Embed Size (px)
Citation preview

Supplement to Sponsored by NicOx
September 2013
Updating the
differential diagnosis
Raising the standard of ophthalmic care with point-of-care testing for adenovirus.

Updating the differential diagnosis
2 Supplement to CataRaCt & RefRaCtive SuRgeRy today SeptembeR 2013
“think tank” panel discussioninaugural nicox ophthalmology
Richard L. Lindstrom, MD, (Moderator) is the founder of and an attending surgeon at Minnesota Eye Consultants, PA, in Bloomington. He is a consul-tant to NicOx, Inc. Dr. Lindstrom may be reached at (612) 813-3600; [email protected].
Edward J. Holland, MD, is a professor of ophthal-mology at the University of Cincinnati in Ohio and the director of cornea at the Cincinnati Eye Institute. He acknowledge no financial interest in the product or company mentioned herein.
Dr. Holland may be reached at (859) 331-9000, ext. 3064; [email protected].
Terry Kim, MD, is a professor of ophthalmol-ogy, specializing in cornea, cataract, and refrac-tive surgery at the Duke University Eye Center in Durham, North Carolina. He acknowledged no financial interest in the product or company
mentioned herein. Dr. Kim may be reached at (919) 681-3568; [email protected].
Jodi I. Luchs, MD, is director of the Department of Refractive Surgery, North Shore/Long Island Jewish Health System, in Great Neck, New York. He acknowledged no financial interest in the product or company mentioned herein. Dr. Luchs
may be reached at (516) 785-3900; [email protected].
Francis S. Mah, MD, is director, cornea and external disease, and also co-director, refractive surgery, at the Scripps Clinic in La Jolla, California. He acknowledged no financial interest in the product or company mentioned herein.
Dr. Mah may be reached at (858) 554-7996; [email protected].
Marguerite B. McDonald, MD, is a cornea/refrac-tive specialist with the Ophthalmic Consultants of Long Island in New York, a clinical professor of ophthalmology at the NYU School of Medicine in New York, and an adjunct clinical professor
of ophthalmology at the Tulane University Health Sciences Center in New Orleans. She acknowledged no financial interest in the product or company mentioned herein. Dr. McDonald may be reached at (516) 593-7709; [email protected].
Terrence P. O’Brien, MD, is a professor of oph-thalmology and the Charlotte Breyer Rodgers dis-tinguished chair in ophthalmology at the Bascom Palmer Eye Institute, University of Miami, Miller School of Medicine, in Palm Beach, Florida. He
acknowledged no financial interest in the product or com-pany mentioned herein. Dr. O’Brien may be reached at (561) 515-1544; [email protected].
Jai G. Parekh, MD, MBA, is a managing partner at Brar-Parekh Eye Associates in Woodland Park, New Jersey. Dr. Parekh is also chief of cornea and external diseases/director of the Research Institute at St. Joseph’s HealthCare System in Paterson, New
Jersey, and clinical associate professor of ophthalmology on the Cornea Service at the New York Eye & Ear Infirmary/New York Medical College in New York. He acknowledged no finan-cial interest in the product or company mentioned herein. Dr. Parekh may be reached at (973) 785-2050; [email protected].
Jay S. Pepose, MD, PhD, is the director of the Pepose Vision Institute and a professor of clinical ophthalmology and visual sciences at the Washington University School of Medicine in St. Louis. He acknowledged no financial interest in
the product or company mentioned herein. Dr. Pepose may be reached at (636) 728-0111; [email protected].
Rajesh K. Rajpal, MD, is the medical director of Cornea Consultants, PC, in McLean, Virginia, and a clinical associate professor at Georgetown University Medical Center in Washington, DC. He acknowledged no financial interest in the product
or company mentioned herein. Dr. Rajpal may be reached at (703) 287-4122; [email protected].
Neda Shamie, MD, is an associate professor of oph-thalmology at the Doheny Eye Institute, University of Southern California Keck School of Medicine, and the medical director at the University of Southern California Doheny Eye Center-Beverly Hills. She
acknowledged no financial interest in the product or company mentioned herein. Dr. Shamie may be reached at [email protected].
John D. Sheppard, MD, MMSc, serves as professor of ophthalmology, microbiology & immunology, as well as program director for ophthalmology residency training at the Eastern Virginia Medical School in Norfolk, Virginia. He is also clinical direc-
tor of the Thomas R. Lee Center for Ocular Pharmacology. He acknowledged no financial interest in the product or company mentioned herein. Dr. Sheppard may be reached at (757) 622-2200; [email protected]
William B. Trattler, MD, is the director of cor-nea at the Center for Excellence in Eye Care in Miami. He acknowledged no financial interest in the product or company mentioned herein. Dr. Trattler may be reached at (305) 598-2020;

SeptembeR 2013 Supplement to CataRaCt & RefRaCtive SuRgeRy today 3
Updating the differential diagnosis Updating the differential diagnosis
Adenovirus accounts for up to 90% of all cases of viral conjunctivitis, including approximately one out of four cases of acute conjunctivitis diagnosed by eye care practitioners.1-4 However, diagnosing adenoviral versus bacterial conjunctivitis can be challenging for eye care providers; it has been estimated that even corneal specialists correctly diagnose conjunc-tivitis less than 50% of the time.5 To assist with this diagnosis, NicOx, Inc. (Dallas, TX), designed the first and only CLIA-waived, disposable point-of-care test, called AdenoPlus (Figure 1). The AdenoPlus diagnostic test has a high specificity and sensitivity for detecting adenovirus (and thereby also rules out bacterial and allergic conjunctivitis). Therefore, this test saves clinicians and patients the time, frustration, and cost of a misdiagnosis and inappropriate treatment.
To help clinicians use the AdenoPlus test most effectively, NicOx, Inc., also developed a three-step Red Eye Protocol for conjunctivitis to use in conjunction with the point-of-care test. In this roundtable discussion, noted ophthalmologists describe their clinical experience with the AdenoPlus test and the Red Eye Protocol as well as the impact these tools have had on their practices. I am confident that you will learn valuable insights from these colleagues on diagnosing and effec-tively treating adenoviral conjunctivitis.
—Richard L. Lindstrom, MD
Dr. Lindstrom: My first question to the panel is, why should ophthalmologists and optometrists implement the Red Eye Protocol for conjunctivitis (Figures 2 – 4)?
Dr. Mah: There are many reasons why vision care specialists should implement the conjunctivitis protocol. The first reason is to make a correct diagnosis. Epidemic keratoconjunctivitis (EKC) and adenovirus can impart a significant socioeconomic impact. Affected children must be kept home from school, which may necessitate a babysitter or time off from work for the parent. Adults who have EKC may not be able to work.
A second justification for a conjunctivitis protocol is so that treating physicians can identify those patients who have EKC and exclude from follow-up those patients who test negative. When a patient tests positive, the practitioner can have the clinic’s rooms cleaned to help prevent the disease from spreading.
Patients will also benefit from the conjunctivitis proto-col by gaining the peace of mind that they are receiving the appropriate treatment and can expect quick relief without further doctor visits. They can view the positive or negative results of their test and then follow through on their clinician’s recommendations.
Dr. Lindstrom: Dr. Holland, are we clinicians effective at making the differential diagnosis for conjunctivitis?
Dr. Holland: Unfortunately, we are not, and the rea-son is that the symptoms of viral, bacterial, and allergic conjunctivitis are very similar (Figure 5). The studies that have examined conjunctivitis and potential treatments have shown that even corneal specialists make a correct diagnosis less than 50% of the time.3-5 If we extrapolate to comprehensive ophthalmologists and optometrists, this rate could be even lower. Clearly, we need help in making the correct diagnosis. In clinical trials, the AdenoPlus test showed 90% sensitivity in detecting adenovirus (Figure 6).
Dr. Lindstrom: Dr. Sheppard, what are your experiences with epidemic keratoconjunctivitis? What are the risks of missing this diagnosis?
Dr. Sheppard: The risk is huge. Primarily, all health-care professionals are at an increased risk of contracting keratoconjunctivitis. I know dozens of ophthalmologists who have lost significant time in the OR because they themselves contracted the disease.
The risk to the patient is twofold. Not only may affect-ed individuals lose vocational time, but they are at risk
figure 1. the adenoplus diagnostic test for adenovirus.
figure 2. the red eye protocol for conjunctivitis.
Isolate FRONT OFFICE identi�es and isolates patient
EvaluateClinical signs and symptoms and patient historyTECHNICIAN performs AdenoPlus test (<2 minutes to complete;results within 10 minutes) if acute conjunctivitis is determined
Interpret and TreatEYE CARE PRACTITIONER interprets test results and determinesappropriate treatment based on diagnostic evidence

4 Supplement to CataRaCt & RefRaCtive SuRgeRy today SeptembeR 2013
Updating the differential diagnosis
of transmitting the infection to relatives and children as well. Thus, the pyramid of an epidemic is almost always triggered out of an eye care clinic, and it creates an expo-nential expense to individuals and the greater society in missed days of work and school. It is very difficult to block such an epidemic and repair the reputation of the practice where it originated.
IMPLEMENTATION INTO THE PRACTICEDr. Lindstrom: In my clinic, we designate a significant
responsibility of the first-line detection and testing of red eyes to ancillary personnel. Dr. McDonald, you have imple-mented the Red Eye Protocol at your practice. Has the staff embraced it?
Dr. McDonald: Our staff at Ophthalmic Consultants of Long Island have absolutely embraced the new con-junctivitis protocol. Since we implemented it, our clinical days have been uneventful and easy. All of the staff mem-bers were eager to use the AdenoPlus test. The techni-cians love to be more engaged in patient care. I already consider the Red Eye Protocol and the AdenoPlus test best-in-class management for conunctivitis.
Dr. Lindstrom: Dr. Rajpal, you have also implemented the Red Eye Protocol over the past few months. What has been your experience?
Dr. Rajpal: Our experience has been extremely posi-tive as well, similar to Dr. McDonald’s. Since my partners and I educated our staff about the Red Eye Protocol for conjunctivitis, they have fully bought into the concept. Our technicians and support staff like the idea of being able to discuss the protocol with patients directly, and the patients have been quite impressed that we have a test we can perform to confirm or rule out a worrisome infection. So, the process has been beneficial for us, and it has not slowed down our patient flow.
Dr. O’Brien: A decision tree in which the physician is the last person who decides whether to test a patient for keratoconjunctivitis actually discourages testing by
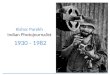
figure 4. part 3 of the red eye protocol: how to proceed with the diagnostic evidence from the adenoplus test.
figure 3. part 2 of the red eye protocol: administering the test.
Continue the di�erential diagnosis(with adenovirus ruled out) to determinelikelihood of bacterial or allergicConsider topical antibiotic or antihistaminetherapy, or a combinationFollow up or refer if decreased vision or pain,or lack of improvement over 7 days
NegativePositiveConsider nonantibiotic therapyPatient counseling: isolation (7 to 10 days); hand washing;no towel sharing or close contactSupportive care: arti�cial tears, antihistamines, cold compresses,or topical corticosteroids with close patient monitoringImplementation of CDC guidelines for decontaminationof exposed surfaces and equipment in the ECP o�ce
“Since we implemented it, our clinical days have been uneventful and easy. All of the staff members were eager to use the AdenoPlus test. The technicians love to be more engaged in patient care. I already consider the Red Eye Protocol and the AdenoPlus test best-in-class management for conunctivitis.”
—Dr. McDonald

SeptembeR 2013 Supplement to CataRaCt & RefRaCtive SuRgeRy today 5
Updating the differential diagnosis Updating the differential diagnosis
the entire staff. It kills the excitement, and thus kills the entire acute conjunctivitis protocol. Empowering the staff to use the AdenoPlus test on appropriate patients is ideal.
Thanks to years of inaccurate diagnoses and the inappropriate use of antimicrobial agents, we now have a global concern about the emergence and spread of microbial resistance. From a pharmacoeconomic stand-point, the cost of the unnecessary, inappropriate use of antibiotics in the United States is about a $500,000,000 per year.4 Furthermore, as healthcare reform evolves, indiscriminant antibiotic usage will see greater govern-ment regulation. Therefore, I think a diagnostic test for ocular infection that has high specificity and high sen-sitivity makes sense from the perspective of the global microbiosphere.
Dr. Kim: We have all talked about the importance of diagnosing keratoconjunctivitis correctly. EKC can be a severe disease. I think practitioners tend to think about it as pink eye with the watery, itchy symptoms, but these cases can progress. Some people get infiltrates in the cor-nea, corneal scarring, decreased vision, and conjunctiva membrane formation and scarring. So, it is not neces-sarily a benign disease. For this reason, I think one of the benefits of diagnosing EKC early is to establish a protocol that the patient can follow and that we can follow-up to hopefully prevent this condition from progressing and causing permanent damage to the vision and the corneal structures.
THE RED EYE PROTOCOL FOR CONJUNCTIVITISDr. Lindstrom: Let us describe the Red Eye Protocol for
conjunctivitis and how one goes about implementing it into clinical practice.
Dr. Shamie: The entire clinic must buy into the protocol in order for it to be successful. There must be consensus about what conjunctivitis is and what the pre-senting symptoms include.
When the patient arrives in the office and begins undergoing assessment, the front-office staff member should identify him or her as either a red-eye patient or a pink-eye patient. Then, they should isolate the indi-vidual in the waiting room and attempt to bring him or her back for further assessment immediately, rather than expose other patients and staff to the infection.
An ideal scenario would be to have a red-eye room, an examination room that is isolated from the oth-ers. When the technician identifies a red eye, he or she could take the patient to that room for initial questioning and preliminary history points if he or she suspects acute conjunctivitis. Directly after making the assessment, the technician should perform a diagnos-tic test with the AdenoPlus point-of-care test, which takes about 2 minutes to perform and gives results in 10 minutes. When the doctor sees the patient, he or she already has a positive or negative AdenoPlus test for verification. Thus, this protocol helps with the flow of patients’ assessment and treatment for adenoviral conjunctivitis.
figure 5. Viral, bacterial, and allergic conjunctivitis have overlapping signs and symptoms that make a differential diag-
nosis challenging for physicians. ([1] fitch Cp, rapoza pa, owens s, et al. epidemiologyand diagnosis of acute conjuctivitis
at an inner-city hospital. Ophthalmology. 1989;96:1215-1220. [2] solomon as. symptoms of allergic conjunctvitis. Arch
Ophth. 1985;103(7):891. [3] Kosrirukvongs p, Visitsunthorn n, Vichyanond p, et al. allergic conjunctivitis. Asian Pac H Allergy.
2001;19:237-244.)

6 Supplement to CataRaCt & RefRaCtive SuRgeRy today SeptembeR 2013
Updating the differential diagnosis
THE AdenoPlus TESTDr. Lindstrom: Dr. Pepose, how does AdenoPlus work?
Dr. Pepose: The AdenoPlus testing strip utilizes an immunoassay to detect adenovius antigens. It recognizes the hexon protein that is common to all of the adenovi-rus serotypes. Although different serotypes of adenovirus are involved in various epidemics and locations world-wide, the hexon protein identifies them all.6
The AdenoPlus test uses a proprietary microfiltra-tion system to detect the hexon viral protein. After the sample is collected from the inferior palpebral conjunctiva, the sample collector is snapped into the test cassette and then dipped into a buffer solution. If viral antigens are present, the buffer solution creates a red immunoprecipitation line. This line is very easy to read and leaves no room for misinterpretation. The test has demonstrated 90% sensitivity and 96% speci-ficity versus culture results; these may be even higher compared to polymerase chain reaction (PCR). The ease of use of the AdenoPlus test is superb for both physicians and patients—it can be done right in the office, where we can counsel the patient if there is a positive diagnosis.
Dr. Trattler: I think the simplicity of this test is what makes it so useful in clinical practice. Even technicians are qualified to administer this test to patients and achieve a reliable result.
Dr. Luchs: I find it meaningful to be able to show the results of the AdenoPlus test to patients. A single blue line is a negative reading, and two lines, red and blue, is a positive reading. Having a visual representation really hits home with patients—they do not question the diagno-sis, and then they buy into the entire treatment program. This test really makes the care and treatment of affected patients a lot smoother.
Dr. Mah: This latest generation of the AdenoPlus test is much easier than the original version. My team and I conducted some studies on the first generation of the test, and this new generation of the test is much easier to read.
MANAGING PATIENTS WHO TEST POSITIVE FOR ADENOVIRUS
Dr. Lindstrom: How do we manage patients who test positive for adenovirus with AdenoPlus—particularly those individuals who are not showing severe effects?
Dr. Parekh: Education is the key. We must educate the patient, his or her family, and any other close con-tacts about the risk of contagion. Therapeutically, we can teach the patient to use cool compresses, artificial tears, and other supportive strategies to help them endure the first several days of infection, especially while they are shedding virus. I am against using corti-costeroids as an initial therapy because of these agents’ propensity to prolong viral shedding. I tend to begin treatment with conservative therapies and then add additional medications 5 to 7 days later as needed.
Dr. Lindstrom: Dr. Sheppard, what is your recommen-dation to patients about returning to work or school after they leave your office?
Dr. Sheppard: Before antiviral therapies were avail-able, we were obliged to calculate the initial day of viral shedding using the onset of symptoms minus 5 days. We would then treat patients for the 7 days that they were actively infectious and advise them to not transmit the infection through fomites or any type of personal contact, particularly if they worked in a healthcare environment.
Recently, some evidence has emerged that topical antivirals can significantly reduce viral shedding.2,7-9 This is an off-label indication, but in the absence of antiviral therapy, we are committed to keeping infected patients away from other individuals for 7 full days—a prescrip-tion that can strongly impact the patient’s professional life and/or family life.
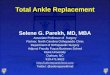
figure 6. adenoplus was evaluated in a prospective, multi-
center, mass sequential clinical trial performed at eight clini-
cal centers (both private and academic ophthalmology prac-
tices). the study enrolled 128 patients who presented with
a clinical diagnosis of acute viral conjunctivitis; 31 patients
were confirmed positive for adenovirus by cell culture.
twenty-eight of the 31 subjects showed a 90% sensitivity on
the adenoplus test. the specificity was 96% (93 out of 97). of
the four presumed false-positives, however, at least two were
determined to be positive by polymerase chain reaction (pCr)
testing, which raised the specificity of the adenoplus test to
approximately 98%.

SeptembeR 2013 Supplement to CataRaCt & RefRaCtive SuRgeRy today 7
Updating the differential diagnosis Updating the differential diagnosis
Dr. Lindstrom: Dr. Donnenfeld, you have advocated for antiviral medications in the past. What are your thoughts?
Dr. Donnenfeld: My partners and I have been inter-ested in antiviral therapy for adenoviral conjunctivitis for a long time. In Dr. Mah’s previous practice at the University of Pittsburgh, Jerry Gordon, MD, was consid-ered one of the world’s leaders in this therapy. Today, there is no approved antiviral medication for EKC, but there is strong in vitro evidence that ganciclovir acts against adenovirus. Clinical studies presented by Dr. McDonald this year7 and by Tabarra in 20012 showed patients had significantly faster resolution of their disease with ganciclovir as well as fewer subepithelial infiltrates. The ongoing study that Dr. Pepose is sharing is examin-ing that very issue; perhaps he can address it.
Personally, I feel that there is sufficient evidence that the off-label use of ganciclovir can reduce the duration of shedding associated with adenovirus and the inci-dence of subepithelial infiltrates. I put into practice the therapies I think are best for patients.
I always ask myself, if this were my eye, would I want to have a therapy? The answer is yes. Now, with AdenoPlus’ accurate diagnosis of adenovirus, including the EKC-causing serotypes, I feel more empowered than ever to treat these patients. I always tell my patients that my use of ganciclovir is off label, and I have them sign an informed consent, but it has become the standard of care at my practice. I prescribe ganciclovir drops five times per day for 1 week followed by three times per day for 1 week. If the patient only has one eye involved, I treat the other eye three times per day, and I prescribe the same for very close family members. If I were diagnosed with EKC, I would treat my family three times a day for 2 weeks with ganciclovir during the duration of shedding to reduce the risk of an outbreak. Although this drug does not yet have good clinical trials behind it, I believe it is a do-no-harm therapy that has the potential to greatly improve EKC sufferers’ quality of life.
Dr. Rajpal: I think this discussion about therapeutic strategies for EKC exemplifies exactly how important accurate testing of the disease is. As mentioned previous-ly, we are very poor at diagnosing adenoviral conjuncti-vitis without this test—potentially; we could be treating half of our patients unnecessarily. I think it is important to understand that a negative test is very helpful to us in preventing the inappropriate treatment of patients.
Dr. Pepose: I concur. In the cidofovir trial in which many of us were involved (Bausch + Lomb; data on file), only 27% (49 of 181 study eyes) diagnosed clinical-ly as having adenovirus conjunctivitis had positive viral cultures or polymerase chain reactions. Although all the individuals who made the diagnoses were corneal
specialists, we were wrong three out of four times. Some of these patients were culture-positive for herpes, some for Chlamydia, and some had bacterial infections. This example goes to prove that we cannot make a confident diagnosis just by looking at symptoms; we really need a definitive test.
Dr. Parekh: I think that changing insurance guide-lines will place more emphasis on looking at outcomes and managing our risk up front of making an incorrect diagnosis. As Dr. O’Brien described, the frivolous use of antibiotics is not only a socioeconomic problem, but eventually, it may prevent us from getting reimbursed for necessary follow-up visits for the same patient. Therefore, making the correct diagnosis on day zero is incredibly important to our bottom lines. Moreover, attaching the correct treatment algorithm to the patient’s actual dis-ease I think is incredibly cutting edge.
Dr. Sheppard: Speaking to the inability of highly qualified ophthalmologists to make a proper clinical diagnosis, I have personally treated several dozen oph-thalmologists who contracted EKC. These individuals have immediate access to samples, but they do not really know the cause of their conjunctivitis.
There is distinct evidence from articles published by Proctor Foundation faculty8,9 that viral shedding occurs during the prodrome and for 7 to 14 days following the onset of symptoms. Furthermore, initiating therapy with topical steroid or anti-inflammatory medications dur-ing the initial course of infection, encompassing the viral shedding phase, can actually prolong and intensify the clinical course of corneal infiltration.10-12 Thus, this pro-longation of early active viral replication gives the infec-tion the highest likelihood of debilitating the ophthalmic surgeon or any other prematurely treated patient. So, I caution practitioners to not self-treat before using this AdenoPlus tool to self-diagnose. I prefer to treat such infections initially with a topical antiviral during active viral replication, followed thereafter by a topical steroid, but only if significant inflammatory corneal or conjuncti-val complications have arisen.
“We are very poor at diagnosing adenoviral conjunctivitis without this [AdenoPlus] test—potentially; we could be treating half of our patients unneces-sarily. I think it is important to under-stand that a negative test is very helpful to us in preventing the inappropriate treatment of patients.”
—Dr. Rajpal

8 Supplement to CataRaCt & RefRaCtive SuRgeRy today SeptembeR 2013
Updating the differential diagnosis
Dr. Holland: I think another comment on treatment is what not to do. We do not want to treat patients who have viral conjunctivitis with antibiotics. There is enor-mous pressure on us as clinicians to provide relief when we have a patient in the office with a red eye who wants to leave with an antibiotic drop, especially if it’s a parent with a child. If we had a conclusive test, however, such as the AdenoPlus test that would tell us definitively that the infection is viral conjunctivitis, I think it would really change the way we practice. It would give clinicians more evidence to resist that pressure to use a topical antibiotic in a patient with viral conjunctivitis.
Dr. Luchs: For these patients, we could use an antivi-ral instead. All of us panelists here are giving antivirals to our EKC patients instead of an antibiotic.
Dr. Lindstrom: Dr. O’Brien, if you get a negative read-ing on the AdenoPlus test, how confident are you that the infection is not viral conjunctivitis, and then what is on the top of your differential as the alternatives?
Dr. O’Brien: Because of its high sensitivity and specific-ity, a negative AdenoPlus test provides a high level of con-fidence that you are not dealing with adenovirus. You still have to worry about herpes simplex viruses, as Dr. Pepose mentioned, which certainly could be exacerbated by the use of corticosteroids early in the treatment course.
Chlamydia is a condition that is sexually transmitted; it may mimic adenoviral conjunctivitis, so that has to be considered. Also, some forms of nonvirulent bacterial con-junctivitis may also mimic the viral conjunctivitis. I think, however, that a negative AdenoPlus test certainly gives us a high confidence that the infection is not adenovirus.
Dr. Lindstrom: Do you sometimes see patients in this category who ultimately have allergic conjunctivitis?
Dr. O’Brien: Yes, some turn out to be allergic con-junctivitis, or even exacerbations of dry eye or blepharitis.
Dr. Lindstrom: In the study you are conducting, Dr. Pepose, were any of the false-negative readings deter-mined to be in the allergic conjunctivitis category?
Dr. Pepose: Yes, a number of patients presented with overlapping symptoms that turned out to be adenovirus negative, and many of them were confirmed as allergic conjunctivitis or other etiologies.
EXPERIENCE AND SUCCESS STORIESDr. Lindstrom: What success stories or pearls have
you panelists observed since implementing the Red Eye Protocol for conjunctivitis and AdenoPlus into your prac-tice? Any surprises that you didn’t expect?
Dr. McDonald: The AdenoPlus test was very easy to implement into our practice. In the beginning, the technicians were a little tentative about using the test on appropriate patients. They gained confidence in their abilities quickly, however, and so far, they have never used it on a patient whose presentation didn’t warrant the test. Our practice is large—we have approximately 30 doctors and 380 employees—and to my knowledge, not once has a technician performed the test on an acute corneal ulcer or an eye with severe uveitis, or some other grossly inappropriate situation.
Yes, there have been several surprise positive read-ings that I did not expect. Which is exactly why we use the test! Our staff is very excited to be empow-ered to test patients, and the patients are impressed with the technology. They comment that they have never before seen such a test, and that the physician who referred them did not have it. Furthermore, they respect a positive test reading, and accept that they cannot walk out with a prescription for an antibiotic. There’s no argument.
Dr. Linstrom: Those of you who have been using the AdenoPlus test routinely, do you have any pearls for new adopters?
Dr. O’Brien: I find the test helpful with the delicate issues Dr. Sheppard alluded to. The ability of patients to supply their employers with a positive test result from their physician helps them secure the necessary furlough and time off from work. In that way, the AdenoPlus test helps keep infected individuals away from environments where they can transmit the disease to others.
Dr. Donnenfeld: There were several patients who, I was absolutely convinced, had adenovirus, but their tests turned out to be negative. Before I had diagnostic evidence, I would have instructed them to stay home from work for a week. Thus, it is just as important to have diagnostic evidence of a negative test to prevent unnecessary cost to the individual as well as to society in the form of missed work days. Furthermore, I was able to change my treatment protocol in light of the negative diagnostic information.
“There have been several surprise positive readings that I did not expect. Which is exactly why we use the test! Our staff is very excited to be empow-ered to test patients, and the patients are impressed with the technology.”
—Dr. McDonald

SeptembeR 2013 Supplement to CataRaCt & RefRaCtive SuRgeRy today 9
Updating the differential diagnosis Updating the differential diagnosis
Dr. Sheppard: I have treated similar patients with very acute membranous conjunctivitis that I was convinced was either adenovirus or streptococcal or Haemophilus. With a negative test reading, I can aggressively pursue steroidal therapy to avoid conjunctival cicatization, loss of lacrimal ductal function, and the various issues of comfort that come with early steroid therapy. I am comfortable with these side effects when treating an acute bacterial conjunc-tivitis, but I am not comfortable with them in an adenovirus situation.
Dr. Lindstrom: How do you clinicians anticipate the AdenoPlus test being adopted? Do you think it will spawn other diagnostic tests? What does the ophthalmologist or optometrist have to do in regards to CLIA in order to be waived and able to perform these point-of-care tests?
Dr. Rajpal: Although I am no expert in this area, I believe the CLIA waiver process varies by state. For my partners and I, it was a relatively straightforward application process that we submitted to the State Department of Health with office information, location tax ID, et cetera. Then, we simply wait-ed a few weeks for the approval to come through. It was not a complicated or difficult process, just a little time con-suming. I believe the company marketing the AdenoPlus test will help offices that are not CLIA-waived to get started,
Dr. Luchs: My staff and I had the same experience, and we practice in New York. Fortunately, the NicOx team shepherds its customers through the process of submitting the paperwork for the CLIA waiver. We found the process seamless and effortless.
Dr. Lindstrom: I believe there are a few states where ophthalmologists can obtain CLIA waivers, but optometrists cannot, so all practitioners need to look at their own local rules and regulations (Figure 7).
Dr. Donnenfeld: Many practices have already crossed this hurdle with the use of TearLab’s osmolarity test. The
same CLIA waivers apply to the AdenoPlus test, which makes it easy for practitioners who have already been through the process.
Dr. Lindstrom: That is correct.
POINT-OF-CARE TESTINGDr. Lindstrom: Ophthalmologists have not had
much experience with point-of-care tests. Now, we have TearLab’s osmoloarity test and the AdenoPlus Test from Nicox, Inc., and several more are in the pipeline. Do we anticipate these types of tests to be a growing trend?
Dr. O’Brien: Now that we have seen impressive clini-
cal results regarding the sensitivity and specificity of the AdenoPlus test, I think we can expect to see more point-of-care technologies become available. We have already listed a number of valuable benefits of such a test: an accurate, confident diagnosis such that we can treat appropriately, and that we can also use to help pre-vent the spread of infection and to reduce unnecessary missed days of school or work.
Dr. Sheppard: I think these tests will expand logarith-mically in our practices, just as we have seen with cho-lesterol screening. At first, that was a simple test; it was fractionated. Then, triglycerides and even lipoproteins were added, and now we have a much better way to tar-get a person’s cholesterol. Likewise, we ophthalmic prac-titioners now have much better ways to target against multiple etiologies and multiple subfractionations of a red-eye patient.
That being said, I also think that as these tests become more widely accepted, we will see increased regulatory pressures—through monitoring of electronic medi-cal records and pharmacoeconomics studies from our healthcare payers—to comply with what is perceived as a preferred practice pattern.
Dr. Donnenfeld: Point-of-care tests will allow for
evidence-based diagnoses that in turn will enable better
figure 7. reimbursement details for the adenoplus test.
“Point-of-care tests will allow for evi-dence-based diagnoses that in turn will enable better treatment algorithms and more targeted therapies that will improve physicians’ standards of care and make healthcare more cost effective. That is what is exciting about having these tests available in our practices.”
—Dr. Donnenfeld

10 Supplement to CataRaCt & RefRaCtive SuRgeRy today SeptembeR 2013
Updating the differential diagnosis
treatment algorithms and more targeted therapies that will improve physicians’ standards of care and make healthcare more cost effective. That is what is exciting about having these tests available in our practices.
Dr. Holland: I agree—point-of-care tests will expand. Our aging population is a huge issue. Medicare adds 10,000 subscribers per day, and we ophthalmologists will be overwhelmed with just the surgical eye diseases—cataract, glaucoma, and the management of macular degeneration.
Many of us advocate the integrated eye care model: transferring primary and secondary eye care to optom-etrists. Having point-of-care tests such as AdenoPlus will improve the efficiency of this integrated eye care model.
Dr. McDonald: Point-of-care tests are evidence-based medicine at its best. I agree that eventually, physicians assistants or other practitioners will be making these diagnoses and writing the prescriptions, while we sur-geons spend all our time in the OR addressing the epi-demic of cataracts and macular degeneration. So, in the interest of serving the public need, I am in favor of taking some of the art out of medicine and replacing it with science-based protocols.
Moreover, I am always astonished at how quickly pathogenic resistance develops. Manufacturers spend billions of dollars to develop these drugs that have a lifes-pan of just a few years, as Dr. O’Brien explained earlier. I am waiting for the moment when R&D becomes too prohibitive, because I believe that prolonging the gap between new antibiotics will slow the development of microbial resistance.
Dr. Pepose: I think we have all been trained to practice evidence-based medicine, but what has been lacking are the in-office tools to deliver point-of-care testing with a rapid diagnosis. Now that we have this available, I think it will enhance our ability to practice high-quality ophthalmology.
Dr. Luchs: What I find really exciting is how these point-of-care tests will likely be developed over the next few years to detect other ocular-surface diseases. I predict we will see an expansion of these tests toward better diagnostic accuracy for ocular surface diseases that do not necessarily present with a red eye, such as dry eye syndrome or allergy. Where there is a significant source of diagnostic confusion for many ophthalmic technicians, having such point-of-care tests available as routine care for a majority of our patients will play a significant role in how we practice ophthalmology going forward.
Dr. Mah: I also agree that point-of-care testing is going to expand. One of the most difficult tasks for clini-cians to perform is making a diagnosis. Having a reliable
diagnosis will save a lot of clinical time for patients and practitioners alike.
Dr. Shamie: In any specialty, knowledge is power. In ophthalmology, a diagnostic test that gives accurate results can give clinicians power in the form of targeted treatments. As we all know, effective treatments make happy patients, which improves the reputation of and grows the practice.
The other point here is that point-of-care diagnostics encourages scientists and clinicians to develop consensus on diagnostic and treatment protocols. Without tools for us to work with, there is less motivation to develop con-sensus on these algorithms. I embrace any technology that helps us fine-tune how we assess and treat our patients.
Dr. Luchs: I agree. Point-of-care testing will enable
us to perform better science, because we will be able to collect patient information on the diagnosis of ocular surface disease. That in turn will give us a better cohort of patients with which to perform studies and learn even more about these diseases.
Dr. Rajpal: I absolutely agree that point-of-care test-ing is part of the future of eye care. It is necessary. I think all of our colleagues in primary care, especially pediatrics, are already accustomed to these tests, and patients are accustomed to them as well. I think our patients already expect that we should be able to offer this type of test-ing to make a correct diagnosis and treatment plan.
Dr. Parekh: Our patients demand the best care. I think we have become good at being therapeutic oph-thalmologists, but I believe we still lack in diagnostic ophthalmology. In terms of the ocular surface, for exam-ple, it has pretty much been slit-lamp examination up until now. As point-of-care tests expand, they will give adjuvant testing capabilities to make a better diagnosis.
Dr. O’Brien: I think that periodic, self-critical analysis, while sometimes humbling, is healthy. Over the past decade, first with dry eye, then blepharitis, and now acute conjunctivitis, we have seen that perhaps our fundamental understanding and ability to clinically
“Many of us advocate the integrated eye care model: transferring primary and sec-ondary eye care to optometrists. Having point-of-care tests such as AdenoPlus will improve the efficiency of this inte-grated eye care model.”
—Dr. Holland

SeptembeR 2013 Supplement to CataRaCt & RefRaCtive SuRgeRy today 11
Updating the differential diagnosis Updating the differential diagnosis
detect common conditions in order to diagnose them accurately is less astute than we previously believed. Therefore, I think having a point-of-care test with such high sensitivity and specificity for conjunctivitis will make some fundamental breakthroughs in our ability not only to help our patients, but to understand these conditions better such as to develop treatments that will ultimately be more efficacious for our patients and avoid inappro-priate treatments that have global consequences.
Dr. Lindstrom: Thank you all for the outstanding dis-cussion of the challenges and opportunities in diagnosing acute viral conjunctivitis. The NicOx AdenoPlus test, now
available commercially, and the clinically useful Red Eye Protocol for Conjunctivitis will help clinicians more accu-rately diagnose and treat this important disease, allowing prompt and proper treatment and patient counseling. To me, this represents an important advancement in the diagnosis and management of ocular surface disease. n
1. Infectious Agents Surveillance Report 1995;16:97-98 2. Tabbara KF. Ganciclovir effects in adenoviral keratoconjunctivitis. Poster B253. Association for Research in Vision and Ophthalmology annual meeting. Fort Lauderdale, FL; 2001.3. Leibowitz HM, Pratt MV, Flagstad IJ, et al. Human conjunctivitis. Arch Ophthalmol. 1976;94:1747-1749.4. Stenson S, Newman R, Fedukowicz H. Laboratory studies in acute conjunctivitis. Arch Ophthalmol. 1982;100:1275-1277.5. O’Brien TP, Jeng BH, McDonald M, et al. Acute conjunctivitis: truth and misconceptions. Curr Med Res Opin. 2009; 25(8):1953-1961.6. AdenoPlus product information. NicOx, Inc.; 2012.7. McDonald MB. Topical ganciclovir for the treatment of herpes keratitis and epidemic keratoconjunctivitis. Paper presented at: The Hawaiian Eye Meeting 2013; January 19-25; Big Island.8. Taylor JW, Chandler JW, Cooney MK. Conjunctivitis due to adenovirus type 19. J Clin Microbiol. 1978;8(2):209-213.9. Dawson CR, Hanna L, Wood TR, Despain R. Adenovirus type 8 keratoconjunctivitis in the United States. 3. Epidemiologic, clinical, and microbiologic features. Am J Ophthalmol. 1970;69(3):473-480.10. Romanowski EG, Pless P, Yates KA, Gordon YJ. Topical cyclosporine A inhibits subepithelial immune infiltrates but also promotes viral shedding in experimental adenovirus models. Cornea. 2005;24:1:86-91.11. Gordon YJ, Araullo-CruzT, Romanowski EG. The effects of topical nonsteroidal anti-inflammatory drugs on adenoviral replication. Arch Ophthalmol.1998;116:900-905.12. Trousdale MD, Barlow WE, McGuigan LJB. Assessment of diclofenac on herpes keratitis in rabbit eyes. Arch Ophthalmol. 1989;107(11):1664-1666.
For more information about the AdenoPlus test or for help obtaining a
CLIA waiver, call 855.my.Nicox