Embed Size (px)
Citation preview

Update on the Diagnosis & Update on the Diagnosis & Management of Acute Aortic Dissection Management of Acute Aortic Dissection
Kim A. Eagle, MDKim A. Eagle, MDDirectorDirector
University of MichiganUniversity of MichiganCardiovascular CenterCardiovascular Center

Kim A. Eagle, MD, FACCDirector University of Michigan Cardiovascular Center
Grants: Hewlett Foundation, Mardigian Foundation, Varbedian Fund, GORE
Consultant: NIH NHLBI

““Acute Aortic SyndromesAcute Aortic Syndromes””
•• Classic Aortic Classic Aortic
DissectionDissection
•• Intramural Intramural
HematomaHematoma
•• Penetrating Penetrating
Aortic UlcerAortic Ulcer
AorticAorticDissectionDissection
IMHIMH
PAU

“Atypical" Aortic Dissection(Intramural Hematoma)
“Atypical" Aortic Dissection(Intramural Hematoma)
TL
FL
Typical = Dissection flap and false lumen"Atypical" = No dissection flap; Medial hematoma
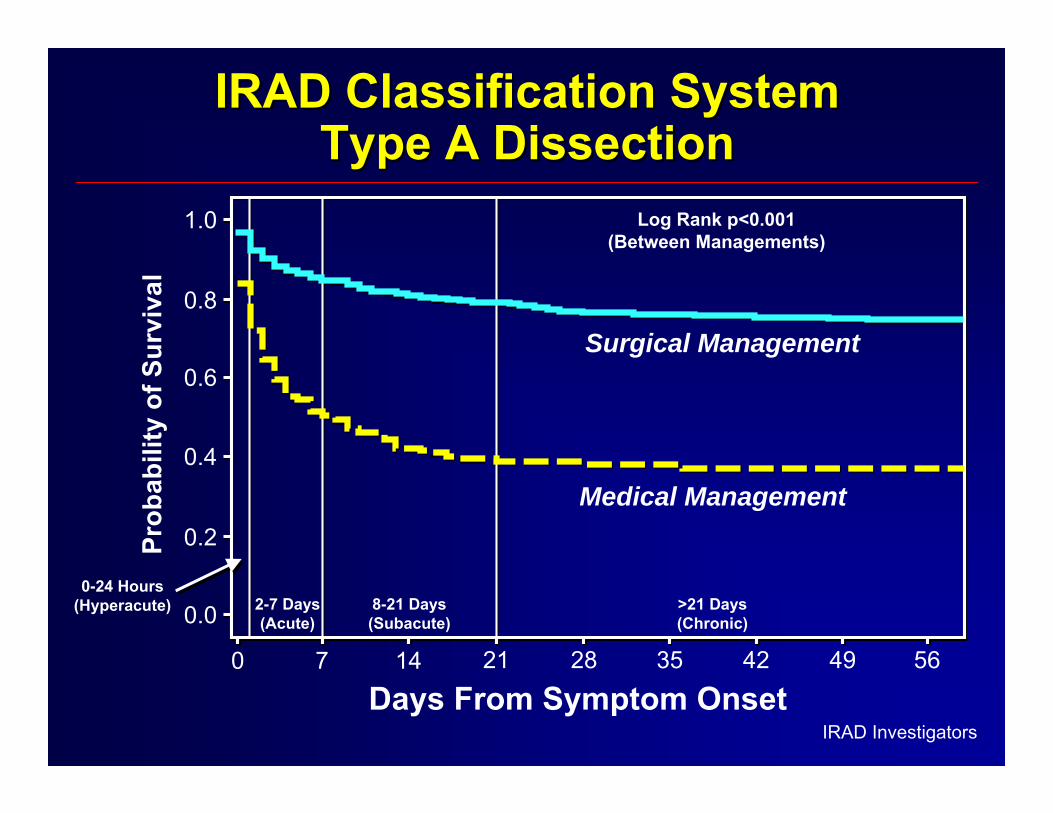
IRAD Classification SystemIRAD Classification SystemType A DissectionType A Dissection
IRAD Investigators
5649423528211470
Days From Symptom Onset
Prob
abili
ty o
f Sur
viva
l
0.0
0.2
0.8
1.0
Surgical Management
Medical Management
Log Rank p<0.001(Between Managements)
8-21 Days(Subacute)
>21 Days(Chronic)
2-7 Days(Acute)
0-24 Hours(Hyperacute)
0.4
0.6

IRAD Classification SystemIRAD Classification SystemType B DissectionType B Dissection
5649423528211470Days From Symptom Onset
Prob
abili
ty o
f Sur
viva
l
0.7
0.8
0.9
1.0
Surgical Management
Medical Management
Endovascular Management
Log Rank p<0.001(Between Managements)
8-21 Days(Subacute)
>21 Days(Chronic)
2-7 Days(Acute)
0-24 Hours(Hyperacute)
IRAD Investigators

Variable All Type A Type B p-value(n=3037) (n=1924) (n=1113)
Age (yrs) 61.9 61.3 63.0 0.003 Male 67.1% 67.2% 67.1% NSHTN 75.2% 72.0% 80.7% <0.001Marfan 4.3% 4.5% 3.8% NS
Prior Heart 16.9% 15.3% 19.8% 0.002Surgery
Iatrogenic 3.3% 3.8% 2.6% 0.09
Demographics and Past HistoryDemographics and Past History
IRAD Investigators

GeneticGeneticSyndromeSyndrome
CommonCommonClinicalClinical
FeaturesFeaturesGeneticGeneticDefectDefect
DiagnosticDiagnosticTestTest
MarfanMarfanSyndromeSyndrome
Skeletal featuresSkeletal featuresEctopic lentleEctopic lentle
FBN1FBN1mutations*mutations*
Ghent diagnosticGhent diagnosticCriteria, DNA for Criteria, DNA for sequencingsequencing
LoeysLoeys--DietzDietzSyndromeSyndrome
Bifid uvula or cleft Bifid uvula or cleft palatepalateArterial tortuosityArterial tortuosityHypertelorismHypertelorism
TGFBR2TGFBR2 ororTGFBR1TGFBR1mutationsmutations
DNA forDNA forsequencingsequencing
EhlersEhlers--DaniosDaniosSyndromeSyndrome
Thin, translucent Thin, translucent skin GI ruptureskin GI ruptureRupture of gravid Rupture of gravid uterusuterusRupture of medium Rupture of medium to large arteriesto large arteries
COL3A1COL3A1mutationsmutations
DNA for sequencingDNA for sequencingDermal fibroblasts Dermal fibroblasts for analysis of type for analysis of type 3 collagen3 collagen
TurnerTurnerSyndromeSyndrome
Short statureShort staturePrimary amenorheaPrimary amenorheaBAVBAVAortic coarctationAortic coarctation
45 X45 Xkaryotypekaryotype
Cells for karyotype Cells for karyotype analysisanalysis
Genetic Disorders:Genetic Disorders:Thoracic Aortic DiseaseThoracic Aortic Disease
*The defective gene at a second locus for MFS is TGFBR2 but the clinical phenotype as MFS is debated.

Genetics of Familial ThoracicGenetics of Familial Thoracic(n = 454 Families)(n = 454 Families)
Defective GeneDefective GeneLeading to Leading to
FamilialFamilialTAADTAAD
Frequency inFrequency inFamilial TAADFamilial TAAD
AssociatedAssociatedClinicalClinical
FeaturesFeatures
Comments onComments onAortic DiseaseAortic DiseaseManagementManagement
TGFBR2 TGFBR2 mutationmutation(R460)(R460)
4%4%
Thin translucent Thin translucent skinskinArterial tortuosity Arterial tortuosity is more common is more common in older in older individualsindividualsAneurysms of Aneurysms of arteriesarteries
Multiple aortic Multiple aortic dissections dissections documented at documented at aortic diameters aortic diameters <5.0cm<5.0cm
MYH11 MYH11 mutationsmutations 1%1% PDAPDA
Patient with Patient with document document dissection at dissection at 4.5cm4.5cm
ACTA2 ACTA2 mutationsmutations 14%14% Livedo reticularisLivedo reticularis
Iris flocculiIris flocculi
2 of 13 patients 2 of 13 patients with documented with documented dissections dissections <5.0cm<5.0cm

TAD Guidelines: Genetic ConditionsTAD Guidelines: Genetic ConditionsConditionMarfan Syndrome
Recommendation• Echo at Dx and 6
months• Echo annually if stable• Echo more often if Ao.
Diam. increasing or >4.5cm
• Prophyllactic surgery at 4.5-5.0cm
• Prophyllactic surgery in women planning pregnancy at 4.0cm
Evid. LevelΙ
ΙΙ
ΙΙa
ΙΙa
Hiratzka LF, et al. JACC 2010;55:1509-44.
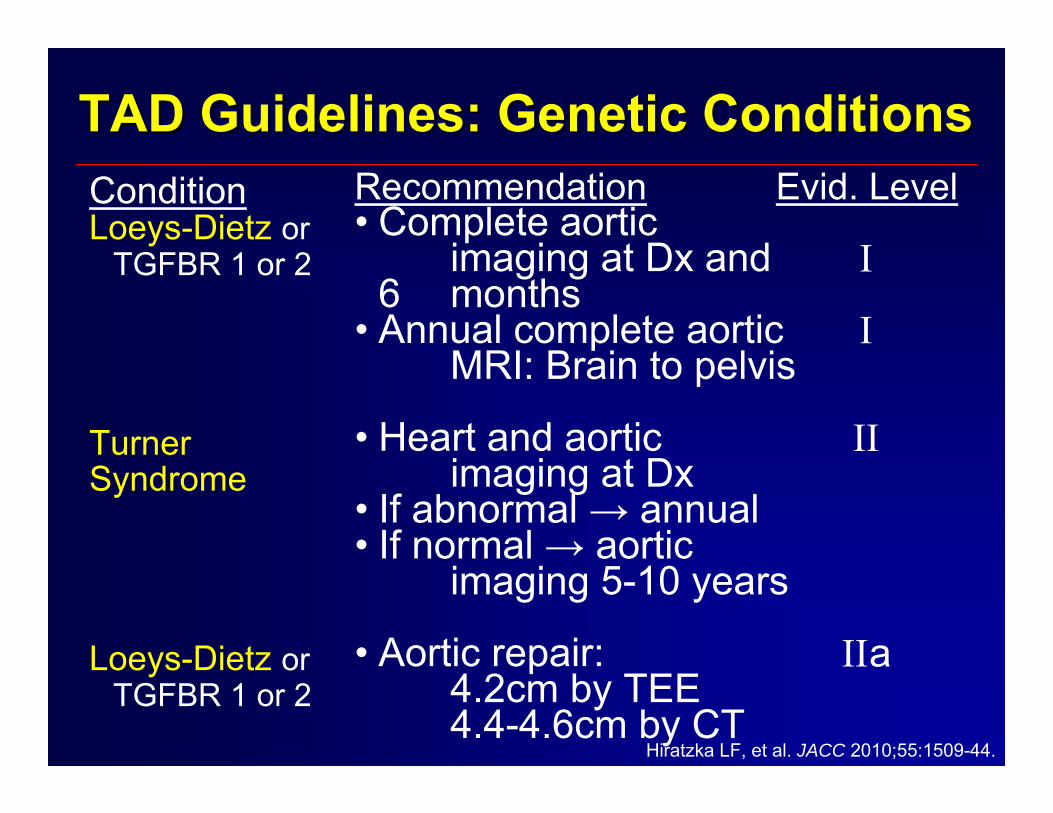
TAD Guidelines: Genetic ConditionsTAD Guidelines: Genetic ConditionsConditionLoeys-Dietz or
TGFBR 1 or 2
Turner Syndrome
Loeys-Dietz orTGFBR 1 or 2
Recommendation• Complete aortic
imaging at Dx and 6 months
• Annual complete aortic MRI: Brain to pelvis
• Heart and aortic imaging at Dx
• If abnormal → annual• If normal → aortic
imaging 5-10 years
• Aortic repair:4.2cm by TEE4.4-4.6cm by CT
Evid. Level
Ι
Ι
ΙΙ
ΙΙa
Hiratzka LF, et al. JACC 2010;55:1509-44.
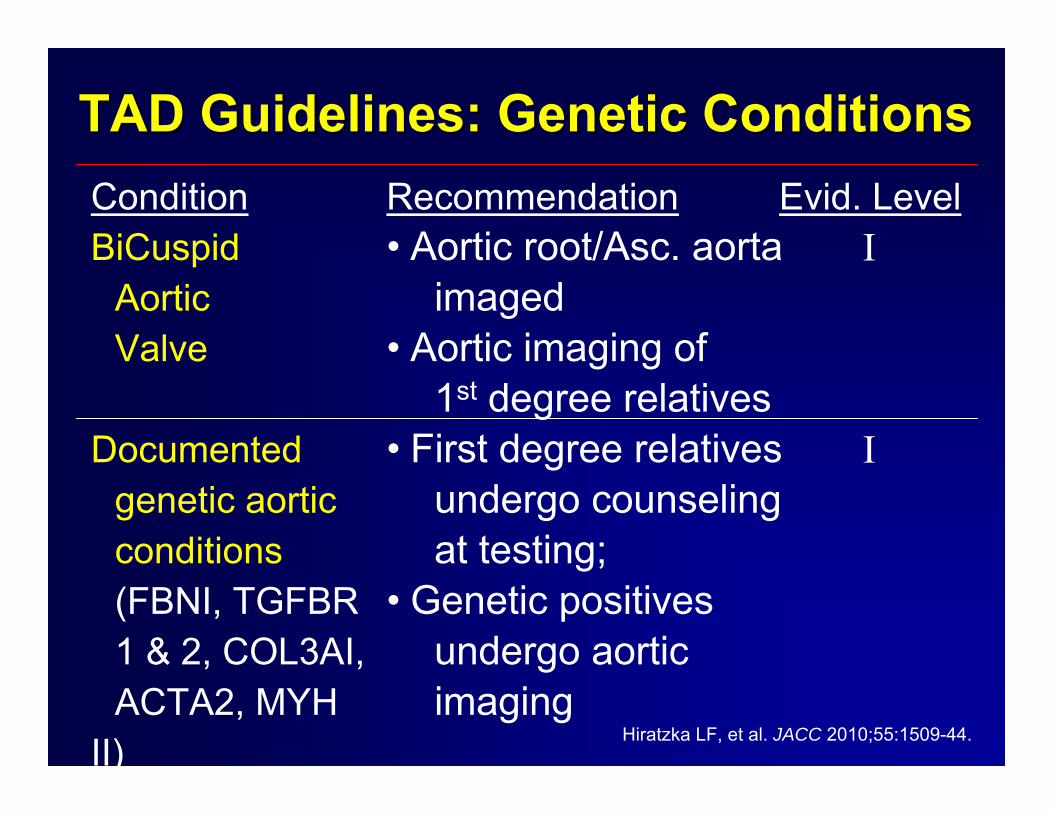
ConditionBiCuspid
AorticValve
Documentedgenetic aortic conditions (FBNI, TGFBR 1 & 2, COL3AI, ACTA2, MYH
II)
TAD Guidelines: Genetic ConditionsTAD Guidelines: Genetic ConditionsRecommendation• Aortic root/Asc. aorta
imaged• Aortic imaging of
1st degree relatives• First degree relatives
undergo counselingat testing;
• Genetic positivesundergo aortic imaging
Evid. LevelΙ
Ι
Hiratzka LF, et al. JACC 2010;55:1509-44.

p-value<0.001
0.06<0.001
<0.001
<0.001
<0.001
0.004
<0.001
IRADIRADPresenting SymptomsPresenting Symptoms
Variable• Pain
AbruptAnterior
Back
Abdominal
Sharp
Tearing
• Syncope
All94.0%
84.0%71.9%
53.1%
31.2%
62.8%
47.1%
12.6%
Type A92.6%
82.9%78.0%
42.8%
25.5%
58.4%
44.0%
18.3%
Type B96.5%
85.7%61.1%
70.5%
40.8%
69.4%
52.0%
2.9%
IRAD Investigators(n=2807)

IRADIRADPhysical ExamPhysical Exam
(n=2820)(n=2820)
VariableHigh BP
Low BP
Shock/Tamponade
Murmur AI
Pulse Deficit
Stroke
All43.3%
11.4%
8.0%
27.6%
25.7%
6.5%
Type A30.3%
16.0%
12.0%
38.3%
30.5%
9.1%
Type B65.3%
3.5%
1.3%
10.7%
18.1%
2.2%
p-value<0.001
<0.001
<0.001
<0.001
<0.001
<0.001
IRAD Investigators

Variable• CXR
Normal Wide Mediast.or Aorta
PL. Effusion• EKG
NormalNSST-T ’sIschemiaNew MI
IRADIRADEKG & CXREKG & CXR
(n=2353)
All
22.4%
67.6%14.4%
32.2%40.7%14.3%
5.5%
Type A
20.2%
69.5%12.5%
29.9%41.2%17.1%
7.4%
Type B
25.9%
64.5%17.3%
36.2%39.8%
9.6%2.1%
p-value
0.001
0.0120.002
0.001NS
<0.001<0.001
IRAD Investigators

DD--Dimer Levels in Aortic DissectionDimer Levels in Aortic Dissection
Suzuki T, et al. Circulation 2009;119:2702-07.
0
1000
2000
3000
4000
5000
D-D
imer
(ng/
ml)
AD+(A)n=19
AD+(B)n=4
MIn=9
Anginan=14
PEn=2
Time after onset (0-6h)
AD+(A)n=26
AD+(B)n=7
MIn=14
Anginan=5
PE
Time after onset (6-12h)
AD+(A)n=19
AD+(B)n=12
MIn=23
Anginan=18
PEn=3
Time after onset (12-24h)

Sensitivity of the First Imaging Study to Sensitivity of the First Imaging Study to Detect AoD and Intramural HematomaDetect AoD and Intramural Hematoma
IRAD Investigators
85.5%85.5%97.3%97.3% 96.9%96.9%
87.3%87.3%559559654654
1880188019331933
31313232 6262
7171
(n=2690)
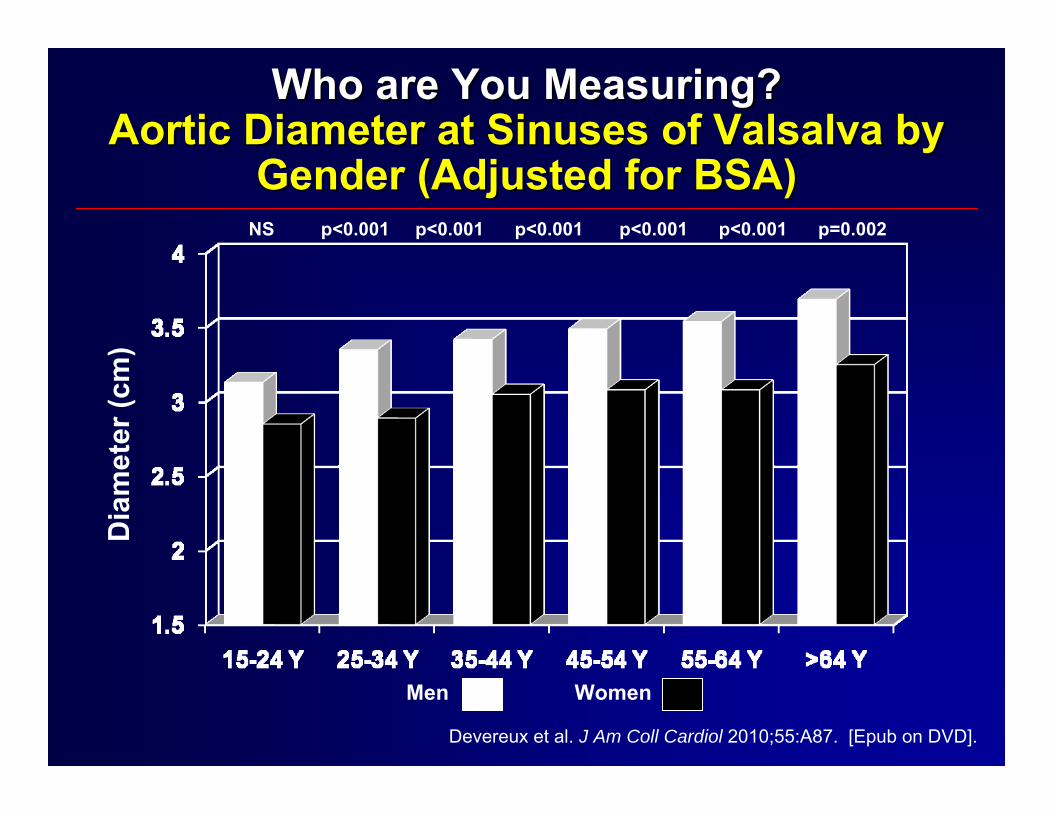
Who are You Measuring?Who are You Measuring?Aortic Diameter at Sinuses of Valsalva by Aortic Diameter at Sinuses of Valsalva by
Gender (Adjusted for BSA)Gender (Adjusted for BSA)NS p<0.001 p<0.001 p<0.001 p<0.001 p<0.001 p=0.002
Men Women
Dia
met
er (c
m)
Devereux et al. J Am Coll Cardiol 2010;55:A87. [Epub on DVD].

Proportion of U.S. Citizens withDilated Ascending Aortas
Proportion of U.S. Citizens withDilated Ascending Aortas
4.2 - 4.4cm 3,800,000+
4.5 – 4.9cm 1,600,000+
≥ 5.0cm 200,000+
+20% caused by genetic condition.
R. Devereux. Aortic Summit. Sept 22, 2009.

Aortic Aneurysms:Aortic Aneurysms:Yearly Risk of ComplicationsYearly Risk of Complications
Scientific American, August: 2005.
Ave
rage
Yea
rly R
ate
of C
ompl
icat
ions
(%)
Rupture Dissection Rupture orDissection
Diameter ofDiameter ofAneurysm (cm)Aneurysm (cm)
4.0 to 4.94.0 to 4.9
5.0 to 5.95.0 to 5.9
6.0 or greater6.0 or greater

Maximum Aorta Diameter:Maximum Aorta Diameter:Type A DissectionType A Dissection
Pape et al. AHA 2005.
(59% < 5.5 cm)

Descending Aortic Diameter Descending Aortic Diameter ≥≥ 6.0cm: A 6.0cm: A Poor Predictor of Type B Aortic DissectionPoor Predictor of Type B Aortic Dissection
Cou
nt
Trimarchi S, et al. J Am Coll Cardiol 2009;53: A452.Descending Diameter
Descending Diameter (categorical)
• Medical Therapy for all, for life
• Surgery if possible….esp A1>A2>A3
• Consider fenestration if surgery not
possible, especially if malperfusion
occurs
Type A DissectionType A Dissection

InIn--hospital Survival hospital Survival in TAin TA--AADAAD
Sinha S, presented ACC 2011.
Follow-up Survival in TA-AAD

• Uncomplicated - No false lumen: Medical
• Uncomplicated - False channel +/- aneurysm - consider stent
• Complicated - stent +/- surgery
Type B DissectionType B Dissection
Nienaber CA, et al. Circulation 2003;108:628-635.Nienaber CA, et al. Circulation 2003;108:772-778.
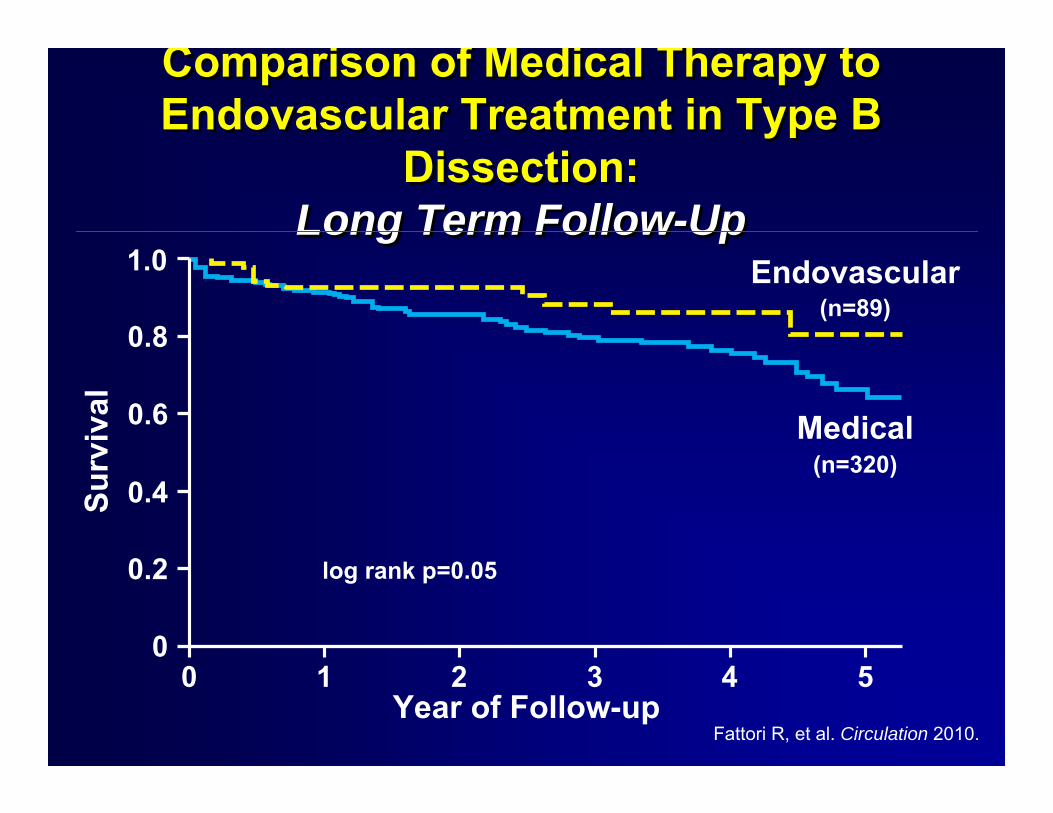
Comparison of Medical Therapy to Endovascular Treatment in Type B
Dissection:Long Term Follow-Up
Comparison of Medical Therapy to Endovascular Treatment in Type B
Dissection:Long Term Follow-Up
Fattori R, et al. Circulation 2010.
Endovascular
Year of Follow-up0 1 2 3 4 5
1.0
0
0.2
0.4
0.6
0.8
Surv
ival
log rank p=0.05
Medical
(n=89)
(n=320)
• Evidence of leakage or subacute rupture
• Extensive false channel despite excellent
medical Rx
• Extensive aneurysm
• Progressive morbidity despite medical Rx
Stent Graft TherapyStent Graft TherapyIndications in Acute DissectionIndications in Acute Dissection
Nienaber CA, et al. Circulation 2003;108:628-635.Nienaber CA, et al. Circulation 2003;108:772-778.
1. Beta-blockers
2. Ca++ blockers
3. ACE/ARB
4. Statins
FollowFollow--up Treatment?up Treatment?

Medical ManagementMedical ManagementCITATION STUDY DESIGN RESULTS
Genoni et al. Eur J CardioThorac Surg. 2001; 5:606-10.
Retrospective: 78/130 pts with chronic dissection on medical therapy only
Dissection Related Surgery51/71 B-blocker → 10 (19%)20/71 other → 9 (45%)
Aortic ExpansionBB 6/51 (12%)
Other 8/20 (40%)Shores, et al. NEJM 1994;330:1335.
Randomized Trial inAortic Root Disease(propranolol 212±68 mg)
Aortic Dilation RatePropranolol 0.023 cm/yrNot on BB 0.084 cm/yr
Ladoceur et al. Am J Cardiol 2007; 99:406.
Retrospective; Ao Dilation in children withMarfan Syndrome
Dilation slowed by 0.2mm/yr

Beta Adrenergic Blockade Slows Beta Adrenergic Blockade Slows Aorta Growth in MarfanAorta Growth in Marfan’’ss
Shores, J. NEJM 1994; 330:1335-1341.
Randomized trial of propranolol in 70 adolescent and adultpatients with classic Marfan's syndrome

BetaBeta--Blockers Lower RiskBlockers Lower Riskin Ehlerin Ehler--DanosDanos
Kaplan-Meier curves of event-free survival in 53 patients with vascular Ehlers-Danlos Primary endpoint (A). Primary and secondary endpoints (B).
Kim-Thanh Ong et al. www.thelancet.com 2010:376;1476-84.

Medical Management: ACE & ARBsMedical Management: ACE & ARBs
CITATION STUDY DESIGN RESULTSHackam et al.
Lancet2006;368:659.
Retrospective, Case control, Population Based
ACE inhibition prior to admission:Decr. likelihood of ruptureAneurysm OR 0.82 (0.74-0.90)
Mochizuki et al. Lancet 2007; 369:
1431.
Randomized with HTN, CAD or CHF to Valsartan (40-160mg) or other.
Valsartan decreased:Composite CV outcome- OR 0.61 (0.47-0.79)Aortic Dissection- OR 0.18 (0.04-0.88)
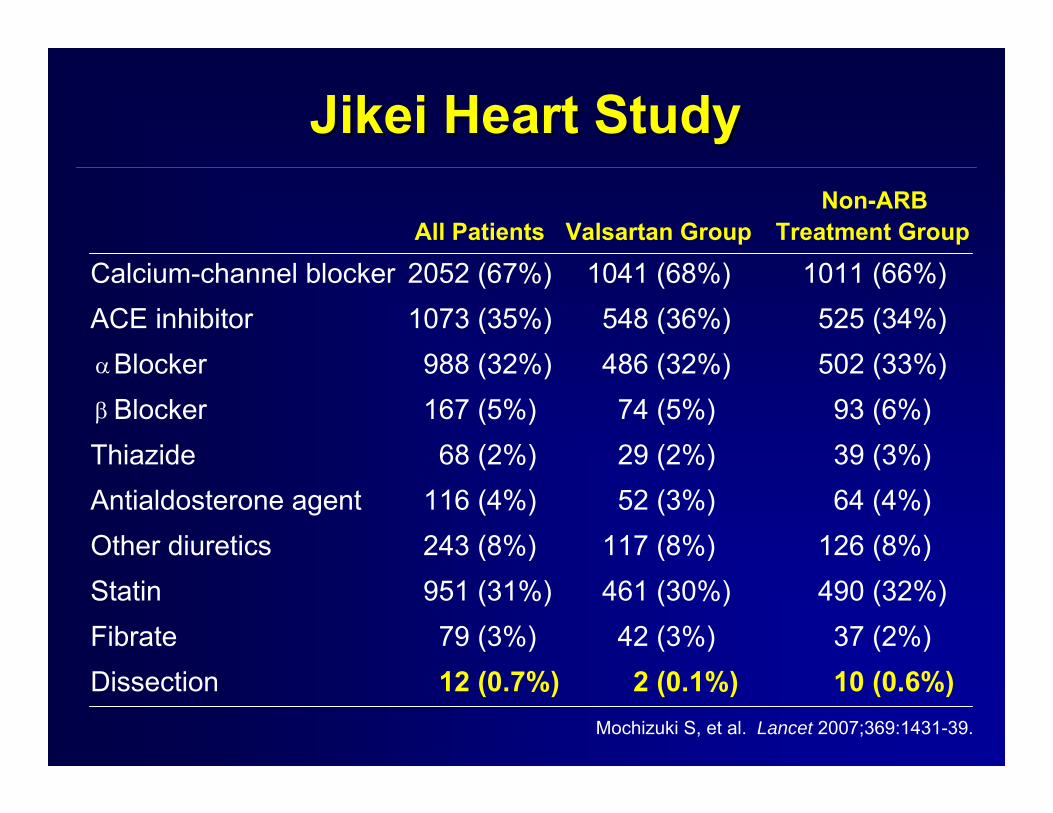
Jikei Heart StudyJikei Heart Study
Mochizuki S, et al. Lancet 2007;369:1431-39.
Non-ARBAll Patients Valsartan Group Treatment Group
Calcium-channel blocker 2052 (67%) 1041 (68%) 1011 (66%)ACE inhibitor 1073 (35%) 548 (36%) 525 (34%)
Blocker 988 (32%) 486 (32%) 502 (33%)Blocker 167 (5%) 74 (5%) 93 (6%)
Thiazide 68 (2%) 29 (2%) 39 (3%)Antialdosterone agent 116 (4%) 52 (3%) 64 (4%)Other diuretics 243 (8%) 117 (8%) 126 (8%)Statin 951 (31%) 461 (30%) 490 (32%)Fibrate 79 (3%) 42 (3%) 37 (2%)Dissection 12 (0.7%) 2 (0.1%) 10 (0.6%)
α
β

LongLong--TermTerm
• B-Blockers: HR <60BPM
• Control Blood Pressure: <120/80 -Prefer ARB’s or ACE’s
• Statins for atherosclerosis
• “Watch” for aneurysm formation: 1, 3, 6, 12 months to start
• Educate the patient: a lifelong disease; sx, activity, meds, f/up

Where is the Future?Where is the Future?
Clinical DataClinical DataTreatmentsTreatmentsFamily HistoryFamily HistoryDemographicsDemographicsEnvironmentalEnvironmental
ImagingImaging
Gene Expression ProfilesGene Expression Profiles
Genomic DataGenomic DataSNPSNP’’ssGenomeGenome--scale sequencescale sequence
Metabolic DataMetabolic DataProteomic DataProteomic Data
??
Predictions:Predictions:RiskRisk
Individualized Prognosis & DiagnosisIndividualized Prognosis & DiagnosisDrug ResponseDrug Response
Environment (e.g. Diet) ResponseEnvironment (e.g. Diet) Response
PatternsPatternsIntegrationIntegration
ModelsModels