Embed Size (px)
Citation preview
5/27/2015
1
Updates In Direct DentistryPart 2 Montreal Program
Lou Graham DDS University Dental Professionals
Catapult Group [email protected]
5/27/2015
2
Age/Health related dentistryConservative/Tooth preserving ideologyA periodontal/restorative approach with state of the art periodontal therapiesHygiene based growthDiagnostic tools that enable my team to follow the philosophyPrevention at every age

5/27/2015
3
Imagine your hygienist looking at:OcclusionMobilityFremitusUsing articulating paperTooth SleuthsWith Loupes (mandatory)CariVuSpectraDigital x-rays
Either 50 or 60 minutes routinely….building Value
Build Relationship
Establish Credibility
Clinical Screenings
Share Findings
Dr. Exam
Oral Hygiene
Instrumentation
Create Value
Hand-Off
Op Break Down
The key is allowing the hygienist enough time to be a total oral care provider
Build Relationship
Establish Credibility
Clinical Screenings
Share Findings
Dr. Exam
Oral Hygiene
Instrumentation
Create Value
Hand-Off
Op Break Down
30 minutes max
5/27/2015
4
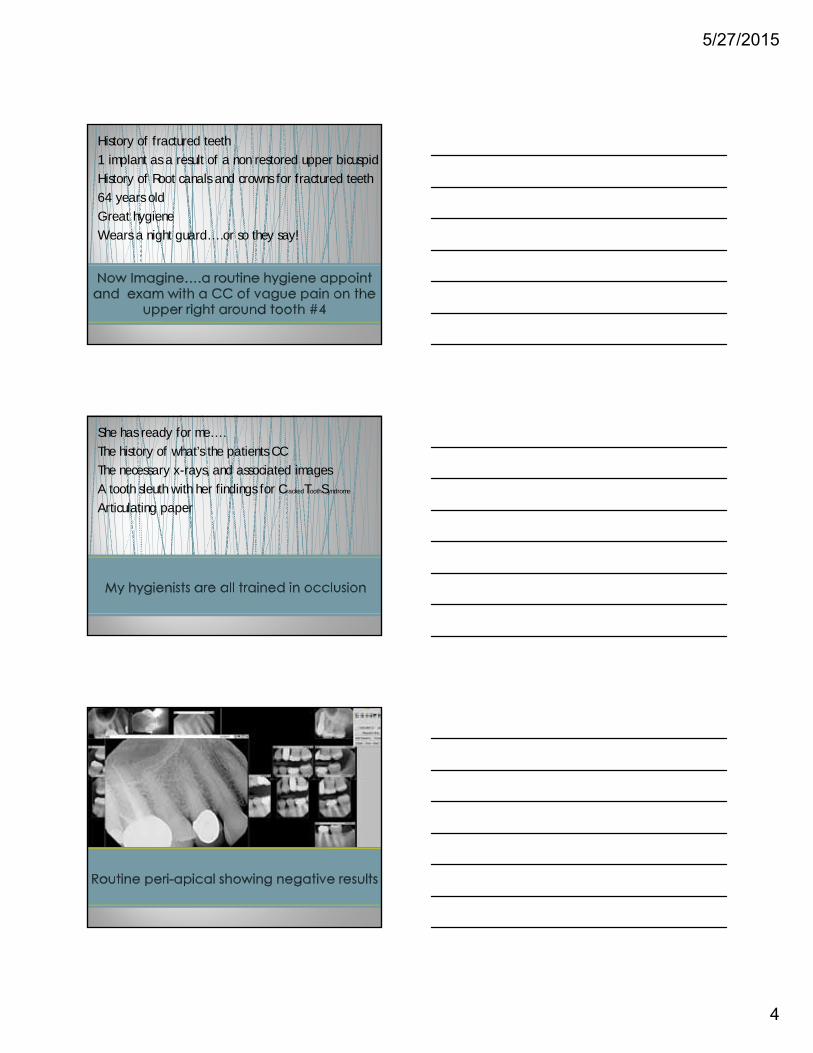
History of fractured teeth
1 implant as a result of a non restored upper bicuspid
History of Root canals and crowns for fractured teeth
64 years old
Great hygiene
Wears a night guard….or so they say!
She has ready for me….
The history of what’s the patients CC
The necessary x-rays, and associated images
A tooth sleuth with her findings for CrackedToothSyndrome
Articulating paper
5/27/2015
5
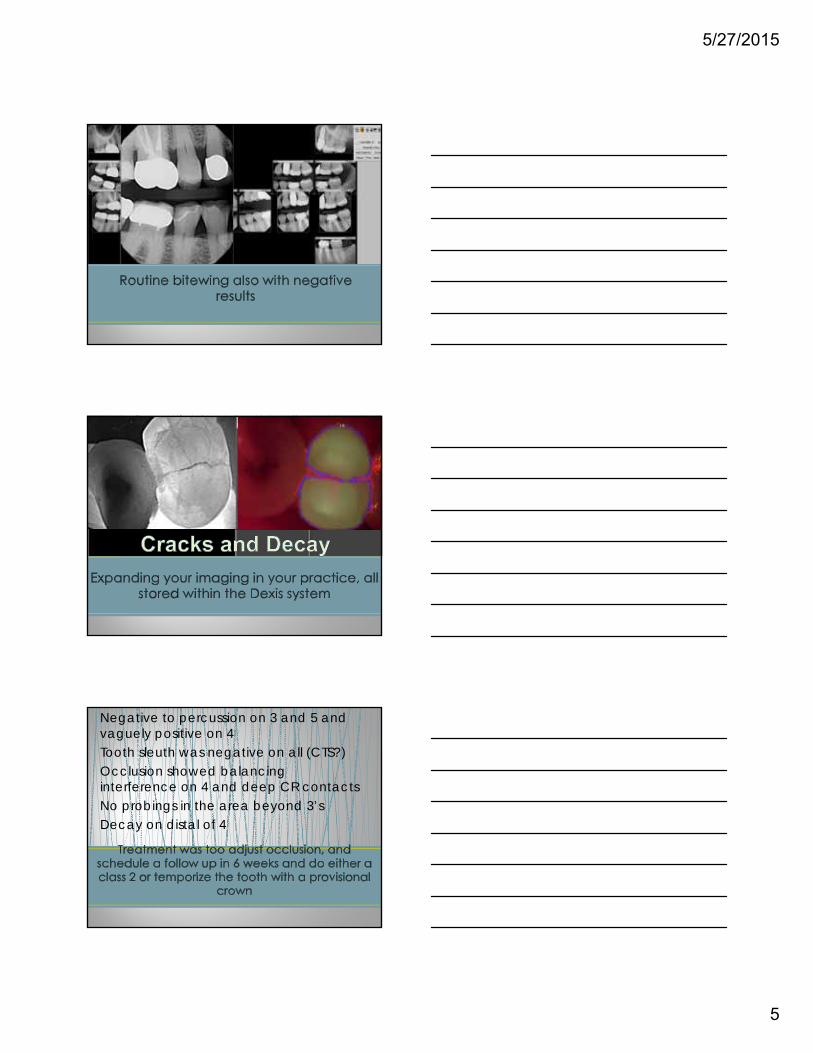
Negative to percussion on 3 and 5 and vaguely positive on 4Tooth sleuth was negative on all (CTS?)Occlusion showed balancing interference on 4 and deep CR contactsNo probings in the area beyond 3’sDecay on distal of 4

5/27/2015
6
Tell me, and I will forget.
Show me, and I will remember.
Involve me, and I will understand.
5/27/2015
7
Intra Oral Camera Digital X-ray TransilluminationFluorescence
A study of the United States Department of Labor showed that 83% of all human learning is done
visually whereas only 11% is done through hearing.
5/27/2015
8
It was found that people retain over 6 times more information when it is presented visually compared
to just verbally
A study conducted by the
Wharton School of Business on the subject of Sales Presentation
revealed that audiences found visual presentations about
70% more persuasive.
It has been suggested that the majority of all plans that go untreated are a direct result of the patient’s lack of
understanding.
5/27/2015
9
3 Air Techniques Polaris intra oral camera and 3 Spectra Fluorescence
Dexis Digital…replaced my last system that was 6 years old and now 2 Dexis CariVu
Shofu’s new digital camera, Eye Special 2…easiest and best in my hands yet to date, replaced Canon 20D and Canon 11G
Velscope and 1 NOMAD
5/27/2015
10
Traditional Decay ModelTraditional Decay Model
Caries attack begins in the enamel with demineralization and cavitation. Easily diagnosed
visually, sharp explorer and radiographs.
5/27/2015
11
New Model for DecayNew Model for Decay
Enamel does not cavitate because of protection from fluoride. Caries begins in dentin through fissures, pits, fractures, and enamel pores. Difficult to diagnose with
traditional methods.
The role of genetics?
30- 35 %
5/27/2015
12
Multi- factorial disease
Genetics, diet, medication, oral hygiene, stress
Many strains of bacteria (over 40) contribute to the disease.
Bacterial theory is changing!
Trends Micrl. Solving the etiology of dental caries.Simón-Soro A1, Mira A2.Author information
Abstract
For decades, the sugar-fermenting, acidogenic species Streptococcus mutans has been considered the main causative agent of dental caries and most diagnostic and therapeutic strategies have been targeted toward this microorganism. However, recent DNA- and RNA-based studies from carious lesions have uncovered an extraordinarily diverse ecosystem where S. mutans accounts only a tiny fraction of the bacterial community.
5/27/2015
13
PLoS One. 2012;7(10):e47722. doi: 10.1371/journal.pone.0047722. Epub 2012 Oct 16.
Beyond Streptococcus mutans: dental caries onset linked to multiple species by 16S rRNA community analysis.
Gross EL1, Beall CJ, Kutsch SR, Firestone ND
Streptococcus mutans was the dominant species in many, but not all, subjects with caries. Elevated levels of S. salivarius, S. sobrinus, and S. parasanguinis were also associated with caries, especially in subjects with no or low levels of S. mutans, suggesting these species are alternative pathogens, and that multiple species may need to be
targeted for interventions. Veillonella, which metabolizes lactate, was associated with caries and was highly correlated with total acid producing species.
This study evaluated 1341 lesions that were described as:• Having roughness• Surface opacity
• Not detectable on x-ray
• No cavitation
• Staining
5/27/2015
14
The study concluded:
For questionable lesions the recommended course of action was simple follow up. This is the same model in Scandinavia where they follow non cavitated lesions with no visible evidence on x-ray
An explorer….a probe….traditional x-rays
5/27/2015
15
Transference of infective S mutans to other sites?
52% sensitivity / low reliability
False positives & false negatives
Disrupts intact surface layer, eliminating potential for reversal
Loesche et al, J Dent Res 1979Hujoel et al, Caries Res 1995
Lussi, Caries Res 1991
Al-Sehaibany showed tug back by an explorer was only 24% diagnostic, meaning that 76% of the time that tug back was present, there was no caries!
Ekstrand showed that a sharp explorer tip can damage an early de-mineralized white spot lesion of the enamel by cavitating the surface
.
5/27/2015
16
40-60% demineralization required to produce an image to evaluate
Underestimate size or depth
Insufficient to determine activity level
Low sensitivity39% occlusal50% interproximal
Bader et al 2001
Visual diagnosis can be highly subjective, Kefley and Holt 1993
Treat or NO Treatment
5/27/2015
17
Francescut and Lussi found that with brown or black stains in fissures were
NOT a good indication to drill because 57% of these lesions
exhibited no caries or caries limited to the outer enamel……..so what about
the other 43%?
Steiner and colleagues (1998)found the dark brown and black stains to have the
highest incidence of caries into dentin and concluded there were no clear
guidelines as to management
Lesions with with light brown or yellow stains had 42% demineralization into the middle 1/3 of dentin
Lesions with an opaquelook had 27% caries into the same 1/3 of dentin
5/27/2015
18
About 2/3rds advocate surgical treatment once the dentin has reached the outer dentin 1/3rd (D1) and with the aid of an x-ray (yet Low Sensitivity)
The remainder teach treatment when decay is in the inner enamel (E2)
In Florida, doctors who are graduates from all around the US do the following: 60% treat E2 lesions and 40% treat D1
5/27/2015
19
How many times have you gone into a class 1 and thought it was shallow and “BOOM” your bur just
drops into a large cavity?
Or
Another example, you are removing an alloy or a composite in a class 1 and you see “Brown” as you
are approaching the interproximal?

5/27/2015
20
120° Tactile Switch Control
SpectraBlue LEDs
PolarisWhite LEDs
Ultrasonically Welded & Sealed Switch Bezels
USB Cable assembly
Centrally Located Controls
5/27/2015
21
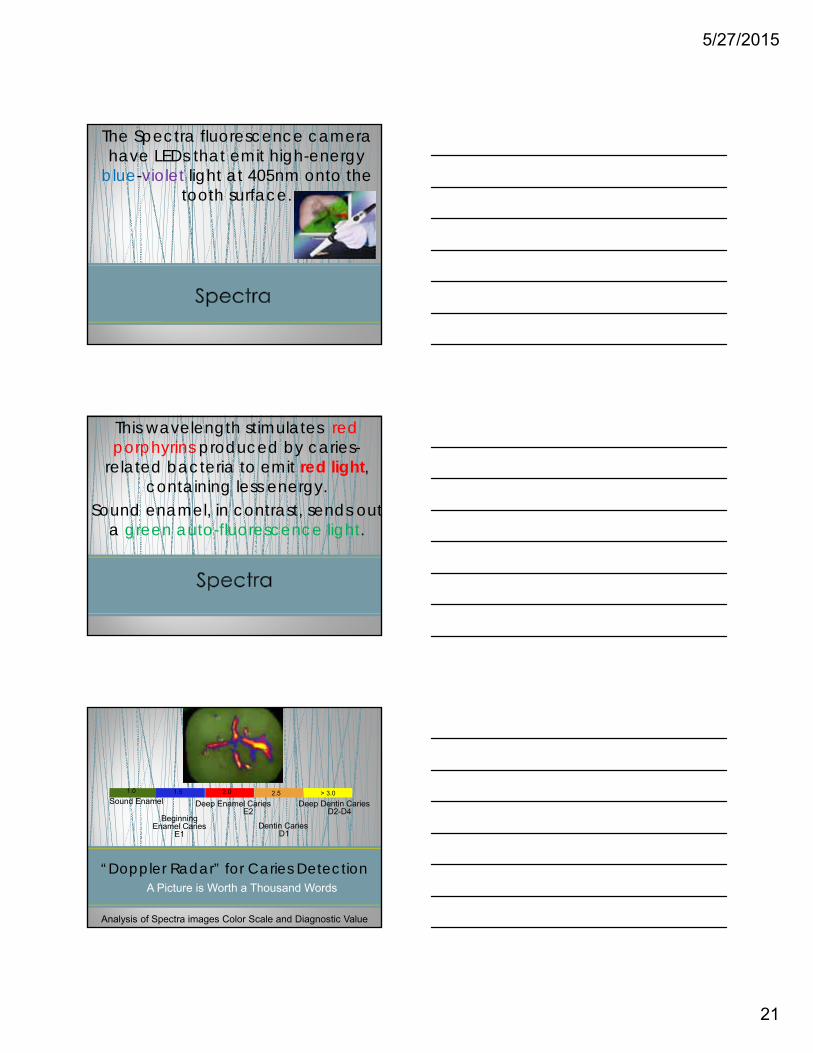
The Spectra fluorescence camera have LEDs that emit high-energy
blue-violet light at 405nm onto the tooth surface.
This wavelength stimulates red porphyrins produced by caries-
related bacteria to emit red light, containing less energy.
Sound enamel, in contrast, sends outa green auto-fluorescence light.
“Doppler Radar” for Caries Detection
Analysis of Spectra images Color Scale and Diagnostic Value
BeginningEnamel Caries
E1
Deep Enamel CariesE2
Dentin CariesD1
Deep Dentin CariesD2-D4
Sound Enamel1.5 2.0 2.51.0 > 3.0
A Picture is Worth a Thousand Words
5/27/2015
22
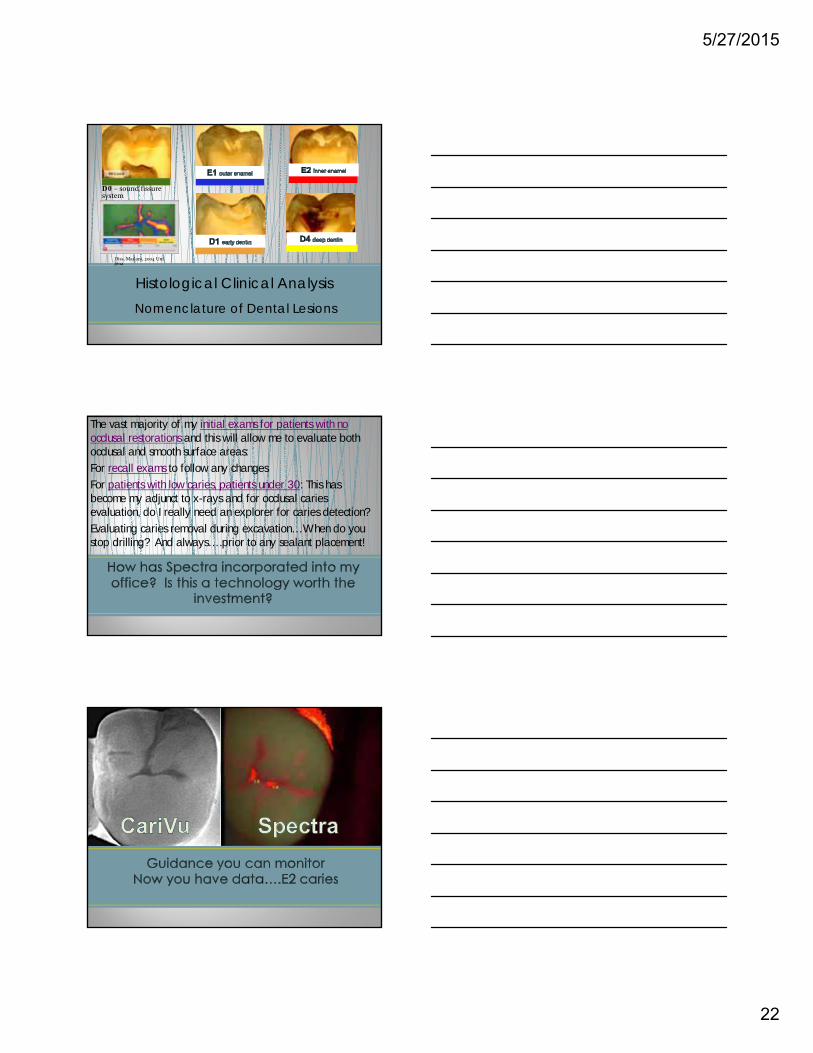
Histological Clinical Analysis
Diss. Madani, 2004 Uni Jena
D0 – sound fissuresystem
Nomenclature of Dental Lesions
The vast majority of my initial exams for patients with no occlusal restorations and this will allow me to evaluate both occlusal and smooth surface areas:
For recall exams to follow any changes
For patients with low caries, patients under 30: This has become my adjunct to x-rays and for occlusal caries evaluation, do I really need an explorer for caries detection?
Evaluating caries removal during excavation…When do you stop drilling? And always….prior to any sealant placement!
5/27/2015
23
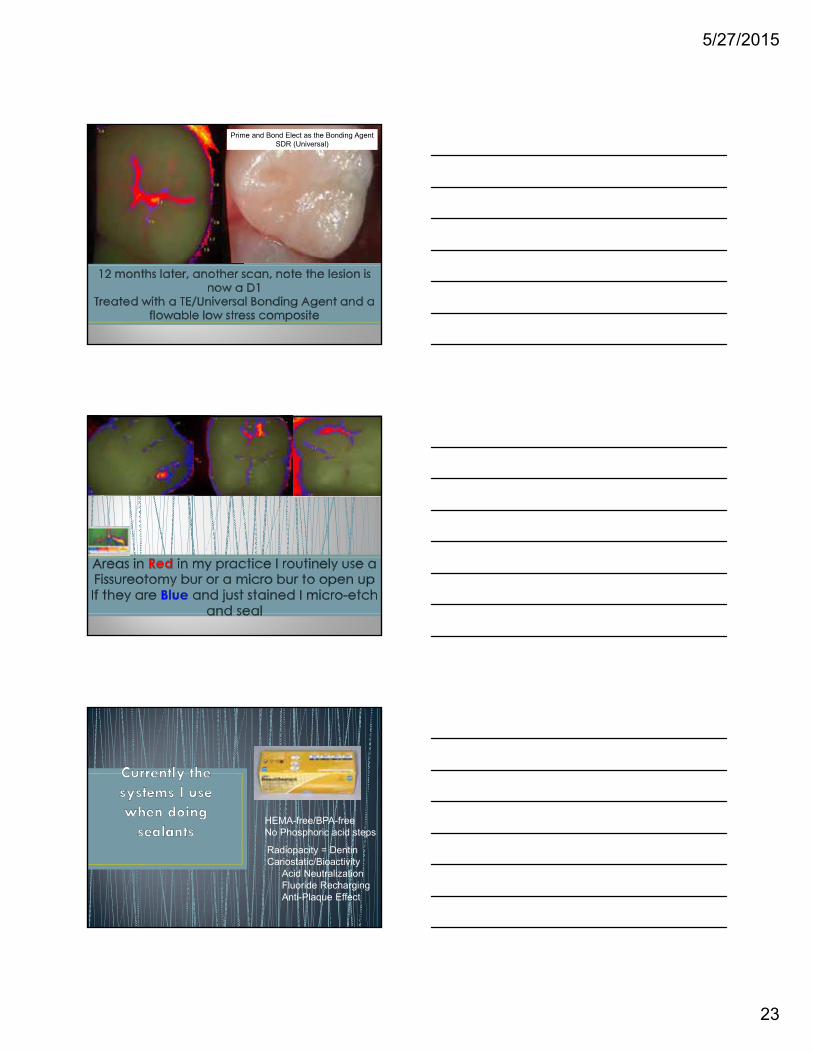
Prime and Bond Elect as the Bonding AgentSDR (Universal)
15 Distal Occlusal Pit 31 Occlusal 18 Occlusal
HEMA-free/BPA-free No Phosphoric acid steps
Radiopacity = DentinCariostatic/Bioactivity
Acid NeutralizationFluoride RechargingAnti-Plaque Effect
5/27/2015
24
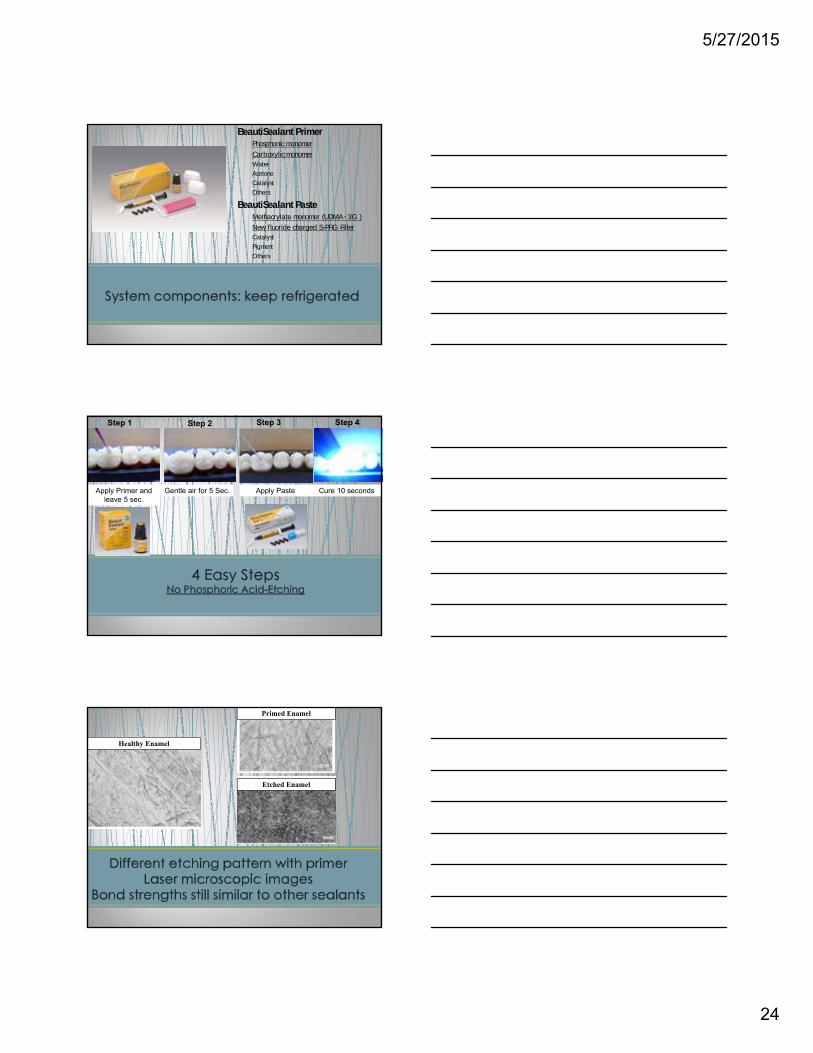
BeautiSealant PrimerPhosphonic monomer
Carboxylic monomerWater
Acetone
Catalyst
Others
BeautiSealant PasteMethacrylate monomer (UDMA、3G )
New fluoride charged S-PRG FillerCatalyst
Pigment
Others
Apply Primer and leave 5 sec.
Gentle air for 5 Sec. Apply Paste
Step 1 Step 2 Step 3 Step 4
Cure 10 seconds
Primed Enamel
Healthy Enamel
Etched Enamel
5/27/2015
25
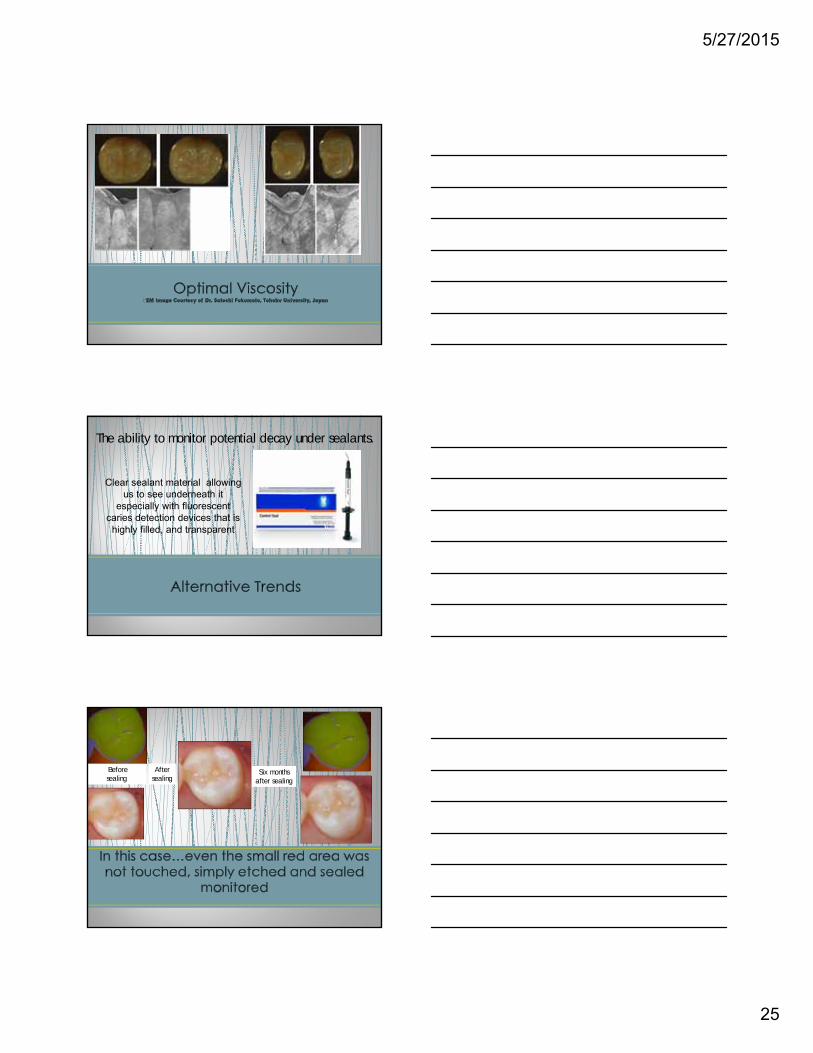
The ability to monitor potential decay under sealants.
Clear sealant material allowing us to see underneath it
especially with fluorescent caries detection devices that is
highly filled, and transparent
Before sealing
After sealing
Six months after sealing
5/27/2015
26
Infared light…no radiation
Enamel appears transparent or light
Porous lesions appear darker by trapping and absorbing the light: these include cracks and caries
Video capture….live scans
Stored in Dexis, excellent for communication to patient and yes…to insurance companies
For Identifying decay pre-treatment, early lesions on smooth, occlusal, and proximal surfaces
For Identifying decay during treatment
For Identifying cracks, and to a certain level, the severity of the cracks
For monitoring lesions and saving within the software
5/27/2015
27
The vast majority of my initial exams for patients who do not have class 2 restorations: Utilized to compliment or substitute for x-rays for evaluation of class 2 lesions, evaluate older restorations for peripheral decay, evaluate for cracks, documentation.
For recall exams same as above
For patients with low caries, patients under 30: This has become my adjunct or replacement of x-rays and for those under 16, do I really need bite wings? In our practice, we use CariVu for these patients and a low dose panorex? Maybe alternate with bite wings?
5/27/2015
28
D0425If used instead of bite-wings our fee is $61
If used instead of one bite-wing our fee is
$32 which is our fee today for 1 periapicalor bite-wing
5/27/2015
29
33 year old mom of two
Low caries rate, or so we thought
Uses floss at Christmas for ornaments
Twice a year hygiene visits
Small breaking down class 1 restorations
Asymptomatic
5/27/2015
30
5/27/2015
31
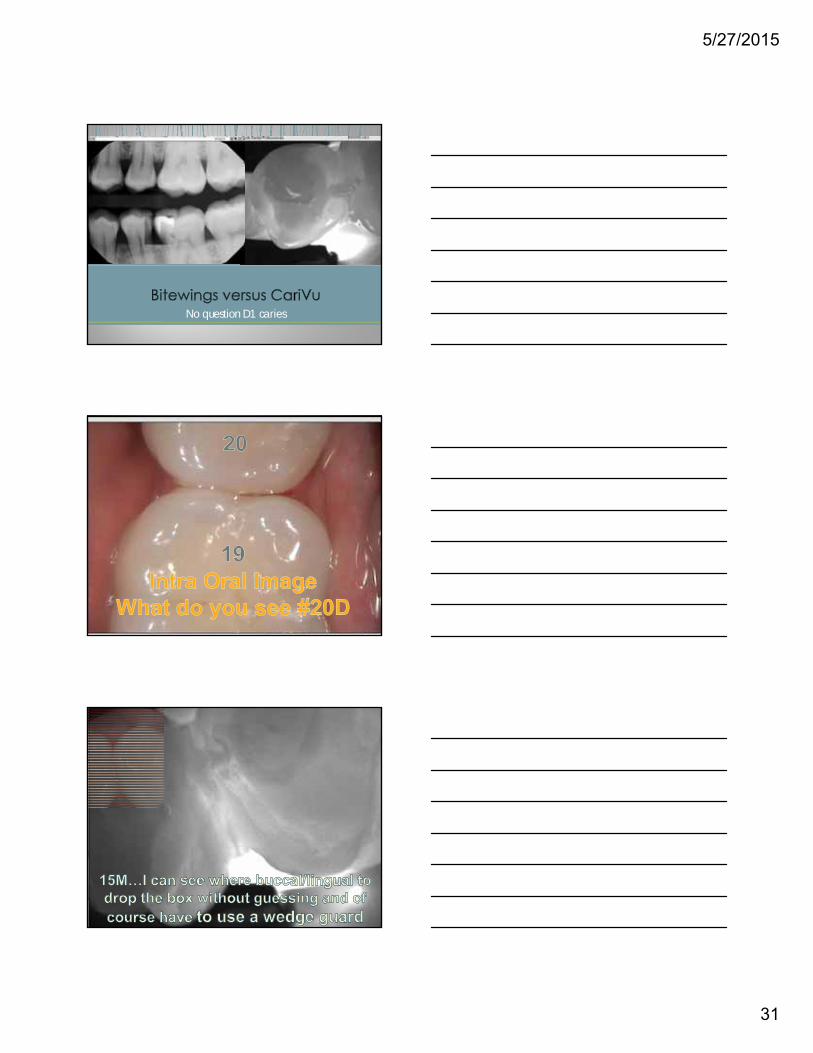
No question D1 caries
5/27/2015
32
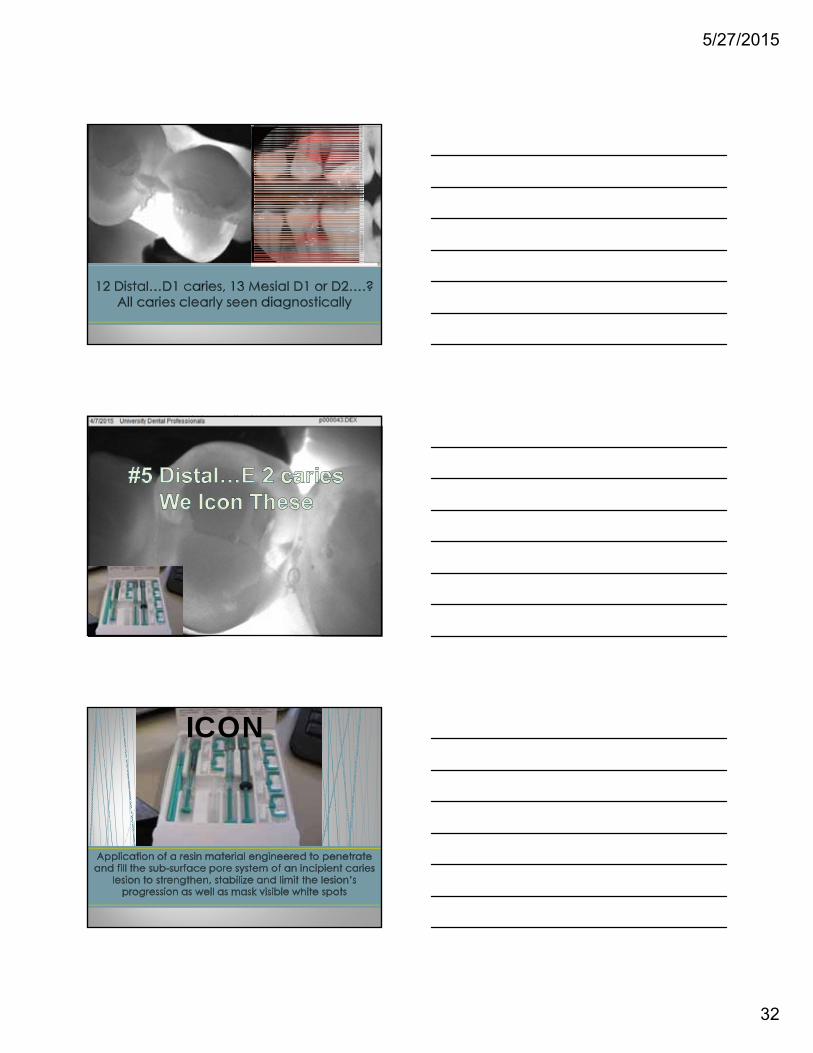
ICON
5/27/2015
33
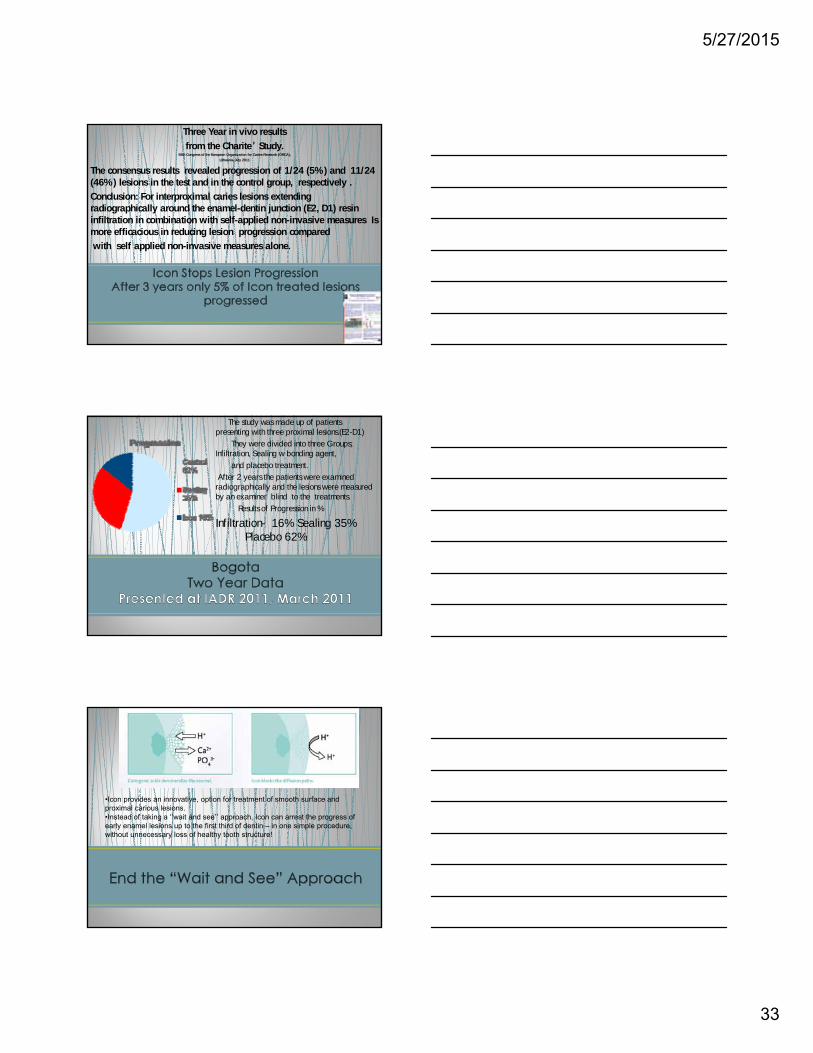
Three Year in vivo results
from the Charite’ Study.58th Congress of the European Organization for Caries Research (ORCA),
Lithuania July 2011
The consensus results revealed progression of 1/24 (5%) and 11/24 (46%) lesions in the test and in the control group, respectively .
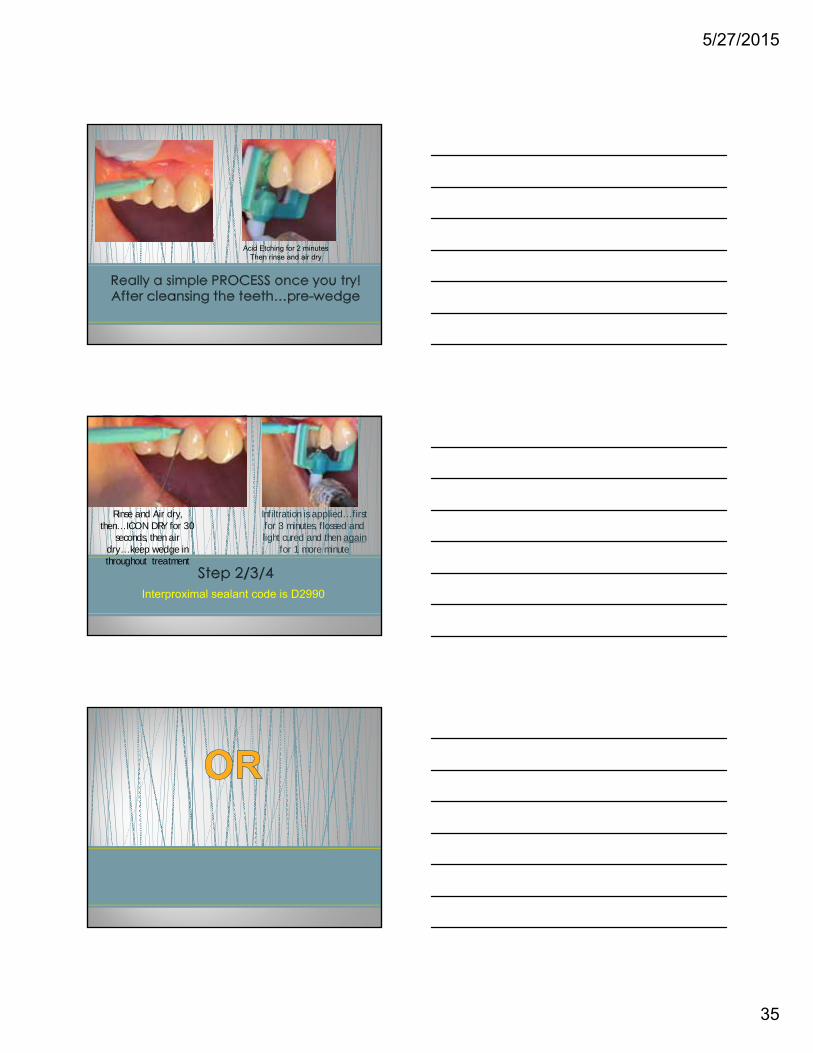
Conclusion: For interproximal caries lesions extending radiographically around the enamel-dentin junction (E2, D1) resin infiltration in combination with self-applied non-invasive measures Is more efficacious in reducing lesion progression compared
with self applied non-invasive measures alone.
The study was made up of patients presenting with three proximal lesions.(E2-D1)
They were divided into three Groups; Infiltration, Sealing w bonding agent,
and placebo treatment.
After 2 years the patients were examined radiographically and the lesions were measured by an examiner blind to the treatments.
Results of Progression in %
Infiltration- 16% Sealing 35% Placebo 62%
•Icon provides an innovative, option for treatment of smooth surface and proximal carious lesions.•Instead of taking a “wait and see” approach, Icon can arrest the progress of early enamel lesions up to the first third of dentin – in one simple procedure, without unnecessary loss of healthy tooth structure!
5/27/2015
34
IS NOT radio-opaque due to the fact that the material would NOT infiltrate. The process takes about 20 minutes per tooth
Billing is 150-200$ and my pitch is…no drilling is best and we follow yearly on x-rays
47 research articles show far less caries after placement than NOT placing
Dam is highly recommended especially in lower posterior
If contacts are tight…orthodontic separator may be required prior to therapy
5/27/2015
35
Acid Etching for 2 minutesThen rinse and air dry
Rinse and Air dry, then…ICON DRY for 30
seconds, then air dry…keep wedge in throughout treatment
• Infiltration is applied…first for 3 minutes, flossed and light cured and then again
for 1 more minute
Interproximal sealant code is D2990
5/27/2015
36
5/27/2015
37