Embed Size (px)
Citation preview

CAPRI CARDIOVASCULAR CONFERENCE 2016 Capri, april 15 – 16. 2016
UPDATE SULLA DOPPIA ANTIAGGREGAZIONE PIASTRINICA
NELLA SINDROME CORONARICA ACUTA ALLA LUCE DELLE
NUONE LINEE GUIDA EUROPEE
Pasquale Perrone Filardi
Università Federico II Napoli


K-M estimate of time to first primary efficacy event (Composite of CV death, MI or stroke)
No. at risk
Clopidogrel
Ticagrelor
9,291
9,333
8,521
8,628
8,362
8,460
8,124
Days after randomisation
6,743
6,743
5,096
5,161
4,047
4,147
0 60 120 180 240 300 360
12
11
10
9
8
7
6
5
4
3
2
1
0
13 C
um
ula
tive i
ncid
en
ce (
%)
9.8
11.7
8,219
HR 0.84 (95% CI 0.77–0.92), p=0.0003
Clopidogrel
Ticagrelor
Completeness of follow-up 99.97% = five patients lost to follow-up
K-M = Kaplan-Meier; HR = hazard ratio; CI = confidence interval
Wallentin L et al. N Engl J Med. 2009 Sep 10;361(11):1045-57
4
~1 in 5 patients will suffer a MI, stroke or CV death within the first year after a MI
APOLLO HELICON Sweden analysis
CV, cardiovascular; MI, myocardial infarction.
Jernberg T, et al. ESC poster 2014: In press.
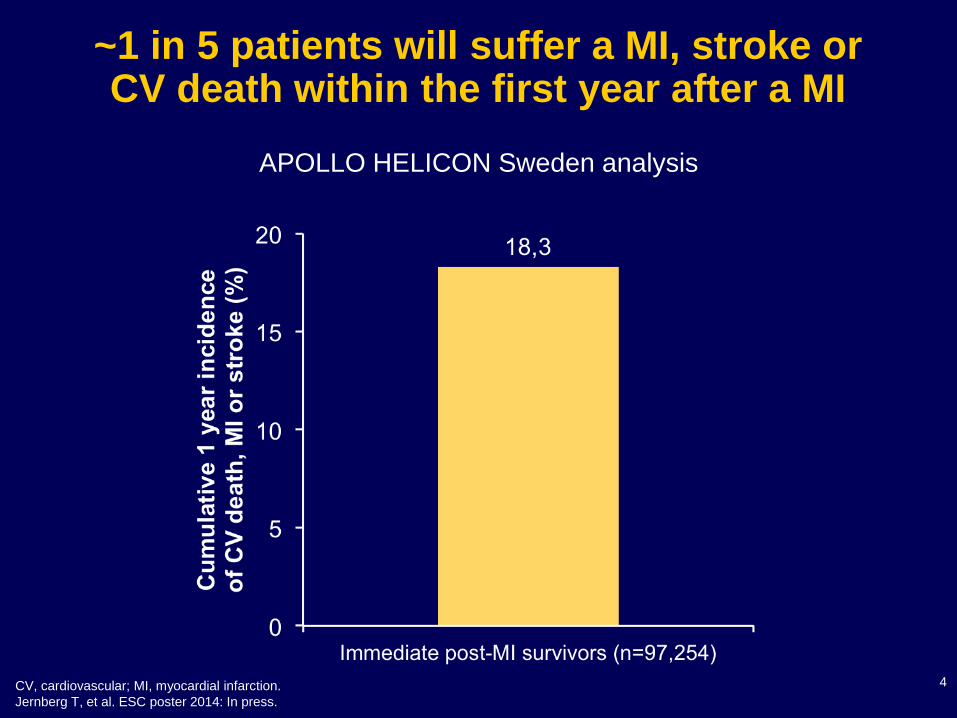
700 pts with ACS UA (with ECGΔ) or NSTEMI or STEMI >24º
undergoing PCI of 1 or 2 major coronary arteries
at up to 40 sites in the U.S. and Europe
PCI of culprit lesion(s)
Successful and uncomplicated
Formally enrolled
Metabolic S.
• Waist circum
• Fast lipids
• Fast glu
• HgbA1C
• Fast insulin
• Creatinine
Biomarkers
• Hs CRP
• IL-6
• sCD40L
• MPO
• TNFα
• MMP9
• Lp-PLA2
• others
PI: Gregg W. Stone
Sponsor: Abbott Vascular; Partner: Volcano
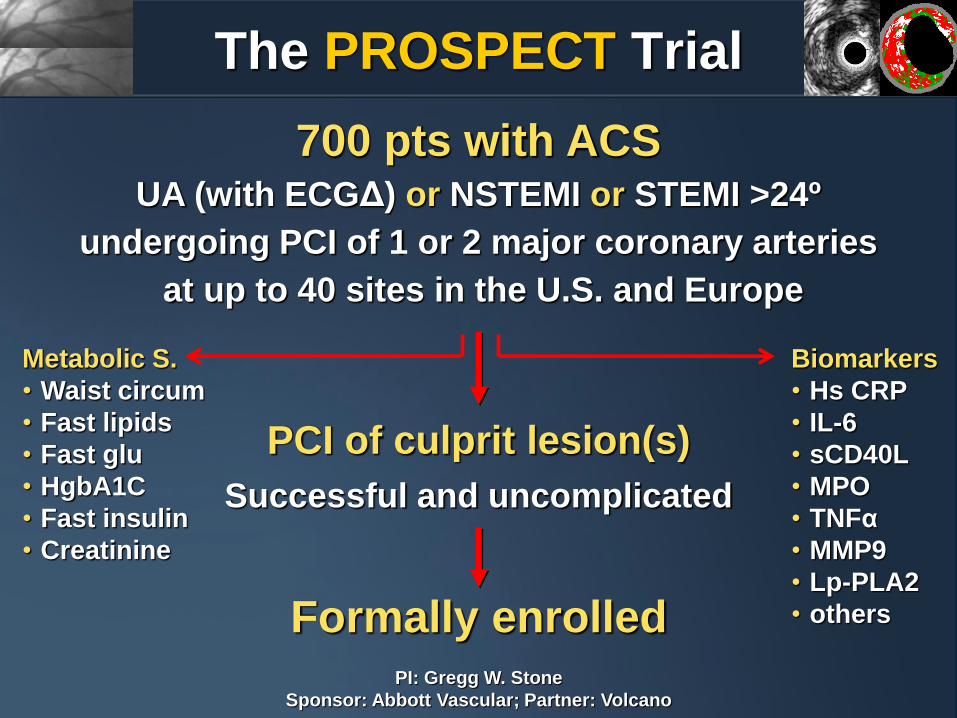
The PROSPECT Trial
PROSPECT: MACE M
AC
E (
%)
Time in Years
0 1 2 3
All
Culprit lesion (CL) related
Non culprit lesion (NCL) related
Indeterminate
0
5
10
15
20
25
Number at risk
ALL 697 557 506 480
CL related 697 590 543 518
NCL related 697 595 553 521
Indeterminate 697 634 604 583
12.9%
20.4%
11.6%
2.7%

PROSPECT: VH-TCFA and Non
Culprit Lesion Related Events
Lesion HR 3.84 (2.22, 6.65) 6.41 (3.35, 12.24) 10.77 (5.53, 21.00) 10.81 (4.30, 27.22)
P value <0.0001 <0.0001 <0.0001 <0.0001
Prevalence* 51.2% 17.4% 11.0% 4.6%
*Likelihood of one or more such lesions being present per patient. PB = plaque burden at the MLA

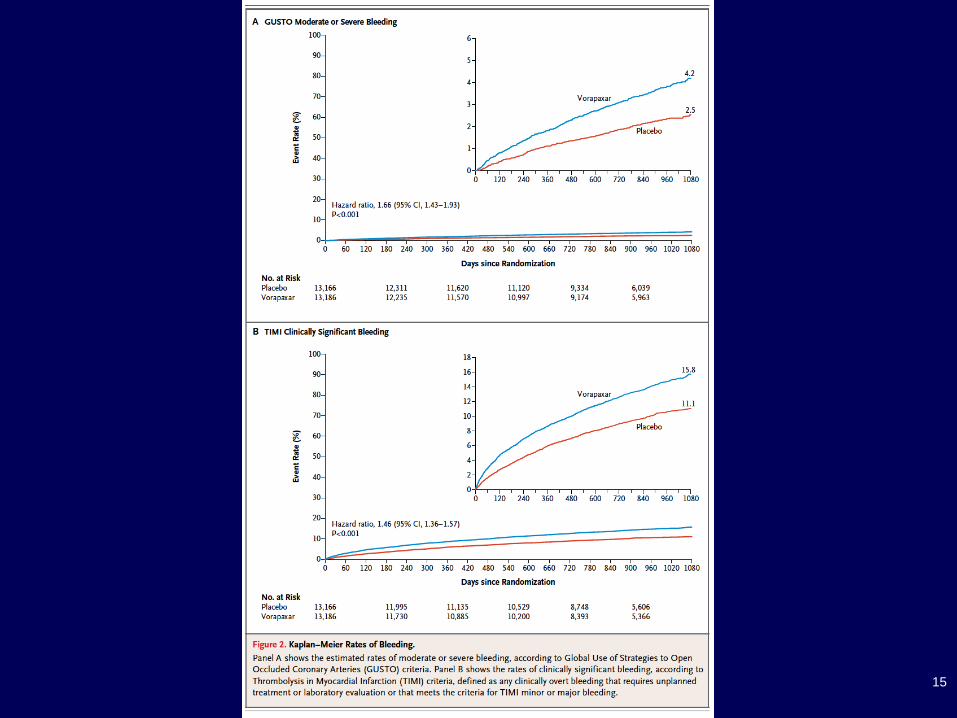
Tricoci P et al. N Engl J Med 2012;366:20-33.
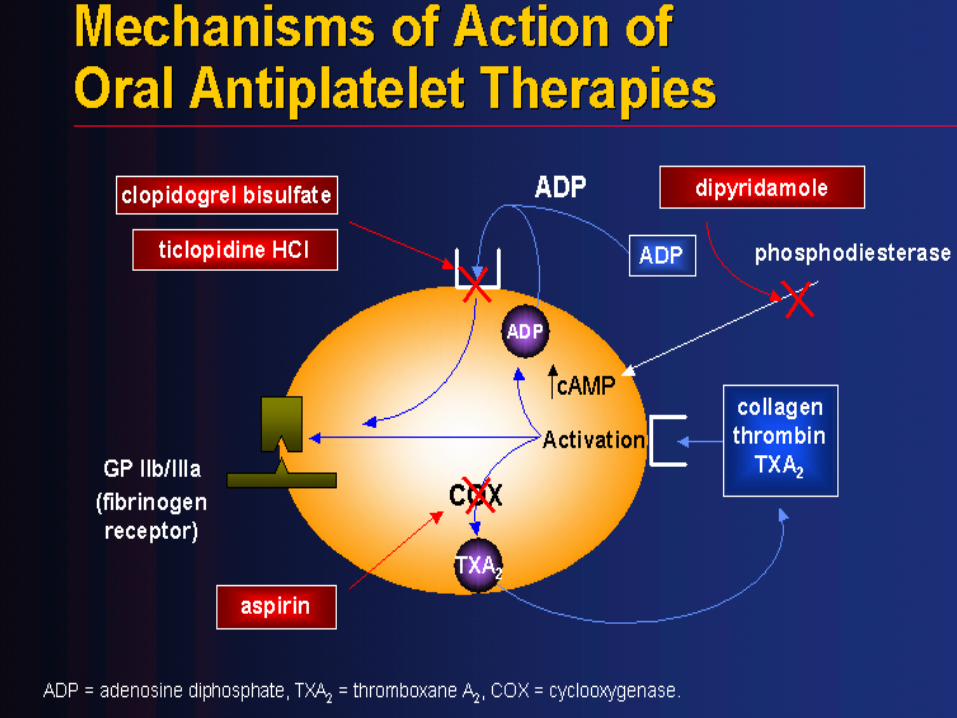
PROTEASE ACTIVATOR RECEPTOR 1 (PAR1) INHIBITION IN ACS

ALMOST
SIGNIFICANT
SIGNIFICANT
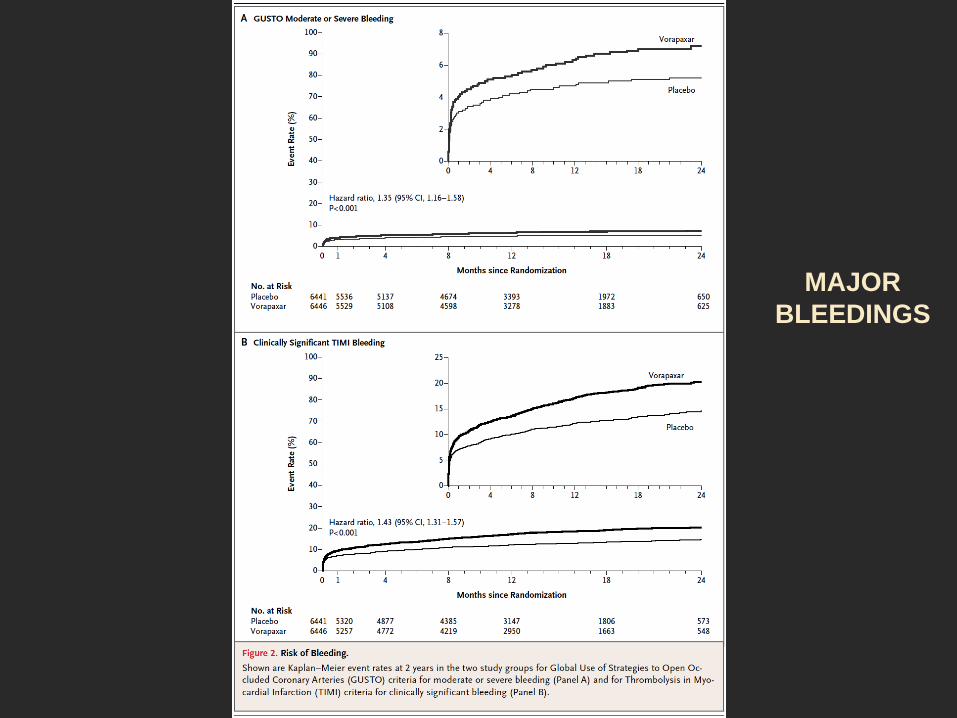
MAJOR
BLEEDINGS

12
Up to a third of patients who are event free for the first year post-MI, will suffer a MI, stroke or
death within 3 years
APOLLO 4-country analysis : Observed Incidence
*US sample restricted to patients aged ≥65 years. MI, myocardial infarction.
Rapsomaniki E, et al. ESC Late Breaking Registry presentation 2014: In press.
13
14
15

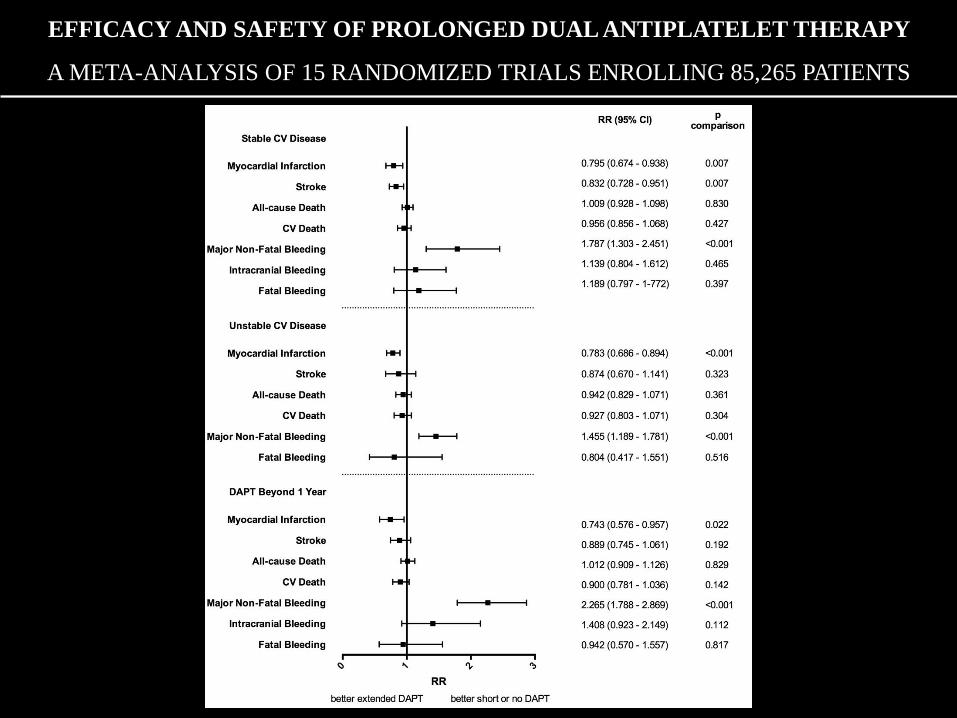
EFFICACY AND SAFETY OF PROLONGED DUAL ANTIPLATELET THERAPY
A META-ANALYSIS OF 15 RANDOMIZED TRIALS ENROLLING 85,265 PATIENTS

Udell JA et al. Eur Heart J 2015
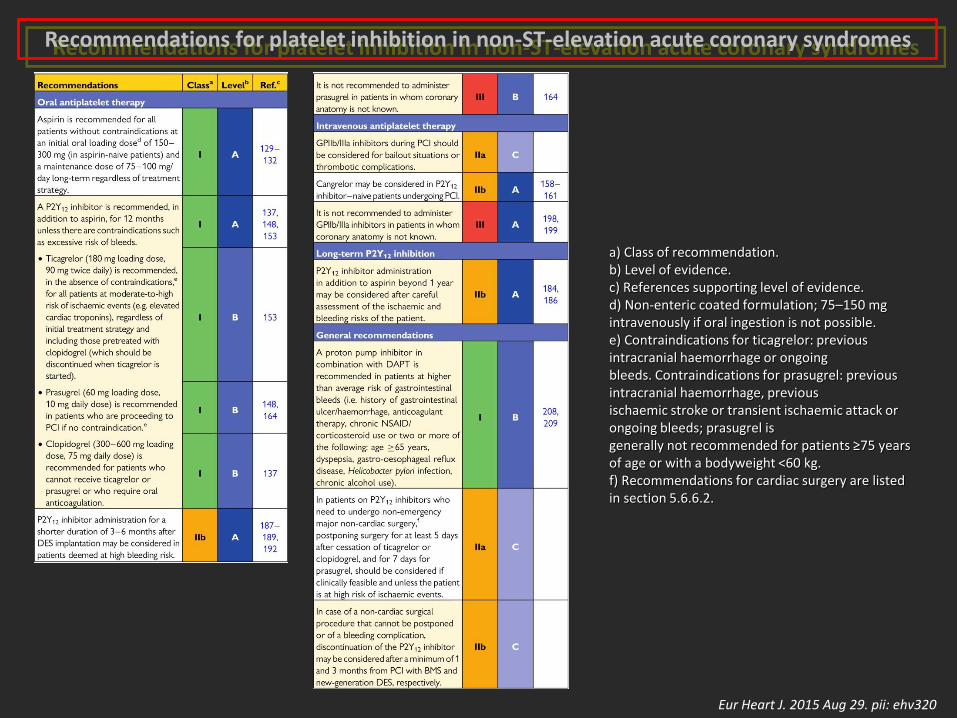
Recommendations for platelet inhibition in non-ST-elevation acute coronary syndromes
Eur Heart J. 2015 Aug 29. pii: ehv320
a) Class of recommendation. b) Level of evidence. c) References supporting level of evidence. d) Non-enteric coated formulation; 75–150 mg intravenously if oral ingestion is not possible. e) Contraindications for ticagrelor: previous intracranial haemorrhage or ongoing bleeds. Contraindications for prasugrel: previous intracranial haemorrhage, previous ischaemic stroke or transient ischaemic attack or ongoing bleeds; prasugrel is generally not recommended for patients ≥75 years of age or with a bodyweight <60 kg. f) Recommendations for cardiac surgery are listed in section 5.6.6.2.

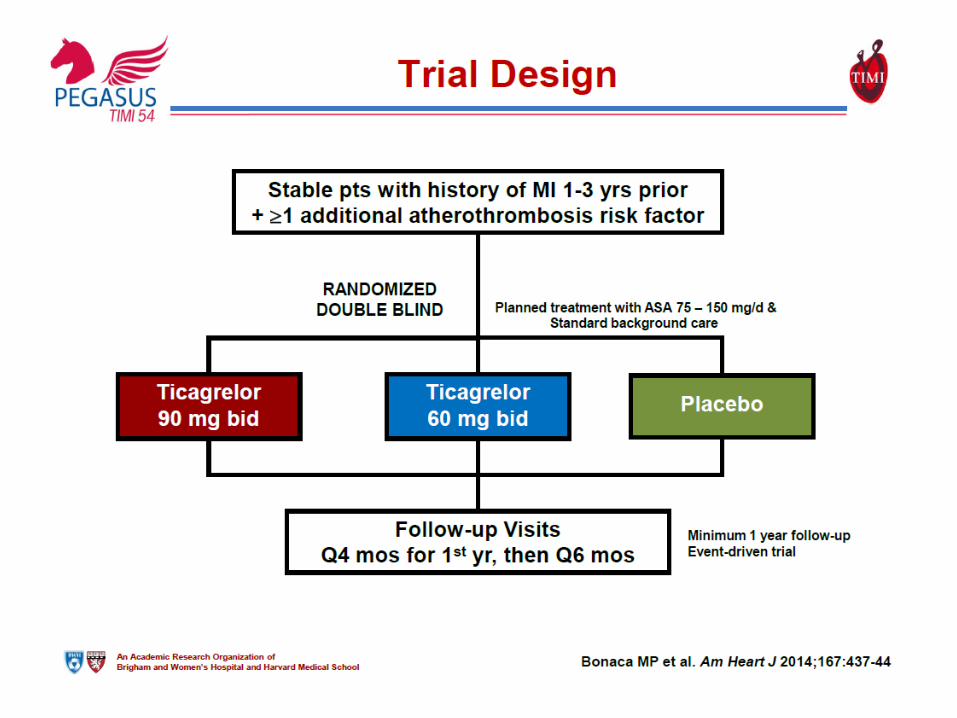
Reduction in Ischemic Events with Ticagrelor in
Diabetic Patients from the PEGASUS-TIMI 54 Trial
Deepak L. Bhatt, MD, MPH, Marc P. Bonaca, MD, MPH,
Sameer Bansilal, MD, MS, Dominick J. Angiolillo,
MD, PhD, Marc Cohen, MD, Robert F. Storey, MD,
Kyungah Im, PhD, Sabina A. Murphy, MPH, Peter
Held, MD, PhD, Eugene Braunwald, MD, Marc S.
Sabatine, MD, MPH, Ph.
Gabriel Steg MD, on behalf of the PEGASUS-TIMI 54
Steering Committee and Investigators
NCT00526474
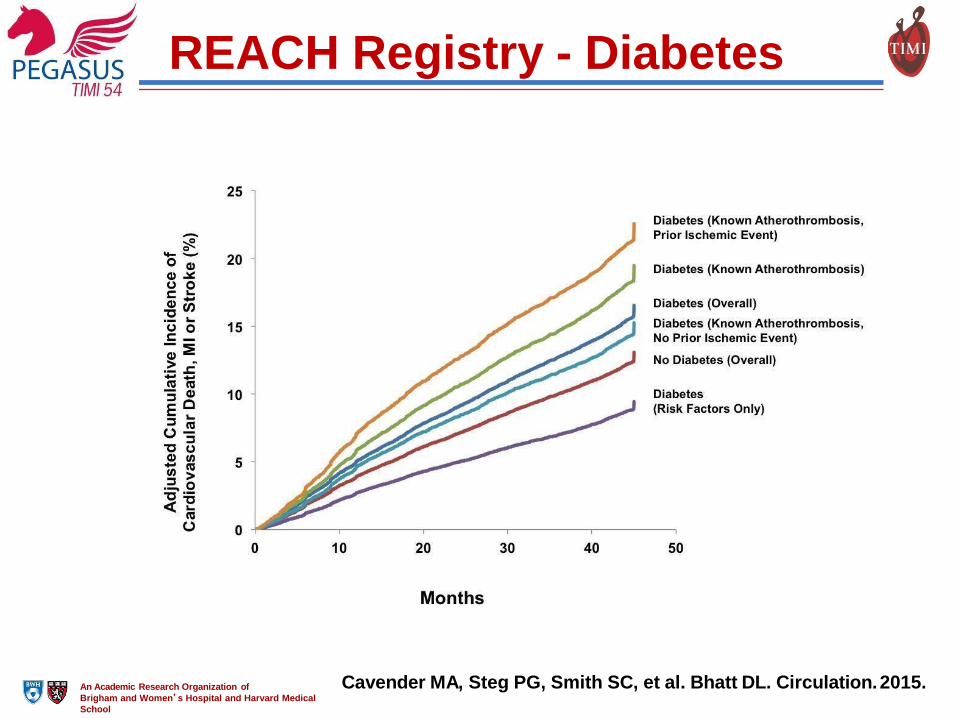
REACH Registry - Diabetes
Cavender MA, Steg PG, Smith SC, et al. Bhatt DL. Circulation. 2015. An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School

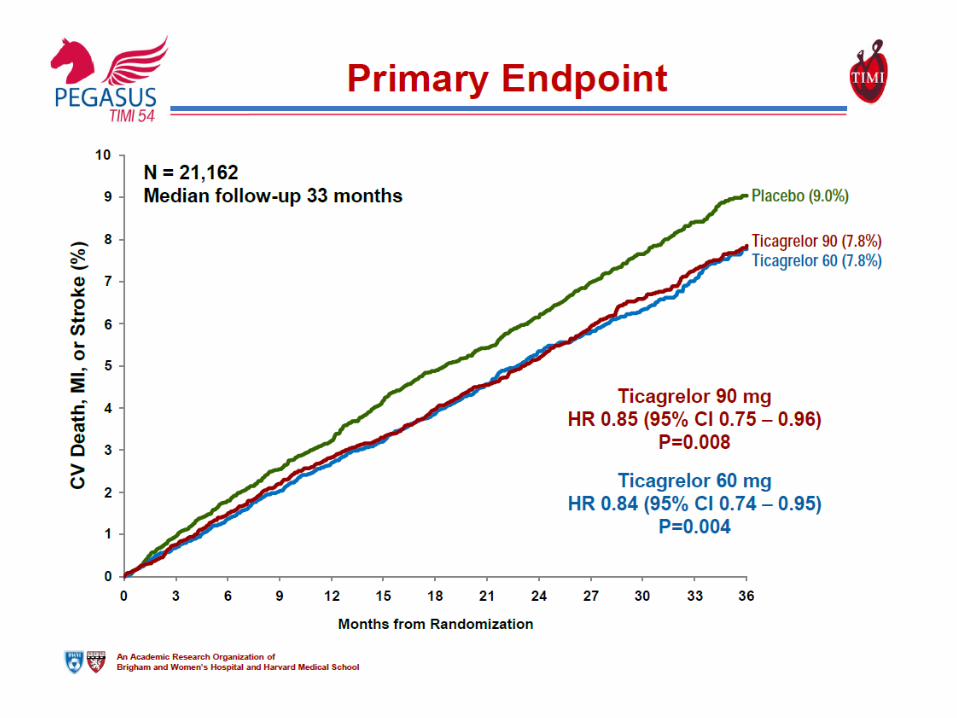
Primary Endpoint - MACE C
V D
eath
, M
I, S
tro
ke
(%
) 11.6%
10.1%
7.8%
6.7%
Benefit in Diabetic vs. Non-Diabetic Patients:
Interaction P=0.99
Ticagrelor in Non-Diabetic Patients
HR 0.84 (95% CI 0.74 – 0.96)
ARR 1.1%; P=0.01
Ticagrelor in Diabetic Patients
HR 0.84 (95% CI 0.72 – 0.99)
ARR 1.5%; P=0.03
Ticagrelor (doses pooled)
Placebo
Days from Randomization An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School
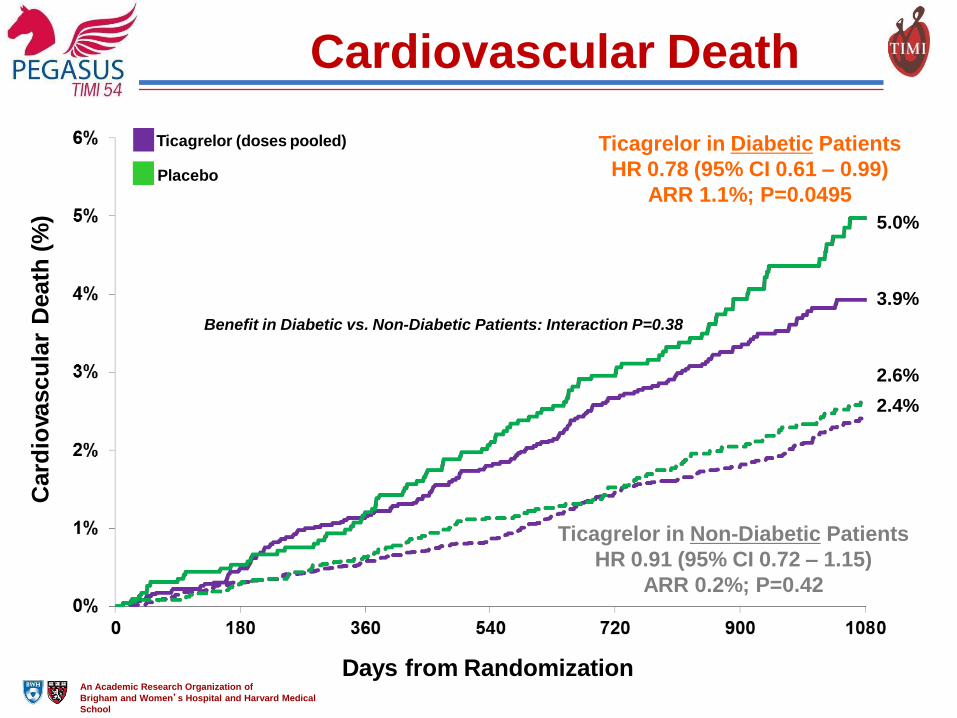
Cardiovascular Death C
ard
iovasc
ula
r D
eath
(%
)
3.9%
Benefit in Diabetic vs. Non-Diabetic Patients: Interaction P=0.38
2.6%
2.4%
Ticagrelor in Non-Diabetic Patients
HR 0.91 (95% CI 0.72 – 1.15)
ARR 0.2%; P=0.42
Ticagrelor in Diabetic Patients
HR 0.78 (95% CI 0.61 – 0.99)
ARR 1.1%; P=0.0495
5.0%
Ticagrelor (doses pooled)
Placebo
Days from Randomization An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School

Efficacy and Safety of Ticagrelor as Long-Term
Secondary Prevention in Patients with Peripheral
Artery Disease and Prior Myocardial Infarction
Marc P. Bonaca, MD, MPH
on behalf of the PEGASUS-TIMI 54 Executive &
Steering Committees and Investigators
NCT00526474
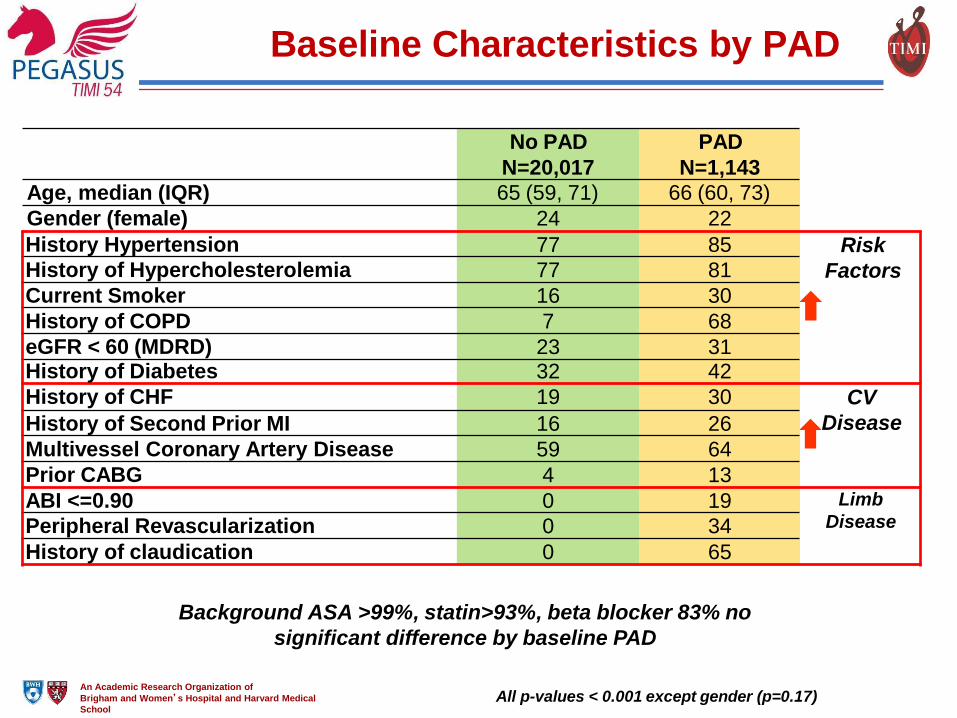
Baseline Characteristics by PAD
An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School All p-values < 0.001 except gender (p=0.17)
Background ASA >99%, statin>93%, beta blocker 83% no
significant difference by baseline PAD
No PAD
N=20,017
PAD
N=1,143
Age, median (IQR) 65 (59, 71) 66 (60, 73)
Gender (female) 24 22
History Hypertension 77 85 Risk
Factors History of Hypercholesterolemia 77 81
Current Smoker 16 30
History of COPD 7 68
eGFR < 60 (MDRD) 23 31 History of Diabetes 32 42
History of CHF 19 30 CV
Disease History of Second Prior MI 16 26
Multivessel Coronary Artery Disease 59 64
Prior CABG 4 13
ABI <=0.90 0 19 Limb
Disease Peripheral Revascularization 0 34
History of claudication 0 65
0 %
0
5%
10%
15%
20%
25%
90 180 270 360 450 540 630 720 810 900 990 108
CV
Death
, M
I, o
r S
tro
ke
(%
)
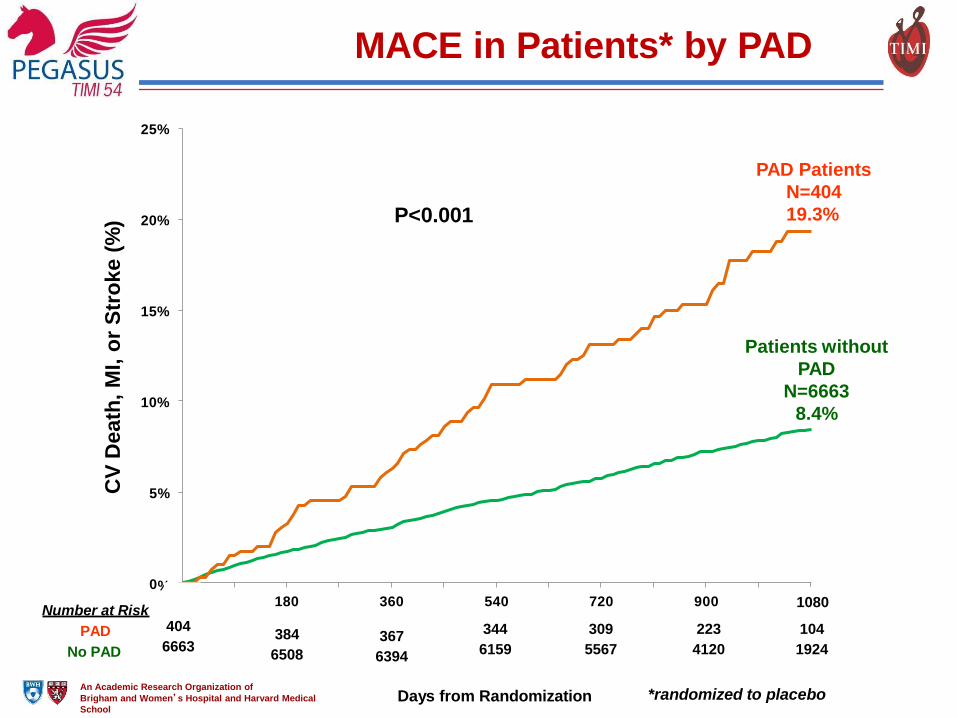
PAD Patients
N=404
19.3%
Patients without
PAD
N=6663
8.4%
Number at Risk
PAD
No PAD
404
6663 384
6508
367
6394
P<0.001
MACE in Patients* by PAD
1080
An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School
*randomized to placebo Days from Randomization
344 309 223 104
6159 5567 4120 1924
An Academic Research Organization of
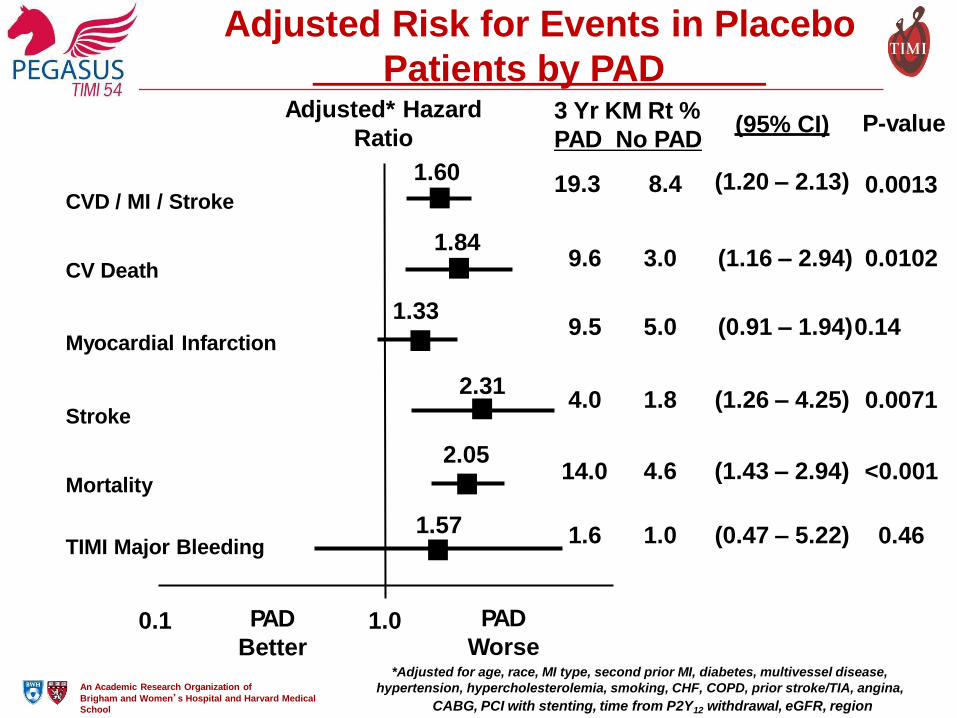
1.0 0.1 PAD
Better
PAD
Worse
1.84
1.33
2.31
2.05
1.57
CVD / MI / Stroke
CV Death
Myocardial Infarction
Stroke
Mortality
TIMI Major Bleeding
0.0013 (1.20 – 2.13)
Adjusted* Hazard
Ratio
1.60
Brigham and Women’s Hospital and Harvard Medical
School CABG, PCI with stenting, time from P2Y12 withdrawal, eGFR, region
3 Yr KM Rt %
PAD No PAD
19.3 8.4
(95% CI) P-value
9.6 3.0 (1.16 – 2.94) 0.0102
9.5 5.0 (0.91 – 1.94) 0.14
0.0071 4.0 1.8 (1.26 – 4.25)
<0.001 4.6 (1.43 – 2.94) 14.0
0.46 1.6 1.0 (0.47 – 5.22)
*Adjusted for age, race, MI type, second prior MI, diabetes, multivessel disease,
hypertension, hypercholesterolemia, smoking, CHF, COPD, prior stroke/TIA, angina,
Adjusted Risk for Events in Placebo
Patients by PAD

An Academic Research Organization of
CV
Death
, M
I, o
r S
tro
ke
(%
)
Days from Randomization
0%
5%
10%
15%
20%
25%
0 90 180 270 360 450 540 630 720 810 900 990 1080
19.3%
15.2%
8.4%
7.4%
PAD
HR 0.75 95% (CI 0.55 – 1.01)
ARR 4.1%
NNT 25
No PAD HR
0.86 95% (CI 0.77 –
0.96)
P-interaction 0.41 Placebo
Ticagrelor
(pooled doses)
ARR 1.0%
NNT 100
MACE with Ticagrelor by PAD at Baseline
Brigham and Women’s Hospital and Harvard Medical
School

Ac
ute
Lim
b I
sch
em
ia o
r
Pe
rip
hera
l R
evascu
lari
za
tio
n f
or
Isch
em
ia (
%)
0.0%
Number at Risk
0.2%
0.8%
0.71%
0.6%
0.46%
0.4%
1.0%
0 180
6988
13929 An Academic Research Organization of
Brigham and Women’s Hospital and Harvard Medical
School Days from Randomization
360
6912
13789
540
6701
13425
720
6077
12186
900
4518
9154
1080
2123
4296
HR 0.65
95% CI (0.44 – 0.95)
P=0.026
Placebo Ticagrelor
7067
14095
Major Adverse Limb Events with Ticagrelor