Embed Size (px)
Citation preview
Updates to the Management of Sepsis
and Septic ShockNeela Bhajandas, PharmD.Clinical Assistant Professor of Pharmacy PracticeTemple University School of PharmacyPSHP Annual Assembly 2017 Meeting
Disclosure StatementI have no conflicts of interest or financial
relationships to disclose.
ObjectivesPharmacist Objectives:Compare and contrast the notable
differences between the 2012 severe sepsis and 2016 sepsis and septic shock management guidelines.Describe the evidence-based pharmacologic
treatment options for sepsis and septic shock.Develop a treatment plan for the
management of a patient with septic shock.
ObjectivesPharmacy Technician Objectives:List the changes to the updated 2016 sepsis
and septic shock management guidelines.List the definitions of sepsis and septic
shock.Describe the Surviving Sepsis Campaign
Care Bundles.
Patient CaseRX is a 52 y/o male admitted to the emergency department (ED) with a 3 day history of fever, chills, cough, myalgia, and increased drowsiness and confusion. RX was recently admitted to an OSH, 2 weeks ago, for an acute exacerbation of COPD secondary to CAP. He is intubated in the ED for respiratory distress.
PMH: HTN, COPD, hyperlipidemiaMedications PTA: not immediately knownAllergies: NKDA
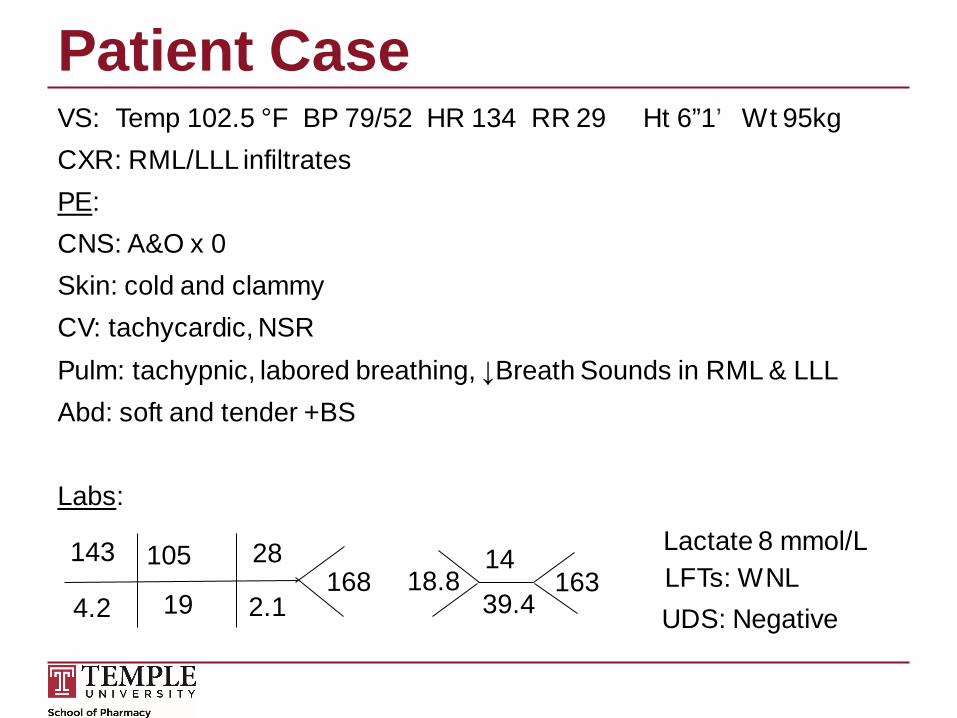
Patient CaseVS: Temp 102.5 °F BP 79/52 HR 134 RR 29 Ht 6”1’ Wt 95kg CXR: RML/LLL infiltrates PE: CNS: A&O x 0Skin: cold and clammyCV: tachycardic, NSRPulm: tachypnic, labored breathing, ↓Breath Sounds in RML & LLL Abd: soft and tender +BS
Labs:
16828
2.119
105
4.2
143 1439.4
18.8 163Lactate 8 mmol/L LFTs: WNLUDS: Negative
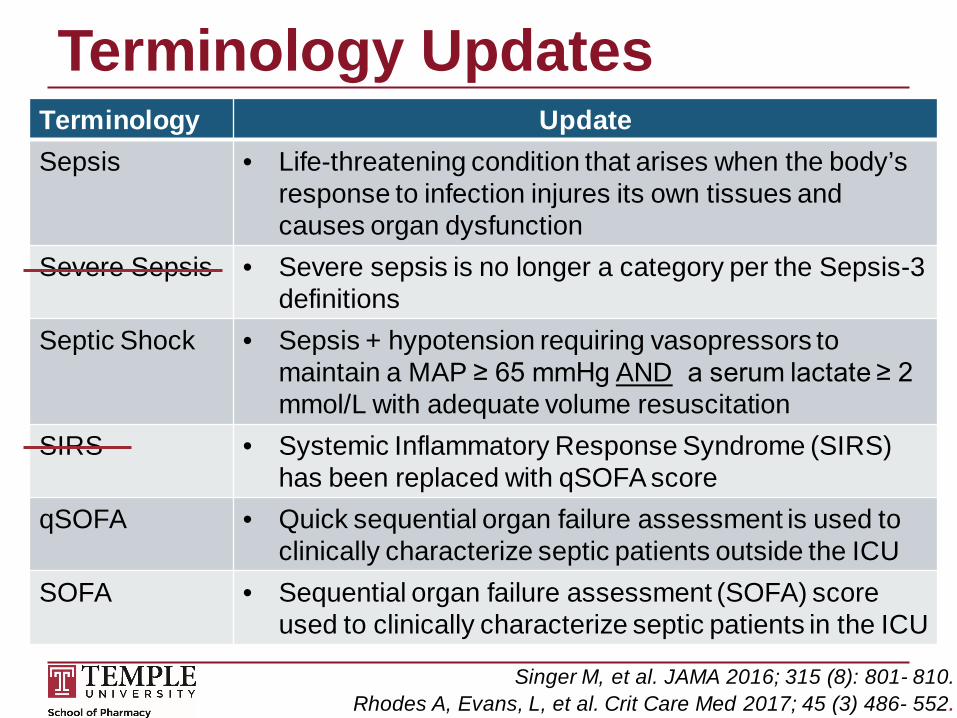
Terminology UpdatesTerminology UpdateSepsis • Life-threatening condition that arises when the body’s
response to infection injures its own tissues and causes organ dysfunction
Severe Sepsis • Severe sepsis is no longer a category per the Sepsis-3 definitions
Septic Shock • Sepsis + hypotension requiring vasopressors to maintain a MAP ≥ 65 mmHg AND a serum lactate ≥ 2 mmol/L with adequate volume resuscitation
SIRS • Systemic Inflammatory Response Syndrome (SIRS)has been replaced with qSOFA score
qSOFA • Quick sequential organ failure assessment is used to clinically characterize septic patients outside the ICU
SOFA • Sequential organ failure assessment (SOFA) scoreused to clinically characterize septic patients in the ICU
Singer M, et al. JAMA 2016; 315 (8): 801- 810. Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
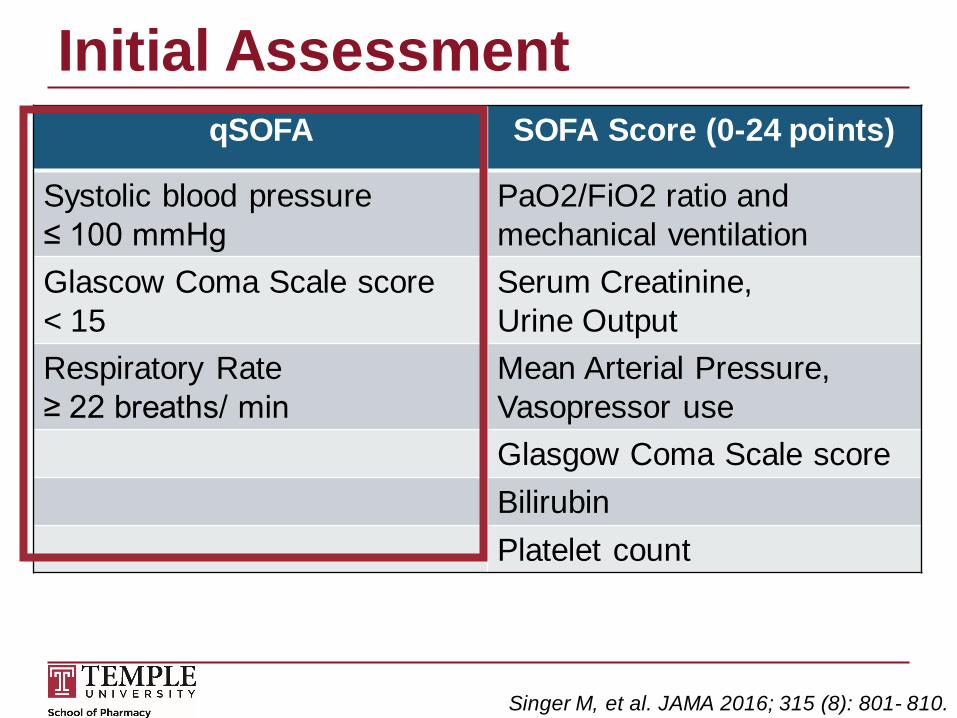
Initial AssessmentqSOFA SOFA Score (0-24 points)
Systolic blood pressure ≤ 100 mmHg
PaO2/FiO2 ratio and mechanical ventilation
Glascow Coma Scale score< 15
Serum Creatinine, Urine Output
Respiratory Rate ≥ 22 breaths/ min
Mean Arterial Pressure, Vasopressor useGlasgow Coma Scale scoreBilirubinPlatelet count
Singer M, et al. JAMA 2016; 315 (8): 801- 810.
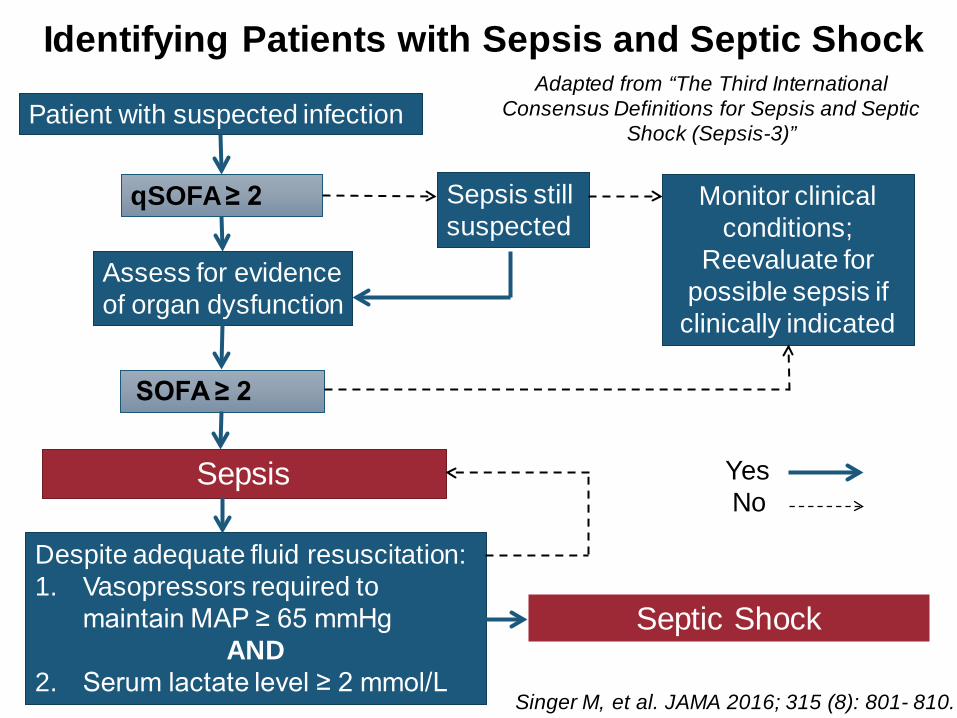
Patient with suspected infection
qSOFA≥ 2
Assess for evidence of organ dysfunction
SOFA ≥ 2
Sepsis
Despite adequate fluid resuscitation: 1. Vasopressors required to
maintain MAP ≥ 65 mmHgAND
2. Serum lactate level ≥ 2 mmol/L
Septic Shock
Sepsis still suspected
Monitor clinical conditions;
Reevaluate for possible sepsis if
clinically indicated
Identifying Patients with Sepsis and Septic Shock
Singer M, et al. JAMA 2016; 315 (8): 801- 810.
Yes No
Adapted from “The Third International Consensus Definitions for Sepsis and Septic
Shock (Sepsis-3)”
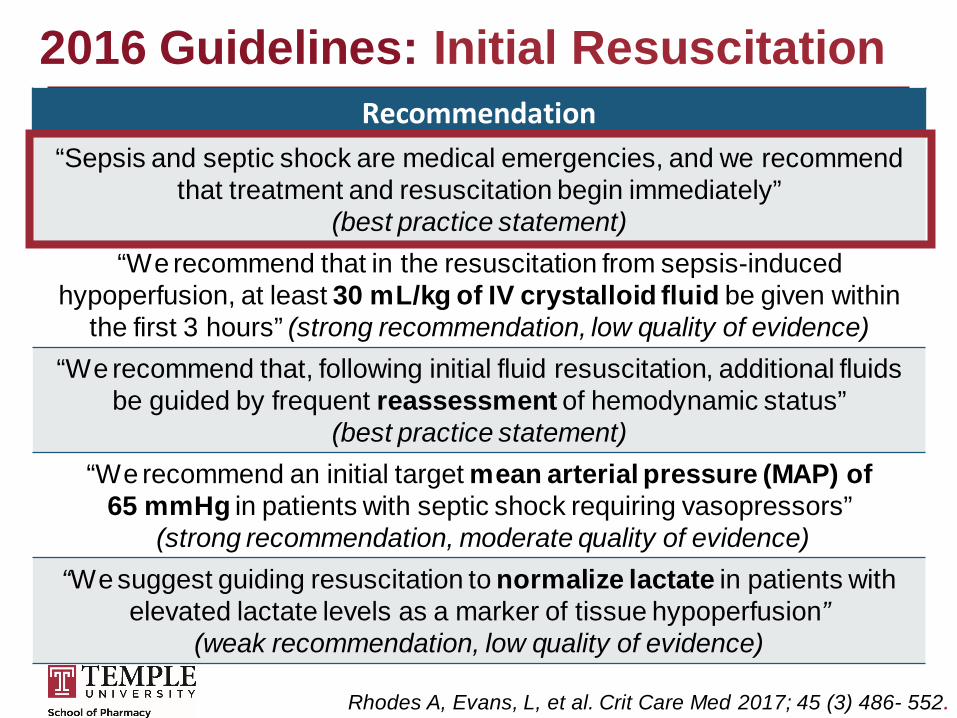
2016 Guidelines: Initial ResuscitationRecommendation
“Sepsis and septic shock are medical emergencies, and we recommend that treatment and resuscitation begin immediately”
(best practice statement)“We recommend that in the resuscitation from sepsis-induced
hypoperfusion, at least 30 mL/kg of IV crystalloid fluid be given within the first 3 hours” (strong recommendation, low quality of evidence)
“We recommend that, following initial fluid resuscitation, additional fluids be guided by frequent reassessment of hemodynamic status”
(best practice statement)“We recommend an initial target mean arterial pressure (MAP) of
65 mmHg in patients with septic shock requiring vasopressors”(strong recommendation, moderate quality of evidence)
“We suggest guiding resuscitation to normalize lactate in patients with elevated lactate levels as a marker of tissue hypoperfusion”
(weak recommendation, low quality of evidence)
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
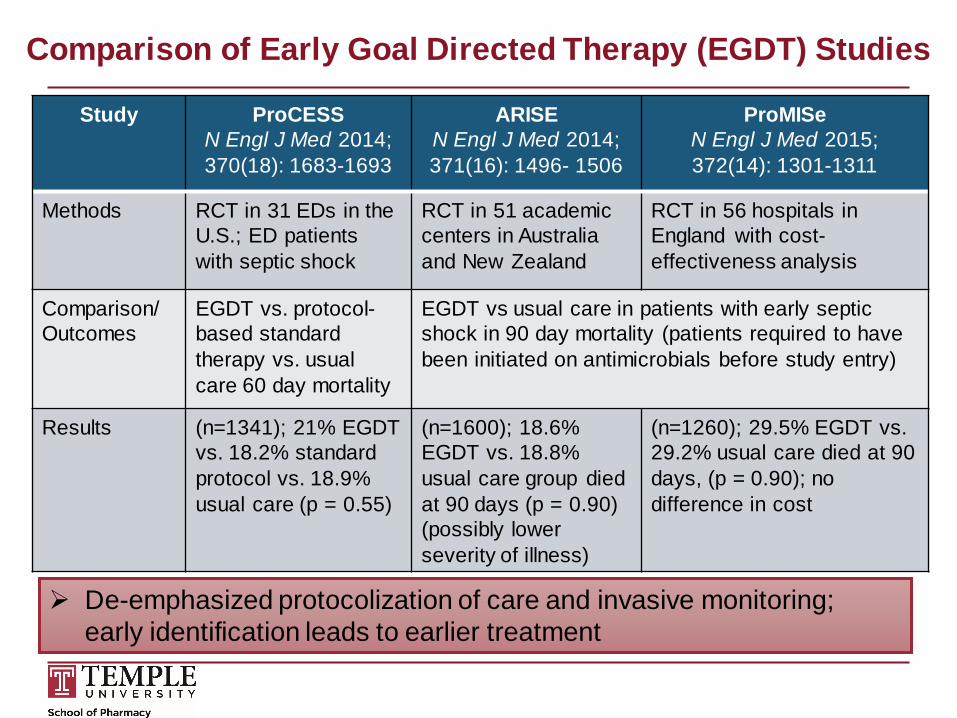
Comparison of Early Goal Directed Therapy (EGDT) Studies
Study ProCESSN Engl J Med 2014; 370(18): 1683-1693
ARISEN Engl J Med 2014; 371(16): 1496- 1506
ProMISeN Engl J Med 2015; 372(14): 1301-1311
Methods RCT in 31 EDs in the U.S.; ED patients with septic shock
RCT in 51 academic centers in Australia and New Zealand
RCT in 56 hospitals in England with cost-effectiveness analysis
Comparison/ Outcomes
EGDT vs. protocol-based standard therapy vs. usual care 60 day mortality
EGDT vs usual care in patients with early septic shock in 90 day mortality (patients required to have been initiated on antimicrobials before study entry)
Results (n=1341); 21% EGDT vs. 18.2% standard protocol vs. 18.9% usual care (p = 0.55)
(n=1600); 18.6% EGDT vs. 18.8% usual care group died at 90 days (p = 0.90) (possibly lower severity of illness)
(n=1260); 29.5% EGDT vs. 29.2% usual care died at 90 days, (p = 0.90); nodifference in cost
De-emphasized protocolization of care and invasive monitoring; early identification leads to earlier treatment
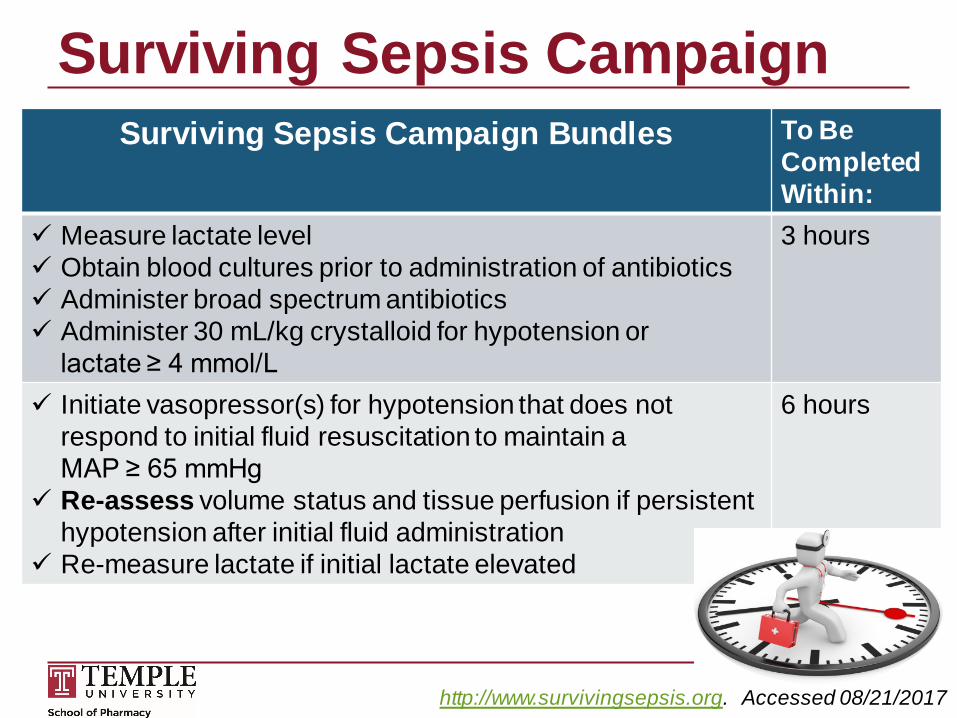
Surviving Sepsis CampaignSurviving Sepsis Campaign Bundles To Be
Completed Within:
Measure lactate level Obtain blood cultures prior to administration of antibiotics Administer broad spectrum antibiotics Administer 30 mL/kg crystalloid for hypotension or
lactate ≥ 4 mmol/L
3 hours
Initiate vasopressor(s) for hypotension that does not respond to initial fluid resuscitation to maintain a MAP ≥ 65 mmHg
Re-assess volume status and tissue perfusion if persistent hypotension after initial fluid administration
Re-measure lactate if initial lactate elevated
6 hours
http://www.survivingsepsis.org. Accessed 08/21/2017
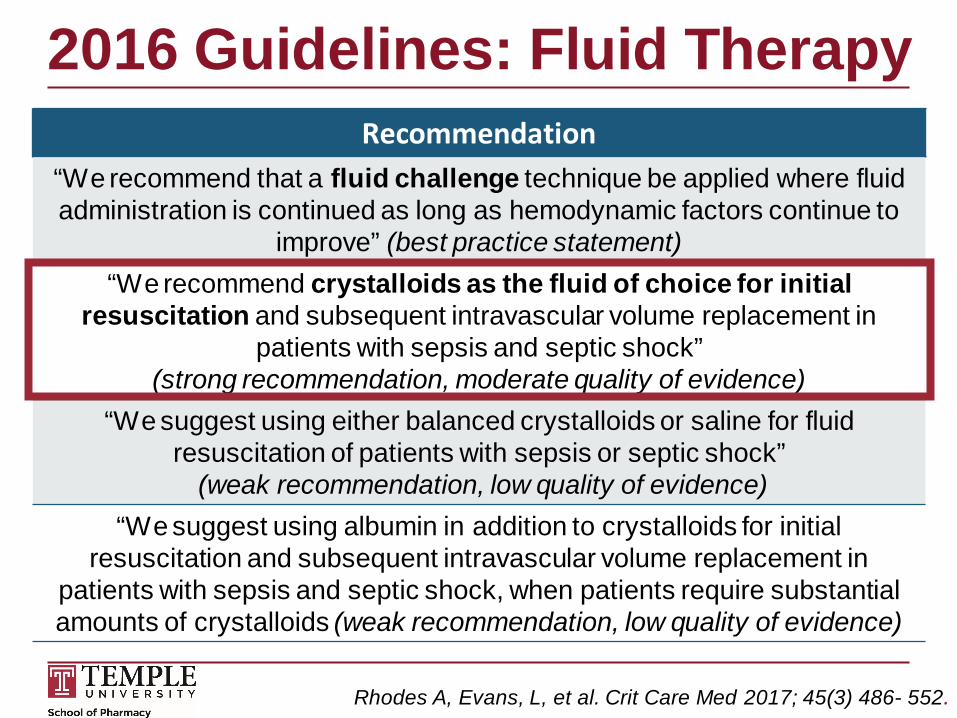
2016 Guidelines: Fluid TherapyRecommendation
“We recommend that a fluid challenge technique be applied where fluid administration is continued as long as hemodynamic factors continue to
improve” (best practice statement)“We recommend crystalloids as the fluid of choice for initial
resuscitation and subsequent intravascular volume replacement in patients with sepsis and septic shock”
(strong recommendation, moderate quality of evidence)“We suggest using either balanced crystalloids or saline for fluid
resuscitation of patients with sepsis or septic shock”(weak recommendation, low quality of evidence)
“We suggest using albumin in addition to crystalloids for initial resuscitation and subsequent intravascular volume replacement in
patients with sepsis and septic shock, when patients require substantial amounts of crystalloids (weak recommendation, low quality of evidence)
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45(3) 486- 552.
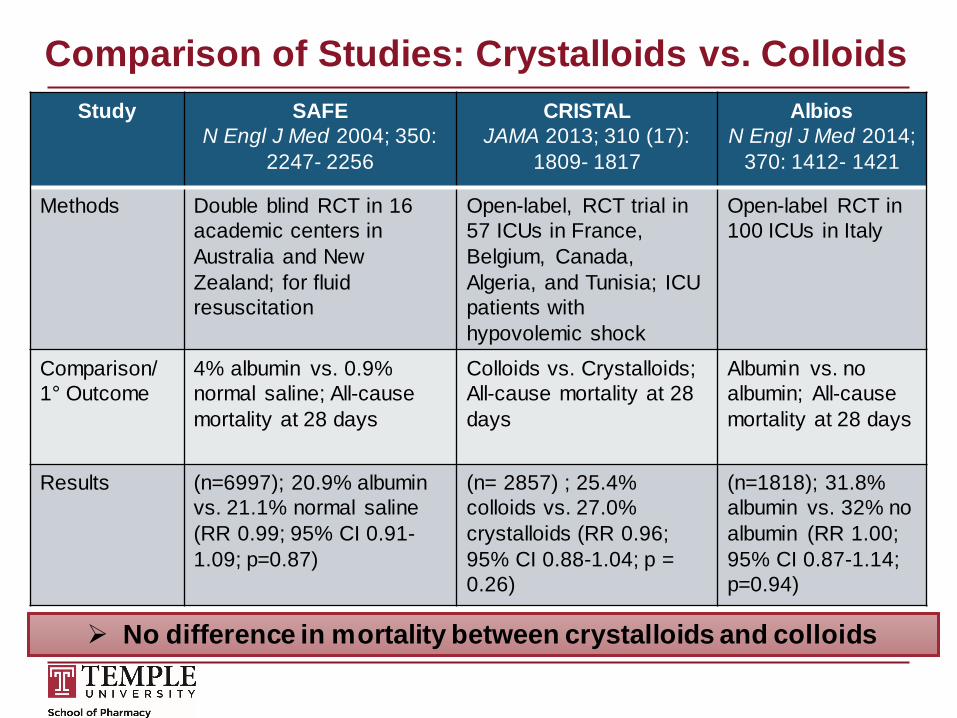
Comparison of Studies: Crystalloids vs. ColloidsStudy SAFE
N Engl J Med 2004; 350: 2247- 2256
CRISTAL JAMA 2013; 310 (17):
1809- 1817
AlbiosN Engl J Med 2014;
370: 1412- 1421
Methods Double blind RCT in 16 academic centers in Australia and New Zealand; for fluid resuscitation
Open-label, RCT trial in 57 ICUs in France, Belgium, Canada, Algeria, and Tunisia; ICU patients with hypovolemic shock
Open-label RCT in 100 ICUs in Italy
Comparison/ 1° Outcome
4% albumin vs. 0.9% normal saline; All-cause mortality at 28 days
Colloids vs. Crystalloids; All-cause mortality at 28 days
Albumin vs. noalbumin; All-causemortality at 28 days
Results (n=6997); 20.9% albumin vs. 21.1% normal saline (RR 0.99; 95% CI 0.91-1.09; p=0.87)
(n= 2857) ; 25.4% colloids vs. 27.0% crystalloids (RR 0.96; 95% CI 0.88-1.04; p = 0.26)
(n=1818); 31.8%albumin vs. 32% no albumin (RR 1.00; 95% CI 0.87-1.14; p=0.94)
No difference in mortality between crystalloids and colloids
Yunos NM, et al. JAMA 2012;308 (15):1566-72.Young P, et al. JAMA 2015;314 (16):1701-10.
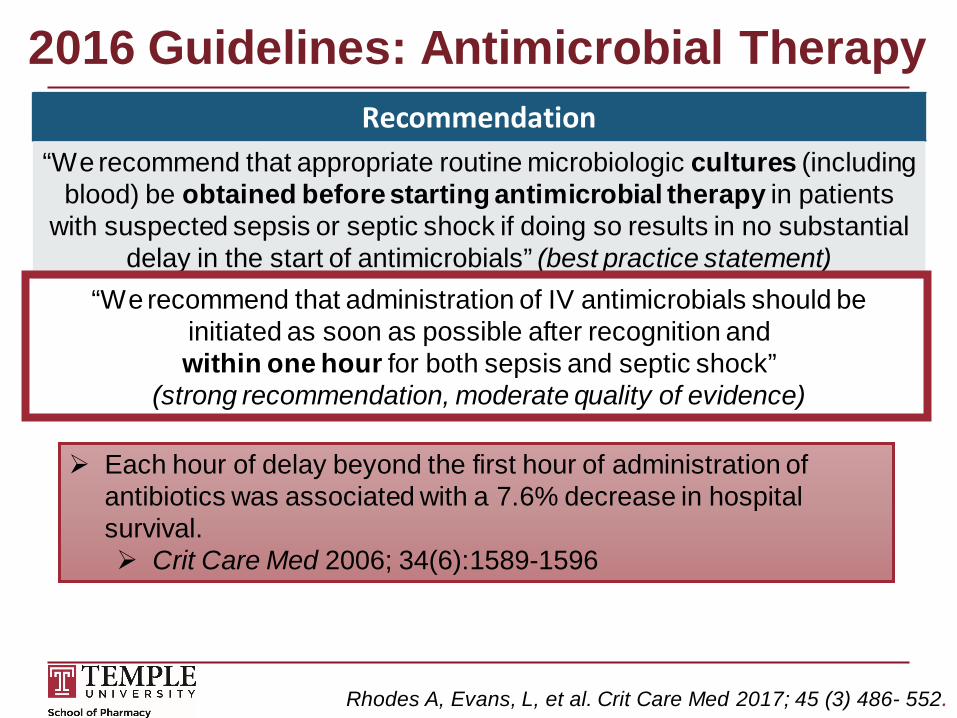
2016 Guidelines: Antimicrobial TherapyRecommendation
“We recommend that appropriate routine microbiologic cultures (including blood) be obtained before starting antimicrobial therapy in patients
with suspected sepsis or septic shock if doing so results in no substantial delay in the start of antimicrobials” (best practice statement)
“We recommend that administration of IV antimicrobials should be initiated as soon as possible after recognition and within one hour for both sepsis and septic shock”
(strong recommendation, moderate quality of evidence)
Each hour of delay beyond the first hour of administration of antibiotics was associated with a 7.6% decrease in hospital survival. Crit Care Med 2006; 34(6):1589-1596
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
2016 Guidelines: Antimicrobial TherapyRecommendation
“We recommend empiric broad-spectrum therapy with one or more antimicrobials for patients presenting with sepsis or septic shock to cover
all likely pathogens (including bacterial and potentially fungal or viral coverage” (strong recommendation, moderate quality of evidence)
“We recommend that empiric antimicrobial therapy be narrowed once pathogen identification and sensitivities are established and/or
adequate clinical improvement is noted” (best practice statement)
Empiric broad-spectrum coverage: inappropriate antibiotics for septic shock resulted in a 5- fold reduction in survival
Consider additional gram-negative coverage (double-coverage) in patients at high risk for multidrug-resistant (MDR) pathogens
Consider empiric antifungal coverage in patients at risk for invasive Candida infection (e.g. immunocompromised state, TPN, necrotizing pancreatitis, recent abdominal surgery, and recent fungal infection)
Kumar A, et al. Chest 2009; 136(5): 1237-1248. Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
2016 Guidelines: Antimicrobial TherapyRecommendation
“We recommend that dosing strategies of antimicrobials be optimized based on accepted pharmacokinetic/ pharmacodynamic principles
and specific drug properties in patients with sepsis or septic shock”(best practice statement)
Initial empiric antimicrobial dosing: Increased volume of distribution due to aggressive fluid
resuscitation Initiate higher end-loading dose Vancomycin IV loading dose of 25-30 mg/kg
(based on actual body weight) β-lactams given as a bolus or rapid infusion to rapidly
achieve therapeutic blood levels
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
2016 Guidelines: Antimicrobial TherapyRecommendation
“We suggest that an antimicrobial treatment duration of 7- 10 days is adequate for most serious infections associated
with sepsis and septic shock” (weak recommendation, low quality of evidence)
“We suggest that longer courses are appropriate in patients who have a slow clinical response, undrainable foci of infection, bacteremia with
Staphylococcus aureus, some fungal and viral infections, or immunologic deficiencies, including neutropenia”
(weak recommendation, low quality of evidence)“We suggest that shorter courses are appropriate in some patients,
particularly those with rapid clinical resolution following effective source control of intra-abdominal or urinary sepsis and those with anatomically
uncomplicated pyelonephritis” (weak recommendation, low quality of evidence)
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
2016 Guidelines: Vasoactive MedicationsRecommendation
“We recommend Norepinephrine (NE) as the first-choice vasopressor”(strong recommendation, moderate quality of evidence)
“We suggest adding either vasopressin (up to 0.03 units/ min) (weak recommendation, moderate quality of evidence) or epinephrine (weak
recommendation, low quality of evidence) to NE with the intent of raising MAP to target, or adding vasopressin (up to 0.03 units/min) (weak
recommendation, moderate quality of evidence) to decrease NE dosage”“We suggest using dopamine as an alternative vasopressor agent to NE
only in highly selected patients (e.g. patients with low risk of tachyarrhythmias and absolute or relative bradycardia)”
(weak recommendation, low quality of evidence).“We suggest using dobutamine in patients who show evidence of
persistent hypoperfusion despite adequate fluid loading and use of vasopressor agents”(weak recommendation, low quality of evidence)
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
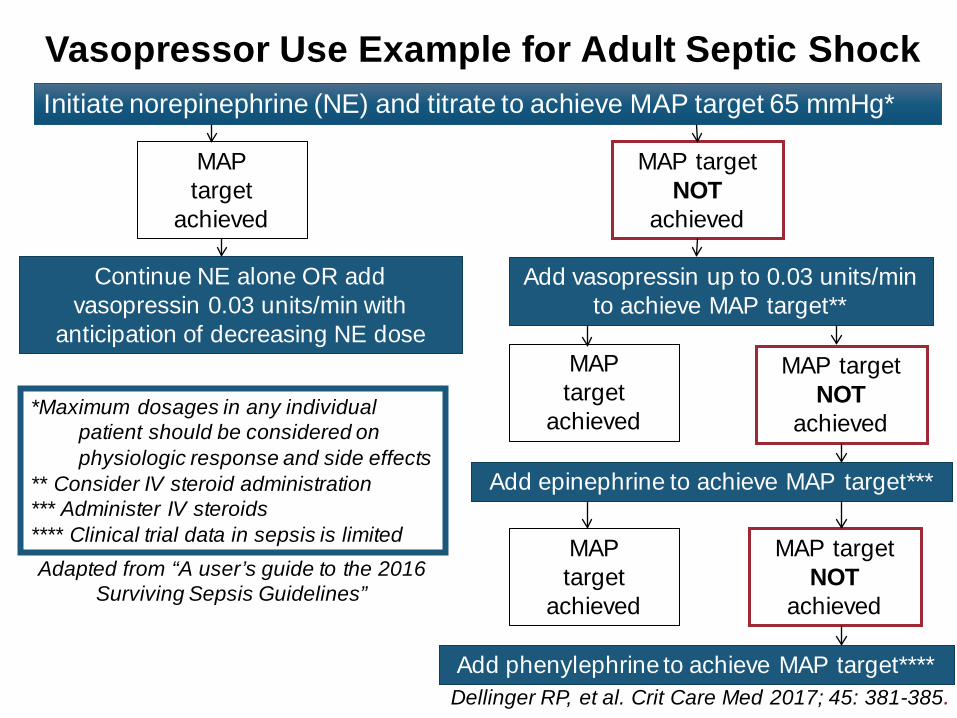
Vasopressor Use Example for Adult Septic ShockInitiate norepinephrine (NE) and titrate to achieve MAP target 65 mmHg*
MAP target
achieved
MAP target NOT
achieved
Continue NE alone OR add vasopressin 0.03 units/min with
anticipation of decreasing NE dose
Add vasopressin up to 0.03 units/min to achieve MAP target**
Add epinephrine to achieve MAP target***
Add phenylephrine to achieve MAP target****
MAP target NOT
achieved
MAP target NOT
achieved
MAP target
achieved
MAP target
achieved
*Maximum dosages in any individual patient should be considered on physiologic response and side effects
** Consider IV steroid administration*** Administer IV steroids**** Clinical trial data in sepsis is limited
Dellinger RP, et al. Crit Care Med 2017; 45: 381-385.
Adapted from “A user’s guide to the 2016 Surviving Sepsis Guidelines”
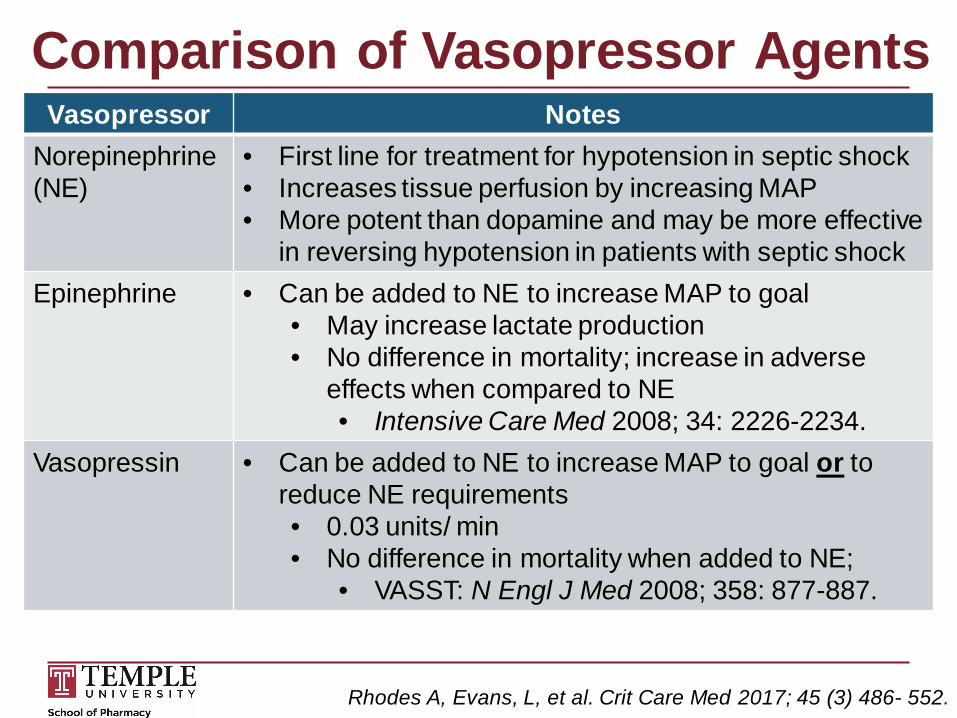
Comparison of Vasopressor AgentsVasopressor Notes
Norepinephrine(NE)
• First line for treatment for hypotension in septic shock• Increases tissue perfusion by increasing MAP• More potent than dopamine and may be more effective
in reversing hypotension in patients with septic shockEpinephrine • Can be added to NE to increase MAP to goal
• May increase lactate production• No difference in mortality; increase in adverse
effects when compared to NE• Intensive Care Med 2008; 34: 2226-2234.
Vasopressin • Can be added to NE to increase MAP to goal or to reduce NE requirements • 0.03 units/ min• No difference in mortality when added to NE;
• VASST: N Engl J Med 2008; 358: 877-887.
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
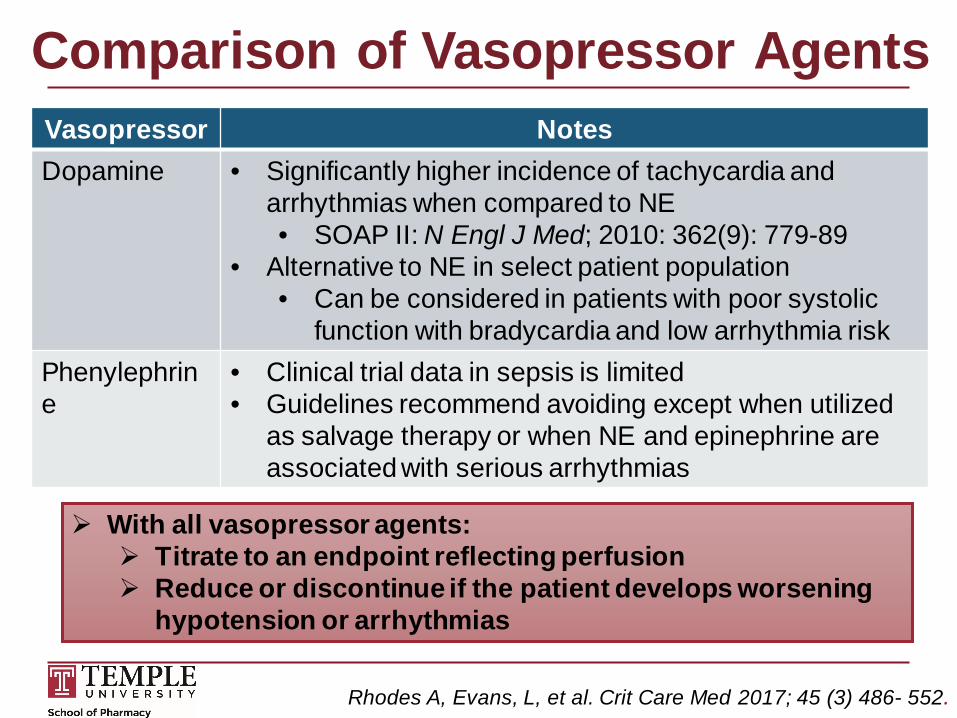
Comparison of Vasopressor AgentsVasopressor NotesDopamine • Significantly higher incidence of tachycardia and
arrhythmias when compared to NE• SOAP II: N Engl J Med; 2010: 362(9): 779-89
• Alternative to NE in select patient population• Can be considered in patients with poor systolic
function with bradycardia and low arrhythmia riskPhenylephrine
• Clinical trial data in sepsis is limited• Guidelines recommend avoiding except when utilized
as salvage therapy or when NE and epinephrine are associated with serious arrhythmias
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
With all vasopressor agents: Titrate to an endpoint reflecting perfusion Reduce or discontinue if the patient develops worsening
hypotension or arrhythmias
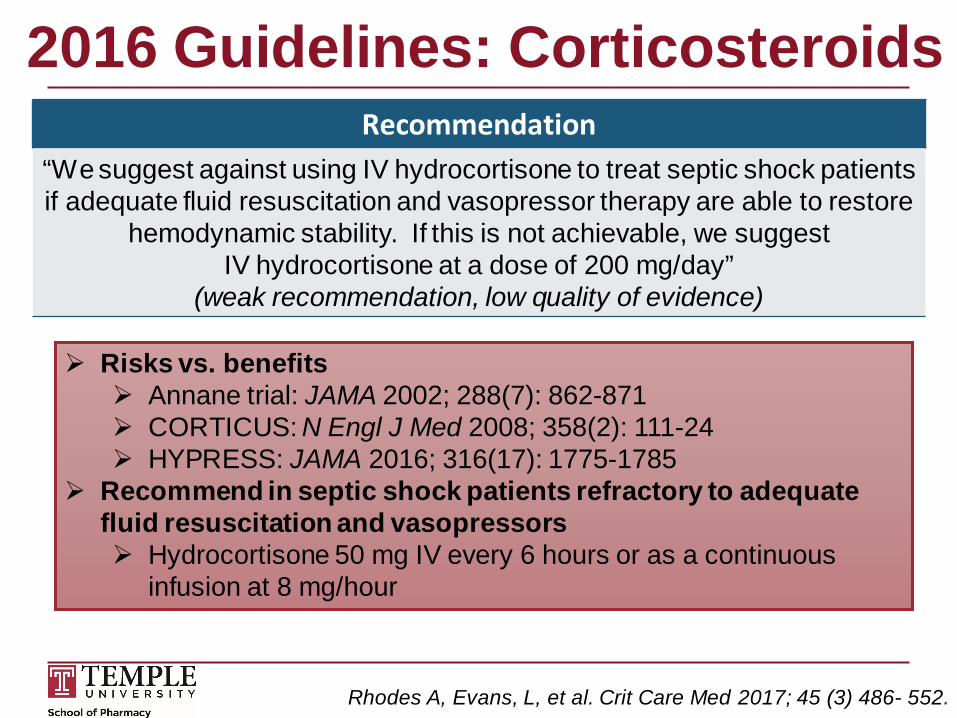
2016 Guidelines: CorticosteroidsRecommendation
“We suggest against using IV hydrocortisone to treat septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore
hemodynamic stability. If this is not achievable, we suggest IV hydrocortisone at a dose of 200 mg/day”
(weak recommendation, low quality of evidence)
Risks vs. benefits Annane trial: JAMA 2002; 288(7): 862-871 CORTICUS: N Engl J Med 2008; 358(2): 111-24 HYPRESS: JAMA 2016; 316(17): 1775-1785
Recommend in septic shock patients refractory to adequate fluid resuscitation and vasopressors Hydrocortisone 50 mg IV every 6 hours or as a continuous
infusion at 8 mg/hour
Rhodes A, Evans, L, et al. Crit Care Med 2017; 45 (3) 486- 552.
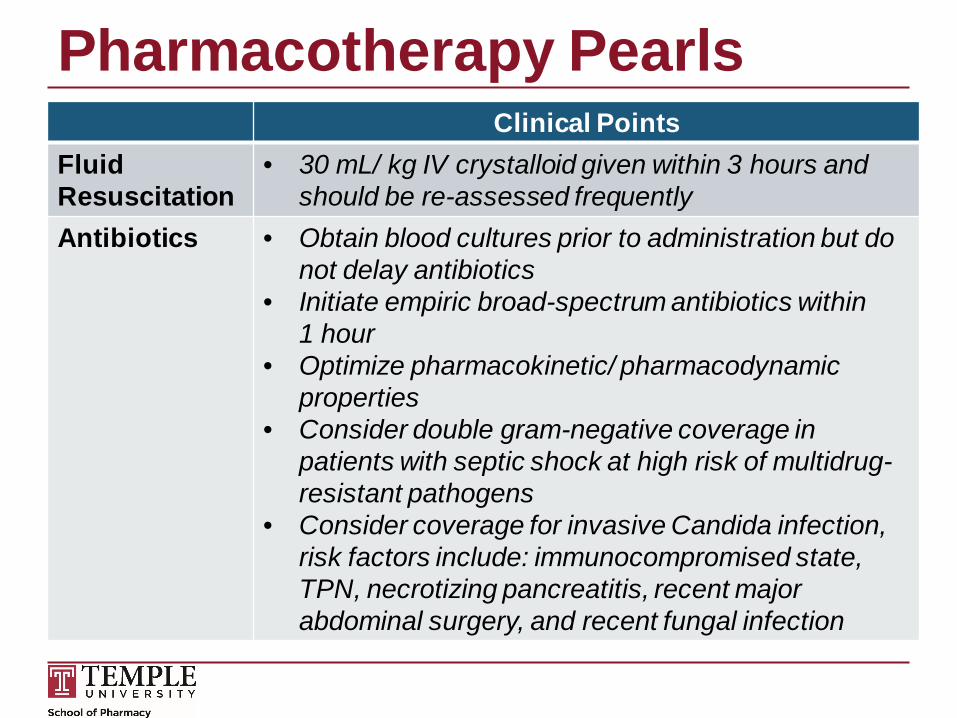
Pharmacotherapy PearlsClinical Points
Fluid Resuscitation
• 30 mL/ kg IV crystalloid given within 3 hours and should be re-assessed frequently
Antibiotics • Obtain blood cultures prior to administration but do not delay antibiotics
• Initiate empiric broad-spectrum antibiotics within 1 hour
• Optimize pharmacokinetic/ pharmacodynamic properties
• Consider double gram-negative coverage in patients with septic shock at high risk of multidrug-resistant pathogens
• Consider coverage for invasive Candida infection, risk factors include: immunocompromised state, TPN, necrotizing pancreatitis, recent major abdominal surgery, and recent fungal infection
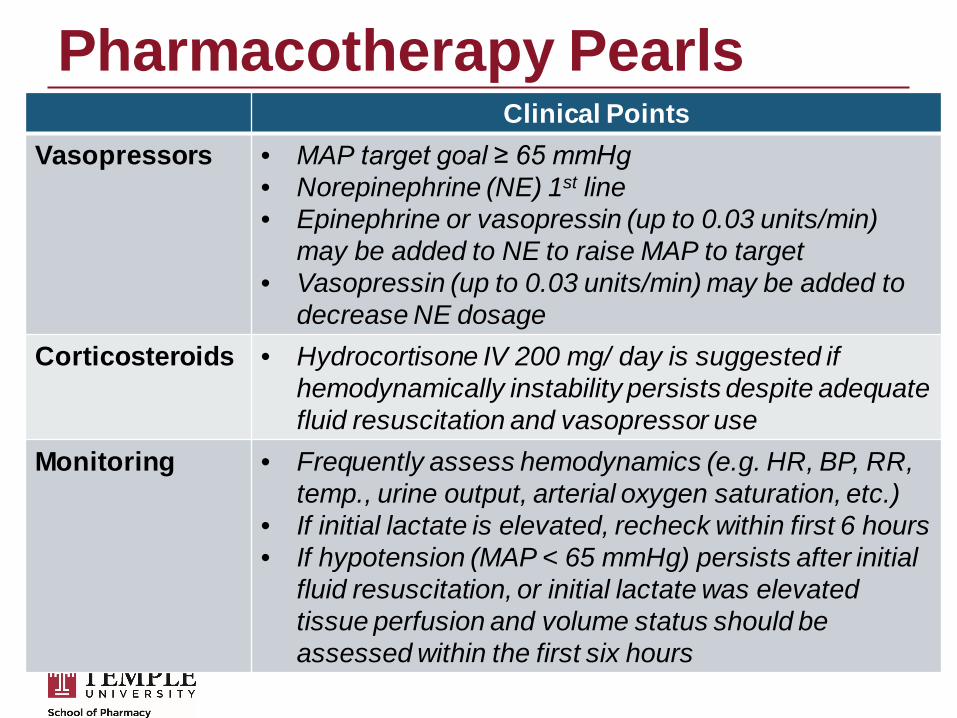
Pharmacotherapy PearlsClinical Points
Vasopressors • MAP target goal ≥ 65 mmHg• Norepinephrine (NE) 1st line• Epinephrine or vasopressin (up to 0.03 units/min)
may be added to NE to raise MAP to target• Vasopressin (up to 0.03 units/min) may be added to
decrease NE dosageCorticosteroids • Hydrocortisone IV 200 mg/ day is suggested if
hemodynamically instability persists despite adequate fluid resuscitation and vasopressor use
Monitoring • Frequently assess hemodynamics (e.g. HR, BP, RR, temp., urine output, arterial oxygen saturation, etc.)
• If initial lactate is elevated, recheck within first 6 hours• If hypotension (MAP < 65 mmHg) persists after initial
fluid resuscitation, or initial lactate was elevated tissue perfusion and volume status should be assessed within the first six hours
Patient Case1. Which evidence-based therapy should be immediately initiated
during the initial phase of resuscitation?a. Normal Saline (NS)b. Hydrocortisone IVc. Vasopressin IV continuous infusion d. 5% Albumin
2. According to the Surviving Sepsis Campaign Bundles what should be done within the first 3 hours?
a. Obtain a lactate levelb. Obtain blood cultures prior to administration of antibioticsc. Administer broad spectrum antibioticsd. Administer IV crystalloid for hypotension or lactate level ≥
4 mmol/Le. All of the above
Patient Case3. RX received 2 Liters of NS. Is the amount of IV fluid received
adequate for RX?a. Yesb. No
4. The ED team is impressed with all of your helpful and amazing recommendations. However, one hour later, despite adequate fluid resuscitation RX is tachycardic, hypotensive, and has septic shock. What evidence-based recommendation should be initiated next?
a. Hydrocortisone IVb. Dopamine IV continuous infusionc. Norepinephrine IV continuous infusiond. Watch and wait… reassess in 1 hour
References Singer M, Deutschman CS, Seymour CW, et al. The Third International Consensus
Definitions for Sepsis and Septic shock (Sepsis-3). JAMA. 2016; 315(8): 801-810.
Rhodes A, Evans LE, Alhazzani W, et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Crit Care Med 2017; 45(3):486-552 .
Surviving Sepsis Campaign. Bundles. http//www.survivingsepsis.org/Bundles/Pages/default.aspx. (Accessed 08/21/2017).
Angus DC, Barnato AE, Bell D, et al. A systematic review and meta-analysis of early goal –directed therapy for septic shock: the ARISE, ProCESS, and ProMISeInvestigators. Intensive Care Med 2015; 41(9): 1549-60.
Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001; 345(19); 1368-1377.
ProCESS Investigators, Yealy DM, Kellum JA, Juang DT, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med 2014; 370(18): 1683-1693.
ARISE Investigators and the ANZICS Clinical Trials Group. Goal-directed resuscitation for patients with early septic shock. N Engl J Med 2014; 371(16): 1496-1506.
Mouncey PR, Osborn TM, Power GS, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med 2015; 372(14): 1301-1311.
References Asfar P, Meziani, F, Hamel JF, et al. High versus low blood pressure target in patients
with septic shock. N Engl J Med 2014; 370(17): 1583-1593.
Caironi P, Tognoni G, Masson S, et al. Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med 2014; 370: 1412-21.
Casserly B, Phillips GS, Schorr C, et al. Lactate measurements in sepsis-induced tissue hypoperfusion: results from the Surviving Sepsis Campaign database. Crit Care Med. 2015; 43(3): 567-573.
Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline based performance improvement program. Crit Care Med. 2014; 42(8): 1749-1755.
Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med. 2006; 34(6): 1589-1596.
Kumar A, Ellis P, Arabi Y, et al. Initiation of inappropriate antimicrobial therapy results in a fivefold reduction of survival in human septic shock. Chest 2009; 136(5): 1237-1248.
Gaieski DF, Mikkelsen ME, Band RA, et al. Impact of time to antibiotics on survival in patients with severe sepsis or septic shock in whom early goal-directed therapy was initiated in the emergency department. Crit Care Med 2010; 38(4): 1045-53.
References Finfer S, Bellomo R, Boyce N, et al. A comparison of albumin and saline for fluid for fluid
resuscitation in the intensive care unit. N Engl J Med 2004; 350: 2247-56.
Annane D, Siami S, Jaber S, et al. Effects of fluid resuscitation with colloids vs. crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA 2013; 310(17): 1809-17.
Caironi P, Tognoni G, Masson, S, et al. Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med 2014; 370(15): 1412-1421.
Yunos NM, Bellomo, R, Hegarty C, et al. Association between a chloride-liberal vs. chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA 2012; 308(15): 1566-1572.
Young P, Bailey M, Beasley R, et al. Effect of a buffered crystalloid solution vs. saline on acute kidney injury among patients in the intensive care unit. JAMA 2015; 314(16): 1701-1710.
De Backer, D, Biston, P, Devriendt J, et al. Comparison of Dopamine and Norepinephrine in Treatment of Shock. N Engl J Med 2010; 362(9): 779-789.
Myburgh JA, Higgins A, Jovanovska A, et al; CAT Study Investigators: A comparison of epinephrine and norepinephrine in critically ill patients. Intensive Care Med 2008; 34: 2226-2234.
References Russell JA, Walley KR, Siger J, et al. VASST Investigators: Vasopressin versus
norepinephrine infusion in patients with septic shock. N Engl J Med 2008; 358: 877-887.
Annane D, Sebille, v, Charpentier C. et al. Effect of treatment with low doses of hydrocortisone and fludrocortisone on mortality in patients with septic shock. JAMA2002; 288(7): 862-871.
Sprung C, Annane D, Keh D, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med 2008; 358(2): 111-24.
Keh D, Trips E, Marx G, et al. Effect of hydrocortisone on development of shock among patients with severe sepsis. JAMA 2016(17): 1775-1785.
Questions and DiscussionThank You!
Neela Bhajandas, Pharm.D.Clinical Assistant Professor of Pharmacy Practice
Temple University School of [email protected]