Embed Size (px)
Citation preview

Urbanization, Poverty and NCDs in SSA
Catherine Kyobutungi
6th INTEREST Workshop Mombasa
10th May 2012

Outline
Urbanization and poverty in African cities Population trends: global, SSA, slum growth
Health challenges in urban SSA Urban Environments and NCDs Challenges in NCD control
2

Urbanization, Poverty and Health in African Cities
Key Points – The world will remain increasingly urban – All future population growth will be in urban areas in LDC – Africa’s population will double from 1 to 2 billion by 2050 – By 2050, Africa will account for 22% of world population, up
from 15% in 2010 – In Africa, natural increase accounts for about 75% of urban
growth – Majority of urban population in Africa live in slums: very poor
livelihood and environmental sanitation conditions – Poverty, obesogenic environments and weak health systems
in urban Africa portend for a bleak future with NCD

0,35
-0,52
0,46
1,66
1,98
0,54
2,53
3,65
2,22
0,72
2,37
4,53
-1 0 1 2 3 4 5
Slum Urban Rural
World
MD
LDC
SSA
Population Growth Rate by Region and Residence, 2005-2010
Source: UNPD 2009; UNHabitat 2006

769
266 191
1.081
521
372
0
200
400
600
800
1.000
1.200
Total Pop Urban Slum
2005 2020
Projected Growth of Total, Urban and Slum Populations in SSA (In Millions)
By 2020, one in three SSA residents will live in a slum

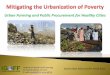
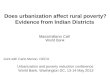
The Urbanization of Poverty
2002 estimates: National: 56%, Rural: 57%, Urban: 53%
Trends in proportion of Kenyans living in absolute poverty

Nairobi CBD
A slum, less than 10 km from the CBD
Urban Africa: Two Worlds

Health Challenges in Urban SSA
• Huge burden of infectious diseases
• Non-communicable diseases (NCD) will outstrip CD in next few decades – Increases in behavioural risk
factors (diet, alcohol, tobacco use)
– Diet: lack of dietary diversity and high use of street and fast foods; high salt consumption
– Limited access to screening and other preventive services
• In Kenya, prevalence of overweight & obesity among women of reproductive age almost doubled over a 15-year period (13% to 25%)1
•Increase more marked in urban than rural areas •In 2008: obesity & overweight in urban women was 40% c.f. 20% of rural women in Kenya 1 ; 35% and 16% in Ghana2

Health Challenges in Urban SSA • High NCD Risk
Environments – Increasing traffic
volumes – Infrastructural
development geared towards easing motorised transport – not physical activity
– High stress levels – Environmental factors
(air, water and soil pollution)
– Crime and insecurity

The four main risk factors among Nairobi slum residents
Current smoker
N %
Male 557 19.6
Female 22 0.9
Current alcohol user (a) Frequent heavy drinker (% of a)
N % %
Male 427 15.9 31.9
Female 68 2.8 34.2
Insufficient physical activity from all sources*
N %
Male 266 7.0
Female 636 26.3
Insufficient fruit and vegetable intake High salt intake
N % N %
Male 1,438 61.0 1,100 40.4
Female 1,352 48.2 702 31.7

CVD risk factors in 2 Nairobi slums (2)
Categories Overweight Obesity
N % N %
Male 400 11.5 59 1.4 Female 628 24.2 358 10.4
Hypertension Diabetes
N % N %
Male 498 12.0 141 4.1 Female 550 12.7 166 4.9 ASP 18.4 5.7

People in risk group
People coming to screening
People aware of possibility of screening
People aware of risk on
hypertension
~
-50-75%
-50-75%
Reduced risk on CVD /
Controlled BP
People being long-term compliant
-80% ~ ~ -60% ~
~
People aware and
understanding of diagnosis
People seeking treatment
People getting right medicines / lifestyle advice
People taking meds for 1st time / Adopt
healthier lifesty
People diagnosed
with ’medium/ high’ risk
People adequately diagnosed with risk
-x% ~%
People change lifestyle
People informed about
need for lifestyle change
People diagnosed with ’low’
risk
Leakages in a CVD prevention (HPT control) continuum
Current hypotheses for key causes of leakages
Source: CVD study, WDF study, APHRC expert opinion
Population screening Population intervention Patient intervention
People aware of
risk People aware of preventive
services
People using preventive
services
People seeking
treatment
People being compliant long term

Addressing the leakages: The SCALE-UP model
Note: All costs are in USD
Elements of model
Cost
s Pe
ople
Prog mgmt
Variable Fixed
Investments
Variable pp
Subtotal
Total yearly costs
Total costs (10 yrs)
Awareness Access High risk Incentive Consultation
+ Meds Incentive Consultation
+ Meds
• Baraaza • Religious
Radio
• Door 2 Door campaign by CHW
• Patients with high risk
• Voucher for patient
• Incentive CHW
• Consultation • Medication
• Consultation • Medication
Average running
costs yr 2–10
13,884
0 665 278
2,042 4,979
11,639
0 0 0
2,756 0 0
3,048 0
231
4,454 4,305
0
10,908 1,666
0
0 0.32 0 2.89 3.20 4.67 17.16
943 18,660 0 2,756 3,279 8,759 12,574
60,855 27,160
305,290
Total costs yr 1
46,971
Total population
• Screening age above 35
Leakage 85% 90% 21% 80% 100% 65% 100% 21%
# of ppl enrolled 7,414 6,302 5,672 1,191 953 953 619 34,491
- - -
-
-
Awareness Access to screening
Seeking treatment
Long term compliance
• Train trainer • SMS • Discount
for com- pliance
• Compliance bonus CHW
% of people moving
on to next step
65% compliant in year 1

Summary
• Rapid Urbanization in SSA • Urbanization gone wrong • Urban environments – high risk for NCD • Weak health systems • Challenges in risk reduction across the
continuum of care • Many lessons to learn from the management
of HIV