Embed Size (px)
Citation preview

Urinary steroid metabolites in a case of florid Ectopic Cushing’s syndrome and clinical correlations
Angelos Kyriacou,1 Karolina M. Stepien,2 Basil Issa1
1Department of Endocrinology & Diabetes, 2Department of Clinical Biochemistry, University Hospital of South Manchester (UHSM), Manchester, UK
AbstrAct
A 51-year old woman was admitted with multiple cerebral, pulmonary and intra-abdominal abscesses. The combination of apparent immunosuppression, obesity, diabetes mellitus, hyper-tension, hypokalaemia, osteoporotic fractures and bilateral shoulder avascular necrosis led to a clinical diagnosis of Cushing’s syndrome (CS). This was biochemically confirmed as follows: midnight serum cortisol 4275 nmol/L (60-250), non-suppressed overnight dexamethasone sup-pression test, raised salivary cortisol 716 nmol/L (5-46) and ACTH 639 ng/L (0-46). Urinary free cortisol was elevated >75,000 nmol/L (<165). Urinary steroid metabolites measured by Gas Chromatography Mass Spectrometry were markedly increased: tetrahydrocortisol (THF) 219024 µg/24h and tetrahydrocortisone (THE) 88848 µg/24h. The (THF+5αTHF)/(THE) ratio was 2.8 (≤1). Pituitary MRI was unremarkable and whole body CT scanning showed a thymic tumour and bilateral adrenal hyperplasia. Urinary 5HIAA was marginally raised with a normal chromogranin A. She underwent a thymectomy which confirmed a ‘paraganglioid’ variant of a thymic carcinoid tumour. We describe a case of ACTH-secreting thymic carcinoid that presented with florid clinical and biochemical features of CS, but no carcinoid syndrome. The (THF+5αTHF)/(THE) ratio is reported to be a useful indicator in differentiating the aetiolo-gies of CS, although this was not the case in our patient. In this article we examine the degree to which the various urinary steroid metabolites were raised in this patient with florid CS and compare them with some normative data obtained from patients with either Cushing’s disease or the normal population. We hereby postulate that steroid metabolomics profiling may be helpful in establishing the differential diagnosis of CS.
Key words: Thymic carcinoid, Cushing’s syndrome, ACTH, Urinary glucocorticoid metabolites
Case report
HORMONES
Address for correspondence:Angelos Kyriacou, Southmoor Road, Wythenshawe, Manchester, UK, M23 9LT, E-mail: [email protected]: 21-07-2016, Accepted: 01-09-2016
and 4.44 per 100,000 persons per year in Norway and the USA, respectively,1 although the incidence of these tumours appears to have gradually been increasing.2 Approximately 85% of NETs arise from the GI tract, 10% in the lungs, with the remainder in various organs such as the thymus.3 Thymic carcinoids have a distinct expression pattern characterized by deregulation of
INTRODUCTION
NETs are rare tumours with an incidence of 3.24

A. KyRIACoU ET AL
many bio-functions including abnormal proliferation and differentiation signals, which may be involved in the development of NETs. other abnormalities, like activation of neuropeptide signalling and inhibition of immune responses, may explain the hormonal disorders and immunity defects evident in ectopic ACTH syndrome.4 Thymic carcinoids are rare tumours that exhibit a predilection for men, with a 3:1 male to female ratio.2,5 In 30% of cases these tumours are usually an incidental finding on routine radiography. The tumours often show cytological and architectural features of neuroendocrine differentiation, hence can be positive for CD56, neuron-specific enolase, chro-mogranin, somatostatin and synaptophysin.5
Most carcinoids are benign in behaviour, but thymic carcinoids display a much more aggressive phenotype and can be associated with ectopic ACTH syndrome, which in itself seems to be linked with poorer prog-nosis.6-7 It is unclear whether this latter correlation is due to metabolic complications secondary to Cush-ing’s Syndrome (CS) or to inherently more aggressive tumour behaviour.
Urine steroid metabolomics make use of the dif-ferentiating expression of various steroid metabolites (measured by mass spectrometry) in order to try and distinguish between various conditions. It is an evolving field and has been applied for example to discriminate between benign and malignant adrenal tumours8 for early detection of recurrence of adreno-cortical carcinoma9 and for the differential diagnosis of primary hyperaldosteronism.10 Here, we present a patient with ectopic Cushing’s syndrome (CS) where urine steroid metabolites were measured in an effort to determine whether there exists a specific metabo-lomic fingerprint for this rare condition.
CASE REPORT
A 51-year old lady was admitted with multiple cerebral, pulmonary and intra-abdominal abscesses. She was referred to the endocrine team because of newly-diagnosed type 2 Diabetes Mellitus. The com-bination of apparent immunosuppression, obesity (BMI 33.2 kg/m2; 18-25), diabetes mellitus (HbA1c 8.5%; ≤6.5%), hypertension (average blood pressure 154/90 mmHg), hypokalaemia (K+ 2.9 mmol/L; 3.5-5.0), osteoporotic fractures and bilateral shoulder
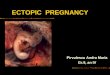
avascular necrosis (BSAN) led to a clinical diagnosis of Cushing’s syndrome (CS). This was biochemically confirmed by non-suppressed cortisol in an overnight dexamethasone suppression test, midnight serum cortisol 4275 nmol/L (60-250), raised midnight sali-vary cortisol 716 nmol/L (5-46) and ACTH 639 ng/L (0-46). Urinary free cortisol (UFC) was elevated in excess of 75,000 nmol/24h (<165) on two occasions. Urinary steroids metabolites were markedly increased (Table 1) and the relevance of these metabolites to the steroid metabolic pathway can be seen in Figure 1. In particular, tetrahydrocortisol (THF) and tetrahy-drocortisone (THE) were markedly raised at 219024 µg/24h (435-1709) and 88848 µg/24h (997-3870), respectively, with a (THF+5αTHF)/(THE) ratio also raised at 2.8 (≤1) (Table 1).
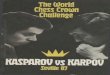
Given the markedly raised ACTH, cortisol and cortisol metabolites in association with hypokalaemia ectopic CS was more likely than Cushing’s disease; indeed, given the computed tomography (CT) and positron emission tomography (PET) CT imaging ap-pearances (Figure 2) of a thymic tumour and normal pituitary magnetic resonance imaging, a diagnosis of ectopic CS due to a thymic neuroendocrine tu-mour (NET) was reached without needing to embark on the high-dose dexamethasone suppression test, corticotrophin-releasing hormone stimulation test or bilateral inferior petrosal sinus sampling (IPSS). Urine 5-hydroxyindoleacetic acid (5HIAA) was marginally raised at 55 μmol/24h (<45) and chromogranin A was normal at 52 pmol/L (<60). octreotide scanning showed increased focal activity in the thymus. Multiple Endocrine Neoplasia type 1 (MEN1) was deemed to be quite unlikely given that the calcium was normal (2.36 mmol/L; 2.1-2.6) and there was no evidence of other NETs seen on abdominal CT imaging (which showed appearances of bilateral adrenal hyperplasia) and fasting gut peptides were within normal limits. Genetic testing was not required, especially given that our patient did not have any family history sug-gestive of MEN1.
Given that this woman presented with gross CS she required stabilization before surgical resection. This included the use of multiple and recurrent courses of potent antibiotic, antiviral and antifungal medica-tions in order to treat the underlying infections. Me-tyrapone was prescribed to treat hypercortisolaemia

Urinary steroid metabolites in a case of florid Ectopic Cushing’s syndrome and clinical correlations
Table 1. Urinary steroid metabolite levels in two separate collections of urine (µg/24h) done pre-operatively; before (testing 1) and after (testing 2) metyrapone use. Values obtained from the study of Brossaud et al for normal controls and patients with active Cushing’s syndrome are also included.20
Steroid MetabolitesTesting 1
for case patient(pre-metyrapone)
Testing 2 for case patient
(post-metyrapone)
Median values (95% CI) in
normal controls20
Median values (95%CI) in active Cushing’s disease20
Androgen Precursors (µg/24h)Androsterone 2734 1615Etiocholanolone 15835 4659Dehydroepiandrosterone 3033 58916α-dehydroepiandrosterone 1243 555-Pregnanetriol 3879 5315-Pregnanediol 3412 1783Pregnedien 6774 730Mineralocorticoids and Mineralocorticoid PrecursorsTetrahydrodehydrocorticoste-rone 4213 16125α-Tetrahydrodehydrocorticoste-rone 1084 1120Tetrahydrocorticosterone 30600 98645α-Tetrahydrodehydrocorticoste-rone 13473 43233α5β-Tetrahydroaldosterone 0 2Tetrahydrodeoxycorticostero-ne 3830 26765α-Tetrahydrodeoxycorticostero-ne 371 205Glucocorticoid PrecursorsPregnanediol 4983 14053α,5α, 17-Hydroxypregnenolone 250 4717-Hydroxypregnanolone 4588 1740Pregnanetriol 5344 2751Pregnanetriol-one 403 51Tetrahydrodeoxycortisol 56866 32292GlucocorticoidsCortisol 36716 20272 73 (25-135) 362 (180-2155)6β-OH-Cortisol 25285 17831Tetrahydrocortisol (THF) 219024 77524 2193 (809-411) 8637 (4561-37710)5α-Tetrahydrocortisol (5αTHF) 26484 4130α-Cortol 33272 34684 154 (48-313) 609 (226-3431)β-Cortol 34829 9846 243 (75-650) 965 (328-6900)11β-OH-Androsterone 7774 120911β-OH-Etiocholanolone 32316 689Cortisone 1909 1380 115 (38-193) 301 (135-619)Tetrahydrocortisone (THE) 88848 29393 2706 (1020-6124) 8561 (1742-23472)A-cortolone 13775 13722 1036 (439-1956) 2712 (1222-5392)B-cortolone 14042 4152 247 (81-570) 907 (385-3260)11-oxo-Etiocholanolone 7558 18018 oH Tetrahydrodeoxycorticosterone 114 57(THF+5αTHF)/THE 2.8 2.8

A. KyRIACoU ET AL
Figu
re 1
. Ster
oid
meta
bolic
path
way
with
the v
alues
obt
ained
from
a 24
hou
r urin
e col
lectio
n in
our
pati
ent i
n br
acke
ts (u
nits=
μmol
/24h
rs). P
lease
not
e tha
t the
re is
not
one
path
-wa
y tha
t can
inclu
de al
l ster
oid a
nd ur
inar
y ana
lytes
desc
ribed
in T
able
1. A
lso, t
his p
athwa
y illu
strate
s tha
t one
ster
oid m
etabo
lite c
an of
ten be
the p
rodu
ct of
one o
r mor
e ster
oids
in
the b
ioch
emica
l path
way.

Urinary steroid metabolites in a case of florid Ectopic Cushing’s syndrome and clinical correlations
and reduce progression of CS complications; her urinary steroid metabolite profile post-metyrapone and pre-operatively is given in Table 1. Insulin was used to manage her hyperglycaemia. Potassium sup-plements, spironolactone and ramipril were given to achieve normotension and normokalaemia. once the patient was rendered eucortisolaemic and haemody-namically and metabolically stable, she underwent thymectomy. Histology confirmed a paraganglioid variant of a thymic carcinoid tumour.
Post-operatively her 9am cortisol (off glucocorti-coids) was below 50 nmol/L, which was indicative of disease remission. Thereafter, she displayed remark-able clinical and biochemical recovery, but poorly controlled diabetes, hypertension, obesity and BSAN continued to be active problems. She has now been in remission for the past five years.
DISCUSSION
We describe a case of ACTH-secreting thymic carcinoid that presented with florid clinical and bio-chemical features of CS. Profoundly elevated cortisol concentrations were observed in saliva, serum and urine, with loss of diurnal variation. Indeed, her UFC has possibly been the highest ever described. The markedly elevated total urinary excretion of cortisol in
CS secondary to ectopic ACTH production was previ-ously described.11,12 In one case of ACTH-secreting CS, the UFC was as high as 45000 nmol/24h despite treatment with octreotide or ketoconazole.11 In a review of all thymic carcinoids over a 25-year period from the National Institute of Health (NIH) in the US, the medium and highest UFC observed were 5,890 and 18,390 μg/24hrs, respectively.13
Additionally, her detailed urine steroids analysis showed markedly high levels of cortisol and cortisone metabolites (THF and THE, respectively), which is pathognomonic for patients with CS.14 The analysis of urinary steroids metabolites was performed us-ing Gas Chromatography Mass Spectrometry (GC/MS) in the Centre for Endocrinology, Diabetes and Metabolism in Birmingham. The exact methodology has previously been described.8 The (THF+5αTHF)/THE ratio is used as an index of 11β-hydroxysteroid dehydrogenase (11β-HSD) activity and a ratio value of approximately 1 is considered as normal.15 11β-HSD involves an enzyme system that functions to catalyse the conversion of cortisol into cortisone;16-18 11β-HSD1 (relevant gene is HSD11B1 on chromosome = 1q32-q41) is present in the liver, testis, lung, adipose tissue and is a reduction enzyme that converts cortisone to cortisol; 11β-HSD2 (relevant gene is HSD11B2 on chromosome 16q22) is found in the kidneys and placenta and is a dehydrogenase enzyme that converts cortisol to cortisone. The (THF+5αTHF)/THE ratio has previously been shown to be significantly increased in CS regardless of aetiology. However, it has been observed as being markedly higher in patients with ectopic ACTH syndrome as compared to pituitary-dependent CS (4.12 vs. 1.49, respectively; p<0.01) and inversely correlated with serum potassium levels.14 In our case, the cortisol metabolites ratio was 2.8, which fell between the results mentioned above. To our knowledge, there are no definite cut-off values for (THF+5αTHF)/THE ratio that can differentiate between Cushing’s disease and ectopic ACTH syn-drome. There is a degree of overlap between these conditions, therefore the (THF+5αTHF)/THE ratio should be interpreted with caution. Indeed, it has been noted that a ratio between 1 and 3 may still be consid-ered as normal. Therefore, based on this value only it is impossible to make a diagnosis of CS or indeed to ascertain its aetiology (Norman Taylor, personal
Figure 2. PET CT of the thorax indicating a large tumour in the anterior mediastinum (arrow) consistent with a thymic NET.

A. KyRIACoU ET AL
communication). The quantity of cortisol excretion and the rate of its excretion are very individual and vary between cases; the more florid CS is, the higher the UFC. Hence in our practice, we often interpret the (THF+5αTHF)/THE ratio along with the UFC result. The raised ratio of 5β-THF to 5α-THF (8.3 in this case) is of more clinical use and is usually indicative of CS (Norman Taylor, personal communi-cation). Moreover, the (THF+5αTHF)/THE ratio has also been demonstrated to be clinically important in the diagnosis of hypertension caused by congenital absence of 11β-HSD2 or inhibition of the enzyme after liquorice ingestion.19 With excessive cortisol secretion, 11β-HSD2 can be saturated, causing an increase in the urine free cortisol to cortisone ratio and subsequently in the THF:THE ratio.
The inversion of the THF/THE ratio in our patient (Table 1) is likely due to a combination of increased expression of 11β-HSD1 in adipose tissue and the florid hypercortisolaemia per se. Most of the glu-cocorticoid metabolites were profoundly decreased following treatment with metyrapone. It was surpris-ing, however, that the inhibition of 11β-hydroxylase did not increase upstream metabolites such as the androgens and tetrahydro-11-deoxycortisol (Table 1). The mechanism of this remains unclear.
our case demonstrates not only that glucocorti-coid metabolites are markedly increased in Ectopic Cushing’s Syndrome but also that mineralocorticoid and sex hormone metabolites are significantly in-creased as well (Table 1). The various metabolites were increased to varying degrees in our own patient (Table 1). A recent study has examined urinary glu-cocorticoid metabolites to provide biomarkers for the classification of adrenal incidentalomas and has provided median values for 48 normal controls and 26 patients with active (pituitary) Cushing’s disease.20 With reference to these data, glucocorticoid metabolites were massively increased in our patient compared to normal control values (ranging from a ratio of 13 to 216 for α-cortolone and α-cortol, respectively) and increased even when compared with patients with active Cushing’s disease (ranging from a ratio of 5 for α-cortolone and cortisone and 101 for α-cortol) (Table 2). The degree of increase in the various glu-cocorticoid metabolites in our patient followed the same order whether the values were compared to
normal controls or to Cushing’s disease and obeyed the following incremental sequence: α-cortolone, THE, β-cortolone, THF, β-cortol and α-cortol; these were lower than the comparative values for cortisol (Table 2). It should be emphasised that the analysis of urine steroids profile and serum cortisol were completed in different laboratories and as a result they have different units.
Approximately 200 cases of ACTH-secreting thymic carcinoid have been reported in the litera-ture.6,11-13,21-23 Thymic carcinoids, which are asso-ciated with CS, occur over a wide age range of 4 to 64 years and show no gender predilection. The most common features of CS are manifestations of tumours producing ectopic ACTH, with hypertension, oedema, severe hypokalemia and myasthenia being more common in ectopic ACTH-producing tumours than in Cushing’s disease.23,24 Incomplete process-ing of ACTH precursors causing higher levels of pro-opiomelanocortin (PoMC) have been described with ectopic ACTH, which has been proposed as a way of differentiating it from Cushing’s disease.25 We have previously shown that cross-reactivity of PoMC in currently available ‘ACTH’ immunoas-says varied from a mean of 1.6-4.7% which caused
Table 2. Mean urinary glucocorticoid metabolite levels in index patient and comparison with mean values in normal controls and in active Cushing’s disease. All measurements are in μg/24h.Urinary glucocorticoid metabolite
Baseline value in
index patient
Ratio of baseline value in index patient over
median value in normal
population20
Ratio of baseline value
in index patient over median
value in active Cushing’s disease20
Cortisol 36716 502 101Cortisone 1909 17 6THF 219024 100 25THE 88848 33 10THF/THE 0.03 0.25 2.47α-cortol 33272 216 55β-cortol 34829 143 36A-cortolone 13775 13 5B-cortolone 14042 57 15Total 442415 65 19

Urinary steroid metabolites in a case of florid Ectopic Cushing’s syndrome and clinical correlations
a large percentage increase in measured ACTH of up to 261%,26 albeit we have not measured PoMC in this particular patient.
our patient experienced various bacterial, fungal and viral infections and septicaemia that were dis-seminated in time and site and proved difficult to treat despite use of strong antibiotics, antiviral and antifungal agents and input from an on-site infectious disease team. It is possible that the accompanying hyperglycaemia has contributed to this phenomenon. our case illustrates that hypercortisolaemia should be part of the differential diagnosis of acquired im-munosuppression. Indeed, when 54 patients with ectopic ACTH production, but without lung cancer, were examined, it was shown that the more severe the hypercortisolaemia the more likely is the presence of severe infections (including sepsis); often these infections behaved atypically with no/mild fever and normal/near-normal white cell counts.27
once the tumour is successfully removed, lifelong surveillance involves similar investigations to those used for monitoring patients with CS i.e. UFC, oDST and/or salivary cortisol. Primary thymic NETs have a poor prognosis. This is due to the aggressive nature of the tumour with a high post-operative recurrence rate. Low-grade thymic carcinoids present a 5-year survival of 50% and 10-year survival of 9%, whereas high-grade thymic carcinoids have a 5-year survival of 0%.5 Patients with tumour recurrence are likely to develop CS again and an important part of their management is controlling hypercortisolism, either with ketoconazole and/or metyrapone or bilateral adrenalectomy.20
CONClUSION
This case demonstrates the biochemistry that one may expect to see with florid ectopic CS. It also emphasizes that one steroid metabolite can be the product of one or more steroids in the biochemical pathway, as was noted with various mineralocorticoid and sex hormone steroid metabolites that were raised in our case. Furthermore, it is conceivable that that urinary steroid metabolomics could be increasingly used in the near future for diagnosing ectopic CS as it seems to be associated with much higher urinary glucocorticoid metabolites than Cushing’s syndrome;
similarly such metabolites may be useful for monitor-ing disease recurrence in ectopic CS.
DEClARATION OF COMPETING INTERESTS
All authors declare no competing interests.
FUNDING
No funding was obtained for this study.
ETHICAl APPROvAl
No ethical approval was required for this study. Written informed consent was obtained from the aforementioned patient.
ACkNOwlEDGMENTS
We would like to thank Dr Tim Cooksley (Depart-ment of Acute Medicine, UHSM) and Dr Richard Sawyer (Department of Radiology, UHSM) for their support in the management of this patient, Prof Brian Keevil (Biochemistry Laboratory, UHSM) for cortisol measurement as well as Dr Norman Taylor (Depart-ment of Biochemistry, King’s College Hospital) and Dr Angela Taylor (the Centre for Endocrinology, Diabetes and Metabolism in Birmingham) for their general advice on urinary steroid profiling.
REFERENCES 1. Hauso o, Gustafsson BI, Kidd M, et al, 2008 Neuro-
endocrine tumor epidemiology: contrasting Norway and North America. Cancer 113: 2655-2664.
2. Modlin IM, oberg K, Chung DC, et al, 2008 Gastroen-teropancreatic neuroendocrine tumours. Lancet oncol 9: 61-72.
3. Barakat MT, Meeran K, Bloom SR, 2004 Neuroendo-crine tumours. Endocr Relat Cancer 11: 1-18.
4. Bi y, Liu R, ye L, et al, 2009. Gene expression pro-files of thymic neuroendocrine tumors (carcinoids) with ectopic ACTH syndrome reveal novel molecular mechanism. Endocr Relat Cancer 16: 1273-1282.
5. Öberg K, Hellman P, Ferolla P, 2012 Neuroendocrine bronchial and thymic tumors: ESMo Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann oncol 23: 120-123.
6. Duh Qy, Hybarger CP, Geist R,et al, 1987 Carcinoids associated with multiple endocrine neoplasia syndromes. Am J Surg 154: 142-148.

A. KyRIACoU ET AL
7. Kondo K, Monden y, 2003 Lymphogenous and hema-togenous metastasis of thymic epithelial tumors. Ann Thorac Surg 76: 1859-1864.
8. Arlt W, Biehl M, Taylor AE, et al, 2011 Urine steroid metabolomics as a biomarker tool for detecting ma-lignancy in adrenal tumors. J Clin Endocrinol Metab 96: 3775-3784.
9. Chortis V, Bancos I, Sitch AJ, et al, 2016 Urine steroid metabolomics is a highly sensitive tool for post-operative recurrence detection in adrenocortical carcinoma. Euro-pean conference of endocrinology. Endocrine abstracts.
http://www.endocrine-abstracts.org/ea/0041/ea0041 oC1.4.htm.
10. Lang K, Beuschlein F, Biehl M, et al, 2015 Urine steroid metabolomics as a diagnostic tool in primary aldosteronism. Endocrine abstracts.
http://www.endocrine-abstracts.org/ea/0038/ea0038 oc1.6.htm
11. Jansson Jo, Svensson J, Bengtsson BA, et al, 1998 Acromegaly and Cushing’s syndrome due to ectopic production of GHRH and ACTH by a thymic carcinoid tumour: in vitro responses to GHRH and GHRP-6. Clin Endocrinol 48: 243-250.
12. Laat JM de, Pieterman CR, van den Broek MF, et al, 2014 Natural Course and Survival of Neuroendocrine Tumors of Thymus and Lung in MEN1 Patients. J Clin Endocrinol Metab 99: 3325-3333.
13. Neary NM, Lopez-Chavez A, Abel BS, et al, 2012 Neuroendocrine ACTH-producing tumor of the thymus--experience with 12 patients over 25 years. J Clin Endocrinol Metab 97: 2223-2230.
14. Stewart PM, Walker BR, Holder G, et al, 1995 11 beta-Hydroxysteroid dehydrogenase activity in Cushing’s syndrome: explaining the mineralocorticoid excess state of the ectopic adrenocorticotropin syndrome. J Clin Endocrinol Metab 80: 3617-3620.
15. Wolthers BG, Kraan GP, 1999 Clinical applications of gas chromatography and gas chromatography-mass spectrometry of steroids. J Chromatogr A 843: 247-274.
16. Palermo M, Shackleton CH, Mantero F, et al, 1996 Urinary free cortisone and the assessment of 11 beta-hydroxysteroid dehydrogenase activity in man. Clin Endocrinol 45: 605-611.
17. Fong BM-W, Tam S, Leung KS-y, 2010. Improved
liquid chromatography-tandem mass spectrometry method in clinical utility for the diagnosis of Cushing’s syndrome. Anal Bioanal Chem 396: 783-790.
18. Stiefel P, García-Morillo JS, Jimenez L, et al, 2002 Role of ketoconazole treatment in urinary-free cortisol-to-cortisone and tetrahydrocortisol-to-tetrahydrocortisone ratios in nonectopic Cushing’s syndrome. Endocrine 18: 279-284.
19. Turpeinen U, Markkanen H, Sane T, et al, 2006 Determi-nation of free tetrahydrocortisol and tetrahydrocortisone ratio in urine by liquid chromatography-tandem mass spectrometry. Scand J Clin Lab Invest 66: 147-159.
20. Brossaud J, Ducint D, Corcuff J-B, 2016 Urinary glu-cocorticoid metabolites: biomarkers to classify adrenal incidentalomas? Clin Endocrinol 84: 236-243.
21. Valeriani M, Agolli L, Falco T, et al, 2012 A case report of metastatic atypical thymic carcinoid with ectopic ACTH production: locoregional control after adaptive radiation treatment. Tumori 98: 172-175.
22. Modlin IM, Sandor A, 1997 An analysis of 8305 cases of carcinoid tumors. Cancer 79: 813-829.
23. McEvoy MP, Rich BS, New M, et al, 2011Thymic carcinoid presenting with Cushing’s syndrome in a 17-year-old boy: a case report and review of the lit-erature. J Clin oncol 29: 716-718.
24. Isidori AM, Kaltsas GA, Pozza C, et al, 2006 The ec-topic adrenocorticotropin syndrome: clinical features, diagnosis, management, and long-term follow-up. J Clin Endocrinol Metab 91: 371-377.
25. Page-Wilson G, Freda PU, Jacobs TP, et al, 2014 Clini-cal Utility of Plasma PoMC and AgRP Measurements in the Differential Diagnosis of ACTH-Dependent Cushing’s Syndrome. J Clin Endocrinol Metab 99: 1838-1845.
26. Monaghan PJ, Kyriacou A, Sturgeon C, et al, 2016 Proopiomelanocortin interference in the measurement of adrenocorticotrophic hormone: a United Kingdom National External Quality Assessment Service study. Clin Endocrinol. doi: 10.1111/cen.13118. [Epub ahead of print]
27. Ilias I, Torpy DJ, Pacak K, et al, 2005 Cushing’s syn-drome due to ectopic corticotropin secretion: twenty years’ experience at the National Institutes of Health. J Clin Endocrinol Metab 90: 4955-4962.