Embed Size (px)
Citation preview

US Prevalence of Down syndrome
1
Please cite as Supplemental Material for Presson et al.:
Presson AP, Partyka G, Jensen KM, Devine OJ, Rasmussen S, McCabe L, McCabe ERB (2013). "Current estimate of Down syndrome population prevalence in the United States." J Pediatr 163(4): 1163-1168. PMID: 23885965 http://www.sciencedirect.com/science/article/pii/S0022347613007269
Corresponding Author:
Edward RB McCabe, MD, PhD Senior Vice President, Medicine and Health Promotion Chief Medical Officer March of Dimes Foundation (Distinguished Professor Emeritus, Department of Pediatrics, and Inaugural Mattel Executive Endowed Chair of Pediatrics, UCLA School of Medicine, Inaugural Physician-in-Chief, Mattel Children’s Hospital UCLA) National Office 1275 Mamaroneck Avenue White Plains, NY 10605 T 914.997.4649 F 914.428.7849 [email protected]
SUPPLEMENTAL MATERIAL: TABLE OF CONTENTS METHODS AND RESULTS ...................................................................................................................................... 2
0. Details of data ascertainment and Monte Carlo methods ............................................................................ 2
1. Estimation of annual live births of people with DS for 1909-2008 ............................................................ 3
2. Estimation of age-specific annual deaths of people with DS for 1900-2007 ............................................... 5
3. Estimation of 2008 population size of people with DS using proportions of deaths ................................... 6
4. Estimation of projected population size of people with DS in 2100 ........................................................... 8
5. Analysis limitations ..................................................................................................................................... 8
SUPPLEMENTAL FIGURES .................................................................................................................................. 10
Figure S1 ....................................................................................................................................................... 10
Figure S2 ....................................................................................................................................................... 11
Figure S3 ....................................................................................................................................................... 12
Figure S4 ....................................................................................................................................................... 13
Figure S5 ....................................................................................................................................................... 15
SUPPLEMENTAL TABLES .................................................................................................................................... 16
Table S1 ........................................................................................................................................................ 16
Table S2 ........................................................................................................................................................ 19
Table S3 ........................................................................................................................................................ 22
REFERENCES .......................................................................................................................................................... 23

US Prevalence of Down syndrome
2
METHODS AND RESULTS
0. Details of data ascertainment and Monte Carlo methods US birth data (1940-2008)
US birth data by maternal age group for 1968-2008 were attained from the Centers for Disease Control and
Prevention (CDC) national vital statistics system data (NVSS)
(http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Births), and from CDC’s archival data for the years
1940 through 1968. Total US births were available for 1909-1994 at
(http://www.cdc.gov/nchs/data/statab/t941x01.pdf) and a subset of this data from 1909-1939 was used to estimate
numbers of US live births per maternal age group for these years.
US mortality data (1900-2007) and mortality data specific to people with DS (1968-2007)
Age-specific mortality data for the US and people with DS were obtained for 1968-2007 from the CDC at:
http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Mortality_Multiple. Data retrieved from these sources
included: age, sex, resident status, year, underlying cause of death, and either up to 14 or 20 contributory causes of
death depending on the availability of this auxiliary cause of death information. The imported data were filtered to
exclude foreign residents and separated into groupings based on ICD coding standards to reflect the use of ICDA-8
from 1968 through 1978, ICD-9 from 1979 through 1998 and ICD-10 from 1999 through 2007. The data were then
restricted to only records where either the underlying or any of the listed contributory causes contained an ICD
coding for DS (coded as 759.3, 758.0, and Q90). However, any DS associated records were excluded if pregnancy
termination was included as a cause of death (coded as 773,7796 and p96.4 for ICDA-8, ICD-9, and ICD-10,
respectively). Similarly, records with a pregnancy termination cause were excluded from US death certificates.
Total US deaths by ten year age group for 1900-1998 were available from the "unpublished tables" at
http://www.cdc.gov/nchs/nvss/mortality/hist290a.htm, and were used to estimate age-specific mortality for the US
population and for people with DS for 1900-1967.
US population size (January 1, 2008)

US Prevalence of Down syndrome
3
The Annual US population size for January 1, 2008 of 302,977,371 was obtained by averaging the July 1, 2007
(301,579,895) and July 1, 2008 (304,374,846) population sizes from the US Census Bureau
http://www.census.gov/popest/national/asrh/NC-EST2009-srh.html.
Population projection data (1999-2100)
The projected population size estimate of people with DS was based on middle and high projections for the US
population (1999-2100) available from the US Census Bureau
http://www.census.gov/population/www/projections/natdet-D3.html.1
Monte Carlo sampling methods
Monte Carlo (MC) sampling was used to estimate uncertainties in estimates of live births, deaths, and the population
size estimates of people with DS.2 The goal in using the MC approach was to propagate the uncertainties in the
various model inputs through to the final estimate for the number of persons living with DS. As a first step,
uncertainty distributions, as described below, were assigned to each model input parameter. The MC process was
then carried out by repeatedly sampling possible values for the parameters from these distributions and using the
sampled values to compute a collection of possible realizations for the final modeled estimate. In our application,
the MC process was repeated for 10,000 iterations resulting in an uncertainty distribution consisting of 10,000
possible estimates of the DS population size. The median of this distribution was considered to be the final DS
population size estimate, and the uncertainty associated with this estimate was summarized using the 5th and 95th
percentiles of the distribution to construct a 90% uncertainty interval (UI). At the start of each iteration all birth and
death counts were re-sampled using Poisson distributions with the distribution means set to total live births of people
with DS per year for 1909-2007 and age-specific mortality data of people with DS for 1968-2007. Uncertainty in
DS birth rates with maternal age categories was modeled by sampling from normal distributions, using published
rates of DS by maternal age as the distribution means. The assumed uncertainty distributions for other model input
parameters are described in the following sections.
1. Estimation of annual live births of people with DS for 1909-2008
US live births by maternal age were available for 1940-2008 for the following maternal age groups (in years): < 15,
15-19, 20-24, 25-29, 30-34, 35-39, 40-44, 45-49, and ≥50. Data were missing for the ≥50 year age group for 1964-

US Prevalence of Down syndrome
4
1996, and we imputed these missing values by extrapolating the available age-specific birth rates using a non-
parametric loess smoothing function in R (supsmu). 3 Total US live births were available for 1909-1994, and this
information for 1909-1939 along with the relative proportions of child-bearing women by age were used to estimate
the number of live births per maternal age group back to 1909. Uncertainty in the annual live births per maternal
age group was estimated using a Poisson distribution with a mean value assumed to be equal to the rate observed in
the final two years of US data (1940-1941) multiplied by the average population size for 1909-1939. Using the
complete numbers of US live births by maternal age group for 1909-2007, we estimated total births of people with
DS (where total includes live births, stillbirths, and abortions) using birth rates for people with DS by maternal age
group. The Carothers et al.4 rates used births by individual year of maternal age in an English cohort along with
age-specific rates for people with DS provided by Hecht and Hook5 to derive the following rates per 1,000 live
births for five year maternal age groups: 15-19 = 0.60, 20-24 = 0.71, 25-29 = 0.91, 30-34 = 1.54, 35-39 = 4.24, 40-
44 = 16.22, and 45-49 = 53.3. These rates were considered to be reliable over time, location and across ethnic
groups.4 Younger <15 year and older 50+ year rates were not available and were thus estimated from a non-
parametric loess smoothing function in R (supsmu)3 as 0.49 for <15 years and 84..85 for women ≥50 years of age.
Uncertainty associated with these parameters was described using a normal distribution with means set to the
estimated rates and standard deviations for each age group set to the values from Table 2 of Hecht and Hook.5
Samples for possible values of these rates were truncated at zero (by re-sampling if values were less than zero) and
required to increase with increasing age group (for example, the rate for 20-24 year olds was greater than the rate for
15-19 year olds, but less than the rate for 25-29 year olds). These sampled rates were applied to the total US live
birth numbers by maternal age group to estimate total births for people with DS.
The Carothers et al.4 estimates included live births and elective pregnancy terminations; but we were only interested
in the annual numbers of live births of people with DS. As a result, we reduced the annual birth estimates of people
with DS from 1980 onwards by a selected amount corresponding to the difference in prevalence per 10,000 births
presented in Parker et al. Table 3 between live births 13.51 and live births plus pregnancy terminations 15.45 (15.45
= 13.51 + 16.08 – 14.14).6 We chose to start this adjustment in 1980 because while abortions and prenatal tests for
DS were available in the 1970s, elective pregnancy terminations did not become widespread until the early 1980s.4, 7
We directly applied each sampled rate rather than adjusting it over time because the elective termination rate has
been shown to be fairly constant in the US throughout the 1980s and 1990s.8 Uncertainty in the percentage

US Prevalence of Down syndrome
5
reduction in annual birth estimates was modeled using two Poisson distributions with mean rates of 575 and 658
corresponding to the number of live and live births plus pregnancy terminations , respectively.6 These mean rates
were estimated from the Parker et al. Table 3 prevalence rates6 and an estimate of the total number of births for
Georgia, Iowa and Utah for 2002-2006 (709,778). 9 We estimated the total number of births for 2004-2006 as
3/5*(709,778) = 425,867, and multiplying this value by the prevalance rates gave the mean rates of live births 575
and total births 658.. The sampled total births was required to exceed the sampled live births, and the adjustment for
pregnancy terminations was then given by: 100%*(live births/total births), where the average was 100%*(1-
575/658) = 12.61%. We did not need to adjust for stillbirths because they were not included in the Carothers et al.
estimates.4, 10 Each iteration in the MC process provided an estimate for the number of annual births of people with
DS by year for 1909-2008, and after 10,000 iterations we computed the median of the distribution to provide the
final estimates.
2. Estimation of age-specific annual deaths of people with DS for 1900-2007
Age-specific US deaths and deaths of people with DS were available for 1968-2007. Data were missing from both
data sets for 1980 and were estimated for the people with DS by averaging the age-specific values for 1979 and
1981. Deaths by age in 1972 were multiplied by two as instructed in the Mortality User's guide for 1968-78 (page
2). Total US deaths by age group (in years) <1, 1-4, 5-14, 15-24, 25-34, 35-44, 45-54, 55-64, 65-74, 75-84, 85+, and
unknown, were available for 1900-1968 and were used to estimate US deaths by age for 1909-1967, where the
unknown group was distributed proportionately among the known age groups for each year. Age-specific deaths
were averaged for 1968-1969 and used to estimate age-specific US mortality for 1900-1967, Uncertainty in these
estimates was modeled using a Poisson distribution with the mean number of deaths set to the observed value. Next,
we estimated the average fraction of DS-associated deaths by age for 1968-1969. We chose to use only the final two
years of data due to the variability in mortality rates of people with DS over time and across age groups (Fig. 2). We
averaged the age-specific mortality of people with DS for 1968-1969, re-sampled these values from an assumed
Poisson uncertainty distribution, and divided each sampled value by a realization for the corresponding average US
age-specific mortality for those years sampled from an independent Poisson uncertainty distribution. These ratios
provide an estimate of the US population's fraction of DS-associated mortality by age. Finally, we adjusted the
mortality for 1999-2007 due to the change from ICD-9 to ICD-10 as described in the following section.

US Prevalence of Down syndrome
6
Correction to 1999-2007 ICD-10 mortality data
Mortality data were derived from several versions of International Cause of Death (ICD) codes, where ICDA-8 was
effective 1968-1978, ICD-9 was effective 1979-1998 and ICD-10 was effective for 1999-2007. Comparability
ratios for ICD-10 and ICD-9 codes were published for 113 causes of death in adults and 130 causes of death in
infants by categorizing death certificate data from 80% of US deaths in 1996 according to both ICD-10 and ICD-9
codes.11 Comparability data were available in adults for the parent category of Down syndrome: "Congenital
malformations, deformations and chromosomal abnormalities" where the comparability ratio C = ICD-10/ICD-9 =
5,950/7,025 = 0.847 and its confidence interval (95% CI: 0.8362-0.8577) indicated an under-count for Down
syndrome in ICD-10. In infants the comparability ratio for Down syndrome included 1.0, and thus we did not
correct ICD-10 mortality data for ages < 1. To reflect uncertainty in ICD comparability, we sampled ICD-10 and
ICD-9 counts of people with DS from independent Poisson distributions with means equal to 5,950 and 7,025,
respectively. Only samples in which the ICD-9 count exceeded ICD-10 were retained in the MC estimation, and the
comparability ratio C was formed by taking the ratio of the two samples. We corrected the ICD-10 codes by
multiplying by 1/C with the intent to improve homogeneity since the ICD-10 codes covered a shorter period of time
and since we expected ICD-9 to be more similar to ICD-8. The end result was an estimate of age-specific mortality
of people with DS by year for 1909-2007.
3. Estimation of 2008 population size of people with DS using proportions of deaths
Annual estimated deaths are likely to be less accurate than annual estimated births because these data are more
likely to suffer from under-reporting. Each death certificate consists of an underlying cause with up to 14-20 co-
morbidities, so that if a person died in a manner that was clearly unrelated to DS, DS may not have been recorded as
a co-morbidity.12, 13 Since the annual death certificate records reported ages, it was possible to estimate the number
of deaths that occurred by 2008 among people born in 1909. This estimate was 2,742 deaths, which given that there
were 4,528 births in 1909 would imply that 1,786 people with DS born in 1909 were still alive in 2008. Since this
was highly implausible, and because we had more confidence in the birth estimates, we decided to hinge our
population size estimate on the birth data and proportions of deaths by age rather than absolute death counts. We
adopted a time-specific life table approach, where death rates were fixed at a certain point in time, to form several
estimates of population size of people with DS for Jan 1st, 2008.14 We report population size estimates based off of

US Prevalence of Down syndrome
7
proportions of deaths by age from 1) the two most recent years of death certificate data (2006-2007), 2) the ten most
recent years (1998-2007), 3) two sets of death certificate data: applying death certificate data from 2006-2007 to
birth data from 1970-2007 and applying death certificate data from 1968-1969 to birth data from 1909-1969, and 4)
matching death certificate years with birth certificate years. The final method is similar to a time-varying life table
approach, but it is limited by the fact that we are using proportions of deaths from different time points (thus they
did not sum to one across ages). The proportions corresponding to births from 1909 could be standardized to 1 since
1909-2007 covers a full generation of people with DS (assuming a maximum life span of 98 years), but with each
advancing year the generation coverage diminishes so that we cannot acquire proportions of all ages 0.98 and thus
they cannot be standardized to sum to one across ages. As a result, the counts of 2008 survivors born between 1909
and 1965 were negative and were set to zero.
We estimated modern death rates da for a person age a from death certificate data for 2006-2007, by summing the
total age-specific deaths and dividing by the total deaths that occurred over this 2-year time frame
∑ /∑ ∑ , assuming a maximum life span for a person with DS of 98 years, where nay is
the number of deaths that occurred for age a in year y. The proportion of individuals with DS surviving to greater
than a years, or the "life expectancy", sa, is given by 1 ∑ . We refer to the number of deaths that have
occurred for a specific birth year as "cohort deaths", and similarly the number of survivors by birth year as "cohort
survivors". The number of cohort survivors for year y in 2007 is given by Py = s2007-y * By where By is the number of
births in year y, and summing the cohort survivors who were born in 1909-2007: ∑ estimates the January 1,
2008 population size of people with DS. In this manner we obtained the following population size estimates: 1)
using the two most recent years of death certificate data (2006-2007) the population size was estimated as 250,700
(90% UI: 185,900 – 321,700), 2) using the final 10 years of data (1998-2007) gave 241,000 (90% UI: 178,500 –
309,000), 3) using two sets of death certificate data 2006-2007 for births from 1970-2007 and 1968-1969 for births
from 1909-1968 estimated 180,400 (90% UI: 134,100 – 231,400, and 4) matching death certificate years with birth
certificate years yielded 133,200 (90% UI: 97,900 – 172,500). While these methods yield different prevalence
estimates, most of the 90% UIs overlap, with the exception of the prevalence estimates from Methods 1 and 4. As
noted above, a problem with Method 4 is that the proportions of deaths by age did not sum to one since they were
derived from different years of mortality data. This could explain why the Method 4 estimate is notably lower than
the others.

US Prevalence of Down syndrome
8
To validate our approach we similarly estimated the US population size for January 1, 2008 using all four of the
estimation methods. Since there were few variables for estimating the US population size, the resulting uncertainty
intervals were much smaller. The population size estimates for the full US population were 1) 258,832,900 (90%
UI:258,750,300-258,915,700), 2) 258,881,900 (95% UI:258,810,900-258,953,600), 3) 240,870,100 (90%
UI:240,791,100-240,949,900), and 4) 236,617,200 (90% UI:236,586,700-236,647,300). Method 2 was very similar
to Method 1, but Methods 3-4 were 6.9 and 8.6% lower than Method 1. The Method 1 estimate was about 14.6%
lower than the actual US population size which was 302,977,371, but it gave the closest estimate. Thus we consider
the Method 1 estimate to be the most defensible, and we present only this method in the main text. It is possible that
the population size of people with DS could also be about 14.6% higher, which would be 293,600 for Method 1.
Note that this size would be covered by our uncertainty interval 185,900 – 321,700.
4. Estimation of projected population size of people with DS in 2100
The US Census Bureau provides low, middle, and high projections for the US population size through 2100. The
middle projection for 1/1/2008 was 293,855,190, and there was a projected 1.94-fold increase to 569,162,440 for
1/1/2100. The high projection for 1/1/2008 was 301,456,107, and there was a projected 3.89-fold increase to
1,173,850,547 for 1/1/2100. These projections were made for 1999-2100, and the actual population size in 1/1/2008
was 302,977,371. Thus it is possible that both projections could underestimate the true population size in 2100.
5. Analysis limitations
A major limitation of our analysis is the under-reporting of the diagnosis of Down syndrome in death certificate data
which led to using only proportions of age-specific deaths rather than actual numbers for estimating the population
size of people with DS.12,13 By using this proportion-based approach, we made the unverifiable assumption that the
level of underreporting in death certificates is the same across all causes of death. Furthermore, our population size
estimate was derived from 1) estimated births based on maternal rates of DS that were then adjusted by a pregnancy
termination rate, and 2) death certificate data for 2006-2007 that had to be adjusted by an ICD9/ICD10 conversion
ratio. All of these inputs were themselves estimates, and introduced variability into our population size estimate.
We attempted to address the limitations of these estimates using Monte Carlo sampling to provide uncertainty
intervals. However this approach assumes independence between the input estimates, which is probably an
unreasonable assumption. Thus, the UIs likely underestimate uncertainty. Finally, our life table approach

US Prevalence of Down syndrome
9
incorrectly assumes that the population size and the age-structure are constant over time. We attempted to address
this limitation by using two different age-structures (2006-2007 and 1968-1969) and a time varying age structure
(see the Methods and Results section of the Supplementary Appendix). However, the resulting population estimates
were lower for both the US population (6.9% and 8.6%, respectively) and the DS prevalence estimates (28% and
47%, respectively) than the estimate achieved using 2006-2007 death certificate data. Since the US population size
estimate achieved using 2006-2007 death certificate data was closest to the actual population size for January 1st,
2008, we considered this estimation procedure to be the most defensible.

US Prevalence of Down syndrome
10
SUPPLEMENTAL FIGURES
Figure S1. Diagram of birth and death data ascertainment for people with DS. A The number of births of
people with DS was estimated using US birth data and DS rates by maternal age published by Carothers et al.4 B
Mortalities of people with DS were estimated from US mortality data on the full population and death certificates
that listed DS as an associated condition. The dashed brackets indicate estimated data. The numbers 1-8 refer to the
following data sources: 1. US Births (http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Births), 2. CDC
historic archives, 3. Total US Births (http://www.cdc.gov/nchs/data/statab/t941x01.pdf), 4. DS rates from Carothers
et al.,4 5. Adjustment to rates, 6. US deaths
(http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Mortality_Multiple), 7. US Deaths
(http://www.cdc.gov/nchs/nvss/mortality/hist290a.htm), 8. Deaths of people with DS
(http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Mortality_Multiple)
A Births of people with DS
B Deaths of people with DS

US Prevalence of Down syndrome
11
Figure S2. Deaths for the US population and percent of deaths among people with DS for 1909-2007. This plot
shows an alternative view of Figure 1B where annual deaths of people with DS have been standardized to the total
US deaths. Blue corresponds to the US population and red corresponds to the population of people with DS. Solid
lines indicate 50th percentile estimates from Monte Carlo sampling for both the US and DS data. Dashed lines
indicate a 90% uncertainty interval (UI) for the DS data. The UI is absent from the US data because they are too
narrow.
0.00%
0.05%
0.10%
0.15%
0.20%
0.25%
0.30%
0.35%
0.40%
0.45%
0.50%
0
500,000
1,000,000
1,500,000
2,000,000
2,500,000
3,000,000
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
% Deaths Among People with DS
US Deaths
Year
US Deaths% Deaths Among People with DS90% UI for People with DS

US Prevalence of Down syndrome
12
Figure S3. Births of people with DS by 5-year maternal age group (1909-2008). Births of people with DS by
maternal age group are plotted below for Carothers et al.4 birth rates, where the birth numbers were adjusted for
pregnancy terminations as described in the Methods and Results section of the Supplementary Appendix. From
1980 onward there is a trend for more births of people with DS to older women (> 30 years). The black line
corresponds to 50th percentile estimates from Monte Carlo sampling. Grey lines indicate 90% uncertainty intervals.
1920 1940 1960 1980 2000
04
812
<15
Year
1920 1940 1960 1980 2000
100
400
700
15-19
Year
# B
irths
1920 1940 1960 1980 2000
400
800
1200
20-24
Year
# B
irths
1920 1940 1960 1980 2000
400
800
1400
25-29
Year
1920 1940 1960 1980 2000
500
1500
30-34
Year
# B
irths
1920 1940 1960 1980 20000
1500
3000
35-39
Year
# B
irths
1920 1940 1960 1980 2000
010
0025
00
40-44
Year
1920 1940 1960 1980 2000
040
080
0
45-49
Year
# B
irths
1920 1940 1960 1980 2000
020
4060
>49
Year
# B
irths
50th percentile
90% UI

US Prevalence of Down syndrome
13
Figure S4. Deaths in the US and among people with DS for select ages (1900-2007). Blue indicates US deaths,
and red corresponds to deaths among people with DS. The patterns align well for ages < 5, with a notable peak in
deaths around 1918-1920 due to the influenza pandemic. The older age groups show increasing deaths among
individuals with DS since 1980 due to more people with DS surviving to 35+ years.

US Prevalence of Down syndrome
14
0
1,000
2,000
3,000
0
20,000
40,000
60,000
80,000
100,000
120,000
1900 1950 2000
Deaths of people with
DS
1‐4 Years
0
200
400
0
50,000
100,000
150,000
200,000
1900 1950 2000
US Deaths
Year
35‐44 Years
0
1,000
2,000
0
1,000,000
2,000,000
3,000,000
1900 1950 2000
Deaths of people with
DS
Year
45+ Years
0
500
1000
1500
2000
0
50000
100000
150000
200000
1900 1950 2000
US Deaths
<1 YearUS Deaths
Deaths of people with DS

US Prevalence of Down syndrome
15
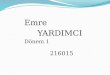
Figure S5. Relative deaths of people with DS by age from 1900-2007 and relevant historic events. Alternate
view of Figure 2 where panel A shows relative deaths by age and panel B shows a timeline of historic events.
Figure S5. Relative deaths of people with DS by age from 1900-2007 and relevant historic events. Alternate view of Figure 2 where panel A shows relative deaths by age and panel B shows a timeline of historic events.
1960 Birth Control Pill: Birth rate decrease due to contraception.
1946‐1964 Baby Boom: Birth rate increase due to
return of soldiers.
1929‐1941 Great
Depression: Birth rate decrease.
1941‐1945 World War II: Birth rate decrease due to deployment of
soldiers.
Early 1950s‐1975 Deinstitutionalization: Parents pushed for equal rights for
handicapped children, culminating in the 1975 Education for Handicapped Children Act. Resulted in improved health and life
expectancy of children with DS.
1980‐1990s Pre‐natal
testing for DS: Birth rate decrease.
1990 Surgery for DS: Life expectancy increase in children with congenital
heart defects.
1918‐1920 Flu Pandemic: Children, elderly and
people with DS have higher mortality due to a weakened
immune system.
B Timeline
0%
10%
20%
30%
40%
50%
60%
1900 1910 1920 1930 1940 1950 1960 1970 1980 1990 2000 2010
% Deaths
<1
1‐4
5‐24
25‐44
45‐64
65‐84
85+
A Relative deaths among people with DS by year and age group

US Prevalence of Down syndrome
16
SUPPLEMENTAL TABLES
Table S1. Data sources, estimates, and sampling distributions for the Monte Carlo uncertainty model
organized by model input component (births, deaths).
Model
Compo
nent
Model Input
Parameters Data Source Estimate
Sampling
distribution
Births
Number of USA
live births by
maternal age
(1968‐2008)
Centers for Disease
Control and Prevention
(CDC) National Vital
Statistics System (NVSS)
http://www.cdc.gov/nchs/da
ta_access/Vitalstatsonline.ht
m#Births
Independent
Poisson
distributions
Births
Number of USA
live births by
maternal age
(1940‐1967)
CDC archival data Available upon request
Independent
Poisson
distributions
Births
Annual live
USA births
1909‐1939
CDC NVSS data http://www.cdc.gov/nchs/da
ta/statab/t941x01.pdf
Independent
Poisson
distributions
Births
Rates of births
with DS per
1000 births by
5‐year
maternal age
Carothers et al.4
15‐19 = 0.60, 20‐24 = 0.71,
25‐29 = 0.91, 30‐34 = 1.54,
35‐39 = 4.24, 40‐44 = 16.22,
and 45‐49 = 53.3
Normal, with
non‐negative
values, and
increasing
values for

US Prevalence of Down syndrome
17
group 15‐49 increasing
maternal age
Births
Rates of births
with DS per
1000 births by
maternal age
<15 years and
>49 years
Estimated from Carothers
et al. 4 <15 = 0∙49 and >49 = 84∙85
Births
Standard
deviations for
rates of births
with DS by
maternal age
Hecht and Hook5 Table 2
<15 = 0∙30, 15‐19 = 0∙30, 20‐
24 = 0.10, 25‐29 = 0.21, 30‐34
= 0.40, 35‐39 = 2.19, 40‐44 =
10.28, 45‐49 = 43.65, and >49
= 43.65
Births
Pregnancy
terminations
from 1980
onward
Parker et al.6 Table 3,
NBDPN
575 live births versus 658 live
births + pregnancy
terminations: 100%*(1‐
575/658) = 12.61%
Two
independent
Poisson
distributions
with means of
575 and 658;
required total
births to
exceed live

US Prevalence of Down syndrome
18
births
Deaths
Age‐specific
USA deaths
(1968‐2007)
CDC NVSS data (see
Supplemental Methods
and Results for filtering
details)
http://www.cdc.gov/nchs/da
ta_access/Vitalstatsonline.ht
m#Mortality_Multiple
Independent
Poisson
distributions
Deaths
Age‐specific
deaths of
people with DS
(1968‐2007)
CDC NVSS data (see
Supplemental Methods
and Results for filtering
details)
http://www.cdc.gov/nchs/da
ta_access/Vitalstatsonline.ht
m#Mortality_Multiple
Independent
Poisson
distributions
Deaths
Total USA
deaths by 10‐yr
age group
(1900‐1967)
CDC NVSS data (see
Supplemental Methods
and Results for filtering
details)
http://www.cdc.gov/nchs/nv
ss/mortality/hist290a.htm
Independent
Poisson
distributions
Deaths
Age‐specific
USA deaths
(1900‐1967)
Estimated from age‐
specific USA deaths (1968‐
1969) and total USA
deaths by age 1900‐1967
http://www.cdc.gov/nchs/da
ta_access/Vitalstatsonline.ht
m#Mortality_Multiple
Independent
Poisson
distributions
Deaths
Age‐specific
deaths of
people with DS
Estimated by average
fraction of age‐specific
USA deaths that were due
http://www.cdc.gov/nchs/da
ta_access/Vitalstatsonline.ht
Independent
Poisson

US Prevalence of Down syndrome
19
(1900‐1967) to DS in 1968‐1969 m#Mortality_Multiple distributions
Deaths
Correction
factor for ICD‐
10 to ICD‐9
(applied to
deaths from
1999‐2007)
Anderson et al. 11
5950 deaths by ICD‐10 versus
7025 by ICD‐9: 7025/5950 =
1∙18
Two
independent
Poisson
distributions
with means of
5950 and
7025,
required ICD‐
9 to exceed
ICD‐10
Table S2. Birth prevalence of people with DS in published studies. We compared published empirical estimates
of birth prevalence of people with DS with our live birth estimates based on Carothers et al.4 birth rates adjusted for
pregnancy terminations. Population refers to the study population and/or the population relevant to the reported
prevalence estimate. “Year” refers to the years during which the study data was collected. Prevalence estimates are
per 10,000 live births. “Our Study - Births” refers to the average number of births of people with DS during the
time frame specified by “Year”. Our estimates are on average 15.84% higher than the empirical studies, ranging
from 26.81% lower to 42.43% higher.

US Prevalence of Down syndrome
20
Study Year Population
US Live
Birthsa
Other Study Our Study %
DifferencePrevalence Birthsb Prevalenceb Births
Shin et al. 200915 1979 10 states Live Births
3494516 9.00 3,145 11.49 4,015 21.67%
Besser et al.
200716 1979-1983 Atlanta Live Births
3611240 8.90 3,214 10.53 3,802 15.48%
Berry et al. 201017 1980's US Live Births
3750870 14.00 5,251 11.04 4,140 -26.81%
Forrester et al.
200218 1986-1997 Hawaii Live Births
3956445 8.67 3,430 13.01 5,147 33.36%
Egan et al. 200819 1989 US Live Births
4041107 11.07 4,474 12.22 4,937 9.41%
Berry et al. 201017 1989-1996 US Live Births
4015076 12.00 4,818 13.29 5,335 9.71%
Canfield et al.
200620 1999-2001 11 states Total Births
4014719 13.65 5,480 15.45 6,204 11.65%
Shin et al. 200915 2003 10 states Live Births
4089969 11.80 4,826 16.13 6,599 26.84%
Besser et al.
200716 2003 Atlanta Live Births
4089969 13.00 5,317 16.13 6,599 19.40%
Parker et al. 20106 2004-2006
24 programs Total
Births
4171973 14.47 6,037 16.28 6,793 11.12%

US Prevalence of Down syndrome
21
Egan et al. 200819 2006 US Live Births
4265497 9.35 3,988 16.24 6,929 42.43%
aAverage annual number of US live births during the specified time period (Year). Average15.84%
bEstimates were based off of the US live births data.

US Prevalence of Down syndrome
22
Table S3. Mean, median, 25th and 75th percentiles for age at death among people with DS from 1983-2007 vs.
Yang et al.12 A comparison of the mean, median, and interquartile range of age at death by year for people with DS
between A theYang et al.12 study and B our study. The Yang et al.12 study covered 1983-1997, so we provide values
starting in 1983 but extending through 2007. Values are nearly identical because they were derived from the same
national registry of death certificate data
(http://www.cdc.gov/nchs/data_access/Vitalstatsonline.htm#Mortality_Multiple).
A Yang et al. 2002 B This Study
Year Mean Median 0.25 0.75 Mean Median 0.25 0.75
1983 27.7 25 1 53 27.8 25 1 53
1984 29.0 28 1 55 29.0 28 1 55
1985 31.0 32 1 55 31.1 32 1 55
1986 30.6 31 1 54 30.6 31 1 54
1987 31.4 34 1 56 31.4 34 1 56
1988 30.9 32 1 56 30.8 32 1 56
1989 32.8 36 1 56 32.9 36 1 56
1990 32.7 36 1 56 32.7 36 1 56
1991 33.4 38 2 56 33.3 38 2 56
1992 33.9 39 1 57 33.8 39 1 57
1993 37.6 45 15 58 37.6 45 15 58
1994 39.1 47 21 58 39.1 47 21 58
1995 39.4 47 24 58 39.5 47 24 58
1996 39.2 47 22 58 39.3 47 22 58
1997 41.4 49 25 59 41.4 49 25 59
1998 ‐‐ ‐‐ ‐‐ ‐‐ 40.3 49 23 58
1999 ‐‐ ‐‐ ‐‐ ‐‐ 43.1 50 33 58
2000 ‐‐ ‐‐ ‐‐ ‐‐ 42.9 50 31 59
2001 ‐‐ ‐‐ ‐‐ ‐‐ 43.3 51 32 59
2002 ‐‐ ‐‐ ‐‐ ‐‐ 43.3 51 33 59
2003 ‐‐ ‐‐ ‐‐ ‐‐ 45.2 52 38 59
2004 ‐‐ ‐‐ ‐‐ ‐‐ 49.1 54 41 62
2005 ‐‐ ‐‐ ‐‐ ‐‐ 45.7 53 38 59
2006 ‐‐ ‐‐ ‐‐ ‐‐ 46.0 53 39 59
2007 ‐‐ ‐‐ ‐‐ ‐‐ 47.3 53 42 60

US Prevalence of Down syndrome
23
REFERENCES
1. Hollmann FW, Mulder TJ, Kallan JE. Methodology and Assumptions for the Population Projections of the United States: 1999 to 2100. Population Division Working Paper No 38 2000. 2. Schieve LA, Devine O, Boyle CA, Petrini JR, Warner L. Estimation of the contribution of non‐assisted reproductive technology ovulation stimulation fertility treatments to US singleton and multiple births. Am J Epidemiol 2009; 170(11): 1396‐407. 3. Friedman JH. A variable span scatterplot smoother: Laboratory for Computational Statistics, Stanford University, 1984. 4. Carothers AD, Hecht CA, Hook EB. International variation in reported livebirth prevalence rates of Down syndrome, adjusted for maternal age. J Med Genet 1999; 36(5): 386‐93. 5. Hecht CA, Hook EB. Rates of Down syndrome at livebirth by one‐year maternal age intervals in studies with apparent close to complete ascertainment in populations of European origin: a proposed revised rate schedule for use in genetic and prenatal screening. Am J Med Genet 1996; 62(4): 376‐85. 6. Parker SE, Mai CT, Canfield MA,Rickard R, Wang Y, Meyer RE et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004‐2006. Birth Defects Res A Clin Mol Teratol 2010; 88(12): 1008‐16. 7. Canick J. Prenatal screening for trisomy 21: recent advances and guidelines. Clin Chem Lab Med 2011. 8. Mansfield C, Hopfer S, Marteau TM. Termination rates after prenatal diagnosis of Down syndrome, spina bifida, anencephaly, and Turner and Klinefelter syndromes: a systematic literature review. European Concerted Action: DADA (Decision‐making After the Diagnosis of a fetal Abnormality). Prenat Diagn 1999; 19(9): 808‐12. 9. Population‐based Birth Defects Surveillance data from selected states, 2002‐2006. Birth Defects Res A Clin Mol Teratol 2009; 85(12): 939‐1055. 10. Leoncini E, Botto LD, Cocchi G, Anneren G, Boser C, Halliday J,et al. How valid are the rates of Down syndrome internationally? Findings from the International Clearinghouse for Birth Defects Surveillance and Research. Am J Med Genet A 2010; 152A(7): 1670‐80. 11. Anderson RN, Minino AM, Hoyert DL, Rosenberg HM. Comparability of cause of death between ICD‐9 and ICD‐10: preliminary estimates. Natl Vital Stat Rep 2001; 49(2): 1‐32. 12. Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down's syndrome in the USA from 1983 to 1997: a population‐based study. Lancet 2002; 359(9311): 1019‐25. 13. Friedman JM. Racial disparities in median age at death of persons with Down syndrome‐‐United States, 1968‐1997. MMWR Morb Mortal Wkly Rep 2001; 50(22): 463‐5. 14. Putnam RJ, Wratten SD. Principles of ecology. Berkley and Los Angeles, CA: University of California Press; 1984. 15. Shin M, Besser LM, Kucik JE, Lu C, Siffel C, Correa A. Prevalence of Down syndrome among children and adolescents in 10 regions of the United States. Pediatrics 2009; 124(6): 1565‐71. 16. Besser LM, Shin M, Kucik JE, Correa A. Prevalence of down syndrome among children and adolescents in metropolitan Atlanta. Birth Defects Res A Clin Mol Teratol 2007; 79(11): 765‐74. 17. Berry JG, Bloom S, Foley S, Palfrey JS. Health inequity in children and youth with chronic health conditions. Pediatrics 2010; 126 Suppl 3: S111‐9. 18. Forrester MB, Merz RD. Epidemiology of Down syndrome (Trisomy 21), Hawaii, 1986‐97. Teratology 2002; 65(5): 207‐12. 19. Egan J, Benn P, Turner G, Spencer J, Smith K, Campbell W. An update on trends in down syndrome livebirths in the U.S. from 1989 to 2005. Society for maternal‐fetal medicine (SMFM): American Journal of Obstetrics & Gynecology; 2008. p. S168.

US Prevalence of Down syndrome
24
20. Canfield MA, Honein MA, Yuskiv N, et al. National estimates and race/ethnic‐specific variation of selected birth defects in the United States, 1999‐2001. Birth Defects Res A Clin Mol Teratol 2006; 76(11): 747‐56.