Embed Size (px)
Citation preview

What is up-to-date today will be obsolete tomorrow

.
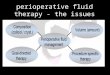
RESUSCITATION REPAIR MAINTENANCE PN
PERFUSION & OXYGENATION
CORRECTELECT & AB
HOMEOSTASIS/SUPPORTIVE
CORRECTNUTRITION ST
PARENTERAL FLUID THERAPY

RESUSCITATIONRESUSCITATION MAINTENANCEMAINTENANCE
NUTRITIONNUTRITIONCrystalloidCrystalloid
1. Replace acute loss (hemorrhage, GI loss, 3rd space etc)
1. Replace acute loss (hemorrhage, GI loss, 3rd space etc)
1. Replace normal loss (IWL + urine+ faecal)2. Nutrition support
1. Replace normal loss (IWL + urine+ faecal)2. Nutrition support
ELECTROLYTESELECTROLYTES
FLUID THERAPYFLUID THERAPY
Colloid
Na > 100 mEq/l(RA/RL/NS)
Na 30-60 mEq/LK 20 mEq/L
Repair
DextranHESGelatin
Amino acidsCarbohydratesFat
Intraoperative Hemodynamically stable
Preop & post recovery period

Preoperative
Intra-operative
Post-operative
Preop nutrition or Carbohydrate
Load 800 ml + 200 ml
Intraop isotonic crystalloid> 12-14 ml/kg/hr
Postop Maintenance fluid< 30 ml/kg/24 hr; Na+ 60-100 mEq
1. Nygren J. Best Practice & Research Clinical Anaesthesiology Vol. 20, No. 3, pp. 429e438, 20062. Fearon KCH. Enhanced recovery after surgery: A consensus review of clinical care for patients undergoing colonic resection
Clinical Nutrition (2005) 24, 466–4773. Futier E et al. Conservative vs Restrictive Individualized Goal-Directed Fluid Replacement Strategy in Major Abdominal
Surgery. Arch Surg. 2010;145(12):1193-12004. Lobo DN et al.Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection. Lancet
2002 May 25.359(5320):1792-35. Brandtsruo B. Fluid therapy for the surgical patient. Best Practice & Research Clinical Anaesthesiology Vol. 20, No. 2, pp.
265–283, 2006
(1,2) (3) (4,5)

Dr Iyan Darmawan
RESUSCITATIONRESUSCITATION MAINTENANCEMAINTENANCE
Resuscitation vs MaintenanceResuscitation vs Maintenance
Elect of High sodium > 100 mmol/L or colloid Low or no K+ 20-30 ml/kg/hr (DSS, diarrhea) 2-3 L/10-15 min (hemorrhagic shock)
• Moderate sodium 30-60 mmol/L• K+ based on daily req • 20 drops/min 500 ml/6 hr
ASERING, RL, NS, RD KAEN MG3
AMINOFLUID

Dr Iyan Darmawan
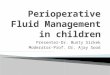
Fearon KCH, Ljungqvist O, Von Meyenteldt M; Revhavy A, Dejong CHC, Lassen K, Nygren J, Hausel J, Soop M, Andersen J, Kehlet ; Enhanced recovery after surgery: A consensus review of clinical care for patients undergoing colonic resection. Clinical Nutrition 2005; 24: 466-477 Pre-
admission conselling
Perioperative oral nutrition
Stimulation of gut mortility
ERAS
Main elements of the ERAS protocol
Fluid and CHO- loading/no fasting
Prevention of nausea and vomiting
Avoidance of sodium/ fluid overload

Dr Iyan DarmawanSummary of stress response
STRESS
HYPOTHALAMUS
SYMPATHETIC ADENOHYPOFISIS
ADRENAL MEDULLA ADRENAL CORTEX THYROID GLANDCardiac function↑Blood pressure ↑Blood redistribution ↑ Adrenaline
↑ Noradrenaline
↑ Cardiac function↑ Blood redistribution↑ Glycogenolysis↑ Blood glucose↑ Lipolysis↑ Free fatty acids
↑ Glucocorticoid ↑ T4
↑ Glucagon
↑ Metabolism
↑ Glycogenolysis↑ Blood glucose↑ Gluconeogenesis↑ Lipolysis
1. Na+ retention2. Water retention3. ↑ Free Amino Acids4. ↑ Gluconeogenesis
Purpose: Maintain homeostasis, increase body resistance, tissue healing etc

Dr Iyan Darmawan

Dr Iyan Darmawan
04/10/23
4 D 1-2 D
2-8 W months

Vasopressin changes by various solutions
NaCl vasopressin elevation
Glucose vasopressin suppression

Dr Iyan Darmawan
Sequestration of fluid from ECW
35
30
25
20
15
10
5
% BODYWEIGHT
NORMAL ACUTE INJURY ELECT & IV Col PHASE OF RESOLUTION
ICF
IV
I.V. fluids Diuresis
FormingSequestratedECF
SequestratedECF
ResolvingSequestratedECF
3rd space
Kokko & Tannen Fluids & Electrolytes. WB Saunders 3 ed.p738
ICF =intracellualr fluid; ISF =interstitial fluid; IV =intravascular
ISF

Dr Iyan Darmawan
Urine outputis not a reliable marker of
hydration status in postoperative Patients
Stress-induced ADH and Aldosterone cause water retention

Dr Iyan Darmawan
Fluid balance is ideally determined by weighing your patients pre and postoperatively?

Dr Iyan Darmawan
Low SodiumRestricted volume
Perioperative IV Fluid Restrictions Helpful in Colorectal resection
Perioperative IV Fluid Restrictions Helpful in Colorectal resection
Better outcome
1. Bandstrup. Ann Surg.2003;238:641-6482. Lobo DN. Lancet. 2002 May 25;359(9320):1812-8.

Dr Iyan Darmawan
Lobo DN, Bostock KA, Neal KR, Perkins AC, Rowland BJ, Allison S; Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection : a randomized controlled trial. Lancet 2002; 359; 1812-1818
Twenty patients for elective colonic resection were divided into 2 groups.
Standard group : at least 154 mmol sodium and 3 L water/day (generally 1 L 0.9% saline and 2 L 5% dextrose)
Restricted group: no more than 77 mmol sodium and 2 L water/day (generally 0.5 L 0.9% saline and 1.5 L 5% dextrose or 2 L 4% dextrose)

Dr Iyan Darmawan
Weight change and 24-hr total fluid input, intravenous sodium and urine output in patients undergoing elective colonic resection
0 1 2 3 4 pop 0 1 2 3 4 5 pop
0 1 2 3 4 pop 0 1 2 3 4 pop Lobo DN, et al: Lancet 2002; 359;1812-1818; Standard: at least 154 mmol sodium and 3 L water/day; Restricted: no more than 77 mmol sodium and 2 L water/day
Change inWeight (kg)
IV sodium(mmol)
Total fluid input (ml)
Urine output (ml)

Dr Iyan Darmawan
> 3 L; 154 mEq < 2 L; 77 mEq
Mean Gastric emptying time 175 72.5(minutes)Median passage of flatus 4 3(days)Median postop hospital stay 9 6(days)No of patient with complication 7 1

Dr Iyan Darmawan
Brandstrup B, Tonnsen H, Beier-Holgersen R, Hjortso E, Ording H, et al. Effects of Intravenous fluid restriction on postoperative complications : Comparison of two perioperative fluid regimens. A randomized assesor-blinded multicenter trial. Ann Surg 2003; 238:641-648
Intravenous fluids
Body weight increase
L kg
The restricted fluid regimen significantly reduced postoperative complications both by intention to treat (33% vs 51% P.0013) and per-protocol (30% vs 56% P0.003 ) analysis . The members of both cardiopulmonary (7% vs 24% P0.007) and tissue-healing complications 16% vs 31% P0.04) were significantly reduced.

Dr Iyan Darmawan
Results (restricted vs standard)Results (restricted vs standard)
• Overall postop complications 33% vs 51% (p = 0.013)
• Cardiopulmonary comp 7% vs 24% (p=0.007)
• Tissue-healing complications 16% vs 31% (p =0.04)
• Deaths 0% vs 4.7% (p=0.12)
Brandstrup B . Ann Surg.2003;238:641-648

Dr Iyan Darmawan
BUT...
• New evidence exists that Excessive fluid restriction increased the level of hypovolemia, leading to reduced ScvO2 and thereby increased incidence of postoperative complications.
Arch Surg. 2010;145(12):1193-1200

Dr Iyan Darmawan
Arkilic C, Taguchi A, Sharma N, Ratnaraj J, Sessler Dl, read TE, Fllshan JW, Kurg A; Supplemental perioperative fluid administration increase tissue oxygen pressure. Surgery 2003; 133: 49 -55
Fifty-six patients undergoing colon resection assigned into two groups
Aggressive : a bolus of 10 ml/kg before induction of anesthesia.16-18 ml/kg/hr fluid management
Conservative : 8 ml/kg/hr
Conclusion. Supplemental perioperative (intra- and post-) fluid administration significantly increase tissue perfusion and tissue oxygen pressure(subcutaneous oxygen tension)

Dr Iyan Darmawan
Holte K. Klarkov B, Christensen DS, Lund C, Nielsen KG, Bie P, Kehlet H: Liberal versus restrictive fluid administration to improve recovery after laparoscopic cholecystectomy: A randomized, double-blind study. Ann Surg 2004; 240: 829-829.
Methods 48 ASA I-III patients undergoing laparoscopic cholecystectomy Randomized to 15 ml/kg (restrictive group) or 40 ml/kg (liberal group) intraoperative lactated Ringer Solution
Results
Liberal group Improved postoperative pulmonary function Improved exercise capacity after surgery
Reduced stress response (aldostrenone, ADH and angiotensin II)
Nausea, general well-being, thirst, dizziness, drowsiness, fatigue, and balance function also significantly improved.
Liberal fluid administration improved recovery after surgery

Dr Iyan Darmawan
Maharaj CH, Kallam SR, Malik A, Hassett P, Grady D, Laffey G: Preoperative intravenous fluid therapy decrease postoperative nausea and pain in high risk patients. Anesth Analg 2005; 100: 675- 82.
Eighty ASA grade 1-III patients for diagnostic gynecologic laparoscopy
Large volume : (2 ml/kg/h fasting) Control : (3 ml/kg alone)
Overall incidence and interval frequency of postoperative nausea and vomiting
The preoperative administration of 2 ml/kg of compound sodium lactate solution for every hour of fasting is recommended to patients with an increased PONV risk presenting for ambulatory surgery

Dr Iyan Darmawan
The reasons why intravenous infusion therapy are controversial
Historical background and diverse indications for various patients of different pathophysiological situations.
Shires’ theory has been easily accepted in trauma patients with strong heart, the benefit of youth and a good renal system who tolerate liter and liter of fluid. While renal failures is avoided, the abdominal compartment syndrome has appeared and been the price for this aggressive fluid replacement.
Liberal fluid administration : Arkilic C et al (2003): Colon Resection, Maharaj CH et al: Gynecologic Laparoscopy(20005) Holte et al (2004): Laparoscopic Chotecystectomy Holte et al (2004): Knee Anthroplasty
Restrictive administration Labo DN et al (2002): Elective Colonic Resection Randstrup B et al (2003): Colorectal Resection Other reasons




Dr Iyan Darmawan
Hypoalbuminemia, ECF expansion and Picking the right infusion
Hypoalbuminemia, ECF expansion and Picking the right infusion
Hill G.L. Disorders of nutrition and metabolism in clinical surgery. Churchill Livingstone 1990
Should prescribe
Low sodium!!

Dr Iyan Darmawan
Minimum 400- 600 kcal is sufficient in early postop period (Protein-sparing effect)
1. Arieff Allen L. Fatal Postoperative Pulmonary Edema. Pathogenesis & Literature Review. CHEST 1999;115:1371-1377
2. Lobo DN et al.Effect of salt and water balance on recovery of gastrointestinal function after elective colonic resection. Lancet 2002 May 25.359(5320):1792-3
3. Hill G.L. Disorders of nutrition and metabolism in clinical surgery. Churchill Livingstone 19904. Fiona REID, Dileep N. LOBO, Robert N. WILLIAMS, Brian J. ROWLAND Sand Simon P. ALLISON
(Ab)normal saline and physiological Hartmann's solution: a randomized double-blind crossover study Clinical Science (2003) 104, (17–24)
Pulmonary oedema may ensue within 36 hr postoperatively if net water retention > 67 ml/kg/d
Recovery of GI function is faster in patients of colonic resection receiving postop fluid < 2 L; 77 mEq Na+ than group receiving > 3 L; 154 mEq Na+
Patients with hypoalbuminemia have expanded ECV, and administration of high sodium may aggravate delayed wound healing
Water and sodium excretion is slower in postop patients receiving infusion containing higher sodium
postop water input should be < 2000 ml
Post op Na+ intake 60-100 mEq/day


Dr Iyan Darmawan
1982: Hill Harris-Benedict > 90% patients will get excess of 500 kcal TEE 40 kcal/kg/day 30% overfeeding
1989 Saito TEE 25-30 kcal/kg/day
2005 Marik PE : 20 kcal/kg/day in septic patients
2006: Boitano M : 10-20 kcal/kg/day
1. Hill G.L. Disorders of nutrition and metabolism in clinical surgery. Churchill Livingstone 19902. Saito H. Perioperative Nutrition Support. Nutr & Met Support in Clinical Practice.1998 Pensa.3. Boitano M. Hypocaloric feeding of the critically ill. Nutrition in Clinical Practice 21:617-622.December 2006

Thanks for your kind attention