Embed Size (px)
Citation preview
Use of Drug Eluting Stents for In-Stent Restenosis: Are We
There Yet?
Jose Diez, M.D.
Robert Smith, M.D.
Cardiac Catheterization Conference
March 23, 2004
Outline
• Case presentation with LHC results• Traditional approaches for dealing with in-stent
restenosis– Cutting Balloon Angioplasty (CBA)– Brachytherapy– PTCA– Bare Metal Stent
• Drug eluting stents for in-stent restenosis• Conclusions
Case PresentationJD is a 72 yo AAF with h/o CAD s/p stenting to RCA and LAD in 10/03 who was referred for elective LHC after describing a history of progressive SOB and chest pain. She described the chest pain as precordial, pressure like, and similar to previous episodes of angina. Her chest pain was typically less than a few minutes, relieved with SL NTG, and occurred sometimes with exertion and sometimes at rest. It was usually associated with SOB. She first experienced the chest pain approximately 2 months after stent placement (12/03) and underwent a negative stress echo at that time. In 2/04, she was evaluated and discharged from the ER for similar episodes of chest pain with SOB. Subsequently, an adenosine cardiolyte stress test was negative for ischemia. Because of persistence of her symptoms, she was referred for LHC.
Past Medical History• CAD s/p STEMI in 10/03 with stent to culprit RCA lesion (Medtronic
Zipper) and stent to LAD (Cypher)• Exercise stress echo 12/03 negative for ischemia. Pt exercised for 7
minutes• Adenosine cardiolyte stress test 2/04 negative for ischemia• TTE 2000 showed moderate AI, concentric LVH, mild MR• HTN for > 10 years• Type II DM on oral hypoglycemics• Hyperlipidemia• PVD• Cerebrovascular disease s/p left CEA and 60% lesion in the right
internal CA (h/o TIA’s)• Obstructive Sleep Apnea on home CPAP
Medications
• Plavix 75mg PO QD
• ASA 81mg PO QD
• Lopressor 50mg PO BID
• Lisinopril 40mg PO QD
• Atorvastatin 80mg PO QHS
Social History
• Retired Nurse
• Denies h/o cigarette smoking
• Denies EtOH
• Denies drug use
• Lives with daughter
• Husband is deceased

Family History
• Father died of “congestive heart failure”
• Also significant for DM, HTN
Physical Exam
• 152/88 52 14 36.0 SaO2 97%
• Gen: NAD, symptom free
• Neck: Right Carotid Bruit, No JVD
• CV: nlS1S2, 2/6 HSM apex axilla
• Chest: clear
• Abd: NABS, NT, ND
• Ext: no edema
Labs• Na 133• K 4.1• Cl 101• CO2 29• Glu 172• BUN 11• Cr 0.6• Ca 1.8• Mg 1.8• Tn <0.04• Myo 22• CK 68
• WBC 6.6• Hgb 12.5• Hct 36.5• MCV 87.5• Plt 221• PTT 26• INR 1.02
ECG
• NSR with q waves in the inferior leads
Restenosis
• Occurs in 30-40% of patients by 6 months after PTCA• Occurs in 20-30% of patients by 6 months after PTCA
with stenting 1,2
• Restenosis is thought secondary to combination of vessel wall remodeling and neointimal hyperplasia with smooth muscle cell and matrix proliferation
• Elastic recoil and thrombosis may also play a role
1Fischman et al., N Engl J Med 1994;331:496-5012Serruys et al., N Engl J Med 1994;331:489-495
ISR; Available Therapies
• Cutting Balloon Angioplasty (CBA)
• Angioplasty
• Brachytherapy
• Stent within Stent– Bare Metal Stents– Drug Eluting Stents
Cutting Balloon Angioplasty
• The cutting balloon is a device with 3-4 longitudinal atherotome blades mounted on the outer surface of the device
• It produces longitudinal incisions in a target lesion resulting in more effective dilatation of the lesion
• Keeps the balloon from moving proximally or distally during inflation
• May help facilitate extrusion of in-stent hyperplasia through the stent struts
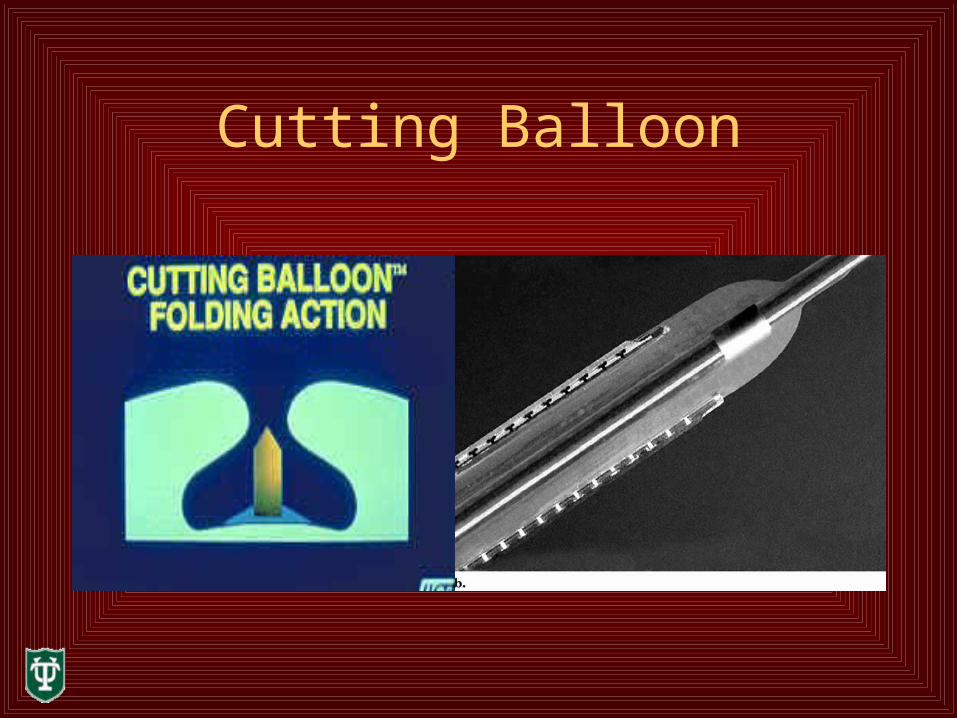
Cutting Balloon
Cutting Balloon Angioplasty for ISR• In a 2001 study, CBA was compared to rotational
atherectomy, PTCA, or restenting in a study of 684 patients with ISR1
• At angiographic f/u, CBA was associated with less lumen loss than that seen with atherectomy and stent
• This corresponded to a 6 month restenosis rate of 20% for CBA, 36% for atherectomy, and 41% for restenting
• At 11 month follow up, there was no difference in the incidence death, MI, or bypass surgery
1Adamian et al. J Am Coll Cardiol 2001 Sep;38(3):672-9
Brachytherapy for ISR• Intracoronary brachytherapy reduces vessel wall
remodeling and causes a reduction in the proliferation of the neointima
• The SCRIPPS Trial1 was a double blind randomized trial that compared gamma irradiation to placebo for treatment of ISR (n=55). Follow up was performed at 6 months, 3 years, and 5 years
• 23% of patients had recurrent stenosis at angiographic follow up
1Grise et al., Circulation. 105(23):2737-2740, June 11, 2002
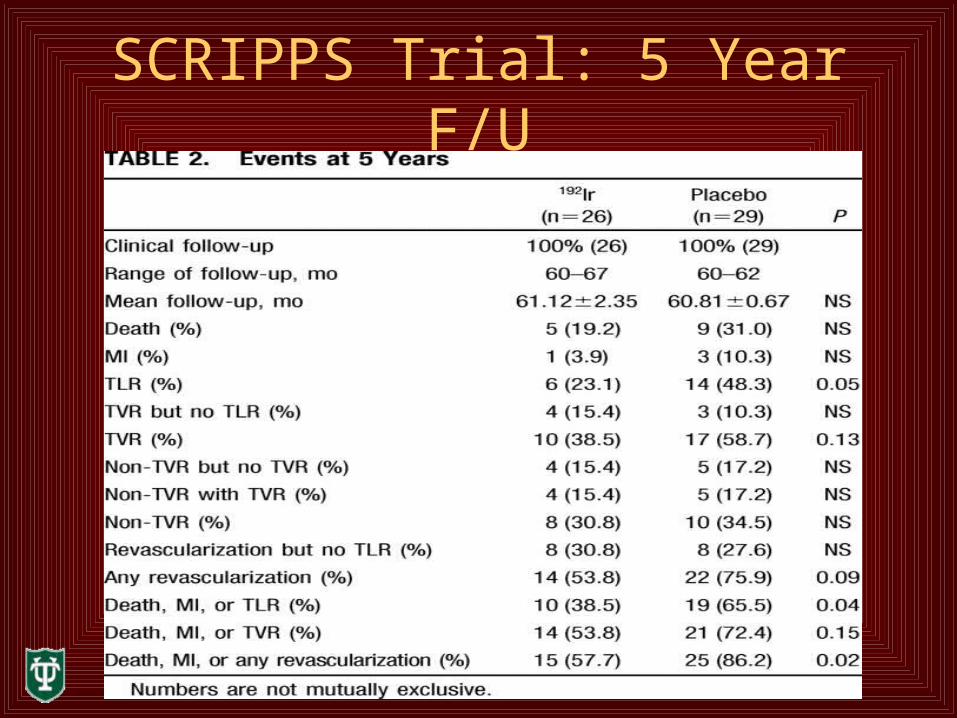
SCRIPPS Trial: 5 Year F/U
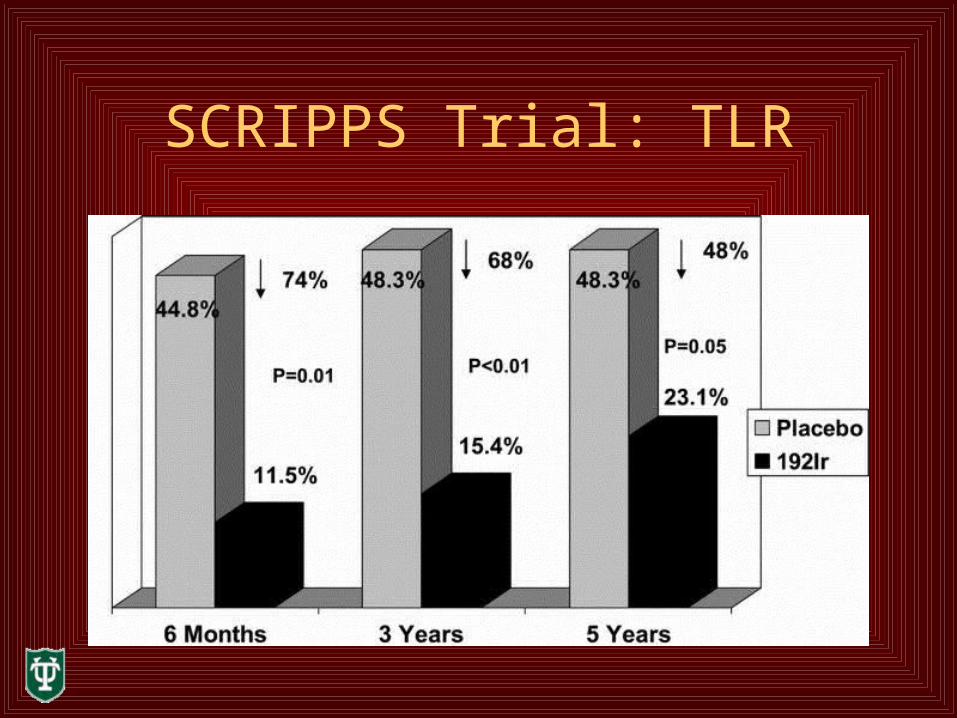
SCRIPPS Trial: TLR
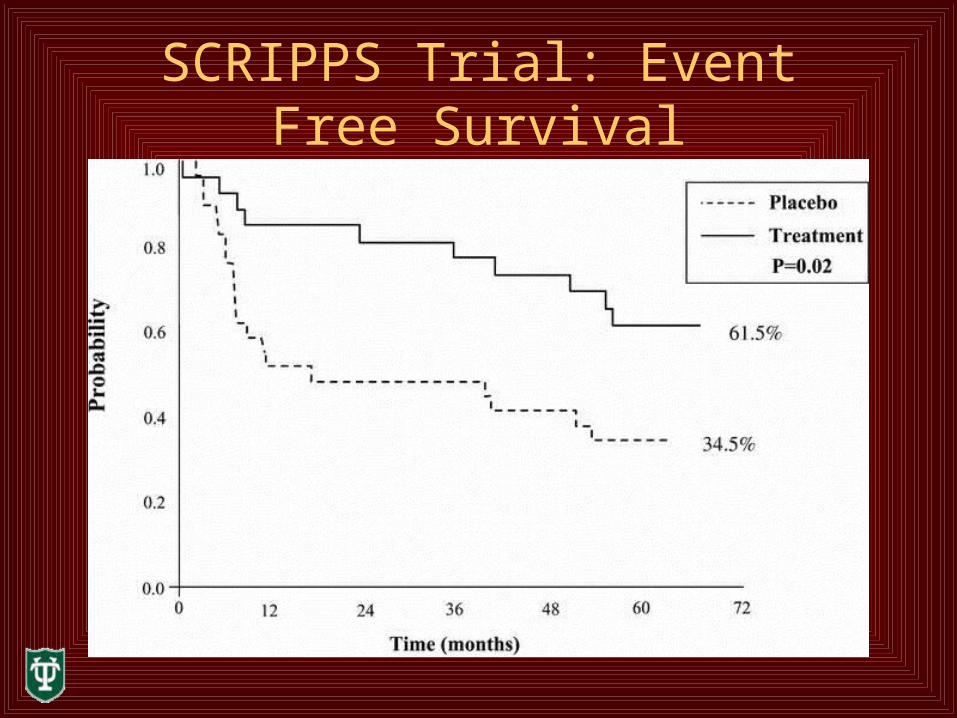
SCRIPPS Trial: Event Free Survival
PTCA for ISR
• In a 1998 study, PTCA was performed in 52 patients presenting with ISR 1
• Initial angiographic success rate was 100%• At 6 month follow up, angiographic restenosis rate was
54% • 18 patients (35%) had TVR• No patients died• Conclusions: PTCA for ISR is safe but has a high rate of
recurrent stenosis
1Eltchaninoff et al., J Am Coll Cardiol 1998 Oct;32(4): 980-984
Repeat Stenting for ISR
• In a study from 2000, 65 patients underwent repeat stenting as treatment for ISR 1
• Angiographic success was obtained in all patients• 3 patients had acute adverse events (1 death, 2
NQWMI’s)• During follow up (17+/- 11 months), TVR was
required in 14%• Angiographic follow up (mean of 9 months) showed
ISR in 30%
1Alfonso et al., Am J Cardiol 2000 Feb 1;85(3):327-32
Repeat Stenting vs. PTCA
• Addressed in the RIBS trial1 (compared repeat stenting to PTCA alone in 450 patients)
• Restenosis rate and event free survival at 6 months were similar in the two groups
• Among patients with a target vessel diameter > or equal to 3mm, stenting was associated with a significantly lower restenosis rate (27% vs. 49% for PTCA) at 6 months
1Alfonso et al., J Am Coll Cardiol 2003 Sep 3;42(5):796-805

Repeat Stenting vs. PTCA
• In vessels > or equal to 3mm, patients who were restented had better event free one year survival (84% vs. 62%)
• There was an almost significant trend toward worse outcomes with re-stenting when the vessel diameter was less than 3mm

Summary of Restenosis Rates
• Brachytherapy: 12% at 6 months and 23% at 5 years
• CBA: 20% at 6 months
• PTCA: 54% at 6 months, 49% at 6 months
• Bare Metal Stents: 41% at 6 months, 30% at 9 months, 27% at 6 months
Drug Eluting Stents for ISR
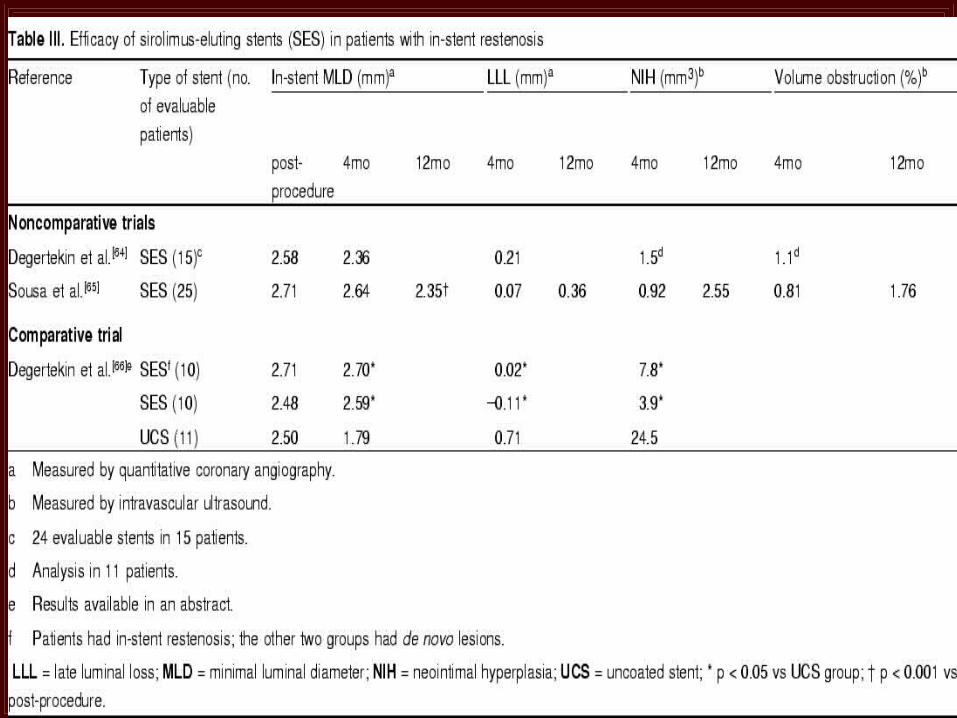
• The efficacy of Sirolimus Eluting Stents has been evaluated in 2 small, noncomparative trials 1,2
• The efficacy of Paclitaxel eluting stents has also been evaluated in a single noncomparative trial 3
1Degertekin et al., J Am Coll Cardiol 2003 Jan 15;41(2):184-92Sousa et al., Circulation 2003; 107:243Tanabe et al., Circulation 2003 Feb 4;107(4): 559-564
Drug Eluting Stents for ISR
• In an initial series of 25 patients with ISR in whom a SES was implanted, all vessels were patent at 1 year and only one patient developed ISR within the newer stent 1
• Exclusion criteria for this study included lesions in SVG’s, patients who had undergone previous brachytherapy to the target vessel, and lesions greater than 36mm in length
• No ostial lesions were treated in this study
1Sousa et al., Circulation 2003; 107:24
Drug Eluting Stents for ISR
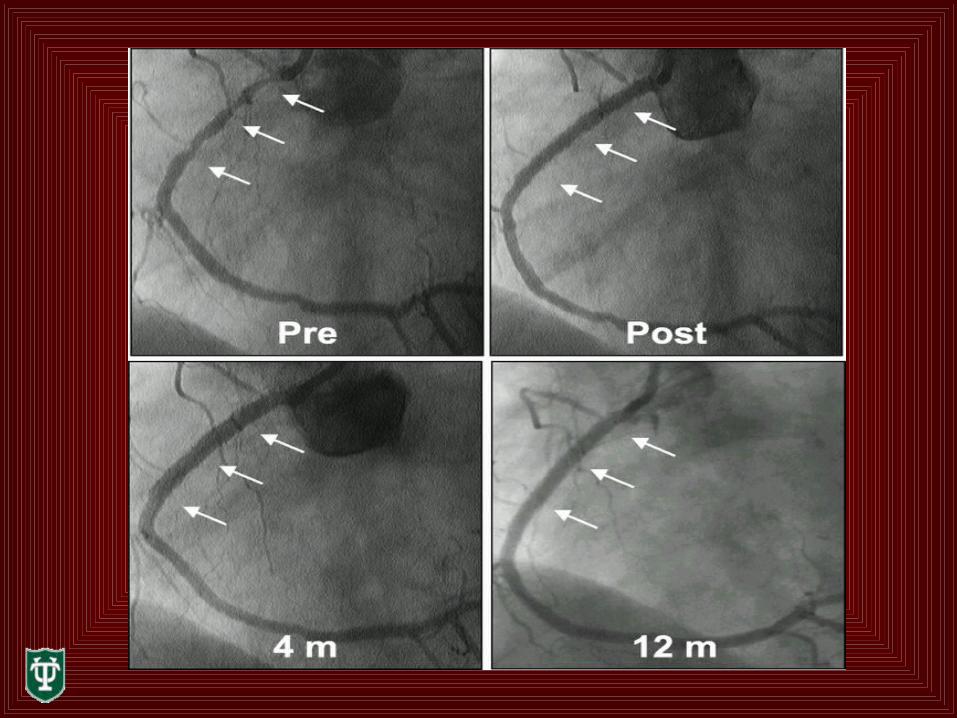
• Post procedure angiography and IVUS was performed at 4 and 12 months
• All patients were free of angina after 1 year• There were no repeat revascularizations, stent
thromboses, or major clinical events (CVA, MI, Death) after 1 year
• On 4 month angiographic follow up, lumen diameter was unchanged in 50% of patients, and slightly greater in some patients
Drug Eluting Stents for ISR
• There was a slight but significant decrease in mean lumen diameter between 4 and 12 months (angiographic late loss averaged 0.07mm at 4 months and 0.36mm at 12 months)
• Volume obstruction by IVUS was 0.81% at 4 months and 1.76% at 12 months
• No patients had ISR at 4 months and 1 patient had ISR at 1 year
• All stents were properly deployed
Drug Eluting Stents for ISR• In a second report1, 16 patients with severe, recurrent
ISR in a native coronary vessel received a SES (average lesion length 18.4mm)
• Patients with objective evidence of ischemia were excluded
• 4 patients has total occlusions pre-procedure and 3 others had received brachytherapy
• Quantitative angiographic and IVUS follow up was performed at 4 months and clinical follow up at 9 months
1Degertekin et al., J Am Coll Cardiol 2003 Jan 15;41(2):184-9
Drug Eluting Stents for ISR
• At 4 month follow up, one patient had died and three patients had angiographic evidence of restenosis (18.8%)
• Late lumen loss averaged 0.21mm and volume obstruction of the stent by IVUS was 1.1%
• At 9 months clinical follow up, 3 patients had experienced major adverse events (2 deaths and 1 MI)
Drug Eluting Stents for ISR• The TAXUS III Trial1 evaluated paclitaxel eluting
stents for treatment of ISR• This was a noncomparative 2 center study that
evaluated 28 patients with ISR• Inclusion criteria were lesions < or = to 30mm, 50-99%
stenosis, and vessel diameter 3.0 to 3.5mm• Exclusion criteria were AMI, LVEF <30%, CVA within
6 months, SCr >1.7, and contraindication to antiplatelet therapy
1Tanabe et al., Circulation 2003 Feb 4;107(4): 559-564
Drug Eluting Stents for ISR
• There was no subacute stent thrombosis• 25 of 28 patients completed angiographic follow up at 6
months• 4 patients had angiographic evidence of restenosis (16%)• One of these patients had total occlusion of a lesion
previously treated with a gold coated stent (he was asymptomatic)
• One patient had ISR in a bare metal stent used to treat a dissection at the end of a PES
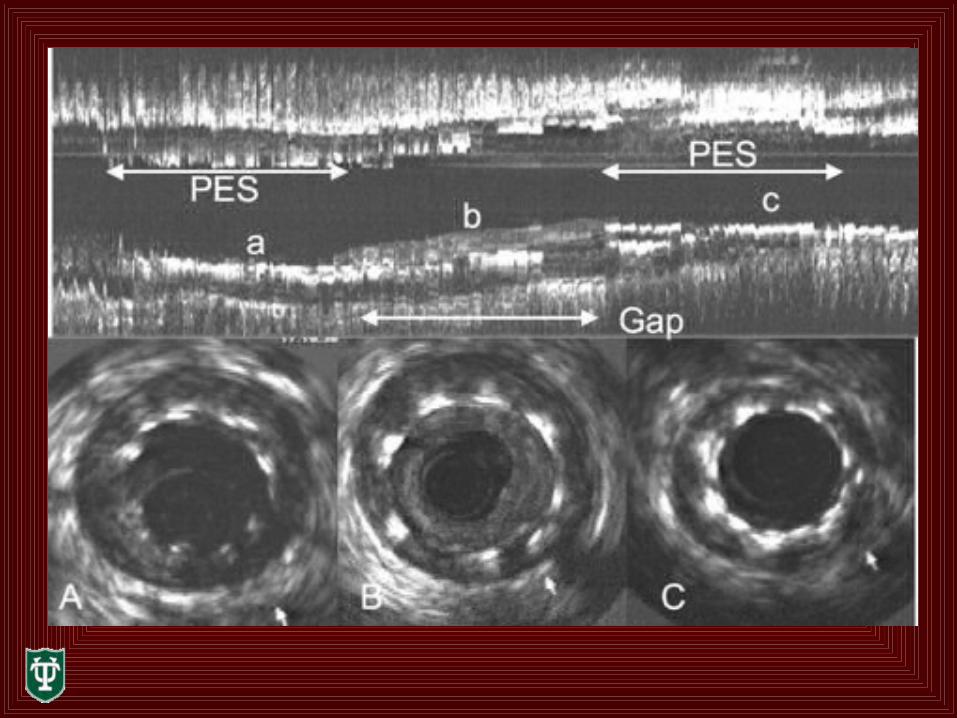
• Two patients has ISR in gaps between sequential PES’s• The mean lumen late loss was 0.54mm
Drug Eluting Stents for ISR
• The major adverse cardiac event rate was 29% (8 patients)
• This included 1 NQWMI, 1 CABG, and 5 TLR’s• 1 patient with ISR of bare metal stent and 2
patients with stenoses of gaps between PES’s• 2 patients without angiographic restenosis
underwent TLR as result of IVUS assessment at follow up (1 incomplete apposition and 1 insufficient expansion of the stent
Conclusions
• Treating ISR is a major challenge facing interventional cardiologists
• With traditional treatments (PTCA, CBA, re-stenting), restenosis develops in 30-80% of patients
• Prior to drug eluting stents, the best therapy was intravascular brachytherapy (23% restenosis in the SCRIPPS trial)
• Early studies indicate that drug eluting stents may prove effective for treating in-stent restenosis
Conclusions
• Between all DES studies, there was no subacute thrombosis
• Between all studies, there were only 4 compelling cases of ISR within a DES
• When the DES’s were properly deployed, there were only 6 adverse cardiac events between the studies
• Sirolimus eluting stents and paclitaxel eluting stents both appear to be effective for treating ISR
• Early data indicates that DES’s are superior than traditional methods for treating ISR
• Are we there yet? Maybe…