Embed Size (px)
Citation preview
Vito BorzìU.O. I Medicina
Az. Osp. Univ. Vittorio Emanuele – Ferrarotto – S.Bambino
Catania
Nuove frontiere della terapia insulinica
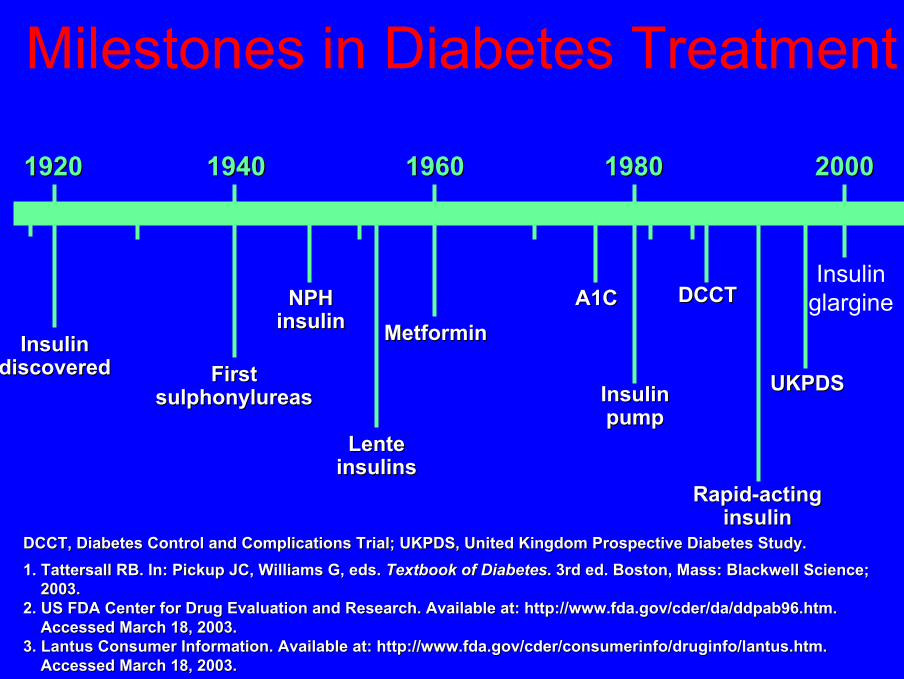
Milestones in Diabetes Treatment
Insulin glargine
Insulin Insulin discovereddiscovered First First
sulphonylureassulphonylureas
NPHNPHinsulininsulin
LenteLenteinsulinsinsulins
MetforminMetformin
Insulin Insulin pumppump
RapidRapid--acting acting insulininsulin
UKPDSUKPDS
19201920 19401940 19601960 19801980 20002000
A1CA1C DCCTDCCT
DCCT, Diabetes Control and Complications Trial; UKPDS, United KiDCCT, Diabetes Control and Complications Trial; UKPDS, United Kingdom Prospective Diabetes Study.ngdom Prospective Diabetes Study.1. 1. TattersallTattersall RB. In: Pickup JC, Williams G, eds. RB. In: Pickup JC, Williams G, eds. Textbook of DiabetesTextbook of Diabetes. 3rd ed. Boston, Mass: Blackwell Science; . 3rd ed. Boston, Mass: Blackwell Science;
2003.2003.2. US FDA Center for Drug Evaluation and Research. Available at:2. US FDA Center for Drug Evaluation and Research. Available at: http://www.fda.gov/cder/da/ddpab96.htm. http://www.fda.gov/cder/da/ddpab96.htm.
Accessed March 18, 2003.Accessed March 18, 2003.3. Lantus Consumer Information. Available at: http://3. Lantus Consumer Information. Available at: http://www.fda.gov/cder/consumerinfo/druginfo/lantus.htmwww.fda.gov/cder/consumerinfo/druginfo/lantus.htm. .
Accessed March 18, 2003.Accessed March 18, 2003.

Complications DCCT1,2 Ohkubo3 UKPDS4
of diabetes mellitus (9% 7%) (9% 7%) (8% 7%)
Retinopathy -63% -69% -21%
Nephropathy -54% -70% -34%
Neuropathy -60% – –
Macrovascular disease -41%* – -16%*
Risk reduction by decrease in A1C (%)
Good Glycaemic Control Reduces Incidence of Complications
*Not statistically significant. *Not statistically significant. DCCT, Diabetes Control and Complications Trial; UKPDS, United KiDCCT, Diabetes Control and Complications Trial; UKPDS, United Kingdom Prospective Diabetes Study.ngdom Prospective Diabetes Study.1. DCCT Research Group. 1. DCCT Research Group. N Engl J MedN Engl J Med. 1993;329:977. 1993;329:977--986. 986. 2. DCCT Research Group. 2. DCCT Research Group. DiabetesDiabetes. 1995;44:968. 1995;44:968--983.983.3. Ohkubo Y et al. 3. Ohkubo Y et al. Diabetes Res Clin PractDiabetes Res Clin Pract. 1995;28:103. 1995;28:103--117. 117. 4. UKPDS Group. 4. UKPDS Group. LancetLancet. 1998;352:837. 1998;352:837--853.853.
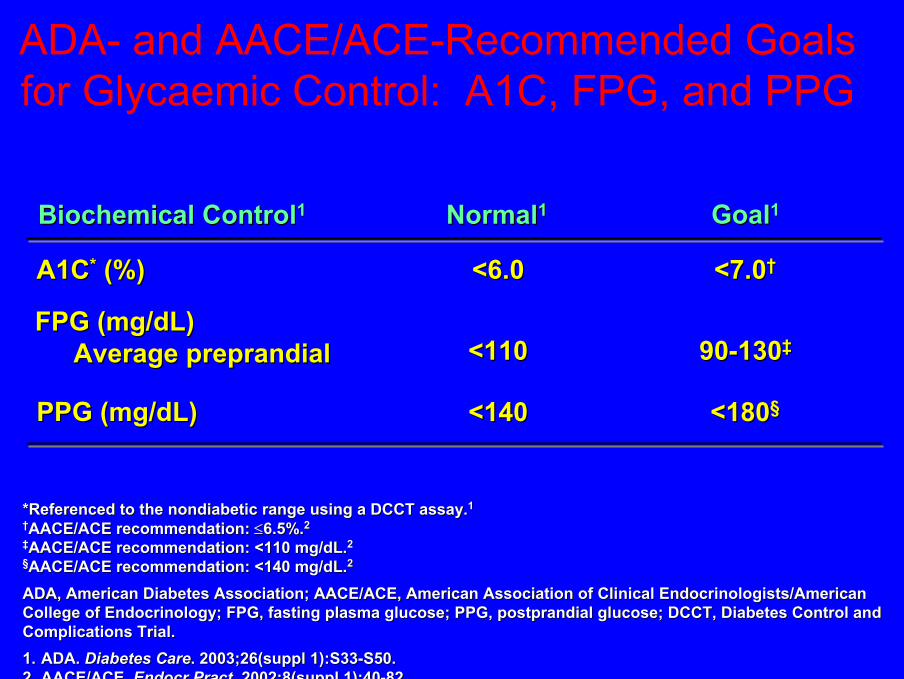
ADA- and AACE/ACE-Recommended Goals for Glycaemic Control: A1C, FPG, and PPG
NormalNormal11 GoalGoal11Biochemical ControlBiochemical Control11
A1CA1C** (%)(%) <6.0<6.0 <7.0<7.0††
FPG (mg/dL)FPG (mg/dL)Average preprandialAverage preprandial <110<110 9090--130130‡‡
PPG (mg/dL)PPG (mg/dL) <140<140 <180<180§§
*Referenced to the *Referenced to the nondiabeticnondiabetic range using a DCCT assay.range using a DCCT assay.11
††AACE/ACE recommendation: AACE/ACE recommendation: ≤≤6.5%.6.5%.22
‡‡AACE/ACE recommendation: <110 mg/dL.AACE/ACE recommendation: <110 mg/dL.22
§§AACE/ACE recommendation: <140 mg/dL.AACE/ACE recommendation: <140 mg/dL.22
ADA, American Diabetes Association; AACE/ACE, American AssociatiADA, American Diabetes Association; AACE/ACE, American Association of Clinical Endocrinologists/American on of Clinical Endocrinologists/American College of Endocrinology; FPG, fasting plasma glucose; PPG, postCollege of Endocrinology; FPG, fasting plasma glucose; PPG, postprandial glucose; DCCT, Diabetes Control and prandial glucose; DCCT, Diabetes Control and Complications Trial.Complications Trial.1.1. ADA. ADA. Diabetes CareDiabetes Care. 2003;26(suppl 1):S33. 2003;26(suppl 1):S33--S50.S50.2.2. AACE/ACE. AACE/ACE. EndocrEndocr PractPract. 2002;8(suppl 1):40. 2002;8(suppl 1):40--82.82.

Optimising Insulin Therapy

Glu
cose
(G
luco
se ( m
mol
/lm
mol
/l )) 9.09.0
5.05.0
160160
00
7.07.0
320320
480480
Insu
lin (
Insu
lin ( p
mol
/lpm
ol/l ))
Glucose HomeostasisGlucose Homeostasis
Mean Mean ±± 2SD 2SD
07000700 12001200 18001800 24002400 0600 hrs0600 hrs
Normal SubjectsNormal Subjects
CiofettaCiofetta M. et al., M. et al., DIabetesDIabetes CareCare 22:79522:795--800, 1999800, 1999
MealsMeals

Glucose
Post-challenge insulin secretion
Time
Phasic insulin release: basal vs. post-challenge
Insu
lin

Glucose
Post-challenge insulin secretion
Time
Insu
lin
Basal insulin secretion
Phasic insulin release: basal vs. post-challenge

Mimicking Nature for Effective Therapy
• Meal-related medication to mimickprandial insulin secretion1
– Short-acting insulin and insulin analogues2
• Medication that mimicks basal insulin secretion2,3
– Long-acting insulin
1.1. McCall AL. In: Leahy JL, McCall AL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin TherapyInsulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.. New York, NY: Marcel Dekker, Inc.; 2002.2.2. Leahy JL. In: Leahy JL, Leahy JL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin TherapyInsulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.. New York, NY: Marcel Dekker, Inc.; 2002.3.3. WittlinWittlin SD et al. In: SD et al. In: Leahy JL, Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin TherapyInsulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.. New York, NY: Marcel Dekker, Inc.; 2002.

BB DDLL HSHS
Insu
lin E
ffect
Insu
lin E
ffect
Bolus InsulinBolus Insulin
Basal InsulinBasal Insulin
Endogenous InsulinEndogenous Insulin
B, breakfast; L, lunch; D, dinner; HS, bedtime.B, breakfast; L, lunch; D, dinner; HS, bedtime.
Adapted from:Adapted from:1.1. Leahy JL. In: Leahy JL, Leahy JL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin Therapy. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.New York, NY: Marcel Dekker, Inc.; 2002.2.2. BolliBolli GB et al. GB et al. DiabetologiaDiabetologia. . 1999;42:11511999;42:1151--1167.1167.
Normal Insulin Secretion: The Basal-Bolus Insulin Concept
Time of AdministrationTime of Administration

Insulin Onset of Peak of Duration ofPreparations Action Action (h) Action (h)
Short-actingRegular human 30-60 min 2-4 6-8Lispro/Aspart 5-15 min 1-2 3-4
Intermediate-actingNPH 1-3 h 5-7 13-16Lente 1-3 h 4-8 13-20
Long-actingGlargine 1-2 h Peakless >24 Ultralente 2-4 h 8-14 <20
Time course of action of any insulin can vary in different people or at different times in the same person; thus, time periods indicated here should only be considered general guidelines.
Comparison of Human Insulins and Analogues
Leahy JL. In: Leahy JL, Leahy JL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin TherapInsulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.y. New York, NY: Marcel Dekker, Inc.; 2002.

40
80
120
0
insu
linem
ia (mU/l)
colazionepranzo cena
08 13 20 08

Insu
lin E
ffect
MEALBOLUS
Afternoon
MEALBOLUS
Evening
BASALINFUSION
Night
MEALBOLUS
Morning
Continuous Subcutaneous Insulin InfusionContinuous Subcutaneous Insulin Infusion

DISSOCIATION
Short-acting(soluble) insulin
Hexamer
Monomer
CapillaryLong-actinginsulins
Insulin crystalor particle
DISSOLUTION
Dimer
Tissue-boundinsulin
Monomer
DIFFUSION
Injection Site

80
60
40
20
00 2 4 6 8 10 12
Plas
ma
Free
Insu
lin (µ
U/m
l)
Time After Insulin Injection or Meal Ingestion (Hrs)
Normal postprandial values(Mean±SD, n=23)
S.c. injection of soluble insulinin diabetic subjects(Mean ± SEM, n=20)
Bolli G.B., N.Engl.J.Med. 310:1706-11, 1984
PLASMAPLASMAINSULININSULIN
S.c. injection of lisproin diabetic subjects(Mean ± SEM, n=10)

Time-Action Curves of Regular and Lispro/Aspart Insulin
MealMealSC injectionSC injection
Time (min)Time (min) Time (min)Time (min)
AspartAspart
Glu
cose
Infu
sion
Rat
e G
luco
se In
fusi
on R
ate
(mg/
min
)(m
g/m
in)11
Plas
ma
Insu
lin (p
mol
/L)
Plas
ma
Insu
lin (p
mol
/L)22
MealMealSC injectionSC injection
SC, subcutaneous.SC, subcutaneous.
1. Campbell RK et al. 1. Campbell RK et al. Ann Pharmacother.Ann Pharmacother. 1996;30:12631996;30:1263--1271.1271.2. 2. MudaliarMudaliar SR et al. SR et al. Diabetes CareDiabetes Care. 1999;22:1501. 1999;22:1501--1506.1506.
00 5050 100100 150150 200200 300300250250
400400350350300300250250200200150150100100505000
450450500500LisproLispro
RegularRegularhumanhumaninsulininsulin
00 6060 120120 180180 240240
400400
300300
200200
100100
00
500500
600600
700700
300300
RegularRegularhumanhumaninsulininsulin

Formulazione Humalog® Mix25™ e Mix50™
Humalog Mix25
Humalog Mix50
NPL
75%
50%
25%
50%
Humalog

Farmacocinetica: Humalog®, Miscele di Humalog e NPL
Dati adattati da Heise T et al. Diabetes Care 1998;21(5):800-803.
Tempo (ore dopo la somministrazione)0 2 4 6 8 10 12 14 16 18 20 22 24
Con
cent
razi
oni s
eric
he d
’insu
lina
(ng/
ml)
0
1
2
3
4
5
6
7
Le proprietà farmacocinetiche di Humalog, inclusa la rapidità d’azione,
sono mantenute nelle miscele stabili di Humalog e NPL
Humalog
Humalog Mix25™Humalog Mix50™
Humalog NPL
N=30 Soggetti non-diabeticidosaggio 0.3 U/kg

BB DDLL HSHS
Insu
lin E
ffect
Insu
lin E
ffect
Bolus InsulinBolus Insulin
Basal InsulinBasal Insulin
Endogenous InsulinEndogenous Insulin
B, breakfast; L, lunch; D, dinner; HS, bedtime.B, breakfast; L, lunch; D, dinner; HS, bedtime.
Adapted from:Adapted from:1.1. Leahy JL. In: Leahy JL, Leahy JL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin Therapy. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.New York, NY: Marcel Dekker, Inc.; 2002.2.2. BolliBolli GB et al. GB et al. DiabetologiaDiabetologia. . 1999;42:11511999;42:1151--1167.1167.
Normal Insulin Secretion: The Basal-Bolus Insulin Concept
Time of AdministrationTime of Administration

Physiologic Basal Insulin Secretion
• Characteristics of normal pancreatic basal insulin
– Endogenous secretion over 24 h
– Relatively constant insulin release without peaks
– Predictable secretion pattern in healthy individuals without diabetes
BolliBolli GB et al. GB et al. DiabetologiaDiabetologia. 1999;42:1151. 1999;42:1151--1167.1167.

Why NPH and LENTE Why NPH and LENTE
((SemilenteSemilente, , UltralenteUltralente) are not ) are not
idealideal
•• peak effectpeak effect
nocturnal nocturnal hypoglycaemiahypoglycaemia
•• relatively short durationrelatively short duration
fasting fasting hyperglycaemiahyperglycaemia
High variability in s.c. absorptionHigh variability in s.c. absorption
wide blood glucose fluctuations fromwide blood glucose fluctuations from
dayday--toto--dayday
Inappropriate PharmacokineticsInappropriate Pharmacokinetics

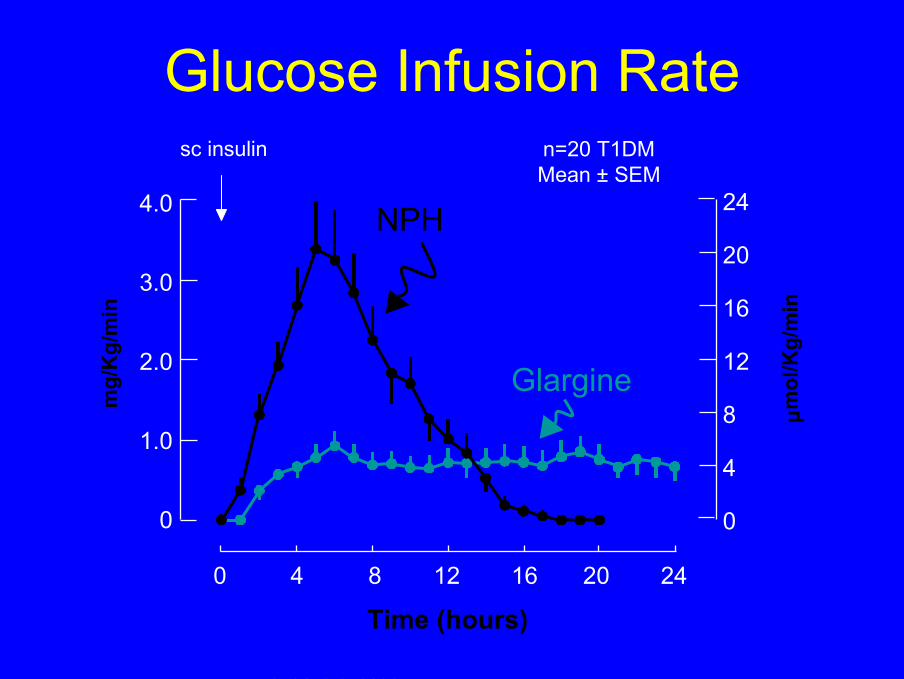
Glucose Infusion Raten=20 T1DMMean ± SEM
sc insulin
4.0
3.0
2.0
1.0
0
24
20
16
12
8
4
0
0 4 8 12 16 20 24
Time (hours)
mg/
Kg/
min
mol
/Kg/
min
µ
LeporeLepore M. et al., M. et al., Diabetes Diabetes 49: 2142-8, 2000
NPH
Glargine


Basal-Bolus Insulin Therapy: Insulin Glargine at HS and Mealtime Lispro or Aspart
BB DDLL HSHS
Insulin GlargineInsulin Glargine
Insulin Insulin LisproLispro or or AspartAspart
Time of AdministrationTime of AdministrationB, breakfast; L, lunch; D, dinner; HS, bedtime.B, breakfast; L, lunch; D, dinner; HS, bedtime.
Adapted from:Adapted from:1.1. Leahy JL. In: Leahy JL, Leahy JL. In: Leahy JL, CefaluCefalu WT, eds. WT, eds. Insulin Therapy. Insulin Therapy. New York, NY: Marcel Dekker, Inc.; 2002.New York, NY: Marcel Dekker, Inc.; 2002.2.2. BolliBolli GB et al. GB et al. DiabetologiaDiabetologia. . 1999;42:11511999;42:1151--1167.1167.
Type 1 DMType 1 DM

Design of study
RunRun--inin
00 12 months12 months
GlargineGlargine dinnertime (N=61)dinnertime (N=61)
NPH 4 times/day (N=60)NPH 4 times/day (N=60)
Both groups continued Both groups continued lisprolispro at mealsat mealsPorcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002

100
120
140
160
180
mm
ol/
l
5 .0
6 .0
7 .0
8 .0
9 .0
10 .0
mg
/dl
BR E AKF AS T LU N C H DINNER BE D T IM Ebefore afterbeforeafter before after 03:00 h
N P H
G la rg inebe f o re d inne r
Blood Glucose Monitoring
Porcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002

% HbA1c
5.5
6.0
6.5
7.0
7.5
0 2 4 6 8 10 12 months
GlargineNPH
%
**
* **
*
*p<0.05Porcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002

Frequency of hypoglycaemia(BG < 4.0 mmol/L, 72 mg/dl)
0
2
4
6
8
10
12
14
NPH glargine
dinnertime
Epis
odes
/pat
ien
t-m
onth
TOTAL EPISODES
*
*p<0.05
Porcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002

Frequency of hypoglycaemia(BG < 4.0 mmol/L, 72 mg/dl)
0
2
4
6
8
10
12
14
NPH glargine
dinnertime
Epis
odes
/pat
ien
t-m
onth Night-time (24:00-07:00 h)
*
*p<0.05
Porcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002
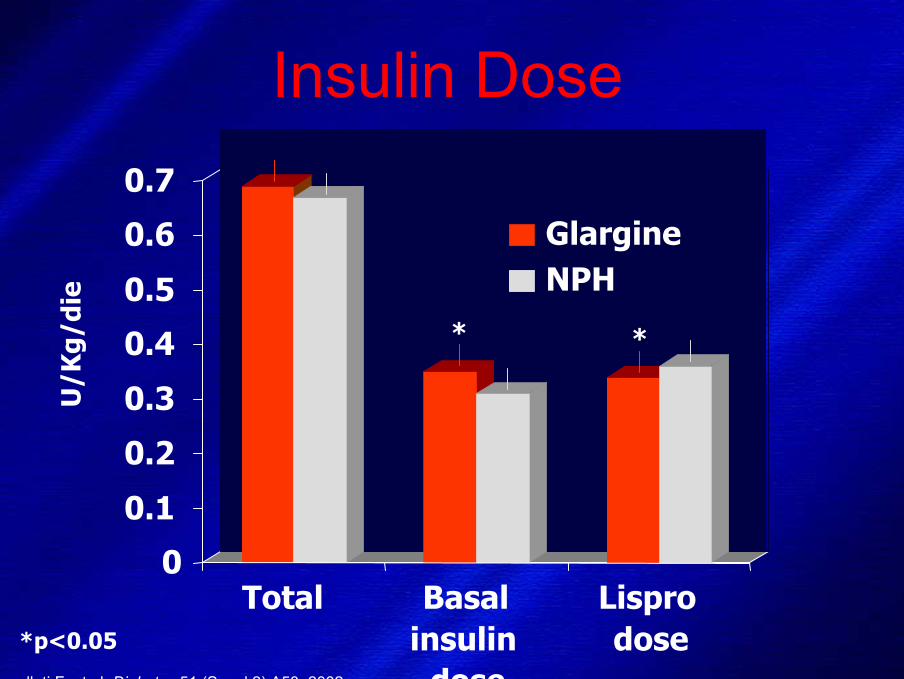
Insulin Dose
dose
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
Total Basalinsulin
Lisprodose
GlargineNPH
U/K
g/di
e
* *
*p<0.05
Porcellati F. et al. Diabetes 51 (Suppl.2):A53, 2002

INTRANASAL
• Nasal administration of certain proteins (e.g., oxytocin, desmopressin, and calcitonin) is now well established
• Permeability enhancers are generally required to augment insulinbioavailability; insulin bioavailability is typically in the range of 8-15% with enhancers
• Nasal irritation is common (e.g., with lecithin, bile salts, or laureth-9 as enhancers)
• Nasal tolerance and high rates of treatment failure are major limitations
• Recent clinical studies have shown more promising results (e.g., with gelified nasal insulin)
SISTEMI ALTERNATIVI PER LA SOMMINISTRAZIONE DI INSULINA
CefaluCefalu WT. WT. DiabetesDiabetes Care 27: 239Care 27: 239--46, 200446, 2004

INSULINA INTRANASALE
• Il trattamento intranasale non rappresenta un’alternativa realistica alla via sottocutanea per la bassa biodisponibilità e l’alto tasso di fallimento
(Pontiroli AE et Al. Br Med J 284:303-306, 1982)
• Alcuni studi più recenti effettuati in pazienti con diabete, sia tipo 1 sia tipo 2, hanno dato risultati incoraggianti sul controllo dell’iperglicemia postprandiale
(Coates PA et al. Diabet Med 12:235-239,1995)(Lalej-Bennis D et al Diabetes Metab 27:372 377,2001)(Lalej-Bennis D et al Diabet Med 18:614-618,2001)
L’intolleranza, l’ irritazione nasale e l’alto tasso di trattamenti falliti rimangono un ostacolo per il futuro di questa via alternativa
(Cefalu WT. Diabetes Care 27:239-246, 2004)

PULMONARY
• High permeability and large surface area provide a favorable anatomy for protein/drug uptake
• Very rapid absorption of insulin after inhalation mimicstime-activity profile of fast-acting insulin; appropriate forpremeal delivery
• Appears comparable to subcutaneous insulin on glycemicparameters for both type 1 and type 2 diabetic patients
• Several pulmonary insulin delivery systems are in development and in phase III testing
SISTEMI ALTERNATIVI PER LA SOMMINISTRAZIONE DI INSULINA
CefaluCefalu WT. WT. DiabetesDiabetes Care 27: 239Care 27: 239--46, 200446, 2004

INSULINA INALATORIA
RidottoRidotto spessorespessore delladellapareteparete alveoloalveolo capillarecapillare(2.2 microns) (2.2 microns)
Enorme superficie d’assorbimento ed elevata vascolarizzazionealveolare

L’ASSORBIMENTO è essenzialmente per via ematica.
La quantità di particelle che viene depositata dipende dalle loro dimensioni, ma anche dal loro peso e da altri fattori sconosciuti. La misura ideale è da 2 a 3 microns. Le particelle più grosse vengono fermate nell’orofaringe o nei bronchioli, quelle più fini vengono espirate (30%).
In totale circa il 70% dell’insulina raggiunge gli alveoli e viene assorbita.
VALUTAZIONI PRE-TRATTAMENTO
Test di funzionalità polmonare (SPIROMETRIA, DLCO)
Esclusione di: fumatori, pazienti affetti da BPCO, asma, altre patologiepolmonari
INSULINA INALATORIAINSULINA INALATORIA

EXUBERA (Nektar Therapeutics, Pfizer, Aventis)
• Questa metodica utilizza il principio dell’ aria compressa; l’insulina in polvere liberata da una capsula (1 mg equivale a 2-3 U di insulina rapida) si vaporizza nella camera di nebulizzazione e si mantiene in sospensione (nube di particelle di 3,8 micron).
• La nube di insulina può essere inalata nel momento in cui il paziente lo decide, nel corso di una inspirazione profonda
• Elevata concentrazione di insulina per puff
• Minore rischio di contaminazione• Dose media giornaliera circa 15
mg

EXUBERA: STUDI DI FASE III NEL EXUBERA: STUDI DI FASE III NEL DIABETE DI TIPO 1 E TIPO 2DIABETE DI TIPO 1 E TIPO 2
TipoTipo 11
Controllo glicemicoControllo glicemicoequiparabileequiparabile a un a un trattamentotrattamento insulinicoinsulinicoconvenzionale convenzionale
((QuattrinQuattrin T et Al. Diabetes T et Al. Diabetes Care 27: 2622Care 27: 2622--7, 2004)7, 2004)
TipoTipo 22
Effetto comparabileEffetto comparabile nelnel controllocontrollodelladella glicemiaglicemia postpost--prandiale prandiale e e nellanella riduzioneriduzione di di HbA1c HbA1c tratrainsulina inalatoriainsulina inalatoria e e sottocutanea sottocutanea
(Hollander PA et Al. Diabetes Care (Hollander PA et Al. Diabetes Care 27: 235627: 2356--62, 2004)62, 2004)
• Per molto tempo è prevalso il convincimento che fosse irrealistica qualunque via non invasiva per la somministrazione dell’insulina
• Oggi vi sono evidenze convincenti che la somministrazione dell’insulina attraverso vie alternative è possibile
• Al momento, la via inalatoria per la somministrazione polmonare è quella che ha fornito i migliori risultati ed appare ormai prossima all’ impiego clinico routinario
CONCLUSIONI

Somministrazione inalatoria mediante Exubera
Vantaggi• Efficacia paragonabile alla via s.c.• Maggiore accettabilità e soddisfazione dei
pazienti• Miglior controllo glicemico post-prandiale• Minori ipoglicemie
CONCLUSIONI

Somministrazione inalatoria mediante Exubera
Svantaggi• Effetti polmonari indesiderati a breve
come tosse e minore diffusibilità del CO• Aumento degli anticorpi anti-insulina
Incognite• Effetti polmonari a lungo termine
CONCLUSIONI

1922 – Child with type 1 diabetes before and after several months of insulin therapy
The miracle of insulin
Grazie per
l’attenzione !





























