Embed Size (px)
Citation preview

U.S. Department of StateMedical Bureau
Travel, Health & Immunizations
Standardizing Immunization Procedure
&
Preserving the cold chain
Andrea Anderson1

QUESTION:WHY ARE WE CONCERNED ABOUT VACCINE GUIDELINES & DOCUMENTATION?
ANSWER: BECAUSE IMMUNIZATIONS MISTAKES ARE MEDS LARGEST REPORTED ERRORS.
2

Immunization Errors Reported to QM
Year
Immunization
Assessment
Vaccine
Identification
Expired
Vaccine
Dose
Calculation
Immunization
Administration Documentation TOTAL
2008 3 1 2 6
2009 3 4 7
2010 2 3 1 1 7
2011 3 1 4
2012 6 4 1 1 2 14
2013 1 3 4 1 1 10
2014 8 2 2 1 1 14
2015 2 3 1 3 2 11
2016 10 5 3 1 1 1 21
2017 1 2 3
3

Immunization Guidelines
• Assessment Prior to Visit (Review current records and abstract previous immunization information)
• Identification of Vaccine/s needed
• Control Environment (No Rushing)
• Immunization administration (Use 5 Rs)
• Documentation
4

Assessing Patient’s Records
• Ask the patient to bring in vaccine records before the vaccination appointment.
• Carefully go over vaccine history by studying
original records and/or yellow book.
• If records are incomplete ask patient if they have had vaccines by other health providers.
• Make a TRAVEL CARE PLAN. (Adult)
5

U.S. Department of State Travel Health & Immunization Clinic TRAVEL IMMUNIZATION CARE PLAN
Name: ________________________________________ DOB ________________ Age:________ Itinerary: _______________________________________________ MR #:___________________ Allergies: ________________G6PD__________________ Rx__ ___________________________ Leave Date: ______________________ Return Date:__________________ P/L: _____________ PPD within last 2 years Yes NoRequired Immunizations:
_____Yellow Fever MD consulted (if applicable) ______________________________Consultation Date___________________
Immunizations Recommended: _____Typhoid ________________ Oral _______________ Injection _____Tdap / Td _____Polio (Single booster or series ) D 0 __________ 1m ______________ 2m__________ _____Hepatitis A Day 0___________ 6 m__________________Hepatitis B Day 0___________ 1 m_____________ 6 m _______________ _____Twinrix (A & B): Day 0___________ 1m______________ 6 m ____________________Twinrix (Accel. Sched.) Day 0________ D7_________ D21-30________ 12m ________
Meningococcal vaccines:_____ Menveo Infants 2-7m: 2m_________ 4m_________ 6m_________ 12m__________
Menveo Child 7-23m: 7-12m _________ 3m after primary_____________Menveo 2-55y: Single dose _________
_____ Menactra (9 –23 m) Initial ___________ 3 m ___________Menactra (2 -55 y) Single dose _________
_____ Menomune (>2 y) Single dose __________
_____ Ixiaro (J. Encephalitis Virus) D 0 _______ D28 ____________ Booster @ 12 m__________ _____ Rabies D 0 __________ D7________________ D21 to 28 ___________________ _____ Measles/Mumps/Rubella (born after 1956) D0 __________ D28 ____________ _____ Varicella (born after 1979) Titer ordered?_______ D0__________ D28 ____________
MALARIA SUPPRESSANTS: Needed: ______________ NOT Needed: _______________ _____Atovaquone/proguanil (Malarone) #: __________ _____Mefloquine #: ________ Child’s Wt: ____________ _____Chloroquine #: ________ _____Doxycycline # :________ Empiric Diarrhea Treatment: #1 Azithro #2 Levo_____Primaquine #: _________ _____ Acetazolamide (Diamox) (Altitude medicine) #:_________
Handouts given to the patient—check all that may applyTRAVAX Country ______ Malaria Rx information _________ Altitude Illness __________ Traveler Health Handout _______ Other _______________
Vaccine Information sheets from CDC: Yellow Fever_____ Typhoid____ Oral Typhoid_____Td / Tdap_____ Polio_____ Hep A_____ Hep B_____ Meningitis______ J. Encephalitis_____ Rabies_____ MMR_____ Varicella_____ Other_________
Work-up prepared by RN (Print, Sign and Date)_________________________________________Plan Counseled & initiated by RN (Print, Sign, and Date)
6

Identify the vaccines the patient’s needs
• On the day of visit be prepared by reviewing the Travel Plan to see if you missed anything
• Control your clinic, see only one child at a time
• Administer the immunizations using the 5 Rs
Above all
Don’t Rush!7

8

Vital Reasons for Vaccine Documentation
• Providers accept only written, dated records. (Except Flu vaccine)
• Creates a permanent record of care• Conveys information to other providers• Tells us if the patient is vaccine protected• Helps to differentiate the diagnosis.• Supports the management of care and assists with
treatment of the disease. • Helps prevent medical errors• It’s the law
9

Vaccine Documentation and the Law
• Prior to 1986 documentation of vaccines was up to the individual healthcare facility or provider.
• IN 1986 the National Childhood Law Vaccine Injury Act of 1986 was passed. (42 US CODE 300AA 26)
• This law requires 3 things:
– Provide a copy of the VIS
– Record vaccine in a permanent record
– Document adverse reactions following vaccine.
10

This Law also hits us in the pocket bookAs part of 1986 law, Federal Excise tax placed on each vaccine dose
Currently a tax of $0.75/dose is collected for each dose.This tax money is used to:• Ensure there is an adequate supply of vaccines by
working with vaccine manufacturers.• Helps stabilize vaccine costs• Established and maintain an accessible and efficient
forum for individuals found to be injured by certain vaccines. (Vaccine Adverse Event Reporting System-(VAERS)
• Allows patients to sue for vaccine injuries.
11

Standardizing Vaccine documentation
Do’s
• Use vaccine correct name
& manufacturer
name
• Use acceptable abbreviations
• Use Specific
language
Examples Don’t
• Hep A (Havrix) Don’t use names like
Imovax , Rabies alone
• Hep A, Hep B, DTaP Don’t make up
your own
abbreviations
• Use words like “given Don’t use “offered or
or administered” presented”
12

Where do we document Vaccines?
Records Required by law
• Record vaccine in permanent record or log
• Record/update patient’s personal vaccination record or provide a card.
Records we actually document
• Record in permanent record or log electronic or hard copy
• Record/update patient’s personal vaccination record or provide a card (yellow book)
• Record in log book.
13

Abstracting
Abstracting, consolidating, merging, copying, transposing, all mean the same thing.
• Why do it: it helps you assess the patient’s immunization status.
• Reduces chances for unnecessary doses of vaccine.
• Makes sure the patient has had a complete series.
** Be sure to record all doses in a series.
14

Improving documentation of vaccines?
• Document in a clear and precise way
• Use universal forms in the ISO system
• Easy to read writing (possibly print)
• Do not use abbreviations that are not recognizable.
• DON’T RUSH!
• CONTROL YOUR SPACE!
15

Final analysis of immunization records
•We review them
•We abstract them
•We create them
•We depend on them16

Website Resources
Travel Immunization Care Plan –Go to- Office of Medical Services-Quality Improvement- ISO 9001 Docs-TRAVEL MEDICINE-Index-ISO3751
Foreign Vaccines Appendix B Table 1: Diseases, Vaccines, and related terms Go to-https://www.cdc.gov/vaccines/pubs/pinkbook/drint warning!
Vaccine Storage & Handling Toolkit(A printed version of this toolkit may not be the most up-to-date version. Always refer to the online version) www.cdc.gov/vaccines/hcp/admin/ storage/toolkit/storage-handlingownloads/appendices/appdx-full-b.pdf
17

VACCINE STORAGE
18

Vaccine Excursion
• When ever vaccines are subject to temperature changes outside their recommended range that is called
a temperature excursion.
• In the last 2 years:–MED has had 7 reported excursions
totaling approximately $50,000.
19

What are we protecting vaccines against?
We protect against exposure to:
• Heat
• Cold
• Light
WHY: Once vaccine potency is lost, it cannot be restored.If potency is lost, vaccines are useless.
20

The objective is to have zero excursions!
• To do that we must:
•Acquire ways to improve the cold chain custody of vaccines
21

Importance of Vaccine Storage
Failure to store vaccine properly or a break in the cold chain may result in:
• Reduced potency of the vaccine
• Inadequate immune response in patients
• Poor protection against disease
• High cost of replacing unusable vaccines
• Almost always patients who received inadequately stored vaccine have to be re-vaccinated.
22

Who is responsible for Vaccine storage?
***Anyone who handles and stores vaccines
This includes:
• Medical providers
• Health unit staff
• Facilities/building staff
***Again, anyone who handles vaccines
23

How do we protect Vaccines?(Recommended Temperature Ranges)
• The new recommended Fahrenheit temperature range is between 36° F and 46°F (previously between 35° F and 46° F).
• The Celsius temperature range (between 2° C and 8° C) remains unchanged.
• BE CAUTIOUS! At times specific temps will be stated in manufacturer package inserts.
• If at all possible obtain delivery dates.
24

Keep vaccines in the dark
Light exposure is one that is easy to forget: You are encouraged to keep vial/syringes in original boxes with lids closed. (If you have a multi-pack of pre-drawn vaccine take out what you need close the box and put it back in the refrigerator. Don’t wait until after the dose is given.)Proper Storage requires:• Vaccine organization and storage. Alphabetize the
vaccines and label shelves. • Refrigerator/freezer temperature monitoring and
storage equipment (Beginning and end of shift) • Vaccine inventory management, transport monitoring(Check
shipping tag monitor alerts)• Backup plan for emergencies shared with staff members.
25

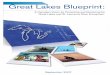
26

Properly storedvaccine
Full potency
Can you see the
difference?-
Improperly stored
vaccine with
Diminished potency
Can you spot the difference?

There is no difference!
• Appearance is NOT an reliable indicator that vaccines have been stored properly.
• Improperly stored vaccine diminishes the potency of vaccines.
28

Cold Chain Failure
• First get the facts:
• Do you know how low or high the temperature reached?
• Do you know how long that temperature was sustained?
• For extended exposure to light, when you examined the vaccine was there a particulate?
• Do you have a thermometer that records temperature 24/7?
29

All may not be lost!
Post vaccine excursion you need to:• Obtain the facts of the exposure• Contact each vaccine manufacturer separately and
given the details of the excursion.(You must call the exact manufacturer: i.e. if vaccinemade in Germany you call them, if made in USA then call USA.)
• The manufacturer will make the decision according to the exposure time. They will give advise on which vaccines may still be OK to use and for how long they may be used.
30

Practical Cold Chain Tips
• If you find a physical refrigeration problem act immediately
• Use “DO NOT UNPLUG” signs on
the electrical outlet
• Keep refrigeration unit coils free from dust and dirt by checking them every 6 months
• Double unit use only one socket
31

To Have an Effective Cold Chain
You need:• A well-trained staff• Reliable storage and
temperature monitoring• Accurate vaccine inventory
management
32

Cold Chain Websites
• Vaccine storage and handling home page: www.cdc.gov/vaccines/recs/storage/default. htm (sign up for notifications about updates)
• www.cdc.gov/vaccines/recs/storage/default. htm
• “You Call the Shots: Vaccine Storage and Handling,”* and many immunization programs*
33

THANK YOU! QUESTIONS?
34

Vaccine UpdateHealth Unit Immunization Issues
Gregory J. Martin MD
Tropical Medicine – Infectious Diseases
35

What we will cover Influenza vaccine recs
HPV vaccine fewer doses in children
Yellow Fever recs after WHO changes
Cholera vaccine recs with new vaccine FDA approved
JEV boosters, it lasts longer than we thought
Dengue vaccine development, almost there
A better Zoster vaccine down the line?
Vaccines in special groups Egg allergic
Pregnant or breast feeding
HIV infected
Post splenectomy
Questions from Andrea’s presentation and mine36

Influenza Vaccines for 2016-17No LAIV for at least this season
The effectiveness of seasonal influenza vaccines varies from season to season and is determined by a number of factors including the match between circulating influenza strains and influenza strains in the vaccine.
During the 2015-2016 influenza season, data from the US Influenza Vaccine Effectiveness Network indicated that inactivated influenza vaccine (IIV) was 63 percent effective in preventing influenza in children, but live attenuated influenza vaccine (LAIV) was not effective.
Findings of poor or lower than expected LAIV effectiveness were also noted during the 2013-2014 and 2014-2015 seasons in the US.
Findings are inconsistent with studies sponsored by the manufacturer and from other countries that found LAIV was effective (ranging from 46 to 58 percent) during the 2015-2016 season;
however, LAIV was less effective than IIV in all of these studies.
In August 2016, the CDC recommended that LAIV not be used during the 2016-2017 influenza season.
Some countries have elected to continue using LAIV
This may not be a permanent recommendation37

Reduced HPV dosingACIP recs from Oct 2016
HPV vaccine dosing for individuals younger than 15 years:
Two doses at least six months apart
New schedule is similar to that used in other countries data demonstrates two vaccine doses in young females have similar immunogenicity to three doses.
Efficacy of <3 doses for prevention of cervical neoplasia has not been directly established.
Three doses still recommended for >15 years due to lower HPV vaccine immune response
Number of rec doses is based on age at 1st dose (e.g. 1st dose at 14 yo and now 16 yo only needs 1 additional dose)
Meites et al. Use of a 2-Dose Schedule for HPV Vaccination — Updated Recs of the ACIP. MMWR 2016;65:1405–0838

Yellow Fever VaccineIt’s good for a lifetime!
WHO Strategic Advisory Group of Experts (SAGE) recs
Concerned with endemic populations and not travelers.
At least 80% of vaccinees respond to primary vaccination
Protection appears to last at least 20-35 years
>90% recipients have detectable levels of neutralizing Ab up to 20 years post vaccination
~80% of healthy U.S. WW II vets had neutralizing Ab 30-35 years after a single dose of vaccine.
Extreme rarity of documented vaccine failures
Seronegativity is not definitively correlated with lack of protection; immune memory may still exist.
39

No more Yellow Fever boostersNot so fast!
WHO Strategic Advisory Group of Experts (SAGE):
May 2014 IHR amended: indefinite validity of Int’l Certificate of Vaccination or Prophylaxis (ICVP) after YF vaccination an ICVP issued before or after amendment date meets the requirement
officially took effect June 2016 but some countries have not changed
On new ICVPs, "life of person vaccinated" should be entered in the validity space on the certificate
http://www.who.int/ith/ith_country_list.pdf?ua=1
40

Yellow Fever ImmunizationUS CDC-APIC Recs
For 2-week stay, estimated YF risk for unvax travelers:
West Africa 50 cases per 100,000
South America 5 five cases per 100,000
Single dose of YF vaccine provides long-lasting protection and is adequate for most travelers.
At-risk laboratory personnel and certain travelers should receive q10y doses of yellow fever vaccine: Pregnant women, hematopoietic stem cell transplant recipients,
and HIV-infected persons
Persons traveling to an area with an ongoing outbreak
Persons traveling for a prolonged period in an endemic area
Staples et al. Yellow Fever Vaccine Booster Doses: Recommendations of the Advisory Committee on Immunization Practices, 2015. MMWR. June 19, 2015 / 64(23);647-65041

Yellow Fever ImmunizationsDoS MED recs
As worldwide deployable and on some assignments prolonged periods in YF endemic areas:
direct hires should be kept on q10y YF booster
Family members who are going to a no threat or a low threat YF country that accepts lifetime immunization, do not need to be immunized
Family members who will be PCSing to Brazil and West Africa should be offered YF booster at 10 years but are unlikely to be required to have it for entry
With fewer countries requiring boosters last minute travel to a YF area is less likely to be held up for a booster immunization42

CholeraLive attenuated Vibrio cholerae vaccine
Rarely seen in travelers, risk estimated at 1 in 500,000
Previous vaccines required 2 doses
Vaxchora: single dose live oral vaccine that can provide rapid protection.
Approved by the US FDA in June 2016 for ages 18-64.
Provided 90% efficacy at day 10 and 80% efficacy at 3 months; ? booster
Requires cold chain which may limit use in rural, endemic areas
ACP recs use for a limited group of travelers:
Travelers unable to consistently follow safe food and water precautions and personal
hygiene measures in an area of active transmission
HCWs and others who have direct contact with body fluids (vomitus or stool) from
cholera patients
NOT recommended by MED for use in embassy populations who do not meet above
43Chen at al. Single-dose Live Oral Cholera Vaccine CVD 103-HgR Protects Against Human Experimental Infection With Vibrio cholerae O1 El Tor. Clin Infect Dis. 2016 Jun 1;62(11):1329-35

JE Vaccine AdministrationIxiaro Vero cell JE vaccine
44
http://wwwnc.cdc.gov/travel/yellowbook/2016/infectious-diseases-related-to-travel/japanese-encephalitisPaulke et al. Persistence of antibodies six years after booster vaccination with inactivated vaccine against Japanese encephalitis.
Vaccine. 2015 Jul 9;33(30):3600-4.
Dosing regimen at 0 and 28d:
3 yo to adults receive 0.5 mL IM; 2 mo through 2 yo receive 0.25 mL IM
96% of adults and 100% of children with neutralizing Ab after 2nd dose
Duration of protection appears to favor long term protection for ten years after initial series and one booster NOT YET AN ACIP rec
96% had adequate titers 9 years after booster dose.
Side effects:
Headache, myalgia, fatigue and an influenza like illness in ~10% of adults
Fever most common side effect in children
No delayed allergic responses reported to date as seen with old mouse brain vaccine
Not tested in pregnancy
recs are to defer but pregnant women who must travel to a high risk area should be vaccinated

Do we have a dengue vaccine for HU use?
Not quite!
Approved in Mexico, Philippines and Brazil for use in age 9-45 yo living in endemic areas; licensure sought in 20 other tropical countries.
3 doses at 0, 6 and 12 months protected 66% of individuals aged 9 and older.
greater protection against severe dengue (93%) and hospitalization due to dengue (80%).
Increased risk hospitalization among children < 9yo, particularly those aged 2-5yo
Less efficacious against dengue 2
Not yet shown effective in those without previous ongoing dengue exposure
not suitable nor under consideration for approval for use in travelers from non-tropical areas
Other candidate vaccines may offer protection for different populations (including travelers) but are several years from approval.
45

Dengue vaccineNIAID TV003
In Brazil, February 2016 multicenter phase 3 trial expects to enroll some 17,000 participants at 14 endemic locations and be completed in 2018.
Mutated wild type of all 4 strains
>90% seroconversion to all 4 strains with a single dose
Early human trials was 100% effective in preventing dengue
This vaccine will be indicated for expats and is likely to be the choice of MED (as well as the FDA!)
Schwartz et al. The dengue vaccine pipeline: Implications for the future of dengue control. 2015, Vaccine;33:3293-98Durbin AP et al. A 12-Month Interval Dosing Study in Adults Indicates That a Single Dose of the NIAID Tetravalent Dengue Vaccine Induces a Robust Neutralizing Ab Response J Infect Dis. 2016;214:832-835.46

Zoster vaccineThe best is yet to come
The live attenuated zoster vaccine (Zostavax) reduces the risk of zoster:
vaccine efficacy of 60 to 70 percent in adults 50 years and older
decreased efficacy in adults 70 years and older
Novel recombinant inactivated zoster vaccine (HZ/su), administered in two doses:
overall vaccine efficacy was 97 percent in adults 50 years and older
Additional randomized, placebo-controlled trial of 13,900 patients aged 70 and older, vaccine efficacy for preventing herpes zoster and postherpeticneuralgia was each approximately 90 percent after a mean 3.7-year follow-up
no serious adverse events were reported in either trial
may be particularly useful for older and immunocompromised individuals who cannot receive live vaccines
requires two doses for initial protection
Cunningham AL et al. Efficacy of the Herpes Zoster Subunit Vaccine in Adults 70 Years of Age or Older. N Engl J Med. 2016 Sep;375(11):1019-3247

What about Egg Allergy?Not a reason to avoid influenza vaccine
Most inactivated influenza vaccines (IIV) and Yellow Fever (YF) are prepared in embryonated chicken eggs Hx egg allergy but can eat eggs or egg products can safely receive both
IIV or YF Hx of hives from eggs may safely receive any of the IIV 513 patients with severe allergic reactions to eggs were given IIV and
only mild reactions occurred suggesting anaphylaxis to IIV is unlikely Safest option in those with anaphylaxis to eggs is to use recombinant IIV (Flublok)
YF vaccine recs are to not vaccinate or for skin testing and/or desensitization for those who are at high risk of YF and need immunization
Measles and mumps vaccine virus are grown in chick embryo fibroblast tissue cx Even those with severe egg allergy can receive MMR without skin
testing or desensitization
48CDC. General Recommendations on Immunization from the ACIP. MMWR,2011;60:1-61Des Roches et al. Egg-allergic patients can be safely vaccinated against influenza. J Allerg ClinImmun, 2012;130:1213-1216

Special Populations Pregnancy & Breastfeeding
Very few vaccines tested for safety and efficacy in large numbers of pregnancies
Theoretical risk to the fetus
No direct evidence of teratogenicity of any commonly used vaccine, including live attenuated vaccines
Inadvertent administration of live vaccine is NOT an indication for termination of pregnancy
Only anthrax and smallpox show possible risk to fetus and are only given if risk of disease outweighs risk to fetus
Smallpox is the only vaccine contraindicated in household contacts of a pregnant woman
Delayed vaccination until 2nd or 3rd trimester is recommended to minimize concerns of teratogenicity (despite evidence that this does not occur)
Influenza and Tdap are strongly recommended to be given during pregnancy
Breastfeeding is not a contraindication to any vaccine including live attenuated vaccine except for pre-event use of smallpox.49

Special PopulationsHIV Infected
Increases in HIV viral load with some (flu, pneumococcal, tetanus) immunizations due to T cell activation
Immunize early after diagnosis before CD4 drops
Asymptomatic infection (i.e. HIV without AIDS) may receive all routine and travel immunizations
Should have HAV, HBV, pneumococcal, meningococcal, annual flu and HPV (if <26 yo)
Advanced HIV CD4 <200 (especially CD4 <100) respond poorly to vaccines and should NOT receive:
MMR, Yellow Fever, LAIV, Varicella, Oral typhoid, Oral cholera or Zoster vaccine
50

Meningococcal VaccinesA Bewildering Array
Meningococcal Polysaccharide Vaccine (MPSV4) - Menomune Main indication now is for adult travelers to meningitis endemic areas
Meningococcal Diphtheria Conjugate Vaccine (MenACWY-D) – Menactra
Meningococcal CRM Conjugate Vaccine (MenACWY-CRM) – Menveo
Hib Meningococcal Tetanus Conjugate Vaccine (Hib-MenCY-TT) – MenHibrix
Meningococcal B Vaccine (MenB) – Trumenba
Meningococcal B Vaccine (MenB) - Bexsero
51 Cohn et al. Prevention and Control of Meningococcal Disease. 2013 MMWR, 62(RR02);1-22

Meningococcal vaccine in HIV
HIV-infected individuals have a disproportionate incidence of invasive meningococcal disease,
estimated risk 5 to 13 times that of the general population.
CDC now recommends meningococcal conjugate vaccination for all HIV-infected individuals older than two months
MenACWY-CRM (Menveo)
MenACWY-D (Menactra)
This includes primary vaccine series and interval booster doses every five years (for adults).
Individuals may also have separate indications for serogroup B meningococcal vaccination. Evidence of vaccine efficacy in HIV-infected patients is limited to immunologic outcomes52

Special PopulationsAnatomic and Functional Asplenia
Risk of infection with encapsulated organisms especially pneumococcus
Vaccine Recs Pneumococcus: PCV13 (Prevnar) followed >8 weeks later by PPSV23
(Pneumovax) with single booster PPSV23 five years after initial dose Hemophilus: single dose of Hib vaccine for lifetime Meningococcus: conjugate vaccine preferred, 2 doses at least 2
months apart and then booster with conjugate vaccine q 5 years.
Timing Preferable to administer 14 days prior to surgery
Administer at least 14 days post surgery if not pre-op If administered <14 days post op, give booster at 8 weeks
Administer at least 3 months following immunosuppressive drug
53

A Universal Mosquito-Borne Disease VaccineSounds crazy but wouldn’t it be nice?!
Vaccine targets the vector saliva and may provide prophylaxis against a wide variety of pathogens
Potentially sickens any mosquitoes who feed on vaccinated people and diminishes their lifespan.
54

Thanks for your attention!
Gregory J. Martin, MD
Infectious Diseases- Tropical MedicineBureau of Medical Services
US Department of State2401 E St NW
Washington DC 20522
55