Embed Size (px)
Citation preview

Use Irinotecan or a Taxane for Use Irinotecan or a Taxane for 22ndnd Line GE Cancer Therapy: Line GE Cancer Therapy:
Don’t Use What Dr. Fuchs Don’t Use What Dr. Fuchs Tells You to UseTells You to UseJordan D. Berlin, M.D.
Ingram Professor of Cancer Research
Co-director, GI Oncology
Director, Phase I Research
Vanderbilt-Ingram Cancer Center

DisclosuresDisclosures
• Advisory Boards here and there in last year– Genentech/Roche– Karyopharm– Amgen – Astra Zeneca– BMS– Lilly/Imclone– Symphogen– Celgene– Vertex– Ipsen
• Current Research Support– Amgen, Lilly/Imclone,
Pfizer, Novartis, Abbvie, Immunomedics, Otsuka, Merrimack, Oncomed, Genentech/Roche, Taiho

So what is the data for second-line So what is the data for second-line chemotherapy?chemotherapy?

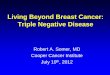
Fig. 2 Overall survival (intention to treat population) Median survival Irinotecan: 4.0 months, BSC: 2.4 months; one sided logrank test: p = 0.012; HR: 0.48 (95% CI: 0.25–0.92).
Peter C. Thuss-Patience , Albrecht Kretzschmar , Dmitry Bichev , Tillman Deist , Axel Hinke , Kirstin Breithaupt ,...European Journal of Cancer, Volume 47, Issue 15, 2011, 2306 - 2314
AIO: Small trial of irinotecan vs BSC

Salvage Chemotherapy for Pretreated Salvage Chemotherapy for Pretreated Gastric Cancer: A Randomized Phase Gastric Cancer: A Randomized Phase
III Trial Comparing Chemotherapy Plus III Trial Comparing Chemotherapy Plus Best Supportive Care With Best Best Supportive Care With Best
Supportive Care AloneSupportive Care Alone
Jung Hun Kang, Soon Il Lee, Do Hyoung Lim, Keon-Woo Park,
Sung Yong Oh, Hyuk-Chan Kwon, In Gyu Hwang, Sang-Cheol
Lee, Eunmi Nam, Dong Bok Shin, Jeeyun Lee, Joon Oh Park,
Young Suk Park, Ho Yeong Lim, Won Ki Kang and Se Hoon
Park⇑
JCO Aug 20, 2012:3035

Next 2Next 2ndnd line Chemotherapy (SLC) RCT line Chemotherapy (SLC) RCT
Refused RCT, but prefer SLC
Willing to participate RCT
Screening & consent for RCT
Refused RCT, but prefer BSC
SLC SLC BSC BSC
2:1 randomization
RCT
RCT + PPT
Docetaxelor irinotecan
ClinicalTrials.gov,NCT00821990
RCT: randomized controlled trialPPT: patient-preference trial
N = 202
From Park ASCO 2011

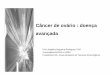
Kaplan-Meier estimates for overall survival in randomly assigned patients.
Kang J H et al. JCO 2012;30:1513-1518©2012 by American Society of Clinical Oncology
OS 5.3 vs 3.8 months, HR 0.66, p = 0.007

COUGAR-02: Randomised phase III study of COUGAR-02: Randomised phase III study of docetaxel versus active symptom control in patients docetaxel versus active symptom control in patients
with relapsed esophago-gastric adenocarcinomawith relapsed esophago-gastric adenocarcinoma
N Cook, A Marshall, JM Blazeby, JA Bridgewater, J Wadsley, FY Coxon, W Mansoor, S Madhusudan, S Falk,
GW Middleton, D Swinson, I Chau, J Thompson, D Cunningham, P Kareclas, JA Dunn, HER Ford
On behalf of COUGAR 02 investigators and NCRI Upper GI Clinical Studies Group
Trial funded by Cancer Research UK grant CRUK/07/013
EudraCT Number: 2006-005046-37ISRCTN 13366390

Trial DesignTrial Design
Adenocarcinoma of esophagus,
esophagus-gastric junction or
stomach refractory to platinum and fluoropyrimide
Arm A (n=84): Docetaxel 75mg/m2 IV every 3
weeks for up to 6 cycles+ ASC
Arm B (n=84): Active symptom control
May include: Radiotherapy, analgesia, anti-emetics,
steroids
Assess every 3 weeks for 18 weeks, then
every 6 weeks
RANDOMISE1:1
n=168
Stratified by:
1.Disease status (Locally advanced vs metastatic); 2. Site of disease (Esophagus vs GEJ vs Stomach); 3. Time to progression after previous chemotherapy ( 0 vs 0-3 vs 3-6 months); 4. ECOG PS ( 0/1 vs 2)

0
25
50
75
100
0 2 4 6 8 10 12 14 16 18
Perc
enta
ge s
urvi
ving
Months from randomisation
DocetaxelASC
No. at Risk:Docetaxel 84 69 53 33 25 17 10 8 5 4 ASC 84 70 38 19 13 9 6 2 1 1
Overall survivalMedian survival: 5.2 months (95% CI 4.1-5.9) for Docetaxel 3.6 months (95% CI 3.3-4.4) for ASC
Hazard ratio 0.67 (95% CI 0.49-0.92), p=0.01

This is a difficult population to treatThis is a difficult population to treat
• These patients are sick
• Most do not complete treatment plan
• We still need to learn how best to select patients who will benefit
Docetaxel BSC
Completed 18 weeks
23% 36%
Reason off
Death 15% 38%
PD 40% 2%
Tox 31% N/A
Treatment N/A 14%

Randomized phase III study of Randomized phase III study of irinotecan (IRI) versus weekly paclitaxel irinotecan (IRI) versus weekly paclitaxel
(wPTX) for advanced gastric cancer (AGC) (wPTX) for advanced gastric cancer (AGC) refractory to combination chemotherapy refractory to combination chemotherapy
(CT) of fluoropyrimidine plus platinum (FP): (CT) of fluoropyrimidine plus platinum (FP):
WJOG4007 trialWJOG4007 trial
Ueda S, Hironaka S, Yasui H, Nishina T, Tsuda M, Tsumura T, Sugimoto N, Shimodaira H, Tokunaga S,
Moriwaki T, Esaki T, Nagase M, Fujitani K, Yamaguchi K, Ura T, Hamamoto Y,
Morita S, Okamoto I, Boku N, Hyodo I,
Gastrointestinal Group of West Japan Oncology Group

WJOG4007 Trial – Second line WJOG4007 Trial – Second line chemotherapy for metastatic gastric chemotherapy for metastatic gastric
cancercancer
RANDOMIZATIONStratified by
Institution, PS 0-1/2, target lesion -/+
IRI150 mg/m2 d1, 15 q4w
weekly Paclitaxel80 mg/m2 d1, 8, 15 q4w
AGC refractory to prior FP confirmed by imagingAge 20-75, PS 0-2, No history of CPT-11 or Taxane
Ueda ASCO 2012

Progression Free SurvivalProgression Free Survival
(Months)
Pro
bab
ility
(%
)
2.33.6
108111
6646
1618
98
36
22
wPTXIRI
Number at risk
21
00
00
IRI
wPTX
n
111
108
Median
2.3M
3.6M
P
0.33
HR (95% CI)
1.14 (0.88-1.49)
Log-rank test
FAS

Overall SurvivalOverall SurvivalP
rob
abili
ty (
%)
(Months)108111
8075
3629
1010
23
01
wPTXIRI
Number at risk
01
IRI
wPTX
n
111
108
Median
8.4M
9.5M
P
0.38
HR (95% CI)
1.13 (0.86-1.49)
Log-rank test
Udea ASCO 2012

Reasons for Treatment DiscontinuationReasons for Treatment Discontinuation
wPTX(n=106)
IRI(n=110)
Total(n=216)
Disease Progression
93 ( 88%) 96( 87%)
189
Adverse Event 6 ( 6%) 10 ( 9%) 16
Withdraw 5 ( 5%) 2 ( 2%) 7
Death 1 ( 1%) 1 ( 1%) 2
Other 1 ( 1%) 1 ( 1%) 2
PPS

Post-Study Chemotherapy (3Post-Study Chemotherapy (3rdrd line) line)
wPTX(n=108)
IRI(n=111)
P
Received 3rd line CT
97 (90%) 80 (72%) 0.001
CPT-11 containing 81 (75%) 5 ( 5%)
Taxane containing 8 ( 7%) 67 (60%)
Others 8 ( 7%) 8 ( 7%)Fisher’s exact test
FAS

Kaplan-Meier estimates for overall survival in patients treated with best supportive care (BSC), docetaxel, or irinotecan.
Kang J H et al. JCO 2012;30:1513-1518
©2012 by American Society of Clinical Oncology
FROM KANG STUDY SHOWN EARLIER

Chemotherapy ConclusionsChemotherapy Conclusions
• Basically, it works– It is not super, but HR of 0.67 or better fairly consistently
– Either irinotecan or taxane—both are reasonable
– Don’t give both at the same time. That’s just mean
• Probably works best in highly selected patients as in the WJOG study – PS 0-1
– Doubtful it benefits PS = 2
– But it would be nice to have more selection factors

Phase 3 Trial of Everolimus in Phase 3 Trial of Everolimus in Previously Treated Patients With Previously Treated Patients With
Advanced Gastric Cancer: Advanced Gastric Cancer: GRANITE-1 GRANITE-1
Eric Van Cutsem*,
K. H. Yeh, Y. J. Bang, L. Shen, J. A. Ajani, Y. X. Bai, H. C. Chung, H. M. Pan, K. Chin, K. Muro, Y.
H. Kim, H. Smith, C. Constantini, S. Rizvi, T. Sahmoud, A. Ohtsu
On behalf of the GRANITE-1 Investigators
* University Hospital Leuven/Belgium
Presented at the 2012 Gastrointestinal Cancers Symposium. 20

Overall Survival (FAS)Overall Survival (FAS)
21
Pro
bab
ilit
y o
f o
vera
ll s
urv
ival
(%
) 100
80
60
40
20
00 2 4 6 8 10 12
Time (months)
14
Censoring TimesEverolimus + BSC (n/N = 352/439)Placebo + BSC (n/N = 180/217)
Everolimus + BSC: 5.39 months Placebo + BSC: 4.34 months
Hazard ratio: 0.90 (95% CI, 0.75-1.08)Log-rank P value = 0.1244
No. of patients still at riskTime (months)EverolimusPlacebo
16 18 20 22 24
0 2 4 6 8 10 12 14 16 18 20 22 24
217 172 117 82 60 35 28 16 12 8 4 1 0439 355 253 195 139 87 52 30 13 6 3 1 0

Figure 2 Kaplan-Meier estimates of overall survival (A) and progression-free survival (B)
Charles S Fuchs , Jiri Tomasek , Cho Jae Yong , Filip Dumitru , Rodolfo Passalacqua , Chanchal Goswami , Howard S...
Ramucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trial
The Lancet, Volume 383, Issue 9911, 2014, 31 - 39
http://dx.doi.org/10.1016/S0140-6736(13)61719-5
REGARD TRIALOS HR = 0.776

Let’s Compare: Trials vs BSCLet’s Compare: Trials vs BSC
Chemotherapy Targeted Therapy
AIO (irinotecan) HR 0.48 Granite-1 (everolimus) HR 0.90
Kang (irinotecan or docetaxel)
HR 0.66 REGARD (ramucirumab) HR 0.776
Cougar-02 (docetaxel) HR 0.67
It all comes down to hazard ratio: For chemotherapy, it is very consistent, but for targeted agents, it is consistently not as good

So, if I were Dr. Fuchs, I would So, if I were Dr. Fuchs, I would concede defeat andconcede defeat and
“If you can’t beat ‘em, join ‘em”

RAINBOW: A Global, Phase 3, Randomized, Double-Blind Trial of Ramucirumab and Paclitaxel (PTX) Versus Placebo and PTX in the Treatment of Metastatic Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma Following Disease Progression on First-Line Platinum- and Fluoropyrimidine-Containing Combination Therapy
H. Wilke*
Eric Van Cutsem, Sang Cheul Oh, György Bodoky, Yasuhiro Shimada, Shuichi Hironaka, Naotoshi Sugimoto, Oleg Lipatov, Tae You Kim, David Cunningham, Atsushi Ohtsu, Philippe Rougier, Michael Emig, Roberto Carlesi, Kumari Chandrawansa, Kei Muro
*On behalf of the RAINBOW Investigators

RAINBOW: Randomized Phase III Trial RAINBOW: Randomized Phase III Trial 22ndnd Line Paclitaxel +/- Ramucirumab Line Paclitaxel +/- Ramucirumab
1:1Second line
metastatic gastric and GEJ adenocarcinoma
R
Paclitaxel 80 mg/m2 d1, 8, 15 +
Ramucirumab IVq 2 weeks
Paclitaxel 80 mg/m2 d1, 8, 15 +
Placeboq 2 weeks
26
Primary EP: OSN = 665

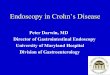
RAINBOW: Overall SurvivalRAINBOW: Overall SurvivalHR (95% CI) = 0.807 (0.678, 0.962)
Stratified log rank p-value = 0.0169
RAM + PTX PBO + PTXPatients / Events 330 / 256 335 / 260Median(mos) (95% CI) 9.63 (8.48, 10.81) 7.36 (6.31, 8.38)
6-month OS 72% 57%12-month OS 40% 30%
RAM + PTX 330 308 267 228 185 148 116 78 60 41 24 13 6 1 0
PBO + PTX 335 294 241 180 143 109 81 64 47 30 22 13 5 2 0
No. at risk
Censored
Δ mOS = 2.3 months

Overall conclusionOverall conclusion
• Thanks to the organizers for giving me the obviously better choice– I can stick with hazard ratio and not even point out the
price differentials
• And also, thank the organizers for not giving Dr. Fuchs the option of combining targeted and chemo
• And also, thank Drs. Van Cutsem, Bendell, Kang, and Cook for the slides of theirs I used.