat private pharmacies in Vietnam. Ann Pharmacother 2001;35:1283–8.
8. Zuckerman IH, Perencevich EN, Harris AD. Concurrent acute illnessand comorbid conditions poorly predict antibiotic use in upper res-piratory tract infections: a cross-sectional analysis. BMC Infect Dis2007;7:47.
9. Hoa NQ, Larson M, Kim Chuc NT, Eriksson B, Trung NV, Stalsby CL.Antibiotics and paediatric acute respiratory infections in rural Viet-nam: health-care providers’ knowledge, practical competence andreported practice. Trop Med Int Health 2009;14:546–55.
10. Butler CC, Hood K, Verheij T, Little P, Melbye H, Nuttall J, et al. Vari-ation in antibiotic prescribing and its impact on recovery in patientswith acute cough in primary care: prospective study in 13 countries.BMJ 2009;338:b2242.
11. van de Sande-Bruinsma N, Grundmann H, Verloo D, Tiemersma E,Monen J, Goossens H, et al. Antimicrobial drug use and resistance inEurope. Emerg Infect Dis 2008;14:1722–30.
12. Song JH, Jung SI, Ko KS, Kim NY, Son JS, Chang HH, et al. Highprevalence of antimicrobial resistance among clinical Streptococcuspneumoniae isolates in Asia (an ANSORP study). Antimicrob AgentsChemother 2004;48:2101–7.
13. Hoa NQ, Trung NV, Larsson M, Eriksson B, Phuc HD, Chuc NT, et al.Decreased Streptococcus pneumoniae susceptibility to oral antibioticsamong children in rural Vietnam: a community study. BMC Infect Dis2010;10:85.
14. Hoa NQ, Ohman A, Lundborg CS, Chuc NT. Drug use and health-seeking behavior for childhood illness in Vietnam—a qualitativestudy. Health Policy 2007;82:320–9.
15. Chuc NT, Diwan V. FilaBavi, a demographic surveillance site, an epi-demiological field laboratory in Vietnam. Scand J Public Health Suppl2003;62:3–7.
16. WHO Collaborating Centre for Drug Statistics Methodology. Anatom-ical Therapeutic Chemical (ATC) classification index with defined dailydoses (DDDs) 2009. Oslo, Norway: WHO Collaborating Centre for DrugStatistics Methodology; 2008.
17. Larsson M, Kronvall G, Chuc NT, Karlsson I, Lager F, Hanh HD, et al.Antibiotic medication and bacterial resistance to antibiotics: a sur-vey of children in a Vietnamese community. Trop Med Int Health2000;5:711–21.
18. Arroll B, Kenealy T. Antibiotics for the common cold and acute puru-lent rhinitis. Cochrane Database Syst Rev 2005;(3):CD000247.
19. Tenover FC. Mechanisms of antimicrobial resistance in bacteria. AmJ Med 2006;119(6 Suppl 1):S3–10, discussion S62–70.
20. Arason VA, Sigurdsson JA, Erlendsdottir H, Gudmundsson S,Kristinsson KG. The role of antimicrobial use in the epidemi-ology of resistant pneumococci: a 10-year follow up. MicrobDrug Resist 2006;12:169–76. Erratum in: Microb Drug Resist2006;12:289.
21. Bruinsma N, Hutchinson JM, van den Bogaard AE, Giamarellou H,Degener J, Stobberingh EE. Influence of population density on antibi-otic resistance. J Antimicrob Chemother 2003;51:385–90.
22. Holloway KA, Karkee SB, Tamang A, Gurung YB, Kafle KK, Pradhan R,et al. Community intervention to promote rational treatment ofacute respiratory infection in rural Nepal. Trop Med Int Health2009;14:101–10.
23. Butler CC, Rollnick S, Pill R, Maggs-Rapport F, Stott N. Understandingthe culture of prescribing: qualitative study of general practition-ers’ and patients’ perceptions of antibiotics for sore throats. BMJ1998;317:637–42.
24. Hazir T, Nisar YB, Abbasi S, Ashraf YP, Khurshid J, Tariq P, et al.Comparison of oral amoxicillin with placebo for the treatment ofWorld Health Organization-defined nonsevere pneumonia in chil-dren aged 2-59 months: a multicenter, double-blind, randomized,

6 of Trop
36 N.Q. Hoa et al. / Transactions of the Royal Societyplacebo-controlled trial in Pakistan. Clin Infect Dis 2011;52:293–300.
25. Bulla A, Hitze KL. Acute respiratory infections: a review. Bull WorldHealth Organ 1978;56:481–98.
26. Petersen I, Johnson AM, Islam A, Duckworth G, Livermore DM,Hayward AC. Protective effect of antibiotics against serious com-
plications of common respiratory tract infections: retrospectivecohort study with the UK General Practice Research Database. BMJ2007;335:982.27. Ashworth M, Charlton J, Latinovic R, Gulliford M. Age-related changesin consultations and antibiotic prescribing for acute respiratory
ical Medicine and Hygiene 105 (2011) 628– 636
infections, 1995–2000. Data from the UK General Practice ResearchDatabase. J Clin Pharm Ther 2006;31:461–7.
28. Thuan NT, Lofgren C, Chuc NT, Janlert U, Lindholm L. Household out-of-pocket payments for illness: evidence from Vietnam. BMC PublicHealth 2006;6:283.
29. Grigoryan L, Haaijer-Rysjamp FM, Burgerhof JG, Mechtler R,
Deschepper R, Tambic-Andrasevic A, et al. Self-medication withantimicrobial drugs in Europe. Emerg Infect Dis 2006;12:452–9.30. Yin RK. Case study research: design and methods. Applied SocialResearch Methods Series, Vol. 5. Thousand Oaks, CA: SagePublications; 2003.