Embed Size (px)
Citation preview

UPDATE on Evaluation and Management of
TIA and Stroke
Claire J. CreutzfeldtUW Harborview Stroke Center
January 2015

Outline
1. Some stroke facts2. Approach to evaluation and management of Stroke3. Acute management of• Ischemic stroke
TIA Stroke Thrombectomy
4. Chronic management Antithrombotic therapy
5. Hemorrhagic stroke6. Time for questions

Stroke facts
• ~700,00 strokes each year in the USo a stroke every 45 seconds
o 200,000 of those are recurrent strokes
• Kills >150,000 people/yr in US
• 28% of stroke victims < 65 years old
• 3rd most common cause of death, ranking behind diseases of the heart and cancer
• 4,500,000+ stroke survivors are alive in US
• leading cause of long-term disability in the US
4th
AHA Heart and Stroke Statistical Update 2014

Stroke classification
Normal Ischemic Intracerebral Subarachnoid stroke hemorrhage hemorrhage(80%) (15%) (5%)

“A stroke happens, when…
Mechanisms
Causes of initial event Prevention of recurrent stroke
Large vessel arteriosclerosis Carotid endarterectomy, Antiplatelet
Cardioembolism Anticoagulation Small vessel disease Antiplatelet agent Other Cryptogenic (Antiplatelet
agent)
…blood flow to a part of the brain is interrupted”

EvaluationBASIC STROKE EVALUATION• Thorough H&P• Non-con head CT• Imaging of extracranial arteries• EKG and telemetry• Routine blood studies• (TTE)
COMPREHENSIVE STROKE EVALUATION• MRI• Imaging of intra- and extracranial arteries• TEE• Prolonged cardiac monitoring• U-tox• Blood tests for hypercoagulable state• Genetic tests for rare causes such as CADASIL,
Fabry’s disease, MELAS…

Case 1
• 70 y/o m with h/o diabetes and hypertension presents to clinic and tells you about this episode yesterday where he couldn’t move his entire right side. Symptoms resolved within half an hour.
• BP 165/85, neurologically intact
What is your next step?

Case 1
A. Do a thorough neurological exam. If he really has no residual neurological deficits, no need for imaging
B. Optimize his blood pressure management and have him follow up in a month
C. Refer him to a TIA clinic (urgently), offer him admission to the hospital OR get an expedited workup yourself consisting of MRI brain, vascular imaging, EKG, Echocardiogram and blood work.
D. Educate him about the difference between TIA and stroke and have him follow up in a month
E. Add Clopidogrel to his daily baby Aspirin and have him follow up in a month

Risk of Stroke after TIA
1707 TIA patientsStroke event rates:•10.5% at 90 days• 5.3% at 2 days
JAMA 2000;284:2901-2906

ABCD2 score for TIA Risk Stratification
5 Factors Points
Age > 60 1
BP > 140/90 on first assessment after TIA
1
Clinical features unilateral weakness speech impairment without
weakness
21
Duration of TIA ≥60 minutes 10–59 minutes
21
Diabetes 1
Lancet 2007; 369: 283–92

ABCD2 score
Lancet 2007; 369: 283–92

Early TIA management
• Our system: offer admission to all• Others: TIA clinic• Treat:
– Risk factors– Antithrombotics– CEA
• Test:– Brain imaging (CT or MRI)– Vascular imaging – Cardiac evaluation (Echo, EKG)– blood work including basics + lipids, HbA1c, others

Case 2
70 y/o m with h/o diabetes and hypertension presents to the ER with sudden onset R-sided numbness and weakness.
• BP 165/85, awake and able to walk
What is your next step?

Case 2
A. Refer him to a TIA clinic (urgently), offer him admission to the hospital OR get an expedited workup yourself consisting of brain and vascular imaging, EKG, Echocardiogram and blood work.
B. Admit him to the stroke unit, add Clopidogrel to his daily baby Aspirin and order an MRI brain
C. Thorough H&P with time of onset and NIHSS followed by stat lab draw, EKG, head CT

Additional History I
• Symptoms started one hour ago • EKG: normal• NIHSS 11
What medication would you want to use acutely?

IV tPA for Acute Ischemic StrokeIndividual Patient Data Meta-analysis
Lancet 2004; 363: 768-74

tPA inclusion/exclusion criteria
IN: >18yrs, ischemic stroke w/in 3*hrs
EX: * symptoms minor or rapidly improving* seizure at stroke onset* stroke or head trauma w/in 3 months* major surgery w/in 2 weeks* h/o ICH* sustained BP >185/110 (aggressive tx
necessary)* GI or UT hemorrhage w/in 21 days* arterial puncture at noncompressible site w/in
7d* INR >1.7, platelets <100,000, glucose <50 or
>400
3-4.5 hrs * Age >80, NIHSS >25, large stroke,
][
Lancet 2004; 363: 768-74 NEJM 2008;359:1317-29.

What about mechanical thrombectomy?

Mechanical thrombectomy- a word of caution -
• FDA clearance was based on single-group, nonrandomized trials comparing device treatment with historical controls from PROACT II
• Effective recanalization but no better outcome
• These devices were not approved as clinically effective treatments for acute stroke but were cleared for use as devices to remove thrombus in acute stroke
• “Drip and ship” – method, wherein ‘smaller’ hospital starts intravenous tpa and ships the patient to a larger center for subsequent mechanical thrombectomy
Circulation. 2011;123:2591-2601

Mechanical thrombectomyback in 2013…
+2
N Engl J Med 2013;372:11-20

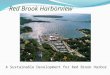
Mechanical thrombectomyfast forward to 2015…
N Engl J Med 2015;372:11-20

Modified Rankin Scale Scores at 90 Days in the Intention-to-Treat Population.
N Engl J Med 2015;372:11-20.
MR CLEAN

What happened?
• ‘Old’ trials were criticized for – Use of older devices
– Long interval between onset and intervention
– Low recruitment rates
– Did not require evidence of large vessel occlusion
• MR CLEAN: Thrombectomy devices in Holland were payed for exclusively in the context of the trial
• MR CLEAN: onset to iv tpa was much faster
• More results soon– ISC 2015:
more trials, more subgroup analyses, more discussion

Additional History II
• Patient woke up with symptoms, last seen normal > 15 hours ago
• EKG: normal• Symptoms: stable or progressing
• bbbb

Early supportive care
• Reverse ischemia (enhance perfusion)– Antithrombotic Medications – Blood Pressure– Interventions
• Limit injury (neuroprotection)– Glycemia (aggressively normalize)– Core body temperature
• Avoid infections
– Glutamate antagonists– Free radical scavengers
• High quality care– Joint Commission Stroke Centers
• Stroke units• Performance measures

Aspirin
RR = 1.0
Aspirin better Placebo better
0.8795% CI
0.81 to 0.94
Risk significantly reduced by 13%
Doses ranged from 30 to 1500 mg per day
Risk of stroke, MI, or vascular death
BMJ. 2002; 324: 71–86

Other Antiplatelet agents
Profess trial: NEJM 2008;359:1238-1251
SPS3 trial: NEJM 2012;367;817-825
SAMMPRIS trial: NEJM 2011;365:993-1003

A brief look at Anticoagulation
• Warfarin vs. Aspirin in Afib: SPAF studies • N Engl J Med 1990; 323:1505-1511
• Warfarin vs. Aspirin for Intracranial stenosis: WASID• N Engl J Med 2005; 352:1305-1316
• Warfarin vs Aspirin + Clopidogrel in Afib: ACTIVE W• Stroke. 2008;39:1482-1486
• Warfarin in Congestive Heart Failure: WARCEF• N Engl J Med 2012; 366:1859-1869
• The Newer Anticoagulants

Case 3
70 y/o m comes to your clinic as a hospital follow up after an ischemic stroke.
PMH: Diabetes, borderline hypertension, smoking
Exam today: BP 135/69, mild right-sided weakness and occasional word finding difficulties.He also seems withdrawn and depressed.
Medications: ASA 81, Niacin, HCTZ 25, Insulin sq
What is your next step?

Case 3
A. Change Niacin to a Statin
B. Change HCTZ to Chlorthalidone
C. Educate patient on life-style change, diet and smoking cessation
D. Consider an SSRI
E. All of the above

Case 4
A 65 y/o woman with known hypertension had complained to her husband about a severe headache shortly before she collapsed.
In the ER, she has decreased LOC, right-sided hemiparesis and aphasia.
Initial BP is 230/120

Case 4 - CT

Case 4
What is the most likely etiology of her hemorrhage?
A. Cerebral amyloid angiopathy
B. Hypertension
C. Ischemic stroke turned hemorrhagic

AmyloidAngiopathyICH
HypertensiveICH
Intraparenchymal hemorrhage

Goals of ICH therapy
• Prevent hematoma enlargement • Blood pressure treatment
• Hemostatic agents
• Surgery
• Limit injury (neuroprotection)– Reduce Raised ICP
– Glycemic control
– Temperature
• Prevent Complications– Swallow screening, DVT prophylaxis, Seizure
prophylaxis

Hematoma Expansion
• Prevent hematoma enlargement/Reduce ICP
- Blood pressure treatment (goals, agents)- Hemostatic agents- Surgery

Stroke complications
Semin Neurol. 2010

Thank you