Embed Size (px)
DESCRIPTION
PJP infection
Citation preview

A
uCtcPc©
K
R
mlpiitrp©
M
0h
Disponible en ligne sur
ScienceDirectwww.sciencedirect.com
Médecine et maladies infectieuses 44 (2014) 185–198
General review
Update on pulmonary Pneumocystis jirovecii infection in non-HIV patients
L’infection pulmonaire à Pneumocystis jirovecii chez les patients VIH négatifs : mise au point
A. Roux a, F. Gonzalez b, M. Roux c, M. Mehrad d, J. Menotti e,f, J.-R. Zahar g,h, V.-X. Tadros b,E. Azoulay i,f, P.-Y. Brillet c,j, F. Vincent k,∗,
for the Groupe de recherche respiratoire en réanimation en onco-hématologie (Grrr-OH)a Service de pneumologie, hôpital Foch, 92151 Suresnes, France
b Service de réanimation médico-chirurgicale, hôpital Avicenne, Assistance publique–Hôpitaux de Paris (AP–HP), 93009 Bobigny, Francec Service de radiologie, hôpital Avicenne, Assistance publique–Hôpitaux de Paris (AP–HP), 93009 Bobigny, France
d Service des urgences, Gustave Roussy, Cancer Campus Grand Paris, 94805 Villejuif, Francee Service de parasitologie-mycologie, hôpital Saint-Louis, Assistance publique–Hôpitaux de Paris (AP–HP), 75010 Paris, France
f Université Paris-Diderot, Sorbonne Paris-Cité, 75010 Paris, Franceg UPLIN, CHU d’Angers, 49100 Angers, France
h Université d’Angers, 49100 Angers, Francei Service de réanimation médicale, hôpital Saint-Louis, Assistance publique–Hôpitaux de Paris (AP–HP), 75010 Paris, France
j Université Paris-13, 93009 Bobigny, Francek Service de réanimation polyvalente, CHI Le Raincy-Montfermeil, 10, rue du Général-Leclerc, 93370 Montfermeil, France
Received 14 July 2013; received in revised form 4 December 2013; accepted 15 January 2014Available online 11 March 2014
bstract
Pneumocystis jirovecii is the only fungus of its kind to be pathogenic in humans. It is primarily responsible for pneumonia (PJP). The key tonderstanding immune defences has focused on T-cells, mainly because of the HIV infection epidemic. Patients presenting with PJP all have aD4 count below 200/mm3. The introduction of systematic primary prophylaxis and the use of new anti-retroviral drugs have significantly reduced
he incidence of this disease in the HIV-infected population, mainly in developed countries. The increasingly frequent use of corticosteroids,hemotherapy, and other immunosuppressive drugs has led to an outbreak of PJP in patients not infected by HIV. These patients presenting withJP have more rapid and severe symptoms, sometimes atypical, leading to delay the initiation of a specific anti-infective therapy, sometimes aause of death. However, the contribution of new diagnostic tools and a better understanding of patients at risk should improve their survival.
2014 Elsevier Masson SAS. All rights reserved.
eywords: Pneumocystis jirovecii; Immunodepression; Pneumonia
ésumé
Pneumocystis jirovecii est le seul champignon de son espèce à être pathogène chez l’être humain. Il est essentiellement responsable de pneu-opathie (PJP). L’essentiel de la compréhension des défenses immunitaires s’est concentré sur les lymphocytes T, essentiellement du fait de
’épidémie d’infection par le VIH. Les patients développant une PJP ont tous un taux de CD4 inférieur à 200/mm3. L’instauration de prophylaxierimaire systématique et le recours aux nouveaux anti-rétroviraux ont considérablement diminué l’incidence de cette pathologie dans la population
nfectée par le VIH, essentiellement dans les pays développés. L’utilisation de plus en plus fréquente de corticoïdes, chimiothérapies et autresmmunosuppresseurs a conduit à une éclosion de PJP chez les patients non infectés par le VIH. Chez ceux-ci, la PJP se manifeste par une symp-d à la
omatologie plus rapide et grave, parfois atypique, conduisant au retar esponsable de décès. Il semble cependant que l’apport de nouveaux outilsuissent améliorer la survie.2014 Elsevier Masson SAS. Tous droits réservés.
ots clés : Pneumocystis jirovecii ; Immunodépression ; Pneumopathie
∗ Corresponding author.E-mail address: [email protected] (F. Vincent).
399-077X/$ – see front matter © 2014 Elsevier Masson SAS. All rights reserved.ttp://dx.doi.org/10.1016/j.medmal.2014.01.007
mise en route d’un traitement anti-infectieux spécifique pouvant être
diagnostiques et qu’une meilleure connaissance des patients à risque
1 adies infectieuses 44 (2014) 185–198
1
(1aedHspippSici(tedriepottrt
2
toPeaa
Table 1Main drugs associated with pneumonia (PJP).Principaux médicaments associés avec la survenue de pneumocystose pul-monaire.
Corticosteroids
Alkylating agentsCyclophosphamideTemozolomide
AntibioticsBleomycin
AnticalcineurinsCyclosporineTacrolimus
AntimetabolitesCytarabineFluorouracilMethotrexate
Purine analogsAzathioprineCladribineFludarabine
TNF α inhibitorsAdalimumabEtanerceptInfliximab
Monoclonal antibodiesAbataceptAlemtuzumabRituximab
MiscellaneousSirolimusTocilizumab
Adapted from Carmona and Limper [3].T
tfaba(
TPP
PHS
S
C
M
86 A. Roux et al. / Médecine et mal
. Introduction
Pneumocystis pneumonia is caused by Pneumocystis jiroveciiP. jirovecii) in humans. The fungus was identified in the early900s, but cases of PJP were first reported among prematurend malnourished children especially in Central Europe at thend of the Second World War and in the early 1950s. The inci-ence increased later with the emergence of HIV in the 1980s.owever, many other non-HIV-patients are at risk of PJP, and
ome observations suggest an increase of the incidence in theseatients (Fig. 1). The authors of a retrospective study performedn Sweden between 1991 and 2001, reported that in the lasteriod of the study, 75% of PJP cases occurred in non-HIV-atients; only 13% of these patients had received prophylaxis.everal factors may have caused the increased incidence of PJP
n these patients. Immunosuppressive drugs were used moreommonly, in higher doses, or in combinations that may havencreased the susceptibility of patients to P. jirovecii infectionTable 1). Improved diagnostic procedures may also have con-ributed to a better detection of PJP. Moreover, the physician’sxperience with similar cases in AIDS-patients may improve theiagnostic suspicion of PJP in non-HIV-patients [1]. Some newisks have regularly been reported, all related to the use of newmmunomodulatory or antineoplastic agents (Table 1) [2]. How-ver, the diagnosis of PJP remains challenging, despite recentrogress in diagnostic methods [3]. Moreover, the pathogenesisf P. jirovecii infection from latent to fulminant fatal pneumoni-is in immunocompromised hosts remains to be explained. Thus,he aim of this review was to better determine the new risks,equiring preventive measures, the contribution of new diagnos-ic tools, and to address so-called “pending questions”.
. Patients at risk
New groups of patients have been identified at risk, afterhe epidemic of PJP in AIDS-patients (Fig. 1). Several authorsf retrospective studies have described the epidemiology of
JP in non-HIV-patients (Table 2). Many hypotheses couldxplain the increased risk of PJP in these populations, suchs the use of intensive immunosuppressive treatments, newnticancer and immunomodulating agents, and progress incaht
able 2athologies associated with pneumonia (PJP) in five series of non-HIV-patients.athologies associées à la survenue de pneumocystose pulmonaire chez des patients
Sepkowitz et al. [5]n = 142 (%)
Yale et al. [4]n = 116 (%)
eriod of inclusion 1978–1989 1985–1991
ematological malignancies 67 (47.2) 35 (30.2)
olid malignancies andcorticosteroids
37 (26) 15 (12.9)
olid organ transplantrecipients
0 29 (25)
hronic inflammatorydiseases
0 26 (22.4)
iscellaneous 38 (26.8)a 11 (9.5)
a Twenty-five (17.6%) allogeneic bone marrow transplant recipients, 7 (4.9%) solid
NF: tumor necrosis factor alpha.
he diagnosis of infection. The most significant risk factorsor PJP in non-HIV-patients are the use of corticosteroidsnd defects in cell-mediated immunity. Corticosteroids haveeen administered in 90% and as the sole immunosuppress-nt in 17–28% of non-HIV-patients [4]. Lymphocytopeniaidiopathic or drug-induced), immunomodulatory agents, mono-lonal or polyclonal antibody therapies, calcineurin inhibitors
nd other immunosuppressive medications, solid cancers orematological malignancies (Table 3), solid organ transplan-ation (Table 4), anti-transplant rejection treatment, treatmentséronégatifs pour le VIH.
Zahar et al. [6]n = 39 (%)
Roblot et al.n = 130 (%)
Bollée et al. [7]n = 56 (%)
1989–1999 1995–1999 2001–200628 (71.8) 75 (57.7) 44 (78.6)7 (17.9) 18 (13.8) 9 (16.1)
0 9 (6.9) 0
0 27 (20.8) 0
4 (10.3) 1 (0.8) 3 (5.4)
malignancies without corticosteroids.

A. Roux et al. / Médecine et maladies infectieuses 44 (2014) 185–198 187
s at ri risq
fdss
2
r
TPIt
LAOSBA
A
TIPIl
O
KLHH
A
lrecipients. Multiple factors may contribute to higher risks inthese patients, including corticosteroid therapy, purine ana-logues, and other cytostatic agents (i.e. fludarabine, cytarabine,
Table 5
Fig. 1. Non-HIV patientPatients séronégatifs pour le VIH à
or some inflammatory conditions (particularly rheumatologiciseases) (Tables 5–7), primary immunodeficiencies (especiallyevere combined immunodeficiency and X-linked hyper-IgMyndrome), and severe malnutrition are additional risk factors.
.1. Hematological malignancies
The most frequent underlying hematological malignancieselated to a higher risk of PJP are lymphoproliferative diseases,
able 3neumonia (PJP) according to the type of malignancy.ncidence de pneumocystose pulmonaire chez les patients d’oncologie en fonc-ion du type de cancer.
Cases Number ofpatients
Incidence(%)
ymphomas 34 9907 0.34cute lymphoblastic leukemia 5 2929 0.17ther types of leukemia 16 5023 0.32olid malignancies and corticosteroids 30 26085 0.11rain malignancies and corticosteroids 21 3098 0.68llogeneic bone marrow transplantation 22 1348 1.63
dapted from Sepkowitz et al. [5].
able 4ncidence of pneumonia (PJP) among solid organ recipients in the absence of. jirovecii prophylaxis.ncidence de la pneumocystose pulmonaire chez des transplantés d’organe en’absence de prophylaxie.
rgan transplanted Incidence (%)
idney 0.6–14iver 3–11eart 2–41eart-lung/lung 6.5–43
dapted from Martin et al. [27].
ItIa
D
GPPSR
TRmFl
H
RC
T
AMt
sk for pneumonia (PJP).ue de pneumocystose pulmonaire.
ymphoid leukemia, and bone marrow or stem cell transplant
ncidence of pneumonia (PJP) among patients with autoimmune and inflamma-ory diseases.ncidence de la pneumocystose pulmonaire au cours de différentes pathologiesuto-immunes ou inflammatoires.
isease Incidence (%) References
ranulomatosis with polyangiitis 8–12 [1]eriarteritis nodosa 6.5 [1,4]olymyositis and dermatomyositis 2.7 [9]ystemic lupus erythematosus 2 [10]heumatoid arthritis 0.1–0.3 [1]
able 6isk factors of pneumonia (PJP) among patients with systemic lupus erythe-atosus.acteurs de risque de pneumocystose pulmonaire chez des patients souffrant de
upus érythémateux disséminé.
PJP+(n = 15)
PJP–(n = 60)
P
igher activityindex (MEX-SLEDAI)
13.6 ± 5.83 6.73 ± 3.22 < 0.01
enal involvement 86% 11.1% < 0.01umulative doseof prednisone(mean ± SD)
49 ± 29 mg/day 20 ± 4.8 mg/day < 0.001
otal lymphocytecount(mean ± SD)
520 ± 226/mm3 1420 ± 382/mm3 < 0.01
dapted from Lertnawapan et al. [11].EX-SLEDAI: Mexican Systemic Lupus Erythematosus; SD: standard devia-
ion.

188 A. Roux et al. / Médecine et maladies
Table 7Drugs associated with pneumonia (PJP) in rheumatoid arthritis patients.Traitements associés ave la survenue de pneumocystose pulmonaire chez lespatients traités pour polyarthrite rhumatoïde.
Drug Action PJP incidence (%)
Infliximab (Remicade®) Anti-TNF � 0.3Etanercept (Embrel®) Anti-TNF � 0.1Adalimumab (Humira®) Anti-TNF � 0.3Tocilizumab (RoActemra®) Anti IL6 0.2Abatacept (Orencia®) Anti CD 28 0.1
A
vasPH4rat
2
coCtioaagow
2
pommlac(ah((uoao
ao
2
pcsa
2
tmTsPa
2
irm
2
tcnl[i
2
abpg[
2
wscopctCThe authors stressed the pivotal role of corticosteroids. How-
dapted from Mori et al. [12].
incristine, cyclophosphamide, methotrexate, and monoclonalntibody therapy such as anti-CD52). These therapies induceevere and prolonged T-cell immunosuppression predisposing toJP. Corticosteroids play a major role in the occurrence of PJP.igh doses of corticosteroids (i.e. > 20 mg prednisone daily for
weeks) and steroid dose tapering have been identified as majorisk factors. However, the intensity of chemotherapy is probably
very important issue and should be taken into account whenhe diagnosis is suspected.
.2. Solid tumors
Primary or metastatic brain tumors, lung, and breast can-ers are associated with higher risk of PJP; whereas PJP rarelyccurs in patients with malignancies of the digestive organs [5].orticosteroid use and radiotherapy are considered as risk fac-
ors [5]. The incidence of PJP in patients with solid tumors hasncreased, probably because of better overall survival and usef more aggressive chemotherapy; but only a few authors havessessed this issue. However, the most important risks seems toffect some subgroups of patients, such as those with high-gradelioma receiving temozolomide (75 mg/m2) during 6 to 7 weeks,r a high-dose temozolomide regimen, especially associatedith a chronic use of corticosteroids.
.3. Solid organ transplantation
Five to 15 percent of patients who undergo solid organ trans-lantation present with PJP without any prophylaxis, dependingn organ type, transplant center, and immunosuppressive regi-ens (Table 4). Most cases of PJP occur in the first 6onths after transplantation but some infections are reported
ater. Moreover, individual risk increases during the period ofnti-rejection treatment. The risk factors for PJP are corti-osteroid treatment associated with immunosuppressive drugscyclosporine, tacrolimus, sirolimus, mycophenolate mofetil),nd anti-lymphocyte therapies. Mycophenylate mofetil mayave some intrinsic anti-P. Jirovecii activity, while tacrolimusFK506) boosts its growth in vitro. Active cytomegalovirusCMV) infection may boost the growth of Pneumocystis. It isnclear whether the CMV directly stimulates the proliferation
f Pneumocystis, acts systemically as an immunosuppressivegent, or is a fellow-traveler. Prediction of PJP risk in solidrgan transplant recipients is not assessed. Lymphocytopenia iseog
infectieuses 44 (2014) 185–198
ssociated with a higher risk of infection, but prophylaxis basedn CD4+ T-cell count (< 200 or 300/mm3) failed (Table 8).
.4. Autoimmune and inflammatory diseases
Patients with autoimmune or inflammatory diseases mayresent with PJP, usually in the setting of long-termorticosteroid therapy, combined or not with another immuno-uppressive therapy. It is unclear if PJP is more frequent in someutoimmune or inflammatory disease (Table 5).
.4.1. Rheumatoid arthritis (RA)The early use of methotrexate as a first-line treatment and
he emergence of innovative biologic agents targeted at specificolecules and pathways in the immune system, especially anti-NF-�, have altered the course of RA and improved patient andocial outcome [12]. But this has come with an increased rate ofJP in this population (Table 7). Outbreaks have been observedmong outpatients as in renal transplant recipients [12].
.4.2. Granulomatosis with polyangiitisThe authors of a systematic review focusing on infection
n patients with connective tissue diseases, published in 2007,eported that granulomatosis with polyangiitis was the diseaseost frequently associated with PJP (Table 5).
.4.3. Systemic lupus erythematosus (SLE)Gupta et al. reported that the frequency of PJP in SLE patients
reated with cyclophosphamide remained low (0.1588%) andoncluded that routine prophylaxis against P. jirovecii was notecessary, given the high incidence of severe drug reactions andupus flares with trimethoprim-sulfamethoxazole (TMP/SMX)13]. However, they and others identified risk factors suggestingnitiation of prophylaxis (Table 6) [11].
.4.4. Other connective tissue and autoimmune diseasesPJP has been described in all other connective tissue and
utoimmune diseases, although only a few case reports haveeen published on patients with dermatoses such as pemphigus,emphigoid, or Behcet’s syndrome (Table 5). Some reports sug-est that patients with dermatomyositis are at higher risk for PJP9].
.4.5. Inflammatory bowel diseases (IBD)Patients with Crohn’s disease and ulcerative colitis are treated
ith an increasing number of immunomodulatory and immuno-uppressive medications, including corticosteroids, thiopurines,yclosporine, and antibody-based biologic agents. The authorsf a large retrospective epidemiological study including 50,932atients with Crohn’s disease, 56,403 patients with ulcerativeolitis, and 1269 patients with unspecified IBD, reported thathe raw incidence of PJP was 10.6/100,000 [14]. Patients withrohn’s disease were identified as being at the highest risk.
ver, there are no clear guidelines concerning the managementf PJP in this population. A recent survey was performed amongastroenterology providers for PJP prophylaxis in patients with

adies infectieuses 44 (2014) 185–198 189
irip
3
mcdh
3
tstsmtca8ctpnPciw(lat(l(
3
lt
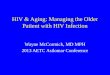
Fig. 2. HRCT scan of a 63-year-old male patient treated with long-term corti-costeroid therapy for a pemphigus, showing bilateral symmetrical ground-glassopacities (GGO) predominant in the upper lung.Scanner thoracique d’un homme de 63 ans traités par corticoïdes pour unpp
ddd
3
lnbppigimaae
TLL
NMMCC
A. Roux et al. / Médecine et mal
nflammatory bowel disease. Eight percent of the respondentseported that patients had developed PJP on immunosuppress-ve therapy, 11% reported initiating PJP prophylaxis, mostly foratients on triple immunosuppressive therapy.
. Clinical and radiological diagnosis
Non-HIV-patients exhibit more atypical presentations, aore fulminant course and higher mortality, and are more diffi-
ult to diagnose because of the lower inoculum. These clinicalifferences of PJP are thought to be caused by differences in theost immune response [15].
.1. Clinical presentation
Pneumonia is the primary manifestation of P.jirovecii infec-ion in non-HIV-patients. Extra-respiratory symptoms as well ashock remain very rare and should lead to consider co- infec-ion or another diagnosis [3,16]. The time from the onset ofymptom to diagnosis/treatment is a main risk factor for PJPortality. So the first, and not the least important reaction, is
o consider the diagnosis in case of association of: underlyingondition at risk of PJP; absence of any specific prophylaxis,nd common, but non-specific presentation, with fever (54 to6%), dyspnea (24 to 81%), and dry cough (8% to 76%). Thisommon presentation must lead to diagnostic investigations ando initiation of a prompt probabilistic specific treatment. Sevenercent of patients are asymptomatic, so if 1 or more of theseon-specific symptoms are absent, it does not allow ruling outJP [3]. For non-typical PJP presentations, clinician should firstonsider the wide spectrum of differential diagnosis in thosemmunosuppressed/multi treated patient. AIDS-patients presentith sub-acute onset (a few weeks) and longer symptom duration
25–28 days) than non-HIV-patients (a few days, 5–6 days), andess than 3 days in 20% of the cases [7]. But these PJP symptomsre missing in non-HIV-patients because of immunosuppressivereatment. Lungs examination ranges from normal auscultation20%, even in hypoxemic presentation) to bilateral diffuse crack-es [7]. A pneumothorax may present as acute respiratory failure2%–4%).
.2. Biological findings
No biological finding can suggest PJP. Neither the absoluteymphocyte count nor the subpopulation study are contribu-ive for the diagnosis of PJP (Table 8). Higher levels of lactate
mbGm
able 8ymphocytes count at the diagnosis of pneumonia (PJP) in 3 series of non-HIV-patieymphocytes totaux et sous populations au diagnostic de pneumocystose pulmonaire
Roblot et al. (2004)
umber of patients 25
edian CD4 cells (range) 280 (10–1000)
edian CD4/CD8 ratio NA
D4 < 300/mm3 80%
D4 < 400/mm3 80%
emphigus, montrant des opacités en verre dépoli bilatérales, symétriques,rédominant dans les territoires supérieurs.
ehydrogenase (LDH), as lung injury marker, correlate with theisease severity but this is not contributive for the etiologicaliagnosis.
.3. Radiological features
Radiographic imaging in non-HIV-patients is almost simi-ar to that of AIDS-patients. The chest radiographic images areon-specific and may even seem normal. They typically showilateral, symmetric, reticular or granular opacities. In mildresentations, these opacities are typically perihilar. In severeresentations, the opacities are diffuse, stemming from the hilan a butterfly pattern. Typically, reticular and poorly definedround-glass opacities (GGO) progress to alveolar consolidationn 3 to 4 days. High-resolution computed tomography (HRCT)
ay be indicated for non-HIV-patients patients with normal orlmost normal chest radiograph [17]. The sensitivity is 100%nd the specificity is 89%. Indeed, a normal HRCT may allowxcluding PJP [18] (Figs. 2 and 3). Extensive GGO are theain findings [17]. Several patterns of GGO distribution have
een described: central distribution with symmetric distributedGO and relative peripheral sparing (33 to 54% of patients),osaic pattern (57%), diffuse and nearly homogeneous
nts. dans 3 séries de patients séronégatifs pour le VIH.
Mansharamani et al. (2000) Overgaard et al. (2007)
22 1761 (0–546) 280 (42–900)0.6 1.591% 52%95% 40%

190 A. Roux et al. / Médecine et maladies
Fig. 3. HRCT scan of a 62-year-old male patient with arthropathic psoriasistreated with anti-TNF � therapy, revealing diffuse patchy GGO in the upperlung with relative peripheral sparing. In this case, PJP was associated withPseudomonas aeruginosa pneumonia.Scanner thoracique d’un homme de 62 ans traité pour un rhumatisme psoria-sique par anti-TNF � mettant en évidence des opacité en verre dépoli respectantla corticalité et prédominant dans les territoires supérieurs. Pneumocystosep
diewt6rsc6ipwwdeiuoaicotcfbgc(
cmGn
aao(edstbeiuicmirm(
4
4
apddasdnsp
4
onfivoGoMmscopic diagnosis performed by experienced microscopists issufficient to diagnose P. jirovecii in BAL fluids from AIDSpatients. However, the microscopic diagnosis has a weak
ulmonaire associée à une pneumonie à Pseudomonas aeruginosa.
istribution (24%). An apical predominance is also describedn 86% patients. In more advanced disease stages, some bilat-ral areas of consolidation may appear (17-21%). Septal linesith or without intralobular lines superimposed on GGO (pat-
ern commonly referred to as “crazy paving”) are observed in to 18% patients [19]. The presence of cavitations, intratho-acic adenopathy, and pleural effusion is uncommon and coulduggest another diagnosis [19]. Pulmonary cysts or pneumato-eles of varying shape, size, and wall thickness occur in 3 to% of non-HIV-patients with PJP. They are associated with anncreased frequency of spontaneous pneumothorax [19]. Com-ared to AIDS-patients, a more rapid spread and larger extentithout peripheral sparing of GGO is sometimes described,ith more common lung consolidations, reflecting pulmonaryamage from the host immune response. A second differ-nce is the lower incidence of pulmonary cysts (3 vs. 56%n non-HIV vs. AIDS-patients). Parenchymal bands, centrilob-lar nodules, and thickened interlobular septal lines are alsobserved more often in non-HIV-patients. HRCT images maylso differ according to the underlying condition and the level ofmmunodepression. Leukemic patients who undergo intensivehemotherapy or BMT sometimes present with centrilobularpacities or Y-shaped branching structures in association withypical GGO pattern, corresponding to bronchiolitis and bron-hioles that are impacted with inflammatory material. Nodularorms (solitary nodule or mass, or multiple nodules) haveeen described in non-HIV-patients, reflecting the presence ofranulomatous inflammation. The usual diagnostic techniquesan all be negative for P. jirovecii in these nodular patternsFig. 4).
The authors of several retrospective studies suggest that PJPan be discriminated from other infections in immunocompro-
ised patients. The initial diagnosis of PJP based on bilateralGO on HRCT is accurate in most pulmonary infections amongon-HIV-patients (87,5%) [20]. Extensive symmetric bilateralspt
infectieuses 44 (2014) 185–198
reas of GGO are not seen in other types of pneumonia except inssociation with areas of consolidation and nodules [20]. Areasf consolidation are less frequently observed in patients with PJP9%) than in patients with other types of pneumonia (75 to 85%),xcluding viral pneumonia [7]. PJP is also sometimes difficult toifferentiate, on imaging, from other pulmonary comorbiditiesuch as pulmonary edema, specific hematologic causes, drugoxicity, or transfusion related acute lung injury. Differencesetween CT findings of pulmonary edema and PJP include:nlargement of pulmonary vessels, pleural effusion and rapidmprovement after treatment. The radiographic improvementsually lags behind clinical improvement, and early radiolog-cal follow-up must be kept for patients with clear evidence oflinical worsening or a suspected complication such as pneu-othorax. GGO resolved completely after initiation of treatment
n 97% of patients after a median period of 13 days (mean 26,ange 1–58) [19]. Occasionally, patients recovering from PJPay present with mild or severe residual interstitial fibrosis
Fig. 5).
. Microbiological diagnosis
.1. Samples
The diagnosis of PJP is preferentially performed on broncho-lveolar lavage (BAL) fluid or induced sputum; the latter isroposed in some hospitals as the initial diagnostic proce-ure so as to decrease the need for bronchoscopy. A higheretection sensitivity allows using less invasive procedure suchs swabbing or aspiration. The development of highly sen-itive detection techniques such as real-time PCR or antigenetection assays offers the opportunity to assess the diag-ostic contribution of these techniques with less invasiveamples from the upper respiratory tract or blood sam-les.
.2. Usual techniques
The usual diagnostic techniques rely on the microscopicbservation of P. jirovecii cysts (which actually should beamed asci and correspond to the sexual forms of theungus) and/or trophic forms. Both forms can be visual-zed after May-Grünwald Giemsa staining or its RAL 555ariant (RAL Diagnostics®, Martillac, France), but severalther staining techniques have been proposed, such as therocott or toluidine blue staining. The use of an immunoflu-rescence assay with anti-Pneumocystis antibodies (Biorad®,arnes-la-Coquette, France) can improve the sensitivity oficroscopic detection of cysts. The sensitivity of micro-
ensitivity for the diagnosis of PJP in non-HIV immunocom-romised patients, requiring the use of molecular diagnosticechniques.

A. Roux et al. / Médecine et maladies infectieuses 44 (2014) 185–198 191
Fig. 4. 53-year-old male patient with chemotherapy for an angioimmunoblastic T-cell lymphoma: a: acute PJP the day of the onset of symptoms: discrete GGO isseen bilaterally in the upper lobes, with pre-existent lesions of pulmonary emphysema; b: 2 days later in the course of the disease, still without any specific treatment,GGO have increased. After initiating therapy, GGO progressively resolved; c: three months later, no GGO can be observed; a few small irregular linear opacitieswith discrete structural distortion persisted.Patient de 53 ans traité par chimiothérapie pour un lymphome T angio-immunoblastique : a : scanner thoracique réalisé le jour du début des symptômes dep d’emd nt, cet istors
4
4
ingtiluttcPsdo
4
at
•
•
epand radiological presentation (Table 10).
Table 9Diagnostic performance of Polymerase Chain Reaction (PCR) according to therespiratory sample in HIV negative patients.Valeur diagnostique de la PCR chez les patients séronégatifs pour le VIH enfonction du type de prélèvement respiratoire.
Inducedsputum (%)
Broncho-alveolarlavage fluid (%)
Sensibility 100 84Specificity 90 93
neumocystose pulmonaire : discret verre dépoli bilatéral des sommets ; lésionsépoli se sont majorées et sont devenues plus denses. Après le début du traitemeotalement disparu. Il ne persistait plus que quelques opacités réticulées avec d
.3. New diagnostic tools
.3.1. Polymerase Chain ReactionPolymerase Chain Reaction (PCR) can improve the sensitiv-
ty of detection, particularly in non-HIV-patients. Given its highegative predictive value, close to 100%, some authors have sug-ested that a negative PCR allows discontinuing cotrimoxazoleherapy [21]. Several targets have been used for PCR, includ-ng the major surface glycoprotein gene and the mitochondrialarge subunit ribosomal RNA gene. The development of molec-lar techniques for the diagnosis of PJP has allowed provinghe presence of P. jirovecii DNA in BAL fluids or induced spu-um from patients with no sign of pneumonia, leading to theoncept of P. jirovecii carriage or colonization. ConventionalCR cannot differentiate PJP from P. jirovecii colonization,o real-time quantitative PCR assays have been proposed toiscriminate between these two entities, using threshold valuesf fungal load.
.3.2. Limits of PCRThe differentiation between infection and colonization
ccording to a threshold remains the main difficulty for quanti-ative PCR interpretation for two obvious reason:
as most reports concern non commercial PCR kits, the extrap-olation of a threshold from one technique to another isdifficult;
PN
A
physème ; b : 2 jours plus tard, en l’absence de traitement, les opacités en verrelles-ci ont régressé ; c : trois mois plus tard les opacités en verre dépoli avaientions bronchiques.
qPCR diagnostic performance is supposed to be higherthan the current gold standard (standard coloration andimmunofluorescence), so defining a PJP case with eithergold standard negative subsequently confirmed PJP occur-ring early in the follow-up or expert analysis [22](Table 9).
Since the diagnostic performance depends on the dis-ase prevalence, it would be necessary to quantify pre-testrobability of PJP according to underlying diseases, clinical,
ositive predictive value 87 53.1egative predictive value 100 98.3
dapted from Takahashi [23].

192 A. Roux et al. / Médecine et maladies infectieuses 44 (2014) 185–198
Table 10Clinical and radiological prediction of pneumonia (PJP) in non-HIV-patients.Probabilité clinique et radiologique de pneumocystose pulmonaire chez les patients séronégatifs pour le VIH.
Typical Possible Unlikely
Context Absence of prophylaxis and knownrisk factors as lymphoidhemopathies, use ofimmunosuppressive therapies(Table 1), solid tumors withcorticosteroids, especially brain
Prophylaxis with lomidine and knownrisk factorsNeutropenia associated withcorticosteroids especially in solid organcancers
Compliance with prophylaxisMyeloid hemopathiesNeutropenia without corticosteroids
Onset of symptoms Abrupt in a few days One week More than one week
Clinical presentation Hacking coughAbsence of expectorationMild feverAcute respiratory failureProfound hypoxemia(PaO2 < 60 mmHg while breathingambient room air)Absence of extra-respiratorysymptom
Loose coughPurulent expectorationsAssociated septic shock
Loose coughPurulent expectorationsHemoptysisAbsence of feverProgressive respiratory failureAbsence of hypoxemiaPresence of extra-respiratory symptom
Lung auscultation NormalDiffuse crackles
Focal abnormalityPleural fremitus
Chest X-ray and HRCTfindings
NormalBilateral interstitial opacitiesExtensive ground-glass opacities(GGO)central, bilateral and symmetricdistribution, with relative peripheralsparingmosaic patterndiffuse and nearly homogeneousdistributionapical predominance
Unilateral interstitial opacitiesNodular opacityCrazy paving (septal lines ± intralobularlines superimposed on GGO)Pulmonary cystsinitially developed in areas ofconsolidationmultiseptate unusual-appearingthick-walled cystsincreased risk of pneumothoraxParenchymal bandsCentrilobular nodulesNodular pattern: solitary nodule or mass,or multiple nodules
CavitationPleural effusionMediastinal or hilar adenomegalyNormal HRCT
Biology Normal LDH level
HRCT: high-resolution computerized tomography; LDH: lactic dehydrogenase.
4
awwpvwP(db3obi(i(g
pnprat[
•
••
•
.3.3. Serum β-D-glucanSerum �-D-glucan (BDG) detection has also been proposed
s a diagnostic tool for PJP since this component of fungal cellall has been observed in high levels in the serum of patientsith PJP [24]. Serum BDG detection test has a good negativeredictive value. However, as many factors can induce BDG ele-ation (Table 9), a specific diagnosis of PJP cannot be achievedith this pan-fungal marker. The diagnostic performance forJP seems to be better than for invasive fungal infections (IFI)i.e. candidemia and aspergillosis). A meta-analysis of BDGetection performance for PJP diagnostic studies was conductedy Karageorgopoulos et al. [25]. Fourteen studies including57 patients with PJP and 1723 controls were included. Mostf the authors used the Fungitel® test with a threshold setetween 80 and 100 �g/mL. The average (95% confidencenterval) sensitivity and specificity of BDG were 94.8%90.8–97.1) and 86.3% (81.7–89.9) respectively, and the pos-
tive and negative likelihood ratios were 6.9 (5.1–9.3) and 0.060.03–0.11), respectively. The very high sensitivity of BDG sug-ests that a negative result in patients without a high pretestui
robability of PJP should lead to considering an alternative diag-osis. Karageorgopoulos et al. concluded that it was necessary toretest for PJP to improve the diagnostic performance. Sax et al.eported a high PJP prevalence (65%) in their study, but the neg-tive predictive value was only 80% [26]. So we do agree withhem about the imperative need for pretest prevalence evaluation26]. This study had many limitations:
among the 14 mixed studies, some were retrospective andother were prospective, and their purpose was diagnostic per-formance for either IFI (including PJP) or only PJP;
different techniques with different thresholds were tested; since the method for control case differed, the frequency of
PJP in the various populations were very different; the case definition of PJP (excluding or including only positive
P. jirovecii PCR) differed among the various studies.
Those limitations stress that the study methods for the eval-ation of serum BDG for the diagnosis of PJP are clearlynsufficient and that there is an urgent need for accurate

A. Roux et al. / Médecine et maladies infectieuses 44 (2014) 185–198 193
Table 11Main indications for prophylaxis against pneumonia (PJP) in non-VIH/AIDS patients.Principales indications de prophylaxie de la pneumocystose chez les patients séronégatifs pour le VIH.
Solid tumorsPrednisone, or equivalent, of at least 20 mg/day fore more than 4 weeksTemozolomide and radiation therapy until CD4 > 200 mm3
Hematological malignanciesAlemtuzumab: during treatment and for at least 2 months after cessation until CD4 > 200 mm3
Fludarabine and T-cell depleting agents (e.g., cladribine) until CD4 > 200 mm3
All ALL patients while receiving anti leukemic therapyAllogeneic stem cells recipients for at least 6 monthsAutologous stem peripheral stem cells recipients for 3-6 monthsAllogeneic bone marrow recipients receiving immunosuppressive therapy or with chronic GVHD for > 6 months or the duration of immunosuppression
Solid organ transplant recipientsAll for 6–12 monthsRenal transplant recipients for a minimum of 4 months after transplantation; consider longer duration for other organs recipientsKeep in mind to reinstitute, for a length of at least 6 weeks, in case of transplant rejection treatment
Vasculitis and inflammatory diseasesGranulomatosis with polyangiitis (i.e. Wegener) treated with cyclophosphamide, especially if receiving corticosteroidsPrimary systemic vasculitis treated with corticosteroids and steroid-sparing agent (e.g., methotrexate)ANCA-associated vasculitis treated with cyclophosphamide and corticosteroidsRheumatoid arthritis treated with TNF-� inhibitors, especially if on corticosteroids or other immunosuppressionConnective tissue diseases treated with prednisolone > 20 mg per day, or equivalent, for more than 2 weeks
Inflammatory bowel diseasesPatients receiving TNF-� inhibitors, especially if on corticosteroids or other immunosuppression
Primary immunodeficienciesSevere combined immunodeficiencyIdiopathic T CD4+ -lymphocytopeniaX-linked hyper-IgM syndrome
A nd ToA ia; G
epPnb
F4GpSce
5
dapted from Carmona and Limper [3], Martin and Fishman [27] and, Tasaka aNCA: anti-neutrophil cytoplasmic antibodies; ALL: acute lymphocytic leukem
valuation. No correlation was found between clinical feature,rognosis, P. jirovecii load in the lungs detected by Real-TimeCR, and serum BDG levels. It should be stressed that all these
ew diagnostic tools should be included in the pre-test proba-ility of PJP (Table 10).ig. 5. HRCT scan of a 54-year-old male patient, under chemotherapy for a stage pulmonary adenocarcinoma, showing bilateral diffuse infiltrates, includingGO and patchy consolidations with inhomogeneous distribution and sparederipheral lung parenchyma.canner thoracique d’un homme de 54 ans traité par chimiothérapie pour adéno-arcinome bronchique stade 4. Infiltrats pulmonaires diffus associant opacitésn verre dépoli et consolidations inhomogènes épargnant la corticalité.
p
5
ap
5
pfa(liCsrapsto
kuda [28].VHD: graft versus host disease; TNF-�: tumor necrosis factor �.
. Prophylaxis and treatment
Most of the data was drawn from experience with AIDS-atients.
.1. Primary prophylaxis
There is no consensus on the strategy of disease preventiongainst P. jirovecii in non-HIV-patients, contrary to AIDS-atients, (Table 11).
.1.1. For which patients?The incidence of PJP could be increasing in non-HIV-
atients, but little data is available to determine the indicationsor primary prophylaxis, except in patients having undergonellogeneic bone marrow transplantation, organ transplantationespecially kidney), or in children with acute lymphoblasticeukemia. It should be kept in mind that in such patients, theres no reliable marker for susceptibility (low peripheral bloodD4+ cell count, Table 8). Thus, the benefit of prophylaxis
hould be balanced with the risk of severe adverse events andelies on the cumulative incidence of PJP. A systematic reviewnd meta-analysis of available randomized controlled trials was
ublished in 2007 [29]. The authors suggested that prophylaxishould be initiated when the risk of PJP is higher than 3.5%. Onhe other hand, the results of a cost-benefit analysis, performedn patients presenting with granulomatosis with polyangiitis,
1 adies
scoip
5
wspmtttpSeLra[
5
psecilhcnodtcwTiw(toSap(dmwd[lti
recatiaB1bShtsp
5
lwtn
5
5
STSdffe[rr1mrafcoawuoIdni
94 A. Roux et al. / Médecine et mal
howed increased life expectancy and reduced lifetime medicalosts for patients receiving TMP-SMX prophylaxis [8]. The rec-mmendations for solid organ transplant recipients were updatedn 2013 [27]. These guidelines are often updated since newatients at risk are regularly reported.
.1.2. DurationThis question remains unsolved, especially for patients
ith autoimmune or inflammatory diseases. Some recent datauggests that treatment duration can vary according to the trans-lanted organ; from 1month in kidney recipients to 1 year orore in lung recipients [30]. Although studied for long years,
here are still discrepancies in the recommendations for kidneyransplant recipients, although the have been studied for a longime [31]. The European Renal Association recommends a pro-hylaxis period of 4 months after transplantation, the Americanociety of Transplantation 6 to 12 months, and the Kidney Dis-ase Improving Global Outcomes guidelines 3 to 6 months [31].ifelong prophylaxis with TMP-SMX is not recommended for
enal transplant recipients; however, in many cases, PJP occurredfter the recommended post-transplantation prophylaxis periods32].
.1.3. Which agent?TMP-SMX should be considered as the first line for PJP pro-
hylaxis in non-HIV-patients [33]. All other prophylactic agentshould be considered as second-line agents due to breadth of cov-rage, drug intolerance, cost, and effectiveness issues that cannotompare with TMP-SMX. Its effectiveness and good tolerancen the prevention of PJP for patients presenting with hemato-ogical malignancies was demonstrated 30 years ago. It alsoas the potential advantage being active against other infectiousomplications (such as common bacterial infections, listeriosis,ocardiosis, and toxoplasmosis). The authors of a meta-analysisf 12 randomized trials, including 1245 patients (50% chil-ren) having undergone autologous bone marrow or solid organransplantation, or who presented with hematological malignan-ies, reported no difference between once-daily and three timeseekly administration schedules and suggested effectiveness ofMP-SMX as prophylaxis for PJP [29]. However, in daily clin-
cal practice, TMP-SMX administration, especially for patientsith rheumatic diseases, can sometimes lead to adverse effects
drug allergy, renal dysfunction, thrombocytopenia, and elec-rolyte disorders). However, it should be noted that in a reviewf methotrexate drug interactions, none was reported with TMP-MX used as a prophylactic agent against PJP. Dapsone isn alternative for preventive treatment. It is contraindicated inatients with documented glucose-6-phosphate dehydrogenaseG6PD) deficiencies. Like TMP-SMX, it inhibits the enzymeihydropteroate synthase (DHPS). Some authors argue that theutation of DHFS may be a leading cause of prophylaxis failurehen using these drugs. However no sufficient data has beenocumented in large clinical trials to support this hypothesis
34]. Dapsone, alone or associated with pyrimethamine, seemsess effective than association TMP-SMX, but this is still ques-ionable. It must be kept in mind that TMP-SMX intolerances often predictive of dapsone intolerance. So dapsone is notobwd
infectieuses 44 (2014) 185–198
ecommended as an alternative drug in case of TMP-SMX intol-rance. Atovaquone has been studied in small prospective trialsoncerning stem cell and solid organ transplant recipients. Itppears to be effective and well tolerated, even in bone marrowransplantation receivers. It was initially thought to be a promis-ng alternative for PJP, despite the unknown optimal dosagend its extremely variable absorption (enhanced by fatty food).reakthrough infections were documented in patients taking000 mg or less daily [35]. Finally, inhaled pentamidine shoulde considered as a third-line agent. It is less effective than TMP-MX, dapsone, or atovaquone. The use of inhaled pentamidineas been associated with breakthrough infections, especially inhe upper lung. Inhaled pentamidine may negatively affect theensitivity of diagnostic assays using respiratory secretions inatients with PJP.
.2. Secondary prophylaxis
The data in this field is even smaller than for primary prophy-axis. Some authors recently suggested that patients presentingith PJP during rituximab therapy should benefit from such
reatment until immune reconstitution was ensured. However,o definitive recommendations were issued.
.3. Curative treatment
.3.1. Anti-infectious agentsHistorically, the mainstay of treatment for PJP was TMP-
MX given orally or intravenously for 3 weeks (Table 12).MP-SMX acts by interfering on folate metabolism: TMP andMX respectively inhibit dihydrofolate reductase (DHFR) andihydropteroate synthase (DHPS), which are 2 integral enzymesor folate synthesis. It is still the recommended first-line therapyor patients with mild, moderate, and severe disease. Adverseffects occur less commonly (around 15%) in non-HIV-patients36]. Combination with other antimicrobial molecules is notecommended to treat PJP due to the lack of synergy and theisk of adverse effects. The recommended daily dose is TMP5–20 mg/kg plus SMX 75–100 mg/kg. But this dose recom-endation was not based on a randomized controlled trial
esults, so the optimal dose of TMP-SMX remains unclear. Someuthors recommend that SMX drug levels should be monitoredor patients receiving IV therapy, although published data isontroversial and there are no current guidelines as to whenr how often the levels should be monitored [3]. Patients with
seriously compromised pulmonary status (PaO2 < 60 mmHghile breathing ambient room air) or pending respiratory fail-re (PaCO2 normal or elevated in a patient with low PaO2r high respiratory rate) should probably receive IV therapy.n other cases, oral administration seems effective, in accor-ance with findings in AIDS-patients. It is very important toote that the recommended duration of treatment is 21 daysn AIDS-patients and 14 days in non-HIV-patients. The rec-
mmendation for longer treatment in HIV-infected patients isased on the higher fungal load and slower clinical response,hich may result in a higher risk of relapse after only 14ays of treatment. Extended treatment should be considered for
A. Roux et al. / Médecine et maladies infectieuses 44 (2014) 185–198 195
Table 12Therapeutic options for treating pneumonia (PJP).Anti-infectieux utilisés dans le traitement de la pneumocystose pulmonaire.
Agents Dosing Comments
Trimethoprim-sulfamethoxazole(TMP-SMX)
15–20 mg/kg/day in divided doses every 6–8 hours Drug of choice considered to be the most effective
Pentamidine isethionate 4 mg/kg/day IV over 1–2 hours Many adverse effects including pancreatitis (consider avoiding incase of pancreas transplantation), hypo- or hyperglycemia, bonemarrow suppression, renal failure, electrolyte disordersRarely used as aerosol (600 mg/kg/day) with risk of failure.
Atovaquone 750 mg/12 hours per os Reserved for mild or moderate PJP (PaO2 on ambient roomair > 70 mmHg)Optimal dose uncertain (up to 1500 mg/12 hours)Variable oral absorption (best with fatty foods)
Dapsone 50 mg/day per os Not to be used in case of G6PD deficiencyProposed in case of sulfamide allergy despite the fact that dapsonemay elicit sulfamide allergy
Caspofungin 70 mg IV loading dose on day one followed by50 mg/day
Case reports as salvage therapy
A
nftPmtarteacttaaashaamcdfotHr
5
edBt
agwdciPd[tr
6
w18vd7tPhdrihocIn
dapted from Martin and Fishman [38].
on-HIV-patients, in case of severe immunosuppression, highungal load, or delayed clinical improvement. No randomizedrial has validated risk factors for TMP-SMX treatment failure.atients usually worsen within the first 3 to 5 days of treat-ent without corticosteroid treatment. Therefore changes in the
reatment should not be made before 5 to 8 days of treatment;nd concurrent infectious or non-infectious processes should beuled out. Patients who fail to improve after 5 to 7 days of oralherapy should be switched to an IV regimen and those whoxperience treatment failure on IV therapy should receive anlternative IV regimen. Other drugs may be administrated inase of intolerance to TMP-SMX, despite the fact that data onheir use comes from studies performed on AIDS-patients. Pen-amidine can be administrated intravenously. The most commondverse drug reaction to pentamidine is renal toxicity, which usu-lly occurs after 2 weeks of treatment and can be prevented bydequate hydration. Other adverse effects, including hypoten-ion (especially in case of rapid infusion), heart arrhythmia,ypo or hyperglycemia, hypercalcemia, hyperkalemia, pancre-titis, and metallic taste may also occur. Atovaquone, dapsone,nd clindamycin-primaquine are the other options for the treat-ent of PJP in AIDS-patients. A combination of primaquine and
lindamycin seems to be the most effective regimen. However,ue to the lack of data, these drugs cannot be recommendedor routine use in non-HIV-patients with PJP. Caspofungin actsn the P. jirovecii cell wall by inhibiting BDG synthesis: It hashus been reported to be effective, especially in salvage therapy.owever the recently reviewed data mainly comes from case
eports and remains highly controversial [37].
.3.2. Adjuvant corticosteroidsThe usefulness of adjunctive corticosteroid therapy is well
stablished for AIDS-patients with moderate-to-severe PJP,efined as PaO2 < 70 mmHg while breathing ambient room air.ut it remains questionable for non-HIV-patients with moderate-
o-severe PJP. Very few authors have addressed this question,
siAp
nd all their studies were retrospective, including very hetero-eneous populations of non-HIV-patients, most of them treatedith corticosteroids at the onset of PJP, with very heterogeneousosage of corticosteroids, the whole leading to contradictoryonclusions. The authors of a recent study, although performedn a single center and retrospectively, included 139 cases ofJP in non-HIV-patients; they suggested that an adjunctive highose corticosteroids (> 1 mg/kg/day) increased the death rate39]. This was unrelated to a higher rate of nosocomial infec-ions. Thus, we believe that there is currently not enough data toecommend adding such a treatment for these patients.
. Prognosis of PJP in non-HIV-patients
The prognosis of PJP is worse in these patients than in patientsith AIDS. The reported death rate ranges from 30 to 40% (vs.0% to 20% in AIDS-infected patients). It may reach 80.9% and6.8%, respectively, for patients requiring invasive mechanicalentilation and for those with an acute respiratory distress syn-rome (ARDS). Initiating an anti-infectious treatment within
days after onset of symptoms is important because intuba-ion and mechanical ventilation may be avoided in many cases.oor control of the underlying disease, performans status over 2,igh temperature, and high oxygen flow at presentation, shock,evelopment of ARDS, and clinical worsening at day 5 areelated to a poor prognosis [40]. Hypoalbuminemia is anotherndependent predictor of mortality. Pulmonary co-infection witherpes simplex virus (HSV) or CMV may contribute to a fatalutcome. A high neutrophil count in BAL samples is also asso-iated with more severe hypoxemia and higher mortality [6,15].t seems crucial to identify patients at risk of PJP consideringew immunosuppressive or immunomodulatory drugs, because
everal authors have reported that the morbidity and mortal-ty are significantly worse in this population than in those withIDS [4]. It is important to keep in mind that conventionalrognostic guidelines for community-acquired pneumonia could
1 adies
upwwsic
7
7
odhswthpsatas
7
tacensb
gMcrrsePwncmimtaisttAtv
7
adpdpia
TSSd
T
C
S
I
C
Q
B
B
96 A. Roux et al. / Médecine et mal
nderestimate the severity of non-HIV PJP, leading to a thera-eutic delay resulting in higher mortality. The most importantays to decrease mortality among non-HIV patients presentingith PJP are to make an early diagnosis and initiate the PJP-
pecific antimicrobial therapy as soon as possible. Thus, keepingn mind a high level of suspicion especially in patients receivingorticosteroids is crucial.
. Pending questions
.1. P. jirovecii colonization
P. jirovecii colonization occurs in patients without any signsr symptoms of acute pneumonia. The recent use of newetection tools suggests that colonization prevalence could beigher than previously thought. Ponce et al., in an autopsytudy, found that 65% of individuals in a general populationere colonized [41]. The colonization rate ranged from 13
o 23% when examining only oral lavage or nasal swabs. Aigh colonization prevalence was also reported among variousopulations of immunosuppressed patients and/or patients pre-enting with chronic lung disease [23]. Using corticosteroidsppears to be a major risk factor for colonization. The contribu-ion of serum BDG to distinguish infection from colonizationmong patient with positive PCR detection needs to be furthertudied.
.2. P. jirovecii transmission
Whether PJP occurs after reactivation of latent infec-ion/colonization (earlier preferred theory) or is due to de novocquisition is still debated. Convincing evidence has recentlyhallenged the “reactivation theory. Indeed, the results of sev-
ral genotyping epidemiological studies seem to support deovo person-to-person or environmental P. jirovecii transmis-ion and subsequent infection. This hypothesis is also supportedy reports of patients having experienced 2 episodes of PJP withtrta
able 13ensibility and specificity of various techniques on various samples in non-HIV-patieensibilité et spécificité des différentes techniques utilisées pour le diagnostic de pneu type de prélèvement respiratoire.
echnique Sample Sensibil
onventional staining BAL 86
IS 92–97
ilver or DQ BAL 81
IS 92
mmunofluorescence BAL 60–90
IS 97
onventional PCR BAL 100
uantitative PCR BAL 87.2–10IS 100
NPA 100
DG Plasma 94.8
AL: broncho-alveolar lavage; BDG: beta-d-glucan; IS: induced sputum; NPA: naso
infectieuses 44 (2014) 185–198
enetically different isolated strains associated to each episode.oreover, studying PJP outbreaks shows that clusters of spe-
ific genotypes are geographically associated with the place ofesidence rather than the birth place, supporting the “infection-einfection theory”. Another argument for the latter theory is thehort P. jirovecii cyst clearance period observed after PJP, neverxceeding one year. The authors of other studies have reportedJP occurring after a short period of colonization by P. jiroveciiith the same genotype, emphasizing the fact that PJP mightot be due to reactivation of childhood colonization, but thatolonized individuals are at risk for PJP. The results of severalolecular studies of PJP outbreaks seem to support the possibil-
ty of a nosocomial acquisition of the infection. Even though theain route of P. jirovecii transmission is airborne, the mode of
ransmission itself, i.e. direct person-to-person spread or fromn environmental source, remains unclear. P. jirovecii colonizedndividuals, including healthcare workers, may serve as a tran-ient reservoir for disease transmission, raising the question ofhe appropriateness of respiratory isolation of patients suspectedo have PJP, even though current guidelines do not recommend it.s recently underlined by Hauser et al., whether outbreak geno-
ypes are always predominant and whether these harbor specificirulence factors remain open questions [42].
.3. New insights into PJP infection control
PJP infection control relies upon identification of patientst risk and chemoprophylaxis, but not just that. The risk ofeveloping PJP was not prevented by the use of chemopro-hylaxis as demonstrated among kidney transplant receiversuring PJP outbreaks. Considering new evidence on person-to-erson airborne and environmental transmission, and de novonfection, supported by several reports of nosocomial outbreaksmong immunocompromised patients, and taking into account
hat immunocompetent asymptomatic carriers may act as fungaleservoirs and infection sources of limited duration, new infec-ion control measures could be recommended such as geographicnd respiratory isolation of infected patients from susceptiblents.umocystose pulmonaire chez les patients séronégatifs pour le VIH en fonction
ity (%) Specificity (%) Reference
97 [44]92
97100
100–
87 [45]
0 84.9–99.1 [21,46]100100
86.3 [25]
pharyngeal aspirate; PCR: polymerase chain reaction.

adies
phlMimfscltcbtttpi
7
Dstueta
8
cstilicwiTphpc
•••
Tr
bt
D
c
A
piA
A
i2
R
[
[
[
[
A. Roux et al. / Médecine et mal
atients, in single room. Some authors suggest that patientsighly suspected of having PJP without previous chemoprophy-axis should be preventively isolated until PJP has been ruled out.
oreover, even if there is no positive evidence of any benefit,t might be effective to provide surgical masks for compro-
ised outpatient visits. The definitive eradication of P. jiroveciirom colonized patients seems both ineffective and illusory,ince fungal acquisition and clearance appear to be dynamic,yclic, and depend on the variations of the patient’s immuno-ogic status. Indeed, since the global population is a main butransient source of infection, reducing PJP carriage in immuno-ompromised patient would only reduce the potential for spreadetween immunocompromised hospitalized patients. We believehat a multimodal approach considering monitoring of coloniza-ion, fungal load, type of used or to-be-used immunosuppressiveherapy, length and severity of current or expected immunosup-ression, and pre-emptive therapy should allow lowering PJPncidence among immunocompromised patients.
.4. Non-invasive diagnosis strategy
The high sensitivity of PCR allows detecting P. jiroveciiNA in non-invasive samples (oral lavage, nasopharyngeal
wab or lavage). To et al. recently reported a positive predic-ive value of 78.9% and a negative predictive value of 100%sing nasopharyngeal aspirate in non-HIV-patients [43]. How-ver, more studies with adapted methods are needed to confirmhe performance of a strategy associating pre-test PJP probabilitynd use of these samples (Tables 10 and 13).
. Conclusions
PJP is a severe opportunistic respiratory infection that canomplicate the evolution of many diseases related to immuno-uppression. Long-term corticosteroid therapy appears to behe main but not the only risk factor. of the availability ofmmunomodulatory treatments, intensive chemotherapy, pro-onged cancer survival, make it mandatory for the clinician tontegrate easily this disease in the spectrum of a possible etiologi-al diagnosis when confronted by a non-HIV-patient presentingith clinical respiratory signs. The prognosis of this disease
s closely related to the precocity of diagnosis and treatment.he availability of PCR, of non-invasive and easy samplingrocedures (oropharyngeal lavage), or of serum BDG dosageave greatly contributed to the diagnosis of PJP and optimalatient care. Yet, many clinical issues still have to be dealt withoncerning PJP in non-HIV patients:
how should PCR be uses for PJP diagnosis? how should serum BDG testing be used as a diagnostic aid? how and when should adjunctive corticosteroid therapy be
used?
Finally, the attention of searchers was mainly focused on-cell quantitative or qualitative defects, but the results ofecent animal studies suggest that B-cell deficiency may also
[
infectieuses 44 (2014) 185–198 197
e integrated in the process of prophylaxis, diagnosis, andreatment.
isclosure of interest
The authors declare that they have no conflicts of interestoncerning this article.
cknowledgements
This review is dedicated to the memory of Patricia Roux whoassed away recently. She was an eminent physician, workingn the laboratory of parasitology and mycology of the Saint-ntoine teaching hospital (Paris, France).
ppendix A. Supplementary data
Supplementary data associated with this article can be found,n the online version, at http://dx.doi.org/10.1016/j.medmal.014.01.007.
eferences
[1] Ward MM, Donald F. Pneumocystis carinii pneumonia in patients withconnective tissue diseases: the role of hospital experience in diagnosis andmortality. Arthritis Rheum 1999;42(4):780–9.
[2] Reid AB, Chen SC, Worth LJ. Pneumocystis jirovecii pneumonia in non-HIV-infected patients: new risks and diagnostic tools. Curr Opin Infect Dis2011;24(6):534–44.
[3] Carmona EM, Limper AH. Update on the diagnosis and treatment of Pneu-mocystis pneumonia. Ther Adv Respir Dis 2011;5(1):41–59.
[4] Yale SH, Limper AH. Pneumocystis carinii pneumonia in patients with-out acquired immunodeficiency syndrome: associated illness and priorcorticosteroid therapy. Mayo Clin Proc 1996;71(1):5–13.
[5] Sepkowitz KA. Pneumocystis carinii pneumonia among patients with neo-plastic disease. Semin Respir Infect 1992;7(2):114–21.
[6] Zahar JR, et al. Pneumocystis carinii pneumonia in critically ill patientswith malignancy: a descriptive study. Clin Infect Dis 2002;35(8):929–34.
[7] Bollee G, et al. Clinical picture of Pneumocystis jiroveci pneumonia incancer patients. Chest 2007;132(4):1305–10.
[8] Chung JB, Armstrong K, Schwartz JS, Albert D. Cost-effectiveness of pro-phylaxis against Pneumocystis carinii pneumonia in patients with Wegner’sgranulomatosis undergoing immunosuppressive therapy. Arthritis Rheum2000;43(8):1841–8.
[9] Marie I, et al. Opportunistic infections in polymyositis and dermatomyosi-tis. Arthritis Rheum 2005;53(2):155–65.
10] Liam CK, Wang F. Pneumocystis carinii pneumonia in patients with sys-temic lupus erythematosus. Lupus 1992;1(6):379–85.
11] Lertnawapan R, Totemchokchyakarn K, Nantiruj K, Janwityanujit S. Riskfactors of Pneumocystis jeroveci pneumonia in patients with systemic lupuserythematosus. Rheumatol Int 2009;29(5):491–6.
12] Mori S, Sugimoto M. Pneumocystis jirovecii infection: an emergingthreat to patients with rheumatoid arthritis. Rheumatology (Oxford)2012;51(12):2120–30.
13] Gupta D, Zachariah A, Roppelt H, Patel AM, Gruber BL. Prophylac-tic antibiotic usage for Pneumocystis jirovecii pneumonia in patientswith systemic lupus erythematosus on cyclophosphamide: a survey ofUS rheumatologists and the review of literature. J Clin Rheumatol
2008;14(5):267–72.14] Long MD, et al. Increased risk of pneumocystis jiroveci pneumoniaamong patients with inflammatory bowel disease. Inflamm Bowel Dis2013;19(5):1018–24.

1 adies
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[46] Seah C, et al. Comparison of the FXG: RESP (Asp+) real-time PCR
98 A. Roux et al. / Médecine et mal
15] Limper AH, Offord KP, Smith TF, Martin 2nd WJ. Pneumocystis cariniipneumonia. Differences in lung parasite number and inflammation inpatients with and without AIDS. Am Rev Respir Dis 1989;140(5):1204–9.
16] Monnet X, et al. Critical care management and outcome of severe Pneu-mocystis pneumonia in patients with and without HIV infection. Crit Care2008;12(1):R28.
17] Kanne JP, Yandow DR, Meyer CA. Pneumocystis jiroveci pneumonia:high-resolution CT findings in patients with and without HIV infection.AJR Am J Roentgenol 2012;198(6):W555–61.
18] Vogel MN, et al. Differences and similarities of cytomegalovirus and pneu-mocystis pneumonia in HIV-negative immunocompromised patients thinsection CT morphology in the early phase of the disease. Br J Radiol2007;80(955):516–23.
19] Vogel MN, et al. HRCT-features of Pneumocystis jiroveci pneumonia andtheir evolution before and after treatment in non-HIV immunocompromisedpatients. Eur J Radiol 2012;81(6):1315–20.
20] Demirkazik FB, Akin A, Uzun O, Akpinar MG, Ariyurek MO. CT findingsin immunocompromised patients with pulmonary infections. Diagn IntervRadiol 2008;14(2):75–82.
21] Azoulay E, et al. Polymerase chain reaction for diagnosing pneumocys-tis pneumonia in non-HIV immunocompromised patients with pulmonaryinfiltrates. Chest 2009;135(3):655–61.
22] Linssen CF, et al. Inter-laboratory comparison of three different real-timePCR assays for the detection of Pneumocystis jiroveci in bronchoalveolarlavage fluid samples. J Med Microbiol 2006;55(Pt 9):1229–35.
23] Takahashi T, et al. Pneumocystis carinii carriage in immunocompromisedpatients with and without human immunodeficiency virus infection. J MedMicrobiol 2002;51(7):611–4.
24] Damiani C, et al. Serum (1->3)-beta-D-glucan levels in primary infectionand pulmonary colonization with Pneumocystis jirovecii. J Clin Microbiol2011;49(5):2000–2.
25] Karageorgopoulos DE, et al. Accuracy of beta-D-glucan for the diagnosis ofPneumocystis jirovecii pneumonia: a meta-analysis. Clin Microbiol Infect2013;19(1):39–49.
26] Sax PE, et al. Blood (1->3)-beta-D-glucan as a diagnostic testfor HIV-related Pneumocystis jirovecii pneumonia. Clin Infect Dis2011;53(2):197–202.
27] Martin SI, Fishman JA. Pneumocystis pneumonia in solid organ transplan-tation. Am J Transplant 2013;13(Suppl. 4):272–9.
28] Tasaka S, Tokuda H. Pneumocystis jirovecii pneumonia in non-HIV-infected patients in the era of novel immunosuppressive therapies. J InfectChemother 2012;18(6):793–806.
29] Green H, Paul M, Vidal L, Leibovici L. Prophylaxis of Pneumocystispneumonia in immunocompromised non-HIV-infected patients: system-
atic review and meta-analysis of randomized controlled trials. Mayo ClinProc 2007;82(9):1052–9.30] Wang EH, et al. Pneumocystis pneumonia in solid organ transplant recipi-ents: not yet an infection of the past. Transpl Infect Dis 2012;14(5):519–25.
infectieuses 44 (2014) 185–198
31] Goto N, Oka S. Pneumocystis jirovecii pneumonia in kidney transplanta-tion. Transpl Infect Dis 2011;13(6):551–8.
32] Chapman JR, Marriott DJ, Chen SC, MacDonald PS. Post-transplant Pneu-mocystis jirovecii pneumonia–a re-emerged public health problem? KidneyInt 2013;84(2):240–3.
33] Rodriguez M, Fishman JA. Prevention of infection due to Pneumocys-tis spp. in human immunodeficiency virus-negative immunocompromisedpatients. Clin Microbiol Rev 2004;17(4):770–82.
34] Stein CR, Poole C, Kazanjian P, Meshnick SR. Sulfa use, dihydropteroatesynthase mutations, and Pneumocystis jirovecii pneumonia. Emerg InfectDis 2004;10(10):1760–5.
35] Rodriguez M, Sifri CD, Fishman JA. Failure of low-dose atovaquone pro-phylaxis against Pneumocystis jiroveci infection in transplant recipients.Clin Infect Dis 2004;38(8):e76–8.
36] Kovacs JA, et al. Pneumocystis carinii pneumonia: a comparisonbetween patients with the acquired immunodeficiency syndrome andpatients with other immunodeficiencies. Ann Intern Med 1984;100(5):663–71.
37] Kim T, et al. Is caspofungin really an effective treatment for Pneumocys-tis jirovecii pneumonia in immunocompromised patients without humanimmunodeficiency virus infection? Experiences at a single center and aliterature review. Scand J Infect Dis 2013;45(6):484–8.
38] Martin SI, Fishman JA. Pneumocystis pneumonia in solid organ transplantrecipients. Am J Transplant 2009;9(Suppl. 4):S227–33.
39] Lemiale V, Debrumetz A, Delannoy A, Alberti C, Azoulay E. Adjunc-tive steroid in HIV-negative patients with severe Pneumocystis pneumonia.Respir Res 2013;14(1):87.
40] Toper C, et al. [Pneumocystis jirovecii pneumonia in non-HIV infectedpatients: a study of 41 cases]. Rev Pneumol Clin 2011;67(4):191–8.
41] Ponce CA, Gallo M, Bustamante R, Vargas SL. Pneumocystis colonizationis highly prevalent in the autopsied lungs of the general population. ClinInfect Dis 2010;50(3):347–53.
42] Hauser P, Rabodonirina M, Nevez G. Pneumocystis jirovecii genotypesinvolved in pneumocystis pneumonia outbreaks among renal transplantrecipients. Clin Infect Dis 2013;56(1):165–6.
43] To KK, et al. Use of nasopharyngeal aspirate for diagnosis of pneumocystispneumonia. J Clin Microbiol 2013;51(5):1570–4.
44] Cregan P, et al. Comparison of four methods for rapid detectionof Pneumocystis carinii in respiratory specimens. J Clin Microbiol1990;28(11):2432–6.
45] Ribes JA, Limper AH, Espy MJ, Smith TF. PCR detection of Pneumocystiscarinii in bronchoalveolar lavage specimens: analysis of sensitivity andspecificity. J Clin Microbiol 1997;35(4):830–5.
assay with direct immunofluorescence and calcofluor white staining for thedetection of Pneumocystis jirovecii in respiratory specimens. Med Mycol2012;50(3):324–7.