Embed Size (px)
DESCRIPTION
US Pharmacist
Citation preview

THE JOURNAL FOR PHARMAC ISTS ’ EDUCAT ION
MARCH 2010
w w w . u s p h a r m a c i s t . c o m
Focus on Pediatric &
Adolescent Health
FOR FREE CE, GO TO:www.uspharmacist.com
A JOBSON PUBLICATION
2 CE Credits
Pediatric Accidental IngestionsTreating Apnea of Prematurity
Hypertension and Children
Tools for Assessing Kidney Disease
Risks and Benefits of BotoxU
.S. P
harm
acist Health
System
s Ed
ition
Vol. 35, N
o. 3 M
arch 2010
New Products in This Issue:Fanapt / Novartis Pharmaceuticals Corporation • Humalog /
Eli Lilly and Company • Injectables / Pfizer Injectables • Onglyza /AstraZeneca • Welchol / Daiichi-Sankyo
HEALTH SYSTEMS EDITION
00 MAR COV 3_2sc.indd CV200 MAR COV 3_2sc.indd CV2 3/4/10 1:48 PM3/4/10 1:48 PM
®
dextromethorphan polistirex
12 hours of cough relief is time well spent.
That’s a Delsym day.™
• Delsym®—the fi rst and ONLY FDA-approved OTC liquid cough suppressant for 12-hour relief with a single dose1,2
• Give patients an uninterrupted day by eliminating the burden of multiple dosing
Use as directed.Do not use in children under 4 years old.
References: 1. Delsym product labeling. 2. Food and Drug Administration Web site. Electronic Orange Book. http://www.fda.gov/cder/ob. Accessed March 18, 2009.
For more information, call 1-888-963-3382 or visit www.delsym.com.
© RBI 2009 1160 REV. 032309Delsym is a registered trademark of Reckitt Benckiser Inc.

1U.S. Pharmacist • March 2010 • www.uspharmacist.com
Straight Talk
W ith all the political posturing and the inaccurate information
being disseminated on health care reform, I’m afraid most Americans have lost sight of the primary reasons we need to over-haul our current health care sys-tem. Without getting into the minutiae of the House and Sen-ate bills, I think most legislators from both sides of the aisle agree on the same basic tenets of health care reform. These are a desire to reduce inflated costs in today’s health care system; to make health insurance available to millions of Americans who currently have none; and, finally, to assure that Americans are never without health insurance as a result of losing their job or having a preexist-ing health condition. While these issues are not being contested, there is still no consensus as to how we are going to accomplish them.
The road to health care reform is full of potholes and other obstacles, making it onerous for all sides to agree on how best to fix the system. I know that one way is by involving pharmacists. Pharmacists have been, and will continue to be, an integral part of the U.S. health care delivery system. Because pharmacists see patients more often than any other health professionals outside of an institutional set-ting, it only makes sense that pharmacists play a major role in any future health care reform.
And that means that pharmacists have to take on more consultative responsibilities. There has been much talk about medication therapy management (MTM) services, and while there are geographic pockets where pharmacists are practicing MTM on a regular basis, the concept has still not been widely adopted by most chains and independents. There are many reasons for this, but primarily it is because they’ve had little or no financial incentive to perform these duties from either insurers or the state and federal governments. I really don’t under-stand why. There is solid evidence that performing these kinds of consultative services could save our
health care system billions of dollars, which of course is one of the goals of health care reform. In a recently published article in Population Health Management, researchers pointed out that there are some 23.6 million undiag-nosed cases of diabetes in the U.S.; the researchers estimate that diagnosed cases of diabetes cost the nation $174 billion per year in higher medical costs due to lost productivity. Just imagine
what the health care bill for diabetes would be if even a fraction of the 24 million undiagnosed cases were discovered.
I am not suggesting that pharmacists diagnose cases of diabetes, but they can help keep it under control and possibly reduce the $174 billion it costs to treat the disease by consulting with their patients with diabetes to make sure they are com-pliant and that they recognize the signs and symp-toms of taking their medication incorrectly. Diabe-tes is only one chronic disorder adding billions to this nation’s health care costs.
Pharmacists and their employers have to become proactive if they are going to get involved in health care reform. Until now the excuse was that there were not enough pharmacists. Today, more phar-macy schools are graduating PharmDs who want to go into retail and wrap their arms around more than just filling prescriptions. They want to serve the health care marketplace in a way that really makes a difference, both financially and professionally.
Pharmacists should pave the way to health care reform. Pharmacists need to get more vocal about their desire to add value to our health care system. If not, the road to health care may end up just being a dead end.
Harold E. Cohen, [email protected]
The Road to Health Care Reform
01 REVStraight talk 2_24rdsc.indd 101 REVStraight talk 2_24rdsc.indd 1 3/2/10 1:32 PM3/2/10 1:32 PM

38549_elhups_HI62055_phrm_A_size_fa.indd 2 1/21/10 3:40:16 PM
YOU’RE USED TO ANSWERING JUST ABOUT ANY QUESTION CUSTOMERS COME UP WITH. Teaching customers about Humalog® KwikPen™ doesn’t change that. Humalog KwikPen is part of the Humalog® approach, designed to help fi t mealtime therapy into a patient’s life. And now, the maker of Humalog is offering a complimentary Humalog KwikPen Pharmacy Kit with a demonstration pen to help educate your customers and information to answer their questions.
For more details or to order a kit, visit www.kwikpenpharmkit.com.
Humalog is for use in patients with diabetes mellitus for the control of hyperglycemia. Hypoglycemia is the most common adverse effect associated with insulins, including Humalog.
For complete safety profi le, please see Important Safety Information on adjacent page and accompanying Brief Summary of full Prescribing Information.
Please see full user manual that accompanies the pen.
38549_elhups_HI62055_phrm_A_size_fa.indd 1 1/21/10 3:40:02 PM
Indication
Humalog (insulin lispro injection [rDNA origin]) is for use in patients with diabetes mellitus for the control of hyperglycemia. Humalog should be used with longer-acting insulin, except when used in combination with sulfonylureas in patients with type 2 diabetes.
Important Safety Information
Humalog is contraindicated during episodes of hypoglycemia and in patients sensitive to Humalog or one of its excipients.
Humalog differs from regular human insulin by its rapid onset of action as well as a shorter duration of action. Therefore, when used as a mealtime insulin, Humalog should be given within 15 minutes before or immediately after a meal.
Due to the short duration of action of Humalog, patients with type 1 diabetes also require a longer-acting insulin to maintain glucose control (except when using an insulin pump). Glucose monitoring is recommended for all patients with diabetes.
The safety and effectiveness of Humalog in patients less than 3 years of age have not been established. There are no adequate and well-controlled clinical studies of the use of Humalog in pregnant or nursing women.
Starting or changing insulin therapy should be done cautiously and only under medical supervision.
Hypoglycemia
Hypoglycemia is the most common adverse effect associated with insulins, including Humalog. Hypoglycemia can happen suddenly, and symptoms may be different for each person and may change from time to time. Severe hypoglycemia can cause seizures and may be life-threatening.
Other Side Effects
Other potential side effects associated with the use of insulins include: hypokalemia, weight gain, lipodystrophy, and hypersensitivity. Systemic allergy is less common, but may be life-threatening. Because of the difference in action of Humalog, care should be taken in patients in whom hypoglycemia or hypokalemia may be clinically relevant (eg, those who are fasting, have autonomic neuropathy or renal impairment, are using potassium-lowering drugs, or taking drugs sensitive to serum potassium level).
For additional safety profi le and other important prescribing considerations, see accompanying Brief Summary of full Prescribing Information.
Please see full user manual that accompanies the pen.
Humalog® is a registered trademark of Eli Lilly and Company and is available by prescription only. Humalog® KwikPen™ is a trademark of Eli Lilly and Company and is available by prescription only.
HI62055 0110 PRINTED IN USA ©2010, LILLY USA, LLC. ALL RIGHTS RESERVED.
38549_elhups_HI62055_phrm_A_size_fa.indd 2 1/21/10 3:40:16 PM38549_elhups_HI62055_phrm_A_size_fa.indd 1 1/21/10 3:40:02 PM
HUMALOG® INSULIN LISPRO INJECTION (rDNA ORIGIN)BRIEF SUMMARY: Consult package insert for complete prescribing information.
INDICATIONS AND USAGE: Humalog is an insulin analog that is indicated in the treatment of patients with diabetes mellitus for the control of hyperglycemia. Humalog has a more rapid onset and a shorter duration of action than regular human insulin. Therefore, in patients with type 1 diabetes, Humalog should be used in regimens that include a longer-acting insulin. However, in patients with type 2 diabetes, Humalog may be used without a longer-acting insulin when used in combination therapy with sulfonylurea agents. Humalog may be used in an external insulin pump, but should not be diluted or mixed with any other insulin when used in the pump. Humalog administration in insulin pumps has not been studied in patients with type 2 diabetes.
CONTRAINDICATIONS: Humalog is contraindicated during episodes of hypoglycemia and in patients sensitive to Humalog or any of its excipients.
WARNINGS: This human insulin analog differs from regular human insulin by its rapid onset of action as well as a shorter duration of activity. When used as a mealtime insulin, the dose of Humalog should be given within 15 minutes before or immediately after the meal. Because of the short duration of action of Humalog, patients with type 1 diabetes also require a longer-acting insulin to maintain glucose control (except when using an external insulin pump). External Insulin Pumps: When used in an external insulin pump, Humalog should not be diluted or mixed with any other insulin. Patients should carefully read and follow the external insulin pump manufacturer’s instructions and the “PATIENT INFORMATION” leaflet before using Humalog. Physicians should carefully evaluate information on external insulin pump use in the Humalog physician package insert and in the external insulin pump manufacturer’s instructions. If unexplained hyperglycemia or ketosis occurs during external insulin pump use, prompt identification and correction of the cause is necessary. The patient may require interim therapy with subcutaneous insulin injections (see PRECAUTIONS, For Patients Using External Insulin Pumps, and DOSAGE AND ADMINISTRATION). Hypoglycemia is the most common adverse effect associated with the use of insulins, including Humalog. As with all insulins, the timing of hypoglycemia may differ among various insulin formulations. Glucose monitoring is recommended for all patients with diabetes and is particularly important for patients using an external insulin pump. Any change of insulin should be made cautiously and only under medical supervision. Changes in insulin strength, manufacturer, type (eg, regular, NPH, analog), species, or method of manufacture may result in the need for a change in dosage.
PRECAUTIONS: General—Hypoglycemia and hypokalemia are among the potential clinical adverse effects associated with the use of all insulins. Because of differences in the action of Humalog and other insulins, care should be taken in patients in whom such potential side effects might be clinically relevant (eg, patients who are fasting, have autonomic neuropathy, or are using potassium-lowering drugs or patients taking drugs sensitive to serum potassium level). Lipodystrophy and hypersensitivity are among other potential clinical adverse effects associated with the use of all insulins. As with all insulin preparations, the time course of Humalog action may vary in different individuals or at different times in the same individual and is dependent on site of injection, blood supply, temperature, and physical activity. Adjustment of dosage of any insulin may be necessary if patients change their physical activity or their usual meal plan. Insulin requirements may be altered during illness, emotional disturbances, or other stress. Hypoglycemia—As with all insulin preparations, hypoglycemic reactions may be associated with the administration of Humalog. Rapid changes in serum glucose concentrations may induce symptoms of hypoglycemia in persons with diabetes, regardless of the glucose value. Early warning symptoms of hypoglycemia may be different or less pronounced under certain conditions, such as long duration of diabetes, diabetic nerve disease, use of medications such as beta-blockers, or intensified diabetes control. Renal Impairment—The requirements for insulin may be reduced in patients with renal impairment. Hepatic Impairment—Although impaired hepatic function does not affect the absorption or disposition of Humalog, careful glucose monitoring and dose adjustments of insulin, including Humalog, may be necessary. Allergy—Local Allergy—As with any insulin therapy, patients may experience redness, swelling, or itching at the site of injection. These minor reactions usually resolve in a few days to a few weeks. In some instances, these reactions may be related to factors other than insulin, such as irritants in a skin cleansing agent or poor injection technique. Systemic Allergy—Less common, but potentially more serious, is generalized allergy to insulin, which may cause rash (including pruritus) over the whole body, shortness of breath, wheezing, reduction in blood pressure, rapid pulse, or sweating. Severe cases of generalized allergy, including anaphylactic reaction, may be life-threatening. Localized reactions and generalized myalgias have been reported with the use of cresol as an injectable excipient. In Humalog-controlled clinical trials, pruritus (with or without rash) was seen in 17 patients receiving Humulin R® (N=2969) and 30 patients receiving Humalog (N=2944) (P=.053). Antibody Production—In large clinical trials, antibodies that cross-react with human insulin and insulin lispro were observed in both Humulin R- and Humalog-treatment groups. As expected, the largest increase in the antibody levels during the 12-month clinical trials was observed with patients new to insulin therapy. Usage of Humalog in External Insulin Pumps—The infusion set (reservoir syringe, tubing, and catheter), Disetronic® D-TRON®2,3 or D-TRONplus®2,3 cartridge adapter, and Humalog in the external insulin pump reservoir should be replaced and a new infusion site selected every 48 hours or less. Humalog in the external insulin pump should not be exposed to temperatures above 37°C (98.6°F). In the D-TRON®2,3 or D-TRONplus®2,3 pump, Humalog 3 mL cartridges may be used for up to 7 days. However, as with other external insulin pumps, the infusion set should be replaced and a new infusion site should be selected every 48 hours or less. When used in an external insulin pump, Humalog should not be diluted or mixed with any other insulin (see INDICATIONS AND USAGE, WARNINGS, PRECAUTIONS, For Patients Using External Insulin Pumps, Mixing of Insulins, DOSAGE AND ADMINISTRATION, and Storage). Information for Patients—Patients should be informed of the potential risks and advantages of Humalog and alternative therapies. Patients should also be informed about the importance of proper insulin storage, injection technique, timing of dosage, adherence to meal planning, regular physical activity, regular blood glucose monitoring, periodic hemoglobin A1C testing, recognition and management of hypoglycemia and hyperglycemia, and periodic assessment for diabetes complications. Patients should be advised to inform their physician if they are pregnant or intend to become pregnant. Refer patients to the “PATIENT INFORMATION” leaflet for timing of Humalog dosing (<_15 minutes before or immediately after a meal), storing insulin, and common adverse effects. For Patients Using Insulin Pen Delivery Devices: Before starting therapy, patients should read the “PATIENT INFORMATION” leaflet that accompanies the drug product and the User Manual that accompanies the delivery device. They should also reread these materials each time the prescription is renewed. Patients should be instructed on how to properly use the delivery device, prime the Pen to a stream of insulin, and properly dispose of needles. Patients should be advised not to share their Pens with others. For Patients Using External Insulin Pumps: Patients using an external infusion pump should be trained in intensive insulin therapy and in the function of their external insulin pump and pump accessories. Humalog was tested in the MiniMed®1 Models 506, 507, and 508 insulin pumps using MiniMed®1 Polyfin®1 infusion sets. Humalog was also tested in the Disetronic®2 H-TRONplus® V100 insulin pump (with plastic 3.15 mL insulin reservoir), and the Disetronic D-TRON®2,3 and D-TRONplus®2,3 insulin pumps (with Humalog 3 mL cartridges) using Disetronic Rapid®2 infusion sets. The infusion set (reservoir syringe, tubing, catheter), D-TRON®2,3 or D-TRONplus®2,3 cartridge adapter, and Humalog in the external insulin pump reservoir should be replaced, and a new infusion site selected every 48 hours or less. Humalog in the external pump should not be exposed to temperatures above 37°C (98.6°F). A Humalog 3 mL cartridge used in the D-TRON®2,3 or D-TRONplus®2,3 pump should be discarded after 7 days, even if it still contains Humalog. Infusion sites that are erythematous, pruritic, or thickened should be reported to medical personnel, and a new site selected. Humalog should not be diluted or mixed with any other insulin when used in an external insulin pump. Laboratory Tests—As with all insulins, the therapeutic response to Humalog should be monitored by periodic blood glucose tests. Periodic measurement of hemoglobin A1C is recommended for the monitoring of long-term glycemic control. Drug Interactions—Insulin requirements may be increased by medications with hyperglycemic activity, such as corticosteroids, isoniazid, certain lipid-lowering drugs (eg, niacin), estrogens, oral contraceptives, phenothiazines, and thyroid replacement therapy (see CLINICAL PHARMACOLOGY). Insulin requirements may be decreased in the presence of drugs that increase insulin sensitivity or have hypoglycemic activity, such as oral antidiabetic agents, salicylates, sulfa antibiotics, certain antidepressants (monoamine oxidase inhibitors), angiotensin-converting-enzyme inhibitors, angiotensin II receptor blocking agents, beta-adrenergic blockers, inhibitors of pancreatic function (eg, octreotide), and alcohol. Beta-adrenergic blockers may mask the symptoms of hypoglycemia in some patients. Mixing of Insulins—Care should be taken when mixing all insulins as a change in peak action may occur. The American Diabetes Association warns in its Position Statement on Insulin Administration, “On mixing, physiochemical changes in the mixture may occur (either immediately or over time). As a result, the physiological response to the insulin mixture may differ from that of the injection of the insulins separately.” Mixing Humalog with Humulin® N or Humulin® U does not decrease the absorption rate or the total bioavailability of Humalog.
Given alone or mixed with Humulin N, Humalog results in a more rapid absorption and glucose-lowering effect compared with regular human insulin. Pregnancy—Teratogenic Effects—Pregnancy Category B—Reproduction studies with insulin lispro have been performed in pregnant rats and rabbits at parenteral doses up to 4 and 0.3 times, respectively, the average human dose (40 units/day) based on body surface area. The results have revealed no evidence of impaired fertility or harm to the fetus due to Humalog. There are, however, no adequate and well-controlled studies with Humalog in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed. Although there are limited clinical studies of the use of Humalog in pregnancy, published studies with human insulins suggest that optimizing overall glycemic control, including postprandial control, before conception and during pregnancy improves fetal outcome. Although the fetal complications of maternal hyperglycemia have been well documented, fetal toxicity also has been reported with maternal hypoglycemia. Insulin requirements usually fall during the first trimester and increase during the second and third trimesters. Careful monitoring of the patient is required throughout pregnancy. During the perinatal period, careful monitoring of infants born to mothers with diabetes is warranted. Nursing Mothers—It is unknown whether Humalog is excreted in significant amounts in human milk. Many drugs, including human insulin, are excreted in human milk. For this reason, caution should be exercised when Humalog is administered to a nursing woman. Patients with diabetes who are lactating may require adjustments in Humalog dose, meal plan, or both. Pediatric Use—In a 9-month, crossover study of prepubescent children (n=60), aged 3 to 11 years, comparable glycemic control as measured by A1C was achieved regardless of treatment group: regular human insulin 30 minutes before meals 8.4%, Humalog immediately before meals 8.4%, and Humalog immediately after meals 8.5%. In an 8-month, crossover study of adolescents (n=463), aged 9 to 19 years, comparable glycemic control as measured by A1C was achieved regardless of treatment group: regular human insulin 30 to 45 minutes before meals 8.7% and Humalog immediately before meals 8.7%. The incidence of hypoglycemia was similar for all 3 treatment regimens. Adjustment of basal insulin may be required. To improve accuracy in dosing in pediatric patients, a diluent may be used. If the diluent is added directly to the Humalog vial, the shelf life may be reduced (see DOSAGE AND ADMINISTRATION). Geriatric Use—Of the total number of subjects (n=2834) in 8 clinical studies of Humalog, 12% (n=338) were 65 years of age or over. The majority of these were patients with type 2 diabetes. A1C values and hypoglycemia rates did not differ by age. Pharmacokinetic/pharmacodynamic studies to assess the effect of age on the onset of Humalog action have not been performed.
ADVERSE REACTIONS: Clinical studies comparing Humalog with regular human insulin did not demonstrate a difference in frequency of adverse events between the 2 treatments. Adverse events commonly associated with human insulin therapy include the following: Body as a Whole—allergic reactions (see PRECAUTIONS). Skin and Appendages—injection site reaction, lipodystrophy, pruritus, rash. Other—hypoglycemia (see WARNINGS and PRECAUTIONS).
OVERDOSAGE: Hypoglycemia may occur as a result of an excess of insulin relative to food intake, energy expenditure, or both. Mild episodes of hypoglycemia usually can be treated with oral glucose. Adjustments in drug dosage, meal patterns, or exercise may be needed. More severe episodes with coma, seizure, or neurologic impairment may be treated with intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate intake and observation may be necessary because hypoglycemia may recur after apparent clinical recovery.
DOSAGE AND ADMINISTRATION: Humalog is intended for subcutaneous administration, including use in select external insulin pumps (see DOSAGE AND ADMINISTRATION, External Insulin Pumps). Dosage regimens of Humalog will vary among patients and should be determined by the healthcare provider familiar with the patient’s metabolic needs, eating habits, and other lifestyle variables. Pharmacokinetic and pharmacodynamic studies showed Humalog to be equipotent to regular human insulin (ie, one unit of Humalog has the same glucose-lowering effect as one unit of regular human insulin), but with more rapid activity. The quicker glucose-lowering effect of Humalog is related to the more rapid absorption rate from subcutaneous tissue. An adjustment of dose or schedule of basal insulin may be needed when a patient changes from other insulins to Humalog, particularly to prevent premeal hyperglycemia. When used as a mealtime insulin, Humalog should be given within 15 minutes before or immediately after a meal. Regular human insulin is best given 30 to 60 minutes before a meal. To achieve optimal glucose control, the amount of longer-acting insulin being given may need to be adjusted when using Humalog. The rate of insulin absorption and consequently the onset of activity are known to be affected by the site of injection, exercise, and other variables. Humalog was absorbed at a consistently faster rate than regular human insulin in healthy male volunteers given 0.2 U/kg regular human insulin or Humalog at abdominal, deltoid, or femoral sites, the 3 sites often used by patients with diabetes. When not mixed in the same syringe with other insulins, Humalog maintains its rapid onset of action and has less variability in its onset of action among injection sites compared with regular human insulin (see PRECAUTIONS). After abdominal administration, Humalog concentrations are higher than those following deltoid or thigh injections. Also, the duration of action of Humalog is slightly shorter following abdominal injection, compared with deltoid and femoral injections. As with all insulin preparations, the time course of action of Humalog may vary considerably in different individuals or within the same individual. Patients must be educated to use proper injection techniques. Humalog in a vial may be diluted with STERILE DILUENT for Humalog, Humulin N, Humulin R, Humulin 70/30, and Humulin® R U-500 to a concentration of 1:10 (equivalent to U-10) or 1:2 (equivalent to U-50). Diluted Humalog may remain in patient use for 28 days when stored at 5°C (41°F) and for 14 days when stored at 30°C (86°F). Do not dilute Humalog contained in a cartridge or Humalog used in an external insulin pump. Parenteral drug products should be inspected visually before use whenever the solution and the container permit. If the solution is cloudy, contains particulate matter, is thickened, or is discolored, the contents must not be injected. Humalog should not be used after its expiration date. The cartridge containing Humalog is not designed to allow any other insulin to be mixed in the cartridge or for the cartridge to be refilled with insulin. External Insulin Pumps—Humalog was tested in MiniMed®1 Models 506, 507, and 508 insulin pumps using MiniMed®1 Polyfin®1 infusion sets. Humalog was also tested in the Disetronic®2 H-TRONplus® V100 insulin pump (with plastic 3.15 mL insulin reservoir) and the Disetronic D-TRON®2,3 and D-TRONplus®2,3 pumps (with Humalog 3 mL cartridges) using Disetronic Rapid®2 infusion sets. Humalog should not be diluted or mixed with any other insulin when used in an external insulin pump.
HOW SUPPLIED: Humalog (insulin lispro injection, USP [rDNA origin]) is available in the following package sizes (with each presentation containing 100 units insulin lispro per mL [U-100]): 10 mL vials NDC 0002-7510-01 (VL-7510) 3 mL vials NDC 0002-7510-17 (VL-7533) 5 x 3 mL cartridges3 NDC 0002-7516-59 (VL-7516) 5 x 3 mL prefilled insulin delivery devices (Pen) NDC 0002-8725-59 (HP-8725) 5 x 3 mL prefilled insulin delivery devices (Humalog® KwikPen™) NDC 0002-8799-59 (HP-8799)
1 MiniMed® and Polyfin® are registered trademarks of MiniMed, Inc.2 Disetronic®, H-TRONplus®, D-TRON®, and Rapid® are registered trademarks of Roche Diagnostics GMBH. 3 3 mL cartridge is for use in Eli Lilly and Company’s HumaPen® MEMOIR™ and HumaPen® LUXURA™ HD insulin
delivery devices, Owen Mumford, Ltd.’s Autopen® 3 mL insulin delivery device, and Disetronic D-TRON® and D-TRONplus® pumps. Autopen® is a registered trademark of Owen Mumford, Ltd. HumaPen®, HumaPen® MEMOIR™ and HumaPen® LUXURA™ HD are trademarks of Eli Lilly and Company. Other product and company names may be the trademarks of their respective owners.
Storage —Unopened Humalog should be stored in a refrigerator (2° to 8°C [36° to 46°F]), but not in the freezer. Do not use Humalog if it has been frozen. Unrefrigerated (below 30°C [86°F]) 12 vials, cartridges, Pens, and KwikPens must be used within 28 days or be discarded, even if they still contain Humalog. Protect from direct heat and light. Use in an External Insulin Pump—A Humalog 3mL cartridge used in the D-TRON®2,3 or D-TRONplus®2,3 should be discarded after 7 days, even if it still contains Humalog. Infusion sets, D-TRON®2,3 and D-TRONplus®2,3 cartridge adapters, and Humalog in the external insulin pump reservoir should be discarded every 48 hours or less.
Literature revised December 7, 2009
KwikPens manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA. Pens manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA or Lilly France, F-67640 Fegersheim, France. Vials manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA or Hospira, Inc., Lake Forest, IL 60045, USA or Lilly France, F-67640 Fegersheim, France. Cartridges manufactured by Lilly France, F-67640 Fegersheim, France for Eli Lilly and Company, Indianapolis, IN 46285, USA. www.humalog.com
Copyright © 1996, 2008, Eli Lilly and Company. All rights reserved.
38549_elhups_HI62055_phrm_A_size_fa.indd 3 1/21/10 3:40:19 PM
5U.S. Pharmacist • March 2010 • www.uspharmacist.com
U.S. PharmacistEditorial Board of Advisors
Joseph Bova, RPhCommunity Pharmacy Owner, Cary’s Pharmacy, Dobbs Ferry, New York; Member, NYS Board of Pharmacy
Carmen Catizone, RPhExecutive Director, National Association of Boards of Pharmacy
John M. Coster, PhD, RPhSenior VP of Government Affairs National Community Pharmacists Assoc.
Hewitt (Ted) W. Matthews, PhDDean, Southern School of Pharmacy, Mercer University, Atlanta
David G. Miller, RPhPharmacy Affairs, Merck & Co., Inc.,West Point, Pennsylvania
Mario F. Sylvestri, PharmD, PhDSenior Director, Medical Science Liaisons, Amylin Pharmaceuticals
Ray A. Wolf, PharmDMedical Education, Sanofi Aventis
Mary Ann E. Zagaria, PharmD, MS, CGPSenior Care Consultant and President, MZ Associates, Inc., Norwich, New York
Contributing Editors
Loyd V. Allen, Jr., PhD
Connie Barnes, PharmD
Bruce Berger, PhD
R. Keith Campbell, RPh, CDE
Patrick N. Catania, PhD, RPh
R. Rebecca Couris, PhD, RPh
Ed DeSimone, PhD, RPh
Ronald W. Maddox, PharmD
Somnath Pal, BS (Pharm), MBA, PhD
W. Steven Pray, PhD, DPh
M. Saljoughian, PharmD, PhD
Jesse C. Vivian, BS Pharm, JD
Send your comments via
Mail: 160 Chubb Avenue, Suite 306
Lyndhurst, NJ 07071
Telephone: (201) 623-0999
Editorial Dept. Fax: (201) 623-0991
Internet: www.uspharmacist.com
What’s News
Walgreens to Acquire Duane ReadeDeerfield, IL — Walgreens has announced that it will purchase the entire 257-store Duane Reed chain, all located in the New York City area. The deal, which is contingent upon regulatory approvals, is valued at $1.08 billion. Duane Reade will continue to operate under its brand name after the transaction closes by the end of the summer. Walgreens said that it expects to retain Duane Reade’s store, phar-macy, and distribution-center employees and many members of Duane Reade’s senior management team. Walgreens currently operates more than 7,100 retail out-lets across the United States. “Duane Reade is a compelling strategic acquisition that will immediately provide Walgreens with a leading position in the largest drugstore market in the U.S.,” said Walgreens President and CEO Greg Wasson.
More McNeil OTCs RecalledFort Washington, PA — Some 500 lots of OTC drugs made by McNeil Con-sumer Healthcare were recalled following an earlier recall of Tylenol Arthritis Pain Caplet 100-count bottles that started in November 2009, the FDA said. The latest recalls, also arising from consumer complaints of nausea, vomiting, stomach pain, and diarrhea, include lots of various adult and children’s Tylenol products, Motrin IB tablets and caplets, Benadryl Allergy tablets, Rolaids antacid tablets, Simply Sleep mini-caplets, and St. Joseph chewable and safety-coated aspirin. Not all lots have been linked to complaints of unusual odors, but they all have the potential to be affected, according to McNeil.
Jury Awards More Than $25 Million Over Acne DrugAtlantic City, NJ — A New Jersey Superior Court jury found that Hoffmann-La Roche failed to adequately warn Andrew McCarrell’s prescribing physician of possible long-term inflammatory bowel disease (IBD) associated with the acne drug Accutane, awarding McCarrell $25.16 million in compensatory damages. McCarrell, prescribed the powerful acne medication at the age of 23, then devel-oped a severe case of IBD and later had his colon removed. The decision follows a string of plaintiffs’ wins against Roche over charges that Accutane was a cause of severe bowel maladies, chronic bowel disease, and, in some cases, removal of part or all of plaintiffs’ colons and intestines. Roche, which faces as many as 800 cases across the U.S., first advised physicians about a possible association between Accutane and IBD in 1984.
FDA Approves Statin for Primary CVD PreventionSilver Spring, MD — The FDA has approved rosuvastatin (Crestor) for the pri-mary prevention of cardiovascular disease (CVD), making it the first statin to receive this indication. The new labeling is also the first to include an indication based on the inflammatory biomarker C-reactive protein (CRP). The new indica-tion would be for men aged 50 years or older and women aged 60 years or older who have a fasting LDL of less than 130 mg/dL, a highly sensitive CRP of 2.0 mg/L or greater, triglycerides of less than 500 mg/dL, and no prior history of heart attack or stroke or risk of coronary heart disease. The basis for the new labeling was the JUPITER trial, a randomized, placebo-controlled trial sponsored by AstraZeneca, the drug’s marketer, involving 17,802 men and women with a mean age of 66 and no history of atherosclerosis.
05 REVWhats New 3_2sc.indd 505 REVWhats New 3_2sc.indd 5 3/2/10 1:38 PM3/2/10 1:38 PM

MARCH 2010 The Journal for Pharmacists’ Education
U.S. Pharmacist is a Peer-Reviewed Journal
Vol.
35 N
o. 3
Measles is a viral disease caused by the virus of the same name. It is virtually nonexistent in the United
States today as a result of an effective vaccination campaign that began in the early 1960s. Measles
remains a serious disease in developing countries that do not offer the benefit of routine vaccination.
The measles virus is very contagious. It is transmitted by droplets in the air or on surfaces by an
infected person who sneezes, coughs, or even breathes in a room with a person who is not immune.
Almost everyone exposed to someone with the measles will develop the disease themselves within 1
to 2 weeks after exposure unless they are protected by vaccination. The measles vaccine is most often
given to children in the U.S. as part of a series of childhood vaccinations at 12 to 15 months, and
then repeated at 4 to 6 years. The measles vaccine is typically part of a combination vaccine (MMRV)
that also includes protection against mumps, rubella (German measles), and varicella (chickenpox).
Initial symptoms include fever, sore throat, nasal congestion, cough, fatigue, and red, watery eyes. After
a few days, tiny white spots may appear inside the mouth, and shortly afterward, the characteristic body
rash begins at the head and spreads to the feet. The measles usually last a total of 2 weeks. A person infected
with the measles virus is contagious for several days before and after the rash appears.There is no specific treatment for measles. Rest, plenty of fluids, acetaminophen or a nonsteroidal
anti-inflammatory drug (NSAID) for fever, and a decongestant and/or cough medication are all used
to help ease symptoms. Aspirin should not be used to treat children or teens with measles (or any viral
disease) to avoid the development of Reye’s syndrome.Measles can lead to various complications, including ear infections, pneumonia, severe diarrhea, and
an inflammation of the brain known as encephalitis. Further complications that can result from the
measles infection are deafness, seizures, blindness, mental retardation, and even death.
PATIENT TEACHING AIDMeasles
TE
AR
AL
ON
G P
ER
FO
RA
TIO
N
An Avoidable Viral Infection in Children
Copyright Jobson Medical Information LLC, 2010 continued
Koplik’s spots found on inner buccal surface of mouth
Koplik’s spots founnd
• Fever for 2-4 days• Red, watery eyes• Runny nose and cough• Blotchy, red rash covers body
PTA1003 Measles 2_16bo.indd 1PTA1003 Measles 2_16bo.indd 1
2/16/10 3:50 PM
HEALTH SYSTEMS EDITION
U.S. PHARMACIST® (ISSN 01484818; USPS No. 333-490) is published monthly by Jobson Medical Information LLC, 100 Avenue of the Americas, New York, NY 10013-1678. Periodicals postage paid at New York, and additional mailing offices. Postmaster: Send address changes to U.S. PHARMACIST, P.O. Box 2027, Skokie, IL 60076-7927. Canada Post: Publications Mail Agreement #40612608. Canada Returns to be sent to Bleuchip International, P.O. Box 25542, London, ON N6C 6B2. Subscriptions: One-year subscription rate: USA $58.00; Faculty and Students at U.S. Colleges of Pharmacy $39.00; Canada $81.00 (U.S.); and air mail to all other countries $157.00. Single copies are $6.00 each. All subscriptions payable in U.S. dollars. Payment must accompany order. Send checks and subscription requests to U.S. PHARMACIST, P.O. Box 2027, Skokie, IL 60076-7927 or call Customer Service:1-877-529-1746 (U.S. only) or 1-847-763-9630. Copyright 2010 by Jobson Medical Information LLC, 100 Avenue of the Americas, New York, NY 10013-1678. Reproduction of articles without permission from the publisher is expressly prohibited. Acceptance of advertising by U.S. PHARMACIST does not constitute endorsement of the advertiser, its products or services. The opinions, statements and views expressed by contributors to U.S. PHARMACIST are the authors’ and do not necessarily reflect those of the publisher, editor-in-chief, editors, editorial board of advisors, or the staff of U.S. PHARMACIST.
6U.S. Pharmacist • March 2010 • www.uspharmacist.com
PATIENT TEACHING AIDMeasles. See page 17
Senior Care
Hot Flashes and Night Sweats . . . . 20At menopause, the decline in ovarian function is associated with changes in the brain’s thermoregulatory centers.Mary Ann E. Zagaria, PharmD, MS, CGP
Prevalence of Substance Abuse in the Adolescent Population . . . . . 31Education and provision of resources are necessary to help stem this growing problem among teens.Timothy R. Ulbrich, PharmD
Pharmacy Law
A Prescription for Car Trouble . . . . 38Claiming ignorance of controlled substances in your vehicle may not excuse you from liability, even if you’re a pharmacist.Jesse C. Vivian, RPh, JD
Management of Pediatric Otitis Media . . . . . . . . . . . 44Mechanical, genetic, infectious, immunologic, and environmental factors may predispose children to ear infections.Ann McMahon Wicker, PharmD, BCPS, and Brice Labruzzo Mohundro, PharmD
●2 CE Credits
Pediatric Accidental Ingestions: Monitoring and Treatment Options . . . . . . . . . . 51Although most unintentional ingestions by children do not cause permanent harm, vigilance remains of utmost importance.Lela S. Fung, PharmD, BCPS
F E AT U R E S
Apnea of Prematurity Pharmacotherapy . . . . . . . . . . . . . . . . . . . . . . . . HS-2Theophylline and caffeine are equally effective treatment modalities for this condition.Anita Siu, PharmD, and Anitha James, MD
Pediatric Hypertension: A Review of Diagnosis and Treatment. . . . . . . HS-8High blood pressure in children usually is secondary to another disease process.Terri M. Wensel, PharmD, BCPS, and Shannon Williams, PharmD
Practical Assessment Tools for Identifying Kidney Disease . . . . . . . . HS-16Awareness of chronic renal disorders is low in the U.S., so screening and assessment are important.Timothy V. Nguyen, PharmD, CCP, FASCP
In-Service Primers
Botox Applications: A Review of Risks and Benefits . . . . . . . . . . . . . . HS-22The different botulinum toxin products available come in varying degrees of potency, and therefore are not interchangeable.Manouchehr Saljoughian, PharmD, PhD
HEALTH SYSTEMS EDITION
THIS MONTHEditorial Focus: Pediatric and Adolescent Health
NEXT MONTHEditorial Focus: Ophthalmology
View the Digital Edition of this issue and earn additional CE credits online at:www.uspharmacist.com
CUSTOMER SERVICE
Continuing Education (CE) ProgramsPhone: (800) 825-4696
Fax: (212) 219-7849E-mail:
Subscription ServicesPhone: (877) 529-1746 (U.S. only)
or (847) 763-9630E-mail:
COVER IMAGE:
Despite the requirement to dispense prescription medications in child-resistant containers, many cases of inadvertent consumption occur.
Illu
strat
ion:
© 2
010
Cyn
thia
Tur
ner
www.cynthiaturner.com
06 REV MAR TOC 3_2sc.indd 906 REV MAR TOC 3_2sc.indd 9 3/2/10 2:36 PM3/2/10 2:36 PM

FREE2010 GBR...
with ourcompliments!
Pharmacy Essentials
As part of our ongoing commitment to pharmacy professionals, we are pleased to provide pharmacistsand pharmacy technicians with the 2010 Generic Brand Reference (GBR®) ... FREE. It is our way ofsaying “Thank You” for supporting Mylan products.
The GBR is a handbook that contains a cross-referenced listing of generic and brand pharmaceuticalsas well as a color identification section that includes photographs and NDC numbers for all products inthe Mylan product portfolio.
©2010 Mylan Pharmaceuticals Inc. MYNMKT366A
To receive your FREE 2010 GBR,go to www.mylanpharms.com andclick “FREE GBR Offer.”
800.RX.MYLAN • 800.796.9526 • www.mylanpharms.com
Senior Vice President–Editor-in-ChiefHarold E. Cohen, RPh
Executive EditorRobert Davidson
Senior EditorBonnie Ostrowski
Senior Associate EditorMarjorie Borden
Consulting Clinical EditorMary Gurnee, PharmD, RPh
Senior Vice President–PublisherHarold E. Cohen, RPh (201) 623-0982
Associate PublisherJack McAleer (201) 623-0987
East Coast Regional Sales ManagerMark Hildebrand (201) 623-0984
Midwest/West Regional Sales ManagerMegan Conley (773) 450-7339
Sales & Marketing AssistantDeborah Mortara (201) 623-0990
Classified Advertising SalesHeather Brennan (800) 983-7737 x106
Design DirectorSharyl Sand Carow
Production ManagerDina Romano (201) 623-0942
Corporate Production DirectorJohn Anthony Caggiano
Director, Continuing Education ProcessingRegina Combs (800) 825-4696
Vice President, Circulation DirectorEmelda Barea
Vice President, Creative Services and ProductionMonica Tettamanzi
Chief Executive OfficerJeff MacDonald
Chief Financial OfficerDerek Winston
CEO, Information Services DivisionMarc Ferrara
Senior Vice President, OperationsJeff Levitz
Vice President, Human ResourcesLorraine Orlando
U.S. Pharmacist160 Chubb Avenue, Suite 306Lyndhurst, NJ 07071Phone: (201) 623-0999 Fax: (201) 623-0991E-mail: [email protected]: www.uspharmacist.com
PharmacistA Jobson Publication
U.S.
Printed on paper containing an average of 96 percent post-consumer recycled waste.
MARCH 2010 The Journal for Pharmacists’ Education
U.S. Pharmacist is a Peer-Reviewed Journal
Vol.
35 N
o. 3
8U.S. Pharmacist • March 2010 • www.uspharmacist.com
New Products in This IssueFanapt / Novartis Pharmaceuticals Corporation • Onglyza / AstraZeneca • Welchol / Daiichi-SankyoHealth Systems Edition: Humalog / Eli Lilly and Company • Injectables / Pfizer Injectables
Straight Talk
The Road to Health Care Reform . . . . . . . . . . . . . . . . . 1As an integral part of the health care system, pharmacists should be involved in reform decisions.Harold E. Cohen, RPh
What’s News . . . . . . . . . . . . . . . . . 5Pharmaceutical industry updates.
Consult Your Pharmacist
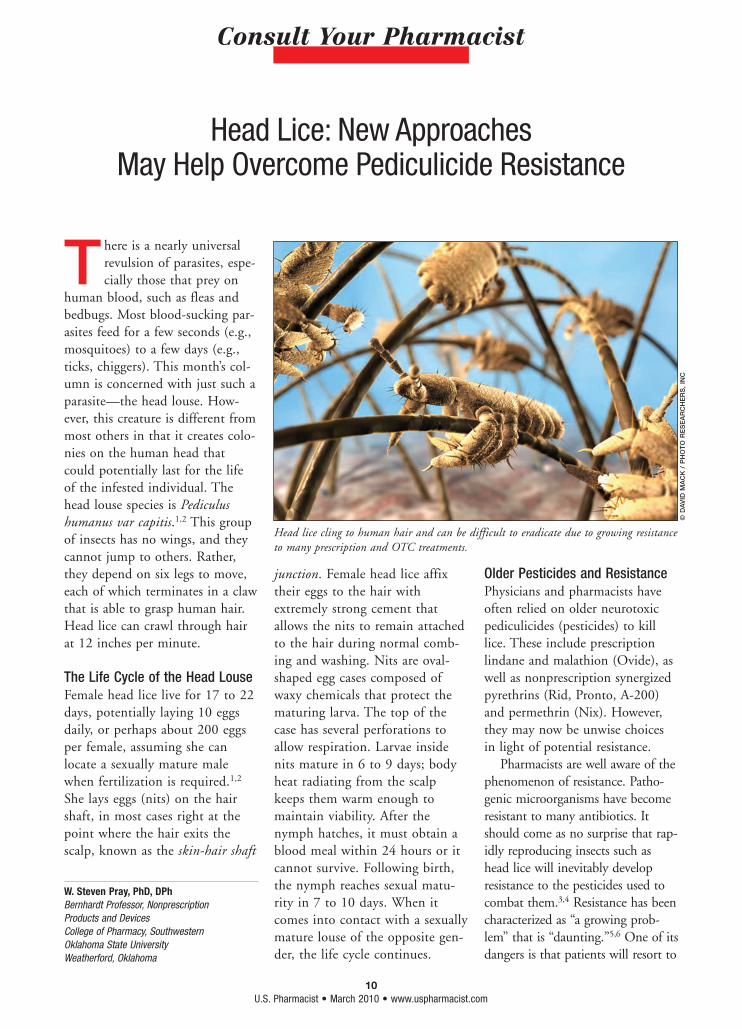
Head Lice: New Approaches May Help Overcome Pediculicide Resistance . . . . . . . 10Growing resistance to many forms of treatment makes this parasite hard to eradicate.W. Steven Pray, PhD, DPh
Contemporary Compounding
Cyclophosphamide 10-mg/mL Oral Liquid . . . . . . . . 42This chemotherapeutic agent isformulated without Aromatic Elixir USP, which is not available commerciallyand is time-consuming to prepare.Loyd V. Allen, Jr, PhD
Classified Advertising. . . . . . . . . 60Career opportunities, products, and services.
TrendWatch
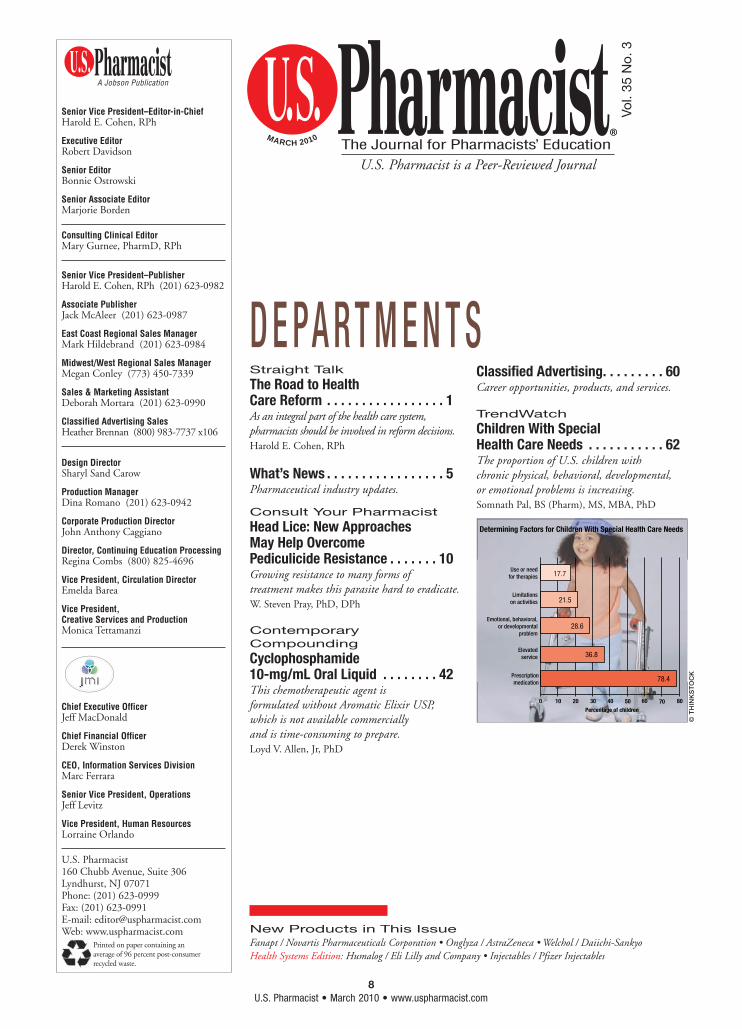
Children With Special Health Care Needs . . . . . . . . . . . 62The proportion of U.S. children with chronic physical, behavioral, developmental, or emotional problems is increasing.Somnath Pal, BS (Pharm), MS, MBA, PhD
D E PA R T M E N T S
© T
HIN
KS
TO
CK
78.4
36.8
28.6
21.5
17.7
0 10 20 30 40
Prescription medication
Elevated service
Emotional, behavioral, or developmental
problem
Limitations
on activities
Use or need for therapies
Percentage of children
Determining Factors for Children With Special Health Care Needs
50 60 70 80
06 REV MAR TOC 3_2sc.indd 806 REV MAR TOC 3_2sc.indd 8 3/2/10 2:36 PM3/2/10 2:36 PM

Rev. 9/09
E. FOUGERA & CO.A division of Nycomed US Inc., Melville, NY 11747 • Toll free: 800-645-9833 • www.fougera.com © 2009 Fougera. All rights reserved.
We’re about to really open it up.
10U.S. Pharmacist • March 2010 • www.uspharmacist.com
Consult Your Pharmacist
T here is a nearly universal revulsion of parasites, espe-cially those that prey on
human blood, such as fleas and bedbugs. Most blood-sucking par-asites feed for a few seconds (e.g., mosquitoes) to a few days (e.g., ticks, chiggers). This month’s col-umn is concerned with just such a parasite—the head louse. How-ever, this creature is different from most others in that it creates colo-nies on the human head that could potentially last for the life of the infested individual. The head louse species is Pediculus humanus var capitis.1,2 This group of insects has no wings, and they cannot jump to others. Rather, they depend on six legs to move, each of which terminates in a claw that is able to grasp human hair. Head lice can crawl through hair at 12 inches per minute.
The Life Cycle of the Head LouseFemale head lice live for 17 to 22 days, potentially laying 10 eggs daily, or perhaps about 200 eggs per female, assuming she can locate a sexually mature male when fertilization is required.1,2 She lays eggs (nits) on the hair shaft, in most cases right at the point where the hair exits the scalp, known as the skin-hair shaft
junction. Female head lice affix their eggs to the hair with extremely strong cement that allows the nits to remain attached to the hair during normal comb-ing and washing. Nits are oval-shaped egg cases composed of waxy chemicals that protect the maturing larva. The top of the case has several perforations to allow respiration. Larvae inside nits mature in 6 to 9 days; body heat radiating from the scalp keeps them warm enough to maintain viability. After the nymph hatches, it must obtain a blood meal within 24 hours or it cannot survive. Following birth, the nymph reaches sexual matu-rity in 7 to 10 days. When it comes into contact with a sexually mature louse of the opposite gen-der, the life cycle continues.
Older Pesticides and ResistancePhysicians and pharmacists have often relied on older neurotoxic pediculicides (pesticides) to kill lice. These include prescription lindane and malathion (Ovide), as well as nonprescription synergized pyrethrins (Rid, Pronto, A-200) and permethrin (Nix). However, they may now be unwise choices in light of potential resistance.
Pharmacists are well aware of the phenomenon of resistance. Patho-genic microorganisms have become resistant to many antibiotics. It should come as no surprise that rap-idly reproducing insects such as head lice will inevitably develop resistance to the pesticides used to combat them.3,4 Resistance has been characterized as “a growing prob-lem” that is “daunting.”5,6 One of its dangers is that patients will resort to
Head Lice: New Approaches May Help Overcome Pediculicide Resistance
© D
AV
ID M
AC
K /
PH
OT
O R
ES
EA
RC
HE
RS
, IN
C
Head lice cling to human hair and can be difficult to eradicate due to growing resistance to many prescription and OTC treatments.
W. Steven Pray, PhD, DPhBernhardt Professor, Nonprescription Products and DevicesCollege of Pharmacy, Southwestern Oklahoma State UniversityWeatherford, Oklahoma
10 Consult 3_1sc.indd 1010 Consult 3_1sc.indd 10 3/2/10 9:45 AM3/2/10 9:45 AM
www.COLCRYS.com | 1.888.351.3786
TOUGH AS EVER, BUTA BIT MORE REFINED
Now, patients who use colchicine for gout fl ares can get the effi cacy they need from gentle COLCRYS™.
Important Safety InformationCOLCRYS (colchicine, USP) tablets are indicated for prophylaxis and the treatment of gout fl ares.
COLCRYS is contraindicated in patients with renal or hepatic impairment who are concurrently prescribed P-gp inhibitors or strong inhibitors of CYP3A4 as life-threatening or fatal toxicity has been reported. Dose adjustments of COLCRYS may be required when co-administered with P-gp or CYP3A4 inhibitors. The most common adverse events in clinical trials for the prophylaxis and treatment of gout
were diarrhea and pharyngolaryngeal pain. Rarely, myelosuppression, thrombo-cytopenia, and leukopenia have been reported in patients taking colchicine. Rhabdomyolysis has been occasionally observed, especially when colchicine is prescribed in combination with other drugs known to cause this effect. Monitoring is recommended for patients with a history of blood dyscrasias or rhabdomyolysis.You are encouraged to report negative side effects of prescription drugs to the FDA. Visit www.fda.gov/medwatch or call 1.800.FDA.1088.
You may also report negative side effects to the manufacturer of COLCRYS by calling 1.888.351.3786.
Please see brief summary on adjacent page.
Distributed by AR Scientifi c, Inc. A URL Pharma company. Philadelphia, PA www.urlpharma.com
©2009 URL Pharma, Inc. All rights reserved. COL-097 Nov 2009 Printed in USA.
COLCRYS™ (colchicine, USP) tablets for oral use
Brief Summary of full Prescribing Information
The following is a brief summary only. Please see full Prescribing Information for complete product information.
INDICATIONS AND USAGECOLCRYSTM (colchicine, USP) tablets are indicated for prophylaxis and the treatment of gout fl ares.
Prophylaxis of Gout Flares: COLCRYS is indicated for prophylaxis of gout fl ares.
Treatment of Gout Flares: COLCRYS is indicated for treatment of acute gout fl ares when taken at the fi rst sign of a fl are.
Familial Mediterranean fever (FMF): COLCRYS is indicated in adults and children 4 years or older for treatment of familial Mediterranean fever (FMF).
CONTRAINDICATIONSPatients with renal or hepatic impairment should not be given COLCRYS in conjunction with P-gp or strong CYP3A4 inhibitors. In these patients, life-threatening and fatal colchicine toxicity has been reported with colchicine taken in therapeutic doses.
WARNINGS AND PRECAUTIONSFatal Overdose: Fatal overdoses, both accidental and intentional, have been reported in adults and children who have ingested colchicine. COLCRYS should be kept out of the reach of children.Blood Dyscrasias: Myelosuppression, leukopenia, granulocytopenia, thrombocytopenia, pancytopenia, and aplastic anemia have been reported with colchicine used in therapeutic doses.Drug Interactions: Colchicine is a P-gp and CYP3A4 substrate. Life-threatening and fatal drug interactions have been reported in patients treated with colchicine given with P-gp and strong CYP3A4 inhibitors. If treatment with a P-gp or strong CYP3A4 inhibitor is required in patients with normal renal and hepatic function, the patient’s dose of colchicine may need to be reduced or interrupted [see DRUG INTERACTIONS]. Use of COLCRYS in conjunction with P-gp or strong CYP3A4 inhibitors is contraindicated in patients with renal or hepatic impairment [see CONTRAINDICATIONS]. Monitor for toxicity and if present consider temporary interruption or discontinuation of COLCRYS.Neuromuscular Toxicity: Colchicine-induced neuromuscular toxicity and rhabdomyolysis have been reported with chronic treatment in therapeutic doses. Patients with renal dysfunction and elderly patients, even those with normal renal and hepatic function, are at increased risk. Concomitant use of atorvastatin, simvastatin, pravastatin, fl uvastatin, gemfi brozil, fenofi brate, fenofi bric acid, or benzafi brate (themselves associated with myotoxicity) or cyclosporine with COLCRYS may potentiate the development of myopathy [see DRUG INTERACTIONS]. Once colchicine is stopped, the symptoms generally resolve within 1 week to several months.
ADVERSE REACTIONS Prophylaxis of Gout Flares: The most commonly reported adverse reaction in clinical trials of colchicine for the prophylaxis of gout was diarrhea.Treatment of Gout Flares: The most common adverse reactions reported in the clinical trial with COLCRYS for treatment of gout fl ares were diarrhea (23%) and pharyngolaryngeal pain (3%).
FMF: Gastrointestinal tract adverse effects are the most frequent side effects in patients initiating COLCRYS, usually presenting within 24 hours, and occurring in up to 20% of patients given therapeutic doses. Typical symptoms include cramping, nausea, diarrhea, abdominal pain, and vomiting. These events should be viewed as dose-limiting if severe as they can herald the onset of more signifi cant toxicity.
DRUG INTERACTIONSCOLCRYS is a substrate of the effl ux transporter P-glycoprotein (P-gp). Of the cytochrome P450 enzymes tested, CYP3A4 was mainly involved in the metabolism of colchicine. If COLCRYS is administered with drugs that inhibit P-gp, most of which also inhibit CYP3A4, increased concentrations of colchicine are likely. Fatal drug interactions have been reported. Physicians should ensure that patients are suitable candidates for treatment with COLCRYS and remain alert for signs and symptoms of toxicities related to increased colchicine exposure as a result of a drug interaction. Signs and symptoms of COLCRYS toxicity should be evaluated promptly and, if toxicity is suspected, COLCRYS should be discontinued immediately. See full Prescribing Information for a complete list of reported potential interactions.
USE IN SPECIFIC POPULATIONS• In the presence of mild to moderate renal or hepatic impairment, adjustment
of dosing is not required for treatment of gout fl are, prophylaxis of gout fl are, and FMF but patients should be monitored closely.
• In patients with severe renal impairment for prophylaxis of gout fl ares the starting dose should be 0.3 mg/day, for gout fl ares no dose adjustment is required but a treatment course should be repeated no more than once every 2 weeks. In FMF patients, start with 0.3 mg/day and any increase in dose should be done with close monitoring.
• In patients with severe hepatic impairment, a dose reduction may be needed in prophylaxis of gout fl ares and FMF patients; while a dose reduction may not be needed in gout fl ares, a treatment course should be repeated no more than once every 2 weeks.
• For patients undergoing dialysis, the total recommended dose for prophylaxis of gout fl ares should be 0.3 mg given twice a week with close monitoring. For treatment of gout fl ares, the total recommended dose should be reduced to 0.6 mg (1 tablet) x 1 dose and the treatment course should not be repeated more than once every two weeks. For FMF patients the starting dose should be 0.3 mg per day and dosing can be increased with close monitoring.
• Pregnancy: Use only if the potential benefi t justifi es the potential risk to the fetus.
• Nursing Mothers: Caution should be exercised when administered to a nursing woman.
• Geriatric Use: The recommended dose of colchicine should be based on renal function.
Manufactured for: AR SCIENTIFIC, INC. Philadelphia, PA 19124 USA by: MUTUAL PHARMACEUTICAL COMPANY, INC.Philadelphia, PA 19124 USA
Rev 02, September 2009
Distributed by AR Scientifi c, Inc. A URL Pharma company.Philadelphia, PAwww.urlpharma.com COL-088 Nov 09
PATIENT INFORMATION
Remember, if you have questions, Consult Your Pharmacist.
✁©
TH
INK
ST
OC
K
13U.S. Pharmacist • March 2010 • www.uspharmacist.com
How to Detect Head LiceFor decades, parents have been given instructions on how to detect head lice. This traditional procedure involved placing gloves on the hands, parting the hair with small wooden paddles under strong light, and looking for tan insects about the size of a sesame seed. Parents also looked for tiny whitish eggs (nits) tightly attached to the hair, especially in the “hot spots” such as the crown of the head, the nape of the neck, and behind the ears. However, a newer method has proven far simpler and better at detection. The Lice-Meister comb is available online for a nominal charge from a non-profit organization known as the National Pediculosis Association (www.headlice.org/licemeister). When used as directed, this comb removes live lice and nits, serving as an excellent detection tool and also as a treatment method, since both lice and their eggs are combed out.
Treating Head LiceSome older lice treatments are outdated and should no longer be used. They include prescription lindane and malathion and nonpre-scription Rid, Nix, Pronto, and A-200. These lotions
and shampoos present medical risks to the patient, and lice may also have become resistant to them (i.e., the treatments will no longer work effectively). A new prescrip-tion product known as Ulesfia Lotion is a safer alternative, and resistance has not been demon-strated. As previously mentioned, the LiceMeister comb is also a good treatment option, as lice can-not develop resistance to it, and the device is harmless to both humans and the environment.
Products to AvoidSprays are available that treat pil-lows, beds, and mattresses for lice. Any head lice found away from the head will die shortly since they cannot get the blood they need to survive. You can vacuum thor-oughly if you wish, but you should not use sprays, as they are of unknown safety. Your child might breathe in the fumes all night if you cover the bedding with them.
Also avoid products that prom-ise to kill or remove lice but con-tain nothing more than diluted table salt in water (labeled as Natrum Muriaticum), neon paint, or dimethicone, and products con-taining herbs such as rue, tea tree oil, pawpaw, sage, rosemary, thyme, pennyroyal, and essential oils. None of these is yet proven safe and effective.
You should avoid so-called “suffocating treatments” that advise you to cover the head with olive oil, salad dressing, full-fat mayonnaise, petrolatum, or some other thick, gooey, or oily sub-stance. You may be instructed to leave the substance on overnight beneath several layers of plastic wrap. Removal of such greasy mat-ter can involve several courses of regular shampoo, which can irri-tate the scalp. These methods have never been proven to kill head lice in any case.
Never resort to potentially deadly treatments such as gasoline, kerosene, and lan-tern oil. These have all exploded in flash fires in people’s homes, causing severe burns and even death. Never use any type of garden or pet insecticide, and never use any industrial strength chemicals.
Head lice can be an annoying and persistent problem for children and their parents during the school year. The first issue is how these parasites can be detected. The second issue is how to remove or kill them safely.
Effectively Combating Head Lice
PHARMACY STAMP
10 Consult 3_1sc.indd 1310 Consult 3_1sc.indd 13 3/2/10 9:45 AM3/2/10 9:45 AM

14U.S. Pharmacist • March 2010 • www.uspharmacist.com
multiple treatments with pesticides, reexposing children needlessly to potentially toxic chemicals.
Reports of resistance to lindane have accelerated since the 1970s.7,8
The mechanism for development of resistance is hypothesized to be alterations in amino acids located at the nerve sheath sodium channel; this phenomenon may also confer resistance to pyrethrins and permethrin.9 Lindane users have experi-enced seizures, lethargy, slurred speech, and neck and extremity stiffness.10,11
Malathion is an odorous, flammable pesticide that must remain on hair until it is dry, perhaps 8 to 12 hours later. It can sting and irritate skin. Although the product marketing claims there is a residual effect, the manufacturer suggests that patients undergo a sec-ond exposure if lice remain after 7 to 9 days. Malathion has had a checkered marketing history in the United States, having been known as Prioderm and Ovide. It was dis-continued but remarketed in 1999.10 Treatment failures were reported as early as 1990, with early reports emanating from Australia and England, where it is a nonpre-scription product.12-14 Early reports cited a failure rate of 8%, but reports from 1999 gave the figure as 64%.15-17 In 2001, a Cochrane Review concluded that resistance was widespread in the United King-dom (UK); resistance in the U.S. has not been widely reported but may eventually develop with contin-ued use, given its emergence in other countries.7,18,19
Pyrethrins are chrysanthemum derivatives that must be synergized
with piperonyl butoxide, a petro-leum derivative, to retain efficacy. They cannot be used in patients allergic to ragweed. Reports of resistance to this nonprescription pesticide began in 1986, growing in scope until 1997 when the Medical Letter reported that treat-
ment failures had become com-mon.20-22 In 1999, researchers reported that synergized pyrethrin’s efficacy was questionable in light of the accelerating number of anecdotal reports of resistance.23 As case reports of resistance con-tinued to accumulate, dermatolo-gists suggested that multiple resis-tance had appeared, and that those patterns would undoubtedly be seen throughout the world.24,25
Permethrin was a prescription product (Nix) in the U.S. from 1986-1990, when it was switched to OTC status. The first reports of resistance to permethrin emerged in 1990, with later reports coming from Israel, the Czech Republic, and Britain in 1995.12,21,26-28 In 1997, the Medical Letter stated that resistance was increasing.22 Resistance was reported in Wash-ington State in 1998.29 In 1999, it was reported to be virtually useless
in the UK; even very high concen-trations had no effect on resistant lice.16,29,30 Allegations of resistance continued to accumulate; resis-tance figures as high as 87% were quoted for the UK.18,19,24,31-33 A 1999 study indicated possible resistance in the U.S.; this was
demonstrated again in 2003.23,34 Permethrin resis-tance may develop through several mechanisms. If the knockdown resistance (kdr) gene is involved, no strength of permethrin will be effective, which elimi-nates consideration of the 5% prescription concentra-tion (e.g., Elimite).
Resistance as a Cumulative PhenomenonResistance is the develop-
ment of mechanisms to survive potentially deadly onslaughts. Once these successful mutations are incorporated into the DNA of the living being, they will continue to be passed to succeeding genera-tions. The numbers of resistant organisms can only stabilize or grow in the face of continual chal-lenge by the provocative agent. Thus, any figure for the percentage of resistant members of a popula-tion is outdated; the actual per-centage of resistant louse strains can only stabilize or increase. Given the dynamic nature of organism adaptation, increase is the only logical conclusion, mean-ing that any figure for percentage is of necessity lower than reality.
Survey of PharmacistsA survey of pharmacists discovered that 81.7% of respondents had encountered patients with appar-
Consult Your Pharmacist
Pubic Lice Are Also a ProblemPharmacists are often asked to help treat pubic lice. It is vital to remember that nonprescription permethrin (Nix) has not been found effective for pubic lice, and the product is not labeled for this. The only other nonprescription alternative is synergized pyrethrins. However, as one would expect, resistance is also an issue, as evidenced by one case report. A 43-year-old male with adult lice and nits in the pubic area was treated with synergized pyrethrins, but the infestation persisted.42 While 5% permethrin cream was eventually successful in this case, resistance may eventually emerge to this product as well.
10 Consult 3_1sc.indd 1410 Consult 3_1sc.indd 14 3/2/10 9:45 AM3/2/10 9:45 AM
15U.S. Pharmacist • March 2010 • www.uspharmacist.com
ent treatment failures after use of synergized pyrethrins; 78.6% had seen failure following use of per-methrin.35 Treatment failures occurred once or twice weekly in 58.1% of pharmacists’ practices, often causing patients to treat themselves more frequently or in higher doses with pesticides.
Manufacturer Explanations of ResistanceThe manufacturers of topical pesti-cides for lice state that they have reports of efficacy. Some reports result from use of laboratory-bred lice. However, lab-bred lice are dif-ferent from free-living lice in the U.S. at large. Data from lab-bred lice populations cannot necessarily be extrapolated to the hardier lice typically found on human heads.36 Manufacturers also blame the patient for resistance by suggesting that the patient failed to apply the pesticide for a second time, that too little product was used, that the patient was reexposed, or by stating that the patient did not remove nits or clean the environ-ment properly.
Innovative Resistance-Free ApproachesPharmacists who wish to recom-mend a nonprescription product for detection and/or treatment of lice may stock and sell the FDA-registered medical device known as the LiceMeister Comb, developed by the nonprofit National Pedicu-losis Association.37 Preliminary research has demonstrated that the LiceMeister is superior to other plastic and metal combs due to its unique construction, having 32 closely spaced, rigid, stainless steel teeth.31 In contrast to the use of
pesticides, combing with the Lice-Meister presents no risk of pesti-cide absorption or toxicity, presents no danger to the environment, and can simultaneously detect and treat an infestation.
Hot Air Treatment: A prescription FDA-registered medical device known as the LouseBuster kills lice and nits in a single 30-minute treat-ment using controlled warm air.38 Resistance cannot develop as hot air destroys all stages of lice and eggs.
Benzyl Alcohol: A prescription product containing 5% benzyl alcohol (Ulesfia Lotion) was approved by the FDA for treat-ment of head lice in April 2009.39 It does not act in the same manner as traditional neurotoxins, and it kills lice by a novel method. Fol-lowing application, benzyl alcohol renders head lice incapable of clos-ing their respiratory spiracles, allowing the product’s vehicle to obstruct them, resulting in death by asphyxiation. Its lack of ovicidal activity means that it does not kill nits, making a second treatment a necessity 7 days after the first treatment. It possesses several important advantages over the tra-ditional treatments. It is not a neu-rotoxin, making it a safer alterna-tive for humans. Due to its mechanism of action, lice cannot adapt via the development of detoxification pathways, as is the case with the four older pesticides. Therefore, resistance should never develop. Unlike malathion, it is not flammable. It is not indicated for patients under the age of 6 months or older than 60 years. If the product contacts the eyes, they should be immediately flushed
with water. Patients must wash their hands after application. The agent may cause contact dermati-tis, in which case the patient should immediately rinse with water and discontinue application until the irritation subsides. If irri-tation persists, the patient should contact a physician.
The most common adverse reac-tions at the site of application are irritation (2%), anesthesia/hypoes-thesia of the application site (2%), and pain (1%). Other reactions include pruritus (12%), erythema (10%), pyoderma (7%), and ocular irritation (6%).39 Patients should be directed to apply Ulesfia Lotion to dry hair, being sure to use suffi-cient lotion to fully saturate the scalp and hair to ensure that each louse is coated with product, wait-ing for a carefully timed 10 min-utes to allow asphyxiation to occur, rinsing the product from the scalp, and repeating the treatment in 7 days. For complete coverage, the lotion must also be applied behind the ears and to the back of the neck. There are no studies of Ulesfia Lotion in pregnant women, and its ability to pass into breast milk is unknown.
Spinosad: An innovative product known as NatrOVA (0.9% spinosad) is of low toxicity to humans and has a method of action different from older pesticides.40 As a result, it should be effective in lice resis-tant to older pesticides. It was found to be significantly more effective than permethrin under actual-use conditions in two stud-ies.41 The FDA is currently review-ing the new drug application (NDA) for spinosad.
Consult Your Pharmacist
References available online at www.uspharmacist.com.
10 Consult 3_1sc.indd 1510 Consult 3_1sc.indd 15 3/2/10 9:45 AM3/2/10 9:45 AM

Finally, a real alternativeto pesticide lice treatments.
LiceMD is Pediatrician tested and clinically proven effective. Alcohol free, it eliminates lice, and lubricates hair for the easy, thorough comb-out of lice, eggs and nits. Plus, the patented dimethicone formula has no pesticide resistance. See for yourself how LiceMD compares to pesticide lice treatments.
For more information, visit www.LiceMD.com
Now you can recommend LiceMD® to moms concerned about pesticides.
Goodbye Lice. Goodbye Pesticides.
com102632a.indd 1 1/20/10 8:09 PM
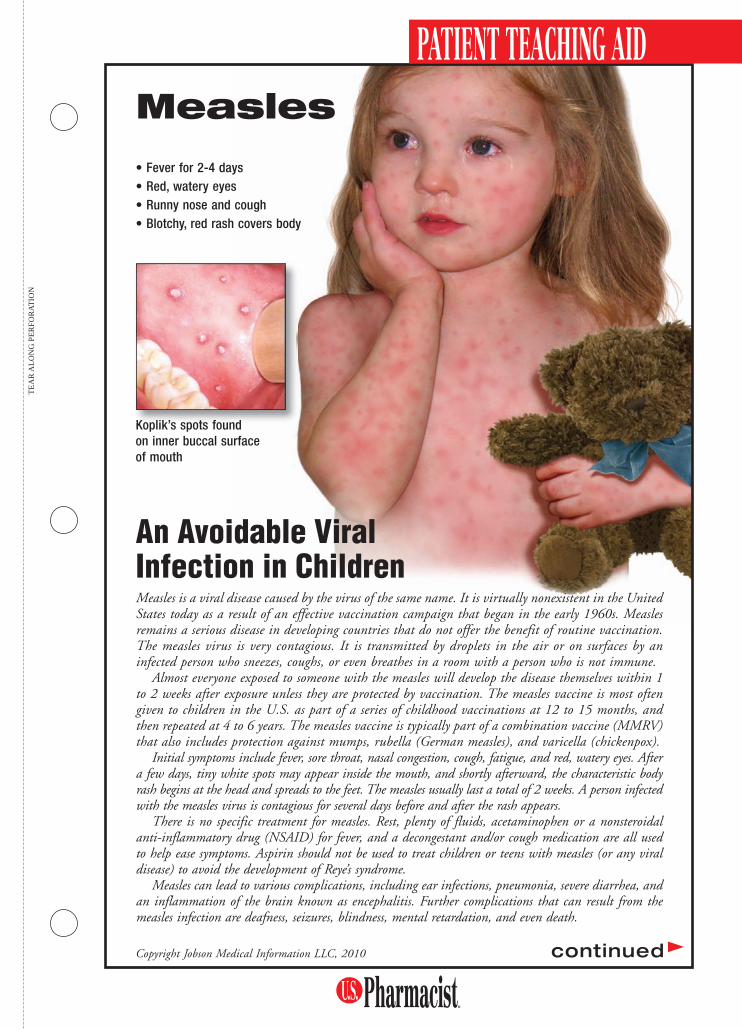
Measles is a viral disease caused by the virus of the same name. It is virtually nonexistent in the United States today as a result of an effective vaccination campaign that began in the early 1960s. Measles remains a serious disease in developing countries that do not offer the benefit of routine vaccination. The measles virus is very contagious. It is transmitted by droplets in the air or on surfaces by an infected person who sneezes, coughs, or even breathes in a room with a person who is not immune.
Almost everyone exposed to someone with the measles will develop the disease themselves within 1 to 2 weeks after exposure unless they are protected by vaccination. The measles vaccine is most often given to children in the U.S. as part of a series of childhood vaccinations at 12 to 15 months, and then repeated at 4 to 6 years. The measles vaccine is typically part of a combination vaccine (MMRV) that also includes protection against mumps, rubella (German measles), and varicella (chickenpox).
Initial symptoms include fever, sore throat, nasal congestion, cough, fatigue, and red, watery eyes. After a few days, tiny white spots may appear inside the mouth, and shortly afterward, the characteristic body rash begins at the head and spreads to the feet. The measles usually last a total of 2 weeks. A person infected with the measles virus is contagious for several days before and after the rash appears.
There is no specific treatment for measles. Rest, plenty of fluids, acetaminophen or a nonsteroidal anti-inflammatory drug (NSAID) for fever, and a decongestant and/or cough medication are all used to help ease symptoms. Aspirin should not be used to treat children or teens with measles (or any viral disease) to avoid the development of Reye’s syndrome.
Measles can lead to various complications, including ear infections, pneumonia, severe diarrhea, and an inflammation of the brain known as encephalitis. Further complications that can result from the measles infection are deafness, seizures, blindness, mental retardation, and even death.
PATIENT TEACHING AIDMeasles
TE
AR
AL
ON
G P
ER
FO
RA
TIO
N
An Avoidable Viral Infection in Children
Copyright Jobson Medical Information LLC, 2010 continued
Koplik’s spots found on inner buccal surface of mouth
Koplik’s spots founnd
• Fever for 2-4 days• Red, watery eyes• Runny nose and cough• Blotchy, red rash covers body
PTA1003 Measles 2_16bo.indd 1PTA1003 Measles 2_16bo.indd 1 2/16/10 3:50 PM2/16/10 3:50 PM
PATIENT TEACHING AID
Before the measles vaccine was available in the U.S., there were more than half a million cases in this country each year. Although the incidence of measles in the U.S. is typically under 100 cases each year as a result of an effective vaccination program that began in the 1960s, there are millions of cases of the disease every year throughout the world. Those few cases of measles in the U.S. are typically seen in people who were not vaccinated or who entered the country from overseas.
Who Should Be Vaccinated? Vaccination against the measles is a safe and effective form of pre-vention and is given routinely in the U.S. to children at 12 to 15 months of age, then repeated with a booster at 4 to 6 years of age. If a measles outbreak occurs, children can receive the vaccine at age 6 to 11 months in addition to the routine measles vaccinations. Adults should also be vacci-nated against the measles virus if they were born after 1956 and have never been vaccinated or had the measles infection. Typically, the measles vaccine is given with the mumps, rubella, and varicella vaccines in a combination product called the MMRV vaccine. People who have a serious allergy to neomycin or gelatin or have had a serious reaction to a previous dose of measles vaccine should not receive the vaccine. Women should not receive the vaccine while they are pregnant. Addition-ally, people with compromised immune systems, such as those with cancer, HIV/AIDS, or blood disorders, or who are taking medications that suppress the immune system, such as cancer drugs or steroids, should check with their doctors before being vaccinated. Receiving the measles vaccine is much safer than suffering from the measles, although there is a chance of a fever, mild rash, or stiff joints after vaccination. Very rarely, the vaccine has been linked to seizures, low platelet count, or allergic reactions. A doctor should be notified if signs of an allergic reaction or a high fever, weak-ness, or unusual behavior occurs after a measles vaccination.
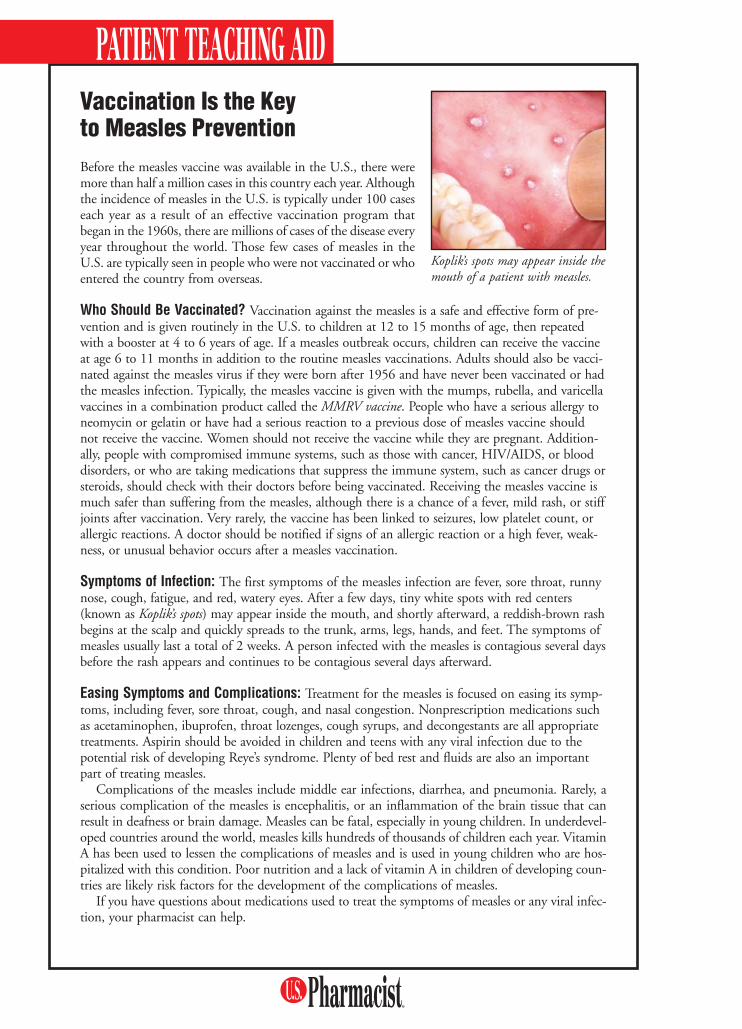
Symptoms of Infection: The first symptoms of the measles infection are fever, sore throat, runny nose, cough, fatigue, and red, watery eyes. After a few days, tiny white spots with red centers (known as Koplik’s spots) may appear inside the mouth, and shortly afterward, a reddish-brown rash begins at the scalp and quickly spreads to the trunk, arms, legs, hands, and feet. The symptoms of measles usually last a total of 2 weeks. A person infected with the measles is contagious several days before the rash appears and continues to be contagious several days afterward.
Easing Symptoms and Complications: Treatment for the measles is focused on easing its symp-toms, including fever, sore throat, cough, and nasal congestion. Nonprescription medications such as acetaminophen, ibuprofen, throat lozenges, cough syrups, and decongestants are all appropriate treatments. Aspirin should be avoided in children and teens with any viral infection due to the potential risk of developing Reye’s syndrome. Plenty of bed rest and fluids are also an important part of treating measles.
Complications of the measles include middle ear infections, diarrhea, and pneumonia. Rarely, a serious complication of the measles is encephalitis, or an inflammation of the brain tissue that can result in deafness or brain damage. Measles can be fatal, especially in young children. In underdevel-oped countries around the world, measles kills hundreds of thousands of children each year. Vitamin A has been used to lessen the complications of measles and is used in young children who are hos-pitalized with this condition. Poor nutrition and a lack of vitamin A in children of developing coun-tries are likely risk factors for the development of the complications of measles.
If you have questions about medications used to treat the symptoms of measles or any viral infec-tion, your pharmacist can help.
Vaccination Is the Key to Measles Prevention
Koplik’s spots may appear inside the mouth of a patient with measles.
PTA1003 Measles 2_16bo.indd 2PTA1003 Measles 2_16bo.indd 2 2/16/10 3:50 PM2/16/10 3:50 PM
Our most important ingredient is integrity.
Solutions Are Our Business.™
Introducing Pfizer Injectables. Dedicated to helping your business thrive with our heritage of quality,reliable manufacturing, and customer-focused flexibility—so essential injectable medicines can reachthe patients who need them, making the world a healthier place.
US100032 ©2009 Pfizer Inc. All rights reserved. Printed in USA/November 2009 www.pfizerinjectables.com

HS-2U.S. Pharmacist • March 2010 • www.uspharmacist.com
Apnea of prematurity (AOP) commonly occurs in infants of less than 37 weeks’ gestation and is characterized by brief episodes of breathing cessa-
tion lasting 20 seconds or less with associated bradycardia or cyanosis. It is a diagnosis of exclusion that can only be confirmed once alternate causes of apnea (e.g., sepsis, metabolic disorders, central nervous system [CNS] pathol-ogy) have been excluded.1 The apnea can be classified as being of central origin, obstructive, or mixed type. Periodic breathing represents a normal occurrence of breathing during sleep and is often confused with apnea. (The dif-ferent types of apnea and periodic breathing are categorized in TABLE 1.) Central apnea refers to the failure of the central CNS to initiate respiratory effort secondary to immaturity of the neurologic pathways. Obstructive apnea, most commonly due to collapse of the pharyngeal airway, results in mechanical interference with respiratory efforts and often leads to bradycardia.2 Mixed-type apnea is a combination of both central and obstructive apneas.3
Studies have shown that the majority of apnea events (~50%) in preterm infants are of mixed origin, 40% are of central origin, and 10% are purely obstructive in origin.4
PathophysiologySeveral theories exist regarding the pathogenesis of AOP, none of which have been confirmed as being the sin-gle cause to date. One theory describes the role of adenosine as a central respi-
ratory inhibitor.5,6 Adenosine is a nucleoside component of compounds such as adenosine triphosphate (ATP) and cyclic adenosine monophosphate (cAMP), which are crucial to numerous biochemical processes. As a therapeu-tic agent, adeno sine is well known for its use and efficacy in the treatment of supraventricular tachycardia.7
Adenosine also plays a role in cellular signaling via its four main receptor subtypes: A1, A2a, A2b, and A3. Certain receptor subtypes, specifically A1 and A2a, are believed to be directly involved in the control of respiratory drive. One study postulates that activation of pre- and postsyn-aptic A1 receptors decreases neuronal activity of the respi-ratory motor outflow tract, thus impeding respiration itself.6 In addition to the role of adenosine, comorbidities like gastroesophageal reflux may further increase the num-ber of apnea episodes in preterm infants.8
The onset of AOP typically occurs near the end of the first week of life, but may begin as early as the first day of life.9 With the occurrence of apnea episodes being inversely related to the gestational age of the infant, a
similar association has also been found in its resolution.10 Resolution of AOP typically occurs by the time “term” gestational age is reached postconception (38-42 weeks’ gestation). Infants having a protracted course of AOP lasting longer than the age of term gestation are often very premature (24-28 weeks’ gestation) and/or have known neurologic dysfunction.11,12
Apnea of Prematurity Pharmacotherapy
Anita Siu, PharmDAssistant Clinical Professor
Clinical Neonatal/Pediatric Pharmacotherapy Specialist, Ernest Mario School of Pharmacy at
Rutgers, the State University of New JerseyPiscataway, New Jersey
Anitha James, MDChief Resident, Pediatrics
K. Hovnanian Children’s Hospital at Jersey Shore University Medical Center
Neptune, New Jersey
HEA
LTH S
YS
TEMS
EDITIO
N
© BLEND IMAGES / GETTY IMAGES
HS02 Apnea 3_1bo.indd HS-2HS02 Apnea 3_1bo.indd HS-2 3/2/10 9:54 AM3/2/10 9:54 AM
Teva is #1inOncology Products
19 Hughes • Irvine, California 92618800.729.9991 • www.tevausa.com
Data derived from the use of information under license from the following IMS HealthInformation Service: IMS NSP Audit, MAT 9/08. Data is proprietary to IMS Health.
©2009, Teva Pharmaceuticals USA 8349 A
ViewTeva’s complete line of oncologyproducts at www.tevausa.com/oncology

HS-4U.S. Pharmacist • March 2010 • www.uspharmacist.com
APNEA OF PREMATURITY
HEA
LTH S
YS
TEMS
EDITIO
N
ComplicationsConsequences of untreated or inadequately treated AOP are extensive and include spastic diplegia or quadriplegia, bilateral retrolental fibroplasia resulting in significant visual impairment, sensorineural deafness, varying degrees of mental retardation, and even death.13 It is interesting to note, however, that AOP does not seem to be a future determinant of sudden infant death syndrome (SIDS).9,14
Goals of TherapyThe clinical management of AOP has not changed in the past three decades and includes both supportive measures and oftentimes pharmacologic therapy. Sup-portive treatment measures include tactile stimulation, proper positioning to maintain an open airway, and ventilatory support such as supplemental oxygen, con-tinuous positive airway pressure (CPAP), and mechan-ical ventilatory support. The treatment goals in the management of AOP include preventing apnea episodes, preventing bradycardia and desaturation, improving diaphragmatic activity, and maintaining respiratory ventilation.
Pharmacologic Management OptionsPharmacologic measures include the use of methylxanthines, particularly theophylline and aminophylline or caffeine citrate, and other respiratory stimulants such as doxapram.15 The consensus on when to begin pharmacotherapy is not well established. However, if apnea episodes persist despite supportive or nonpharmacologic measures, then drug therapy may be considered.
MethylxanthinesSince the early 1970s, methylxanthines have been admin-istered as respiratory stimulants in the treatment of AOP and are considered to be the primary treatment option. Chemically, methylxanthines contain a xanthine molecule, which is found in caffeine (1,3,7-trimethylxanthine) and theophylline (1,3-dimethylxanthine) (FIGURE 1). Caffeine is metabolized by the CYP450 isoenzyme 1A2. The chemical structure is demethylated to produce the dimeth-ylxanthines, including theophylline, theobromine, and
paraxanthine. Despite their similar chemical structures, these agents possess different kinetic properties.
Although methylxanthines primarily work by stimu-lating the respiratory drive in the CNS, several other mechanisms have been postulated. Since adenosine is known as a central respiratory depressant, methylxanthines also act by inhibiting phosphodiesterase enzymes. This inhibitory mechanism causes the breakdown of cAMP and cyclic guanosine monophosphate (cGMP), thus increasing its availability in the blood to relax the airway. These agents also work by competitively antagonizing the adenosine receptor or increasing catecholamine release by modulating the flux of calcium.16,17 Other effects include improving ventilation and neural impulses, reducing rapid eye movement (REM) sleep, improving oxygenation, and improving skeletal muscle contraction to prevent diaphragmatic fatigue.18
Pharmacokinetics: In regard to absorption, aminophyl-line, the ethylenediamine tetraacetic acid salt, is composed of 80% theophylline. During drug metabolism, theoph-ylline undergoes methylation and may produce caffeine plasma levels of up to 50% of theophylline concentra-tions in preterm neonates.19 Linear first-order pharma-cokinetics occurs when theophylline is within the normal therapeutic range (6-14 mcg/mL) for the treatment of AOP. Therapeutic levels above normal may produce nonlinear zero-order pharmacokinetics with adverse effects. Clearance is slower in preterm as compared to full-term infants, with half-life approximately 30 hours versus 25 hours.20 On the other hand, caffeine undergoes demethylation to produce theophylline and follows linear first-order pharmacokinetics. Unlike theophylline, caffeine’s half-life is more prolonged (72-96 hours), allow-ing for once-daily administration.21
Therapeutic Drug Monitoring: The therapeutic range for the treatment of AOP with theophylline is 6 to 14 mcg/mL, while caffeine has a wider therapeutic range of 8 to 20 mcg/mL. Steady state is achieved much earlier with theophylline compared to caffeine (1-3 days vs. 9-12 days) in full-term infants. Theophylline requires close
Table 1. Comparison of Apnea and Periodic BreathingCriteria Central Apnea Obstructive Apnea Mixed-type Apnea Periodic Breathing
Duration of breathing cessation At least 20 seca At least 20 seca At least 20 seca 5-10 secRespiratory effort Absent Present Absent/present AbsentMovement of air Absent Reduced/absent Reduced/absent Reduced/absentBradycardia/desaturation May occur May occur May occur Noa May be less than 20 seconds if there is associated bradycardia or cyanosis.Source: Reference 4.
HS02 Apnea 3_1bo.indd HS-4HS02 Apnea 3_1bo.indd HS-4 3/2/10 9:54 AM3/2/10 9:54 AM
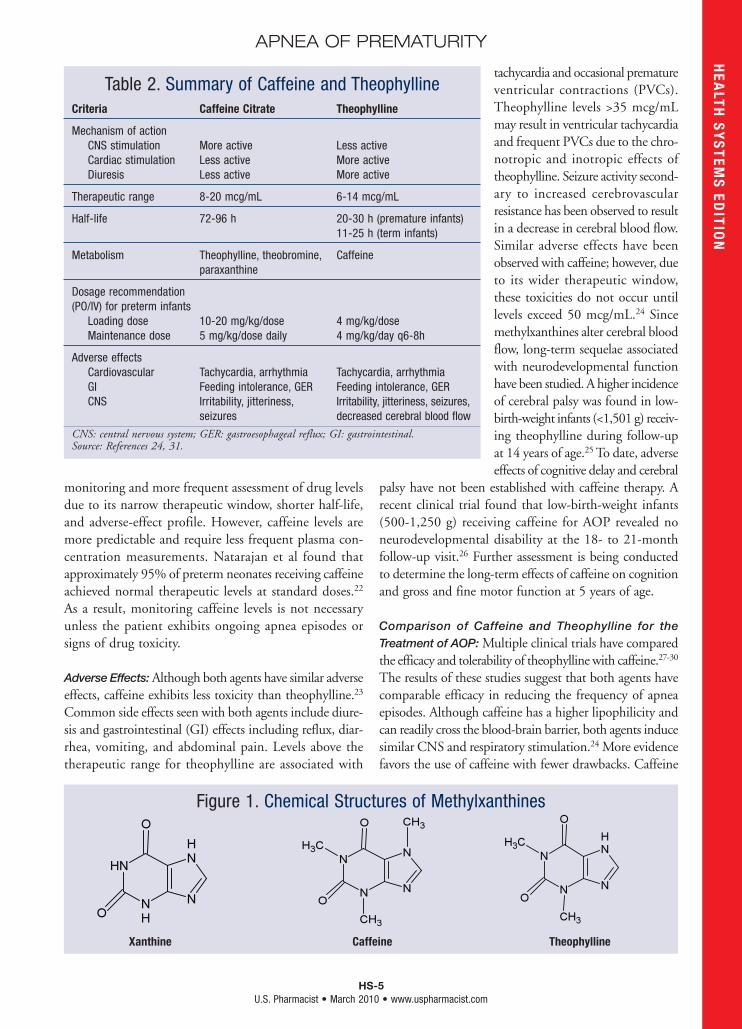
HS-5U.S. Pharmacist • March 2010 • www.uspharmacist.com
APNEA OF PREMATURITYH
EALTH
SY
STEM
S ED
ITION
monitoring and more frequent assessment of drug levels due to its narrow therapeutic window, shorter half-life, and adverse-effect profile. However, caffeine levels are more predictable and require less frequent plasma con-centration measurements. Natarajan et al found that approximately 95% of preterm neonates receiving caffeine achieved normal therapeutic levels at standard doses.22 As a result, monitoring caffeine levels is not necessary unless the patient exhibits ongoing apnea episodes or signs of drug toxicity.
Adverse Effects: Although both agents have similar adverse effects, caffeine exhibits less toxicity than theophylline.23 Common side effects seen with both agents include diure-sis and gastrointestinal (GI) effects including reflux, diar-rhea, vomiting, and abdominal pain. Levels above the therapeutic range for theophylline are associated with
tachycardia and occasional premature ventricular contractions (PVCs). Theophylline levels >35 mcg/mL may result in ventricular tachycardia and frequent PVCs due to the chro-notropic and inotropic effects of theophylline. Seizure activity second-ary to increased cerebrovascular resistance has been observed to result in a decrease in cerebral blood flow. Similar adverse effects have been observed with caffeine; however, due to its wider therapeutic window, these toxicities do not occur until levels exceed 50 mcg/mL.24 Since methylxanthines alter cerebral blood flow, long-term sequelae associated with neurodevelopmental function have been studied. A higher incidence of cerebral palsy was found in low-birth-weight infants (<1,501 g) receiv-ing theophylline during follow-up at 14 years of age.25 To date, adverse effects of cognitive delay and cerebral
palsy have not been established with caffeine therapy. A recent clinical trial found that low-birth-weight infants (500-1,250 g) receiving caffeine for AOP revealed no neurodevelopmental disability at the 18- to 21-month follow-up visit.26 Further assessment is being conducted to determine the long-term effects of caffeine on cognition and gross and fine motor function at 5 years of age.
Comparison of Caffeine and Theophylline for the Treatment of AOP: Multiple clinical trials have compared the efficacy and tolerability of theophylline with caffeine.27-30 The results of these studies suggest that both agents have comparable efficacy in reducing the frequency of apnea episodes. Although caffeine has a higher lipophilicity and can readily cross the blood-brain barrier, both agents induce similar CNS and respiratory stimulation.24 More evidence favors the use of caffeine with fewer drawbacks. Caffeine
Figure 1. Chemical Structures of Methylxanthines
Xanthine Caffeine Theophylline
Table 2. Summary of Caffeine and TheophyllineCriteria Caffeine Citrate Theophylline
Mechanism of action CNS stimulation More active Less active Cardiac stimulation Less active More active Diuresis Less active More active
Therapeutic range 8-20 mcg/mL 6-14 mcg/mL
Half-life 72-96 h 20-30 h (premature infants) 11-25 h (term infants)
Metabolism Theophylline, theobromine, Caffeine paraxanthine
Dosage recommendation (PO/IV) for preterm infants Loading dose 10-20 mg/kg/dose 4 mg/kg/dose Maintenance dose 5 mg/kg/dose daily 4 mg/kg/day q6-8h
Adverse effects Cardiovascular Tachycardia, arrhythmia Tachycardia, arrhythmia GI Feeding intolerance, GER Feeding intolerance, GER CNS Irritability, jitteriness, Irritability, jitteriness, seizures, seizures decreased cerebral blood flow
CNS: central nervous system; GER: gastroesophageal reflux; GI: gastrointestinal.Source: References 24, 31.
HS02 Apnea 3_1bo.indd HS-5HS02 Apnea 3_1bo.indd HS-5 3/2/10 9:54 AM3/2/10 9:54 AM

HS-6U.S. Pharmacist • March 2010 • www.uspharmacist.com
APNEA OF PREMATURITY
HEA
LTH S
YS
TEMS
EDITIO
N
allows for once-daily administration and infrequent ther-apeutic drug monitoring; it also has a wider therapeutic margin causing fewer side effects. Adverse effects, primar-ily tachycardia and GI effects, were significantly greater in infants treated with theophylline than with caffeine. There-fore, caffeine is recommended as the first-line agent to be used in the treatment of AOP. TABLE 2 summarizes the comparison of caffeine and theophylline.
Other Treatment OptionsAlthough other drug therapies are currently in develop-ment for the treatment of AOP, caffeine remains the standard of care. Doxapram is indicated for patients unre-sponsive to methylxanthines and is currently not available in the United States. Doxapram works as a central respi-ratory stimulant by activating the peripheral carotid che-moreceptors.32 However, severe cardiac adverse effects such as second-degree atrioventricular block, QT interval pro-longation, and arrhythmias limit its use. Administration by continuous infusion, the need for therapeutic drug monitoring, and the inclusion of benzyl alcohol in its formulation also restrict the use of doxapram.
Supplemental agents under investigation for the treat-ment of AOP include carnitine and creatine. Carnitine facilitates the transfer of fatty acids into the mitochondria
for the production of adenosine triphosphate. The lack of energy production from carnitine deficiency in preterm infants may lead to hypotonia. The rationale behind carnitine supplementation is to improve ventilatory wean-ing and reduce the number of apnea events.33 Current studies suggest no additional benefits with carnitine sup-plementation.34 As with carnitine, preterm infants may have a deficiency in creatine.35 Phosphocreatine is essential for ATP synthesis, thus preventing muscle fatigue. How-ever, current evidence does not show symptom improve-ment of AOP with creatine supplementation.
ConclusionIn summary, caffeine and theophylline are equally effective in the treatment of AOP. Caffeine is the preferred meth-ylxanthine since it allows for once-daily administration and infrequent monitoring, has a better tolerability profile, and does not significantly cause neurodevelopmental dis-ability in comparison to theophylline. Discontinuation of drug therapy is largely empirical, typically occurring at 40-weeks’ postconceptional age or when AOP ceases. A small percentage of patients may require home monitoring for apnea episodes upon hospital discharge. Although supplemental agents are undergoing investigation, these agents are currently not recommended.
REFERENCES1. Taeusch HW, Ballard RA, Gleason CA. Avery’s Diseases of the Newborn. 8th ed. Philadelphia, PA: Elsevier, Inc.; 2005:619-620.2. Anas NG, Perkin RM. The pathophysiology of apnea of infancy. Perinatal-Neonatal. 1984;8:58-70.3. Martin RJ, Fanaroff AA, Walsh MC. Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. Philadelphia, PA: Mosby Elsevier; 2006:1135-1141.4. Martin RJ, Miller MJ, Carlo WA. Pathogenesis of apnea in preterm infants. J Pediatr. 1986;109:733-741.5. Wilson CG, Martin RJ, Jaber M, et al. Adenosine A2A receptors interact with GABAergic pathways to modulate respiration in neonatal piglets. Respir Physiol Neurobiol. 2004;14:201-211.6. Herlenius E, Lagercrantz H. Adenosinergic modulation of respiratory neurones in the neonatal rat brainstem in vitro. J Physiol. 1999;518:159-172.7. McIntosh-Yellin NL, Drew BJ, Scheinman MM. Safety and efficacy of central intravenous bolus administration of adenosine for termination of supraventricular tachycardia. J Am Coll Cardiol. 1993;22:741-745.8. Corvaglia L, Zama D, Gualdi S, et al. Gastro-oesophageal reflux increases the number of apneoas in very preterm infants. Arch Dis Child Fetal Neonatal Ed. 2009;94:188-192.9. Krauss AN. Apnea in infancy: pathophysiology, diagnosis, and treatment. NY State J Med. 1986;86:89-96.10. Henderson-Smart DJ. The effect of gestational age on the incidence and duration of recurrent apneoa in newborn babies. Aust Paediatr J. 1981;17:273-276.11. Eichenwald EC, Aina A, Stark A. Apnea frequently persists beyond term gestation in infants delivered at 24 to 28 weeks. Pediatrics. 1997;100:354-359.12. Cheung PY, Barrington KJ, Finer NN, Robertson CM. Early childhood neurodevel-opment in very low birth weight infants with pre-discharge apnea. Pediatr Pulmonol. 1999;27:14-20.13. Jones RA, Lukeman D. Apnoea of immaturity. 2. Mortality and handicap. Arch Dis Child. 1982;57:766-768.14. Grisemer AN. Apnea of prematurity; current management and nursing implications. Pediatr Nurs. 1990;16:606-611.15. Bhatia J. Current options in the management of apnea of prematurity. Clin Pediatr (Phila). 2000;39:327-336.16. Gayan-Ramirez G, Janssens S, Himpens B, Decramer M. Mechanism of theophyl-line-induced inotropic effects on foreshortened canine diaphragm. Eur Respir J. 1995;8:1915-1921.17. Polson JB, Krzanowski JJ, Goldman AL, Szentivanyi A. Inhibition of human pulmonary phosphodiesterase activity by therapeutic levels of theophylline. Clin Exp Pharmacol Physiol. 1978;5:535-539.18. Aubier M, Murciano D, Viires N, et al. Diaphragmatic contractility enhanced by
aminophylline: role of extracellular calcium. J Appl Physiol. 1983;54:460-464.19. Davis JM, Spitzer AR, Stefano JL, et al. Use of caffeine in infants unresponsive to theophylline in apnea of prematurity. Pediatr Pulmonol. 1987;3:90-93.20. Hendeles L, Jenkins J, Temple R. Revised FDA labeling guideline for theophylline oral dosage forms. Pharmacotherapy. 1995;15:409-427.21. Erenberg A, Leff RD, Haack DG, et al. Caffeine citrate for the treatment of apnea of prematurity: a double-blind, placebo-controlled study. Pharmacotherapy. 2000;20:644-652.22. Natarajan G, Botica ML, Thomas R, Aranda JV. Therapeutic drug monitoring for caffeine in preterm neonates: an unnecessary exercise? Pediatrics. 2007;119:936-940.23. Bhatt-Mehta V, Schumacher RE. Treatment of apnea of prematurity. Pediatr Drugs. 2003;5:195-210.24. Aranda JV, Cook CE, Gorman W, et al. Pharmacokinetic profile of caffeine in the premature newborn infant with apnea. J Pediatr. 1079;94:663-668.25. Davis PG, Doyle LW, Rickards AL, et al. Methylxanthines and sensorineural out-come at 14 years in children < 1501 g birth weight. J Paediatr Child Health. 2000;36:47-50.26. Schmidt B, Roberts RS, Davis P, et al. Long-term effects of caffeine therapy for apnea of prematurity. N Engl J Med. 2007;257:1893-1902.27. Brouard C, Moriette D, Murat I, et al. Comparative efficacy of theophylline and caffeine in the treatment of idiopathic apnea of premature infants. Am J Dis Child. 1985;139:698-700.28. Bairam A, Boutroy MJ, Badonnel Y, et al. Theophylline versus caffeine: comparative effects in the treatment of idiopathic apnea in the preterm infant. J Pediatr. 1987;110:636-638.29. Scanlon JE, Chin KC, Morgan ME, et al. Caffeine or theophylline for neonatal apnea? Arch J Dis Child. 1992;67:425-428.30. Larsen PB, Brendstrup, Skov L, Fachs L. Aminophylline versus caffeine citrate for apnea and bradycardia prophylaxis in premature neonates. Acta Paediatr. 1995;84:360-364.31. Taketomo CK, Hodding JH, Kraus DM. Pediatric Dosage Handbook. 16th ed. Houston, TX: Lexi-Comp Inc; 2009.32. Edwards G, Lond MB, Leszczynski SO. A double-blind trial of five respiratory stim-ulants in patients with acute ventilatory failure. Lancet. 1967;290:226-229.33. O’Donnell J, Finer NN, Rich W, et al. Role of L-carnitine in apnea of prematurity: a randomized, controlled trial. Pediatrics. 2002;109:622-626.34. Kumar M, Kabra NS, Paes B. Carnitine supplementation for preterm infants with recurrent apnea. Cochrane Database Syst Rev. 2004;(4):CD004497.35. Bohnhorst B, Geuting T, Peter CS, et al. Randomized, controlled trial of oral creatine supplementation (not effective) for apnea of prematurity. Pediatrics. 2004;113:e303-e307.
HS02 Apnea 3_1bo.indd HS-6HS02 Apnea 3_1bo.indd HS-6 3/2/10 9:54 AM3/2/10 9:54 AM

A Reflection of Outstanding Service.
For the 9th consecutive year, Eisai Inc. has recognized pharmacists who have had anextraordinary impact on the lives of individuals with Alzheimer’s disease and their families.In 2009, Eisai and the Alzheimer’s Association were pleased to honor Heather Allison Greene,PharmD as the recipient of the C.A.R.E. (Commitment to Alzheimer’s. Recognition ofExcellence.) Pharmacy Award.Dr. Greene has played a critical role in helping to educate patients and caregivers aboutAlzheimer’s disease. As a Geriatric Consultant Pharmacist with the Riverside Health
System’s PACE Program in Richmond, Virginia, she is a member of an interdisciplinary team that provides carefor some of the areas frailest seniors. In the nomination for her work with Alzheimer’s disease patients andcaregivers, Dr. Greene was described as someone “who goes far beyond being a pharmacist when she workswith patients and their families.” She received her Doctor of Pharmacy degree from the School of Pharmacy atVirginia Commonwealth University.
Congratulations, Dr. Greene, and thank you for your remarkable efforts on behalf of those affected byAlzheimer’s disease.
©2010 Eisai Inc. EISTRR052 MMG735

HS-8U.S. Pharmacist • March 2010 • www.uspharmacist.com
Hypertension has become a significant pediatric health problem owing to the increased number of overweight children. Over the past two decades,
a steep rise in the prevalence of childhood obesity has been seen.1 As the prevalence of hypertension has increased, a direct relationship between weight and systolic blood pressure (SBP) has been reported.2,3 In 2004, almost 20% of children aged 6 to 11 years were obese (body-mass index [BMI] ≥95th percentile) and slightly more than 30% were overweight or at risk of overweight (BMI ≥85th percentile).4 A recent study estimated the incidence of obesity in 35-year-olds in 2020 based on the prevalence of overweight adolescents in 2000. The investigators projected that there would be a considerable increase in obesity, which could lead to a significant increase in adult coronary heart disease.5
In addition to hypertension, obesity in children and adolescents may lead to other comorbidities, such as type 2 diabetes, obstructive sleep apnea, dyslipidemia, and metabolic syndrome.6 According to recent epide-miologic studies, hypertension is currently diagnosed in approximately 5% of adolescents.7,8
EtiologyHypertension can be secondary to another disease process, or it can be primary (also known as essential). Secondary hypertension, which is more common in pediatric patients, is most often caused by renal disease, coarctation of the aorta, or endocrine disease.9 Primary hypertension usually is associated with a positive family history of hypertension or cardiovas-cular disease. It has been observed that patients with primary hyperten-
sion frequently are overweight and that the prevalence of hypertension increases with increasing BMI.10
Diagnosis and MonitoringThe current guidelines of the National High Blood Pres-sure Education Program Working Group on High Blood Pressure in Children and Adolescents recommend that BP monitoring begin in children over the age of 3 years.11
BP should be measured at each health care visit via auscultation. When measuring BP in children, it is important that the appropriate cuff size be used, based on the size of the child’s upper arm. A cuff that is too large will cause BP to be underestimated, whereas a cuff that is too small will cause it to be overestimated. In addition, it is recommended that the child avoid stimu-lants (e.g., caffeine, medications), be in a nonthreatening environment when measured, and sit quietly for 5 min-utes with the back supported and the arm supported at the level of the heart. Based on certain conditions, some children should have their BP measured before age 3 years.11 Conditions that warrant BP measurement in children younger than 3 years are listed in TABLE 1.11
Classification and StagingIn children and adolescents, normal BP is based on gender, age, and height. The Fourth Report on the
Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents provides tables includ-ing the 50th, 90th, 95th, and 99th percentiles by gender, age, and height (see TABLE 2 for an example).11 The height percentile is determined by using the Centers for Disease Control and Prevention growth charts. Once
Pediatric Hypertension A Review of Diagnosis and Treatment
Terri M. Wensel, PharmD, BCPSAssistant Professor of Pharmacy
Samford University McWhorter School of Pharmacy
Birmingham, Alabama
Shannon Williams, PharmDAssistant Professor
Wingate University School of PharmacyWingate, North Carolina
HEA
LTH S
YS
TEMS
EDITIO
N
© THINKSTOCK
HS08 PedHyperten 3_1mb.indd HS-8HS08 PedHyperten 3_1mb.indd HS-8 3/2/10 10:06 AM3/2/10 10:06 AM
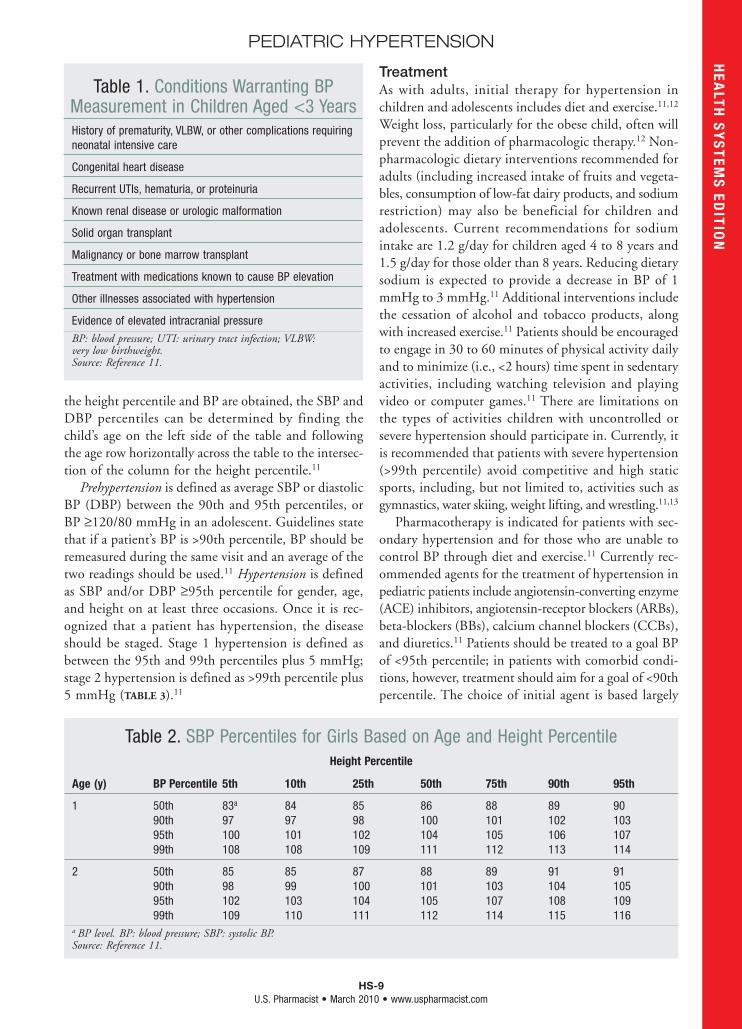
HS-9U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC HYPERTENSION
the height percentile and BP are obtained, the SBP and DBP percentiles can be determined by finding the child’s age on the left side of the table and following the age row horizontally across the table to the intersec-tion of the column for the height percentile.11
Prehypertension is defined as average SBP or diastolic BP (DBP) between the 90th and 95th percentiles, or BP ≥120/80 mmHg in an adolescent. Guidelines state that if a patient’s BP is >90th percentile, BP should be remeasured during the same visit and an average of the two readings should be used.11 Hypertension is defined as SBP and/or DBP ≥95th percentile for gender, age, and height on at least three occasions. Once it is rec-ognized that a patient has hypertension, the disease should be staged. Stage 1 hypertension is defined as between the 95th and 99th percentiles plus 5 mmHg; stage 2 hypertension is defined as >99th percentile plus 5 mmHg (TABLE 3).11
TreatmentAs with adults, initial therapy for hypertension in children and adolescents includes diet and exercise.11,12 Weight loss, particularly for the obese child, often will prevent the addition of pharmacologic therapy.12 Non-pharmacologic dietary interventions recommended for adults (including increased intake of fruits and vegeta-bles, consumption of low-fat dairy products, and sodium restriction) may also be beneficial for children and adolescents. Current recommendations for sodium intake are 1.2 g/day for children aged 4 to 8 years and 1.5 g/day for those older than 8 years. Reducing dietary sodium is expected to provide a decrease in BP of 1 mmHg to 3 mmHg.11 Additional interventions include the cessation of alcohol and tobacco products, along with increased exercise.11 Patients should be encouraged to engage in 30 to 60 minutes of physical activity daily and to minimize (i.e., <2 hours) time spent in sedentary activities, including watching television and playing video or computer games.11 There are limitations on the types of activities children with uncontrolled or severe hypertension should participate in. Currently, it is recommended that patients with severe hypertension (>99th percentile) avoid competitive and high static sports, including, but not limited to, activities such as gymnastics, water skiing, weight lifting, and wrestling.11,13
Pharmacotherapy is indicated for patients with sec-ondary hypertension and for those who are unable to control BP through diet and exercise.11 Currently rec-ommended agents for the treatment of hypertension in pediatric patients include angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs), beta-blockers (BBs), calcium channel blockers (CCBs), and diuretics.11 Patients should be treated to a goal BP of <95th percentile; in patients with comorbid condi-tions, however, treatment should aim for a goal of <90th percentile. The choice of initial agent is based largely
HEA
LTH S
YS
TEMS
EDITIO
N
Table 2. SBP Percentiles for Girls Based on Age and Height PercentileHeight Percentile
Age (y) BP Percentile 5th 10th 25th 50th 75th 90th 95th
1 50th 83a 84 85 86 88 89 90 90th 97 97 98 100 101 102 103 95th 100 101 102 104 105 106 107 99th 108 108 109 111 112 113 114
2 50th 85 85 87 88 89 91 91 90th 98 99 100 101 103 104 105 95th 102 103 104 105 107 108 109 99th 109 110 111 112 114 115 116a BP level. BP: blood pressure; SBP: systolic BP.Source: Reference 11.
Table 1. Conditions Warranting BP Measurement in Children Aged <3 YearsHistory of prematurity, VLBW, or other complications requiring neonatal intensive care
Congenital heart disease
Recurrent UTIs, hematuria, or proteinuria
Known renal disease or urologic malformation
Solid organ transplant
Malignancy or bone marrow transplant
Treatment with medications known to cause BP elevation
Other illnesses associated with hypertension
Evidence of elevated intracranial pressure
BP: blood pressure; UTI: urinary tract infection; VLBW: very low birthweight.Source: Reference 11.
HS08 PedHyperten 3_1mb.indd HS-9HS08 PedHyperten 3_1mb.indd HS-9 3/2/10 10:06 AM3/2/10 10:06 AM

HS-10U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC HYPERTENSION
upon clinician preference or compelling indications, as evidence of the impact on clinical outcomes is lacking.11 For example, a BB or alpha antagonist would be most beneficial in a patient with high catecholamine levels.12 For a diabetic patient, an ACE inhibitor would be ideal.11 Additional conditions to take into consideration when selecting an agent are the presence of symptom-atic hypertension, secondary causes of hypertension, target-organ damage, and persistent hypertension despite nonpharmacologic interventions.11
Several ACE inhibitors have been studied in children, with captopril having the most evidence. Enalapril, lisinopril, and ramipril have been assessed in small tri-als and pharmacokinetic studies.14 In the treatment of
adult hypertension, it is well established that this class of medications has disparities in efficacy according to race. A recently published meta-analysis evaluated results from six trials submitted to the FDA to determine whether these differences were present among children as well. Agents studied included benazepril, enalapril, fosinopril, lisinopril, quinapril, and ramipril. This analysis found that, even with high-dose therapy, Afri-can American children did not respond to ACE inhib-itor therapy as well as children of other races did.15
CCBs are also commonly prescribed for pediatric patients. Nifedipine, isradipine, amlodipine, and nicardipine have the most evidence for use. Short-acting nifedipine is typically used for hypertensive crisis. Data regarding the use of extended-release nifedipine are limited; however, anecdotal reports show that it has been well tolerated when given at doses less than 120 mg/day.16 Retrospective data for isradipine are available. These trials utilized a much higher dose than that recommended for adults and administered the drug multiple times per day, which may limit the usefulness of the drug.16 Amlodipine may be a more desirable alternative owing to its longer half-life and capacity for once-daily dosing. Additionally, an amlodipine suspension may be pre-pared that has extended stability. Nicardipine is largely
HEA
LTH S
YS
TEMS
EDITIO
N
Table 3. Classification of Hypertension in Children and Adolescents
SBP or DBP Percentile
Normal <90thPrehypertension 90th-<95th or if BP >120/80Stage 1 hypertension 95th-99th + 5 mmHgStage 2 hypertension >99th + 5 mmHg
DBP: diastolic blood pressure; SBP: systolic blood pressure.Source: Reference 11.
Table 4. Pharmacologic Options for Treatment of Pediatric HypertensionClass Agent Dose Side Effects
ACE inhibitors Captopril Initial: 0.02-1.5 mg/kg/day Max: 6 mg/kg/day
Enalapril Initial: 0.04 mg/kg/day, up to 5 mg/day Max: 0.6 mg/kg/day, up to 40 mg/day
Lisinopril Initial: 0.07 mg/kg/day, up to 5 mg/day Max: 0.6 mg/kg/day, up to 40 mg/day
ARBs Candesartan Up to 8 mg/day
Irbesartan 6-12 y: 75-150 mg/day ≥13 y: 150-300 mg/day
Losartan Initial: 0.7 mg/kg/day up to 50 mg/day Max: 1.4 mg/kg/day, up to 100 mg/day
Valsartan 20-80 mg/day
CCBs Amlodopine 6-17 y: 2.5-5 mg/day
Isradapine Initial: 0.15-0.2 mg/kg/day Max: 0.8 mg/kg/day up to 20 mg/day
Nifedipine ER Initial: 0.25-0.5 mg/kg/day Max: 3 mg/kg/day up to 120 mg/day
ACE: angiotensin-converting enzyme; ARB: angiotensin-receptor blocker; CCB: calcium channel blocker; ER: extended-release; GFR: glomerular filtration rate; max: maximum; NV: nausea and vomiting.Source: References 10, 11, 13, 15, 16.
Hyperkalemia, cough, angioedema, decreased GFR, loss of taste, thrombocytopenia
Similar to ACE inhibitors without chronic cough
Headache, flushing, dizziness, tachycardia, peripheral edema, gingival hyperplasia, chest pain, NV, constipation
HS08 PedHyperten 3_1mb.indd HS-10HS08 PedHyperten 3_1mb.indd HS-10 3/2/10 10:06 AM3/2/10 10:06 AM
©2009 Mylan Pharmaceuticals Inc. MYNFEN031
In the management of persistent, moderate to severe chronic pain that requirescontinuous, around-the-clock opioid administration for
an extended period of time and cannot be managed by other means*
One patch can cause burns.This matrix patch contains aluminum in its backing, which can overheat during a magnetic resonance imaging (MRI) scan and burn the patient who is wearing it.
Other patches can leak.They contain a reservoir of fentanyl gel that can leak and cause potentially life-threatening complications.
Mylan FENTANYL is the first marketed fentanyl patch designed to avoid the
risks associated with burns and leaks.The Mylan FENTANYL TRANSDERMALSYSTEM CII has no aluminum or othermetals in its backing. Also important to patient safety, Mylan Fentanyl has aproprietary matrix design without a liquid, gel-filled reservoir that can leak. It is an innovative solution in transdermaldrug delivery.
*Other means include non-steroidal analgesics, opioid combination products, or immediate-release opioids.
No metal. No burns. No leaks.
Why Take A Chance With Other Fentanyl Patches?
Fentanyl transdermal system should ONLY be used in patients who are already receiving opioid therapy, who have demonstrated opioid tolerance, and who require a total daily dose at least equivalent to fentanyl transdermal system25 mcg/hr. Patients who are consideredopioid-tolerant are those who have beentaking, for a week or longer, at least 60 mgof morphine daily, or at least 30 mg of oraloxycodone daily, or at least 8 mg of oralhydromorphone daily or an equianalgesicdose of another opioid.
Because serious or life-threateninghypoventilation could occur, fentanyltransdermal system is contraindicated:
• in patients who are not opioid-tolerant • in the management of acute pain or in
patients who require opioid analgesia for a short period of time
• in the management of postoperative pain, including use after out patient or day surgeries (e.g., tonsillectomies)
• in the management of mild pain• in the management of intermittent
pain [e.g., use on an as needed basis(prn)]
The safety of fentanyl transdermal systemhas not been established in children under2 years of age. Fentanyl transdermalsystem should be administered to childrenonly if they are opioid-tolerant and 2 yearsof age or older (see PRECAUTIONS: Pediatric Use).
Patients using fentanyl transdermal systemshould avoid exposure to external heatsources, such as heating pads, hot tubs,long hot baths, and sunbathing. An increasein body temperature may result in a suddenand possible dangerous rise in their bodyfentanyl level. Fentanyl transdermal system may cause death from overdosage; therefore, it is important for healthcare professionals, patients and caregivers toknow the signs of fentanyl overdose, whichcan include trouble breathing and extremesleepiness. Fentanyl transdermal systemshould be stored in a safe place and kept out of the reach of children. Used, unneeded or defective fentanyl patchesshould be safely disposed of by folding the sticky side of the patch together(until it sticks to itself) and flushing it down the toilet.
The most common adverse events reported in clinical trials were fever, nausea, vomiting,constipation, dry mouth, somnolence, confusion, asthenia, and sweating.
Please see adjacent Brief Summary of Prescribing Information, including BOXED WARNING.
FENTANYL TRANSDERMAL SYSTEM
BRIEF SUMMARY: Please see package insert for full prescribing information.FOR USE IN OPIOID-TOLERANT PATIENTS ONLY
INDICATIONS AND USAGE: Fentanyl transdermal system is indicated for management of persistent, moderate to severechronic pain that:
• requires continuous, around-the-clock opioid administration for an extended period of time, and• cannot be managed by other means such as non-steroidal analgesics, opioid combination products, or
immediate-release opioidsFentanyl transdermal system should ONLY be used in patients who are already receiving opioid therapy, who have
demonstrated opioid tolerance, and who require a total daily dose at least equivalent to fentanyl transdermal system25 mcg/hr (see DOSAGE AND ADMINISTRATION in full prescribing information). Patients who are considered opioid-tolerant are those who have been taking, for a week or longer, at least 60 mg of morphine daily, or at least 30 mg of oral oxycodone daily, or at least 8 mg of oral hydromorphone daily, or an equianalgesic dose of another opioid.
Because serious or life-threatening hypoventilation could result, fentanyl transdermal system is contraindicatedfor use on an as needed basis (i.e., prn), for the management of postoperative or acute pain, or in patients who are notopioid-tolerant or who require opioid analgesia for a short period of time (see BOX WARNING and CONTRAINDICATIONS).
An evaluation of the appropriateness and adequacy of treating with immediate-release opioids is advisable priorto initiating therapy with any modified-release opioid. Prescribers should individualize treatment in every case, initiating therapy at the appropriate point along a progression from non-opioid analgesics, such as non-steroidalanti-inflammatory drugs and acetaminophen, to opioids, in a plan of pain management such as outlined by the WorldHealth Organization, the Agency for Health Research and Quality, the Federation of State Medical Boards Model Policy,or the American Pain Society.
Patients should be assessed for their clinical risks for opioid abuse or addiction prior to being prescribed opioids.Patients receiving opioids should be routinely monitored for signs of misuse, abuse, and addiction. Persons atincreased risk for opioid abuse include those with a personal or family history of substance abuse (including drug oralcohol abuse or addiction) or mental illness (e.g., major depression). Patients at increased risk may still be appropriately treated with modified-release opioid formulations; however these patients will require intensive monitoring for signs of misuse, abuse, or addiction. CONTRAINDICATIONS: Because serious or life-threatening hypoventilation could occur, fentanyl transdermal system is contraindicated:
• in patients who are not opioid-tolerant• in the management of acute pain or in patients who require opioid analgesia for a short period of time• in the management of postoperative pain, including use after out-patient or day surgeries (e.g., tonsillectomies)• in the management of mild pain
• in the management of intermittent pain [e.g., use on an as needed basis (prn)]• in situations of significant respiratory depression, especially in unmonitored settings where there is a lack
of resuscitative equipment• in patients who have acute or severe bronchial asthmaFentanyl transdermal system is contraindicated in patients who have or are suspected of having paralytic ileus.Fentanyl transdermal system is contraindicated in patients with known hypersensitivity to fentanyl or any
components of this product.WARNINGS: Fentanyl transdermal systems are intended for transdermal use (on intact skin) only. Do not use a fentanyl transdermal system if the seal is broken or the patch is cut, damaged, or changed in any way.
The safety of fentanyl transdermal system has not been established in children under 2 years of age. Fentanyltransdermal system should be administered to children only if they are opioid-tolerant and 2 years of age or older(see PRECAUTIONS: Pediatric Use in full prescribing information).
Fentanyl transdermal system is ONLY for use in patients who are already tolerant to opioid therapy of comparable potency. Use in non-opioid-tolerant patients may lead to fatal respiratory depression.Overestimating the fentanyl transdermal system dose when converting patients from another opioid medicationcan result in fatal overdose with the first dose. The mean elimination half-life of fentanyl transdermal system is 17 hours. Therefore, patients who have experienced serious adverse events, including overdose, will require monitoring for at least 24 hours after fentanyl transdermal system removal since serum fentanyl concentrationsdecline gradually and reach an approximate 50% reduction in serum concentrations 17 hours after system removal.
Fentanyl transdermal system should be prescribed only by persons knowledgeable in the continuous administration of potent opioids, in the management of patients receiving potent opioids for treatment of pain, andin the detection and management of hypoventilation including the use of opioid antagonists.
All patients and their caregivers should be advised to avoid exposing the fentanyl transdermal system application site and surrounding area to direct external heat sources, such as heating pads or electric blankets,heat or tanning lamps, saunas, hot tubs, and heated water beds, etc., while wearing the system. Patients shouldbe advised against taking hot baths or sunbathing. There is a potential for temperature-dependent increases infentanyl released from the system resulting in possible overdose and death.
Based on a pharmacokinetic model, serum fentanyl concentrations could theoretically increase by approximatelyone-third for patients with a body temperature of 40°C (104°F) due to temperature-dependent increases in fentanylreleased from the system and increased skin permeability. Patients wearing fentanyl transdermal systems whodevelop fever or increased core body temperature due to strenuous exertion should be monitored for opioid sideeffects and the fentanyl transdermal system dose should be adjusted if necessary.
Death and other serious medical problems have occurred when people were accidentally exposed to fentanyltransdermal system. Examples of accidental exposure include transfer of a fentanyl transdermal system from anadult’s body to a child while hugging, accidental sitting on a patch and possible accidental exposure of a caregiver’sskin to the medication in the patch while the caregiver was applying or removing the patch.
Placing fentanyl transdermal system in the mouth, chewing it, swallowing it, or using it in ways other than indicated may cause choking or overdose that could result in death. Misuse, Abuse and Diversion of Opioids
Fentanyl is an opioid agonist of the morphine-type. Such drugs are sought by drug abusers and people with addiction disorders and are subject to criminal diversion.
Fentanyl can be abused in a manner similar to other opioids, legal or illicit. This should be considered when prescribing or dispensing fentanyl transdermal system in situations where the physician or pharmacist is concernedabout an increased risk of misuse, abuse or diversion.
Fentanyl transdermal system has been reported as being abused by other methods and routes of administration.These practices will result in uncontrolled delivery of the opioid and pose a significant risk to the abuser that couldresult in overdose and deaths (see WARNINGS and DRUG ABUSE AND ADDICTION).
Concerns about abuse, addiction and diversion should not prevent the proper management of pain. However, all patients treated with opioids require careful monitoring for signs of abuse and addiction, since use of opioid analgesic products carries the risk of addiction even under appropriate medical use.
Healthcare professionals should contact their state professional licensing board or state controlled substancesauthority for information on how to prevent and detect abuse or diversion of this product. Hypoventilation (Respiratory Depression): Serious or life-threatening hypoventilation may occur at any time duringthe use of fentanyl transdermal system especially during the initial 24 to 72 hours following initiation of therapy andfollowing increases in dose.
Because significant amounts of fentanyl are absorbed from the skin for 17 hours or more after the patch isremoved, hypoventilation may persist beyond the removal of fentanyl transdermal system. Consequently, patients with hypoventilation should be carefully observed for degree of sedation and their respiratory rate monitored until respiration has stabilized.
The use of concomitant CNS active drugs requires special patient care and observation. Respiratory depression is the chief hazard of opioid agonists, including fentanyl the active ingredient in fentanyl
transdermal system. Respiratory depression is more likely to occur in elderly or debilitated patients, usually followinglarge initial doses in non-tolerant patients, or when opioids are given in conjunction with other drugs that depressrespiration.
Respiratory depression from opioids is manifested by a reduced urge to breathe and a decreased rate of respira-tion, often associated with the “sighing” pattern of breathing (deep breaths separated by abnormally long pauses).Carbon dioxide retention from opioid-induced respiratory depression can exacerbate the sedating effects of opioids.This makes overdoses involving drugs with sedative properties and opioids especially dangerous.
Fentanyl transdermal system should be used with extreme caution in patients with significant chronic obstructivepulmonary disease or cor pulmonale, and in patients having a substantially decreased respiratory reserve, hypoxia,hypercapnia, or preexisting respiratory depression. In such patients, even usual therapeutic doses of fentanyl transdermal system may decrease respiratory drive to the point of apnea. In these patients, alternative non-opioid analgesics should be considered, and opioids should be employed only under careful medical supervision at the lowest effective dose. Chronic Pulmonary Disease: Because potent opioids can cause serious or life-threatening hypoventilation, fentanyltransdermal system should be administered with caution to patients with preexisting medical conditions predisposingthem to hypoventilation. In such patients, normal analgesic doses of opioids may further decrease respiratory drive tothe point of respiratory failure. Head Injuries and Increased Intracranial Pressure: Fentanyl transdermal system should not be used in patients whomay be particularly susceptible to the intracranial effects of CO2 retention such as those with evidence of increasedintracranial pressure, impaired consciousness, or coma. Opioids may obscure the clinical course of patients with headinjury. Fentanyl transdermal system should be used with caution in patients with brain tumors. Interactions with other CNS Depressants: The concomitant use of fentanyl transdermal system with other centralnervous system depressants, including but not limited to other opioids, sedatives, hypnotics, tranquilizers (e.g., benzodiazepines), general anesthetics, phenothiazines, skeletal muscle relaxants, and alcohol, may cause respiratory depression, hypotension, and profound sedation or potentially result in coma. When such combined therapy is contemplated, the dose of one or both agents should be significantly reduced. Interactions with Alcohol and Drugs of Abuse: Fentanyl may be expected to have additive CNS depressant effectswhen used in conjunction with alcohol, other opioids, or illicit drugs that cause central nervous system depression.Interactions with CYP3A4 Inhibitors: The concomitant use of transdermal fentanyl with all CYP3A4 inhibitors (suchas ritonavir, ketoconazole, itraconazole, troleandomycin, clarithromycin, nelfinavir, nefazadone, amiodarone, amprenavir, aprepitant, diltiazem, erythromycin, fluconazole, fosamprenavir, grapefruit juice, and verapamil) mayresult in an increase in fentanyl plasma concentrations, which could increase or prolong adverse drug effects andmay cause potentially fatal respiratory depression. Patients receiving fentanyl transdermal system and any CYP3A4inhibitor should be carefully monitored for an extended period of time, and dosage adjustments should be made if warranted (see BOX WARNING, CLINICAL PHARMACOLOGY: Drug Interactions in full prescribing information, PRECAUTIONS, and DOSAGE AND ADMINISTRATION in full prescribing information for further information).PRECAUTIONS: General: Fentanyl transdermal system should not be used to initiate opioid therapy in patients whoare not opioid-tolerant. Children converting to fentanyl transdermal system should be opioid-tolerant and 2 years ofage or older (see BOX WARNING).
Fentanyl transdermal system contains a high concentration of a potent Schedule II opioid agonist, fentanyl.Schedule II opioid substances which include fentanyl, hydromorphone, methadone, morphine, oxycodone, andoxymorphone have the highest potential for abuse and associated risk of fatal overdose due to respiratorydepression. Fentanyl can be abused and is subject to criminal diversion. The high content of fentanyl in thepatches (fentanyl transdermal system) may be a particular target for abuse and diversion.Fentanyl transdermal system is indicated for management of persistent, moderate to severe chronic pain that:
• requires continuous, around-the-clock opioid administration for an extended period of time, and• cannot be managed by other means such as non-steroidal analgesics, opioid combination products, or
immediate-release opioidsFentanyl transdermal system should ONLY be used in patients who are already receiving opioid therapy, whohave demonstrated opioid tolerance, and who require a total daily dose at least equivalent to fentanyl trans-dermal system 25 mcg/hr. Patients who are considered opioid-tolerant are those who have been taking, for aweek or longer, at least 60 mg of morphine daily, or at least 30 mg of oral oxycodone daily, or at least 8 mg oforal hydromorphone daily or an equianalgesic dose of another opioid.Because serious or life-threatening hypoventilation could occur, fentanyl transdermal system is contraindicated:
• in patients who are not opioid-tolerant• in the management of acute pain or in patients who require opioid analgesia for a short period of time• in the management of postoperative pain, including use after out patient or day surgeries (e.g., tonsillectomies)• in the management of mild pain• in the management of intermittent pain [e.g., use on an as needed basis (prn)]
(See CONTRAINDICATIONS for further information.)Since the peak fentanyl levels occur between 24 and 72 hours of treatment, prescribers should be aware thatserious or life-threatening hypoventilation may occur, even in opioid-tolerant patients, during the initial appli-cation period.The concomitant use of fentanyl transdermal system with all cytochrome P450 3A4 inhibitors (such as ritonavir, ketoconazole, itraconazole, troleandomycin, clarithromycin, nelfinavir, nefazodone, amiodarone,amprenavir, aprepitant, diltiazem, erythromycin, fluconazole, fosamprenavir, grapefruit juice, and verapamil)may result in an increase in fentanyl plasma concentrations, which could increase or prolong adverse drugeffects and may cause potentially fatal respiratory depression. Patients receiving fentanyl transdermal system and any CYP3A4 inhibitor should be carefully monitored for an extended period of time and dosageadjustments should be made if warranted (see CLINICAL PHARMACOLOGY: Drug Interactions, WARNINGS, PRECAUTIONS and DOSAGE AND ADMINISTRATION in full prescribing information for further information). Thesafety of fentanyl transdermal system has not been established in children under 2 years of age. Fentanyltransdermal system should be administered to children only if they are opioid-tolerant and 2 years of age orolder (see PRECAUTIONS: Pediatric Use in full prescribing information).Fentanyl transdermal system is ONLY for use in patients who are already tolerant to opioid therapy of compa-rable potency. Use in non-opioid-tolerant patients may lead to fatal respiratory depression. Overestimating thefentanyl transdermal system dose when converting patients from another opioid medication can result in fataloverdose with the first dose. Due to the mean elimination half-life of 17 hours of fentanyl transdermal system,patients who are thought to have had a serious adverse event, including overdose, will require monitoring andtreatment for at least 24 hours.Fentanyl transdermal system can be abused in a manner similar to other opioid agonists, legal or illicit. Thisrisk should be considered when administering, prescribing, or dispensing fentanyl transdermal system in situations where the healthcare professional is concerned about increased risk of misuse, abuse or diversion.Persons at increased risk for opioid abuse include those with a personal or family history of substance abuse(including drug or alcohol abuse or addiction) or mental illness (e.g., major depression). Patients should beassessed for their clinical risks for opioid abuse or addiction prior to being prescribed opioids. All patientsreceiving opioids should be routinely monitored for signs of misuse, abuse and addiction. Patients atincreased risk of opioid abuse may still be appropriately treated with modified-release opioid formulations;however, these patients will require intensive monitoring for signs of misuse, abuse, or addiction.Fentanyl transdermal system patches are intended for transdermal use (on intact skin) only. Do not use a fentanyl transdermal system if the seal is broken or the patch is cut, damaged, or changed in any way.Avoid exposing the fentanyl transdermal system application site and surrounding area to direct external heatsources, such as heating pads or electric blankets, heat or tanning lamps, saunas, hot tubs, and heated waterbeds, while wearing the system. Avoid taking hot baths or sunbathing. There is a potential for temperature-dependent increases in fentanyl released from the system resulting in possible overdose and death. Patientswearing fentanyl transdermal systems who develop fever or increased core body temperature due to strenuous exertion should be monitored for opioid side effects and the fentanyl transdermal system doseshould be adjusted if necessary.
Page 1 of 3
Patients, family members and caregivers should be instructed to keep patches (new and used) out of the reach of children and others for whom fentanyl transdermal system was not prescribed. A considerable amount of activefentanyl remains in fentanyl transdermal system even after use as directed. Accidental or deliberate application oringestion by a child or adolescent will cause respiratory depression that could result in death.Cardiac Disease: Fentanyl may produce bradycardia. Fentanyl should be administered with caution to patients withbradyarrhythmias. Hepatic or Renal Disease: Insufficient information exists to make recommendations regarding the use of fentanyltransdermal system in patients with impaired renal or hepatic function. If the drug is used in these patients, it shouldbe used with caution because of the hepatic metabolism and renal excretion of fentanyl. Use in Pancreatic/Biliary Tract Disease: Fentanyl transdermal system may cause spasm of the sphincter of Oddi andshould be used with caution in patients with biliary tract disease, including acute pancreatitis. Opioids like fentanyltransdermal system may cause increases in the serum amylase concentration. Tolerance: Tolerance is a state of adaptation in which exposure to a drug induces changes that result in a diminu-tion of one or more of the drug’s effects over time. Tolerance may occur to both the desired and undesired effects ofdrugs, and may develop at different rates for different effects. Physical Dependence: Physical dependence is a state of adaptation that is manifested by an opioid specific withdrawal syndrome that can be produced by abrupt cessation, rapid dose reduction, decreasing blood level of thedrug, and/or administration of an antagonist. The opioid abstinence or withdrawal syndrome is characterized by someor all of the following: restlessness, lacrimation, rhinorrhea, yawning, perspiration, chills, piloerection, myalgia, mydriasis, irritability, anxiety, backache, joint pain, weakness, abdominal cramps, insomnia, nausea, anorexia, vomiting, diarrhea, or increased blood pressure, respiratory rate, or heart rate. In general, opioids should not beabruptly discontinued (see DOSAGE AND ADMINISTRATION: Discontinuation of Fentanyl Transdermal System in full prescribing information). Ambulatory Patients: Strong opioid analgesics impair the mental or physical abilities required for the performance ofpotentially dangerous tasks, such as driving a car or operating machinery. Patients who have been given fentanyltransdermal system should not drive or operate dangerous machinery unless they are tolerant to the effects of the drug. Information for Patients: Patients and their caregivers should be provided with a Medication Guide each time fentanyl transdermal system is dispensed because new information may be available.
Patients receiving fentanyl transdermal system should be given the following instructions by the physician: 1. Patients should be advised that fentanyl transdermal systems contain fentanyl, an opioid pain medicine
similar to morphine, hydromorphone, methadone, oxycodone, and oxymorphone. 2. Patients should be advised that each fentanyl transdermal system may be worn continuously for 72 hours, and
that each patch should be applied to a different skin site after removal of the previous transdermal patch. 3. Patients should be advised that fentanyl transdermal system should be applied to intact, nonirritated, and
nonirradiated skin on a flat surface such as the chest, back, flank, or upper arm. Additionally, patients shouldbe advised of the following:
• In young children or persons with cognitive impairment, the patch should be put on the upper back to lowerthe chances that the patch will be removed and placed in the mouth.
• Hair at the application site should be clipped (not shaved) prior to patch application.• If the site of fentanyl transdermal system application must be cleansed prior to application of the patch,
do so with clear water.• Do not use soaps, oils, lotions, alcohol, or any other agents that might irritate the skin or alter its
characteristics.• Allow the skin to dry completely prior to patch application.
4. Patients should be advised that fentanyl transdermal system should be applied immediately upon removal from thesealed package and after removal of the protective liner. Additionally the patient should be advised of the following:
• The fentanyl transdermal system should not be used if the seal is broken or the patch is cut, damaged, orchanged in any way.
• The transdermal patch should be pressed firmly in place with the palm of the hand for 30 seconds, making sure the contact is complete, especially around the edges.
• The patch should not be folded so that only part of the patch is exposed.5. Patients should be advised that the dose of fentanyl transdermal system or the number of patches applied to
the skin should NEVER be adjusted without the prescribing healthcare professional’s instruction.6. Patients should be advised that while wearing the patch, they should avoid exposing the fentanyl transdermal
system application site and surrounding area to direct external heat sources, such as:• heating pads,• electric blankets,• sunbathing,• heat or tanning lamps,• saunas,• hot tubs or hot baths, and• heated water beds, etc.
7. Patients should also be advised of a potential for temperature-dependent increases in fentanyl release from thepatch that could result in an overdose of fentanyl; therefore, patients who develop a high fever or increased bodytemperature due to strenuous exertion while wearing the patch should contact their physician.
8. Patients should be advised that if they experience problems with adhesion of the fentanyl transdermal system,they may tape the edges of the patch with first aid tape. If problems with adhesion persist, patients may overlay the patch with a transparent adhesive film dressing (e.g., Bioclusive® or Askina®Derm).
9. Patients should be advised that if the patch falls off before 72 hours a new patch may be applied to a different skin site.
10. Patients should be advised to fold (so that the adhesive side adheres to itself) and immediately flush downthe toilet used fentanyl transdermal systems after removal from the skin.
11. Patients should be advised that fentanyl transdermal system may impair mental and/or physical abilityrequired for the performance of potentially hazardous tasks (e.g., driving, operating machinery).
12. Patients should be advised to refrain from any potentially dangerous activity when starting on fentanyl transdermal system or when their dose is being adjusted, until it is established that they have not beenadversely affected.
13. Patients should be advised that fentanyl transdermal system should not be combined with alcohol or other CNSdepressants (e.g., sleep medications, tranquilizers) because dangerous additive effects may occur, resultingin serious injury or death.
14. Patients should be advised to consult their physician or pharmacist if other medications are being or will beused with fentanyl transdermal system.
15. Patients should be advised of the potential for severe constipation.16. Patients should be advised that if they have been receiving treatment with fentanyl transdermal system and
cessation of therapy is indicated, it may be appropriate to taper the fentanyl transdermal system dose, ratherthan abruptly discontinue it, due to the risk of precipitating withdrawal symptoms.
17. Patients should be advised that fentanyl transdermal system contains fentanyl, a drug with high potential for abuse.
18. Patients, family members and caregivers should be advised to protect fentanyl transdermal system from theftor misuse in the work or home environment.
19. Patients should be instructed to keep fentanyl transdermal system in a secure place out of the reach of children due to the high risk of fatal respiratory depression.
20. Patients should be advised that fentanyl transdermal system should never be given to anyone other than theindividual for whom it was prescribed because of the risk of death or other serious medical problems to thatperson for whom it was not intended.
21. Patients should be informed that, if the patch dislodges and accidentally sticks to the skin of another person,they should immediately take the patch off, wash the exposed area with water and seek medical attention forthe accidentally exposed individual.
22. When fentanyl transdermal system is no longer needed, the unused patches should be removed from theirpouches, folded so that the adhesive side of the patch adheres to itself, and flushed down the toilet.
23. Women of childbearing potential who become, or are planning to become pregnant, should be advised to
consult a physician prior to initiating or continuing therapy with fentanyl transdermal system.24. Patients should be informed that accidental exposure or misuse may lead to death or other serious medical
problems. Drug Interactions: Agents Affecting Cytochrome P450 3A4 Isoenzyme System: Fentanyl is metabolized mainly via the human cytochrome P450 3A4 isoenzyme system (CYP3A4), therefore potential interactions may occur whenfentanyl transdermal system is given concurrently with agents that affect CYP3A4 activity. Coadministration withagents that induce CYP3A4 activity may reduce the efficacy of fentanyl transdermal system. The concomitant use of transdermal fentanyl with all CYP3A4 inhibitors (such as ritonavir, ketoconazole, itraconazole, troleandomycin, clarithromycin, nelfanivir, nefazadone, amiodarone, amprenavir, aprepitant, diltiazem, erythromycin, fluconazole,fasamprenavir, grapefruit juice, and verapamil) may result in an increase in fentanyl plasma concentrations, whichcould increase or prolong adverse drug effects and may cause fatal respiratory depression. Patients receiving fentanyl transdermal system and any CYP3A4 inhibitor should be carefully monitored for an extended period of time,and dosage adjustments should be made if warranted (see BOX WARNING, CLINICAL PHARMACOLOGY: DrugInteractions in full prescribing information, WARNINGS, and DOSAGE AND ADMINISTRATION in full prescribing information for further information).Central Nervous System Depressants: The concomitant use of fentanyl transdermal system with other central nervous system depressants, including but not limited to other opioids, sedatives, hypnotics, tranquilizers (e.g., benzodiazepines), general anesthetics, phenothiazines, skeletal muscle relaxants, and alcohol, may cause respiratorydepression, hypotension, and profound sedation, or potentially result in coma or death. When such combined therapyis contemplated, the dose of one or both agents should be significantly reduced. MAO Inhibitors: Fentanyl transdermal system is not recommended for use in patients who have received MAOI within14 days because severe and unpredictable potentiation by MAO inhibitors has been reported with opioid analgesics.Carcinogenesis, Mutagenesis, and Impairment of Fertility: Studies in animals to evaluate the carcinogenic potential of fentanyl HCl have not been conducted. There was no evidence of mutagenicity in the Ames Salmonellamutagenicity assay, the primary rat hepatocyte unscheduled DNA synthesis assay, the BALB/c 3T3 transformationtest, and the human lymphocyte and CHO chromosomal aberration in vitro assays.
The potential effects of fentanyl on male and female fertility were examined in the rat model via two separateexperiments. In the male fertility study, male rats were treated with fentanyl (0, 0.025, 0.1 or 0.4 mg/kg/day) via continuous intravenous infusion for 28 days prior to mating; female rats were not treated. In the female fertility study,female rats were treated with fentanyl (0, 0.025, 0.1 or 0.4 mg/kg/day) via continuous intravenous infusion for 14 days prior to mating until day 16 of pregnancy; male rats were not treated. Analysis of fertility parameters in bothstudies indicated that an intravenous dose of fentanyl up to 0.4 mg/kg/day to either the male or the female alone produced no effects on fertility (this dose is approximately 1.6 times the daily human dose administered by a 100 mcg/hrpatch on a mg/m2 basis). In a separate study, a single daily bolus dose of fentanyl was shown to impair fertility inrats when given in intravenous doses of 0.3 times the human dose for a period of 12 days.Pregnancy: Teratogenic Effects: Pregnancy Category C: No epidemiological studies of congenital anomalies ininfants born to women treated with fentanyl during pregnancy have been reported.
The potential effects of fentanyl on embryo-fetal development were studied in the rat, mouse, and rabbit models.Published literature reports that administration of fentanyl (0, 10, 100, or 500 mcg/kg/day) to pregnant femaleSprague-Dawley rats from day 7 to 21 via implanted microosmotic minipumps did not produce any evidence of teratogenicity (the high dose is approximately 2 times the daily human dose administered by a 100 mcg/hr patch ona mg/m2 basis). In contrast, the intravenous administration of fentanyl (0, 0.01, or 0.03 mg/kg) to bred female ratsfrom gestation day 6 to 18 suggested evidence of embryotoxicity and a slight increase in mean delivery time in the0.03 mg/kg/day group. There was no clear evidence of teratogenicity noted.
Pregnant female New Zealand White rabbits were treated with fentanyl (0, 0.025, 0.1, 0.4 mg/kg) via intravenousinfusion from day 6 to day 18 of pregnancy. Fentanyl produced a slight decrease in the body weight of the live fetusesat the high dose, which may be attributed to maternal toxicity. Under the conditions of the assay, there was no evidence for fentanyl induced adverse effects on embryo-fetal development at doses up to 0.4 mg/kg (approximately 3 times the daily human dose administered by a 100 mcg/hr patch on a mg/m2 basis).
There are no adequate and well controlled studies in pregnant women. Fentanyl transdermal system should beused during pregnancy only if the potential benefit justifies the potential risk to the fetus.Nonteratogenic Effects: Chronic maternal treatment with fentanyl during pregnancy has been associated with transient respiratory depression, behavioral changes, or seizures characteristic of neonatal abstinence syndrome innewborn infants. Symptoms of neonatal respiratory or neurological depression were no more frequent than expectedin most studies of infants born to women treated acutely during labor with intravenous or epidural fentanyl. Transientneonatal muscular rigidity has been observed in infants whose mothers were treated with intravenous fentanyl.
The potential effects of fentanyl on prenatal and postnatal development were examined in the rat model. FemaleWistar rats were treated with 0, 0.025, 0.1, or 0.4 mg/kg/day fentanyl via intravenous infusion from day 6 of pregnancy through 3 weeks of lactation. Fentanyl treatment (0.4 mg/kg/day) significantly decreased body weight in maleand female pups and also decreased survival in pups at day 4. Both the mid-dose and high-dose of fentanyl animalsdemonstrated alterations in some physical landmarks of development (delayed incisor eruption and eye opening) andtransient behavioral development (decreased locomotor activity at day 28 which recovered by day 50). The mid-doseand the high-dose are 0.4 and 1.6 times the daily human dose administered by a 100 mcg/hr patch on a mg/m2 basis.Labor and Delivery: Fentanyl readily passes across the placenta to the fetus; therefore, fentanyl transdermal systemis not recommended for analgesia during labor and delivery. Nursing Mothers: Fentanyl is excreted in human milk; therefore, fentanyl transdermal system is not recommended foruse in nursing women because of the possibility of effects in their infants. Pediatric Use: The safety of fentanyl transdermal system was evaluated in three open-label trials in 291 pediatricpatients with chronic pain, 2 years of age through 18 years of age. Starting doses of 25 mcg/hr and higher were usedby 181 patients who had been on prior daily opioid doses of at least 45 mg/day of oral morphine or an equianalgesicdose of another opioid. Initiation of fentanyl transdermal system therapy in pediatric patients taking less than 60 mg/day of oral morphine or an equianalgesic dose of another opioid has not been evaluated in controlled clinicaltrials. Approximately 90% of the total daily opioid requirement (fentanyl transdermal system plus rescue medication)was provided by fentanyl transdermal system.
Fentanyl transdermal system was not studied in children under 2 years of age. Fentanyl transdermal system should be administered to children only if they are opioid-tolerant and 2 years of age
or older (see DOSAGE AND ADMINISTRATION in full prescribing information and BOX WARNING). To guard against accidental ingestion by children, use caution when choosing the application site for fentanyl
transdermal system (see DOSAGE AND ADMINISTRATION in full prescribing information) and monitor adhesion of thesystem closely.Geriatric Use: Information from a pilot study of the pharmacokinetics of IV fentanyl in geriatric patients (N = 4) indicates that the clearance of fentanyl may be greatly decreased in the population above the age of 60. The relevanceof these findings to fentanyl transdermal system is unknown at this time.
Respiratory depression is the chief hazard in elderly or debilitated patients, usually following large initial doses innontolerant patients, or when opioids are given in conjunction with other agents that depress respiration.
Fentanyl transdermal system should be used with caution in elderly, cachectic, or debilitated patients as they may have altered pharmacokinetics due to poor fat stores, muscle wasting or altered clearance (see DOSAGE ANDADMINISTRATION in full prescribing information). ADVERSE REACTIONS: In post-marketing experience, deaths from hypoventilation due to inappropriate use of fentanyl transdermal system have been reported (see BOX WARNING and CONTRAINDICATIONS). Premarketing Clinical Trial Experience: Although fentanyl transdermal system use in postoperative or acute painand in patients who are not opioid-tolerant is CONTRAINDICATED, the safety of fentanyl transdermal system was originally evaluated in 357 postoperative adult patients for 1 to 3 days and 153 cancer patients for a total of 510patients. The duration of fentanyl transdermal system use varied in cancer patients; 56% of patients used fentanyltransdermal system for over 30 days, 28% continued treatment for more than 4 months, and 10% used fentanyltransdermal system for more than 1 year.
Hypoventilation was the most serious adverse reaction observed in 13 (4%) postoperative patients and in 3 (2%) ofthe cancer patients. Hypotension and hypertension were observed in 11 (3%) and 4 (1%) of the opioid-naive patients.
Various adverse events were reported; a causal relationship to fentanyl transdermal system was not always determined. The frequencies presented here reflect the actual frequency of each adverse effect in patients whoreceived fentanyl transdermal system. There has been no attempt to correct for a placebo effect, concomitant use of
Page 2 of 3
Call for PapersU.S. Pharmacist is seeking authors to write clinical
articles and continuing education lessons on a variety of topics. While we will entertain all subject
matter, we are particularly interested in articles that correspond to our “Editorial Focus” therapeutic
areas. The therapeutic categories and the months for which they are planned are listed below:
Cardiovascular Diseases – FebruaryEndocrinology – June
Gastroenterologic Diseases – DecemberInfectious Diseases – August
Neurologic Diseases – JanuaryNew Drugs – OctoberOphthalmology – April
Pain Management – MayPediatric and Adolescent Health – March
Psychotropics – NovemberRespiratory Diseases – July
Women’s Health – September
In addition to these topics, we also publish supplements each year covering oncology
and hematology, diabetes, the generic drug industry, and OTC drugs.
In the majority of cases, articles are peer-reviewed and an honorarium is offered based on their
complexity and length. As a general guideline, we would like the articles to be approximately 2,500 words, including references and tables. Continuing education lessons should be approximately 6,000
words, including references, tables, and exam. Prospective authors are urged to review the “Author Guidelines” on the U.S. Pharmacist
Web site at www.uspharmacist.com.
Interested authors should contact Rob Davidson, Executive Editor ([email protected]),
with the topic(s) they would like to cover. All articles must be original and exclusive to U.S. Pharmacist.
other opioids, or to subtract the frequencies reported by placebo-treated patients in controlled trials. Adverse reactions reported in 153 cancer patients at a frequency of 1% or greater are presented in Table 1;
similar reactions were seen in the 357 postoperative patients. In the pediatric population, the safety of fentanyl transdermal system has been evaluated in 291 patients with
chronic pain 2 to 18 years of age. The duration of fentanyl transdermal system use varied; 20% of pediatric patientswere treated for 15 days; 46% for 16 to 30 days; 16% for 31 to 60 days; and 17% for at least 61 days. Twenty-fivepatients were treated with fentanyl transdermal system for at least 4 months and 9 patients for more than 9 months.
There was no apparent pediatric-specific risk associated with fentanyl transdermal system use in children as youngas 2 years old when used as directed. The most common adverse events were fever (35%), vomiting (33%), and nausea (24%).
Adverse events reported in pediatric patients at a rate of 1% are presented in Table 1.TABLE 1: ADVERSE EVENTS (at rate of ≥ 1%)
Adults (N = 380) and Pediatric (N = 291) Clinical Trial Experience
*Reactions occurring in 3% to 10% of fentanyl transdermal system patients**Reactions occurring in 10% or more of fentanyl transdermal system patients
The following adverse effects have been reported in less than 1% of the 510 adult postoperative and cancerpatients studied:Cardiovascular: bradycardiaDigestive: abdominal distentionNervous: aphasia, hypertonia, vertigo, stupor, hypotonia, depersonalization, hostilityRespiratory: stertorous breathing, asthma, respiratory disorderSkin and Appendages, General: exfoliative dermatitis, pustulesSpecial Senses: amblyopiaUrogenital: bladder pain, oliguria, urinary frequencyPost-Marketing Experience: Adults: The following adverse reactions have been reported in association with theuse of fentanyl transdermal system and not reported in the premarketing adverse reactions section above:Body as a Whole: edemaCardiovascular: tachycardiaMetabolic and Nutritional: weight lossSpecial Senses: blurred visionUrogenital: decreased libido, anorgasmia, ejaculatory difficulty
DRUG ABUSE AND ADDICTION: Fentanyl transdermal system contains a high concentration of fentanyl, a potentSchedule II opioid agonist. Schedule II opioid substances, which include hydromorphone, methadone, morphine, oxycodone, and oxymorphone, have the highest potential for abuse and risk of fatal overdose due to respiratory depres-sion. Fentanyl, like morphine and other opioids used in analgesia, can be abused and is subject to criminal diversion.
The high content of fentanyl in the patches (fentanyl transdermal system) may be a particular target for abuseand diversion.
Addiction is a primary, chronic, neurobiologic disease, with genetic, psychosocial, and environmental factorsinfluencing its development and manifestations. It is characterized by behaviors that include one or more of the following: impaired control over drug use, compulsive use, continued use despite harm, and craving. Drug addictionis a treatable disease, utilizing a multidisciplinary approach, but relapse is common.
“Drug seeking” behavior is very common in addicts and drug abusers. Drug-seeking tactics include emergencycalls or visits near the end of office hours, refusal to undergo appropriate examination, testing or referral, repeated“loss” of prescriptions, tampering with prescriptions and reluctance to provide prior medical records or contactinformation for other treating physician(s). “Doctor shopping” to obtain additional prescriptions is common amongdrug abusers and people suffering from untreated addiction.
Abuse and addiction are separate and distinct from physical dependence and tolerance. Physicians should beaware that addiction may be accompanied by concurrent tolerance and symptoms of physical dependence. In addition,abuse of opioids can occur in the absence of true addiction and is characterized by misuse for nonmedical purposes, often in combination with other psychoactive substances. Since fentanyl transdermal system may bediverted for nonmedical use, careful record keeping of prescribing information, including quantity, frequency, andrenewal requests is strongly advised.
Proper assessment of the patient, proper prescribing practices, periodic re-evaluation of therapy, and proper dispensing and storage are appropriate measures that help to limit abuse of opioid drugs.
Fentanyl transdermal systems are intended for transdermal use (to be applied on the skin) only. Do not use afentanyl transdermal system if the seal is broken or the patch is cut, damaged, or changed in any way. OVERDOSAGE: Clinical Presentation: The manifestations of fentanyl overdosage are an extension of its pharmacologic actions with the most serious significant effect being hypoventilation. Treatment: For the management of hypoventilation, immediate countermeasures include removing the fentanyltransdermal system and physically or verbally stimulating the patient. These actions can be followed by administration of a specific narcotic antagonist such as naloxone. The duration of hypoventilation following anoverdose may be longer than the effects of the narcotic antagonist’s action (the half-life of naloxone ranges from30 to 81 minutes). The interval between IV antagonist doses should be carefully chosen because of the possibilityof renarcotization after system removal; repeated administration of naloxone may be necessary. Reversal of the narcotic effect may result in acute onset of pain and the release of catecholamines.
Always ensure a patent airway is established and maintained, administer oxygen and assist or control respiration as indicated and use an oropharyngeal airway or endotracheal tube if necessary. Adequate body temperature and fluid intake should be maintained.
If severe or persistent hypotension occurs, the possibility of hypovolemia should be considered and managedwith appropriate parenteral fluid therapy.
MYLAN®
Mylan Pharmaceuticals Inc.Morgantown, WV 26505
REVISED JUNE 2008 BS:FTS:R16
Body System Adults PediatricsBody as a Whole Abdominal pain*, headache*, fatigue*, Pain*, headache*, fever,
back pain, fever, influenza-like symptoms*, syncope, abdominal pain,accidental injury, rigors allergic reaction, flushing
Cardiovascular Arrhythmia, chest pain Hypertension, tachycardiaDigestive Nausea**, vomiting**, constipation**, Nausea**, vomiting**,
dry mouth**, anorexia*, diarrhea*, constipation*, dry mouth,dyspepsia*, flatulence diarrhea
Nervous Somnolence**, insomnia, confusion**, Somnolence*, nervousness*,asthenia**, dizziness*, nervousness*, insomnia*, asthenia*,hallucinations*, anxiety*, depression*, euphoria*, hallucinations, anxiety,tremor, abnormal coordination, speech disorder, depression, convulsions,abnormal thinking, abnormal gait, dizziness, tremor, speechabnormal dreams, agitation, paresthesia, disorder, agitation, stupor,amnesia, syncope, paranoid reaction confusion, paranoid reaction
Respiratory Dyspnea*, hypoventilation*, apnea*, Dyspnea, respiratoryhemoptysis, pharyngitis*, hiccups, depression, rhinitis, coughingbronchitis, rhinitis, sinusitis,upper respiratory tract infection*
Skin and Appendages Sweating**, pruritus*, rash, application site Pruritus*, application sitereaction – erythema, papules, reaction*, sweating increased,itching, edema rash, rash erythematous, skin
reaction localizedUrogenital Urinary retention*, micturition disorder Urinary retention
Page 3 of 3
HS14 CallforPapVert 2_24sc.indd HS-14HS14 CallforPapVert 2_24sc.indd HS-14 3/2/10 9:55 AM3/2/10 9:55 AM

HS-15U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC HYPERTENSION
used intravenously for treatment of severe hypertension.16
Outside of hypertension associated with renal disease, data are extremely limited regarding the use of ARBs for the treatment of pediatric hypertension. Since the publication of recent guidelines, two studies have been published that examined the use of valsartan and can-desartan.17,18 In an open-label, uncontrolled trial, can-desartan 8 mg was shown to effectively lower BP in 11 children aged 6 to 18 years.17 A study of 90 patients aged 1 year to 5 years found valsartan 20 mg, 40 mg, and 80 mg to be effective. This study also evaluated valsartan’s effects on growth and development. No significant changes between valsartan and placebo were seen for length per height for age or BMI throughout the study. Developmental skills such as language and motor ability and social development all progressed normally.18
Beta-blockers are used less often owing to complica-tions with disease states such as diabetes and asthma and the development of lipid abnormalities after long-term use.11,12 Consideration should be given to BBs in the presence of severe hypertension or when combina-tion therapy is needed. Additionally, the use of diuret-ics is often reserved for patients with renal disease or when combination therapy is needed.14
TABLE 4 describes commonly used medications for the treatment of pediatric hypertension, along with dose recommendations and side effects.11,15,16
MonitoringWhen treatment for hypertension is initiated, a 6-month trial of nonpharmacologic interventions should be attempted. If BP goals are not met after this time, pharmacologic therapy should be started. The patient should be seen every 2 weeks and medications adjusted until the goal BP is achieved. Once the patient has
sustained a normal BP for 6 months, the physician may elect to begin discontinuing pharmacotherapy. If phar-macotherapy is discontinued entirely, the patient should be seen again in 6 months; if normal BP is maintained, yearly visits are appropriate.13 As the long-term effects of antihypertensive therapy, both beneficial and detri-mental, are currently not known, discontinuation of therapy may be warranted in patients who have suc-cessfully incorporated lifestyle modifications into their treatment regimen.11
ConclusionThe prevalence of hypertension among children has increased in response to the increased prevalence of childhood obesity. Despite this increase, secondary causes remain the most common reason for hyperten-sion in this patient population. Monitoring of BP using appropriate techniques should begin when the child reaches the age of 3 years. Percentiles are used to determine whether a child’s BP is appropriate and take into consideration gender, age, and height. Non-pharmacologic measures such as diet and exercise can be very successful, particularly for the obese child; however, pharmacotherapy will likely be needed in patients with secondary causes of hypertension. ACE inhibitors and CCBs are commonly prescribed, owing to a better adverse-effect profile. Additional agents such as ARBs, BBs, and diuretics may be included as part of a multidrug regimen.
Pharmacists can play a key role in the treatment of children with hypertension. Encouraging lifestyle modifications, ensuring that the pharmacotherapy plan is appropriate, providing adequate counseling, and assisting in the monitoring of the patient’s BP are a few examples of how the pharmacist can assist in the treatment of pediatric hypertension.
HEA
LTH S
YS
TEMS
EDITIO
N
REFERENCES1. Ogden CL, Troiano RP, Briefel RR, et al. Prevalence of overweight among pre-school children in the United States, 1971 through 1994. Pediatrics. 1997;99:E1.2. Reich A, Müller G, Gelbrich G, et al. Obesity and blood pressure—results from the examination of 2365 schoolchildren in Germany. Int J Obes Relat Metab Disord. 2003;27:1459-1464.3. Schiel R, Beltschikow W, Kramer G, Stein G. Overweight, obesity and elevated blood pressure in children and adolescents. Eur J Med Res. 2006;11:97-101.4. Ogden CL, Carroll MD, Curtin LR, et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA. 2006;295:1549-1555.5. Bibbins-Domingo K, Coxson P, Pletcher MJ, et al. Adolescent overweight and future adult coronary heart disease. N Engl J Med. 2007;357:2371-2379.6. Daniels SR, Arnett DK, Eckel RH, et al. Overweight in children and adoles-cents: pathophysiology, consequences, prevention, and treatment. Circulation. 2005;111:1999-2012.7. Sorof JM, Turner J, Martin DS, et al. Cardiovascular risk factors and sequelae in hypertensive children identified by referral versus school-based screening. Hyperten-sion. 2004;43:214-218.8. Adrogué HE, Sinaiko AR. Prevalence of hypertension in junior high school-aged children: effect of new recommendations in the 1996 Updated Task Force Report. Am J Hypertens. 2001;14:412-414.9. Sinaiko AR. Hypertension in children. N Engl J Med. 1996;335:1968-1973.10. Sorof J, Daniels S. Obesity hypertension in children: a problem of epidemic
proportions. Hypertension. 2002;40:441-447.11. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The Fourth Report on the Diagnosis, Evaluation, and Treatment of Children and Adolescents. Pediatrics. 2004;114(suppl 2):555-576.12. Bernstein D. Systemic hypertension. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, PA: Saun-ders Elsevier; 2007:1988-1995.13. Mitsnefes MM, McEnery PT. Hypertension. In: Osborn LM, DeWitt TG, First LR, Zenel JA, eds. Pediatrics. Philadelphia, PA: Elsevier Mosby; 2005:1151-1156.14. Robinson RF, Nahata MC, Batisky DL, Mahan JD. Pharmacologic treatment of chronic pediatric hypertension. Paediatr Drugs. 2005;7:27-40.15. Li JS, Baker-Smith CM, Smith PB, et al. Racial differences in blood pressure response to angiotensin-converting enzyme inhibitors in children: a meta-analysis. Clin Pharmacol Ther. 2008;84:315-319.16. Sahney S. A review of calcium channel antagonists in the treatment of pediatric hypertension. Paediatr Drugs. 2006;8:357-373.17. Franks AM, O’Brien CE, Stowe CD, et al. Candesartan cilexetil effectively reduces blood pressure in hypertensive children. Ann Pharmacother. 2008;42:1388-1395.18. Flynn JT, Meyers KE, Neto JP, et al. Efficacy and safety of the angiotensin receptor blocker valsartan in children with hypertension aged 1 to 5 years. Hyperten-sion. 2008;52:222-228.
HS08 PedHyperten 3_1mb.indd HS-15HS08 PedHyperten 3_1mb.indd HS-15 3/2/10 10:06 AM3/2/10 10:06 AM
HS-16U.S. Pharmacist • March 2010 • www.uspharmacist.com
The pharmacist is a crucial member of the health care team and is often the last line of defense in catching excessive or incorrect drug dosing
for patients. Chronic kidney disease (CKD) affects many people in the United States, and more than 500,000 Americans have end-stage renal disease (ESRD) requiring dialysis.1,2 The most common risk factors for developing CKD are diabetes and hypertension. Patients with CKD are at increased risk for cardiovas-cular disease and complications. This brief review will focus on risk factors, assessing renal function, and dosage adjustments.
Risk Factors for Acute Kidney InjuryDrugs are a frequent cause of acute kidney injury (AKI). It is estimated that nearly 50% of all medicines are not used appropriately.3 Many drug clearances are affected by kidney function, and especially in the elderly popu-lation, drugs need to be adjusted due to reduced kidney function as part of the aging process. Drug-induced kidney injury can be as high as 70% in elderly patients.4 Patients increas-ingly take more medications and have more comorbid conditions today than ever before. They are also getting older and receiving more diagnostic and therapeutic procedures that could potentially harm their kidneys.5
Medications that cause kidney injury tend to be more common in certain patient groups and certain specific clinical scenarios. For example, if a patient is dehydrated, avoid using a nonsteroidal anti-inflam-matory drug (NSAID) or a nephrotoxic drug that can lead to development of an AKI. It is important to recognize mechanisms of kidney injury and medication-related and patient-related risk factors. For instance, gentamicin can cause acute tubular necrosis if used concomitantly with furosemide for patients in the intensive care unit (ICU). Both of these drugs can increase the chance of acute kidney injury occurring in ICU patients who already have multiple comorbid conditions. Prevention and constant assessment are important, while targeting early treatment is essential to saving kidneys from further damage. When review-ing and assessing drug therapies, pharmacists should familiarize themselves with important risk factors that could potentially harm the kidneys (TABLE 1).6-10
Patients with poor kidney function are at an increased risk of developing kidney injury from nephrotoxic medications. Pharmacists should recognize that the threat of kidney injury increases if the patient has multiple risk fac-tors. For instance, if a patient has a glomerular filtration rate (GFR) of less than 60 mL/min/1.73 m2
Timothy V. Nguyen, PharmD, CCP, FASCPAssistant Professor of Pharmacy Practice
Arnold & Marie Schwartz College of Pharmacy & Health Sciences
Long Island UniversityBrooklyn, New York
Clinical Pharmacy Specialist, Nephrology & Dialysis, The Mount Sinai Medical Center
New York, New York
HEA
LTH S
YS
TEMS
EDITIO
N
Practical Assessment Tools for Identifying
Kidney Disease
© MEDICALRF / PHOTO RESEARCHERS, INC
HS16 Kidney 3_1bo.indd HS-16HS16 Kidney 3_1bo.indd HS-16 3/2/10 9:57 AM3/2/10 9:57 AM
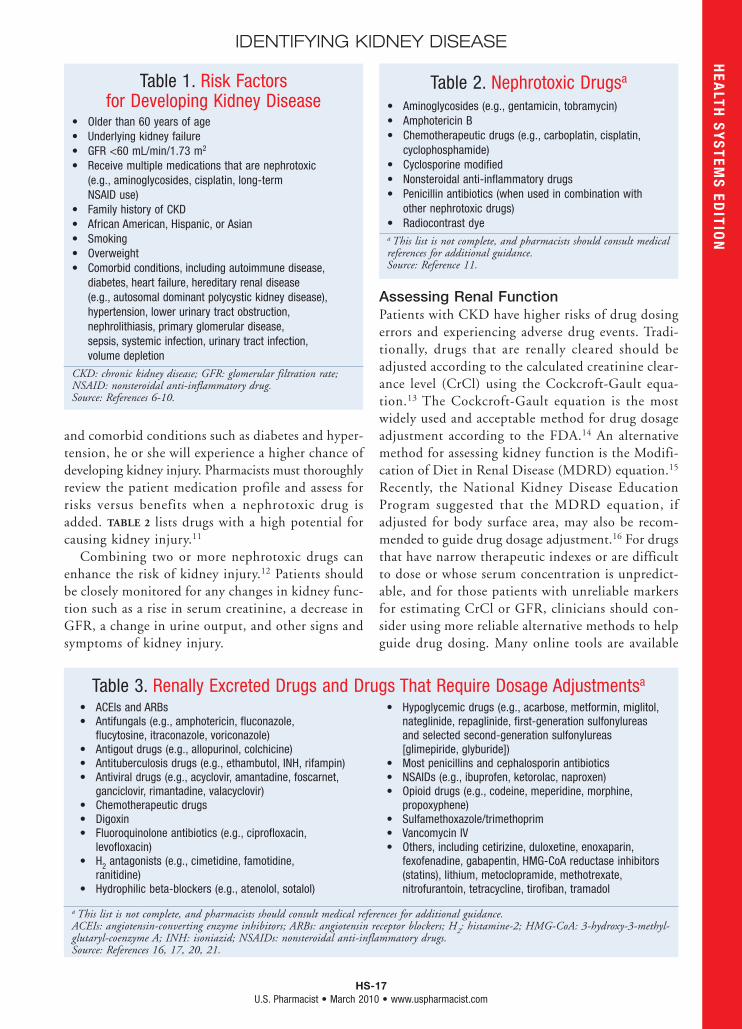
HS-17U.S. Pharmacist • March 2010 • www.uspharmacist.com
IDENTIFYING KIDNEY DISEASEH
EALTH
SY
STEM
S ED
ITION
and comorbid conditions such as diabetes and hyper-tension, he or she will experience a higher chance of developing kidney injury. Pharmacists must thoroughly review the patient medication profile and assess for risks versus benefits when a nephrotoxic drug is added. TABLE 2 lists drugs with a high potential for causing kidney injury.11
Combining two or more nephrotoxic drugs can enhance the risk of kidney injury.12 Patients should be closely monitored for any changes in kidney func-tion such as a rise in serum creatinine, a decrease in GFR, a change in urine output, and other signs and symptoms of kidney injury.
Assessing Renal FunctionPatients with CKD have higher risks of drug dosing errors and experiencing adverse drug events. Tradi-tionally, drugs that are renally cleared should be adjusted according to the calculated creatinine clear-ance level (CrCl) using the Cockcroft-Gault equa-tion.13 The Cockcroft-Gault equation is the most widely used and acceptable method for drug dosage adjustment according to the FDA.14 An alternative method for assessing kidney function is the Modifi-cation of Diet in Renal Disease (MDRD) equation.15 Recently, the National Kidney Disease Education Program suggested that the MDRD equation, if adjusted for body surface area, may also be recom-mended to guide drug dosage adjustment.16 For drugs that have narrow therapeutic indexes or are difficult to dose or whose serum concentration is unpredict-able, and for those patients with unreliable markers for estimating CrCl or GFR, clinicians should con-sider using more reliable alternative methods to help guide drug dosing. Many online tools are available
Table 1. Risk Factors for Developing Kidney Disease
• Older than 60 years of age• Underlying kidney failure• GFR <60 mL/min/1.73 m2
• Receive multiple medications that are nephrotoxic (e.g., aminoglycosides, cisplatin, long-term NSAID use)
• Family history of CKD• African American, Hispanic, or Asian• Smoking• Overweight• Comorbid conditions, including autoimmune disease,
diabetes, heart failure, hereditary renal disease (e.g., autosomal dominant polycystic kidney disease), hypertension, lower urinary tract obstruction, nephrolithiasis, primary glomerular disease, sepsis, systemic infection, urinary tract infection, volume depletion
CKD: chronic kidney disease; GFR: glomerular filtration rate; NSAID: nonsteroidal anti-inflammatory drug.Source: References 6-10.
Table 2. Nephrotoxic Drugsa
• Aminoglycosides (e.g., gentamicin, tobramycin)• Amphotericin B• Chemotherapeutic drugs (e.g., carboplatin, cisplatin,
cyclophosphamide)• Cyclosporine modified• Nonsteroidal anti-inflammatory drugs• Penicillin antibiotics (when used in combination with
other nephrotoxic drugs)• Radiocontrast dyea This list is not complete, and pharmacists should consult medical references for additional guidance.Source: Reference 11.
• ACEIs and ARBs• Antifungals (e.g., amphotericin, fluconazole,
flucytosine, itraconazole, voriconazole)• Antigout drugs (e.g., allopurinol, colchicine)• Antituberculosis drugs (e.g., ethambutol, INH, rifampin)• Antiviral drugs (e.g., acyclovir, amantadine, foscarnet,
ganciclovir, rimantadine, valacyclovir)• Chemotherapeutic drugs• Digoxin• Fluoroquinolone antibiotics (e.g., ciprofloxacin,
levofloxacin)• H2 antagonists (e.g., cimetidine, famotidine,
ranitidine)• Hydrophilic beta-blockers (e.g., atenolol, sotalol)
• Hypoglycemic drugs (e.g., acarbose, metformin, miglitol, nateglinide, repaglinide, first-generation sulfonylureas and selected second-generation sulfonylureas [glimepiride, glyburide])
• Most penicillins and cephalosporin antibiotics• NSAIDs (e.g., ibuprofen, ketorolac, naproxen)• Opioid drugs (e.g., codeine, meperidine, morphine,
propoxyphene)• Sulfamethoxazole/trimethoprim• Vancomycin IV• Others, including cetirizine, duloxetine, enoxaparin,
fexofenadine, gabapentin, HMG-CoA reductase inhibitors (statins), lithium, metoclopramide, methotrexate, nitrofurantoin, tetracycline, tirofiban, tramadol
a This list is not complete, and pharmacists should consult medical references for additional guidance.ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; H2: histamine-2; HMG-CoA: 3-hydroxy-3-methyl-glutaryl-coenzyme A; INH: isoniazid; NSAIDs: nonsteroidal anti-inflammatory drugs.Source: References 16, 17, 20, 21.
Table 3. Renally Excreted Drugs and Drugs That Require Dosage Adjustmentsa
HS16 Kidney 3_1bo.indd HS-17HS16 Kidney 3_1bo.indd HS-17 3/2/10 9:57 AM3/2/10 9:57 AM

41447_elilhg_HI59950-4_Asize_fa2.indd 2 12/16/09 12:31:58 PM
Same Name. New Size.
Introducing 3 mL of Humalog® and Humulin® R U-100 in a Smaller Vial*
The New Smaller Vial, Another Insulin Delivery Option Intended To: Give hospitals more fl exibility when evaluating insulin storage and distribution (fl oor stock vs individual patient supply), in addition to the 10 mL vial and Humalog® KwikPen™.
• Same Bar-Coding Technique, New Size
• Same Color-Differentiating System, New Size
• National Drug Code (NDC)
Humalog - NDC Number - 0002-7510-17Humulin R U-100 - NDC Number - 0002-8215-17
IndicationHumalog is for use in patients with diabetes mellitus for the control of hyperglycemia. Humalog should be used with longer-acting insulin, except when used in combination with sulfonylureas in patients with type 2 diabetes.
Select Safety Information Hypoglycemia is the most common adverse effect associated with insulins, including Humalog.
When used as a mealtime insulin, Humalog should be given within 15 minutes before or immediately after a meal.
*3 mL of Humalog and Humulin R U-100 are in a 5 mL vial.
Pens are for single-patient use only and should not be shared among patients.
Please see Important Safety Information on adjacent page and accompanying Brief Summary of full Prescribing Information.
41447_elilhg_HI59950-4_Asize_fa2.indd 1 12/16/09 12:31:55 PM
IndicationHumalog (insulin lispro injection [rDNA origin]) is for use in patients with diabetes mellitus for the control of hyperglycemia. Humalog should be used with longer-acting insulin, except when used in combination with sulfonylureas in patients with type 2 diabetes.
Important Safety InformationHumalog is contraindicated during episodes of hypoglycemia and in patients sensitive to Humalog or one of its excipients.
Humalog differs from regular human insulin by its rapid onset of action as well as a shorter duration of action. Therefore, when used as a mealtime insulin, Humalog should be given within 15 minutes before or immediatelyafter a meal.
Due to the short duration of action of Humalog, patients with type 1 diabetes also require a longer-acting insulin to maintain glucose control (except when using an insulin pump). Glucose monitoring is recommended for all patients with diabetes.
The safety and effectiveness of Humalog in patients less than 3 years of age have not been established. There areno adequate and well-controlled clinical studies of the use of Humalog in pregnant or nursing women.
Starting or changing insulin therapy should be done cautiously and only under medical supervision.
Hypoglycemia
Hypoglycemia is the most common adverse effect associated with insulins, including Humalog. Hypoglycemiacan happen suddenly, and symptoms may be different for each person and may change from time to time. Severe hypoglycemia can cause seizures and may be life-threatening.
Other Side Effects
Other potential side effects associated with the use of insulins include: hypokalemia, weight gain, lipodystrophy, and hypersensitivity. Systemic allergy is less common, but may be life-threatening. Because of the difference in action of Humalog, care should be taken in patients in whom hypoglycemia or hypokalemia may be clinically relevant (eg, those who are fasting, have autonomic neuropathy or renal impairment, are using potassium-lowering drugs, or taking drugs sensitive to serum potassium level).
For additional safety profi le and other important prescribing considerations, see accompanying Brief Summary of full Prescribing Information.
Please see full user manual that accompanies the pen.
Humalog® is a registered trademark of Eli Lilly and Company and is available by prescription only.Humalog® KwikPen™ is a trademark of Eli Lilly and Company and is available by prescription only. Humulin® is a registered trademark of Eli Lilly and Company.
HI59950-4 1109 PRINTED IN USA ©2009, LILLY USA, LLC. ALL RIGHTS RESERVED.
41447_elilhg_HI59950-4_Asize_fa2.indd 2 12/16/09 12:31:58 PM
HUMALOG® INSULIN LISPRO INJECTION (rDNA ORIGIN)BRIEF SUMMARY: Consult package insert for complete prescribing information.
INDICATIONS AND USAGE: Humalog is an insulin analog that is indicated in the treatment of patients with diabetes mellitus for the control of hyperglycemia. Humalog has a more rapid onset and a shorter duration of action than regular human insulin. Therefore, in patients with type 1 diabetes, Humalog should be used in regimens that include a longer-acting insulin. However, in patients with type 2 diabetes, Humalog may be used without a longer-acting insulin when used in combination therapy with sulfonylurea agents. Humalog may be used in an external insulin pump, but should not be diluted or mixed with any other insulin when used in the pump. Humalog administration in insulin pumps has not been studied in patients with type 2 diabetes.
CONTRAINDICATIONS: Humalog is contraindicated during episodes of hypoglycemia and in patients sensitive to Humalog or any of its excipients.
WARNINGS: This human insulin analog differs from regular human insulin by its rapid onset of action as well as a shorter duration of activity. When used as a mealtime insulin, the dose of Humalog should be given within 15 minutes before or immediately after the meal. Because of the short duration of action of Humalog, patients with type 1 diabetes also require a longer-acting insulin to maintain glucose control (except when using an external insulin pump). External Insulin Pumps: When used in an external insulin pump, Humalog should not be diluted or mixed with any other insulin. Patients should carefully read and follow the external insulin pump manufacturer’s instructions and the “PATIENT INFORMATION” leaflet before using Humalog. Physicians should carefully evaluate information on external insulin pump use in the Humalog physician package insert and in the external insulin pump manufacturer’s instructions. If unexplained hyperglycemia or ketosis occurs during external insulin pump use, prompt identification and correction of the cause is necessary. The patient may require interim therapy with subcutaneous insulin injections (see PRECAUTIONS, For Patients Using External Insulin Pumps, and DOSAGE AND ADMINISTRATION). Hypoglycemia is the most common adverse effect associated with the use of insulins, including Humalog. As with all insulins, the timing of hypoglycemia may differ among various insulin formulations. Glucose monitoring is recommended for all patients with diabetes and is particularly important for patients using an external insulin pump. Any change of insulin should be made cautiously and only under medical supervision. Changes in insulin strength, manufacturer, type (eg, regular, NPH, analog), species, or method of manufacture may result in the need for a change in dosage.
PRECAUTIONS: General—Hypoglycemia and hypokalemia are among the potential clinical adverse effects associated with the use of all insulins. Because of differences in the action of Humalog and other insulins, care should be taken in patients in whom such potential side effects might be clinically relevant (eg, patients who are fasting, have autonomic neuropathy, or are using potassium-lowering drugs or patients taking drugs sensitive to serum potassium level). Lipodystrophy and hypersensitivity are among other potential clinical adverse effects associated with the use of all insulins. As with all insulin preparations, the time course of Humalog action may vary in different individuals or at different times in the same individual and is dependent on site of injection, blood supply, temperature, and physical activity. Adjustment of dosage of any insulin may be necessary if patients change their physical activity or their usual meal plan. Insulin requirements may be altered during illness, emotional disturbances, or other stress. Hypoglycemia—As with all insulin preparations, hypoglycemic reactions may be associated with the administration of Humalog. Rapid changes in serum glucose concentrations may induce symptoms of hypoglycemia in persons with diabetes, regardless of the glucose value. Early warning symptoms of hypoglycemia may be different or less pronounced under certain conditions, such as long duration of diabetes, diabetic nerve disease, use of medications such as beta-blockers, or intensified diabetes control. Renal Impairment—The requirements for insulin may be reduced in patients with renal impairment. Hepatic Impairment—Although impaired hepatic function does not affect the absorption or disposition of Humalog, careful glucose monitoring and dose adjustments of insulin, including Humalog, may be necessary. Allergy—Local Allergy—As with any insulin therapy, patients may experience redness, swelling, or itching at the site of injection. These minor reactions usually resolve in a few days to a few weeks. In some instances, these reactions may be related to factors other than insulin, such as irritants in a skin cleansing agent or poor injection technique. Systemic Allergy—Less common, but potentially more serious, is generalized allergy to insulin, which may cause rash (including pruritus) over the whole body, shortness of breath, wheezing, reduction in blood pressure, rapid pulse, or sweating. Severe cases of generalized allergy, including anaphylactic reaction, may be life-threatening. Localized reactions and generalized myalgias have been reported with the use of cresol as an injectable excipient. In Humalog-controlled clinical trials, pruritus (with or without rash) was seen in 17 patients receiving Humulin R® (N=2969) and 30 patients receiving Humalog (N=2944) (P=.053). Antibody Production—In large clinical trials, antibodies that cross-react with human insulin and insulin lispro were observed in both Humulin R- and Humalog-treatment groups. As expected, the largest increase in the antibody levels during the 12-month clinical trials was observed with patients new to insulin therapy. Usage of Humalog in External Insulin Pumps—The infusion set (reservoir syringe, tubing, and catheter), Disetronic® D-TRON®2,3 or D-TRONplus®2,3 cartridge adapter, and Humalog in the external insulin pump reservoir should be replaced and a new infusion site selected every 48 hours or less. Humalog in the external insulin pump should not be exposed to temperatures above 37°C (98.6°F). In the D-TRON®2,3 or D-TRONplus®2,3 pump, Humalog 3 mL cartridges may be used for up to 7 days. However, as with other external insulin pumps, the infusion set should be replaced and a new infusion site should be selected every 48 hours or less. When used in an external insulin pump, Humalog should not be diluted or mixed with any other insulin (see INDICATIONS AND USAGE, WARNINGS, PRECAUTIONS, For Patients Using External Insulin Pumps, Mixing of Insulins, DOSAGE AND ADMINISTRATION, and Storage). Information for Patients—Patients should be informed of the potential risks and advantages of Humalog and alternative therapies. Patients should also be informed about the importance of proper insulin storage, injection technique, timing of dosage, adherence to meal planning, regular physical activity, regular blood glucose monitoring, periodic hemoglobin A1C testing, recognition and management of hypoglycemia and hyperglycemia, and periodic assessment for diabetes complications. Patients should be advised to inform their physician if they are pregnant or intend to become pregnant. Refer patients to the “PATIENT INFORMATION” leaflet for timing of Humalog dosing (<_15 minutes before or immediately after a meal), storing insulin, and common adverse effects. For Patients Using Insulin Pen Delivery Devices: Before starting therapy, patients should read the “PATIENT INFORMATION” leaflet that accompanies the drug product and the User Manual that accompanies the delivery device. They should also reread these materials each time the prescription is renewed. Patients should be instructed on how to properly use the delivery device, prime the Pen to a stream of insulin, and properly dispose of needles. Patients should be advised not to share their Pens with others. For Patients Using External Insulin Pumps: Patients using an external infusion pump should be trained in intensive insulin therapy and in the function of their external insulin pump and pump accessories. Humalog was tested in the MiniMed®1 Models 506, 507, and 508 insulin pumps using MiniMed®1 Polyfin®1 infusion sets. Humalog was also tested in the Disetronic®2 H-TRONplus® V100 insulin pump (with plastic 3.15 mL insulin reservoir), and the Disetronic D-TRON®2,3 and D-TRONplus®2,3 insulin pumps (with Humalog 3 mL cartridges) using Disetronic Rapid®2 infusion sets. The infusion set (reservoir syringe, tubing, catheter), D-TRON®2,3 or D-TRONplus®2,3 cartridge adapter, and Humalog in the external insulin pump reservoir should be replaced, and a new infusion site selected every 48 hours or less. Humalog in the external pump should not be exposed to temperatures above 37°C (98.6°F). A Humalog 3 mL cartridge used in the D-TRON®2,3 or D-TRONplus®2,3 pump should be discarded after 7 days, even if it still contains Humalog. Infusion sites that are erythematous, pruritic, or thickened should be reported to medical personnel, and a new site selected. Humalog should not be diluted or mixed with any other insulin when used in an external insulin pump. Laboratory Tests—As with all insulins, the therapeutic response to Humalog should be monitored by periodic blood glucose tests. Periodic measurement of hemoglobin A1C is recommended for the monitoring of long-term glycemic control. Drug Interactions—Insulin requirements may be increased by medications with hyperglycemic activity, such as corticosteroids, isoniazid, certain lipid-lowering drugs (eg, niacin), estrogens, oral contraceptives, phenothiazines, and thyroid replacement therapy (see CLINICAL PHARMACOLOGY). Insulin requirements may be decreased in the presence of drugs that increase insulin sensitivity or have hypoglycemic activity, such as oral antidiabetic agents, salicylates, sulfa antibiotics, certain antidepressants (monoamine oxidase inhibitors), angiotensin-converting-enzyme inhibitors, angiotensin II receptor blocking agents, beta-adrenergic blockers, inhibitors of pancreatic function (eg, octreotide), and alcohol. Beta-adrenergic blockers may mask the symptoms of hypoglycemia in some patients. Mixing of Insulins—Care should be taken when mixing all insulins as a change in peak action may occur. The American Diabetes Association warns in its Position Statement on Insulin Administration, “On mixing, physiochemical changes in the mixture may occur (either immediately or over time). As a result, the physiological response to the insulin mixture may differ from that of the injection of the insulins separately.” Mixing Humalog with Humulin® N or Humulin® U does not decrease the absorption rate or the total bioavailability of Humalog.
Given alone or mixed with Humulin N, Humalog results in a more rapid absorption and glucose-lowering effect compared with regular human insulin. Pregnancy—Teratogenic Effects—Pregnancy Category B—Reproduction studies with insulin lispro have been performed in pregnant rats and rabbits at parenteral doses up to 4 and 0.3 times, respectively, the average human dose (40 units/day) based on body surface area. The results have revealed no evidence of impaired fertility or harm to the fetus due to Humalog. There are, however, no adequate and well-controlled studies with Humalog in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed. Although there are limited clinical studies of the use of Humalog in pregnancy, published studies with human insulins suggest that optimizing overall glycemic control, including postprandial control, before conception and during pregnancy improves fetal outcome. Although the fetal complications of maternal hyperglycemia have been well documented, fetal toxicity also has been reported with maternal hypoglycemia. Insulin requirements usually fall during the first trimester and increase during the second and third trimesters. Careful monitoring of the patient is required throughout pregnancy. During the perinatal period, careful monitoring of infants born to mothers with diabetes is warranted. Nursing Mothers—It is unknown whether Humalog is excreted in significant amounts in human milk. Many drugs, including human insulin, are excreted in human milk. For this reason, caution should be exercised when Humalog is administered to a nursing woman. Patients with diabetes who are lactating may require adjustments in Humalog dose, meal plan, or both. Pediatric Use—In a 9-month, crossover study of prepubescent children (n=60), aged 3 to 11 years, comparable glycemic control as measured by A1C was achieved regardless of treatment group: regular human insulin 30 minutes before meals 8.4%, Humalog immediately before meals 8.4%, and Humalog immediately after meals 8.5%. In an 8-month, crossover study of adolescents (n=463), aged 9 to 19 years, comparable glycemic control as measured by A1C was achieved regardless of treatment group: regular human insulin 30 to 45 minutes before meals 8.7% and Humalog immediately before meals 8.7%. The incidence of hypoglycemia was similar for all 3 treatment regimens. Adjustment of basal insulin may be required. To improve accuracy in dosing in pediatric patients, a diluent may be used. If the diluent is added directly to the Humalog vial, the shelf life may be reduced (see DOSAGE AND ADMINISTRATION). Geriatric Use—Of the total number of subjects (n=2834) in 8 clinical studies of Humalog, 12% (n=338) were 65 years of age or over. The majority of these were patients with type 2 diabetes. A1C values and hypoglycemia rates did not differ by age. Pharmacokinetic/pharmacodynamic studies to assess the effect of age on the onset of Humalog action have not been performed.
ADVERSE REACTIONS: Clinical studies comparing Humalog with regular human insulin did not demonstrate a difference in frequency of adverse events between the 2 treatments. Adverse events commonly associated with human insulin therapy include the following: Body as a Whole—allergic reactions (see PRECAUTIONS). Skin and Appendages—injection site reaction, lipodystrophy, pruritus, rash. Other—hypoglycemia (see WARNINGS and PRECAUTIONS).
OVERDOSAGE: Hypoglycemia may occur as a result of an excess of insulin relative to food intake, energy expenditure, or both. Mild episodes of hypoglycemia usually can be treated with oral glucose. Adjustments in drug dosage, meal patterns, or exercise may be needed. More severe episodes with coma, seizure, or neurologic impairment may be treated with intramuscular/subcutaneous glucagon or concentrated intravenous glucose. Sustained carbohydrate intake and observation may be necessary because hypoglycemia may recur after apparent clinical recovery.
DOSAGE AND ADMINISTRATION: Humalog is intended for subcutaneous administration, including use in select external insulin pumps (see DOSAGE AND ADMINISTRATION, External Insulin Pumps). Dosage regimens of Humalog will vary among patients and should be determined by the healthcare provider familiar with the patient’s metabolic needs, eating habits, and other lifestyle variables. Pharmacokinetic and pharmacodynamic studies showed Humalog to be equipotent to regular human insulin (ie, one unit of Humalog has the same glucose-lowering effect as one unit of regular human insulin), but with more rapid activity. The quicker glucose-lowering effect of Humalog is related to the more rapid absorption rate from subcutaneous tissue. An adjustment of dose or schedule of basal insulin may be needed when a patient changes from other insulins to Humalog, particularly to prevent premeal hyperglycemia. When used as a mealtime insulin, Humalog should be given within 15 minutes before or immediately after a meal. Regular human insulin is best given 30 to 60 minutes before a meal. To achieve optimal glucose control, the amount of longer-acting insulin being given may need to be adjusted when using Humalog. The rate of insulin absorption and consequently the onset of activity are known to be affected by the site of injection, exercise, and other variables. Humalog was absorbed at a consistently faster rate than regular human insulin in healthy male volunteers given 0.2 U/kg regular human insulin or Humalog at abdominal, deltoid, or femoral sites, the 3 sites often used by patients with diabetes. When not mixed in the same syringe with other insulins, Humalog maintains its rapid onset of action and has less variability in its onset of action among injection sites compared with regular human insulin (see PRECAUTIONS). After abdominal administration, Humalog concentrations are higher than those following deltoid or thigh injections. Also, the duration of action of Humalog is slightly shorter following abdominal injection, compared with deltoid and femoral injections. As with all insulin preparations, the time course of action of Humalog may vary considerably in different individuals or within the same individual. Patients must be educated to use proper injection techniques. Humalog in a vial may be diluted with STERILE DILUENT for Humalog, Humulin N, Humulin R, Humulin 70/30, and Humulin® R U-500 to a concentration of 1:10 (equivalent to U-10) or 1:2 (equivalent to U-50). Diluted Humalog may remain in patient use for 28 days when stored at 5°C (41°F) and for 14 days when stored at 30°C (86°F). Do not dilute Humalog contained in a cartridge or Humalog used in an external insulin pump. Parenteral drug products should be inspected visually before use whenever the solution and the container permit. If the solution is cloudy, contains particulate matter, is thickened, or is discolored, the contents must not be injected. Humalog should not be used after its expiration date. The cartridge containing Humalog is not designed to allow any other insulin to be mixed in the cartridge or for the cartridge to be refilled with insulin. External Insulin Pumps—Humalog was tested in MiniMed®1 Models 506, 507, and 508 insulin pumps using MiniMed®1 Polyfin®1 infusion sets. Humalog was also tested in the Disetronic®2 H-TRONplus® V100 insulin pump (with plastic 3.15 mL insulin reservoir) and the Disetronic D-TRON®2,3 and D-TRONplus®2,3 pumps (with Humalog 3 mL cartridges) using Disetronic Rapid®2 infusion sets. Humalog should not be diluted or mixed with any other insulin when used in an external insulin pump.
HOW SUPPLIED: Humalog (insulin lispro injection, USP [rDNA origin]) is available in the following package sizes (with each presentation containing 100 units insulin lispro per mL [U-100]): 10 mL vials NDC 0002-7510-01 (VL-7510) 3 mL vials NDC 0002-7510-17 (VL-7533) 5 x 3 mL cartridges3 NDC 0002-7516-59 (VL-7516) 5 x 3 mL prefilled insulin delivery devices (Pen) NDC 0002-8725-59 (HP-8725) 5 x 3 mL prefilled insulin delivery devices (Humalog® KwikPen™) NDC 0002-8799-59 (HP-8799)
1 MiniMed® and Polyfin® are registered trademarks of MiniMed, Inc.2 Disetronic®, H-TRONplus®, D-TRON®, and Rapid® are registered trademarks of Roche Diagnostics GMBH. 3 3 mL cartridge is for use in Eli Lilly and Company’s HumaPen® MEMOIR™ and HumaPen® LUXURA™ HD insulin
delivery devices, Owen Mumford, Ltd.’s Autopen® 3 mL insulin delivery device, and Disetronic D-TRON® and D-TRONplus® pumps. Autopen® is a registered trademark of Owen Mumford, Ltd. HumaPen®, HumaPen® MEMOIR™ and HumaPen® LUXURA™ HD are trademarks of Eli Lilly and Company. Other product and company names may be the trademarks of their respective owners.
Storage —Unopened Humalog should be stored in a refrigerator (2° to 8°C [36° to 46°F]), but not in the freezer. Do not use Humalog if it has been frozen. Unrefrigerated (below 30°C [86°F]) 12 vials, cartridges, Pens, and KwikPens must be used within 28 days or be discarded, even if they still contain Humalog. Protect from direct heat and light. Use in an External Insulin Pump—A Humalog 3mL cartridge used in the D-TRON®2,3 or D-TRONplus®2,3 should be discarded after 7 days, even if it still contains Humalog. Infusion sets, D-TRON®2,3 and D-TRONplus®2,3 cartridge adapters, and Humalog in the external insulin pump reservoir should be discarded every 48 hours or less.
Literature revised December 7, 2009
KwikPens manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA. Pens manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA or Lilly France, F-67640 Fegersheim, France. Vials manufactured by Eli Lilly and Company, Indianapolis, IN 46285, USA or Hospira, Inc., Lake Forest, IL 60045, USA or Lilly France, F-67640 Fegersheim, France. Cartridges manufactured by Lilly France, F-67640 Fegersheim, France for Eli Lilly and Company, Indianapolis, IN 46285, USA. www.humalog.com
Copyright © 1996, 2008, Eli Lilly and Company. All rights reserved.
41447_elilhg_HI59950-4_Asize_fa2.indd 3 12/16/09 12:32:00 PM

HS-21U.S. Pharmacist • March 2010 • www.uspharmacist.com
IDENTIFYING KIDNEY DISEASEH
EALTH
SY
STEM
S ED
ITION
for pharmacists to calculate CrCl or GFR, including information provided on the National Kidney Foun-dation’s Web site (www.kidney.org).
Patients who have low CrCl or GFR and receive renally excreted maintenance drugs should have either the dose reduced, the dosing interval extended, or both. For example, the recommended digoxin main-tenance dose for patients with normal kidney function is usually 0.25 mg administered orally daily. In patients with severe kidney disease, the d i gox in do se shou ld be decreased to 0.125 mg orally every other day.17 This is an example of a renally excreted drug that requires reduction of both the dose and the fre-quency. Loading doses do not usually need to be adjusted in patients with CKD. Many renally excreted drugs require a dosage adjustment when the CrCl falls below 50 mL/min.18 Pharmacists should become familiar with commonly used drugs that required dosage adjustments (TABLE 3).
Recommendations for PharmacistsPharmacists play a vital role in the overall management of patient care. The following are general recommen-dations for practicing pharmacists to observe when reviewing drug therapies:
• Assess and identify underlying risk factors• Recognize combination nephrotoxic medications• Use alternative nonnephrotoxic drugs (e.g., avoid
the use of NSAIDs)• Assess baseline kidney function• Adjust the dosage as needed• Monitor kidney functions and vital signs during
nephrotoxic therapy.Therapy may not be effective and toxicity can occur
if inappropriate drug dosing is taking place in patients with kidney disease. In particular, older patients are at a higher risk of developing advanced kidney disease and related adverse events with the use of multiple medications to treat multiple conditions. Pharma-cists should pay careful atten-tion to patient kidney function when assessing drug therapies in order to use the appropriate dosage and avoid complications for this vulnerable patient population. Awareness of CKD in the U.S. is low,19 and phar-macists can help influence and
educate consumers about the importance of protecting the kidneys. When encountering a prescription, phar-macists should be reminded to screen the patient’s kidney function, as they are the last line of defense for these patients.
REFERENCES1. National Kidney Foundation. KDOQI Clinical Practice Guidelines. www.kidney.org/professionals/kdoqi/guidelines.cfm. Accessed June 2, 20092. Prevalence of reported ESRD. United States Renal Data System. www.usrds.org/2006/ref/B_prevalence_06.pdf. Accessed June 2, 2009.3. WHO Medicines Strategy 2008-2013. Draft 8 (13 June 2008). World Health Organization. www.who.int/medicines/publications/Medicines_Strategy_draft08-13.pdf. Accessed June 13, 2009.4. Kohli HS, Bhaskaran MC, Muthukumar T, et al. Treatment-related acute renal failure in the elderly: a hospital-based prospective study. Nephrol Dial Transplant. 2000;15:212-217.5. Hoste EA, Kellum JA. Acute kidney injury: epidemiology and diagnostic criteria. Curr Opin Crit Care. 2006;12:531-537.6. Rahman M, Pressel S, Davis BR, et al; ALLHAT Collaborative Research Group. Cardiovascular outcomes in high-risk hypertensive patients stratified by baseline glomerular filtration rate. Ann Intern Med. 2006;144:172-180.7. Krop JS, Coresh J, Chambless LE, et al. A community-based study of explanatory factors for the excess risk for early renal function decline in blacks vs. whites with diabetes: the Atherosclerois Risk in Communities study. Arch Intern Med. 1999;159:1777-1783.8. Kaufman J, Dhakal M, Patel B, Hamburger R. Community-acquired acute renal failure. Am J Kidney Dis. 1991;17:191-198.9. Nash K, Hafeez A, Hou S. Hospital-acquired renal insufficiency. Am J Kidney Dis. 2002;39:930-936.10. Bellomo R. The epidemiology of acute renal failure: 1975 versus 2005. Curr Opin Crit Care. 2006;12:557-560.11. Guo X, Nzerue C. How to prevent, recognize, and treat drug-induced nephrotoxicity. Clev Clin J Med. 2002;69:289-297.
12. Schetz M, Dasta J, Goldstein S, Golper T. Drug-induced acute kidney injury. Curr Opin Crit Care. 2005;11:555-565.13. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16:31-41.14. Food and Drug Administration. Guidance for industry: pharmacokinetics in patients with impaired renal function—study design, data analysis, and impact on dosing and labeling. May 1998. www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformation/Guidances/UCM072127.pdf. Accessed February 9, 2009.15. Levey AS, Bosch JP, Lewis JB, et al. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461-470.16. CKD and drug dosing: information for providers. National Kidney Disease Education Program. http://nkdep.nih.gov/professionals/drug-dosing-information.htm. Accessed February 9, 2010.17. Lexi-Comp Online. Hudson, OH: Lexi-Comp, Inc; 2009. www.lexi.com. Accessed August 27, 2009.18. Aronoff GR, Berns JS, Brier ME, et al. Drug Prescribing in Renal Failure: Dosing Guidelines for Adults. 4th ed. Philadelphia, PA: American College of Physicians–American Society of Internal Medicine; 1999.19. Coresh J, Byrd-Holt D, Astor BC, et al. Chronic kidney disease aware-ness, prevalence, and trends among U.S. adults, 1999 to 2000. J Am Soc Nephrol. 2005;16:180-188.20. Drug information. Micromedex Healthcare Series. Greenwood Village, CO: Thomson Micromedex. www.micromedex.com. Accessed February 9, 2010.21. Munar MY, Singh H. Drug dosing adjustments in patients with chronic kidney disease. Am Fam Physician. 2007;75:1487-1496.
If a patient has a GFR of less than
60 mL/min/1.73 m2 and comorbid conditions such as diabetes and
hypertension, he or she will experience a higher chance of developing
kidney injury.
HS16 Kidney 3_1bo.indd HS-21HS16 Kidney 3_1bo.indd HS-21 3/2/10 9:57 AM3/2/10 9:57 AM
In-Service Primers
HS-22U.S. Pharmacist • March 2010 • www.uspharmacist.com
The different botulinum toxin products available come in varying degrees of potency, and therefore are not interchangeable.
Botox, which is a purified form of the toxin botuli-num produced by the bac-
terium Clostridium botulinum, has several medical applications. The C botulinum toxin causes a life-threat-ening type of food poisoning called botulism.1 Recently, the FDA issued some new guidelines and revisions with regard to Botox applications. In August 2009, the FDA issued a special alert regarding changes to the generic names and revisions to the prescribing information for botulinum toxin types A and B, including the newly approved abo-botulinumtoxinA (Dysport) and rimabotulinumtoxinB (Myobloc).2
The FDA issued a boxed warn-ing regarding the risk of a poten-tially life-threatening spread of the toxin’s effect from the local injec-tion site. In addition, it required provision of a medication guide to explain risks to patients and care-givers. The FDA also placed emphasis on the differences in potency among the products (TABLE 1).3
MECHANISM OF ACTIONOnabotulinumtoxinA (previously known as botulinum toxin type A) is a neurotoxin produced by C botulinum, a spore-forming anaer-obic bacillus. In humans, ona-botulinumtoxinA appears to affect only the presynaptic membrane of the neuromuscular junction, where it prevents the calcium-dependent release of acetylcholine and pro-duces a state of denervation. Mus-cle inactivation persists until new
fibrils grow from the nerve and form junction plates on new areas of the muscle-cell walls.1,4
INDICATIONS AND USESBotox products are categorized as neuromuscular blockers and oph-thalmic agents. They are used to treat a variety of conditions.
Labeled Indications and DosingReduction of Glabellar Lines: Botox Cosmetic is used for the temporary improvement of the appearance of facial lines and wrinkles due to moderate-to-severe glabellar lines (lines between the eyebrows) in adult patients up to 65 years of age. For an effective intramuscular (IM) dose, the clini-cian must observe the patient’s ability to activate the superficial muscles injected. The location, size, and use of muscles may vary between individuals. A dose of 4 U (0.1 mL) is injected into each of five sites, two in each corruga-tor muscle and one in the pro-cerus muscle, for a total dose of 20 U (0.5 mL). The dose may be repeated every 3 to 4 months to achieve the desired result.4
Cervical Dystonia: This is a neu-rologic disorder that causes severe neck- and shoulder-muscle contrac-tions. In patients aged 16 years and older, the mean IM dose in patients previously treated with botulinum toxin is 236 U divided among the affected muscles; the initial dose in previously untreated patients should be lower. Subse-
Manouchehr Saljoughian, PharmD, PhDDepartment of Pharmacy ServicesAlta Bates Summit Medical CenterBerkeley, California
Botox ApplicationsA Review of Risks and Benefits
HEA
LTH S
YS
TEMS
EDITIO
N
HS22 InService 3_1sc.indd HS-22HS22 InService 3_1sc.indd HS-22 3/2/10 9:58 AM3/2/10 9:58 AM
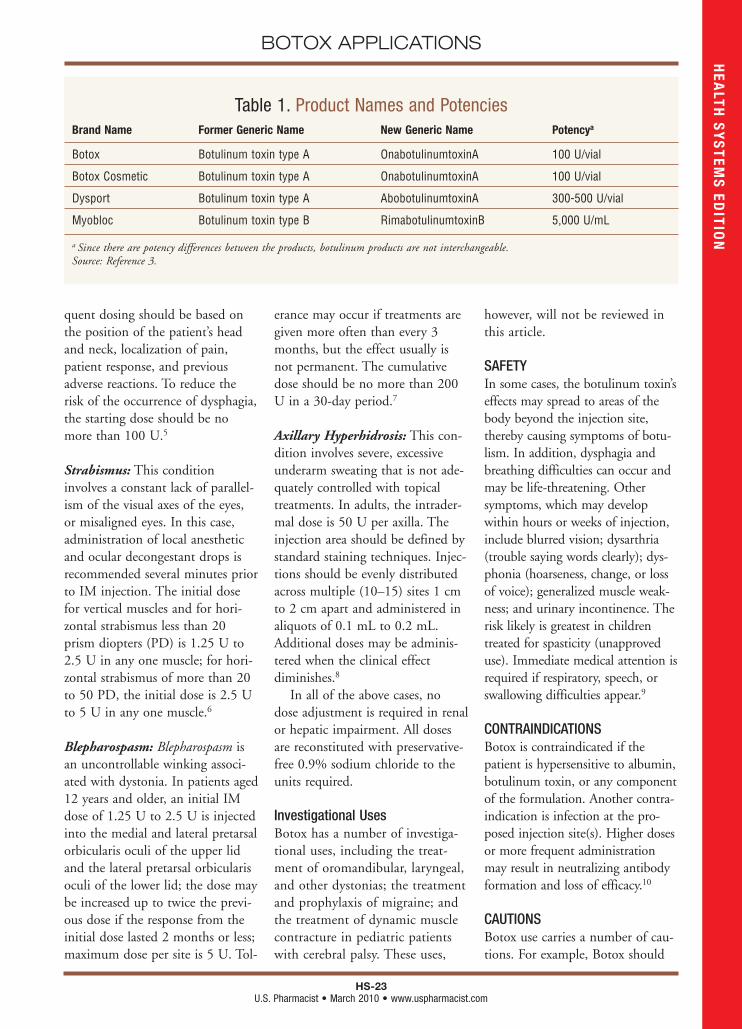
HS-23U.S. Pharmacist • March 2010 • www.uspharmacist.com
BOTOX APPLICATIONS
quent dosing should be based on the position of the patient’s head and neck, localization of pain, patient response, and previous adverse reactions. To reduce the risk of the occurrence of dysphagia, the starting dose should be no more than 100 U.5
Strabismus: This condition involves a constant lack of parallel-ism of the visual axes of the eyes, or misaligned eyes. In this case, administration of local anesthetic and ocular decongestant drops is recommended several minutes prior to IM injection. The initial dose for vertical muscles and for hori-zontal strabismus less than 20 prism diopters (PD) is 1.25 U to 2.5 U in any one muscle; for hori-zontal strabismus of more than 20 to 50 PD, the initial dose is 2.5 U to 5 U in any one muscle.6
Blepharospasm: Blepharospasm is an uncontrollable winking associ-ated with dystonia. In patients aged 12 years and older, an initial IM dose of 1.25 U to 2.5 U is injected into the medial and lateral pretarsal orbicularis oculi of the upper lid and the lateral pretarsal orbicularis oculi of the lower lid; the dose may be increased up to twice the previ-ous dose if the response from the initial dose lasted 2 months or less; maximum dose per site is 5 U. Tol-
erance may occur if treatments are given more often than every 3 months, but the effect usually is not permanent. The cumulative dose should be no more than 200 U in a 30-day period.7
Axillary Hyperhidrosis: This con-dition involves severe, excessive underarm sweating that is not ade-quately controlled with topical treatments. In adults, the intrader-mal dose is 50 U per axilla. The injection area should be defined by standard staining techniques. Injec-tions should be evenly distributed across multiple (10–15) sites 1 cm to 2 cm apart and administered in aliquots of 0.1 mL to 0.2 mL. Additional doses may be adminis-tered when the clinical effect diminishes.8
In all of the above cases, no dose adjustment is required in renal or hepatic impairment. All doses are reconstituted with preservative-free 0.9% sodium chloride to the units required.
Investigational UsesBotox has a number of investiga-tional uses, including the treat-ment of oromandibular, laryngeal, and other dystonias; the treatment and prophylaxis of migraine; and the treatment of dynamic muscle contracture in pediatric patients with cerebral palsy. These uses,
however, will not be reviewed in this article.
SAFETYIn some cases, the botulinum toxin’s effects may spread to areas of the body beyond the injection site, thereby causing symptoms of botu-lism. In addition, dysphagia and breathing difficulties can occur and may be life-threatening. Other symptoms, which may develop within hours or weeks of injection, include blurred vision; dysarthria (trouble saying words clearly); dys-phonia (hoarseness, change, or loss of voice); generalized muscle weak-ness; and urinary incontinence. The risk likely is greatest in children treated for spasticity (unapproved use). Immediate medical attention is required if respiratory, speech, or swallowing difficulties appear.9
CONTRAINDICATIONSBotox is contraindicated if the patient is hypersensitive to albumin, botulinum toxin, or any component of the formulation. Another contra-indication is infection at the pro-posed injection site(s). Higher doses or more frequent administration may result in neutralizing antibody formation and loss of efficacy.10
CAUTIONSBotox use carries a number of cau-tions. For example, Botox should
Table 1. Product Names and PotenciesBrand Name Former Generic Name New Generic Name Potencya
Botox Botulinum toxin type A OnabotulinumtoxinA 100 U/vial
Botox Cosmetic Botulinum toxin type A OnabotulinumtoxinA 100 U/vial
Dysport Botulinum toxin type A AbobotulinumtoxinA 300-500 U/vial
Myobloc Botulinum toxin type B RimabotulinumtoxinB 5,000 U/mL
a Since there are potency differences between the products, botulinum products are not interchangeable.Source: Reference 3.
HEA
LTH S
YS
TEMS
EDITIO
N
HS22 InService 3_1sc.indd HS-23HS22 InService 3_1sc.indd HS-23 3/2/10 9:58 AM3/2/10 9:58 AM

HS-24U.S. Pharmacist • March 2010 • www.uspharmacist.com
BOTOX APPLICATIONS
be used with caution in patients with neuromuscular diseases such as myasthenia gravis or neuropathic disorders (e.g., amyotrophic lateral sclerosis).
Reduced blinking from injec-tion of the orbicularis muscle can lead to corneal exposure and ulcer-ation when treating blepharo-spasm. For this reason, caution should be exercised in patients with angle-closure glaucoma. Careful testing of corneal sensa-tion, avoidance of lower-lid injec-tions, and treatment of epithelial defects are necessary.
Extreme caution should be exercised in patients with preex-isting respiratory disease; treat-ment of cervical dystonia with botulinum toxin may weaken accessory muscles that are neces-sary for these patients to main-tain adequate ventilation. Extreme caution also should be taken in patients receiving other agents that may interfere with neuromuscular transmission (e.g., aminoglycosides, neuromuscular blocking agents).10
PREGNANCY CONSIDERATIONSNo studies have been conducted on the human reproductive sys-tem, but Botox use should be avoided in pregnancy. Based on limited case reports, adverse fetal
effects have not been observed with inadvertent administration during pregnancy. It is currently recommended that adequate con-traception be ensured in women of childbearing potential. Excre-tion in breast milk is unknown, so Botox should be used with caution in nursing women.11
MONITORINGBotox should be used with caution in the presence of disease that affects neuromuscular transmission or coagulation. Prior to adminis-tration, the potential for interac-tions with other medications the patient may be taking (e.g., any-thing that may affect neuromuscu-lar transmission) should be evalu-ated. Therapeutic effects and adverse response should be
assessed following each treatment. Adverse events may occur several hours after injection or be delayed up to several weeks. The patient should be instructed about neces-sary aftercare, possible side effects and appropriate interventions, and adverse symptoms that must be reported.11
PATIENT EDUCATIONThe patient should be advised that this medication is administered by injection. Aftercare instructions should be followed precisely. The patient should be informed that Botox, when used to improve appearance of facial lines or wrin-kles, may cause headache; dry, painful, watery, or bloodshot eyes; a feeling of something in the eye; increased sensitivity to light; or slightly blurred vision. With other uses, the patient should be made aware that Botox may cause head-ache, dizziness, drowsiness, gastro-intestinal upset, neck pain, upper respiratory infection, sore throat, or rhinitis. The patient should report immediately any difficulty swallowing, breathing, or speaking or any muscle weakness, vision problems, loss of bladder control, worsening symptoms, or other persistent or acute adverse symp-toms, even if these occur several weeks following treatment.12
REFERENCES1. Kukreja R, Singh BR. Botulinum neurotox-ins: structure and mechanism of action. In: Proft T, ed. Microbial Toxins: Current Research and Future Trends. Norfolk, UK: Caister Aca-demic Press; 2009.2. FDA. OnabotulinumtoxinA (marketed as Botox/Botox Cosmetic), AbobotulinumtoxinA (marketed as Dysport) and Rimabotulinumtox-inB (marketed as Myobloc) Information. www.fda.gov/Drugs/DrugSafety/Postmarket-DrugSafetyInformationforPatientsandProviders/ucm175011.htm. Accessed February 17, 2010.3. FDA. FDA’s MedWatch Safety Alerts: June 2009. www.fda.gov/ForConsumers/ConsumerUpdates/ucm164442.htm. Accessed February 17, 2010.
4. Rzany B, Dill-Müller D, Grablowitz D, et al. Repeated botulinum toxin A injections for the treatment of lines in the upper face: a retrospec-tive study of 4,103 treatments in 945 patients. Dermatol Surg. 2007;33(suppl 1):S18-S25.5. Velickovic M, Benabou R, Brin MF. Cervical dystonia: pathophysiology and treatment options. Drugs. 2001;61:1921-1943.6. Naumann M, Jankovic J. Safety of botulinum toxin type A: a systematic review and meta-analysis. Curr Med Res Opin. 2004;20:981-990.7. Hsiung GY, Das SK, Ranawaya R, et al. Long-term efficacy of botulinum toxin A in treatment of various movement disorders over a 10-year period. Mov Disord. 2002;17:1288-1293.8. Eisenach JH, Atkinson JL, Fealey RD.
Hyperhidrosis: evolving therapies for a well-established phenomenon. Mayo Clin Proc. 2005;80:657-666.9. Coté TR, Mohan AK, Polder JA, et al. Botu-linum toxin type A injections: adverse events reported to the US Food and Drug Administra-tion in therapeutic and cosmetic cases. J Am Acad Dermatol. 2005;53:407-415.10. Carruthers J, Carruthers A. Complications of botulinum toxin A. Facial Plast Surg Clin North Am. 2007;15:51-54.11. Mejia NI, Vuong KD, Jankovic J. Long-term botulinum toxin efficacy, safety, and immunogenicity. Mov Disord. 2005;20:592-597.12. MedlinePlus. Botox. www.nlm.nih.gov/medlineplus/botox.html. Accessed February 17, 2010.
HEA
LTH S
YS
TEMS
EDITIO
N
In some cases, the effects of the botulinum toxin may spread to areas of the body beyond the injection site, thereby causing symptoms of botulism.
HS22 InService 3_1sc.indd HS-24HS22 InService 3_1sc.indd HS-24 3/2/10 9:58 AM3/2/10 9:58 AM
20U.S. Pharmacist • March 2010 • www.uspharmacist.com
Senior Care
As many as 85% of peri-menopausal women experi-ence hot flashes (flushes),
night sweats, and/or sleep distur-bances secondary to vasomotor instability.1 Hot flashes are the most frequent symptoms of peri-menopause and menopause, and almost all women report hot flashes with induced menopause (e.g., surgery, chemotherapy) or premature menopause (i.e., before age 40 years).2,3 Hot flashes also occur after the discontinuation of exogenous estrogen (e.g., hor-mone-replacement therapy).4
The mean age for onset of menopause in the United States is 51 years (range 40-58 years).5 Hot flashes are typically more severe at the onset of menopause (i.e., within the first 2 years) and become less intense and less fre-quent with age.4,5 In perimeno-pause, hot flashes occur when endogenous estrogen levels decrease, and then resolve as estrogen levels increase; consider-able daily fluctuations occur approximately 1 year prior to menopause.6 At menopause, vaso-motor symptoms are associated with a decline in ovarian func-tion.7 Of the 80% of perimeno-pausal women reporting hot flashes, 85% remain symptomatic for more than 1 year, and 25% to 50% remain symptomatic for up to 5 years.4 According to a 25-year longitudinal study, preva-lence of hot flashes decreases pro-gressively with age.8 The maximal prevalence of hot flashes was
between 52 and 54 years of age in the study, with prevalence reaching 9% by age 72.8 Vasomo-tor symptoms have the potential to interfere with daily function-ing and alter quality of life. While vasomotor symptoms are not considered harmful, they do indicate an estrogen deficiency.9
Sleep disturbances are often a complication of hot flashes. Noc-turnal hot flashes, or night sweats, disrupt sleep and, if recur-rent, may contribute to insom-nia.10 These sleep disturbances can eventually lead to fatigue, irritability, poor concentration, memory problems, anxiety, and depression; a decreased quality of life may be secondary to these symptoms.10 If hot flashes become especially disruptive to daily routines, pharmacists can recommend that patients discuss appropriate treatment options with their health care provider.10
PATHOPHYSIOLOGY OF HOT FLASHESThe exact mechanism of hot flashes is not completely under-stood.5 It is known, however, that the neuroendocrine system has an impact on the thermoregulatory nucleus in the hypothalamus, such that during menopause small temperature changes (as little as 0.01°F) can trigger hot flashes.11 Perspiration and vasodilation (i.e., the symptoms of hot flashes) occur when the body attempts to preserve heat loss and maintain the core body temperature.5,11
Mary Ann E. Zagaria, PharmD, MS, CGPSenior Care Consultant Pharmacist and President of MZ Associates, Inc.Norwich, New Yorkwww.mzassociatesinc.comRecipient of the Excellence in Geriatric Phar-macy Practice Award from the Commission for Certification in Geriatric Pharmacy.
At menopause, the decline in ovarian function is associated with changes in the brain’s thermoregulatory centers.
Hot Flashes and Night Sweats
20 SeniorCare 3_2sc.indd 2020 SeniorCare 3_2sc.indd 20 3/2/10 12:58 PM3/2/10 12:58 PM

21U.S. Pharmacist • March 2010 • www.uspharmacist.com
HOT FLASHES AND NIGHT SWEATS
Changes in the neuroendocrine system that are associated with hot flashes commence with declines in estrogen and proges-terone levels.5 Further, changes in the levels of endorphins, norepi-nephrine, and serotonin take place systemically.11-14 Estrogen-alone therapy or estrogen-proges-tin combination therapy can help balance the neuroendocrine sys-tem and readjust the trigger point in the hypothalamus.5 Antidepres-sants that inhibit norepinephrine or serotonin reuptake, or both, may also help to balance the alter-ations in the hypothalamus and potentially relieve hot flashes.5
CLINICAL PRESENTATION: SIGNS AND SYMPTOMS TABLE 1 outlines the symptoms of hot flashes—a subjective sensation of intense warmth in the upper body typically lasting 30 seconds to 5 minutes; when these flashes manifest during the night, they are referred to as night sweats.6 Hot flashes vary in frequency (i.e., several in 1 day or a few each week).10 Persistent sweating may be experienced throughout the day and night, or patients may just feel occasional warmth.10 Hot flashes may alter-nate with other vasomotor symp-toms such as chilly sensations and, less commonly, paresthesias.7
TREATMENTAvoiding triggers of hot flashes (TABLE 2) may help in decreasing their frequency and intensity.10 If treatment becomes necessary to ameliorate symptoms that inter-fere with everyday functioning, periodic reevaluation for contin-ued need for treatment is recom-mended. Response to treatment is determined by improvement in subjective symptoms.9
Hormone TherapyHormone therapy is recom-mended for moderate-to-severe hot flashes. Estrogen is the most effective treatment for hot flashes, although progestins are used as an alternative in some instances.
Estrogen: Pharmacotherapy with estrogen is specific and is the most effective treatment for vaso-
motor symptoms.7,10 Benefits include a reduction of hot flashes and night sweats (and associated sleep disturbance).6 Women with an intact uterus receive a proges-tin in combination with estrogen to protect against endometrial cancer.10 For women who have had a hysterectomy, an estrogen-only regimen is prescribed. For either regimen, the lowest effec-tive dose for the shortest period of time required to relieve symp-toms is recommended.10
Risks associated with combina-tion therapy include an increased incidence of breast cancer, pul-monary embolism (PE), demen-tia, and coronary artery disease (CAD).6 The increased risk of CAD, which doubles during the first year of therapy and is partic-ularly high in women with ele-vated LDL cholesterol prior to treatment, is not prevented with aspirin and statins.6 Estrogen-only therapy increases the inci-dence of ischemic stroke while having no effect on the incidence of CAD; effects of this therapy decrease the incidence of hip fractures and are less clear with regard to breast cancer and PE.6 Estrogen is contraindicated in patients with a history of venous thromboembolism or breast can-cer.10 If estrogen is contraindi-
Table 1. Symptoms of Hot Flashes• Sensation of pressure in the head on commencement of the hot flash • Sensation of mild warmth to intense heat spreading through upper body
and face • Flushed appearance; red, blotchy skin on face, neck, and upper chest • Rapid heart rate• Perspiration, particularly on upper body • Sensation of body chills as the hot flash subsides • Less commonly: dizziness, faintness, fatigue, weakness
Source: Adapted from References 2 and 9.
Table 2. Potential Triggers of Hot Flashesa • Alcohol• Caffeine• Cigarette smoking• Foods containing nitrites or sulfites• Heat• Hot beverages• Spicy food• Tight clothing
a Obesity (high body mass index) is associated with a higher frequency of hot flashes, and physical inactivity (lack of exercise) is associated with a higher likelihood of the occurrence of hot flashes in menopause.Source: References 2, 6, and 10.
20 SeniorCare 3_2sc.indd 2120 SeniorCare 3_2sc.indd 21 3/2/10 12:58 PM3/2/10 12:58 PM

22U.S. Pharmacist • March 2010 • www.uspharmacist.com
HOT FLASHES AND NIGHT SWEATS
cated in a patient, or deemed undesirable by the patient, other options may be considered.7
Progestins: Progestin-only ther-apy (e.g., megestrol acetate, medroxyprogesterone acetate) can be used as an alternative to estro-gen and may relieve hot flashes, although no long-term safety data exist.2,6,10 Use of micronized pro-gesterone appears to be associated with fewer adverse effects.6 Adverse effects of progestins include abdominal bloating, breast tenderness, increased breast density, headache, increased LDL cholesterol, and decreased HDL cholesterol.6
Nonhormonal Therapy Nonhormonal medications are available and may provide com-parable reduction in the fre-quency and severity of hot flashes.5 While their use may be off-label (i.e., not FDA approved for hot flashes), these agents are approved for other conditions and have been studied in patients with hot flashes.5,10 Available literature reviews (see below) provide assistance with choosing an appropriate nonhor-monal regimen.
Antidepressants: Specific antide-pressants have been found to relieve hot flashes, although not as effectively as hormone therapy for severe hot flashes.2,10 The American College of Obstetri-cians and Gynecologists acknowl-edges that antidepressants are useful in the treatment of hot flashes in patients with a history of breast cancer or in healthy menopausal women who do not wish to take hormonal therapy.15 Carroll and Kelley evaluated the published literature on the use of
antidepressants for the manage-ment of hot flash symptoms via a literature search using PubMed, International Pharmaceutical Abstracts, and MEDLINE data-bases from inception through May 2009.5 Pharmacists can refer to Reference 5 for this evaluation of hot flashes in clinical trials of antidepressants, which includes specific dosages and adverse reac-tions reported.
Low doses of selective serotonin reuptake inhibitors (SSRIs; e.g., paroxetine, sertraline, citalopram, escitalopram, fluvoxamine, fluox-etine) and serotonin and norepi-nephrine reuptake inhibitors (SNRIs; e.g., venlafaxine, desven-lafaxine, duloxetine) may decrease hot flashes through their ability to inhibit the reuptake of neu-rotransmitters.5 Adverse effects (e.g., nausea, dizziness, weight gain, sexual dysfunction) should be considered when weighing benefits versus risks for an indi-vidual patient.10
Carroll and Kelley note that data indicate paroxetine and ven-lafaxine appear to be the most effective of the agents studied in reducing the frequency and sever-ity of hot flashes; paroxetine remains the most studied of the SSRIs.5 These researchers indicate that when patients are unable to tolerate paroxetine or venlafaxine or fail a trial of therapy with these agents, desvenlafaxine, ser-traline, fluoxetine, and citalopram should be considered as second- or third-line options.5 Based on their findings, Carroll and Kelley advise that until more rigorous studies (randomized, controlled trials with diverse menopausal patient populations at least 12 weeks in duration or longer) are conducted to assess their use in the management of hot flashes,
duloxetine, escitalopram, fluvox-amine, and mirtazapine (see below) should be reserved as last-line therapy.5
Mirtazapine possesses potent inhibitory effects on serotonin, histamine, and alpha2-receptors, and is believed to be beneficial in the relief of hot flashes due to its inhibitory effects on serotonin and alpha2-receptors.5,11 Data indicate lack of efficacy, and the drug’s utility may be limited sec-ondary to associated adverse effects of somnolence, appetite stimulation, and weight gain, occurring more frequently and severely than with the SSRIs and SNRIs.5
Gabapentin: The anticonvulsant agent gabapentin, also approved for postherpetic neuralgia, may be moderately effective in reduc-ing hot flashes, especially in those with nocturnal symptoms.10 Adverse effects include drowsi-ness, dizziness, and headaches.10 Clonidine: The alpha2 adrener-gic agonist clonidine relieves vasomotor symptoms in some patients; this is accomplished by the agent’s ability to diminish central adrenergic outflow that regulates blood flow to cutane-ous vessels.7,16 Clonidine may be administered orally or transder-mally. Due to common adverse effects including dizziness, seda-tion, dry mouth/nasal mucosa, and constipation, its usefulness in the treatment of hot flashes may be limited.10,16 Further, clonidine causes sodium and water retention, which may require coadministration with a diuretic.16
Patients should be advised about the risks of abrupt cloni-dine withdrawal; a rapid increase
20 SeniorCare 3_2sc.indd 2220 SeniorCare 3_2sc.indd 22 3/2/10 12:58 PM3/2/10 12:58 PM

*Based on retail price of MiraLAX 30-dose,17.9 oz. (510 g) twin pack at leading club store.Use as directed.
References: 1. Stoltz R, et al. An efficacy and consumer preference study of polyethylene glycol 3350 for the treatment of constipation in regular laxative users. HomeHealth Care Consultant. 2001;8:21-26. 2. Cleveland MvB, et al. New polyethylene glycol laxative for treatment of constipation in adults: a randomized, double-blind,placebo-controlled study. South Med J. 2001;94:478-481. 3. Data on file, Schering-Plough HealthCare Products. 4. Di Palma JA, et al. An open-label study of chronicpolyethylene glycol laxative use in chronic constipation. Aliment Pharmacol Ther. 2006;25:703-708. 5. DiPalma JA, et al. A randomized, multicenter, placebo-controlledtrial of polyethylene glycol laxative for chronic treatment of chronic constipation. Am J Gastroenterol. 2007;102:1436-1441. 6. DiPalma JA, et al. A randomized, multicentercomparison of polyethylene glycol laxative and tegaserod in treatment of patients with chronic constipation. Am J Gastroenterol. 2007;102:1964-1971. 7. DiPalma JA,et al. A randomized, placebo-controlled, multicenter study of the safety and efficacy of a new polyethylene glycol laxative. Am J Gastroenterol. 2000;95:446-450.8. DiPalma JA, et al. Braintree polyethylene glycol (PEG) laxative for ambulatory and long-term care facility constipation patients: report of randomized, cross-over trials.Online J Dig Health.1999;1:1-7. 9. Tran LC, et al. Lack of lasting effectiveness of PEG 3350 laxative treatment of constipation. J Clin Gastroenterol. 2005;39:600-602.
Recommend MiraLAX® to liberateyour patients from occasional constipationand put them in control of their condition
• In multiple clinical trials, MiraLAX has been proven to1-9:— Increase water content and volume of stool— Soften stool to ease passage— Result in a bowel movement within 24-72 hours
of an oral dose— Increase the frequency of bowel movements
• In clinical studies, MiraLAX was well toleratedand had a low incidence of adverse events1-9
• MiraLAX costs as little as 49¢ per dose*—an economical choice for your patients withoccasional constipation
Restore your patients’ natural rhythm™
For occasional constipation
MiraLAX®laxative sets your patients free
©2009, Schering-Plough HealthCare Products, Inc.www.MiraLAX.com

24U.S. Pharmacist • March 2010 • www.uspharmacist.com
HOT FLASHES AND NIGHT SWEATS
in blood pressure and symptoms of sympathetic overactivity can be avoided using a slow taper (e.g., over 1 week for oral dosage) when this agent is discontinued.16,17 If clonidine needs to be discontin-ued in a patient receiving both a beta-blocker and clonidine, the beta-blocker is withdrawn first, several days before clonidine; then clonidine is slowly decreased to discontinuation.17
Alternative Medicine While alternative therapies have shown promise for relieving symptoms such as hot flashes in menopause, more data are required to establish the risks (e.g., adverse effects, interactions with medications) and benefits of these nontraditional reme-dies.2 Of further importance is the non–FDA-regulated status of these formulations.2 Patients should be reminded to inform their health care providers about any alternative therapies they are taking.
Black Cohosh: Black cohosh, which has a good safety record, is popular in the U.S. and is widely used in Europe for the relief of hot flashes.10 While there is little evidence regarding its effectiveness for menopausal
symptom relief, some studies suggest black cohosh may be useful for very short-term (6 months or less) relief of hot flashes and night sweats.2,10 Gas-trointestinal upset is an associ-ated side effect.2
Soy and Red Clover: Isoflavones are estrogen-like compounds in soy, red clover, and numerous other plants and are thought to have weak estrogen-like effects that may reduce hot flashes.2,10 Studies involving soy and women with hot flashes have generally found no benefit, although selected isoflavones have mixed results for menopausal symptom relief.10
Evening Primrose Oil: Although there is no scientific evidence to support its use, this botanical is often used to treat hot flashes.2 Patients taking anticoagulants should not use this product; side effects include nausea and diarrhea.2
Flaxseed: Flaxseed is available as a whole seed and seed oil and may also be referred to as lin-seed.2 There is no evidence sup-porting its use to decrease the symptoms of menopause, particu-larly hot flashes.2
Lifestyle MeasuresPatients should be instructed to avoid triggers of hot flashes (TABLE 2). Keeping the body cool (e.g., use of fans during the day, bedroom cool at night, light lay-ers of clothing with natural fibers such as cotton) and practicing deep breathing (e.g., 15 minutes in the morning, 15 minutes in the evening, and at the onset of hot flashes) have been recom-mended to reduce the likelihood and/or intensity of vasomotor symtoms.2,10 Suggested measures for daily exercise include walk-ing, swimming, dancing, and bicycling.2
CONCLUSIONVasomotor symptoms have the potential to interfere with daily functioning and alter quality of life. Hot flashes are the most fre-quent symptoms of perimeno-pause and menopause, and phar-macologic and lifestyle measures are available options used in their treatment. The choice between hormone therapy and nonhormonal therapy, such as an antidepressant for relief of vaso-motor symptoms, requires con-sideration of the current scien-tific evidence and the patient’s comorbidities and related medi-cation therapy.
REFERENCES1. Santoro N, Brown JR, Adel T, et al. Characteriza-tion of reproductive hormonal dynamics in the peri-menopause. J Clin Endocrinol Metab. 1996;81:1495-1501. 2. Menopause and hot flashes. WebMD. www.webmd.com/menopause/guide/hot-flashes. Accessed February 15, 2010. 3. Dorland’s Pocket Medical Dictionary. 28th ed. Phil-adelphia, PA: Elsevier Saunders: 2009.4. Beers MH, Berkow R, eds. The Merck Manual of Geriatrics. 3rd ed. Whitehouse Station, NJ: Merck & Co; 2000:1208-1209,1211,1216. 5. Carroll DG, Kelley KW. Use of antidepressants for management of hot flashes. Medscape. www.medscape.com/viewarticle/711910. Accessed Febru-ary 15, 2010. 6. Beers MH, Porter RS, Jones TV, et al. The Merck Manual of Diagnosis and Therapy. 18th ed. White-
house Station, NJ: Merck Research Laboratories; 2006:2081-2082.7. Loose DS, Stancel GM. Estrogens and progestins. In: Brunton LL, Lazo JS, Parker KL, eds. Goodman & Gillman’s The Pharmacological Basis of Therapeutics. 11th ed. New York, NY: McGraw-Hill Companies; 2006:1541-1571.8. Rodstrom K, Bengtsson C, Lissner L, et al. A lon-gitudinal study of the treatment of hot flushes: the population study of women in Gothenburg during a quarter of a century. Menopause. 2002;9:156-161. 9. Ruggiero RJ. Gynecologic disorders. In: Herfindeal ET, Gourley DR, eds. Textbook of Therapeutics: Drug and Disease Management. 7th ed. Lippincott Williams & Wilkins: Philadelphia, PA; 2000:2008-2009. 10. Hot flashes. Mayo Clinic Web site. www.mayo-clinic.com/health/hot-flashes/ds01143. Updated June 12, 2009. Accessed February 15, 2010. 11. Perez D, Loprinzi CL, Barton DL, et al. Pilot
evaluation of mirtazapine for the treatment of hot flashes. J Support Oncol. 2004;2:50-56. 12. Berendsen HH. The role of serotonin in hot flushes. Maturitas. 2000;36:155-164. 13. Casper RF, Yen SS. Neuroendocrinology of menopausal flushes: a hypothesis of flush mecha-nism. Clin Endocrin. 1985;22:296-312. 14. Rosenberg J, Larsen SH. Hypothesis: pathogene-sis of postmenopausal hot flush. Med Hypotheses. 1991;35:349-350. 15. American College of Obstetricians and Gynecol-ogists. Vasomotor symptoms. Obstet Gynecol. 2004;4(suppl):S106-S107. 16. Howland RD, Mycek MJ. Pharmacology. 3rd ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2006:77,223-224.17. Semla TP, Beizer JL, Higbee MD. Geriatric Dos-age Handbook. 14th ed. Hudson, OH: Lexi-Comp, Inc; 2009.
20 SeniorCare 3_2sc.indd 2420 SeniorCare 3_2sc.indd 24 3/2/10 12:58 PM3/2/10 12:58 PM


31U.S. Pharmacist • March 2010 • www.uspharmacist.com
The National Survey on Drug Use and Health (NSDUH) and the Monitoring the Future (MTF) survey provide updated, long-term statistics about
and insight into drug use across age, racial, ethnic, gender, and geographic groups, among others.1,2 Both surveys highlight the need for focused attention on combating prescription drug abuse in the adolescent population (age 12–17 years). The NSDUH (previously named the National Household Survey on Drug Abuse), which has been con-ducted since 1971, assesses a sample of individuals over the age of 12 years. The MTF survey, sponsored by the National Institute on Drug Abuse (NIDA), has been conducted by the University of Michigan Institute for Social Research since 1975 and focuses primarily on a sample of 8th-, 10th-, and 12th-graders.
Despite similar trends in both surveys regarding the prevalence of drug abuse, the NSDUH has traditionally reported lower rates of substance abuse among adoles-cents.1,2 While the MTF survey does not assess misuse of prescription medications across all adolescent age groups (e.g., narcotics other than cocaine are reported only in 12th-graders), it is useful for comparison with data reported by the NSDUH. This article will review survey data supporting an epidemic in drug misuse among adolescents, discuss commonly abused prescription and nonprescription medications, examine key components of educational programs, and provide available resources for educating the adolescent population.
EpidemiologyThe explosive increase in the misuse of prescription and nonprescription medications has been referred to as “pharm-ing.”3 The term Generation Rx has been used describe this increase in prescription-drug misuse among the current generation of youths.4 In 2007, 9.5% of adolescents aged 12 to 17 years indicated that they had used an illicit drug (marijuana, cocaine, heroin, hallucinogens, inhalants, or psychotherapeutics used nonmedically)
within the past month. While marijuana was the most-used illicit drug (6.7%), past-month nonmedical use of psychotherapeutics (pain relievers, tranquilizers, stimulants, and sedatives) came in second (3.3%).1 Although past-month nonmedical use of prescription medications among adolescents declined slightly from 2002 to 2007 (4.0% and 3.3%, respectively), this should still be an area of great concern and attention in the medical community.1
It also is important to consider lifetime prevalence of drug use, since earlier onset of nonmedical use of prescrip-tion drugs is a predictor of subsequent drug abuse and dependence.5 While the reported lifetime use of amphet-amines among 8th-, 10th-, and 12th-graders has decreased since 1991, the reported lifetime prevalence of narcotics other than heroin has doubled among 12th-graders, from 6.6% in 1991 to 13.2% in 2008.2 Additionally, the reported use of sedatives has increased slightly among 12th-graders—from 6.2% in 1991 to 8.5% in 2008—but has decreased since a peak of 10.5% in 2005.2
Factors that contribute to the misuse of prescription and nonprescription medications among adolescents should be incorporated into the development of educational programs to render them more effective. Several things to consider are the accessibility of products in the store or in
the household medicine cabinet; ease of purchase OTC (for some products) or on the Internet; misconception of the risks associated with prescription
Timothy R. Ulbrich, PharmDAssistant Professor of Pharmacy PracticeNortheastern Ohio University College of
Pharmacy, Rootstown, Ohio
Prevalence of Substance
Abuse in the Adolescent Population
© THINKSTOCK
31 SubstanceAbuse 2_24sc.indd 3131 SubstanceAbuse 2_24sc.indd 31 3/2/10 9:46 AM3/2/10 9:46 AM

32U.S. Pharmacist • March 2010 • www.uspharmacist.com
PREVALENCE OF SUBSTANCE ABUSE
medications; and lack of oversight by parents.3
With regard to access, the NSDUH reported that more than half of past-year nonmedical users of prescription medications over the age of 12 years obtained the medica-tion from a friend or relative for free.1 The MTF survey echoes these results, noting that, among 12th-graders who reported nonmedical use of amphetamines, tranquilizers, or narcotics other than heroin within the last year, more than half were given the medication for free by a friend or relative (58.2%, 59.8%, and 50.5%, respectively).2 When 8th-, 10th-, and 12th-graders were asked about the difficulty of obtaining narcotics other than heroin, 12.1%, 20.3%, and 34.9%, respectively, said that these substances were “fairly easy” or “very easy” to get. The general upward trend from 8th grade to 12th grade also was seen for amphetamines, sedatives, and tranquilizers.2
With regard to perceived harmfulness, the MTF survey assessed this factor for prescription medications only among 12th-graders. When 12th-graders were asked, “How much do you think people risk harming themselves (physically or in other ways) if they take sedatives (barbiturates) regularly?” 50.2% responded that there was “great risk,”
down from 70.2% in 1992.2 When asked the same ques-tion regarding amphetamines, 65.4% responded that there was “great risk,” down from 72.4% in 1992.2
In terms of parental involvement, past-month use of illicit drugs, cigarettes, and alcohol was lower among teens aged 12 to 17 years who reported that their parents “always” or “sometimes” monitored their behavior, versus teens who reported “seldom” or “never.”1 While 9 in 10 parents reported discussing drugs with their child or teen within the past year, “drugs in general,” “cigarettes,” and “alcohol” topped the list of items discussed and “Rx medicines to get high” and “Non-Rx cough medicine to get high” fell into the bottom half.6
Analysis of differences in drug misuse among gender, ethnic, racial, and geographic groups, as well as of predic-tors of misuse, may provide valuable information in terms of early treatment by clinicians and development of suc-cessful educational programs. Among subjects aged 12 years and older, although males tended to have higher rates of illicit drug use, similar rates between males and females were reported for the nonmedical use of prescrip-tion medications.1 In addition, differences in illicit drug
Table 1. Selected Prescription and OTC Medications With Abuse PotentialType of Medication Trade Names Street Names
Opioids and Morphine DerivativesCodeine Empirin With Codeine, Fiorinal With Codeine, Captain Cody, Cody, schoolboy Robitussin A-C, Tylenol With Codeine #3
Fentanyl Actiq, Duragesic, Sublimaze Apache, China girl, China white, dance fever, friend, goodfella, jackpot, murder 8, TNT
Morphine Duramorph, Roxanol M, Miss Emma, monkey, white stuff
Other opioid pain Hydrocodone: Lortab, Vicodin Oxycodone: hillbilly heroin, oxycet, oxycotton, relievers (hydrocodone, Hydromorphone: Dilaudid oxy 80s, percshydromorphone, Meperidine: Demerol Dilaudid: dillies, juicemeperidine, oxycodone, Oxycodone: Oxycontin, Percocet, Percodan, Tylox Demerol: demmies, painkillerpropoxyphene) Propoxyphene: Darvocet, Darvon
StimulantsAmphetamines Adderall, Dexedrine Bennies, black beauties, crosses, hearts, LA turnaround, speed, truck drivers, uppers
Methylphenidate Concerta, Ritalin JIF, MPH, R-ball, Skippy, the smart drug, vitamin R
CNS DepressantsBarbiturates Mebaral, Nembutal Barbs, phennies, red birds, reds, tooies, yellow jackets, yellows
Benzodiazepines Ativan, Halcion, Librium, Valium, Xanax Candy, downers, sleeping pills, tranks
Sleep medications Ambien, Lunesta, Sonata A-minus, no-go pills, zombie pills
Nonprescription MedicationsDextromethorphan Delsym, Robitussin CoughGels, Red hots, Robo, skittles, triple C Vicks DayQuil Cough
Pseudoephedrine Sudafed, SudoGest Crank, crystal, glass, ice, meth, speed
CNS: central nervous system.Source: Reference 9.
31 SubstanceAbuse 2_24sc.indd 3231 SubstanceAbuse 2_24sc.indd 32 3/2/10 9:46 AM3/2/10 9:46 AM

34U.S. Pharmacist • March 2010 • www.uspharmacist.com
PREVALENCE OF SUBSTANCE ABUSE
use among different races and ethnicities have been noted. Past-month illicit drug use was lowest among Asians (4.2%) and highest among American Indians and Alas-kan Natives (12.6%); in between were adolescents of two or more races (11.8%), African Americans (9.5%), Caucasians (8.2%), and Hispanics (6.6%).1
In terms of geographic location, 34% of rural ado-lescents in one study reported lifetime nonmedical use of prescription medications; this is much higher than the national rate.7 While this was an isolated study of 849 rural high school students in Vermont with high reports of concomitant marijuana use, it is an important consideration for practitioners and educators located in rural settings, and further research is warranted to determine whether the findings are consistent among other rural populations.
Predictors of prescription medication misuse among adolescents include poor academic performance; past-year major depression; higher risk-taking levels; and past-year use of alcohol, cigarettes, marijuana, cocaine, or inhal-ants.8 Among adolescents reporting a past-year major depressive episode (MDE), 35.5% used illicit drugs dur-
ing the episode, versus 17.2% among those who did not have a past-year MDE.1
Commonly Abused Prescription and OTC MedicationsBoth prescription and nonprescription medications are abused in the adolescent population.3 A list of commonly abused prescription and nonprescription medications, organized by medication class and including common street names, is given in TABLE 1.9 Commonly abused medications are painkillers (most commonly, opioid-containing products), stimulants, and central nervous system depressants (including sedatives and tranquilizers).9
One common nonprescription product with significant misuse potential is dextromethorphan.3,10 An ingredient in several OTC cough and cold products, dextromethorphan can produce mind-altering effects in larger doses; in exces-sive doses, it can cause dissociative effects similar to those of ketamine and phencyclidine by antagonizing the N-methyl-d-aspartate receptor.3,10 Dextromethorphan has been used clinically since the 1950s, but abuse of the pills (Romilar) led to removal of the product from the market in the 1960s.11
Table 2. Key Principles for Prevention Programs Targeting Children and AdolescentsCategory and Principle Description of Principle
Risk Factors and Protective FactorsPrinciple 1 Enhance protective factors (e.g., parental supervision/support) and reduce risk factors (e.g., aggressive behavior).Principle 2 Address all forms of drug abuse (e.g., misuse of legal drugs, use of illegal drugs, OTCs).Principle 3 Address drug-abuse problem within the local community; target risk factors and enhance protective factors.Principle 4 Tailor programs to a specific audience (e.g., age, ethnicity).
Prevention Planning
Principle 5a Enhance parent–child relationships and discuss parental policies on substance abuse and methods parents can use to educate children.
Principle 6b Intervention can occur as early as preschool.Principle 7b Elementary school–based interventions should focus on educational and emotional awareness to address risk
factors (e.g., aggression, academic failure, dropping out of school).Principle 8b Junior high and high school programs should focus on academic and social competence (e.g., study habits,
communication, peer relationships, drug-resistance skills).Principle 9c Interventions in general populations at transition points (e.g., middle school to high school) can be successful, as
they do not single out any particular group.Principle 10c Combining ≥2 programs (e.g., school-based, family-based) can be more effective than using 1 program alone.Principle 11c Programs that reach populations in ≥1 setting (e.g., school, church) are effective when a consistent message is
communicated.
Prevention-Program DeliveryPrinciple 12 Core program components (e.g., structure, content, delivery) should be retained after a program is adapted for a
setting or community.Principle 13 Programs should be long-term and have components to enhance/reinforce original content.Principle 14 Programs should train teachers in positive classroom-management techniques (e.g., rewarding positive behavior).Principle 15 Programs should employ techniques that allow for active involvement (e.g., role-playing, discussion).Principle 16 Effective programs can be cost-effective. a Specific to family programs.b Specific to school programs.c Specific to community programs.Source: Reference 13.
31 SubstanceAbuse 2_24sc.indd 3431 SubstanceAbuse 2_24sc.indd 34 3/2/10 9:46 AM3/2/10 9:46 AM

37U.S. Pharmacist • March 2010 • www.uspharmacist.com
PREVALENCE OF SUBSTANCE ABUSE
However, different formulations of the product later became available OTC, and a new surge in misuse occurred in the 1990s.11 The wide availability of OTC products containing dextromethorphan makes it a source of concern in terms of misuse by adolescents.
Another worry with regard to the nonprescription market has been the misuse of methamphetamine among adolescents. Methamphetamine is a stimulant that can be produced from products such as pseudoephedrine.12 Among youths aged 16 to 25 years, approximately 47% of meth-amphetamine misusers also reported misuse of a prescrip-tion stimulant.12 In addition, more than 90% of all young people who misused methamphetamine reported lifetime use of at least three different classes of illicit drugs.12
Educational ProgramsInformation about research-based drug-abuse prevention programs supported by the NIDA is available at www.drugabuse.gov/pdf/prevention/RedBook.pdf.13 This document, published by the NIDA, outlines 16 research-based principles that are important to the selection, construction, and delivery of drug-abuse prevention programs (TABLE 2).13 Among adolescents aged 12 to 17 years in 2007, 75.8% reported having seen or heard of drug or alcohol prevention messages at school.1 Among teens who reported exposure to a prevention message at school, 8.7% had used illicit drugs within the past month, compared with 12.0% of those who did not report exposure to a prevention message.1
Educational programs aimed at preventing the misuse of prescription medications among adolescents should take into account that there are differences in motivation for abuse across different classes of medications.14,15 In addi-tion, differences in the source of the prescription medica-tion, as well as differences in sex, ethnicity, and severity of misuse, should be considered.16 For example, in a study assessing data from the 2005–2006 NSDUH, adolescent
females were found to be more likely to steal opioids or obtain them for free, whereas males were more likely to purchase opioid medication or obtain it from a physician.16
ResourcesPharmacists can play an integral role in the attempt to stem adolescent drug misuse by increasing awareness among consumers, participating in community events and presen-tations, and encouraging the proper disposal of prescription medications through programs such as SMARxT Disposal (www.smarxtdisposal.net). Proper disposal of medications may prevent outdated or unnecessary medications from being accessible to the adolescent population. In addition, many resources are available for parents and providers who want to learn more about drug abuse and for individuals who are interested in educating adolescents in their com-munity. The Web sites of the National Institute on Drug Abuse (www.nida.nih.gov), the Partnership for a Drug-Free America (www.drugfree.org), and the Generation Rx Initia-tive at The Ohio State University (http://pharmacy.osu.edu/outreach/generation-rx) all include valuable resources. In addition, material for parents to educate their children, such as the Substance Abuse and Mental Health Services Admin-istration (SAMHSA) Family Guide (www.family.samhsa.gov/default.aspx) and the Talking to Your Kids About Prescrip-tion Drug Abuse brochure developed by the National Coun-cil on Patient Information and Education and SAMHSA (www.talkaboutrx.org/documents/samhsa_parent_brochure.pdf), may be useful.
ConclusionBoth the prevalence of and potential factors contributing to drug misuse among adolescents are sources of concern. Educational efforts in the home, community, or school may be beneficial, and research-based principles should be implemented to develop programs that are specific, timely, and comprehensive.
REFERENCES1. Substance Abuse and Mental Health Services Admin-istration (SAMHSA). Results From the 2008 National Survey on Drug Use and Health: National Findings. NSDUH Series H-36, HHS Publication No. SMA 09-4434. Rockville, MD: SAMHSA Office of Applied Studies; 2009.2. Johnston LD, O’Malley PM, Bachman JG, Schulen-berg JE. Monitoring the Future: National Results on Ado-lescent Drug Use. Overview of Key Findings, 2008. NIH Publication No. 09-7401. Bethesda, MD: National Insti-tute on Drug Abuse; 2009.3. Levine DA. ‘Pharming’: the abuse of prescription and over-the-counter drugs in teens. Curr Opin Pediatr. 2007;19:270-274.4. Partnership for a Drug-Free America. Generation Rx: national study reveals new category of substance abuse emerging: teens abusing Rx and OTC medications inten-tionally to get high. www.drugfree.org/General/Articles/article.aspx?id=df07cc48-88e2-4fc5-abdf-c83c0e22e943&Site=Print&PrintPage=true. Accessed February 12, 2010.5. McCabe SE, West BT, Morales M, et al. Does early
onset of non-medical use of prescription drugs predict subsequent prescription drug abuse and dependence? Results from a national study. Addiction. 2007;102:1920-1930.6. Partnership for a Drug-Free America and MetLife Foundation. 2008 parents attitude tracking study. May 2009. www.drugfree.org/Files/Full_Report_2008. Accessed November 29, 2009.7. Levine SB, Coupey SM. Nonmedical use of prescrip-tion medications: an emerging risk behavior among rural adolescents. J Adolesc Health. 2009;44:407-409.8. Schepis TS, Krishnan-Sarin S. Characterizing adoles-cent prescription misusers: a population-based study. J Am Acad Child Adolesc Psychiatry. 2008;47:745-754.9. National Institute on Drug Abuse. Selected prescrip-tion drugs with potential for abuse. www.nida.nih.gov/PDF/PrescriptionDrugs.pdf. September 2002 (rev April 2005). Accessed November 17, 2009.10. National Institute on Drug Abuse. NIDA InfoFacts: prescription and over-the-counter medications. www.nida.nih.gov/infofacts/PainMed.html. Accessed Novem-ber 29, 2009.
11. Schwartz RH. Adolescent abuse of dextromethorphan. Clin Pediatr (Phila). 2005;44:565-568.12. Wu LT, Pilowsky DJ, Schlenger WE, Galvin DM. Misuse of methamphetamine and prescription stimulants among youths and young adults in the community. Drug Alcohol Depend. 2007;89:195-205.13. National Institute on Drug Abuse. Preventing Drug Use Among Children and Adolescents: A Research-Based Guide for Parents, Educators, and Community Leaders. 2nd ed. NIH Publication No. 04-4212A. Bethesda, MD: NIDA; 2003.14. Boyd CJ, McCabe SE, Cranford JA, Young A. Ado-lescents’ motivations to abuse prescription medications. Pediatrics. 2006;118:2472-2480.15. Twombly EC, Holtz KD. Teens and the misuse of prescription drugs: evidence-based recommendations to curb a growing societal problem. J Prim Prev. 2008;29:503-516.16. Schepis TS, Krishnan-Sarin S. Sources of prescrip-tions for misuse by adolescents: differences in sex, ethnic-ity, and severity of misuse in a population-based study. J Am Acad Child Adolesc Psychiatry. 2009;48:828-836.
31 SubstanceAbuse 2_24sc.indd 3731 SubstanceAbuse 2_24sc.indd 37 3/2/10 9:46 AM3/2/10 9:46 AM
38U.S. Pharmacist • March 2010 • www.uspharmacist.com
Pharmacy Law
Have you ever entered your own vehicle and consid-ered just what is inside of
it? Is there anything that could get you in trouble if you were pulled over by the police for a traffic infraction? Are you sure about that? Before feeling safe, ask your-self, who recently drove your car? Was it your spouse, your teenage son or daughter, a friend, a valet parking attendant, or an employee making a delivery for your phar-macy? Do you know if any contra-band might have been left inside? What follows are two cases show-ing how reckless behavior, or just plain bad luck, could end up caus-ing more trouble than you could ever have imagined.
Case 1: An Unlucky ErrandA 26-year-old man, Steven, was living with his grandmother, Mamie, in Indianapolis, Indiana. He regularly used her car to run
errands and did not own a vehicle himself. One day while riding together, the grandmother asked her grandson to stop at the phar-macy to pick up a refill of her medication. During this trip, Mamie noticed that she had five tablets left in the prescription vial and dumped the pills out into a cup holder in the center console of the car. She then handed the container to Steven so he could take it to the drugstore and obtain the refill. Steven and Mamie both testified that at the time of this occurrence, she never told her grandson what the medication was or what she was using it for and that he did not look at the pre-scription container to see the name of the medication. After they completed their other tasks, Steven dropped Mamie off at home and drove to the pharmacy.
While waiting for the prescrip-tion to be refilled, Steven bought himself something to drink. After picking up the medication, he went back to his grandmother’s car and went to set his drink in the cup holder. Seeing the five pills that Mamie had left there earlier in the day, he removed them so they would not get wet and put them into a netted pocket on the outside of his backpack, which was sitting on the passenger seat. Apparently, he then forgot about them.
The next evening, again while he was driving Mamie’s car around town with a friend (and with the backpack now in the back seat), a police officer pulled Steven over for
failing to stop at a stop sign. As luck (or the absence thereof ) would have it, the officer, while checking Steven’s driver’s license and registra-tion, learned that his license had been suspended and that there was an outstanding warrant for his arrest. The other passenger in the car with Steven at the time did not have a valid driver’s license either. Accordingly, the police officer made arrangements to have the vehicle towed. Following standard proce-dures in these circumstances, the officer proceeded to inventory the contents of the vehicle. It was dur-ing this search that the five tablets in the backpack were discovered. Steven told the officer that they belonged to his grandmother and that he had intended to return them to her but had forgotten about them. He had possession of the tablets in his backpack for a total of about 30 hours.
The pills were identified as hydrocodone, and Steven was charged with a vehicular misde-meanor for driving on a sus-pended license and a felony count of possession of a controlled sub-stance without legal authority. He did not post bail and spent the next 16 days in jail.
During a bench trial by the judge (without a jury), Steven tes-tified as to the facts stated above. Mamie also appeared and explained that she had put the pills into the cup holder and also forgot about them when Steven handed her the prescription refill bag later in the evening. She told
Jesse C. Vivian, RPh, JDProfessor, Department of Pharmacy PracticeCollege of Pharmacy and Health SciencesWayne State UniversityDetroit, Michigan
Claiming ignorance of controlled substances in your vehicle may not excuse you from liability, even if you’re a pharmacist.
A Prescription for Car Trouble
38 Law 3_1sc.indd 3838 Law 3_1sc.indd 38 3/2/10 9:46 AM3/2/10 9:46 AM

39U.S. Pharmacist • March 2010 • www.uspharmacist.com
A PRESCRIPTION FOR CAR TROUBLE
the judge that the pills were hers, that she did not intend to give them to Steven, that she regularly let Steven drive her car, and that he was driving it with her permis-sion on the night he was stopped and apprehended. She also indi-cated that she had no recollection of telling Stephen what the medi-cation was or what it contained. Her testimony indicated that she was not sure about the distinction between a prescription-only medi-cation and a controlled substance or a narcotic and an opiate. For his part, Steven claimed he did not know what the pills in the cup holder were at the time, that he did not know they were a con-trolled substance, that he did not know the name of the medication, and that he did not pay any atten-tion to the name of the drug on the prescription receipt when he picked up the refill for his grand-mother. Curiously, the court record does not indicate whether Steven knew at the time of this incident that hydrocodone is a controlled substance. In hindsight, that seems like a relevant issue to whether he knowingly was in pos-session of a controlled substance without proper authority.
The judge found him guilty on both the felony possession of a controlled substance and misde-meanor charge of driving without a valid license. Steven was sen-tenced to 180 days in prison, with credit for time served and the remaining time suspended.
Steven appealed his convictions. After all, who would want a crimi-nal conviction for narcotics posses-sion on his record, especially if he felt he had made an innocent mis-take of nothing more than forget-fulness? As to the controlled sub-stance possession charge, he argued that there was insufficient evidence
to convict him. The Indiana Court of Appeals denied his appeal.1
The statute in question states that a person who knowingly or intentionally possesses a controlled substance without authorization is guilty of a felony.2 There are stated exceptions that allow family members or others to pick up pre-scriptions for patients unable to do so for themselves. Specifically, a “recipient representative” is defined as “an individual to whom a controlled substance is dispensed if the recipient is unable to receive the controlled substance.”3 Another provision defines an “ulti-mate user” as “a person who law-fully possesses a controlled sub-stance for the use of the person’s household.”4
This, claimed the defendant, creates a sort of “Good Samaritan” exclusion from criminal liability for those who are doing a favor for someone else. The problem with this argument is that there is no time limit inherent in the dis-tinction of doing someone a favor or possessing the drugs for one’s own use or benefit. One could assert he was holding the pills for a week, a month, or even a year and still suggest he was just doing an errand. The court dismissed this argument because the statute under consideration does not address how long someone can be in possession of a controlled sub-stance without violating the law. In other words, possession is pos-session irrespective of the time that the drugs are held by one person for the putative benefit of another. The court also noted that Steven was not convicted because he did not return Mamie’s pre-scription “quick enough”; he was convicted because the indisputable fact was that he was in possession of the drugs when he was caught.
The court used a very narrow interpretation of these provisions to uphold the conviction. It wrote that the grandson was not charged for having in his possession his grandmother’s prescription and failing to give it to her. Rather, he was charged with being in posses-sion of the five hydrocodone pills that his grandmother emptied from a pill bottle into the cup holder and that he later put into his backpack. Without any expla-nation as to how he knew the pills were hydrocodone or that hydro-codone is a controlled substance, the court summarily concluded that the evidence was sufficient to show he was knowingly in posses-sion of a controlled substance.
Analysis: Based only on the facts we are told in the Court of Appeals’ opinion, Steven got the short shrift of justice. There was no obvious evidence that he knew he was in possession of a controlled substance. Rather, the evidence showed that he was caught in pos-session of five pills that turned out to be a controlled substance. Maybe that is splitting hairs, but it seems to be a significant distinc-tion. Of course, we were not in the courtroom and have no way to judge the credibility of the testi-mony of Steven or Mamie. Maybe 26-year-old men in Indianapolis are presumed to know what hydro-codone is and that the drug is a controlled substance. Maybe Steven was going to use the pills himself, share them with the friend in the car that night, or try to sell them. A very unscientific search of Inter-net sites (search “street price of hydrocodone”) reveals that each pill of hydrocodone sells for between $5 and $10—not much of a get-rich-quick scheme for a 26-year-old vehicleless man who lives with his
38 Law 3_1sc.indd 3938 Law 3_1sc.indd 39 3/2/10 9:46 AM3/2/10 9:46 AM
40U.S. Pharmacist • March 2010 • www.uspharmacist.com
A PRESCRIPTION FOR CAR TROUBLE
grandmother. The only good thing to come out of this case it that Ste-ven probably learned a very valu-able lesson by taking his case up the justice system to the Indiana Court of Appeals—never leave drugs in your backpack. Hopefully, he learned not to drive on a sus-pended license as well.
Case 2: A Pharmacist’s Loose PillsA Michigan pharmacist was con-victed of possession of a controlled substance, operating a vehicle while visibly impaired, and posses-sion of a firearm while under the influence of intoxicants. The guilty verdict was upheld by the Michigan Court of Appeals.5
At approximately 2 am on a rainy night in the summer, the passenger-side front end of the Jeep driven by the pharmacist col-lided with the driver’s-side back door of another car as it was going through an intersection on the border between Detroit and an adjacent suburb. The victim testi-fied she was driving about 20 miles per hour (mph) because of the rain and dense fog when she entered the intersection with the right of way. She estimated the pharmacist’s vehicle was traveling 45 to 50 mph. After the collision, the pharmacist exited his Jeep and approached the other driver, ask-ing why she had stopped in the middle of the road. She responded that she had not stopped.
When the police arrived at the scene of the accident, one officer noticed alcohol on the pharma-cist’s breath. At no time during the investigation did he ever com-municate to the police that he was a licensed pharmacist or that he owned his own pharmacy. The pharmacist denied that he had been drinking and said that he
was just tired. Believing he may have been intoxicated by some-thing other than alcohol, the police issued a citation for reckless driving and put him into a police car to arrange other transportation for him. While sitting in the back of the police car, the pharmacist told the officers that he had a con-cealed weapon permit and that there were two handguns in his vehicle. The police found one loaded gun in the center console of the front seat and another one in a locked safe under the passen-ger seat. While searching the cen-ter console an officer also found seven pills of different colors and shapes without any prescription or other vials to contain them.
The officer put the pills into evidence bags, returned to the police car, told the pharmacist about the pills they had found, and read him his “chemical rights.” He refused to have his blood drawn. The officers obtained a warrant to have a blood sample taken, and the phar-macist was transported to a local hospital. The search of the vehicle and arrest of the pharmacist took place at approximately 2 am, and his blood was drawn at 6 am.
Two white pills were later identified as Tylenol #4. The other pills were carisoprodol (Soma), trazodone, sildenafil (Viagra), diazepam (Valium), and alprazolam (Xanax). A warrant was obtained to take a blood sample from the pharmacist. The blood sample revealed significant amounts of alcohol, alprazolam, diazepam, carisoprodol codeine, paroxetine (Paxil), fluoxetine (Prozac), lidocaine, and the codeine metabolite norcodeine in his system.
The pharmacist was charged with possession of a controlled
substance (codeine) and possession of a firearm while under the influ-ence of intoxicants.6,7 He was not charged with the illegal possession of diazepam, alprazolam, or any of the other drugs found in his vehi-cle or identified in his blood.
The pharmacist testified that he had worked at his pharmacy the day of the accident and that he had been home for about 5 hours without consuming any alcohol or medications. He left his home at 11 pm to go to a bachelor party at a strip club in Detroit and arrived about midnight. He denied taking any pills at the party but admitted to having two cups of punch laced with alcohol and a half bottle of beer. He left the party about 2 am and did not feel lightheaded or intoxicated. He also testified that when he saw the other car in the intersection he slammed on the brakes but began skidding until the collision occurred.
He claimed he had no idea how the pills got into his car. He pos-tulated that a friend he drove to a kidney dialysis center might have put the pills into the center con-sole. That friend admitted carry-ing Tylenol with codeine with him on occasion, but it was always in a labeled vial. He never carried or took diazepam or alprazolam. The pharmacist also noted that his vehicle was driven by several other people and was used to deliver prescriptions to patient homes.
An officer from the state police laboratory testified that she could tell from the blood sample and tests performed on the pills found in the vehicle that the pharmacist was under the influence of intoxi-cants at the time of the accident. The pharmacist argued that it was a procedural error to admit this expert testimony because it unfairly told the jury that he was
38 Law 3_1sc.indd 4038 Law 3_1sc.indd 40 3/2/10 9:46 AM3/2/10 9:46 AM

A PRESCRIPTION FOR CAR TROUBLE
Want
FastCold Sore Healing?
Speed healing. Recommend Abreva.For more information visit www.abrevapharmacist.com
infected cells
protected cells
It’s one thing for an OTC cold sore remedy to say it heals fast. Being able to back it up is quite another.
Only Abreva is FDA-approved to shorten healing time. 1
Only Abreva has a unique “Viral Entry Blocking” mode-of-action. 2
Only Abreva inhibits the virus from entering healthy cells. The virus needs to enter a cell to reproduce. 2*
#1 pharmacist recommended. 3,4
Recommend
The Abreva Diff erence.
* Based on laboratory studies (1) Sacks SL et al. Clinical effi cacy of topical docosanol 10% cream for herpes simplex labialis: a multicenter, randomized, placebo-controlled trial. J Am Acad Dermatol. 2001; 45:222-230. (2) Pope LE et al. Anti-herpes simplex virus activity of n-docosanol correlates with intracellular metabolic conversion of the drug. Jnl Lipid Research V27, Issue 10, 1996: 2167-2178. (3) Pharmacy Times OTC Recommendation Survey 2009 (4) Pharmacy Today Annual OTC Product Survey 2010
© 2010 GlaxoSmithKline Consumer Healthcare
Early treatment with Abreva ensures best results. If a cold sore lasts for more than 10 days, you should encourage your patient to see their physician.
proproproprorop tectectecteddtedtede c ceceellsssllsllprotected cells
guilty of the crimes charged. The trial court judge and the Michigan Court of Appeals disagreed.
The pharmacist was sentenced to 18 months of probation run-ning concurrently on each count of his convictions. His appeal to the Michigan Supreme Court was denied, thereby letting his convic-tions stand.8
At the time of this writing, the online Michigan Board of Phar-macy license verification database did not indicate that there was an open or pending formal complaint or any disciplinary action taken against the pharmacist based on his criminal conviction of posses-
sion of a controlled substance.9 Knowingly possessing a controlled substance in Michigan without legal authority is a criminal felony for which a pharmacist’s license can be sanctioned.10
Analysis: Pharmacists are not above the law just because we carry licenses for controlled sub-stances. Unlawful possession of these medications can result in criminal penalties as well as administrative discipline. As dem-onstrated by this case, trying to pass the buck to someone else you allow to use your vehicle will not be a very useful defense. As health
care professionals, pharmacists are held to the highest standards of care. Feigned ignorance will not excuse responsibility or liability.
Both of these stories should serve as reminders to think about what might be in your vehicle before you get behind the wheel. Unintentional or forgotten posses-sion of a controlled substance, once discovered by the authorities, will be treated seriously, with the very real possibility of criminal fel-ony charges. Excuses as to how the drugs got into your car will gener-ally not be considered a valid defense to the charges. Be aware, and take care before you drive.
REFERENCES1. Matheny v. Indiana, Slip Op No 49A02-0904-CR-358 (January 11, 2010), IN Ct App.2. IN Code § 35-48-7(a).3. IN Code § 35-48-7-7.4. IN Code § 35-48-1-27.5. Michigan v. Bacon, Slip Op No 282833 (May 21,
2009), 2009 Mich App Lexis 1116.6. MCL§ 333.7403(2)(b)(ii).7. MCL § 750.237(1)(a).8. Michigan v. Bacon, 772 NW2d 690; 2009 Mich Lexis 2533.9. Verify a license/registration. Michigan Department of Community Health. http://www.dleg.state.mi.us/
free/publicinfo.asp?rb_name=ON&rb_facility=&l_person_id=529811&l_profession_id=53&l_license_id=1766174&Last_Name=BACON&First_Name=RAUL&License_number=&Facility_Name=&DBA_Name=&profession=53&offset=0. Accessed February 7, 2010.10. MCL § 333.7403.
38 Law 3_1sc.indd 4138 Law 3_1sc.indd 41 3/2/10 9:46 AM3/2/10 9:46 AM

42U.S. Pharmacist • March 2010 • www.uspharmacist.com
Contemporary Compounding
●FORMULA
Rx: Ingredient 000 mg
Ingredient 000 mg Ingredient 000 mg Ingredient 000 mg Ingredient 000 mg
Method of Preparation: Calculate the quantity of each ingredient for the amount to be prepared. Accu-rately weigh or measure each ingredi-ent. Reconstitute the cyclophospha-mide for injection with the 0.9% Sodium Chloride Injection. Place the mixture in an appropriate graduate, add sufficient Ora-Plus or simple syrup to final volume, and mix well.
Use: Cyclophosphamide oral liquid is used in the treatment of many adult and pediatric malignancies.
Packaging: Package in tight, light-resistant containers.
Labeling: Keep out of the reach of children. Shake well. Store in a refrigerator. Discard after 56 days.1,2
Stability: A beyond-use date of 56 days can be used for this preparation only when it is stored in a refrigera-tor.1,2 The reported stability study used the injection as the source of the drug.
Quality Control: Quality-control assessment can include weight/vol-ume, pH, specific gravity, active
drug assay, color, rheologic proper-ties/pourability, physical observation, and physical stability (discoloration, foreign materials, gas formation, mold growth).3
Discussion: Cyclophosphamide is a widely used chemotherapeutic drug for treating a broad range of malig-nancies. It is used in the treatment of Hodgkin’s disease, non-Hodgkin’s lymphoma, multiple myeloma, leu-kemias, cutaneous T-cell lymphoma, neuroblastoma, ovarian cancer, reti-noblastoma, breast cancer, small-cell lung cancer, sarcomas, and other dis-eases. A former method of preparing an oral liquid involved the use of Aromatic Elixir USP and had a reported stability of 14 days. How-ever, Aromatic Elixir USP is no lon-ger commercially available and takes time to prepare, so the current for-mula is presented with a beyond-use date of 56 days when it is stored in a refrigerator.1
It should be noted that storage at room temperature resulted in 10% degradation of the drug in 10.6 days in simple syrup and in 6.0 days in Ora-Plus. Therefore, this preparation must be refrigerated.
Cyclophosphamide (C7H15Cl2N2O2P.H2O, MW 279.10) is a nitrogen mustard deriv-
ative that is used as an antineoplastic and immunosuppressant. It occurs as a white, crystalline powder that liq-uefies upon the loss of its water of crystallization. Cyclophosphamide is soluble in water and in alcohol.1
0.9% Sodium Chloride Injection contains not less than 95.0% and not more than 105.0% of the labeled amount of sodium chloride in water for injection. It has a pH between 4.5 and 7.0, and it contains no added antimicrobial agents. Sodium chloride solutions are chem-ically and physically stable. They can be sterilized by filtration or autoclav-ing. Aqueous sodium chloride solu-tions will react to form precipitates with silver, lead, and mercury salts. When acidified sodium chloride solutions are mixed with strong oxi-dizing agents, chlorine can be liber-ated. Sodium chloride will decrease the solubility of some organic com-pounds; methylparaben is not as sol-uble in sodium chloride solutions as it is in water. Sodium chloride is sol-uble in water to the extent of 1 g in 2.8 mL water, and it is slightly solu-ble in alcohol (1 g in 250 mL of 95% ethanol).4
Ora-Plus is an oral suspending vehicle that accepts dilution of up to 50% or more with water, flavor-ing agents, or syrups and still retains its suspending properties. It has a pH of approximately 4.2 and an osmolality of about 230 mOsm/kg. Ora-Plus is a thixotropic vehicle with a viscosity of approximately 1,000 cps at 25˚C. It contains puri-fied water, microcrystalline cellulose, sodium carboxymethylcellulose,
Loyd V. Allen, Jr, PhDProfessor Emeritus, College of Pharmacy, University of Oklahoma, Oklahoma City
Cyclophosphamide 10-mg/mL Oral LiquidThis chemotherapeutic agent is formulated without
Aromatic Elixir USP, which is not available commercially and is time-consuming to prepare.
●FORMULA
Cyclophosphamide 10-mg/mL Oral Liquid
Rx: Ingredient
Cyclophosphamide 1 g 0.9% Sodium Chloride Injection 50 mL Ora-Plus or simple syrup qs 100 mL
42 Compound 3_1mb.indd 4242 Compound 3_1mb.indd 42 3/2/10 9:47 AM3/2/10 9:47 AM

xanthan gum, carrageenan, sodium phosphate, and citric acid as buffer-ing agents; simethicone as an anti-foaming agent; and potassium sor-bate and methylparaben as preservatives.5
Syrup (simple syrup) is a clear,
sweet vehicle used as a sweetening agent and as the base for many fla-vored and medicated syrups. It con-tains 85% w/v sucrose in water and has a specific gravity of not less than 1.30. Simple syrup is generally self-preserving as long as the sucrose
concentration is maintained suffi-ciently high. Preferably, it is pre-pared without the use of heat, but it can be prepared by the use of boil-ing water. Simple syrup should be stored in tight containers, preferably in a cool place.1
Contemporary Compounding
REFERENCES1. USP Pharmacists’ Pharmacopeia. Rockville, MD: US Pharmacopeial Convention, Inc; 2005:388,775-779,1433.2. Kennedy R, Groepper D, Tagen M, et al. Stability of cyclophosphamide in extemporaneous oral suspensions.
Ann Pharmacother. 2010;44:295-301.3. Allen LV Jr. Standard operating procedure for perform-ing physical quality assessment of oral and topical liquids. IJPC. 1999;3:146-147.4. Maximilien JS. Sodium chloride. In: Rowe RC, Sheskey
PJ, Quinn ME, eds. Handbook of Pharmaceutical Excipi-ents. 6th ed. London, England: Pharmaceutical Press; 2009:637-640.5. Ora-Plus (product information). Minneapolis, MN: Paddock Laboratories, Inc; 1992.
CURRENT TOPICSPediatric Accidental Ingestions
The Treatment and Management ofAtrial Fibrillation
Update on Guillain-Barré Syndrome
Law CE—Prescription Drug Abuse: Strategies to Reduce Diversion
Emergency Contraception: An Updateof Clinical and Regulatory Changes*
Ovarian Cancer: A CommonGynecologic Malignancy
Perimenopause: Management of Common Symptoms
The Role of the Pharmacist in Educating and Counseling Patientson Contact Lens Care*
An Update on the Current Treatment of HIV
Treatment Options in Acute Lung Injury and Acute Respiratory Distress Syndrome
*Free of charge
Earn CE Credits Online!Visit www.uspharmacist.com
42 Compound 3_1mb.indd 4342 Compound 3_1mb.indd 43 3/2/10 9:47 AM3/2/10 9:47 AM
44U.S. Pharmacist • March 2010 • www.uspharmacist.com
Otitis media (OM) is a common illness affecting both infants and children, often multiple times during the first few years of life. Approximately
16 million office visits and 13 million antibiotic pre-scriptions during the year 2000 were associated with OM.1 OM has many degrees of severity, including acute OM (AOM), OM with effusion (OME), and chronic suppurative OM (CSOM).
AOM is one of the most frequently occurring child-hood diseases, second to upper respiratory infections. It is the leading cause of physician visits, antimicrobial therapy, and pediatric surgery in several countries.2 In the United States, AOM is diagnosed more than 5 mil-lion times annually.3 Although AOM can occur in adults, approximately 80% of cases occur in children, with the greatest incidence occurring in those aged 6 to 9 months. By 1 year of age, an estimated 75% of infants will have encountered one episode of AOM, while 17% will have suffered from at least three episodes.2
AOM develops after bacteria invade the middle ear. Factors leading to this invasion include nasopharyngeal colonization, upper respiratory tract infections, and eustachian tube dysfunction.4 After viral respiratory tract infections, ciliary activity in respiratory mucosal cells may be impaired, leading to decreased protection from invading organisms. The eustachian tubes of children aged less than 2 years are shorter than in older children, result-ing in shorter distances for bacteria to travel and increasing the probabil-ity of infection.2 Additionally, the opening mechanism of the eustachian
tubes may be impaired in infants and young children. Furthermore, genetic, infectious, immunologic, and environmental factors can predispose children to ear infections (TABLE 1).5,6
A clinical-practice guideline for the diagnosis and management of AOM was developed by the American Academy of Pediatrics and the American Academy of Family Physicians (AAP/AAFP). According to this guideline, for a diagnosis to be considered “certain,” three specific criteria need to be met: rapid onset, confirmed presence of middle-ear effusion (MEE), and signs and symptoms of middle-ear inflammation. Signs and symptoms of middle-ear inflammation may be indicated by either distinct erythema of the tympanic membrane or distinct otalgia. In infants, pulling of the ear is often indicative of otalgia. Other signs and symp-toms pediatric patients may present with, although not specific to AOM, include irritability in infants or tod-dlers, discharge from the ear, and fever. The presence of MEE is indicated by bulging of the tympanic mem-brane (the best predictor of AOM), limited or absent mobility of the tympanic membrane, air-fluid level behind the tympanic membrane, or otorrhea.7
AOM can progress to either persistent AOM or recurrent AOM. Persistent AOM occurs when there are persistent features of a middle-ear infection during antibi-otic treatment or when a relapse occurs within 1 month of completion of therapy. If a child experiences three or more episodes of AOM within 6 to 18 months, the diagnosis of recur-rent AOM should be made.5
Ann McMahon Wicker, PharmD, BCPSAssistant Professor
University of Louisiana at Monroe College of Pharmacy
Baton Rouge, Louisiana
Brice Labruzzo Mohundro, PharmDAssistant Professor
University of Louisiana at Monroe College of Pharmacy
Baton Rouge, Louisiana
Management of Pediatric Otitis Media
© THINKSTOCK
44 Otitis Media 3_1sc.indd 4444 Otitis Media 3_1sc.indd 44 3/2/10 9:52 AM3/2/10 9:52 AM

47U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC OTITIS MEDIA
OME, or secretory OM, is characterized by fluid in the middle ear without signs or symptoms of infection. It usually occurs when the eustachian tube is blocked and fluid becomes trapped in the middle ear.8 OME may occur spontaneously as part of rhinosinusitis (inflam-mation of the nasal cavity and sinuses), or it may suc-ceed a bout of AOM.9 Approximately 90% of cases occur in children, with the greatest incidence taking place between 6 months and 4 years of age.10
CSOM, the severest form of OM, is usually a com-plication of AOM.9,11 A persistent inflammation of the middle-ear cavity or mastoid air cells, CSOM is char-acterized by a discharge through a perforated tympanic membrane.5 The condition usually is present for more than 2 to 6 weeks.9
MicrobiologyStreptococcus pneumoniae, Haemophilus influenzae, and Moraxella catarrhalis are the most common pathogens isolated from AOM, according to studies.5,7 When middle-ear fluid was examined, S pneumoniae, H influ-enzae, and M catarrhalis were found 25% to 35%, 15% to 30%, and 3% to 20% of the time, respectively.7 Evidence suggests that microbiology may be changing owing to routine vaccination with the heptavalent pneumococcal vaccine; research revealed an increase in H influenzae isolates from 39% to 52% in children aged 7 to 24 months and a decrease in S pneumoniae from 49% to 34% between 1992 and 1998 and between 2000 and 2003.7 Although rare, other pathogens that may be present in AOM include group A streptococ-cus (GAS), Staphylococcus aureus, anaerobic organisms, Gram-negative bacilli, viruses, Mycoplasma pneumoniae, Chlamydia pneumoniae, and Chlamydia trachomatis (in
infants <6 months). S pneumoniae, H influenzae, M catarrhalis, GAS, and S aureus also are responsible for recurrent and persistent OM.7 The bacterial pathogens associated with OME are the same as those seen in AOM. In CSOM, however, Pseudomonas aeruginosa, S aureus, Proteus mirabilis, and Klebsiella species are the most common pathogens isolated, and mixed infections are common. It is important to note that multidrug antibiotic resistance is common with Pseu-domonas infections.5,9
Traditional Pharmacologic TherapySymptom resolution and reduction of recurrence are the goals of treatment for AOM. Analgesics in addition to oral and topical antimicrobials are the mainstay of treatment. The use of antibacterial agents in children with uncomplicated AOM at the time of diagnosis has raised concerns regarding antibacterial resistance; how-ever, AOM is the most common childhood infection for which antibacterial agents are prescribed in the U.S.7 Antihistamines and decongestants may help relieve nasal allergies and congestion, but they have not been shown to improve healing or reduce the complications of AOM.5 Dosing of analgesics and oral antibiotic agents in pediatric patients is based on weight (kg). Recom-mended dosing ranges are given in TABLE 2.
Since episodes of AOM frequently are associated with pain, the use of analgesics—especially during the first 24 hours of an episode—are strongly recommended by the AAP/AAFP guidelines. Treatment options to reduce the pain associated with otalgia include acet-aminophen, ibuprofen, and antipyrine/benzocaine otic solution.7 Antipyrine/benzocaine otic solution is a prescription product used for its local analgesic proper-ties. After the solution is instilled into the ear canal, relief of ear pain occurs in approximately 30 minutes. This product is for otic use only, and it should not be used if the solution is brown or contains a precipitate. Disposal of the bottle is recommended 6 months after the dropper is placed in the solution.12
Treatment with an antibacterial agent is recommended for children younger than 6 months of age, children aged 6 months to 2 years with a certain diagnosis of AOM, and any child with moderate-to-severe otalgia or a fever of 102.2°F (39°C) or greater. Observation without antibacterial treatment may be considered for healthy children aged 6 months to 2 years with nonse-vere illness and an uncertain diagnosis, as well as for children older than 2 years without severe symptoms or with an uncertain diagnosis for 48 to 72 hours; however, appropriate measures should be taken to allow caregiver–physician communication, reevaluation, and
Table 1. Risk Factors for OMMale gender
Early onset of AOM (age 6-24 mo)
Sibling history
Formula-feeding in infancy
Day care attendancea
Ethnicity (Native American, Alaskan, Canadian Inuit)a
Exposure to cigarette smoke
Pacifier use
Underlying pathology (allergic rhinitis, cleft palate, Down’s syndrome)a
Fall and/or winter seasona
Previous antibiotic usea
Previous OMa
a Also increases the risk of recurrent OM.AOM: acute OM.Source: References 5, 6.
44 REVOtitis Media 3_1sc.indd 4744 REVOtitis Media 3_1sc.indd 47 3/2/10 1:42 PM3/2/10 1:42 PM
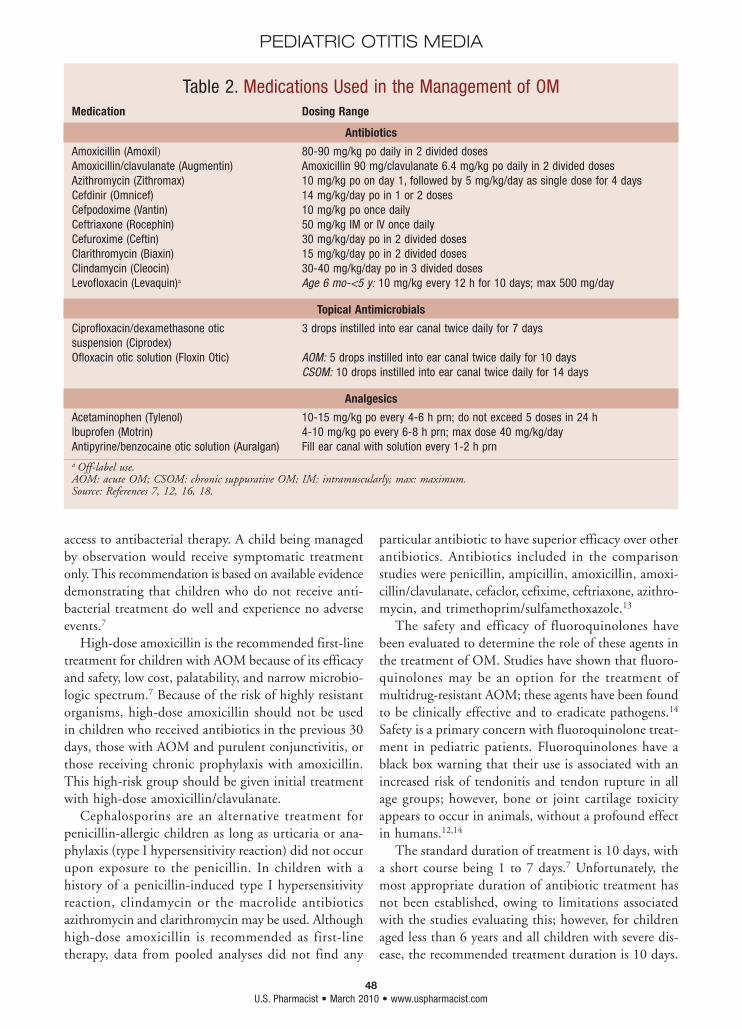
48U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC OTITIS MEDIA
access to antibacterial therapy. A child being managed by observation would receive symptomatic treatment only. This recommendation is based on available evidence demonstrating that children who do not receive anti-bacterial treatment do well and experience no adverse events.7
High-dose amoxicillin is the recommended first-line treatment for children with AOM because of its efficacy and safety, low cost, palatability, and narrow microbio-logic spectrum.7 Because of the risk of highly resistant organisms, high-dose amoxicillin should not be used in children who received antibiotics in the previous 30 days, those with AOM and purulent conjunctivitis, or those receiving chronic prophylaxis with amoxicillin. This high-risk group should be given initial treatment with high-dose amoxicillin/clavulanate.
Cephalosporins are an alternative treatment for penicillin-allergic children as long as urticaria or ana-phylaxis (type I hypersensitivity reaction) did not occur upon exposure to the penicillin. In children with a history of a penicillin-induced type I hypersensitivity reaction, clindamycin or the macrolide antibiotics azithromycin and clarithromycin may be used. Although high-dose amoxicillin is recommended as first-line therapy, data from pooled analyses did not find any
particular antibiotic to have superior efficacy over other antibiotics. Antibiotics included in the comparison studies were penicillin, ampicillin, amoxicillin, amoxi-cillin/clavulanate, cefaclor, cefixime, ceftriaxone, azithro-mycin, and trimethoprim/sulfamethoxazole.13
The safety and efficacy of fluoroquinolones have been evaluated to determine the role of these agents in the treatment of OM. Studies have shown that fluoro-quinolones may be an option for the treatment of multidrug-resistant AOM; these agents have been found to be clinically effective and to eradicate pathogens.14 Safety is a primary concern with fluoroquinolone treat-ment in pediatric patients. Fluoroquinolones have a black box warning that their use is associated with an increased risk of tendonitis and tendon rupture in all age groups; however, bone or joint cartilage toxicity appears to occur in animals, without a profound effect in humans.12,14
The standard duration of treatment is 10 days, with a short course being 1 to 7 days.7 Unfortunately, the most appropriate duration of antibiotic treatment has not been established, owing to limitations associated with the studies evaluating this; however, for children aged less than 6 years and all children with severe dis-ease, the recommended treatment duration is 10 days.
Table 2. Medications Used in the Management of OMMedication Dosing Range
Antibiotics
Amoxicillin (Amoxil) 80-90 mg/kg po daily in 2 divided dosesAmoxicillin/clavulanate (Augmentin) Amoxicillin 90 mg/clavulanate 6.4 mg/kg po daily in 2 divided dosesAzithromycin (Zithromax) 10 mg/kg po on day 1, followed by 5 mg/kg/day as single dose for 4 daysCefdinir (Omnicef) 14 mg/kg/day po in 1 or 2 dosesCefpodoxime (Vantin) 10 mg/kg po once dailyCeftriaxone (Rocephin) 50 mg/kg IM or IV once dailyCefuroxime (Ceftin) 30 mg/kg/day po in 2 divided dosesClarithromycin (Biaxin) 15 mg/kg/day po in 2 divided dosesClindamycin (Cleocin) 30-40 mg/kg/day po in 3 divided dosesLevofloxacin (Levaquin)a Age 6 mo-<5 y: 10 mg/kg every 12 h for 10 days; max 500 mg/day
Topical Antimicrobials
Ciprofloxacin/dexamethasone otic 3 drops instilled into ear canal twice daily for 7 dayssuspension (Ciprodex) Ofloxacin otic solution (Floxin Otic) AOM: 5 drops instilled into ear canal twice daily for 10 days CSOM: 10 drops instilled into ear canal twice daily for 14 days
Analgesics
Acetaminophen (Tylenol) 10-15 mg/kg po every 4-6 h prn; do not exceed 5 doses in 24 hIbuprofen (Motrin) 4-10 mg/kg po every 6-8 h prn; max dose 40 mg/kg/dayAntipyrine/benzocaine otic solution (Auralgan) Fill ear canal with solution every 1-2 h prna Off-label use.AOM: acute OM; CSOM: chronic suppurative OM; IM: intramuscularly; max: maximum.Source: References 7, 12, 16, 18.
44 Otitis Media 3_1sc.indd 4844 Otitis Media 3_1sc.indd 48 3/2/10 9:52 AM3/2/10 9:52 AM
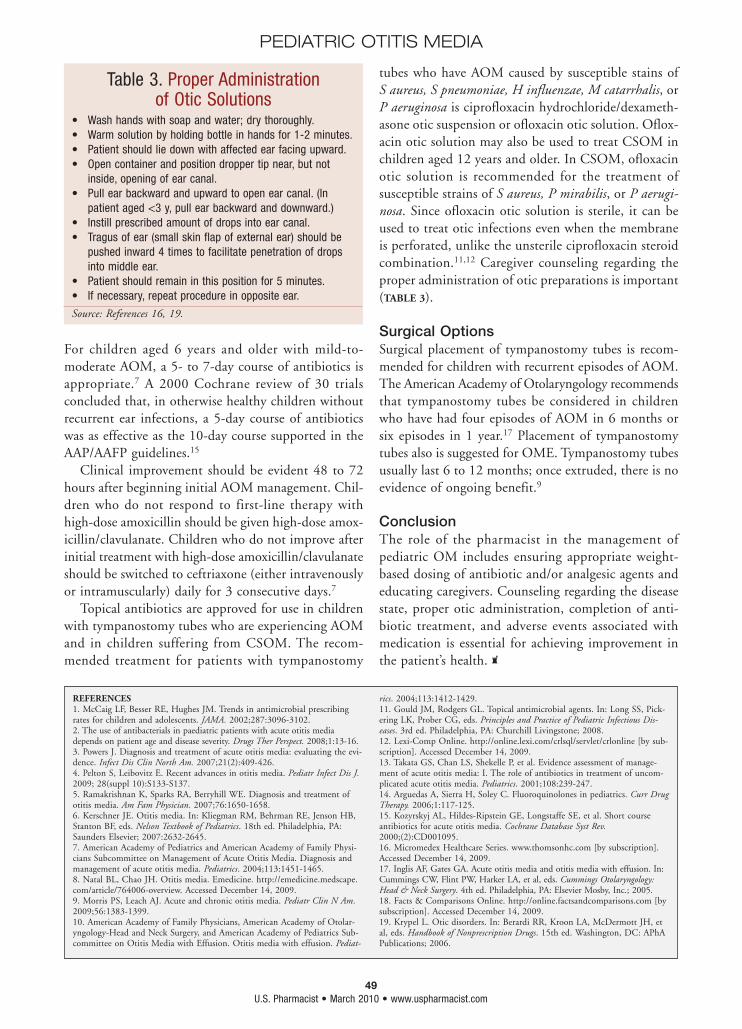
49U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC OTITIS MEDIA
For children aged 6 years and older with mild-to-moderate AOM, a 5- to 7-day course of antibiotics is appropriate.7 A 2000 Cochrane review of 30 trials concluded that, in otherwise healthy children without recurrent ear infections, a 5-day course of antibiotics was as effective as the 10-day course supported in the AAP/AAFP guidelines.15
Clinical improvement should be evident 48 to 72 hours after beginning initial AOM management. Chil-dren who do not respond to first-line therapy with high-dose amoxicillin should be given high-dose amox-icillin/clavulanate. Children who do not improve after initial treatment with high-dose amoxicillin/clavulanate should be switched to ceftriaxone (either intravenously or intramuscularly) daily for 3 consecutive days.7
Topical antibiotics are approved for use in children with tympanostomy tubes who are experiencing AOM and in children suffering from CSOM. The recom-mended treatment for patients with tympanostomy
tubes who have AOM caused by susceptible stains of S aureus, S pneumoniae, H influenzae, M catarrhalis, or P aeruginosa is ciprofloxacin hydrochloride/dexameth-asone otic suspension or ofloxacin otic solution. Oflox-acin otic solution may also be used to treat CSOM in children aged 12 years and older. In CSOM, ofloxacin otic solution is recommended for the treatment of susceptible strains of S aureus, P mirabilis, or P aerugi-nosa. Since ofloxacin otic solution is sterile, it can be used to treat otic infections even when the membrane is perforated, unlike the unsterile ciprofloxacin steroid combination.11,12 Caregiver counseling regarding the proper administration of otic preparations is important (TABLE 3).
Surgical OptionsSurgical placement of tympanostomy tubes is recom-mended for children with recurrent episodes of AOM. The American Academy of Otolaryngology recommends that tympanostomy tubes be considered in children who have had four episodes of AOM in 6 months or six episodes in 1 year.17 Placement of tympanostomy tubes also is suggested for OME. Tympanostomy tubes usually last 6 to 12 months; once extruded, there is no evidence of ongoing benefit.9
ConclusionThe role of the pharmacist in the management of pediatric OM includes ensuring appropriate weight-based dosing of antibiotic and/or analgesic agents and educating caregivers. Counseling regarding the disease state, proper otic administration, completion of anti-biotic treatment, and adverse events associated with medication is essential for achieving improvement in the patient’s health.
REFERENCES1. McCaig LF, Besser RE, Hughes JM. Trends in antimicrobial prescribing rates for children and adolescents. JAMA. 2002;287:3096-3102.2. The use of antibacterials in paediatric patients with acute otitis media depends on patient age and disease severity. Drugs Ther Perspect. 2008;1:13-16.3. Powers J. Diagnosis and treatment of acute otitis media: evaluating the evi-dence. Infect Dis Clin North Am. 2007;21(2):409-426.4. Pelton S, Leibovitz E. Recent advances in otitis media. Pediatr Infect Dis J. 2009; 28(suppl 10):S133-S137.5. Ramakrishnan K, Sparks RA, Berryhill WE. Diagnosis and treatment of otitis media. Am Fam Physician. 2007;76:1650-1658.6. Kerschner JE. Otitis media. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics. 18th ed. Philadelphia, PA: Saunders Elsevier; 2007:2632-2645.7. American Academy of Pediatrics and American Academy of Family Physi-cians Subcommittee on Management of Acute Otitis Media. Diagnosis and management of acute otitis media. Pediatrics. 2004;113:1451-1465.8. Natal BL, Chao JH. Otitis media. Emedicine. http://emedicine.medscape.com/article/764006-overview. Accessed December 14, 2009.9. Morris PS, Leach AJ. Acute and chronic otitis media. Pediatr Clin N Am. 2009;56:1383-1399.10. American Academy of Family Physicians, American Academy of Otolar-yngology-Head and Neck Surgery, and American Academy of Pediatrics Sub-committee on Otitis Media with Effusion. Otitis media with effusion. Pediat-
rics. 2004;113:1412-1429.11. Gould JM, Rodgers GL. Topical antimicrobial agents. In: Long SS, Pick-ering LK, Prober CG, eds. Principles and Practice of Pediatric Infectious Dis-eases. 3rd ed. Philadelphia, PA: Churchill Livingstone; 2008.12. Lexi-Comp Online. http://online.lexi.com/crlsql/servlet/crlonline [by sub-scription]. Accessed December 14, 2009.13. Takata GS, Chan LS, Shekelle P, et al. Evidence assessment of manage-ment of acute otitis media: I. The role of antibiotics in treatment of uncom-plicated acute otitis media. Pediatrics. 2001;108:239-247.14. Arguedas A, Sierra H, Soley C. Fluoroquinolones in pediatrics. Curr Drug Therapy. 2006;1:117-125.15. Kozyrskyj AL, Hildes-Ripstein GE, Longstaffe SE, et al. Short course antibiotics for acute otitis media. Cochrane Database Syst Rev. 2000;(2):CD001095.16. Micromedex Healthcare Series. www.thomsonhc.com [by subscription]. Accessed December 14, 2009.17. Inglis AF, Gates GA. Acute otitis media and otitis media with effusion. In: Cummings CW, Flint PW, Harker LA, et al, eds. Cummings Otolaryngology: Head & Neck Surgery. 4th ed. Philadelphia, PA: Elsevier Mosby, Inc.; 2005.18. Facts & Comparisons Online. http://online.factsandcomparisons.com [by subscription]. Accessed December 14, 2009.19. Krypel L. Otic disorders. In: Berardi RR, Kroon LA, McDermott JH, et al, eds. Handbook of Nonprescription Drugs. 15th ed. Washington, DC: APhA Publications; 2006.
Table 3. Proper Administration of Otic Solutions
• Wash hands with soap and water; dry thoroughly.• Warm solution by holding bottle in hands for 1-2 minutes.• Patient should lie down with affected ear facing upward.• Open container and position dropper tip near, but not
inside, opening of ear canal.• Pull ear backward and upward to open ear canal. (In
patient aged <3 y, pull ear backward and downward.)• Instill prescribed amount of drops into ear canal.• Tragus of ear (small skin flap of external ear) should be
pushed inward 4 times to facilitate penetration of drops into middle ear.
• Patient should remain in this position for 5 minutes.• If necessary, repeat procedure in opposite ear.
Source: References 16, 19.
44 Otitis Media 3_1sc.indd 4944 Otitis Media 3_1sc.indd 49 3/2/10 9:52 AM3/2/10 9:52 AM
Project2 4/28/08 1:59 PM Page 1
51U.S. Pharmacist • March 2010 • www.uspharmacist.com
2 CE Credits
Accidental ingestions are unfortunate common occurrences in children.
Despite efforts to increase aware-ness and prevention, the rates of unintentional ingestions reported by the American Asso-ciation of Poison Control Cen-ters (AAPCC) have remained stable since the early 1990s.1
When natural curiosity is com-bined with unprotected access to medications and household agents, young children are extremely susceptible to toxic ingestions. According to the 2007 annual report of the AAPCC, 61% of the 1 million reported human exposures in children younger than 6 years were unintentional ingestions.2 Fatalities claimed the lives of 13 children in this age group.2 Notably, the overwhelm-ing majority of exposures are not lethal; however, prevent-able fatalities are tragic. Historically, the top offenders for accidental ingestions in children include household sub-stances, OTC products, and prescription medications.
Household SubstancesCleaning Solutions: Cleaning solutions were the second most frequently ingested substances reported in children 5 years and younger.2 Alkaline materials (e.g., drain clean-ers, detergents) seem to be more frequently ingested than acidic solutions (e.g., bleach, toilet bowl cleaners).3 Although many patients (44%) remain asymptomatic, the most frequent symptom following ingestion of caustic substances is vomiting (39%).3 Excessive salivation, hematemesis, and coughing are among other reported symptoms.3 Initial management should include assessment of the airway and administration of supplemental oxygen, if necessary.4 Ingested substances should be diluted with water or milk as soon as possible unless the airway is compromised.4 Attempts to neutralize the substances using weakly acidic or alkaline solutions and to stimulate emesis are not recommended.4
Significant exposures can result in esophageal burns characterized by ery-
thema and ulceration within 24 hours of ingestion.4 In a large analysis of caustic-sub-stances ingestions, alkaline solutions were responsible for about 87% of esophageal burns.3 Dishwasher powders were deemed most dangerous, because 55% of exposed chil-dren developed esophageal burns.3 Esophageal strictures, potentially resulting in dys-
phagia and increased risk of aspiration, are the most wor-risome chronic complication following caustic ingestions. Strictures can develop over time and are a result of scar tissue formation.5 Corticosteroids have been studied for the prevention of esophageal strictures, but available evidence supporting their use and benefits is limited. However, their anti-inflammatory properties and potential for attenuation of granulation and fibrous tissue formation are protective mechanisms against stricture formation.5
Pesticides: Over 40,000 cases of pesticide ingestions were reported in children 5 years and younger in 2007.2 Organo-phosphates, commonly used as pesticides in homes, gardens, and farms, are irreversible cholinesterase inhibitors that cause high synaptic concentrations of acetylcholine, a potent neurotransmitter. The accumulation of acetylcholine leads to overstimulation and disturbances in the autonomic nervous system, neuromuscular junctions, and central nervous system (CNS).6
The most common manifestations demonstrated in a study of children with acute organophosphate poisoning were neurologic and gastrointestinal (GI), with the large majority of patients presenting with multisystem involve-ment.6 About 70% of patients presented with neurologic symptoms that included coma, seizure, agitation, areflexia,
and pinpoint pupils. Over 60% expe-rienced GI symptoms such as salivation or foaming, abdominal pain, vomiting, diarrhea, and pancreatitis. Cardiopul-monary symptoms and complications,
U.S. Pharmacist Continuing EducationGOAL: To raise awareness of pediatric accidental ingestions and review accompanying monitoring and treatment options.OBJECTIVES: After completing this activity, the participant should be able to:1. Discuss the prevalence of reported pediatric accidental ingestions of household chemicals and medications.*2. Identify agents that are commonly involved in accidental ingestions.*3. Review appropriate monitoring and treatment options for specific agents of pediatric exposures.*4. Describe published literature and predicted outcomes according to agent(s) involved.** Also applies to pharmacy technicians.
Pediatric Accidental IngestionsMonitoring and Treatment Options
Lela S. Fung, PharmD, BCPSClinical Pharmacy Specialist, Neonatology/
Pediatrics, Via Christi Regional Medical Center Wichita, Kansas; Adjunct Clinical Assistant Professor, University of Kansas School of
Pharmacy, Lawrence, Kansas
51 CE-Accidental 3_1bosc.indd 5151 CE-Accidental 3_1bosc.indd 51 3/2/10 9:53 AM3/2/10 9:53 AM

52U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
including tachycardia, prolonged QTc interval, pneumonia, and respiratory failure, occurred in about 52% of patients.6
Serum cholinesterase levels may be obtained but should not be used in determining acute management. Instead, the severity of clinical manifestations should guide treat-ment. Abnormal laboratory values may include elevated white blood cells, liver enzymes, l-lactate dehydrogenase, and blood glucose.6,7 These values may be obtained and monitored throughout the patient’s hospitalization, but again, observation of CNS manifestations should be the focus of determining progress.
Airway status and necessity for resuscitation should be evaluated immediately. Endotracheal intubation and mechanical ventilation may be necessary if there are exces-sive secretions or signs of decreased levels of consciousness or hemodynamic instability.7 Treatment for seizures and decontamination of the GI system by gastric lavage and activated charcoal should be initiated promptly. A summary of antidotes is listed in TABLE 1.
Administration of anticholinergic agents is recommended for symptomatic patients.4 Atropine competitively antago-nizes acetylcholine at the muscarinic synapses and relieves sweating, salivation, and lacrimation.8 Intermittent and continuous IV doses have been used.4,7-9 When administered intermittently, doses may be given every 5 to 20 minutes
until decreased secretions and com-fortable respirations have been observed (TABLE 1). Atropine should be continued for at least the first 24 hours.4,7 Pralidoxime (2-PAM) may be used in addition to atropine in cases of persistent muscle weakness with high atropine requirements.8 This antidote reactivates acetylcho-linesterase at the nicotinic synapses, which is phosphorylated and inac-tivated by ingested organophosphates. Upon adequate atropinization, 2-PAM may be initiated with repeated doses every 30 minutes to 2 hours if muscle weakness persists, and addi-tional doses at 8- to 12-hour intervals may be administered if cholinergic symptoms recur (TABLE 1).4,8,9
Obtaining an adequate exposure history, early diagnosis, and treatment are the keys to full clinical recovery. In a study conducted in adults and children, mechanical ventilation was required in 21.2% of patients, and 50% of those patients died.7 The overall mortality rate of ingestions
was 27.6%. Complications reported in this study included respiratory failure, aspiration pneumonia, urinary tract infection, convulsion, and septic shock.7 The average length of stay observed in children was 2.8 days.6
OTC ProductsCough and Cold Products: Over 65,000 cases of children 5 years old and younger ingesting cough and cold prepara-tions were reported to U.S. poison control centers in 2007.2 Due to safety concerns and lack of efficacy data in pediat-ric patients, the FDA has recommended that the use of OTC cough and cold products be prohibited in children younger than 6 years.10 Manufacturers of these products have also voluntarily removed preparations formulated for infants from the market. However, these initiatives do not prevent accidental ingestions of inappropriately stored products. Managing ingestion cases can be difficult since many of these products are combinations of agents that can lead to a variety of symptoms and complications.
Dextromethorphan is a cough suppressant that is sold as a single agent as well as in combination formulations. LoVecchio et al reviewed 304 cases of accidental dextro-methorphan ingestions that yielded relatively benign out-comes.11 The mean age for patients included in the study was 28 months, and the average dose of dextromethorphan
Although prescription medications are required by law to be dispensed in child-resistant packaging, thousands of accidental ingestions are reported every year.
© 2
010
Cyn
thia
Tur
ner
www.cynthiaturner.com
51 CE-Accidental 3_1bosc.indd 5251 CE-Accidental 3_1bosc.indd 52 3/2/10 9:53 AM3/2/10 9:53 AM
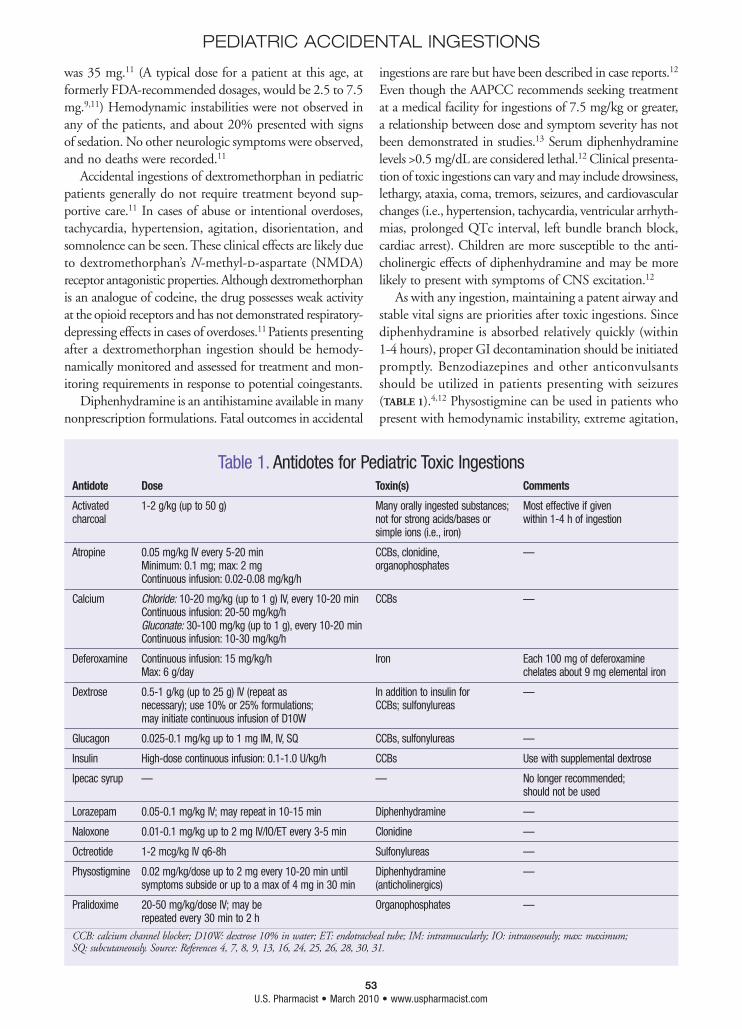
53U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
was 35 mg.11 (A typical dose for a patient at this age, at formerly FDA-recommended dosages, would be 2.5 to 7.5 mg.9,11) Hemodynamic instabilities were not observed in any of the patients, and about 20% presented with signs of sedation. No other neurologic symptoms were observed, and no deaths were recorded.11
Accidental ingestions of dextromethorphan in pediatric patients generally do not require treatment beyond sup-portive care.11 In cases of abuse or intentional overdoses, tachycardia, hypertension, agitation, disorientation, and somnolence can be seen. These clinical effects are likely due to dextromethorphan’s N-methyl-d-aspartate (NMDA) receptor antagonistic properties. Although dextromethorphan is an analogue of codeine, the drug possesses weak activity at the opioid receptors and has not demonstrated respiratory-depressing effects in cases of overdoses.11 Patients presenting after a dextromethorphan ingestion should be hemody-namically monitored and assessed for treatment and mon-itoring requirements in response to potential coingestants.
Diphenhydramine is an antihistamine available in many nonprescription formulations. Fatal outcomes in accidental
ingestions are rare but have been described in case reports.12 Even though the AAPCC recommends seeking treatment at a medical facility for ingestions of 7.5 mg/kg or greater, a relationship between dose and symptom severity has not been demonstrated in studies.13 Serum diphenhydramine levels >0.5 mg/dL are considered lethal.12 Clinical presenta-tion of toxic ingestions can vary and may include drowsiness, lethargy, ataxia, coma, tremors, seizures, and cardiovascular changes (i.e., hypertension, tachycardia, ventricular arrhyth-mias, prolonged QTc interval, left bundle branch block, cardiac arrest). Children are more susceptible to the anti-cholinergic effects of diphenhydramine and may be more likely to present with symptoms of CNS excitation.12
As with any ingestion, maintaining a patent airway and stable vital signs are priorities after toxic ingestions. Since diphenhydramine is absorbed relatively quickly (within 1-4 hours), proper GI decontamination should be initiated promptly. Benzodiazepines and other anticonvulsants should be utilized in patients presenting with seizures (TABLE 1).4,12 Physostigmine can be used in patients who present with hemodynamic instability, extreme agitation,
Table 1. Antidotes for Pediatric Toxic IngestionsAntidote Dose Toxin(s) Comments
Activated 1-2 g/kg (up to 50 g) Many orally ingested substances; Most effective if given charcoal not for strong acids/bases or within 1-4 h of ingestion simple ions (i.e., iron)
Atropine 0.05 mg/kg IV every 5-20 min CCBs, clonidine, — Minimum: 0.1 mg; max: 2 mg organophosphates Continuous infusion: 0.02-0.08 mg/kg/h
Calcium Chloride: 10-20 mg/kg (up to 1 g) IV, every 10-20 min CCBs — Continuous infusion: 20-50 mg/kg/h Gluconate: 30-100 mg/kg (up to 1 g), every 10-20 min Continuous infusion: 10-30 mg/kg/h
Deferoxamine Continuous infusion: 15 mg/kg/h Iron Each 100 mg of deferoxamine Max: 6 g/day chelates about 9 mg elemental iron
Dextrose 0.5-1 g/kg (up to 25 g) IV (repeat as In addition to insulin for — necessary); use 10% or 25% formulations; CCBs; sulfonylureas may initiate continuous infusion of D10W
Glucagon 0.025-0.1 mg/kg up to 1 mg IM, IV, SQ CCBs, sulfonylureas —
Insulin High-dose continuous infusion: 0.1-1.0 U/kg/h CCBs Use with supplemental dextrose
Ipecac syrup — — No longer recommended; should not be used
Lorazepam 0.05-0.1 mg/kg IV; may repeat in 10-15 min Diphenhydramine —
Naloxone 0.01-0.1 mg/kg up to 2 mg IV/IO/ET every 3-5 min Clonidine —
Octreotide 1-2 mcg/kg IV q6-8h Sulfonylureas —
Physostigmine 0.02 mg/kg/dose up to 2 mg every 10-20 min until Diphenhydramine — symptoms subside or up to a max of 4 mg in 30 min (anticholinergics)
Pralidoxime 20-50 mg/kg/dose IV; may be Organophosphates — repeated every 30 min to 2 h
CCB: calcium channel blocker; D10W: dextrose 10% in water; ET: endotracheal tube; IM: intramuscularly; IO: intraosseously; max: maximum; SQ: subcutaneously. Source: References 4, 7, 8, 9, 13, 16, 24, 25, 26, 28, 30, 31.
51 REVCE-Accidental 3_1bosc.indd 5351 REVCE-Accidental 3_1bosc.indd 53 3/2/10 1:39 PM3/2/10 1:39 PM

54U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
and other life-threatening symptoms. Physostigmine is a cholinesterase inhibitor that crosses the blood–brain barrier and can be effective in treating anticholinergic symptoms (TABLE 1).4,12 Vital signs and symptoms should be closely monitored. The clinical value of serum diphenhydramine levels is questionable; therefore, treatment should be deter-mined based on ingested dose and clinical presentation. The toxic effects of diphenhydramine are acute but rarely fatal. Long-term adverse effects have not been demonstrated in pediatric cases.4,12,13
Pseudoephedrine is a decongestant found in many nonprescription cough and cold medications. Pseudoephed-rine is a sympathomimetic agent that is responsible for producing nervous system excitation. The stimulation of alpha- and beta-adrenergic receptors can result in effects on the central nervous, cardiovascular, and GI systems. Alpha-adrenergic receptor stimulation results in vasocon-striction and CNS excitation. Vasodilation, bronchodilation, increased cardiac inotropy, and gluconeogenesis can be seen with beta-adrenergic receptor stimulation. Children seem to be more sensitive to the sympathomimetic effects of pseudoephedrine than adults.14
Upon cardiopulmonary stabilization, gastric decon-tamination should be performed within 1 to 4 hours of ingestion. Gastric lavage generally should be performed between 1 and 2 hours of exposure. The recommendation for lavage in sympathomimetic ingestion cases is 1 hour.4,14 IV benzodiazepines can be administered for sedation in extreme hyperactivity and agitation or for the treatment of seizures. Beta-blockers may be required for treatment of tachycardia, dysrhythmias, and hypertension. A combined alpha- and beta-blocker, such as labetalol, may be preferred in order to prevent worsening hypertension caused by inhibiting beta2-mediated vasodilation and exposing the alpha-mediated vasoconstriction caused by the sympatho-mimetic.14 By promptly addressing the sympathomimetic manifestations of pseudoephedrine and other nonprescrip-tion nasal decongestants, children generally recover from acute ingestions without permanent sequelae.14
Iron: Although many nonprescription products are only associated with minor adverse events in ingestion cases, iron supplements can lead to significant clinical manifes-tations. Iron overdoses have been considered a leading cause of injury and death related to poisoning in young children.15 Toxicities can involve the GI, hepatic, cardio-vascular, and central nervous systems.15 Recognition of the clinical stages of acute poisoning can aid in anticipat-ing treatment and predicting outcomes. However, patients may present asymptomatically despite large doses of ingested iron or, conversely, go directly into shock without ever exhibiting GI symptoms.15
GI symptoms tend to appear first, within 3 hours of ingestion, and include vomiting, hematemesis, diarrhea, and abdominal pain. The symptoms can be a result of corrosive damages caused by large doses of iron.16 Increased iron absorption can lead to an increase in unbound con-centrations that may produce excessive reactive oxygen species. These free radicals can damage proteins and cause cellular dysfunction in various organ systems.16
The GI symptoms can subside, and the patient may seem stabilized for up to 12 hours after ingestion. This may be due to unbound iron redistributing from intravas-cular space into the intracellular compartment.15 (Twelve to 48 hours after ingestion is the stage of mitochondrial toxicity.) The patient may experience shock, acidosis, coma, seizures, hyperglycemia, hypoglycemia, pulmonary hemor-rhage, acute respiratory distress syndrome, coagulopathy, or acute tubular necrosis. Jaundice and encephalopathy related to hepatic necrosis can also occur at this stage. In severe cases, gastric scarring and gastric/pyloric strictures may develop 2 to 6 weeks after acute intoxication.15
The ingested dose of iron, serum iron levels, and total iron-binding capacity (TIBC) can help predict the level of toxicity. Since laboratory values are not immediately available and can be unreliable, symptoms should drive therapeutic decisions. Serum iron levels usually peak between 4 and 6 hours of ingestion. Doses of <20 mg/kg elemental iron and levels <350 mcg/dL with a TIBC greater than the serum iron concentration are associated with low toxicity.4,15 The presence of GI symptoms, leukocytosis, and hyperglycemia are predictive of serum levels >300 mcg/dL.4 Theoretically, free iron is absent when TIBC is greater than the serum iron level, indicating a low risk for toxicity. However, TIBC measurements are inaccurate in cases of iron overload, and studies have demonstrated toxicities even with high TIBC levels.15 Patients ingesting >60 mg/kg of elemental iron with levels >500 mcg/dL are at risk for severe toxicity.4,15
Initial management of the symptomatic patient should be resuscitation by supplemental oxygen, inotropic agents, transfusions, or fluid boluses. Once the patient is hemo-dynamically stable, gastric lavage should be performed. Whole bowel irrigation is an option if an abdominal x-ray confirms undissolved tablets throughout the GI tract.4,15 Activated charcoal is ineffective in binding iron and is thus not routinely recommended for iron-only toxic ingestions.15
Patients with resolving symptoms and low serum iron levels generally do not require additional treatment after gastric lavage or whole bowel irrigation.4 Those who have high serum iron levels, metabolic acidosis, or severe GI bleeding, are in shock, or are comatose should be given iron chelation therapy. Deferoxamine binds chelates to ferric ions and forms ferrioxamine for removal by the kidneys. Defer-oxamine should be given as a continuous infusion and
51 CE-Accidental 3_1bosc.indd 5451 CE-Accidental 3_1bosc.indd 54 3/2/10 9:53 AM3/2/10 9:53 AM

55U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
continued until the patient is clinically stable, serum iron is <100 mcg/dL, or urine is no longer rose colored. (Rose-colored urine indicates the presence of the deferoxamine-iron complex). Each 100 mg of deferoxamine can chelate approximately 9 mg of elemental iron (TABLE 1).4,15 Adverse effects of deferoxamine are associated with rapid IV infu-sions and include hypotension, facial flushing, rash, urticaria, tachycardia, and shock.4,17
Most patients respond well to appropriate therapy for iron intoxication.15,16 A retrospective, descriptive study discussed 21 children presenting to the emergency depart-ment after accidental iron poisoning. Thirteen of those patients ingested more than 60 mg/kg of elemental iron. Two out of three asymptomatic patients ingested 100 mg/kg or more of elemen-tal iron. Nine patients experienced shock and/or impaired consciousness and two children had acute liver failure. The hospital course of four patients who died during the study was com-plicated by shock, coma, acute liver failure, blood glucose abnormalities, leukocytosis, and severe acidosis. None of the remaining children developed any long-term complications based on a follow-up period of 6 months to 3 years.16
Prescription MedicationsAlthough oral prescription medications are required by law to be dispensed in child-resistant packaging, patients have the option to request easy-open lids. Thus, tens of thousands of prescription-medication accidental ingestions are still reported every year.2,18 Medications are often transferred to non-child-resistant containers, such as multiple-day medication organizers or plastic bags. Even a large number of those that remain in appropriate containers are accessed by determined children.1 An all-inclusive review of toxic ingestions of prescription medications cannot be completed within the scope of this article; therefore, a selection of the most common and the most toxic will be discussed.
Antihypertensives: Angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) are widely used for the treatment of hypertension. ACE inhib-itors (e.g., captopril, enalapril) are often prescribed for pediatric patients with congenital heart defects, but ARBs have not been widely studied for use in children. Out of nine reported cases of ACE inhibitor ingestions reviewed by Balit et al, only one child exhibited clinical effects.19 A 2.5-year-old girl experienced transient hypotension (65/40 mmHg) approximately 4 hours after ingesting 28 mg of perindopril (not available in the U.S.). No treatment was given, and her blood pressure returned to normal within
20 minutes.19 Ten cases of ARB ingestions were reported, with one patient experiencing unsteadiness within an hour of ingesting 150 mg of irbesartan. Blood pressure upon presentation to the hospital was slightly low, but the child returned to baseline 3 hours postingestion.19 Based on limited studies, observation of an ACE inhibitor or ARB ingestion patient can reasonably be done at home if doses do not exceed 4 mg/kg or 100 mg of captopril, 1 mg/kg or 30 mg of enalapril, or 1 mg/kg of lisinopril.20,21
Beta-adrenergic antagonists are antihypertensives that can also be used for various health conditions including migraines, dysrhythmias, and thyrotoxicosis. In 2004, the AAPCC reported 4,077 beta-blocker ingestions in children
younger than 6 years.22 Love et al observed ingestions over a 6-year time period and found 208 cases of beta-blocker exposures.22 Only nine of those cases exhibited signs or symptoms related to the ingestion. A correlation between ingested dose and symptoms could not be determined. These nine patients
experienced altered mental status or behavioral changes. Records indicate hypotension, lethargy, ataxia, disorienta-tion, blankly staring, and not acting like themselves. A total of 72% of patients were given activated charcoal. Symptoms spontaneously resolved and were not treated. Bradycardia and hypoglycemia were not observed in these patients. The only significant morbidity observed in this study was aspiration of charcoal.22 This study, among others, con-tributes to literature that reveals minimal toxicity in beta-blocker ingestion cases.
ACE inhibitors, ARBs, and beta-blockers have demon-strated minimal toxicity in accidental ingestions. However, not all antihypertensives can be deemed harmless. Calcium channel blockers (CCBs) rank among the top 10 causes of toxin-related deaths in children younger than 6 years.23 Toxicities of CCBs are typically exaggerations of therapeu-tic effects. Conduction system delays, loss of myocardial contractility, and loss of systemic vascular smooth muscle tone can be seen in toxic ingestions. Clinical presentation of toxicity can vary depending on the class of CCBs.23
Patients who have ingested diltiazem or verapamil tend to present with bradycardia, heart block, atrioventricular (AV) conduction disturbances, and myocardial dysfunction. These agents have more negative inotropic and chronotropic effects than other CCBs. Commonly reported symptoms in verapamil and diltiazem ingestions include mental status changes, vomiting, hypotension, and bradycardia. Symptoms can be seen even after ingestion of one verapamil tablet.23 Toxic doses in the sustained-release formulation of verapamil range from 12 to 120 mg/kg. The mean pediatric toxic dose for diltiazem has been determined as 5.7 mg/kg.23
Contact poison control
by calling 1-800-222-1222.
51 CE-Accidental 3_1bosc.indd 5551 CE-Accidental 3_1bosc.indd 55 3/2/10 9:53 AM3/2/10 9:53 AM

56U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
Dihydropyridines, such as nifedipine and amlodipine, have more effects on vascular smooth muscle tone and, in contrast to the other CCBs, have little effect on cardiac conduction. In overdoses, tachycardia may be the first clinical effect produced in response to decreased systemic vascular resistance. A review of nifedipine ingestions revealed nine deaths.23 Three of these reported deaths occurred after ingestion of just one or two tablets. With standard-release formulations, symptoms occurred within 1 to 2 hours. Onset of symptoms was more variable in sustained-release formulations. Changes in mental status, bradycardia, and tachycardia were noted in ingestion cases, with hypotension being the most common adverse event. Other dihydro-pyridine ingestions have not been described as frequently as nifedipine. The most common symptoms of toxicity from a small number of reported amlodipine ingestions were lethargy and hypotension.23
Administration of activated charcoal should be consid-ered within 2 hours of toxic ingestions. When given within this time frame, CCB absorption decreased by 85% to 99%.23 To treat hypotension associated with CCB intoxi-cation, IV fluids and vasopressors may be given. IV calcium administration can provide competitive channel receptor activity. Atropine should be used for CCB-induced brady-cardia. High-dose insulin with supplemental glucose improves cellular metabolism and exerts positive inotropic effects to reverse myocardial depression (TABLE 1).23,24 Adjunctive therapy with glucagon has demonstrated variable results in providing inotropic and chronotropic support, but has been used successfully in patients with hypotension refrac-tory to fluids, atropine, calcium, and dopamine.23-25
Clonidine is a central alpha2-adrenergic agonist that is used for the treatment of hypertension and also of psychi-atric conditions. With a therapeutic role in the management of attention-deficit/hyperactivity disorder, this medication has become widely available to children and thus prone to accidental ingestions. In 2003, 5,400 clonidine exposures were reported, with 32% of those being in children less than 6 years of age.24 Onset of symptoms occurred within 30 to 90 minutes in most cases, with a mean time of 1.7 hours for maximum CNS depression.25,26 Drowsiness and lethargy were noted in 72% of patients, bradycardia in 12%, hypotension in 9%, and respiratory depression requiring mechanical ventilation in 7%. Six percent of patients were comatose. The more serious effects were reported more frequently in the younger children.26
Clonidine ingestions of doses >5 mcg/kg for children 4 years and younger require direct medical evaluation. Medical attention is also recommended for children 5 to 8 years of age with ingested doses of >0.2 mg and of >0.4 mg for children older than 8 years.26 Management of clonidine ingestions begins with ensuring or establishing
an adequate airway. Activated charcoal should be given within 1 hour of ingestion. Continuous cardiac monitoring and electrocardiograms should be used to rule out brady-cardia, heart block, and hypotension. Since clonidine toxicity presents similarly to opioid intoxication, naloxone has been used for the treatment of severe clonidine overdose (TABLE 1). The mechanism of reversal is likely due to the close proximity within the neuron of the alpha-adrenergic receptor targeted by clonidine and the mu opioid receptors, as well as the functional overlap of the receptors.25 Brady-cardia will generally respond to atropine. Hypotension can be managed with fluid resuscitation and vasopressors, if necessary.25 Death from clonidine overdose is rare, and most patients recover without permanent sequelae; but toxic effects can be seen in doses as low as 10 mcg/kg.24-26
Sulfonylureas: Sulfonylurea agents, such as chlorpropamide, glipizide, glyburide, and glimepiride, are commonly used for the management of type 2 diabetes. In 2003, over 4,000 sulfonylurea exposures were reported to poison control centers, and one-third of those ingestions involved children less than 6 years of age.24 Up to 72% of cases of uninten-tional sulfonylurea cases present asymptomatically.27 How-ever, case reports have described neurologic symptoms or death resulting from just one or two tablets.28 Spiller et al prospectively evaluated 185 cases of accidental sulfonylurea ingestions.29 Thirty percent of patients presented with blood glucose (BG) concentration <60 mg/dL, and 3% of cases presented with BG levels <40 mg/dL. The mean time after ingestion to minimum BG level was 5.3 hours, and the onset of hypoglycemia was typically observed within 8 hours of ingestion.28,29
These hypoglycemic agents stimulate insulin secretion from the pancreas, inhibit gluconeogenesis, and also increase insulin sensitivity.9,29 Symptoms of sulfonylurea ingestions can present with hypoglycemia, loss of appetite, weakness, dizziness, lethargy, seizure, and coma.24,28 General principles of resuscitation and vital-sign stabilization should be applied immediately following discovery of ingestion. Activated charcoal may be useful if given within 1 hour of exposure. Blood glucose concentrations should be monitored every 1 to 2 hours until stabilized >60 mg/dL. Observation of patients for at least 24 hours is a reasonable expectation considering that discovery of hypoglycemia has been delayed for as long as 21 hours in ingestions of extended-release formulations.29,30 Patients with ingestions of ≥0.3 mg/kg of glyburide or glipizide appear to be at higher risk of hypoglycemia.29 However, these dosing parameters should not be used as guidelines for determining monitoring or treatment. Symptomatic patients with hypoglycemia should be treated with dextrose boluses. Continuous infusions of dextrose may also be considered to maintain euglycemia;
51 CE-Accidental 3_1bosc.indd 5651 CE-Accidental 3_1bosc.indd 56 3/2/10 9:53 AM3/2/10 9:53 AM

57U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
however, breakthrough hypoglycemic episodes can occur. In cases where IV access is unattainable, glucagon can be given but is not always recommended because of the risk of rebound hypoglycemia.24,28,30
Octreotide has been used as adjunctive treatment of hypoglycemia from sulfonylurea ingestions. This synthetic peptide analogue of somatostatin is a potent inhibitor of insulin secretion. Doses of 1 mcg/kg up to 50 mcg given subcutaneously every 6 to 8 hours have been recommended (TABLE 1).9,24,30 Doses may be titrated up if hypoglycemia persists or worsens.30 Use of adjunctive octreotide has demonstrated decreased hypoglycemic events and decreased dextrose requirements.25,28 Diazoxide is an antihypertensive agent that also decreases beta–islet cell insulin secretion and can be used to treat hypoglycemia.25,28,30 The injectable formulation is no longer available in the U.S., and dosing of the oral formulation is not defined for the treatment of sulfonylurea-induced hypoglycemia. The unavailability of the IV formulation and the potentially harmful side effects of tachycardia, hypotension, and sodium retention make diazoxide a less-favored antidote.25,30
Treatment of Ingestions at HomeParents were once urged to keep a single bottle of ipecac syrup in case of accidental ingestions. However, stimulation of emesis by administration of ipecac syrup for ingestions of any substance is no longer recommended by the Amer-
ican Academy of Pediatrics (AAP).31 Even when ipecac is administered immediately, the ingested substance is not completely expelled from the stomach. The side effects from ipecac syrup can also delay appropriate diagnosis and treatment. For example, lethargy caused by ipecac can cloud the clinical presentation, potentially making the diagnosis more difficult to obtain. Prolonged vomiting can also delay administration or decrease effectiveness of antidotes.31 The AAP stresses the importance of prevention and reminds parents to contact a poison control center (AAPCC hotline: 1-800-222-1222) in the event of an ingestion.
PreventionGenerally, unintentional ingestions in pediatric patients result in mild or no symptoms. However, there are certain substances that can lead to permanent damage or even death if the ingestion and/or the symptoms resulting from ingestion are not recognized and treated in a timely man-ner. Even though most ingestions do not result in perma-nent physical harm to the patient, placing calls to poison control centers or taking a child to the hospital causes significant emotional trauma for both child and parent. Child-resistant containers are not always adequate barriers to potentially dangerous substances. Ensuring the storage of medications out of the reach of children and direct supervision of curious children are the most effective ways to prevent toxic ingestions.
REFERENCES1. McFee RB, Caraccio TR. “Hang up your pocketbook”—an easy intervention for the granny syndrome: grandparents as a risk factor in unintentional pediatric exposures to pharmaceuticals. J Am Osteopath Assoc. 2006;106:405-411.2. Bronstein AC, Spyker DA, Cantilena LR Jr, et al. 2007 Annual report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 25th annual report. Clin Toxicol. 2008;46:927-1057.3. Casasnovas AB, Martinez EE, Cives RV, et al. A retrospective analy-sis of ingestion of caustic substances by children. Ten-year statistics in Galicia. Eur J Pediatr. 1997;156:410-414.4. Barkin RM, Rosen P. Emergency Pediatrics: A Guide to Ambulatory Care. 6th ed. Philadelphia, PA: CV Mosby Company; 2003.5. Fulton JA, Hoffman RS. Steroids in second-degree caustic burns of the esophagus: a systematic pooled analysis of fifty years of human data: 1956-2006. Clin Toxicol. 2007;45:402-408.6. Levy-Khademi F, Tenenbaum AN, Wexler ID, Amitai Y. Uninten-tional organophosphate intoxication in children. Pediatr Emerg Care. 2007;23:716-718.7. Sungur M, Guven M. Intensive care management of organophos-phate insecticide poisoning. Crit Care. 2001;5:211-215.8. White ML, Liebelt EL. Updates on antidotes for pediatric poison-ing. Pediatr Emerg Care. 2006;22:740-749.9. Taketomo CK, Hodding JH, Kraus DM, eds. Pediatric Dosage Handbook. 15th ed. Hudson, OH: Lexi-Comp; 2008.10. Dart RC, Paul IM, Bond GR, et al. Pediatric fatalities associated with over the counter (nonprescription) cough and cold medications. Ann Emerg Med. 2009;53:411-417.
11. LoVecchio F, Pizon A, Riley B, et al. Accidental dextrometh-orphan ingestions in children less than 5 years old. J Med Toxicol. 2008;4:251-253.12. Goetz CM, Lopez G, Dean BS, Krenzelok EP. Accidental child-hood death from diphenhydramine overdosage. Am J Emerg Med. 1990;8:321-322.13. Stojanovski SD, Baker SD, Casavant MJ, et al. Implications of diphenhydramine single-dose unintended ingestions in young children. Pediatr Emerg Care. 2007;23:465-468.14. Sauder KL, Brady WJ, Hennes H. Visual hallucinations in a tod-dler: accidental ingestion of a sympathomimetic over-the-counter nasal decongestant. Am J Emerg Med. 1997;15:521-526.15. Singhi S, Baranwal AK, Jayashree M. Acute iron poisoning: clinical picture, intensive care needs and outcome. Indian Pediatr. 2003;40:1177-1182.16. Baranwal AK, Singhi SC. Acute iron poisoning: management guidelines. Indian Pediatr. 2003;40:534-540.17. Morris CC. Pediatric iron poisonings in the United States. South Med J. 2000;93:352-358.18. Jacobson BJ, Rock AR, Cohn MS, Litovitz T. Accidental ingestions of oral prescription drugs: a multicenter survey. Am J Public Health. 1989;79:853-856.19. Balit CR, Gilmore SP, Isbister GK. Unintentional paediatric inges-tions of angiotensin converting enzyme inhibitors and angiotensin II receptor antagonists. J Paediatr Child Health. 2007;43:686-688.20. Hogue-Murray K, Horowitz R, Dart R. Outcome of ACE inhib-itor ingestion in children under the age of six years. J Toxicol Clin Toxicol. 1995;33:509-510.21. Spiller HA, Udicious TM, Muir S. Angiotensin converting
enzyme inhibitor ingestion in children. J Toxicol Clin Toxicol. 1989;27:345-353.22. Love JN, Howell JM, Klein-Schwartz W, Litovitz TL. Lack of tox-icity from pediatric beta-blocker exposures. Hum Exp Toxicol. 2006;25:341-346.23. Ranniger C, Roche C. Are one or two dangerous? Calcium chan-nel blocker exposure in toddlers. J Emerg Med. 2007;33:145-154.24. Henry K, Harris CR. Deadly ingestions. Pediatr Clin N Am. 2006;53:293-315.25. Michael JB, Sztajnkrycer MD. Deadly pediatric poisons: nine common agents that kill at low doses. Emerg Med Clin N Am. 2004;22:1019-1050.26. Spiller HA, Klein-Schwartz W, Colvin JM, et al. Toxic clonidine ingestion in children. J Pediatr. 2005;146:263-266.27. Quadrani DA, Spiller HA, Widder P. Five year retrospective evalu-ation of sulfonylurea ingestion in children. J Toxicol Clin Toxicol. 1996;34:267-271.28. Little GL, Boniface KS. Are one or two dangerous? Sulfonylurea exposure in toddlers. J Emerg Med. 2005;28:305-310.29. Spiller HA, Villalobos D, Krenzelok EP, et al. Prospective multi-center study of sulfonylurea ingestion in children. J Pediatr. 1997;131:141-146.30. Calello DP, Kelly A, Osterhoudt KC. Case files of the Medical Toxicology Fellowship Training Program at Children’s Hospital of Phil-adelphia: a pediatric exploratory sulfonylurea ingestion. J Med Toxicol. 2006;2:19-24.31. American Academy of Pediatrics Committee on Injury, Violence, and Poison Prevention. Policy statement: poison treatment in the home. Pediatrics. 2003;112:1182-1185.
■ Disclosure Statements: Dr. Fung has no actual or potential conflicts of interest in relation to this activity.U.S. Pharmacist does not view the existence of relationships as an implication of bias or that the value of the material is decreased. The content of the activ-ity was planned to be balanced, objective, and scientifically rigorous. Occasion-ally, authors may express opinions that represent their own viewpoint. Conclu-sions drawn by participants should be derived from objective analysis of scientific data.
■ Disclaimer: Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The infor-mation presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treat-ment discussed or suggested in this activity should not be used by clinicians without evaluation of their patients’ conditions and possible contraindications or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
51 CE-Accidental 3_1bosc.indd 5751 CE-Accidental 3_1bosc.indd 57 3/2/10 9:53 AM3/2/10 9:53 AM
58U.S. Pharmacist • March 2010 • www.uspharmacist.com
PEDIATRIC ACCIDENTAL INGESTIONS
1. Which of the following is true regarding accidental ingestions?A. Proper storage of medications is the best prevention of
accidental ingestionsB. The majority of pediatric ingestions result in benign
medical coursesC. Children 6 years and younger are most commonly
involved in accidental ingestionsD. All of the above
2. Which of the following statements is false regarding ingestions of household cleaning solutions?A. Alkaline solutions are more likely to cause esophageal
burnsB. Corticosteroids have been proven to prevent
esophageal stricturesC. Ingested substances should be diluted with water or
milk immediatelyD. None of the above
3. What toxin is associated with cholinergic symptoms?A. Organophosphates C. DiphenhydramineB. Iron D. Clonidine
4. Which of the following statements is true regarding the use of pralidoxime (2-PAM)?A. 2-PAM should be initiated based on elevated serum
cholinesterase levelsB. 2-PAM should not be initiated prior to atropine
therapyC. 2-PAM antagonizes acetylcholine at muscarinic
synapses to relieve symptomsD. All of the above
5. The most common presenting symptoms in organophosphate toxicity are:A. Hematologic C. CardiovascularB. Neurologic D. Gastrointestinal
6. The first symptoms to present in iron toxicity are:A. HematologicB. NeurologicC. CardiovascularD. Gastrointestinal
7. Which of the following is not an appropriate treatment approach in iron ingestions?A. Gastric lavageB. Whole bowel irrigationC. Activated charcoalD. Deferoxamine
8. What does rose-colored urine indicate when seen during deferoxamine therapy?A. Hematuria associated with renal toxicity of ironB. Excretion of unchanged deferoxamine C. Discoloration of the urine by ironD. Presence of the deferoxamine-iron complex
9. For every 100 mg of deferoxamine, how much elemental iron can be chelated?A. 9 mg C. 30 mgB. 15 mg D. 60 mg
10. Which of the following statements is true regarding dextromethorphan ingestions?A. Dextromethorphan has strong opioid receptor activity
and can lead to respiratory depression in slight overdoses
B. Anticholinergic symptoms commonly seen with dextromethorphan ingestions can be treated with physostigmine
C. The symptoms seen with dextromethorphan ingestions are most likely due to effects on the N-methyl-d-aspartate receptor
D. All of the above
11. Which of the following is a common sign of pseudoephedrine ingestion?A. TachycardiaB. HypertensionC. DysrhythmiasD. All of the above
12. Which class of antihypertensive medications is most likely to cause severe toxicity in accidental ingestions?A. Calcium channel blockers (CCBs)B. Angiotensin-converting enzyme (ACE) inhibitorsC. Angiotensin II receptor blockers (ARBs)D. Beta-blockers
EXAMINATIONSelect one correct answer for each question and record your responses on the examination answer sheet. Mail it to U.S. Pharmacist, address shown on the answer sheet (photocopies are acceptable). Please allow four weeks for processing. Alternatively, this exam can be taken online at www.uspharmacist.com. Please contact CE Customer Service at (800) 825-4696 or [email protected] with any questions.
Pediatric Accidental Ingestions: Monitoring and Treatment Options
2 CE Credits
51 CE-Accidental 3_1bosc.indd 5851 CE-Accidental 3_1bosc.indd 58 3/2/10 9:53 AM3/2/10 9:53 AM
59U.S. Pharmacist • March 2010 • www.uspharmacist.com
13. The most common clinical effect observed in dihydropyridine CCB ingestion is:A. Bradycardia C. HypotensionB. Tachycardia D. Hypertension
14. Which CCB has the most inotropic and chronotropic effects?A. Verapamil C. NifedipineB. Amlodipine D. Nimodipine
15. High-dose insulin and supplemental glucose have been used to treat what type of toxicity?A. SulfonylureasB. CCBsC. OrganophosphatesD. Clonidine
16. The most common adverse effect observed in clonidine ingestions is:A. HypotensionB. TachycardiaC. DrowsinessD. Hypertension
17. Which of the following statements is true regarding clonidine ingestions?A. Younger children experience more severe adverse
effectsB. The onset of symptoms is delayed and may not
present until 24 hours after ingestionC. Deaths are commonly reported in ingestions of as
little as 5 mcg/kgD. All of the above
18. Which of the following medications can be used to treat clonidine toxicity?A. Octreotide C. InsulinB. Pralidoxime D. Naloxone
19. The majority of sulfonylurea ingestion cases are:A. FatalB. AsymptomaticC. Associated with severe hypoglycemiaD. Associated with respiratory depression
20. The treatment of sulfonylurea ingestion can include all of the following except:A. High-dose insulin and supplemental glucoseB. OctreotideC. Activated charcoalD. Continuous infusion of dextrose
PEDIATRIC ACCIDENTAL INGESTIONS
✁
Examination Answer Sheet Credits: 2.0 hours (0.20 ceu)
Expires: March 31, 2012This exam can be taken online at www.uspharmacist.com. Upon passing, you can print out your statement immediately and view your test history. Alternatively, you
can mail this answer sheet to the address below. Please contact CE Customer Service at (800) 825-4696 or [email protected] with any questions.
Pediatric Accidental Ingestions: Monitoring and Treatment Options
* Also applies to pharmacy technicians.
Please retain a copy for your records. Please print clearly.
You must choose and complete ONE of the following three identifier types:
SS # - -
Last 4 digits of your SS # and date of birth -
State Code and License # (Example: FL12345678)
First Name
Last Name
The following is your: Home Address Business Address
Business Name
Address
City State
ZIP
Telephone # - -
Fax # - -
Profession: Pharmacist Pharmacy Technician Other
By submitting this answer sheet, I certify that I have read the lesson in its entirety and completed the self-assessment exam personally based on the material presented. I have not obtained the answers to this exam by any fraudulent or improper means.
Signature Date
Postgraduate Healthcare Education, LLC is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
1 = Excellent 2 = Very Good 3 = Good 4 = Fair 5 = Poor
Rate the effectiveness of how well the activity:
21. Met objective 1:*
22. Met objective 2:*
23. Met objective 3:*
24. Met objective 4:*
25. Related to your educational needs:
26. The active learning strategies (questions, cases, discussions) were appropriate and effective learning tools:
27. Avoided commercial bias:
28. How would you rate the overall usefulness of the material presented?
29. How would you rate the quality of the faculty?
30. How would you rate the appropriateness of the examination for this activity?
31. Comments on this activity:
1. A B C D
2. A B C D
3. A B C D 4. A B C D
5. A B C D
6. A B C D
7. A B C D
8. A B C D
9. A B C D
10. A B C D
11. A B C D
12. A B C D
13. A B C D
14. A B C D
15. A B C D
16. A B C D
17. A B C D
18. A B C D
19. A B C D
20. A B C D
Directions: Select one answer for each question in the exam and completely darken the appropriate circle. A minimum score of 70% is required to earn credit. An identifier is required to process your exam. This is used for internal processing purposes only.
Mail to: U.S. Pharmacist–CE, PO Box 487, Canal Street Station, New York, NY 10013
®
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1
2
3
Payment:
Check is enclosed (payable to Jobson Medical Information LLC)
Charge my: American Express Mastercard Visa
Name on Card:
Credit Card #:
Expiration Date:
Signature:
Check one: $6.50 per exam, fee enclosed
$45 for grading of 12 lessons, fee enclosed*
1 of 12 lessons,fee previously paid
* Valid for 18 months from date of receipt
0430-0000-10-008-H01-P Lesson 106603 Type of Activity: Knowledge 0430-0000-10-008-H01-T
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
51 CE-Accidental 3_1bosc.indd 5951 CE-Accidental 3_1bosc.indd 59 3/2/10 9:53 AM3/2/10 9:53 AM
To place a classified ad, call:Toll Free: (800) 983-7737
Phone: (610) 854-3770Fax: (610) 854-3780
U.S. Pharmacist ClassifiedsCAREER OPPORTUNITIES
Whois Cardinal Health?• Leading, global provider of information, products, services
and technologies for the health care industry• Ranked 18th in Fortune 500• 30,000 employees worldwide• $87 billion global company
Who is Pharmacy Solutions?• We bring 40 years of expertise in helping hospitals and healthcare
systems improve both the financial predictability of pharmacies and the quality of patient care.
• 1,000 pharmacists employed, including 110 clinical specialists• Participate in more than 140 accreditation survey reviews each year• We process four million order lines remotely each year and identified
20,000 patient safety events through our Rxe-sourceSM centersin 2008
• Rxe-viewTM solution is an automated medication order managementand clinical intervention tracking tool
• We also offer a customized portfolio of drug contracts
� Director of PharmacyIL – SpartaIN – MunsterLA – Shreveport
NC – MarionTX – Bryan; OdessaUT – Layton
WV – Princeton
� Clinical ManagerMD – BaltimoreNC – Wilmington
MO – Springfield
� Staff PharmacistAZ – Tempe (1 F/T);
(1 PRN) CA – San Diego (PRN)CT – Sharon;
New Haven (PRN)
DE – SmyrnaFL– Tampa (PRN)MD – Rockville (PRN)PA – Coudersport;
Waynesburg
TN – OakridgeTX – Port Arthur (PRN);
Sulphur Springs (PRN);San Antonio (PRN)
WV – Bluefield (P/T)
We are currently hiring for the following positions:
For information or to apply,call 800-231-9807 ext. 1315
or fax 281-749-2026
� Manager, Retail Pharmacy
� Rxe-sourceSM (Staff Pharmacists at Remote Centers, 7on/7 off Overnight)CA – Glendale NC – Cary MA – Marlborough OH – Dublin
� Pharmacy TechniciansAZ – Mesa; PhoenixDE – SmyrnaFL – Port St. Lucie
NC – CaryNV – North Las VegasTX – Odessa; Port Arthur
� System Clinical ManagerMI – Grand Rapids
� Assistant Director of PharmacyAZ – TempeMO – Springfield (outpatient)
� Senior Consultant, Clinical OperationsIN – Indianapolis
� Clinical Specialist, Critical CareNY – Valhalla
� NICU SpecialistOK – Tulsa
CAREER OPPORTUNITIESCAREER OPPORTUNITIES
Experience The Sentara Potomac Hospital Difference
Designed with staff input, Sentara Potomac Hospital features all-private patientrooms, a renovated surgical suite/PACU with da Vinci® robotic-assisted technology,an ASMBS Center of Excellence in weight loss surgery and more.
We are seeking a Pharmacist licensed in the Commonwealth of Virginia with aminimum of two years acute care setting experience.
Located near I-95 at Exit 156, our suburban campus is close to Potomac MillsMall in Woodbridge and just 30 minutes south of our beautiful Nation’s Capital.
Experience the difference at Sentara Potomac Hospital in Woodbridge.
To apply, visit “Careers” at PotomacHospital.com or call (703) 670-1509.E-mail Employment Manager at [email protected].
ATTN:PHARMACY TECHNICIANSDISCOVER NPTA...the largest
professional organizationspecifically for pharmacy technicians.
Free CE + Advocacy + ResourcesLearn more at:
www.pharmacytechnician.org/discover
CAREER OPPORTUNITIES

U.S. Pharmacist Classifieds
A D I N D E X
CAREER OPPORTUNITIES
Become a valued member of the world’s largest group practice in providing quality medical care.
CLINICAL PHARMACISTNational Naval Medical Center
Bethesda, MDThis position is located in the Hematology/Oncology Pharmacy. Our
mission is to provide pharmaceutical care in an academic setting to
patients with oncologic and hematologic diagnoses and to support
the academic activities of the Hematology/Oncology Department.
What you will do!
• Work as a team member with other pharmacists to evaluate and process
chemotherapy orders.
• Prepare complex combination chemotherapy regimens for clinical protocols.
• Design drug regimens using current pharmacokinetic principles and
specific patient parameters.
• Serve as consultant to hematology/oncology fellows and staff
hematologists/oncologists.
• Provide training and education to pharmacy residents and nursing staff.
Competitive salary and comprehensive benefits!
• Potential pay incentives.
• Lifetime health insurance (Navy pays portion of your premium, you pay
with pre-taxed dollars) you can carry into retirement and cover your souse.
• Retirement plan with 401K-type investment, employer matching, and
ability to retire between 55-57 with 10 years of employment.
• Life insurance (Navy pays portion of your premium).
• Long term care insurance.
• 13-26 paid vacation days, 13 paid sick days, 10 paid Federal holidays,
and unused vacation/sick days carry over year to year.
• Employee friendly workplace flexibilities.
Requirements
• Bachelor’s or PharmD degree in pharmacy.
• Current Pharmacist license awarded by any state.
• Oncology residency or comparable experience.
• U. S. Citizenship.
Apply Now!
Here’s how:
• E-mail your resume to [email protected] and include 0089USP in
your subject line.
OR
• Mail your resume toU. S. Department of Navy111 S. Independence Mall EastAttn: BUMED/0089USPPhiladelphia, PA, 19106
If you have any questions, please contact Judy Safady at 215-408-4441.
Equal Opportunity Employer
National
AstraZeneca . . . . . . . . . . . . . . . . . . . . CV4Combe, Inc. . . . . . . . . . . . . . . . . . . . . . . . 16Daiichi-Sankyo . . . . . . . . . . . . . . . . . . . . 45Eli Lilly and Company . . . . . . . . . . . . . . . . 2Fougera . . . . . . . . . . . . . . . . . . . . . . . . . . . 9GlaxoSmithKline . . . . . . . . . . . . . . . . . . . 41Mylan Pharmaceuticals Inc. . . . . . . . . . . 7Novartis Pharmaceuticals . . . . . . . . . . . 25Novo Nordisk . . . . . . . . . . . . . . . . . . . . . . 19Reckitt Benckiser . . . . . . . . . . . . . . . . CV2Santarus . . . . . . . . . . . . . . . . . . . . . . . . . . 35Schering-Plough . . . . . . . . . . . . . . . . . . . 23ScriptPro . . . . . . . . . . . . . . . . . . . . . . . . . 33URL Pharma . . . . . . . . . . . . . . . . . . . . . . 11
Health Systems
Eisai Pharmaceuticals . . . . . . . HS07Eli Lilly and Company . . . . . . . HS18Medi-Dose Group . . . . . . . . . . 50-HSMylan Pharmaceuticals Inc. . . .HS11Pfizer Injectables . . . . . . . . . . . HS01Teva Pharmaceuticals . . . . . . . HS03
New Products - National
Fanapt / Novartis Pharmaceuticals .25Onglyza/ AstraZeneca . . . . . . . . . . CV4Welchol / Daiichi-Sankyo . . . . . . . . . .45
New Products - Health SystemsHumalog / Eli Lilly and Company . . HS18Injectables / Pfizer Injectables . . . . . HS01
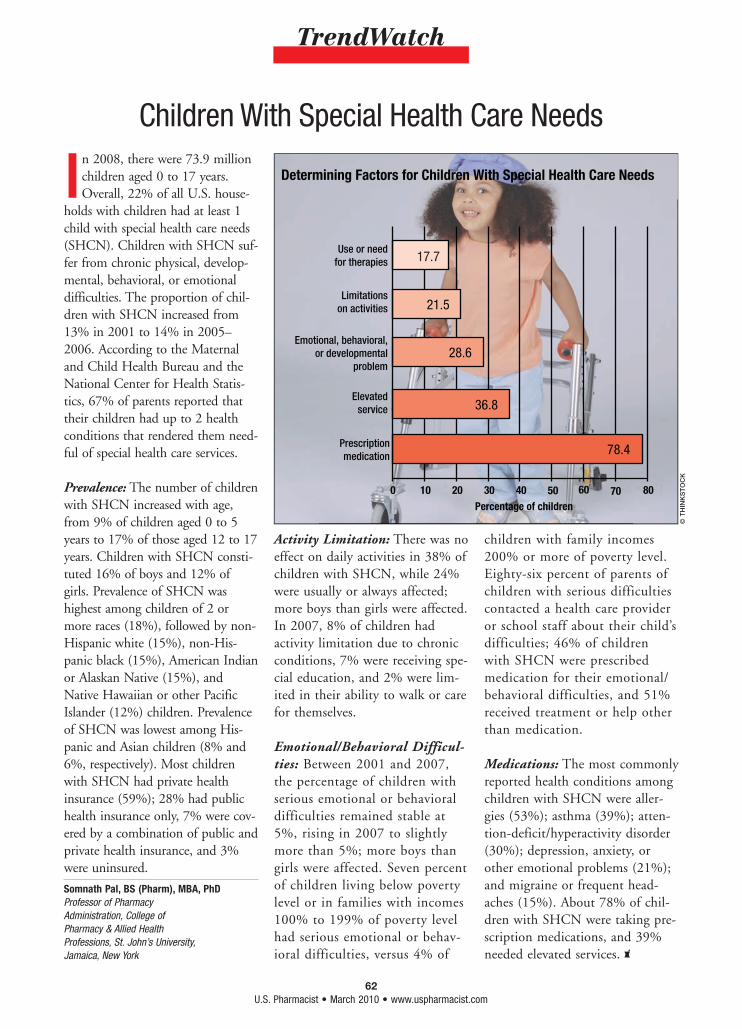
62U.S. Pharmacist • March 2010 • www.uspharmacist.com
TrendWatch
In 2008, there were 73.9 million children aged 0 to 17 years. Overall, 22% of all U.S. house-
holds with children had at least 1 child with special health care needs (SHCN). Children with SHCN suf-fer from chronic physical, develop-mental, behavioral, or emotional difficulties. The proportion of chil-dren with SHCN increased from 13% in 2001 to 14% in 2005–2006. According to the Maternal and Child Health Bureau and the National Center for Health Statis-tics, 67% of parents reported that their children had up to 2 health conditions that rendered them need-ful of special health care services.
Prevalence: The number of children with SHCN increased with age, from 9% of children aged 0 to 5 years to 17% of those aged 12 to 17 years. Children with SHCN consti-tuted 16% of boys and 12% of girls. Prevalence of SHCN was highest among children of 2 or more races (18%), followed by non-Hispanic white (15%), non-His-panic black (15%), American Indian or Alaskan Native (15%), and Native Hawaiian or other Pacific Islander (12%) children. Prevalence of SHCN was lowest among His-panic and Asian children (8% and 6%, respectively). Most children with SHCN had private health insurance (59%); 28% had public health insurance only, 7% were cov-ered by a combination of public and private health insurance, and 3% were uninsured.
Activity Limitation: There was no effect on daily activities in 38% of children with SHCN, while 24% were usually or always affected; more boys than girls were affected. In 2007, 8% of children had activity limitation due to chronic conditions, 7% were receiving spe-cial education, and 2% were lim-ited in their ability to walk or care for themselves.
Emotional/Behavioral Difficul-ties: Between 2001 and 2007, the percentage of children with serious emotional or behavioral difficulties remained stable at 5%, rising in 2007 to slightly more than 5%; more boys than girls were affected. Seven percent of children living below poverty level or in families with incomes 100% to 199% of poverty level had serious emotional or behav-ioral difficulties, versus 4% of
children with family incomes 200% or more of poverty level. Eighty-six percent of parents of children with serious difficulties contacted a health care provider or school staff about their child’s difficulties; 46% of children with SHCN were prescribed medication for their emotional/behavioral difficulties, and 51% received treatment or help other than medication.
Medications: The most commonly reported health conditions among children with SHCN were aller-gies (53%); asthma (39%); atten-tion-deficit/hyperactivity disorder (30%); depression, anxiety, or other emotional problems (21%); and migraine or frequent head-aches (15%). About 78% of chil-dren with SHCN were taking pre-scription medications, and 39% needed elevated services.
Children With Special Health Care Needs
© T
HIN
KS
TO
CK
Somnath Pal, BS (Pharm), MBA, PhDProfessor of Pharmacy Administration, College of Pharmacy & Allied Health Professions, St. John’s University, Jamaica, New York
78.4
36.8
28.6
21.5
17.7
0 10 20 30 40
Prescription medication
Elevated service
Emotional, behavioral, or developmental
problem
Limitations
on activities
Use or need for therapies
Percentage of children
Determining Factors for Children With Special Health Care Needs
50 60 70 80
62 REVTrendwatch 3_2sc.indd 6262 REVTrendwatch 3_2sc.indd 62 3/2/10 1:41 PM3/2/10 1:41 PM
ONGLYZA™ (saxagliptin) tabletsBrief Summary of Prescribing Information. For complete prescribinginformation consult official package insert.
INDICATIONS AND USAGEMonotherapy and Combination TherapyONGLYZA (saxagliptin) is indicated as an adjunct to diet and exercise to improveglycemic control in adults with type 2 diabetes mellitus. [See Clinical Studies(14).]
Important Limitations of UseONGLYZA should not be used for the treatment of type 1 diabetes mellitus ordiabetic ketoacidosis, as it would not be effective in these settings.ONGLYZA has not been studied in combination with insulin.CONTRAINDICATIONSNone.WARNINGS AND PRECAUTIONSUse with Medications Known to Cause HypoglycemiaInsulin secretagogues, such as sulfonylureas, cause hypoglycemia. Therefore,a lower dose of the insulin secretagogue may be required to reduce the riskof hypoglycemia when used in combination with ONGLYZA. [See AdverseReactions (6.1).]Macrovascular OutcomesThere have been no clinical studies establishing conclusive evidence ofmacrovascular risk reduction with ONGLYZA or any other antidiabetic drug.ADVERSE REACTIONSClinical Trials ExperienceBecause clinical trials are conducted under widely varying conditions, adversereaction rates observed in the clinical trials of a drug cannot be directlycompared to rates in the clinical trials of another drug and may not reflect therates observed in practice.
Monotherapy and Add-On Combination TherapyIn two placebo-controlled monotherapy trials of 24-weeks duration, patientswere treated with ONGLYZA 2.5 mg daily, ONGLYZA 5 mg daily, and placebo.Three 24-week, placebo-controlled, add-on combination therapy trials werealso conducted: one with metformin, one with a thiazolidinedione (pioglitazoneor rosiglitazone), and one with glyburide. In these three trials, patients wererandomized to add-on therapy with ONGLYZA 2.5 mg daily, ONGLYZA 5 mgdaily, or placebo. A saxagliptin 10 mg treatment arm was included in one ofthe monotherapy trials and in the add-on combination trial with metformin.In a prespecified pooled analysis of the 24-week data (regardless of glycemicrescue) from the two monotherapy trials, the add-on to metformin trial, theadd-on to thiazolidinedione (TZD) trial, and the add-on to glyburide trial, theoverall incidence of adverse events in patients treated with ONGLYZA 2.5 mgand ONGLYZA 5 mg was similar to placebo (72.0% and 72.2% versus 70.6%,respectively). Discontinuation of therapy due to adverse events occurred in2.2%, 3.3%, and 1.8% of patients receiving ONGLYZA 2.5 mg, ONGLYZA 5 mg,and placebo, respectively. The most common adverse events (reported in atleast 2 patients treated with ONGLYZA 2.5 mg or at least 2 patients treatedwith ONGLYZA 5 mg) associated with premature discontinuation of therapyincluded lymphopenia (0.1% and 0.5% versus 0%, respectively), rash (0.2%and 0.3% versus 0.3%), blood creatinine increased (0.3% and 0% versus 0%),and blood creatine phosphokinase increased (0.1% and 0.2% versus 0%). Theadverse reactions in this pooled analysis reported (regardless of investigatorassessment of causality) in ≥5% of patients treated with ONGLYZA 5 mg, andmore commonly than in patients treated with placebo are shown in Table 1.
Table 1: Adverse Reactions (Regardless of Investigator Assessmentof Causality) in Placebo-Controlled Trials* Reported in 5%of Patients Treated with ONGLYZA 5 mg and More Commonly than in Patients Treated with Placebo
Number (%) of PatientsONGLYZA 5 mg Placebo
N=882 N=799Upper respiratory tract infection 68 (7.7) 61 (7.6)Urinary tract infection 60 (6.8) 49 (6.1)Headache 57 (6.5) 47 (5.9)* The 5 placebo-controlled trials include two monotherapy trials and one
add-on combination therapy trial with each of the following: metformin,thiazolidinedione, or glyburide. Table shows 24-week data regardless ofglycemic rescue.
In patients treated with ONGLYZA 2.5 mg, headache (6.5%) was the onlyadverse reaction reported at a rate ≥5% and more commonly than in patientstreated with placebo.In this pooled analysis, adverse reactions that were reported in ≥2% of patientstreated with ONGLYZA 2.5 mg or ONGLYZA 5 mg and ≥1% more frequentlycompared to placebo included: sinusitis (2.9% and 2.6% versus 1.6%,respectively), abdominal pain (2.4% and 1.7% versus 0.5%), gastroenteritis(1.9% and 2.3% versus 0.9%), and vomiting (2.2% and 2.3% versus 1.3%).In the add-on to TZD trial, the incidence of peripheral edema was higher forONGLYZA 5 mg versus placebo (8.1% and 4.3%, respectively). The incidenceof peripheral edema for ONGLYZA 2.5 mg was 3.1%. None of the reportedadverse reactions of peripheral edema resulted in study drug discontinuation.Rates of peripheral edema for ONGLYZA 2.5 mg and ONGLYZA 5 mg versusplacebo were 3.6% and 2% versus 3% given as monotherapy, 2.1% and 2.1%versus 2.2% given as add-on therapy to metformin, and 2.4% and 1.2% versus2.2% given as add-on therapy to glyburide.The incidence rate of fractures was 1.0 and 0.6 per 100 patient-years,respectively, for ONGLYZA (pooled analysis of 2.5 mg, 5 mg, and 10 mg) andplacebo. The incidence rate of fracture events in patients who receivedONGLYZA did not increase over time. Causality has not been established andnonclinical studies have not demonstrated adverse effects of saxagliptin onbone.An event of thrombocytopenia, consistent with a diagnosis of idiopathicthrombocytopenic purpura, was observed in the clinical program. Therelationship of this event to ONGLYZA is not known.
Adverse Reactions Associated with ONGLYZA (saxagliptin) Coad ministered with Metformin in Treatment-Naive Patients withType 2 DiabetesTable 2 shows the adverse reactions reported (regardless of investigatorassessment of causality) in ≥5% of patients participating in an additional24-week, active-controlled trial of coadministered ONGLYZA and metforminin treatment-naive patients.Table 2: Initial Therapy with Combination of ONGLYZA and Metformin
in Treatment-Naive Patients: Adverse Reactions Reported(Regardless of Investigator Assessment of Causality) in 5%of Patients Treated with Combination Therapy of ONGLYZA5 mg Plus Metformin (and More Commonly than in PatientsTreated with Metformin Alone)
Number (%) of PatientsONGLYZA 5 mg + Metformin* Metformin*
N=320 N=328Headache 24 (7.5) 17 (5.2)Nasopharyngitis 22 (6.9) 13 (4.0)
* Metformin was initiated at a starting dose of 500 mg daily and titrated upto a maximum of 2000 mg daily.
HypoglycemiaAdverse reactions of hypoglycemia were based on all reports of hypoglycemia;a concurrent glucose measurement was not required. In the add-on toglyburide study, the overall incidence of reported hypoglycemia was higher forONGLYZA 2.5 mg and ONGLYZA 5 mg (13.3% and 14.6%) versus placebo(10.1%). The incidence of confirmed hypoglycemia in this study, defined assymptoms of hypoglycemia accompanied by a fingerstick glucose value of ≤50 mg/dL, was 2.4% and 0.8% for ONGLYZA 2.5 mg and ONGLYZA 5 mg and0.7% for placebo. The incidence of reported hypoglycemia for ONGLYZA 2.5 mg and ONGLYZA 5 mg versus placebo given as monotherapy was 4.0%and 5.6% versus 4.1%, respectively, 7.8% and 5.8% versus 5% given asadd-on therapy to metformin, and 4.1% and 2.7% versus 3.8% given asadd-on therapy to TZD. The incidence of reported hypoglycemia was 3.4% intreatment-naive patients given ONGLYZA 5 mg plus metformin and 4.0% inpatients given metformin alone.Hypersensitivity ReactionsHypersensitivity-related events, such as urticaria and facial edema in the5-study pooled analysis up to Week 24 were reported in 1.5%, 1.5%, and 0.4%of patients who received ONGLYZA 2.5 mg, ONGLYZA 5 mg, and placebo,respectively. None of these events in patients who received ONGLYZA requiredhospitalization or were reported as life-threatening by the investigators. Onesaxagliptin-treated patient in this pooled analysis discontinued due togeneralized urticaria and facial edema.Vital SignsNo clinically meaningful changes in vital signs have been observed in patientstreated with ONGLYZA.Laboratory TestsAbsolute Lymphocyte CountsThere was a dose-related mean decrease in absolute lymphocyte countobserved with ONGLYZA. From a baseline mean absolute lymphocyte count ofapproximately 2200 cells/microL, mean decreases of approximately 100 and120 cells/microL with ONGLYZA 5 mg and 10 mg, respectively, relative toplacebo were observed at 24 weeks in a pooled analysis of fiveplacebo-controlled clinical studies. Similar effects were observed whenONGLYZA 5 mg was given in initial combination with metformin compared tometformin alone. There was no difference observed for ONGLYZA 2.5 mgrelative to placebo. The proportion of patients who were reported to have alymphocyte count ≤750 cells/microL was 0.5%, 1.5%, 1.4%, and 0.4% in thesaxagliptin 2.5 mg, 5 mg, 10 mg, and placebo groups, respectively. In mostpatients, recurrence was not observed with repeated exposure to ONGLYZAalthough some patients had recurrent decreases upon rechallenge that led todiscontinuation of ONGLYZA. The decreases in lymphocyte count were notassociated with clinically relevant adverse reactions.The clinical significance of this decrease in lymphocyte count relative toplacebo is not known. When clinically indicated, such as in settings of unusualor prolonged infection, lymphocyte count should be measured. The effect ofONGLYZA on lymphocyte counts in patients with lymphocyte abnormalities(e.g., human immunodeficiency virus) is unknown.PlateletsONGLYZA did not demonstrate a clinically meaningful or consistent effect onplatelet count in the six, double-blind, controlled clinical safety and efficacytrials.DRUG INTERACTIONSInducers of CYP3A4/5 EnzymesRifampin significantly decreased saxagliptin exposure with no change in thearea under the time-concentration curve (AUC) of its active metabolite,5-hydroxy saxagliptin. The plasma dipeptidyl peptidase-4 (DPP4) activityinhibition over a 24-hour dose interval was not affected by rifampin. Therefore,dosage adjustment of ONGLYZA is not recommended. [See ClinicalPharmacology (12.3).]Inhibitors of CYP3A4/5 EnzymesModerate Inhibitors of CYP3A4/5Diltiazem increased the exposure of saxagliptin. Similar increases in plasmaconcentrations of saxagliptin are anticipated in the presence of other moderateCYP3A4/5 inhibitors (e.g., amprenavir, aprepitant, erythromycin, fluconazole,fosamprenavir, grapefruit juice, and verapamil); however, dosage adjustmentof ONGLYZA is not recommended. [See Clinical Pharmacology (12.3).]Strong Inhibitors of CYP3A4/5Ketoconazole significantly increased saxagliptin exposure. Similar significantincreases in plasma concentrations of saxagliptin are anticipated with otherstrong CYP3A4/5 inhibitors (e.g., atazanavir, clarithromycin, indinavir,itraconazole, nefazodone, nelfinavir, ritonavir, saquinavir, and telithromycin).The dose of ONGLYZA should be limited to 2.5 mg when coadministered witha strong CYP3A4/5 inhibitor. [See Dosage and Administration (2.3) and ClinicalPharmacology (12.3).]
USE IN SPECIFIC POPULATIONSPregnancyPregnancy Category BThere are no adequate and well-controlled studies in pregnant women.Because animal reproduction studies are not always predictive of humanresponse, ONGLYZA (saxagliptin), like other antidiabetic medications, shouldbe used during pregnancy only if clearly needed.Saxagliptin was not teratogenic at any dose tested when administered topregnant rats and rabbits during periods of organogenesis. Incompleteossification of the pelvis, a form of developmental delay, occurred in rats at adose of 240 mg/kg, or approximately 1503 and 66 times human exposure tosaxagliptin and the active metabolite, respectively, at the maximumrecommended human dose (MRHD) of 5 mg. Maternal toxicity and reducedfetal body weights were observed at 7986 and 328 times the human exposureat the MRHD for saxagliptin and the active metabolite, respectively. Minorskeletal variations in rabbits occurred at a maternally toxic dose of 200 mg/kg,or approximately 1432 and 992 times the MRHD. When administered to ratsin combination with metformin, saxagliptin was not teratogenic norembryolethal at exposures 21 times the saxagliptin MRHD. Combinationadministration of metformin with a higher dose of saxagliptin (109 times thesaxagliptin MRHD) was associated with craniorachischisis (a rare neural tubedefect characterized by incomplete closure of the skull and spinal column) intwo fetuses from a single dam. Metformin exposures in each combination were4 times the human exposure of 2000 mg daily.Saxagliptin administered to female rats from gestation day 6 to lactation day20 resulted in decreased body weights in male and female offspring only atmaternally toxic doses (exposures ≥1629 and 53 times saxagliptin and itsactive metabolite at the MRHD). No functional or behavioral toxicity wasobserved in offspring of rats administered saxagliptin at any dose.Saxagliptin crosses the placenta into the fetus following dosing in pregnant rats.Nursing MothersSaxagliptin is secreted in the milk of lactating rats at approximately a 1:1 ratiowith plasma drug concentrations. It is not known whether saxagliptin issecreted in human milk. Because many drugs are secreted in human milk,caution should be exercised when ONGLYZA is administered to a nursingwoman.
Pediatric UseSafety and effectiveness of ONGLYZA in pediatric patients have not beenestablished.Geriatric UseIn the six, double-blind, controlled clinical safety and efficacy trials of ONGLYZA,634 (15.3%) of the 4148 randomized patients were 65 years and over, and59 (1.4%) patients were 75 years and over. No overall differences in safety oreffectiveness were observed between patients ≥65 years old and the youngerpatients. While this clinical experience has not identified differences inresponses between the elderly and younger patients, greater sensitivity ofsome older individuals cannot be ruled out.Saxagliptin and its active metabolite are eliminated in part by the kidney.Because elderly patients are more likely to have decreased renal function, careshould be taken in dose selection in the elderly based on renal function. [SeeDosage and Administration (2.2) and Clinical Pharmacology (12.3).]OVERDOSAGEIn a controlled clinical trial, once-daily, orally-administered ONGLYZA in healthysubjects at doses up to 400 mg daily for 2 weeks (80 times the MRHD) had nodose-related clinical adverse reactions and no clinically meaningful effect onQTc interval or heart rate.In the event of an overdose, appropriate supportive treatment should beinitiated as dictated by the patient’s clinical status. Saxagliptin and its activemetabolite are removed by hemodialysis (23% of dose over 4 hours).PATIENT COUNSELING INFORMATIONSee FDA-approved patient labeling.InstructionsPatients should be informed of the potential risks and benefits of ONGLYZAand of alternative modes of therapy. Patients should also be informed aboutthe importance of adherence to dietary instructions, regular physical activity,periodic blood glucose monitoring and A1C testing, recognition andmanagement of hypoglycemia and hyperglycemia, and assessment of diabetescomplications. During periods of stress such as fever, trauma, infection, orsurgery, medication requirements may change and patients should be advisedto seek medical advice promptly.Physicians should instruct their patients to read the Patient Package Insertbefore starting ONGLYZA therapy and to reread it each time the prescriptionis renewed. Patients should be instructed to inform their doctor or pharmacistif they develop any unusual symptom or if any existing symptom persistsor worsens.Laboratory TestsPatients should be informed that response to all diabetic therapies shouldbe monitored by periodic measurements of blood glucose and A1C, with agoal of decreasing these levels toward the normal range. A1C is especiallyuseful for evaluating long-term glycemic control. Patients should be informedof the potential need to adjust their dose based on changes in renal functiontests over time.
Manufactured by:
Princeton, NJ 08543 USA
Marketed by:
Bristol-Myers Squibb Company Princeton, NJ 08543andAstraZeneca Pharmaceuticals LP Wilmington, DE 19850
1256316 1256317 SA-B0001A-07-09 Iss July 2009
422US09AB12921_JA_OSFA.indd 2 1/27/10 1:08 PM
Reference:1. Fingertip Formulary® data as of October 25, 2009. Data on File, October 2009.
©2009 Bristol-Myers Squibb 422US09AB12921 12/09Onglyza™ is a trademark of Bristol-Myers Squibb
292613
For your adult patients with type 2 diabetes struggling to gain glycemic control
Signifi cant reductions in A1C whenpartnered with key oral antidiabetic agents*
• Onglyza is weight neutral
• Discontinuation of therapy due to adverse events
occurred in 3.3% and 1.8% of patients receiving
Onglyza and placebo, respectively
• Convenient, once-daily dosing
• Broad formulary coverage nationally1
– Accessible to almost 75% of patients†
Please read the adjacent Brief Summary of the Product Information. For more information about Onglyza, visit www.onglyza.com.
*metformin, glyburide, or thiazolidinedione (pioglitazone or rosiglitazone)†“Patients” means covered lives as calculated by Fingertip Formulary® as of 10/09.
Indication and Important Limitations of UseONGLYZA is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus.
ONGLYZA should not be used for the treatment of type 1 diabetes mellitus or diabetic ketoacidosis.
ONGLYZA has not been studied in combination with insulin.
Important Safety Information• Use with Medications Known to Cause
Hypoglycemia: Insulin secretagogues, such as sulfonylureas, cause hypoglycemia. Therefore, a lower dose of the insulin secretagogue may be required to reduce the risk of hypoglycemia when used in combination with ONGLYZA
• Macrovascular Outcomes: There have been no clinical studies establishing conclusive evidence of macrovascular risk reduction with ONGLYZA or any other antidiabetic drug
Most common adverse reactions (regardless of investigator assessment of causality) reported in ≥5% of patients treated with ONGLYZA and more commonly than in patients treated with control were upper respiratory tract infection (7.7%, 7.6%), headache (7.5%, 5.2%), nasopharyngitis (6.9%, 4.0%) and urinary tract infection (6.8%, 6.1%). When used as add-on combination therapy with a thiazolidinedione, the incidence of peripheral edema for ONGLYZA 2.5 mg, 5 mg, and placebo was 3.1%, 8.1% and 4.3%, respectively.
422US09AB12921_JA_OSFA.indd 1 1/27/10 1:08 PM





























