Embed Size (px)
Citation preview
VOL. 98-B, No. 1, JANUARY 2016 81
UPPER LIMB
Treatment of nonunions in fractures of the humeral shaft according to the Diamond Concept
M. Miska,S. Findeisen,M. Tanner,B. Biglari,S. Studier-Fischer,P. A. Grützner,G. Schmidmaier,A. Moghaddam
From Trauma and Reconstructive Surgery, Center for Orthopedics, Trauma Surgery and Spinal Cord Injury, Heidelberg University Hospital, Heidelberg, Germany
M. Miska, MD, Resident S. Findeisen, Medical Student M. Tanner, MD, Consultant G. Schmidmaier, MD, PhD, Chairman A. Moghaddam, MD, PhD, Consultant, Trauma and Orthopaedic Surgery, Trauma and Reconstructive Surgery, Center for Orthopedics, Trauma Surgery and Spinal Cord InjuryHeidelberg University Hospital, Schlierbacher Landstraße 200a, 69118 Heidelberg, Germany.
B. Biglari, MD, Consultant S. Studier-Fischer, MD, Consultant P. A. Grützner, MD, PhD, Chairman, Trauma and Orthopaedic Surgery, BG Trauma Center Ludwigshafen, Unfallchirurgische KlinikUniversity of Heidelberg, Ludwig-Guttmann-Straße 13, 67071 Ludwigshafen am Rhein, Germany.
Correspondence should be sent to Dr Med M. Miska; e-mail: [email protected]
©2016 The British Editorial Society of Bone & Joint Surgerydoi:10.1302/0301-620X.98B1.35682 $2.00
Bone Joint J2016;98-B:81–7.Received 20 December 2014; Accepted after revision 14 August 2015
MethodsBetween 2005 and 2012, 50 patients (23 female, 27 male) with nonunion of the humeral shaft were included in this retrospective study. The mean age was 51.3 years (14 to 88). The patients had a mean of 1.5 prior operations (SD 1.2;1 to 8).
All patients were assessed according to a specific risk score in order to devise an optimal and individual therapy plan consistent with the Diamond Concept. In 32 cases (64%), a change in the osteosynthesis to an angular stable locking compression plate was performed. According to the individual risk an additional bone graft and/or bone morphogenetic protein-7 (BMP-7) were applied.
ResultsA successful consolidation of the nonunion was observed in 37 cases (80.4%) with a median healing time of six months (IQR 6). Younger patients showed significantly better consolidation. Four patients were lost to follow-up. Revision was necessary in a total of eight (16%) cases. In the initial treatment, intramedullary nailing was most common.
DiscussionThe use of locking compression plates in combination with autologous cancellous bone graft has been shown to be a safe and effective treatment. In more complex cases, the use of the Masquelet technique and BMP-7 may be indicated at the first revision operation.
Take home message: Our results suggest the Diamond Concept is a successful treatment strategy for nonunions of the humeral shaft.
Cite this article: Bone Joint J 2016;98-B:81–7.
Nonunion after fractures most often appears inthe leg and is less common in humeral fractures.Despite major advances in operative techniquesand the design of implants for osteosynthesis, inhumeral fractures, the rate of nonunion of thehumeral shaft is still reported to range from 3%to 5% of all operatively treated fractures.1,2
Whilst there may be some consensus on thenature of operative treatment in general, thechoice of the fixation device (plate vs nail) is stilldebated.3 The rate of nonunions after non-oper-ative treatment is higher and described as up to23% in literature.4-6 There are several local andsystemic factors known to disrupt the complexprocess of bone healing, leading to nonunion,which may include insufficient stabilisation,extensive soft-tissue trauma with compromisedvascularisation, high age, comorbidities (diabe-tes, rheumatoid arthritis, osteoporosis), medica-tion (steroids, NSAIDs) and smoking.7-11 Oftenthere is a multifactorial origin to nonunion.7
In response to the multifactorial origin ofnonunion, the Diamond Concept for treatmentwas developed and described by Giannoudis,Einhorn and Marsh12 and Giannoudis et al.7
The nonunion is evaluated according to thefollowing criteria:
- osteogenic cells,- osteoconductive scaffolds,- mechanical environment,- growth factors,- vascularity.By identifying missing factors in each
patient, an ideal strategy for treatment may bedevised. A reasonable combination of biologi-cal and biomechanical approaches may greatlyimprove outcome.
In this study, we present our results from thetreatment of nonunions of fractures of thehumeral shaft according to the Diamond Con-cept. The aim of this study was to assess thesuccess of nonunion treatment according to the

82 M. MISKA, S. FINDEISEN, M. TANNER, B. BIGLARI, S. STUDIER-FISCHER, P. A. GRÜTZNER, G. SCHMIDMAIER, A. MOGHADDAM
THE BONE & JOINT JOURNAL
criteria outlined in the Diamond Concept, in order todevelop an individualised plan for each patient, and also toreveal risk factors specific for fractures of the humeral shaftleading to nonunion.
Patients and MethodsPatients. In total, 50 patients (23 female, 27 male) whowere surgically treated for 50 nonunions involving thehumeral shaft in two trauma centres from 2005 to 2012,were included in this retrospective study. This study wasapproved by the institutional review board of Rheinland-Pfalz, “Ethikkommision bei der LandesärztekammerRheinland-Pfalz,” (No. 837.141.08 (6138)) and the ethicscommission of the University of Heidelberg (No. S-532/2011). Patients were considered for the study who had aradiologically detectable nonunion after fracture of thehumeral shaft and who developed a nonunion followingprevious treatment. A nonunion was defined when no heal-ing occurred within six months or strong evidence of ther-apy failure (e.g. instability, infection) without any signs ofimprovement or a critical size gap was present independentof a fixed period of time. Radiological criteria of a nonun-ion were the insufficient bridging of a bone gap, no pro-gress in callus formation and loss of bone alignment. Allpatients were assessed in the same way, using a standard-ised study protocol and were supervised and treated by onemain observer (AM). Exclusion criteria included patients
younger than 18 years, patients unable to give an informedconsent for study and patients with a high risk for electivesurgical treatment (American Society of Anesthesiologists(ASA)13 grade > 3). The mean age at operation for traumawas 50.3 years (standard deviation (SD) 18.4; 14 to 87) and51.3 years (SD 20; 14 to 88) at operation for establishednonunion. A total of 33 patients had one prior operationfor treatment of the fracture, ten patients had two priorrevision procedures, four patients had three prior revisions,one patient had four prior and one patient had eight priorrevisions (Table I). These included internal plate fixation(n = 12), antegrade nailing (n = 17), retrograde nailing(n = 14) and closed retrograde bundle nailing (n = 6). Onepatient underwent initial conservative treatment. In sixpatients an unsuccessful change of osteosynthesis had beenundertaken previously, in three patients with cancellousbone grafting. Four patients underwent revision because ofinfection.
The mean time period from trauma to nonunion surgeryin our clinics was 10.9 months (2 to 53).
In total, two patients had suffered a grade 1 open frac-ture, one patient a grade 2 open fracture, and one patient agrade 3 open fracture.14 In all 13 patients had nerve injuriesin the affected limb (26.0%), affecting the radial nerve in12 patients and the median nerve in one. There was a his-tory of current or previous smoking in 14 patients while 36patients were non-smokers. The mean body mass index(BMI) was 28.8 (20.9 to 43.2). Table II shows the comor-bidities of the cohort.Estimation of individual risk scores. The individual risk fordeveloping a nonunion was estimated using the score devel-oped by Moghaddam et al.15 The score gathers specificparameters regarding the localisation of the fracture withaccompanying injuries of the nerves and soft tissues andadditional patient related risk factors. Risk factors taken intoaccount are medication like NSAIDs and bisphosphonates,the presence of diabetes and, with high impact, the smokerstatus. These parameters add to a total point value leading toa risk classification of the patients, divided in low riskpatients with < 10 points, medium risk patients with 10 to 20points and high-risk patients with > 20 points. In 22 patients(44.0%) a low risk score (type 1) applied, 17 patients(34.0%) had a medium risk (type 2), and 11 patients(22.0%) a high risk (type 3). The median individual riskscore in the patient cohort was ten points (6 to 31) (Table II).
Table I. Characteristics of the patient with humeral nonunion
Age (trauma) Risk score (points)
Previous surgeries (n)
Time† trauma to operation* Time† to heal Follow-up time
Max. 87 Max. 31 8 53 23 29Min. 14 Min. 6 0 2 1 11Mean 50.3 Median 10 1 6 6 12SD 18.4 IQR 13 1 7 6 0
* Nonunion operation in our clinics † Time (mths). Time to heal depends on all patients with consolidated nonunions after our treatmentSD, standard deviation, IQR, interquartile range
Table II. Comorbidities in the patient cohort
Comorbidities Patients (n) %
Obesity 15 30Heart diseases 9 18Diabetes mellitus 6 14Back pain 6 12Other 5 10Gastricdiseases 4 8Mental disorders 4 8Thyroid gland disorders 3 6Renal diseases 3 6Liver diseases 3 6Hypertension 2 4Hypercholesterolemia 2 4Respiratory diseases 2 4Haematological disorders 1 2Cancer 1 2Osteoarthritis 1 2

TREATMENT OF NONUNIONS IN FRACTURES OF THE HUMERAL SHAFT ACCORDING TO THE DIAMOND CONCEPT 83
VOL. 98-B, No. 1, JANUARY 2016
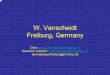
Surgical treatment of nonunions. Each fracture was evalu-ated for individual risk, indications for revision surgery,and the need for osteoinductive and/or osteogenic additivesaccording to the Diamond Concept (Fig. 1). In fractures
with insufficient stability at the primary osteosynthesis butwere considered either low risk or moderate risk, a singlerevision of the osteosynthesis was made (Fig. 2). Cancellousbone grafting was performed to fill bone defects after
Nonunion
Biomechanical instability only
Yes No
NoYes YesNo
Change of osteosynthesis(e.g. compression plate)*
High risk> 20 p.**
Local debridement Debridement and local application of bone graft (e.g. RIA)
and BMP-7*
Debridement, shortening, local application bone graft
(additional BMP-7 application by risk score > 20 p.**)*
Two-step procedure (Masquelet) with bone
graft and BMP-7*
Defect > 2 cm or 5 cm²
Fig. 1
Our treatment concept for nonunions of the humeral shaft. *According to the Diamond Concept. In cases with infection/osteitis, we generally performed a two-step-procedure with change of osteosynthesis. **According to the individual riskscore for developing a nonunion.
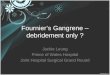
Fig. 2a
A 30-year-old male patient with a nonunion six months after retrograde nailing of a fracture of the humeral shaft (a).b). Necrotic bone was debrided and osteosynthesis was converted to a locking compression plate. c) The radiographobtained six months after revision surgery shows the healed fracture with complete bridging of the defect.
Fig. 2b Fig. 2c

84 M. MISKA, S. FINDEISEN, M. TANNER, B. BIGLARI, S. STUDIER-FISCHER, P. A. GRÜTZNER, G. SCHMIDMAIER, A. MOGHADDAM
THE BONE & JOINT JOURNAL
debridement of the nonunion. In large defects where noshortening was possible (> 2 cm), and especially when devi-talised tissue could be detected, bone morphogenetic pro-tein-7 (BMP-7) (OP-1, Osigraft, Olympus Biotech, Lyon,France) was applied. Complex cases with infection andosteitis underwent a two-stage Masquelet-procedure16,17 todebride the necrotic bone and induce a vascularised mem-brane (Fig. 3). BMP-7 was used in high risk patients and inpatients after one previous failed attempted treatment ofthe nonunion.
The nature of the techniques applied for each nonunionare outlined in Table III. Revision of the existing osteo-synthesis was performed in 45 patients (90.0%), with con-version to locking compression plates (LCP, Johnson &Johnson, New Brunswick, New Jersey) in 32 patients(64%). Whenever possible, broad 4.5 mm LCP with at leastthree angular stable screws in the proximal and distal frag-ment were applied. Cancellous bone was taken from theiliac crest or via reaming/aspiration of the femoral shaft(Reamer Irrigator Aspirator (RIA) system, Johnson &Johnson, New Brunswick, New Jersey). In larger defects,synthetic bone substitutes were used to increase the volumeof the graft to enabling adequate filling of the defect.
The mean Moghaddam risk score15 in the group of ninepatients (18.0%) treated with BMP-7 was 16.5 points
(SD 9.5). Patients treated without BMP-7 (82.0%) had amean individual risk score of 12.6 points (SD 6.9).Follow-up. Regular follow-up examinations were per-formed six weeks, three, six, nine and 12 months after dis-charge from hospital and included a clinical examinationand plain radiographs in two planes. If necessary, follow-upexaminations were continued for longer than 12 months.CT-scans were performed, when bone bridging could notclearly be detected via radiographs. A fracture wasdefined as successfully healed when fusion with bonebridging was observed in three -quarters of the circumfer-ence of cortical bone, and the patient reported they couldload the affected limb without pain. When no progress inbone healing could be detected over a period of one yearafter surgery or complications occurred, revision surgerywas performed. Statistical analysis. Descriptive statistics for normally dis-tributed variables are reported as mean and SD, otherwisemedians and interquartile ranges (IQR) have been calcu-lated. Data analyses were performed with Microsoft Excel2003 (Microsoft, Redmond, Washington) and SigmaPlot12 (Systat Software, Chicago, Illinois) using the Rank SumTest for comparison of groups regarding patients’ age andrisk score. A p-value of < 0.05 was considered statisticallysignificant.
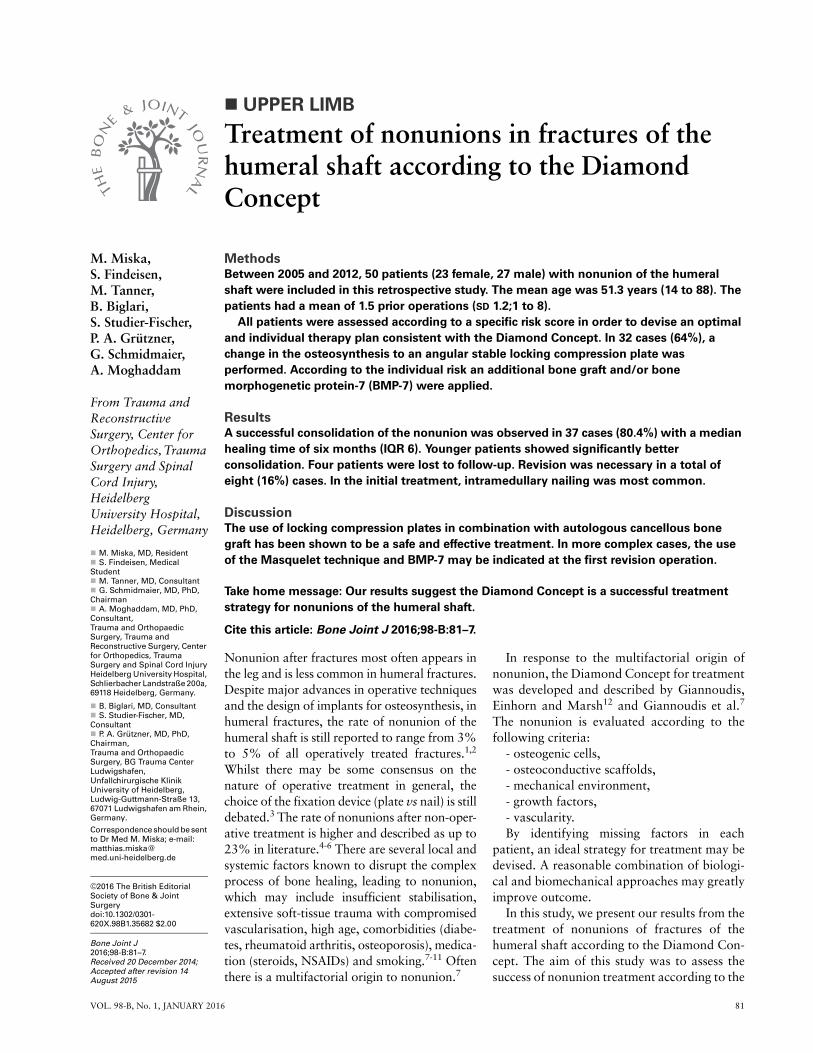
A 34-year-old female patient with a fracture of the humeral shaft initially treated with plate fixation. a) An infection of the plate withfistulas and nonunion of the fracture occurred four months post-operatively. b) The plate was removed, the wound was debrided andgentamycin-polymethyl methacrylate bead chains and a cement inlay were inserted (step 1 of the Masquelet procedure), while thefracture was stabilised with an external fixation device. c) Two months later, the antibiotic bead chains and the cement were removed,the defect was filled with cancellous bone grafted via the Reamer Irrigator Aspirator, augmented with BMP-7, and stabilised with alocking compression plate (step 2 Masquelet). The radiograph at one year follow-up shows the successfully healed fracture.
Fig. 3b Fig. 3cFig. 3a
Table III. Operative treatment of nonunions
Method of treatment Patients (n) %
Angular stable plate 12 24 Angular stable plate + cancellous bone 28 56 Angular stable plate + BMP-7 3 6 Angular stable plate + cancellous bone + BMP-7 6 12 Reaming of the humeral shaft + nailing 1 2 Total 50 100
BMP, bone morphogenetic protein

TREATMENT OF NONUNIONS IN FRACTURES OF THE HUMERAL SHAFT ACCORDING TO THE DIAMOND CONCEPT 85
VOL. 98-B, No. 1, JANUARY 2016
ResultsSuccessful healing could be detected in 37 patients after amedian time period of six months (1 to 23). In ninepatients, there was no healing of the fracture after a mini-mum observation period of 12 months. Four patients werelost to follow up. Median follow-up time was 12 months(11 to 29). The rate of healed fractures from those whoattended follow-up was 80.4%. In the group of patientswho received BMP-7 (n = 9), one patient was lost to follow-up. For the remaining eight patients, consolidation wasobserved in six fractures. In the other two patients, oneneeded revision surgery after post-operative formation of ahaematoma, and one (a high risk patient) progressed to ashoulder joint arthroplasty. This represents a successful rateof healing of 75% (6/8) in the BMP-7 group.
Patients with successful bone healing were significantlyyounger (mean 46.6 years; SD 17.5 years) than patientswith persisting nonunion (mean 62.4 years; SD 16.5)(p = 0.031) (Fig. 4). There was no significant differencebetween the two groups regarding the risk score (p = 0.83).The mean risk in patients with consolidated nonunions wasslightly higher (15.1 points; SD 10.6) than in patients with-out bone union (13.9; SD 7.8).
Revision surgery was necessary in eight patients (16%).Major complications were implant breakage in three cases,plate cut-out in two cases, post-operative haematoma intwo patients, and re-infection in one case. Of the patientswith revision surgery three healed at subsequent follow-upafter replacement of the broken or cut-out implant (TableIV). Overall, in two patients, a prosthesis was used at revi-sion. One older patient (87 years) showed no union but astable reconstruction with the current plate despite persist-ing nonunion. Therefore no further surgery was performed
because of the patient’s age. One patient showed successfulhealing following a second revision with humeral shorten-ing. The remaining five patients with nonunion did not pur-sue further treatment under our care.
DiscussionBy following the Diamond Concept for treatment, we haveseen a bone healing rate of 80.4%. The advantage of thestudy was the inclusion of a large number of patients andapplying a standardised treatment concept for all patients.Treatment of nonunions, especially in patients with largeand complex defects and disturbed biology, remains amajor challenge in orthopaedic and trauma surgery. A lim-itation of the study was the inhomogeneity of the patients.Each fracture presented with a specific risk profile and bio-mechanical situation, requiring individualised treatmentwithin the therapeutic concept, making comparisons diffi-cult. Further limitations were the lack of a control group,no randomisation and the absence of functional outcomescores. However, to the knowledge of the authors, this isthe first documentation of a larger number of patientstreated for nonunions of fractures of the humeral shaft withstandardised data collection and analysis.
Although the overall risk of nonunion dramaticallyincreases in the presence of several risk factors,15 it is pos-sible to avoid the influence of adverse mechanical factorson bone healing. Commencing with a simple avoidablemechanical problem that leads to initial failure, a highnumber of frustrated operative treatments and complica-tions such as infections may lead to a difficult local environ-ment with disturbed biology.7 In our series we observed arate of nonunions of 63% after intramedullary nailing vs.24% after internal plate fixation for initial treatment.Bhandari et al3 did not find a difference in their meta-anal-ysis regarding randomised trials, but in non-randomisedstudies it could be shown that plate fixation had a lowerrelative risk for revision surgery. Other authors clearly pre-fer the use of plate fixation over the intramedullary nail-ing.18,19 However, larger randomised trials are necessary toclarify if this is truly the case.
Borus et al20 reported good results in the treatment ofrefractory nonunion after revision with a cancellous bonegraft and rigid compression plating in a case series of sevenpatients. McKee et al21 also described better results afterplating and cancellous bone grafting in nonunions afternailing of a fracture of the humeral shaft in comparison toa closed procedure with a simple change of the device to alocking nail in 21 cases. These reports seem to reflect ourobservations, with angular stable plating proving be a reli-able treatment in nonunions of the humeral shaft and pro-viding a stable biomechanical environment. Successfultreatment has been described using circular external fixa-tors in 16 patients with a nonunion of the humeral shaft.22
Although this technique provided a good outcome, treat-ment with an external fixator for at least three and up to 17months is very demanding for the patients.
Union Nonunion
Ag
e (y
rs)
0
15
30
45
60
75
90
Fig. 4
Risk Score according to patients’ age. The boxes represent the patientswithin the lower and upper quartile (enclosing the middle half of thesample) and the sample median, as the horizontal line. The whiskersrepresent the sample maximum and minimum, excluding outliers rep-resented by the black dots (patients with the values between 1.5 and 3x interquartile range from the 75th or 25th percentile). Patients whoremained ununited healing after our treatment had a significantlyhigher age (p = 0.031).

86 M. MISKA, S. FINDEISEN, M. TANNER, B. BIGLARI, S. STUDIER-FISCHER, P. A. GRÜTZNER, G. SCHMIDMAIER, A. MOGHADDAM
THE BONE & JOINT JOURNAL
In addition to biomechanical problems, another reasonfor developing a nonunion is the individual risk of theaffected patient. In the applied risk score we classified thepatients according to the type of the fracture, soft-tissuedamage and specific risk factors.15 Only 11 patients (22%)were in the high risk group at initial trauma vs 39 patients(78%) in the low and middle risk group. Furthermore, wewere not able to show any significant difference in distribu-tion of risk scores between patients who progressed tounion and patients whose fracture remained ununited. Thismay be due to the small number of patients with nonunionsbut may also suggest that mechanical stabilisation is a moreimportant factor in fractures of the humeral shaft than wasinitially thought.
Despite the small number of patients in the nonuniongroup, the patients’ age was significantly associated withoutcome (p = 0.031). While young patients with good gen-eral healing potential showed high rates of consolidation,older patients showed higher rates of nonunion independ-ent of their risk score. These findings are in line with theresults of previous studies.23-25
Outcome after nonunion treatment. In 37 fractures, we sawsuccessful healing after multimodal treatment for nonun-ions. The rate of union was 80%, which is a very encourag-ing when considering the patients’ long history. We saw amoderate rate of complications with eight patients havingto undergo revision surgery. This may seem high but thecohort itself mainly included cases with previous revisionoperations, most of them multiple in nature, and manycomplex cases. In these, bone regeneration was compli-cated not only by local factors like scar tissue and insuffi-cient vascularisation but also by systemic factors,comorbidities and low bone quality, and decreased stabilityof the osteosynthesis. Patients were generally over 50 yearsold, representing an age when biologically some limitationsof bone regeneration are present.11,26 We also observedpost-operative hyperthermia and flushing at the applicationsite approximately five days after the use of BMP-7. Thislocal reaction is in accordance with previously describedfindings and seems to the result of an aseptic inflammatoryreaction with the protein.7,27 The median interval fromnonunion therapy to consolidation of the fracture was sixmonths. Possibly this reflects the difficult vascular environ-ment in nonunion. Large defects, especially in high riskpatients, obviously need longer to heal than simple frac-tures.27 Combination of autologous bone graft and BMP-7. In Ger-many, the clinical application of BMP-7 as a drug (OP-1,
Osigraft,) has been approved for tibial shaft nonunionssince 2001. Its use in other sites is ‘off label’ and is consid-ered the responsibility of the attending surgeon.28-31 BMP-7 requires adequate blood perfusion and a vital bone struc-ture to enable complete expression of the bone growth fac-tor.7,32 Accordingly adequate surgical debridement andresection of the necrotic and devitalised tissue at the non-union are essential. The use of cancellous bone grafts to filllarger defect gaps increases primary stability. Additionally,cancellous bone serves as a rich cellular environment forBMP-7 and is assumed to increase the local adhesion ofBMP-7 in the bone defect.7,32-36 The osteoinductive effectof BMP-7 has been shown in several studies.32,27-29,31,37
Latterly we have preferred the use of RIA as a source forautologous bone rich in mesenchymal stem cells from ream-ing material with a higher osteogenic potency than cellsobtained from the iliac crest.38 In some humeri we com-bined autologous bone with synthetic bone replacementmaterial to augment the volume of larger defects. Howevera large multi-centre randomised trial would be needed todetermine any superiority in outcome after use of BMP-7 inthe treatment of nonunions compared with a control group.
In conclusion, in our series the use of angular stable lock-ing compression plates in combination with an autologouscancellous bone graft has been shown to be a safe and effec-tive treatment method for nonunion of the humeral shaft.The Masquelet technique in combination with BMP-7 pro-vided good results in more complex cases. The analysis ofthe individual risk profile and missing factors for eachpatient is probably the most important consideration indefining the optimal treatment. The Diamond Conceptseems to be a successful way to define treatment for nonun-ions of the humeral shaft.
Supplementary materialA table showing the score to estimate the individualrisk of patients for delayed union of long bone frac-
tures is available alongside the online version of this articleat www.bjj.boneandjoint.org.uk
Author contributions:M. Miska: Writing the paper, Performed surgeries, Patient recruitment, Datacollection, Data analysis.S. Findeisen: Writing the paper, Patient recruitment, Data collection, Dataanalysis.M. Tanner: Performed surgeries, Paper correction.B. Biglari: Patient recruitment, Data collection.S. Studier-Fischer: Performed surgeries, Patient recruitment, Data collection.P. A. Grützner: Study design, Performed surgeries.G. Schmidmaier: Study design, Performed surgeries.A. Moghaddam: Study design, Performed surgeries, Writing the paper, Patientrecruitment, Data collection, Data analysis.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
This article was primary edited by G. Scott
References1. Rommens PM, Kuechle R, Bord T, et al. Humeral nailing revisited. Injury
2008;39:1319–1328.2. Kontakis GM, Papadokostakis GM, Alpantaki K, et al. Intramedullary nailing for
non-union of the humeral diaphysis: a review. Injury 2006;37:953–960.
Table IV. Post-operative complications
n % n healed
Implant breakage 3 6 1 (1 case lost)Plate cut-out 2 4 2Haematoma 2 4 0Re-infection 1 2 0Total 8 16 3

TREATMENT OF NONUNIONS IN FRACTURES OF THE HUMERAL SHAFT ACCORDING TO THE DIAMOND CONCEPT 87
VOL. 98-B, No. 1, JANUARY 2016
3. Bhandari M, Devereaux PJ, McKee MD, et al. Compression plating versusintramedullary nailing of humeral shaft fractures--a meta-analysis. Acta Orthop2006;77:279–284.
4. Denard A Jr, Richards JE, Obremskey WT, et al. Outcome of nonoperative vsoperative treatment of humeral shaft fractures: a retrospective study of 213 patients.Orthopedics 2010;33:33–38.
5. Rutgers M, Ring D. Treatment of diaphyseal fractures of the humerus using a func-tional brace. J Orthop Trauma 2006;20:597–601.
6. Toivanen JA, Nieminen J, Laine HJ, et al. Functional treatment of closed humeralshaft fractures. Int Orthop 2005;29:10–13.
7. Giannoudis PV, Einhorn TA, Schmidmaier G, et al. The diamond concept--openquestions. Injury 2008;39(suppl 2):S5–S8.
8. Moghaddam A, Muller U, Roth HJ, et al. TRACP 5b and CTX as osteological mark-ers of delayed fracture healing. Injury 2011;42:758–764.
9. Moghaddam A, Weiss S, Wolfl CG, et al. Cigarette smoking decreases TGF-b1serum concentrations after long bone fracture. Injury 2010;41:1020–1025.
10. Zimmermann G, Henle P, Kusswetter M, et al. TGF-beta1 as a marker of delayedfracture healing. Bone 2005;36:779–785.
11. McKibbin B. The biology of fracture healing in long bones. J Bone Joint Surg [Br]1978;60-B:150–162.
12. Giannoudis PV, Einhorn TA, Marsh D. Fracture healing: the diamond concept.Injury 2007;38(suppl 4):S3–S6.
13. Keats AS. The ASA classification of physical status--a recapitulation. Anesthesiol-ogy 1978;49:233–236.
14. Oestern HJ, Tscherne H. Pathophysiology and classification of soft tissue damagein fractures. Orthopade 1983;12:2–8. (Article in German).
15. Moghaddam A, Zimmermann G, Hammer K, et al. Cigarette smoking influencesthe clinical and occupational outcome of patients with tibial shaft fractures. Injury2011;42-12:1435–1442.
16. Masquelet AC, Begue T. The concept of induced membrane for reconstruction oflong bone defects. Orthop Clin North Am 2010;41:27–37.
17. Moghaddam A, Zietzschmann S, Bruckner T, Schmidmaier G. Treatment ofatrophic tibia non-unions according to 'diamond concept': Results of one- and two-step treatment. Injury 2015;46(Suppl 4):S39–S50.
18. McCormack RG, Brien D, Buckley RE, et al. Fixation of fractures of the shaft ofthe humerus by dynamic compression plate or intramedullary nail. A prospective, ran-domised trial. J Bone Joint Surg [Br] 2000;82-B:336–339.
19. Chapman JR, Henley MB, Agel J, Benca PJ. Randomized prospective study ofhumeral shaft fracture fixation: intramedullary nails versus plates. J Orthop Trauma2000;14:162–166.
20. Borus TA, Yian EH, Karunakar MA. A case series and review of salvage surgery forrefractory humeral shaft nonunion following two or more prior surgical procedures.Iowa Orthop J 2005;25:194–199.
21. McKee MD, Miranda MA, Riemer BL, et al. Management of humeral nonunionafter the failure of locking intramedullary nails. J Orthop Trauma 1996;10:492–499.
22. Patel VR, Menon DK, Pool RD, Simonis RB. Nonunion of the humerus after failureof surgical treatment. Management using the Ilizarov circular fixator. J Bone JointSurg [Br] 2000;82-B:977–983.
23. Gruber R, Koch H, Doll BA, et al. Fracture healing in the elderly patient. Exp Ger-ontol 2006;41:1080–1093.
24. Giannoudis P, Tzioupis C, Almalki T, Buckley R. Fracture healing in osteoporoticfractures: is it really different? A basic science perspective. Injury 2007;38(Suppl1):S90–S99.
25. Gaston MS, Simpson AH. Inhibition of fracture healing. J Bone Joint Surg [Br]2007;89-B:1553–1560.
26. Tonnesen PA, Heerfordt J, Pers M. 150 open fractures of the tibial shaft--the rela-tion between necrosis of the skin and delayed union. Acta Orthop Scand1975;46:823–835.
27. Moghaddam-Alvandi A, Zimmermann G, Büchler A, et al. Results of nonuniontreatment with bone morphogenetic protein 7 (BMP-7). Unfallchirurg 2012;115:518–526. Article in German.
28. Zimmermann G, Moghaddam A, Wagner C, Vock B, Wentzensen A. [Clinicalexperience with bone morphogenetic protein 7 (BMP 7) in nonunions of long bones].Unfallchirurg 2006;109:528–537. Article in German.
29. Zimmermann G, Müller U, Löffler C, et al. [Therapeutic outcome in tibial pseudar-throsis: bone morphogenetic protein 7 (BMP-7) versus autologous bone grafting fortibial fractures]. Unfallchirurg 2007;110:931–938. Article in German.
30. Haag I. Off-Label-Use von Arzneimitteln im Krankenhaus. das Krankenhaus2011;103.
31. Moghaddam A, Elleser C, Biglari B, et al. Clinical application of BMP 7 in longbone non-unions. Arch Orthop Trauma Surg 2010;130:71–76.
32. Goldhahn J, Mitlak B, Aspenberg P, et al. Critical issues in translational and clin-ical research for the study of new technologies to enhance bone repair. J Bone JointSurg [Am] 2008;90-A(suppl 1):43–47.
33. Giannoudis PV, Kanakaris NK, Dimitriou R, et al. The synergistic effect of auto-graft and BMP-7 in the treatment of atrophic nonunions. Clin Orthop Relat Res2009;467:3239–3248.
34. Giannoudis PV, Psarakis S, Kanakaris NK, et al. Biological enhancement of bonehealing with Bone Morphogenetic Protein-7 at the clinical setting of pelvic girdle non-unions. Injury 2007;38(suppl 4):S43–S48.
35. Schmidmaier G, Schwabe P, Wildemann B, et al. Use of bone morphogeneticproteins for treatment of non-unions and future perspectives. Injury 2007;38(suppl4):S35–S41.
36. Giannoudis PV, MacDonald DA, Matthews SJ, et al. Nonunion of the femoraldiaphysis. The influence of reaming and non-steroidal anti-inflammatory drugs. JBone Joint Surg [Br] 2000;82-B:655–658.
37. Giannoudis PV, Tzioupis C. Clinical applications of BMP-7: the UK perspective.Injury 2005;36(suppl 3):S47–S50.
38. Kühlfluck P, Lessl E, Moghaddam A, et al. Reaming material: a vital source forhuman mesenchymal stem cells with high osteogenic potential. European Cells andMaterials 2013;26:15.