Embed Size (px)
Citation preview
UO Epatologia
“Centro di Riferimento Regionale per “la Diagnosi e il Trattamento delleEpatopatie Croniche e del Tumore di Fegato”
Azienda Ospedaliero UniversitariaPisana
Pisa, 16-11-2015
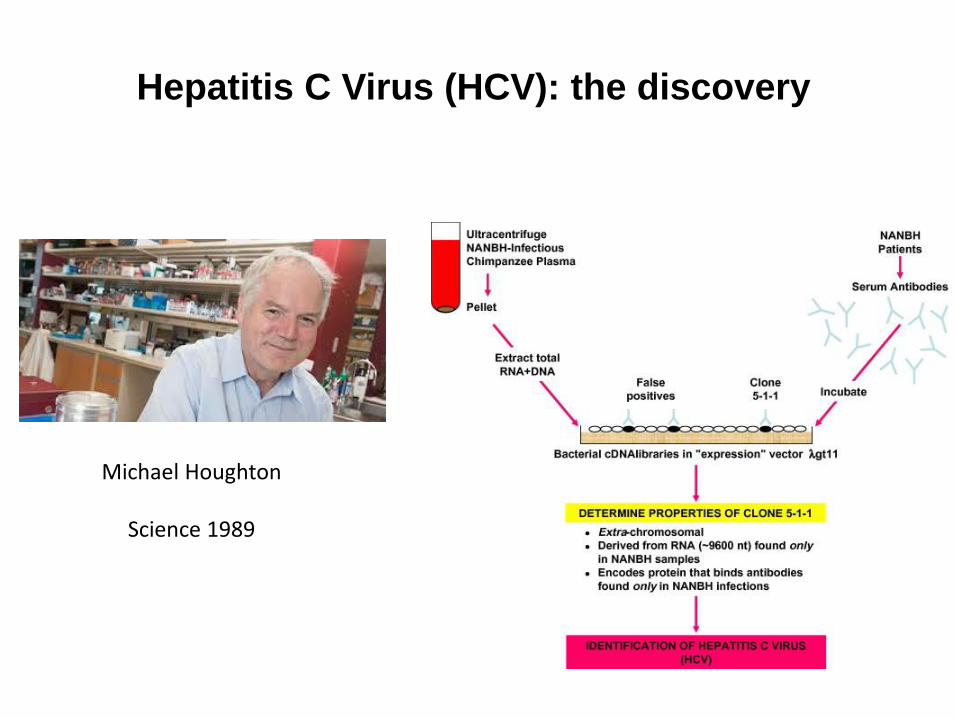
Hepatitis C Virus (HCV): the discovery
Michael Houghton
Science 1989
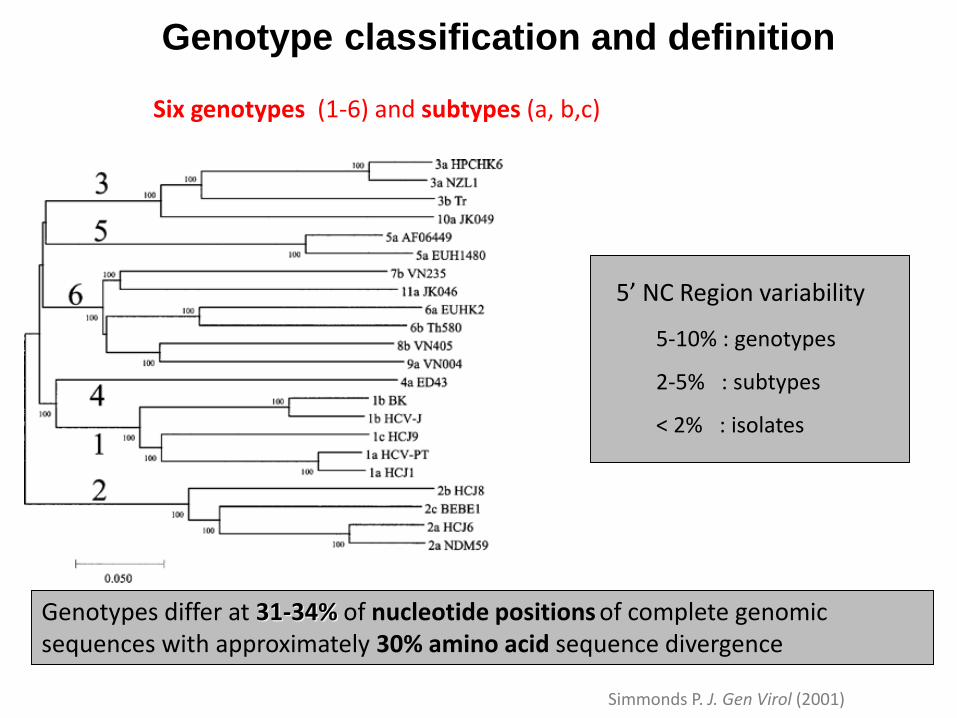
Genotype classification and definition
Six genotypes (1-6) and subtypes (a, b,c)
Genotypes differ at 31-34% of nucleotide positions of complete genomic sequences with approximately 30% amino acid sequence divergence
Simmonds P. J. Gen Virol (2001)
5’ NC Region variability
5-10% : genotypes
2-5% : subtypes
< 2% : isolates
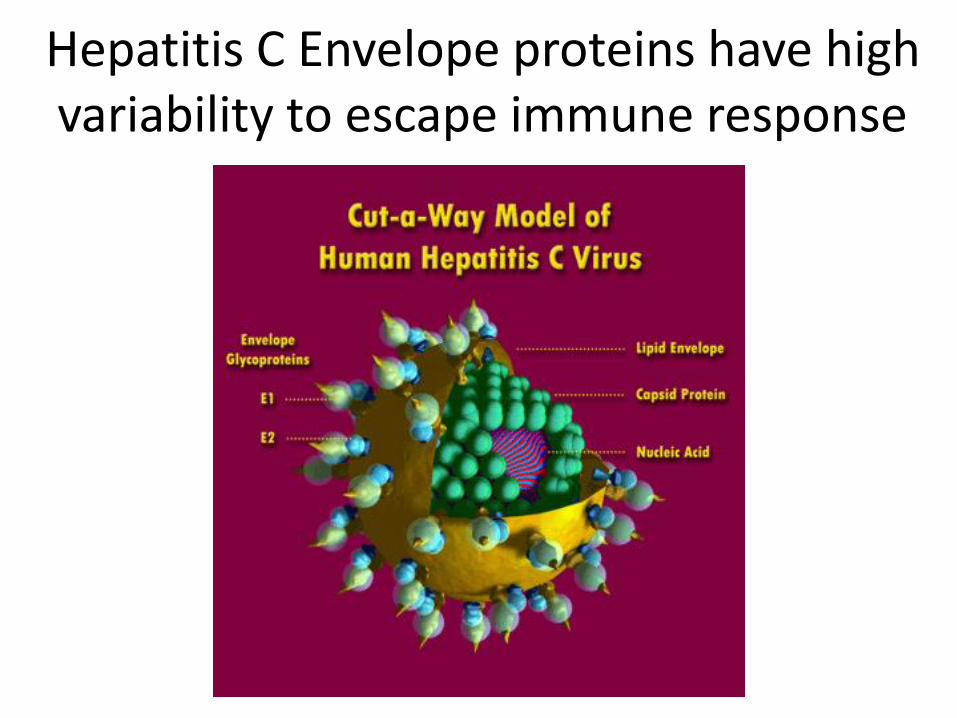
Hepatitis C Envelope proteins have high variability to escape immune response
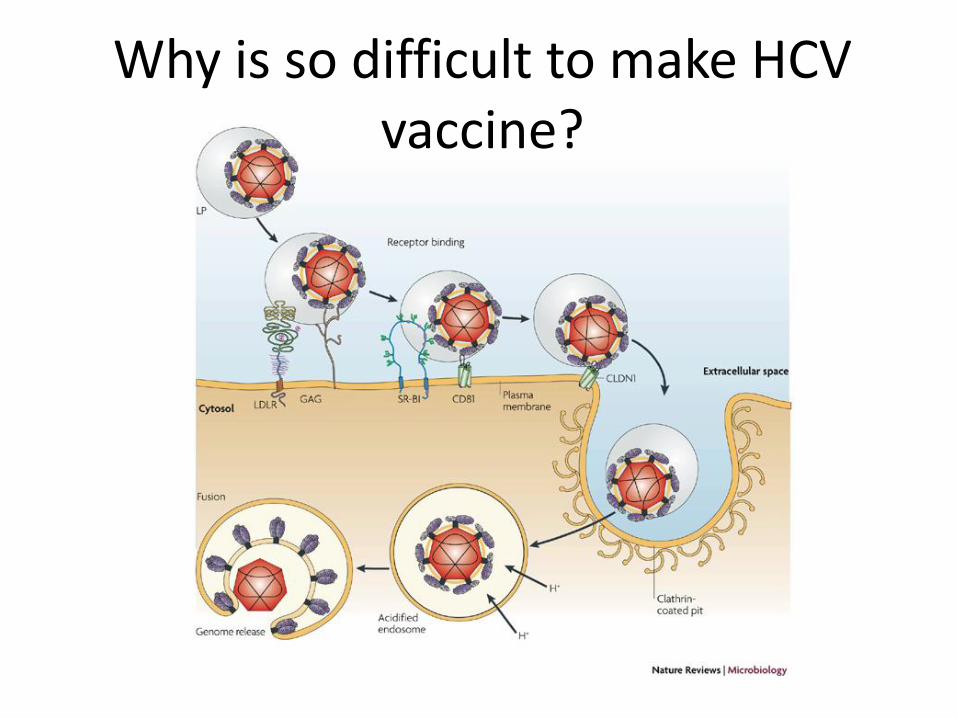
Why is so difficult to make HCV vaccine?
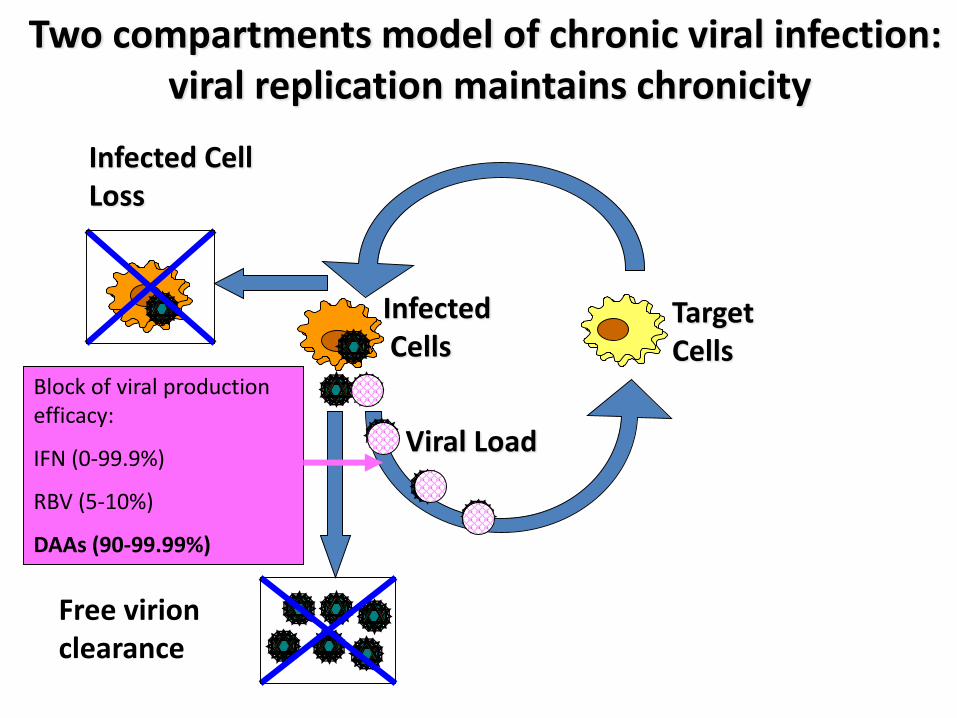
Viral Load
Target Cells
InfectedCells
Infected CellLoss
Free virion clearance
Two compartments model of chronic viral infection: viral replication maintains chronicity
Block of viral production efficacy:
IFN (0-99.9%)
RBV (5-10%)
DAAs (90-99.99%)
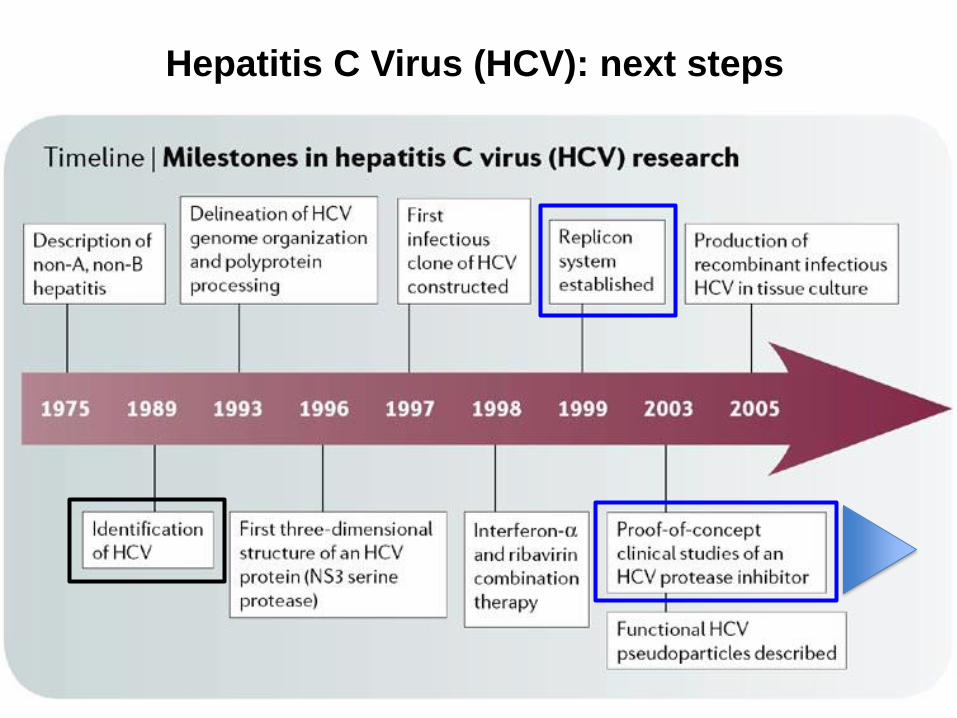
Hepatitis C Virus (HCV): next steps
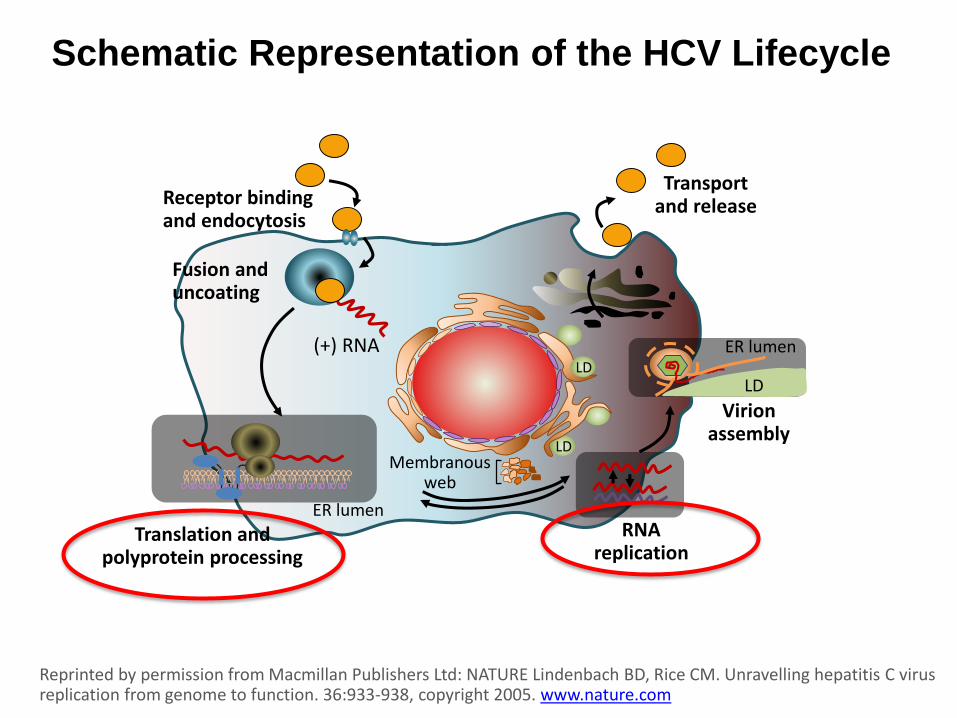
Schematic Representation of the HCV Lifecycle
Reprinted by permission from Macmillan Publishers Ltd: NATURE Lindenbach BD, Rice CM. Unravelling hepatitis C virus replication from genome to function. 36:933-938, copyright 2005. www.nature.com
Receptor bindingand endocytosis
Fusion and uncoating
Transportand release
(+) RNA
Translation andpolyprotein processing
RNAreplication
Virionassembly
Membranousweb
ER lumen
LD
LD
ER lumen
LD
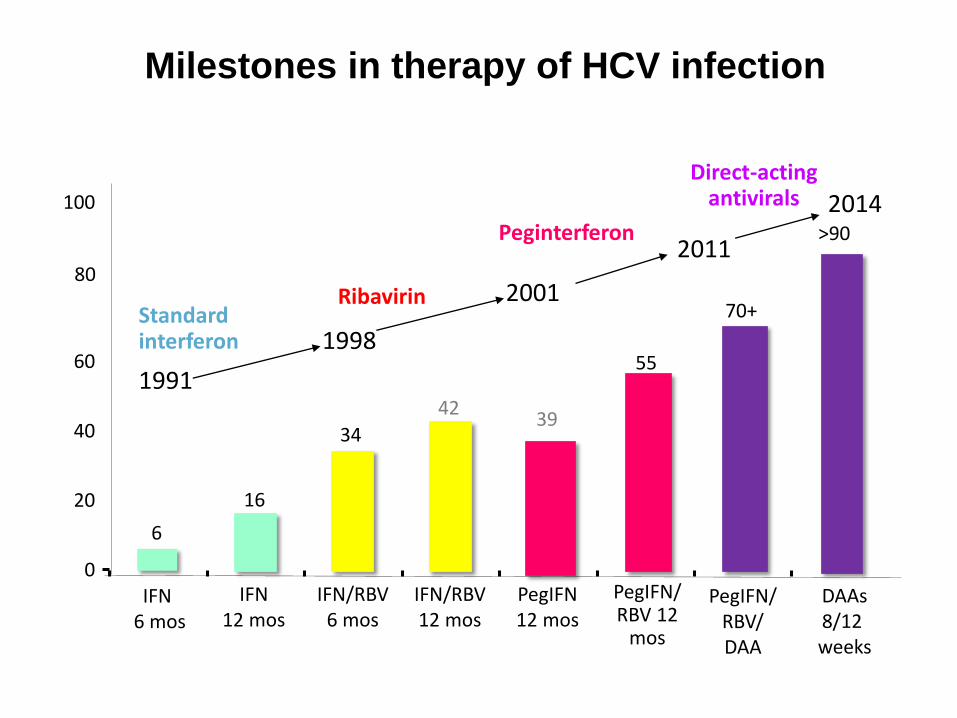
Milestones in therapy of HCV infection
IFN6 mos
PegIFN/ RBV 12
mos
IFN12 mos
IFN/RBV12 mos
PegIFN12 mos
2001
1998
2011
Standardinterferon
Ribavirin
Peginterferon
1991
Direct-actingantivirals
PegIFN/RBV/DAA
IFN/RBV6 mos
6
16
34
4239
55
70+
0
20
40
60
80
100
DAAs8/12 weeks
>90
2014
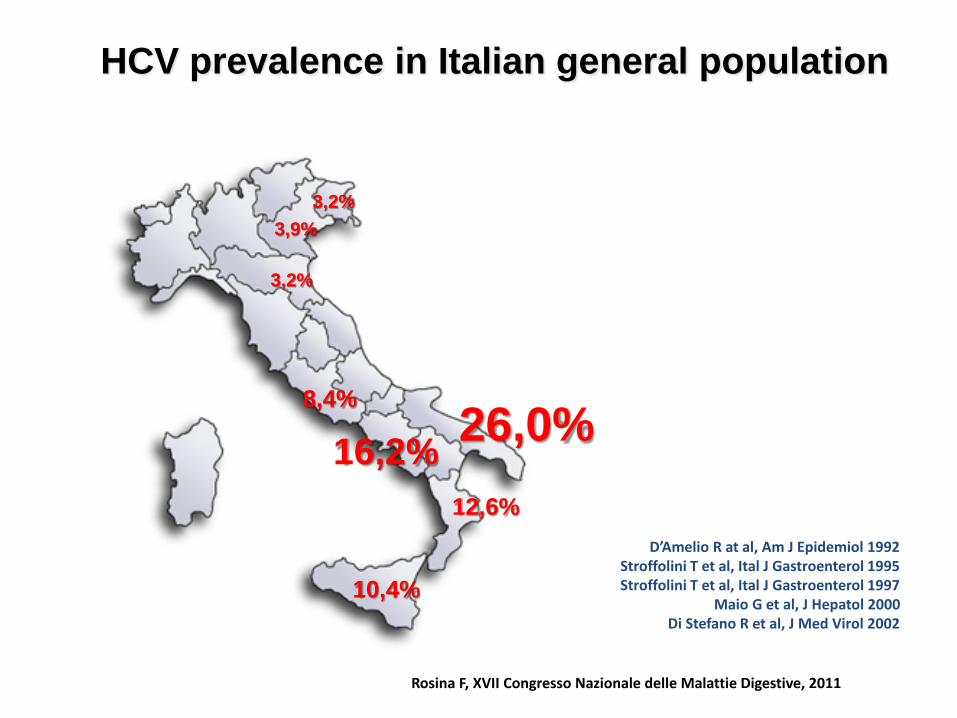
HCV prevalence in Italian general population
Rosina F, XVII Congresso Nazionale delle Malattie Digestive, 2011
D’Amelio R at al, Am J Epidemiol 1992Stroffolini T et al, Ital J Gastroenterol 1995Stroffolini T et al, Ital J Gastroenterol 1997
Maio G et al, J Hepatol 2000Di Stefano R et al, J Med Virol 2002
3,9%
3,2%
8,4%
12,6%
16,2%
10,4%
26,0%
3,2%
Personalized management
of CHC patients:
• accurate selection
of patients to be
treated
• right timing
• tailoring of
antiviral treatment
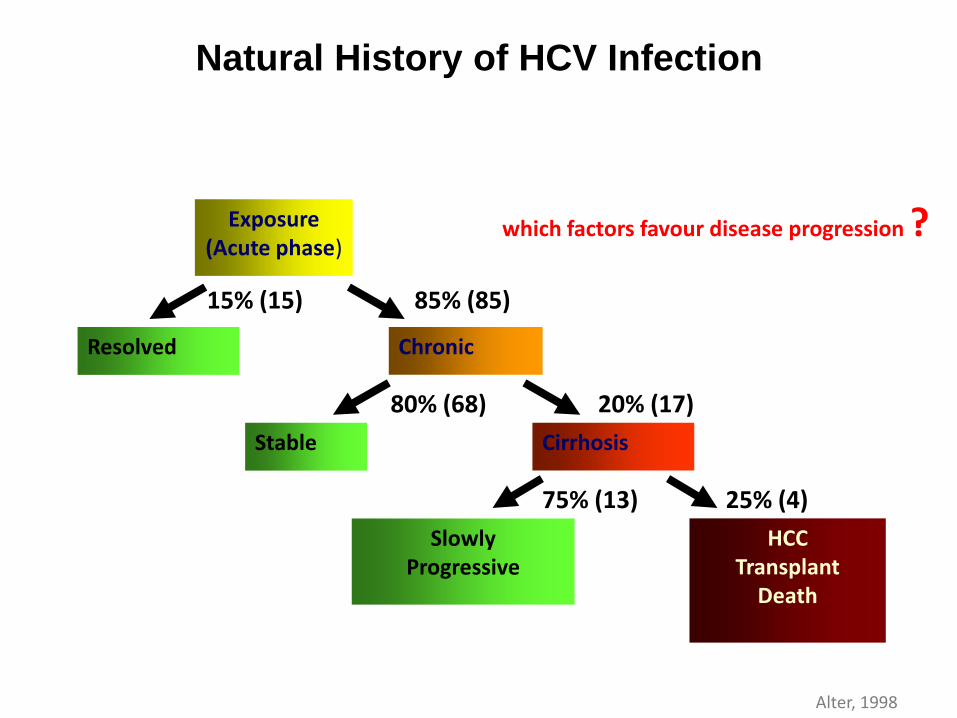
Exposure(Acute phase)
Resolved Chronic
CirrhosisStable
SlowlyProgressive
HCCTransplant
Death
20% (17)
15% (15) 85% (85)
25% (4)
80% (68)
75% (13)
Natural History of HCV Infection
Alter, 1998
which factors favour disease progression ?
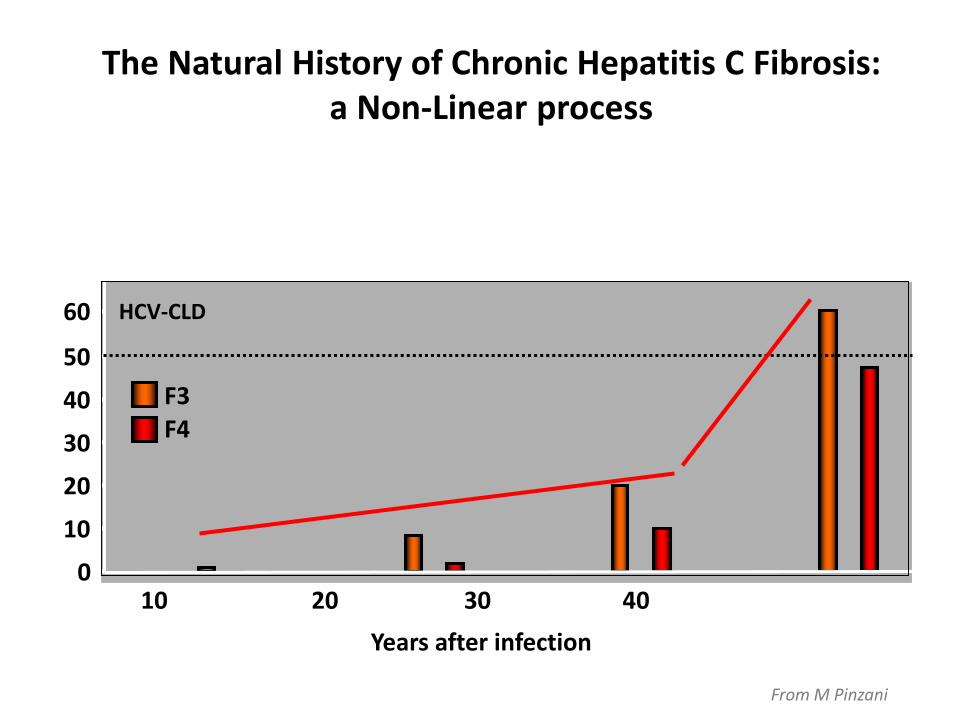
0
10
20
30
40
50
60
10 20 30 40
Years after infection
F3F4
The Natural History of Chronic Hepatitis C Fibrosis: a Non-Linear process
HCV-CLD
From M Pinzani
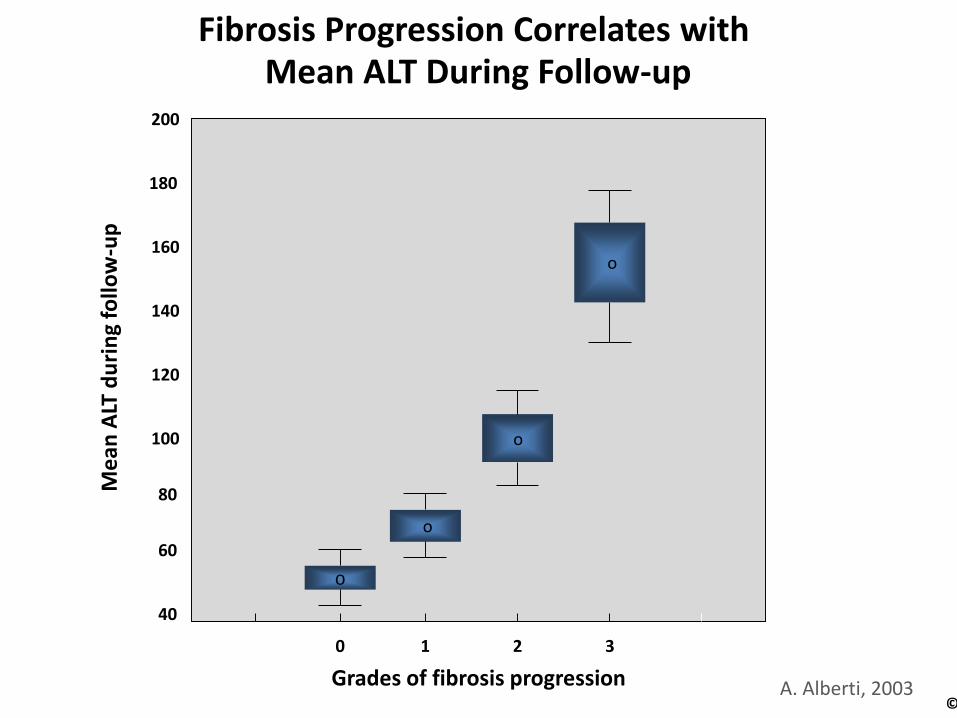
200
180
160
140
100
120
60
80
40
o
o
o
o
Me
an A
LT d
uri
ng
follo
w-u
p
Grades of fibrosis progression
0 1 2 3
Fibrosis Progression Correlates withMean ALT During Follow-up
©A. Alberti, 2003
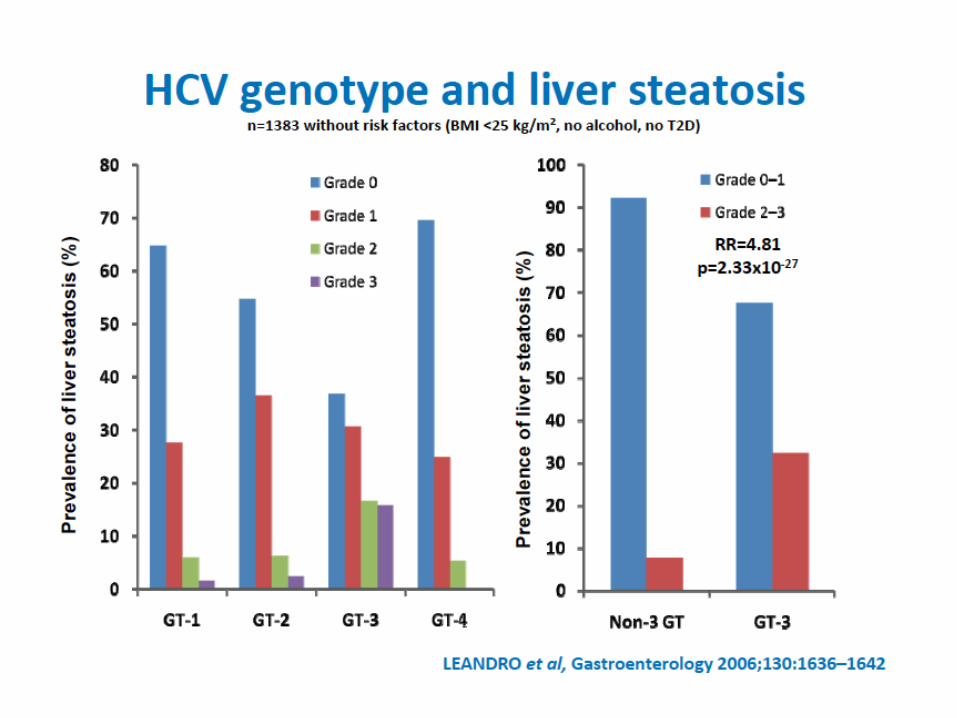
Steatosis
Insulin Resistance
Oxidative Stress
Hepatic Iron storage
Several co-factors may contribute to a faster progression of liver
disease
Cofactors of liver damage
Alcohol
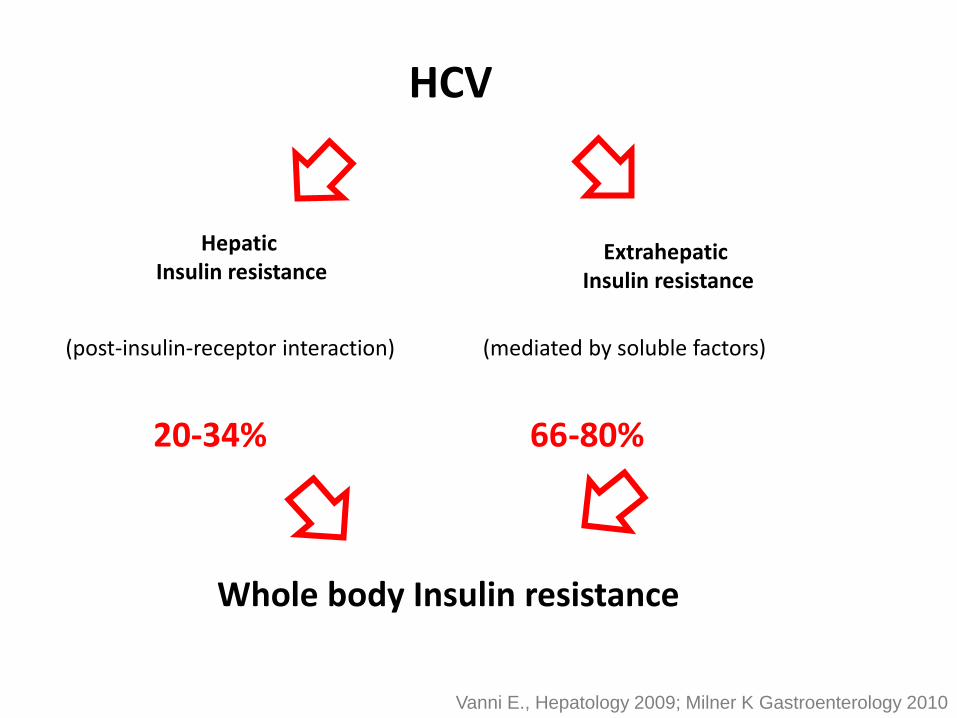
HCV
Hepatic Insulin resistance
Extrahepatic Insulin resistance
(post-insulin-receptor interaction) (mediated by soluble factors)
20-34% 66-80%
Whole body Insulin resistance
Vanni E., Hepatology 2009; Milner K Gastroenterology 2010
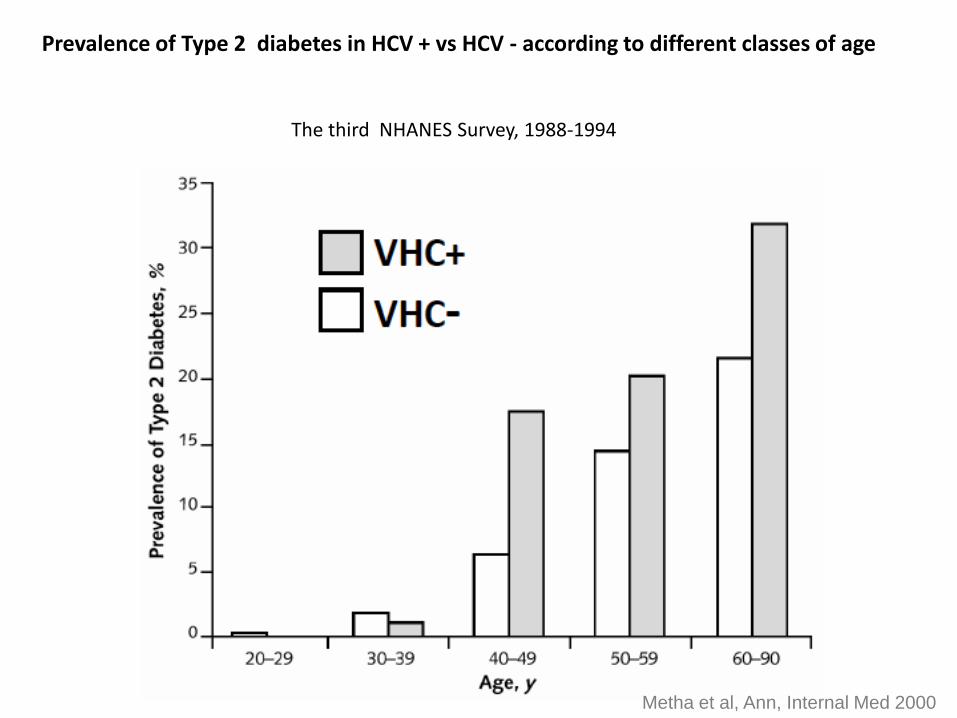
Prevalence of Type 2 diabetes in HCV + vs HCV - according to different classes of age
The third NHANES Survey, 1988-1994
Metha et al, Ann, Internal Med 2000
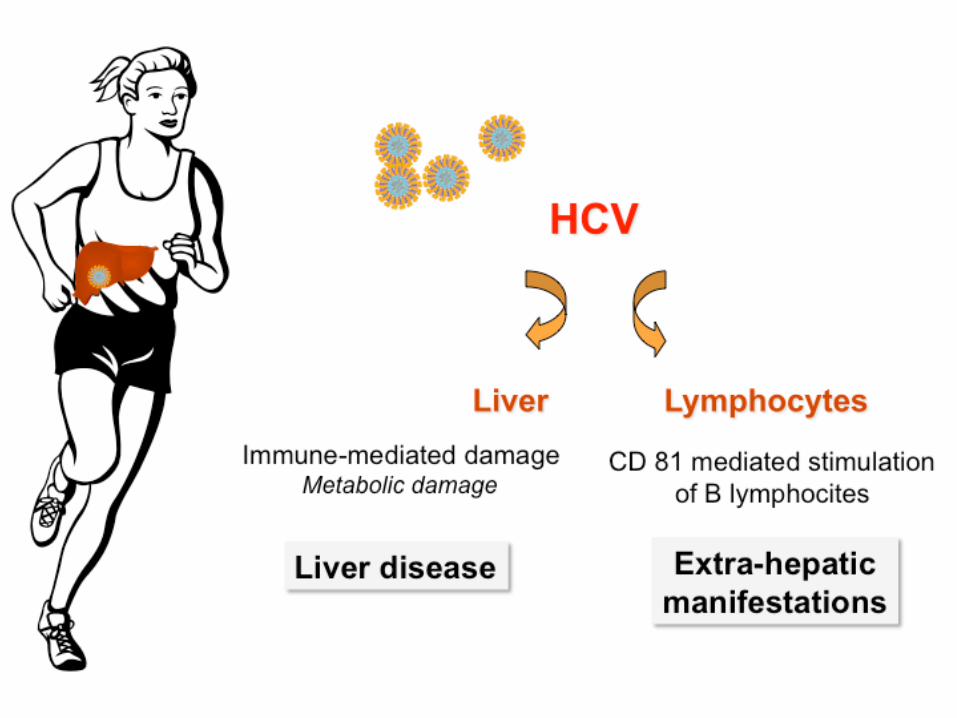
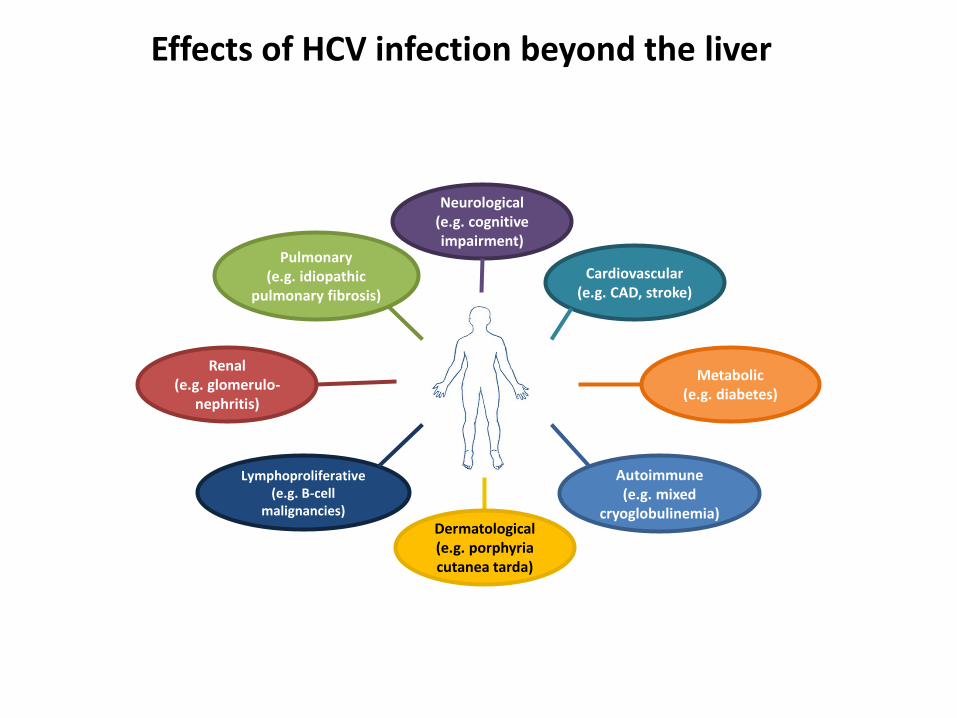
Effects of HCV infection beyond the liver
Renal(e.g. glomerulo-
nephritis)
Pulmonary(e.g. idiopathic
pulmonary fibrosis)
Neurological (e.g. cognitive impairment)
Cardiovascular (e.g. CAD, stroke)
Metabolic (e.g. diabetes)
Lymphoproliferative (e.g. B-cell
malignancies)
Autoimmune(e.g. mixed
cryoglobulinemia)Dermatological (e.g. porphyria cutanea tarda)
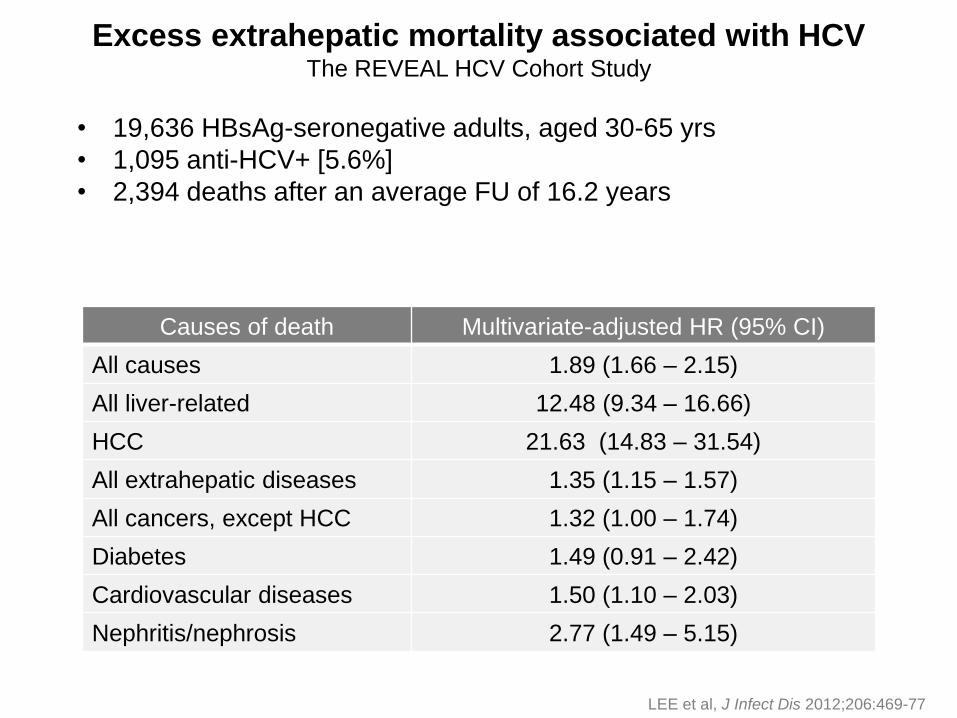
Excess extrahepatic mortality associated with HCVThe REVEAL HCV Cohort Study
• 19,636 HBsAg-seronegative adults, aged 30-65 yrs
• 1,095 anti-HCV+ [5.6%]
• 2,394 deaths after an average FU of 16.2 years
LEE et al, J Infect Dis 2012;206:469-77
Causes of death Multivariate-adjusted HR (95% CI)
All causes 1.89 (1.66 – 2.15)
All liver-related 12.48 (9.34 – 16.66)
HCC 21.63 (14.83 – 31.54)
All extrahepatic diseases 1.35 (1.15 – 1.57)
All cancers, except HCC 1.32 (1.00 – 1.74)
Diabetes 1.49 (0.91 – 2.42)
Cardiovascular diseases 1.50 (1.10 – 2.03)
Nephritis/nephrosis 2.77 (1.49 – 5.15)
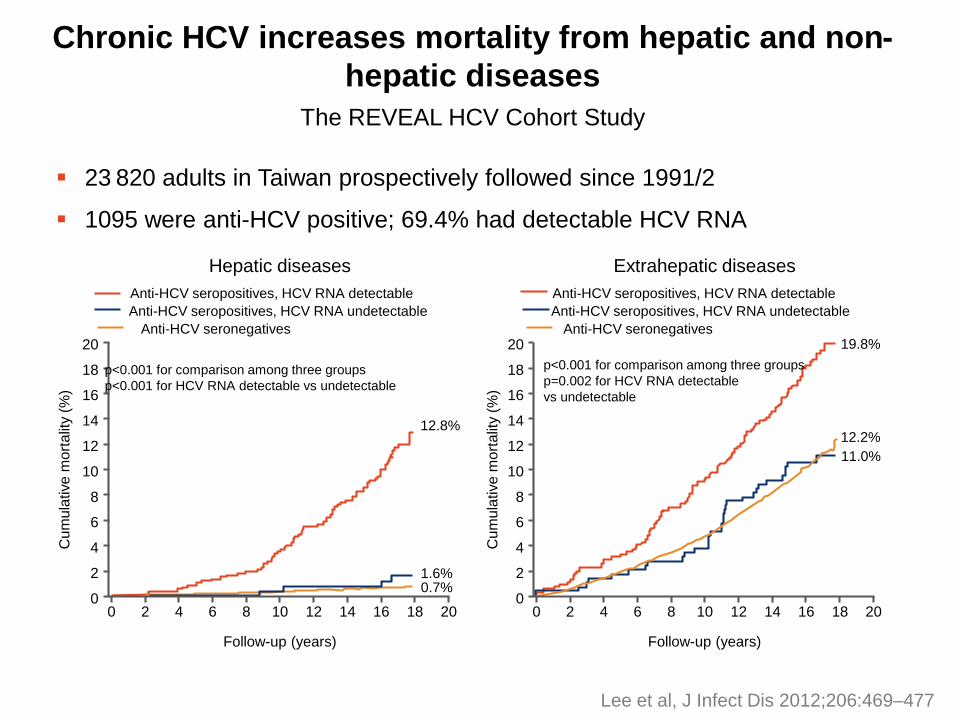
Chronic HCV increases mortality from hepatic and non-
hepatic diseases
23 820 adults in Taiwan prospectively followed since 1991/2
1095 were anti-HCV positive; 69.4% had detectable HCV RNA
The REVEAL HCV Cohort Study
20
18
16
14
12
10
8
6
4
2
0
20
18
16
14
12
10
8
6
4
2
00 2 4 6 8 10 12 14 16 18 20 0 2 4 6 8 10 12 14 16 18 20
Follow-up (years) Follow-up (years)
Cu
mu
lative
mo
rta
lity (
%)
Cu
mu
lative
mo
rta
lity (
%)
Hepatic diseases Extrahepatic diseases
Anti-HCV seropositives, HCV RNA detectable
Anti-HCV seropositives, HCV RNA undetectable
Anti-HCV seronegatives
Anti-HCV seropositives, HCV RNA detectable
Anti-HCV seropositives, HCV RNA undetectable
Anti-HCV seronegatives
p<0.001 for comparison among three groups
p<0.001 for HCV RNA detectable vs undetectable
p<0.001 for comparison among three groups
p=0.002 for HCV RNA detectable
vs undetectable
12.8%
1.6%0.7%
19.8%
12.2%
11.0%
Lee et al, J Infect Dis 2012;206:469–477
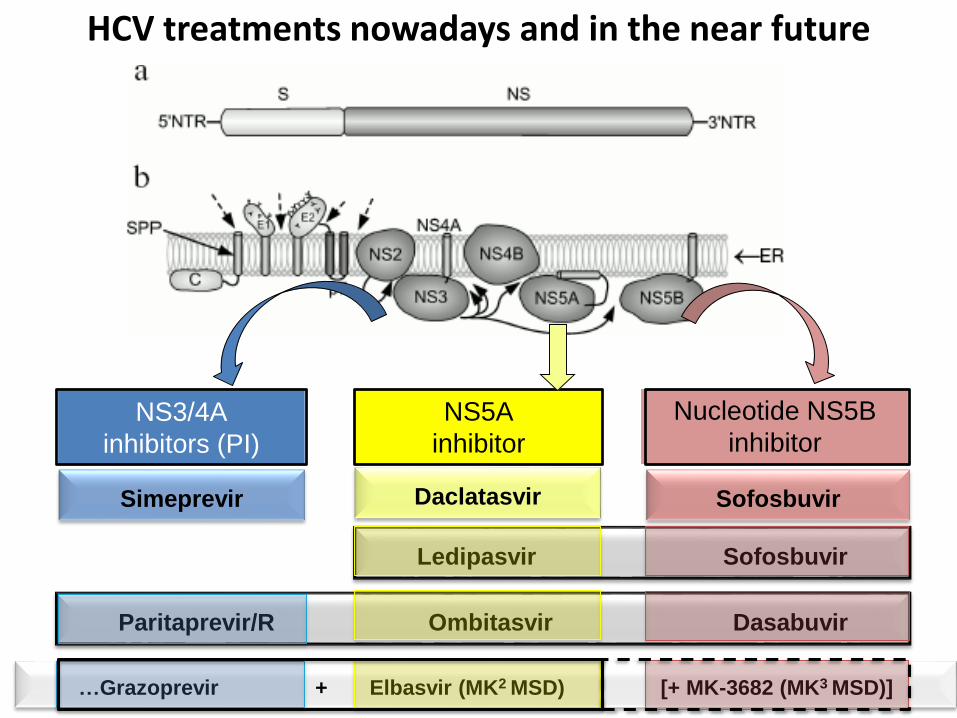
NS3/4A
inhibitors (PI)
NS5A
inhibitor
Daclatasvir
Nucleotide NS5B
inhibitor
HCV treatments nowadays and in the near future
Ledipasvir Sofosbuvir
Simeprevir Sofosbuvir
Paritaprevir/R Ombitasvir Dasabuvir
…Grazoprevir + Elbasvir (MK2 MSD) [+ MK-3682 (MK3 MSD)]
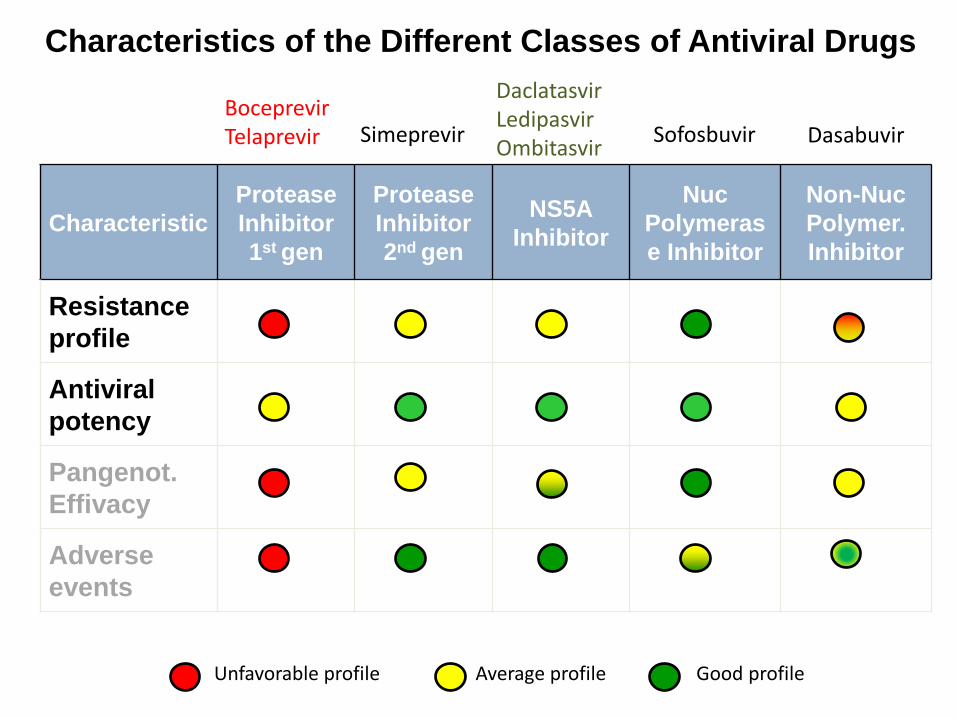
Characteristics of the Different Classes of Antiviral Drugs
Characteristic
Protease
Inhibitor
1st gen
Protease
Inhibitor
2nd gen
NS5A
Inhibitor
Nuc
Polymeras
e Inhibitor
Non-Nuc
Polymer.
Inhibitor
Resistance
profile
Antiviral
potency
Pangenot.
Effivacy
Adverse
events
Good profileAverage profileUnfavorable profile
BoceprevirTelaprevir Simeprevir
DaclatasvirLedipasvirOmbitasvir
Sofosbuvir Dasabuvir
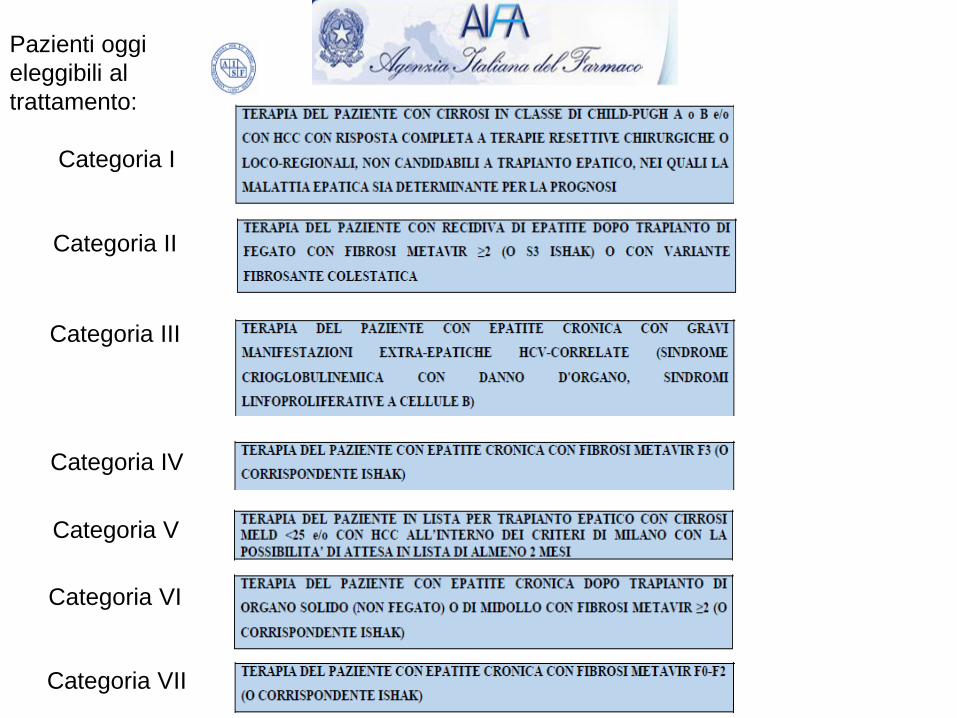
Pazienti oggi
eleggibili al
trattamento:
Categoria I
Categoria II
Categoria VII
Categoria III
Categoria V
Categoria IV
Categoria VI
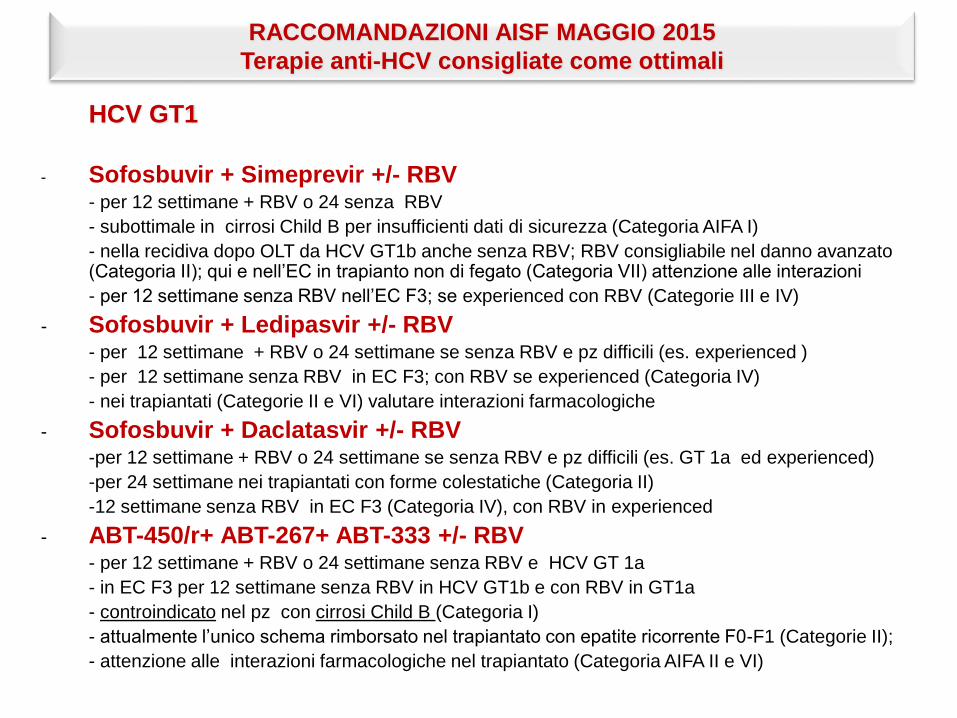
HCV GT1
- Sofosbuvir + Simeprevir +/- RBV - per 12 settimane + RBV o 24 senza RBV
- subottimale in cirrosi Child B per insufficienti dati di sicurezza (Categoria AIFA I)
- nella recidiva dopo OLT da HCV GT1b anche senza RBV; RBV consigliabile nel danno avanzato (Categoria II); qui e nell’EC in trapianto non di fegato (Categoria VII) attenzione alle interazioni
- per 12 settimane senza RBV nell’EC F3; se experienced con RBV (Categorie III e IV)
- Sofosbuvir + Ledipasvir +/- RBV- per 12 settimane + RBV o 24 settimane se senza RBV e pz difficili (es. experienced )
- per 12 settimane senza RBV in EC F3; con RBV se experienced (Categoria IV)
- nei trapiantati (Categorie II e VI) valutare interazioni farmacologiche
- Sofosbuvir + Daclatasvir +/- RBV-per 12 settimane + RBV o 24 settimane se senza RBV e pz difficili (es. GT 1a ed experienced)
-per 24 settimane nei trapiantati con forme colestatiche (Categoria II)
-12 settimane senza RBV in EC F3 (Categoria IV), con RBV in experienced
- ABT-450/r+ ABT-267+ ABT-333 +/- RBV- per 12 settimane + RBV o 24 settimane senza RBV e HCV GT 1a
- in EC F3 per 12 settimane senza RBV in HCV GT1b e con RBV in GT1a
- controindicato nel pz con cirrosi Child B (Categoria I)
- attualmente l’unico schema rimborsato nel trapiantato con epatite ricorrente F0-F1 (Categorie II);
- attenzione alle interazioni farmacologiche nel trapiantato (Categoria AIFA II e VI)
RACCOMANDAZIONI AISF MAGGIO 2015
Terapie anti-HCV consigliate come ottimali
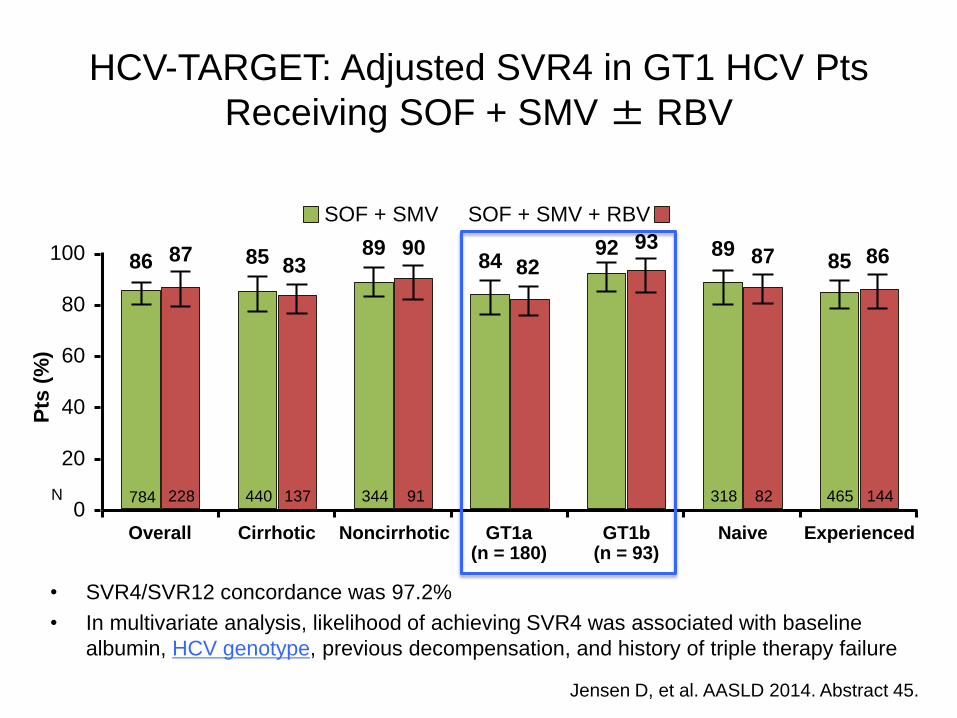
HCV-TARGET: Adjusted SVR4 in GT1 HCV Pts
Receiving SOF + SMV ± RBV
• SVR4/SVR12 concordance was 97.2%
• In multivariate analysis, likelihood of achieving SVR4 was associated with baseline
albumin, HCV genotype, previous decompensation, and history of triple therapy failure
Jensen D, et al. AASLD 2014. Abstract 45.
100
80
60
40
20
0Overall Cirrhotic Noncirrhotic GT1a
(n = 180)GT1b
(n = 93)Naive Experienced
SOF + SMV SOF + SMV + RBV
86 87 85 8389 90
84 8292 93 89 87 85 86
Pts
(%
)
784 228 440 137 344 91 318 82 465 144N
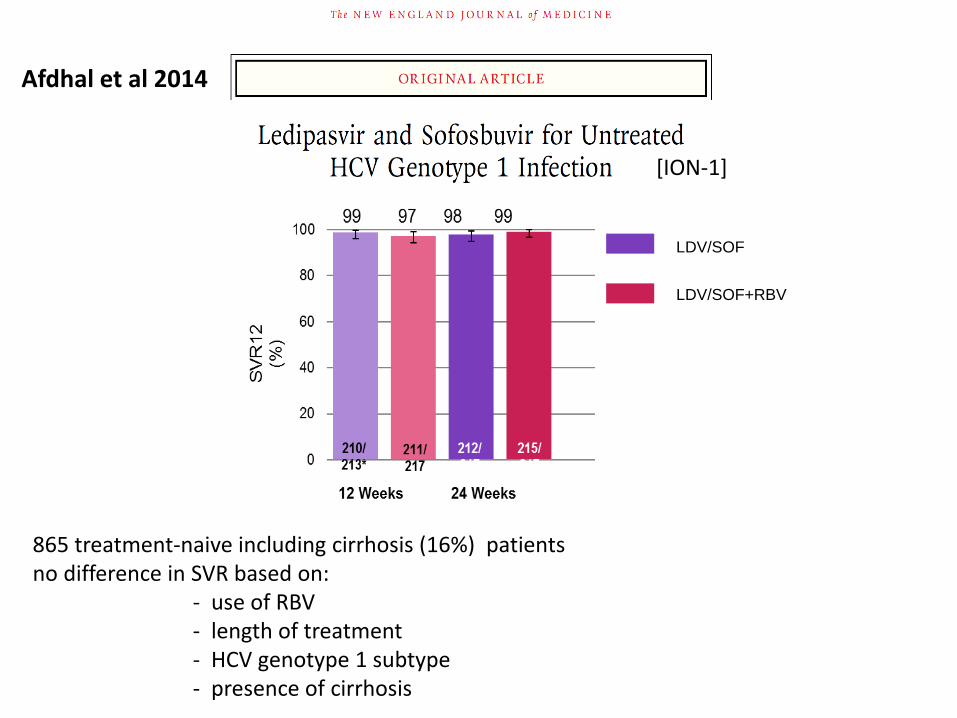
LDV/SOF
LDV/SOF+RBV
Afdhal et al 2014
865 treatment-naive including cirrhosis (16%) patientsno difference in SVR based on:
- use of RBV- length of treatment- HCV genotype 1 subtype- presence of cirrhosis
[ION-1]
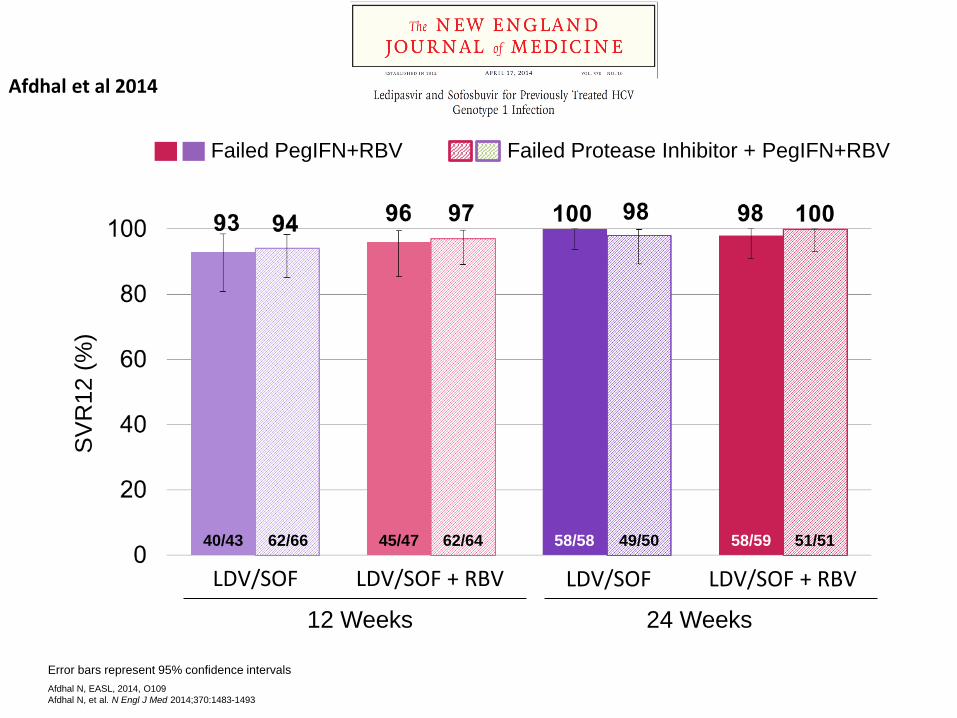
Error bars represent 95% confidence intervals
Afdhal N, EASL, 2014, O109
Afdhal N, et al. N Engl J Med 2014;370:1483-1493
Failed PegIFN+RBV Failed Protease Inhibitor + PegIFN+RBV
SV
R12 (
%)
40/43 62/66 45/47 62/64 58/58 49/50 58/59 51/51
12 Weeks 24 Weeks
LDV/SOF + RBV LDV/SOF + RBVLDV/SOF LDV/SOF
Afdhal et al 2014
100% 100% 100% 100% 95%
0
20
40
60
80
100a
ALIb SOF,
DCV+ SOF
HDCV
+ SOF+ RBV
CDCV
+ SOF
E DCV
+ SOF+ RBV
GDCV
+ SOF
24 weeks
HC
V R
NA
<LL
OQ
Pati
ents
, %
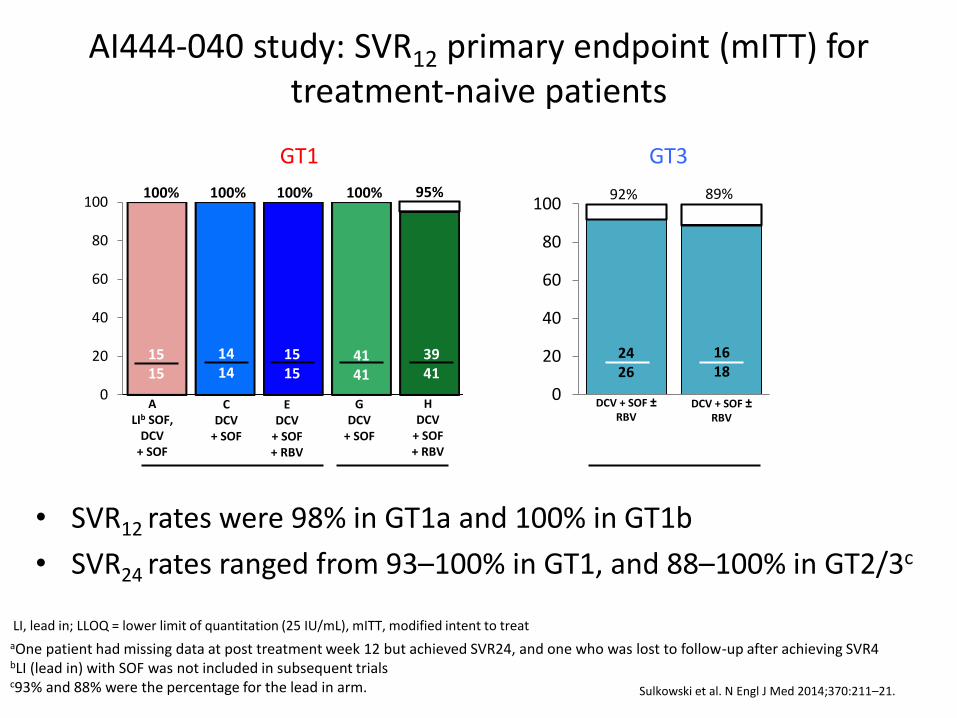
AI444-040 study: SVR12 primary endpoint (mITT) for treatment-naive patients
• SVR12 rates were 98% in GT1a and 100% in GT1b
• SVR24 rates ranged from 93–100% in GT1, and 88–100% in GT2/3c
1515
1414
4141
3941
1515
12 weeks
aOne patient had missing data at post treatment week 12 but achieved SVR24, and one who was lost to follow-up after achieving SVR4bLI (lead in) with SOF was not included in subsequent trialsc93% and 88% were the percentage for the lead in arm.
HC
V R
NA
<LL
OQ
Pati
ents
, %
92% 89%
0
20
40
60
80
100
2426
1618
DCV + SOF ±RBV
24 weeks
DCV + SOF ±RBV
a
LI, lead in; LLOQ = lower limit of quantitation (25 IU/mL), mITT, modified intent to treat
GT1 GT2 GT3
Sulkowski et al. N Engl J Med 2014;370:211–21.
JDCV + SOF
+ RBV
100% 95%
0
20
40
60
80
100
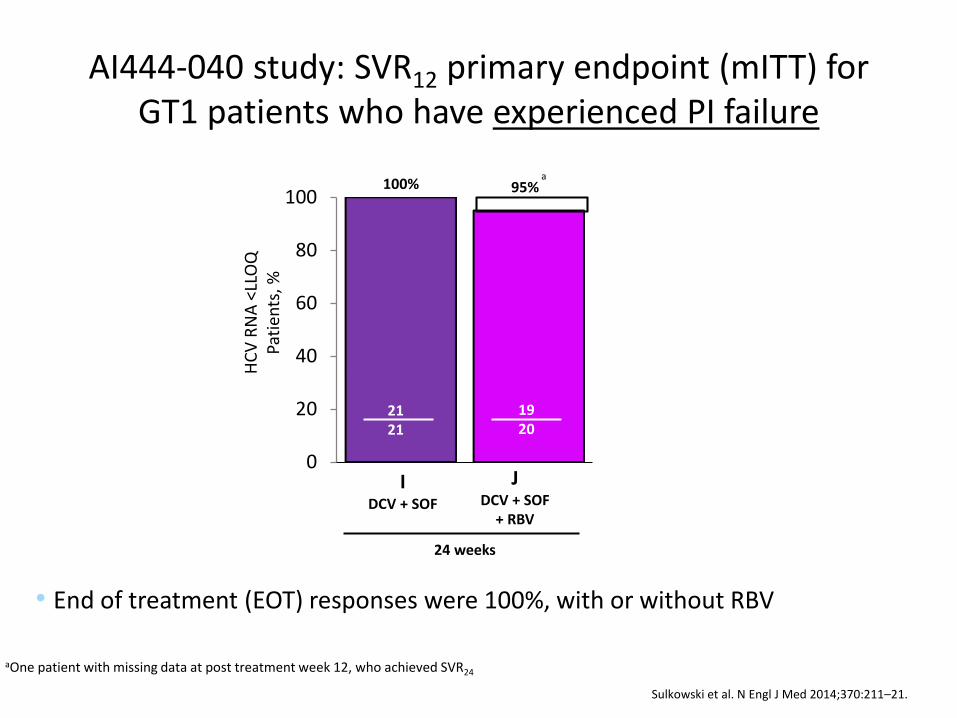
AI444-040 study: SVR12 primary endpoint (mITT) for GT1 patients who have experienced PI failure
aOne patient with missing data at post treatment week 12, who achieved SVR24
IDCV + SOF
2121
1920
24 weeks
a
HC
V R
NA
<LL
OQ
Pati
ents
, %
• End of treatment (EOT) responses were 100%, with or without RBV
Sulkowski et al. N Engl J Med 2014;370:211–21.
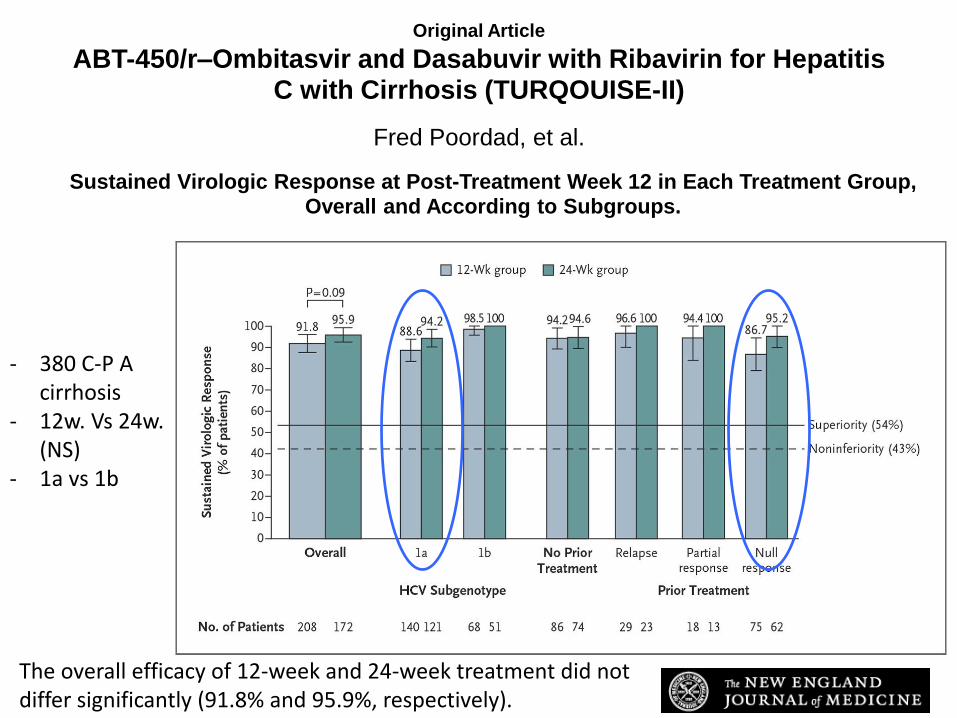
Original Article
ABT-450/r–Ombitasvir and Dasabuvir with Ribavirin for Hepatitis C with Cirrhosis (TURQOUISE-II)
Fred Poordad, et al.
N Engl J MedVolume 370(21):1973-1982
May 22, 2014
Sustained Virologic Response at Post-Treatment Week 12 in Each Treatment Group, Overall and According to Subgroups.
- 380 C-P A cirrhosis
- 12w. Vs 24w. (NS)
- 1a vs 1b
The overall efficacy of 12-week and 24-week treatment did not differ significantly (91.8% and 95.9%, respectively).
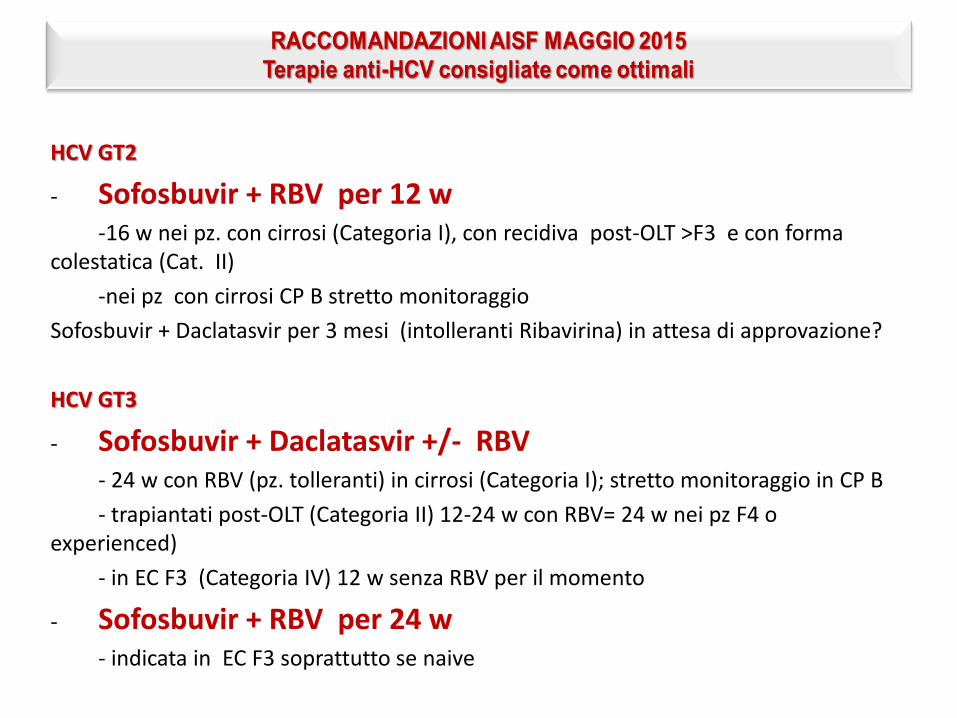
HCV GT2
- Sofosbuvir + RBV per 12 w-16 w nei pz. con cirrosi (Categoria I), con recidiva post-OLT >F3 e con forma
colestatica (Cat. II)
-nei pz con cirrosi CP B stretto monitoraggio
Sofosbuvir + Daclatasvir per 3 mesi (intolleranti Ribavirina) in attesa di approvazione?
HCV GT3
- Sofosbuvir + Daclatasvir +/- RBV - 24 w con RBV (pz. tolleranti) in cirrosi (Categoria I); stretto monitoraggio in CP B
- trapiantati post-OLT (Categoria II) 12-24 w con RBV= 24 w nei pz F4 o experienced)
- in EC F3 (Categoria IV) 12 w senza RBV per il momento
- Sofosbuvir + RBV per 24 w- indicata in EC F3 soprattutto se naive
VALENCE
SOF + RBV
12 wk
LONESTAR-2
SOF + PegIFN + RBV
12 wk
FISSION
SOF + RBV
12 wk
VALENCE
SOF + RBV
12 wk
SV
R12 (
%)
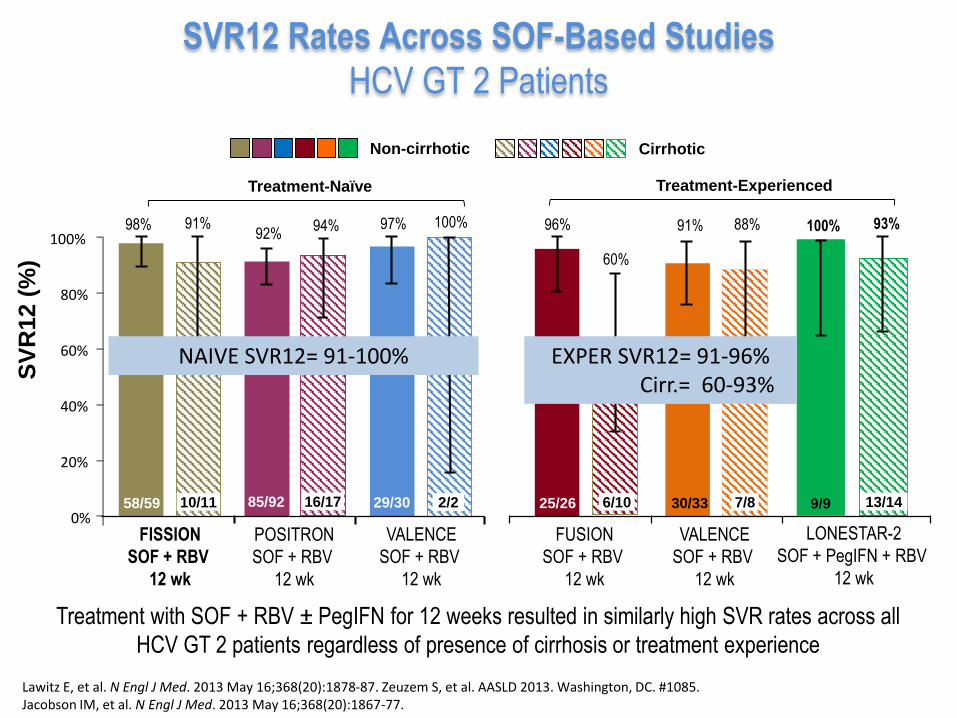
SVR12 Rates Across SOF-Based Studies
HCV GT 2 Patients
Treatment-Naïve Treatment-Experienced
Lawitz E, et al. N Engl J Med. 2013 May 16;368(20):1878-87. Zeuzem S, et al. AASLD 2013. Washington, DC. #1085.Jacobson IM, et al. N Engl J Med. 2013 May 16;368(20):1867-77.
FUSION
SOF + RBV
12 wk
POSITRON
SOF + RBV
12 wk
97% 100%
29/30 2/20%
20%
40%
60%
80%
100%98%
58/59
91%
10/11
60%
96%
25/26 6/10
91% 88%
30/33 7/8
92%
85/92
94%
16/17
100%
9/9
93%
13/14
Non-cirrhotic Cirrhotic
Treatment with SOF + RBV ± PegIFN for 12 weeks resulted in similarly high SVR rates across all
HCV GT 2 patients regardless of presence of cirrhosis or treatment experience
NAIVE SVR12= 91-100% EXPER SVR12= 91-96%Cirr.= 60-93%
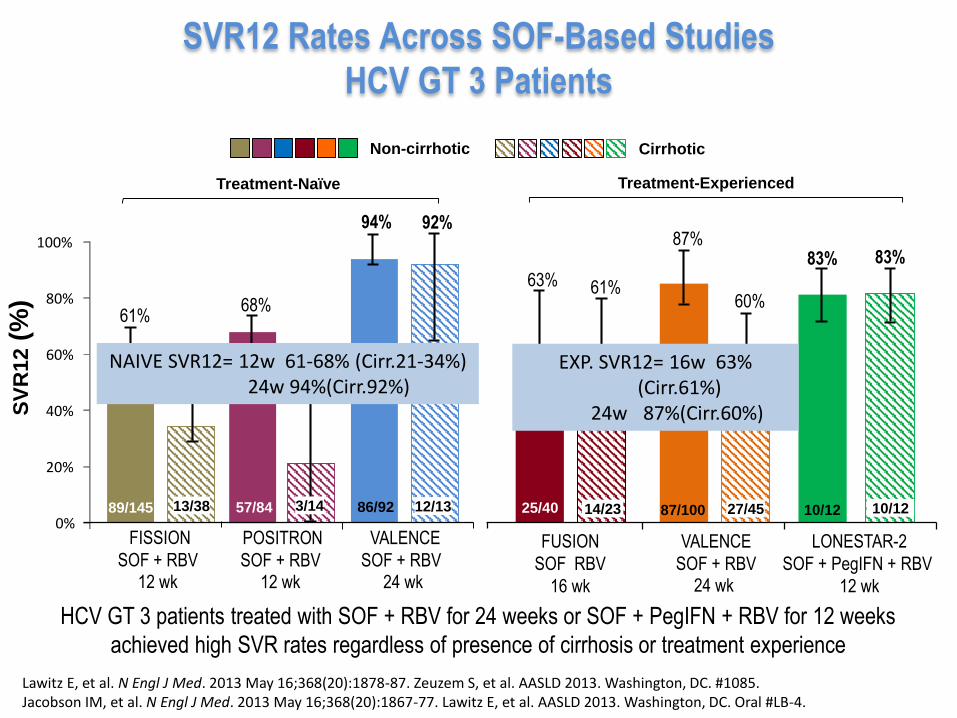
SVR12 Rates Across SOF-Based Studies
HCV GT 3 Patients
Treatment-Naïve Treatment-Experienced
Lawitz E, et al. N Engl J Med. 2013 May 16;368(20):1878-87. Zeuzem S, et al. AASLD 2013. Washington, DC. #1085.Jacobson IM, et al. N Engl J Med. 2013 May 16;368(20):1867-77. Lawitz E, et al. AASLD 2013. Washington, DC. Oral #LB-4.
Non-cirrhotic Cirrhotic
61%
87%
60%
SV
R12
(%)
89/145 86/92
FUSION
SOF RBV
16 wk
VALENCE
SOF + RBV24 wk
LONESTAR-2
SOF + PegIFN + RBV
12 wk
87/10014/23
83%
10/12
92%94%
12/13 25/40
63%
27/45
83%
10/12
68%
21%
61%
34%
0%
20%
40%
60%
80%
100%
FISSION
SOF + RBV 12 wk
VALENCE
SOF + RBV 24 wk
13/38
POSITRON
SOF + RBV 12 wk
57/84 3/14
HCV GT 3 patients treated with SOF + RBV for 24 weeks or SOF + PegIFN + RBV for 12 weeks
achieved high SVR rates regardless of presence of cirrhosis or treatment experience
NAIVE SVR12= 12w 61-68% (Cirr.21-34%)24w 94%(Cirr.92%)
EXP. SVR12= 16w 63% (Cirr.61%)
24w 87%(Cirr.60%)
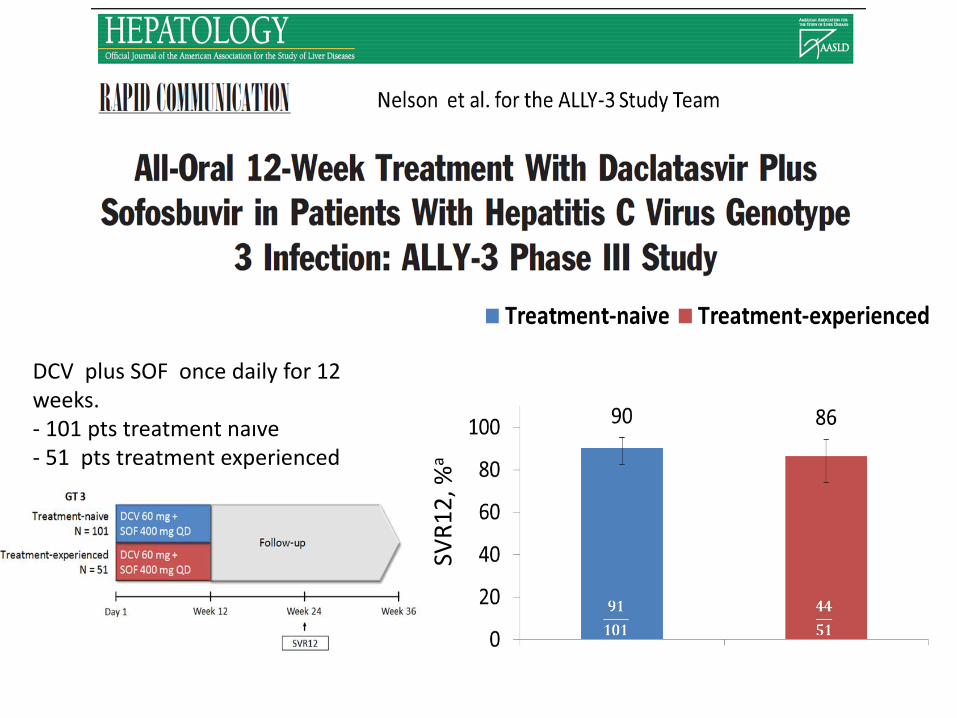
SVR
12
, %a
DCV plus SOF once daily for 12 weeks.- 101 pts treatment naıve - 51 pts treatment experienced
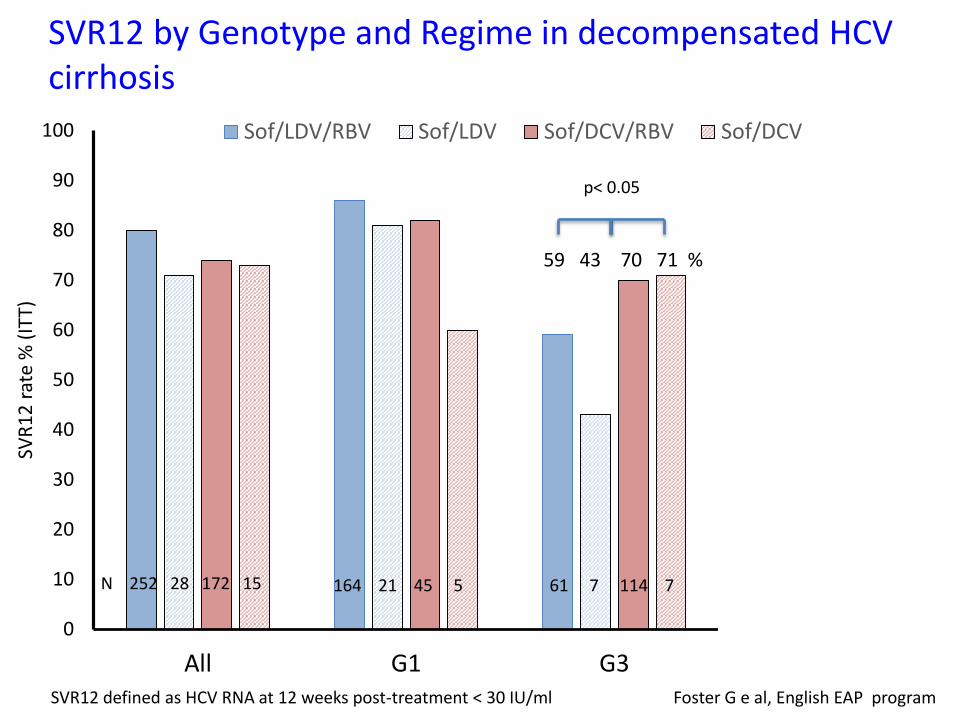
SVR12 by Genotype and Regime in decompensated HCV cirrhosis
0
10
20
30
40
50
60
70
80
90
100
All G1 G3 Others
SVR
12
rat
e %
(IT
T)
Sof/LDV/RBV Sof/LDV Sof/DCV/RBV Sof/DCV
61 7 114 7 27 13 3
59 43 70 71 %
89 85 100 %
SVR12 defined as HCV RNA at 12 weeks post-treatment < 30 IU/ml Foster G e al, English EAP program
N 252 28 172 15 164 21 45 5
p< 0.05
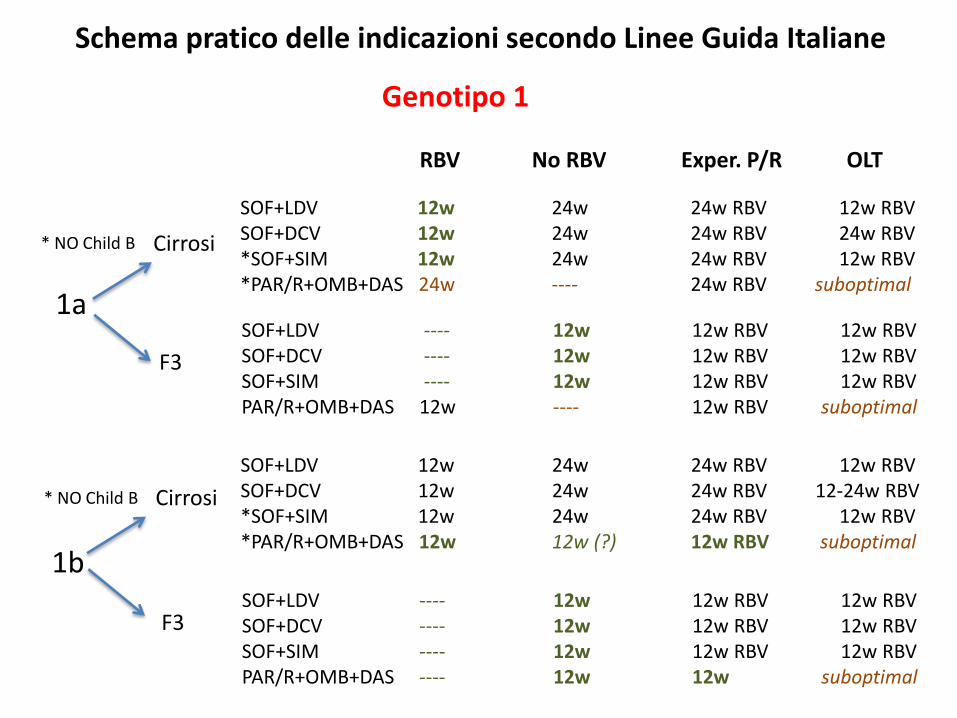
Schema pratico delle indicazioni secondo Linee Guida Italiane
Genotipo 1
1a
1b
RBV No RBV Exper. P/R OLT
Cirrosi
F3
Cirrosi
F3
SOF+LDV 12w 24w 24w RBV 12w RBVSOF+DCV 12w 24w 24w RBV 24w RBV *SOF+SIM 12w 24w 24w RBV 12w RBV*PAR/R+OMB+DAS 24w ---- 24w RBV suboptimal
SOF+LDV 12w 24w 24w RBV 12w RBVSOF+DCV 12w 24w 24w RBV 12-24w RBV *SOF+SIM 12w 24w 24w RBV 12w RBV*PAR/R+OMB+DAS 12w 12w (?) 12w RBV suboptimal
SOF+LDV ---- 12w 12w RBV 12w RBVSOF+DCV ---- 12w 12w RBV 12w RBV SOF+SIM ---- 12w 12w RBV 12w RBVPAR/R+OMB+DAS 12w ---- 12w RBV suboptimal
* NO Child B
* NO Child B
SOF+LDV ---- 12w 12w RBV 12w RBVSOF+DCV ---- 12w 12w RBV 12w RBV SOF+SIM ---- 12w 12w RBV 12w RBVPAR/R+OMB+DAS ---- 12w 12w suboptimal
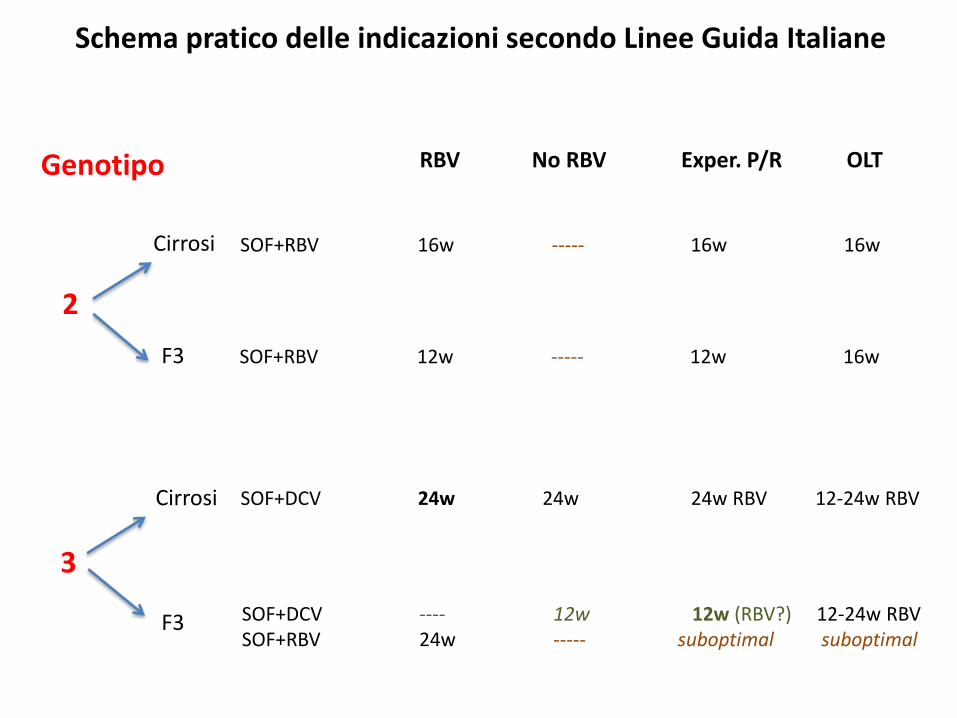
Schema pratico delle indicazioni secondo Linee Guida Italiane
Genotipo
2
3
Cirrosi
Cirrosi
F3
SOF+RBV 16w ----- 16w 16w
SOF+DCV 24w 24w 24w RBV 12-24w RBV
SOF+DCV ---- 12w 12w (RBV?) 12-24w RBV SOF+RBV 24w ----- suboptimal suboptimal
RBV No RBV Exper. P/R OLT
F3 SOF+RBV 12w ----- 12w 16w
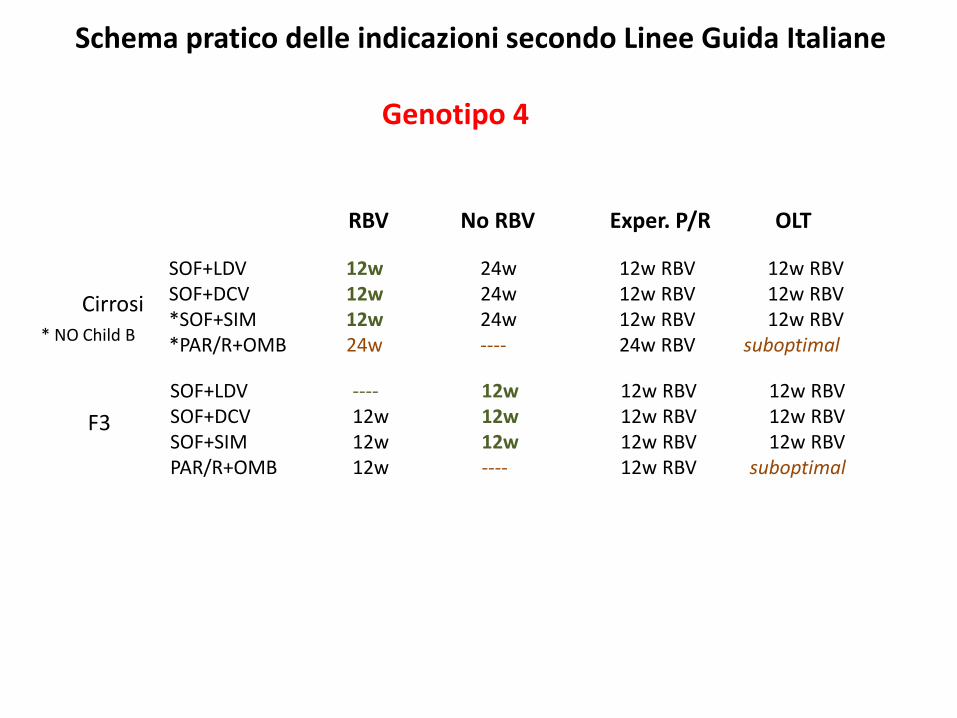
Schema pratico delle indicazioni secondo Linee Guida Italiane
Genotipo 4
RBV No RBV Exper. P/R OLT
Cirrosi
F3
SOF+LDV 12w 24w 12w RBV 12w RBVSOF+DCV 12w 24w 12w RBV 12w RBV *SOF+SIM 12w 24w 12w RBV 12w RBV*PAR/R+OMB 24w ---- 24w RBV suboptimal
SOF+LDV ---- 12w 12w RBV 12w RBVSOF+DCV 12w 12w 12w RBV 12w RBV SOF+SIM 12w 12w 12w RBV 12w RBVPAR/R+OMB 12w ---- 12w RBV suboptimal
* NO Child B
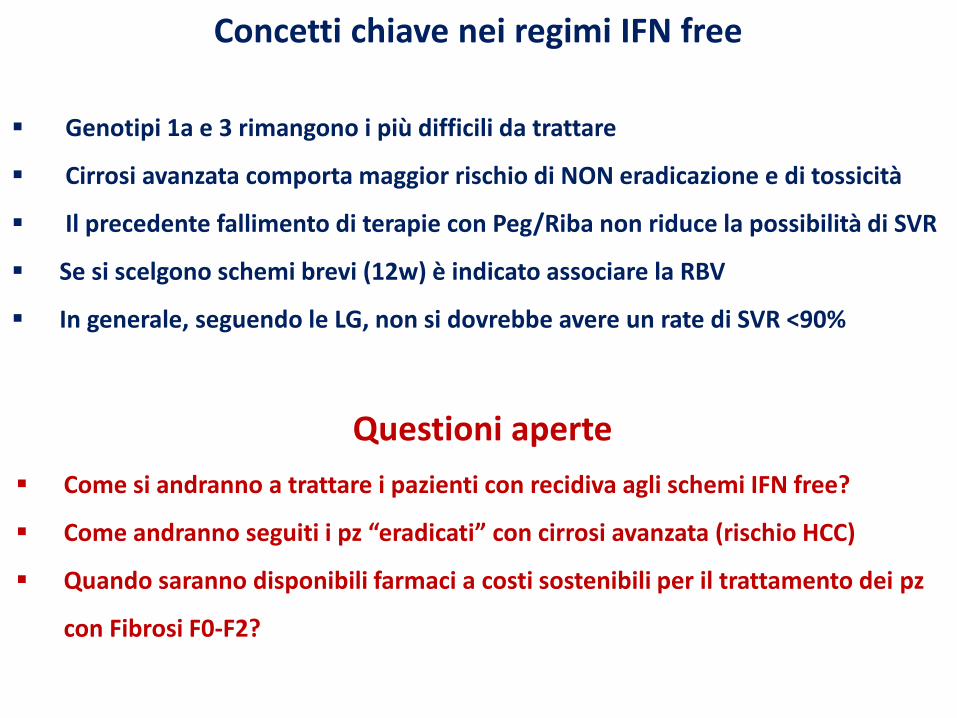
Concetti chiave nei regimi IFN free
Genotipi 1a e 3 rimangono i più difficili da trattare
Cirrosi avanzata comporta maggior rischio di NON eradicazione e di tossicità
Il precedente fallimento di terapie con Peg/Riba non riduce la possibilità di SVR
Se si scelgono schemi brevi (12w) è indicato associare la RBV
In generale, seguendo le LG, non si dovrebbe avere un rate di SVR <90%
Questioni aperte
Come si andranno a trattare i pazienti con recidiva agli schemi IFN free?
Come andranno seguiti i pz “eradicati” con cirrosi avanzata (rischio HCC)
Quando saranno disponibili farmaci a costi sostenibili per il trattamento dei pz
con Fibrosi F0-F2?
Grazie per l’attenzione










![Elizabeth Sherman, PharmD, AAHIVPhivaidsinstitute.med.miami.edu/documents/...HIV-HCV...• SVR rates similar to HCV monoinfected [1,2] • In HCV/HIV coinfection, treat HCV as though](https://img.pdfslide.net/doc/110x75/5fbc30e57653e03e261e9924/elizabeth-sherman-pharmd-aa-a-svr-rates-similar-to-hcv-monoinfected-12.jpg)


















