Embed Size (px)
Citation preview

Use of Network Analysis During a Tuberculosis Investigation
Outbreak Investigation SectionSurveillance and Epidemiology Branch
Division of Tuberculosis EliminationNational Center for HIV, STD, and TB Prevention
Centers for Disease Control and PreventionAtlanta, GA
April 21, 2003

TB Facts
• M. tuberculosis (M.Tb) airborne transmission
• Latent TB infection (LTBI) detected by tuberculin skin test (TST)
• 10 to 15 million LTBI
• 10% lifetime risk of progression to active TB

TB patient Contact
M. tuberculosis Transmission
• Infectiousness
• Exposure duration
• Room size
• Air exchange

Exposedcontacts
Latent TB
infectionActive
TBdisease
Exposure…. Infection…. Disease
TuberculinSkinTest

Concentric Circle ApproachHousehold
Leisure Work TB PATIENT
Close Contacts
Casual Contacts

Multiple Contact Investigations

The Concentric Circle Paradigm Assumes…
• Cases know their contacts
• Cases will reveal their contacts
• Casual contacts are less important
• Interconnections among contacts of contacts are unimportant

Each Contact Investigation Yields an Individual Transmission Unit
TB patient “A” identifies 2 contacts
Contact evaluated and found to be tuberculin skin test (TST) positive
Contact evaluated and found to be tuberculin skin test (TST) negative

County’s Contact Data from Multiple TB Cases (A–D)
Patient C has greater importance, but patient-specific TST-positive rates miss this importance
A
50% TST+
B
50% TST+
D
50% TST+
C
50% TST+

Contacts Data
• Name, address, DOB
• Sex, ethnicity
• Places
• TST status
• Type of contact
• Strength of contact
• All the case variables
No Shortage of Data

Outbreak

Objectives
• Identify case-patients and contacts
• Establish epidemiologic links among case-patients and contacts
• Make recommendations to control the outbreak

Methods
• Case-patients
• Contacts
• Data entered in ACCESS® database*
• InFlow™ 3.0 network analysis software*
*Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of Health and Human Services

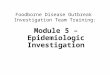
Index Case-Patient
ED Visits
ED Visits
Diagnosisof TB
Restaurant
Fever &Cough
Jail

Contact Investigation: Index Case-Patient
Identified Tested TST+ (5 mm) RR (95%CI)
Household 11 10 10 (100%) 6.4 (2.9,14.3)
Friend 76 63 33 (52%) 3.4 (1.5,7.8)
Jail 125 108 54 (50%) 3.2 (1.4,7.3) Work/School 40 32 5 (16%) Referent
Hospital 42 38 4 (11%) 0.7 (0.2,2.3)
Total 294 251 106 (42%)

Case-Patients by Date of Diagnosis (N=35) Nov 02
Culture confirmed Clinical Case
Index
2001 2002
CDC invited

Contact Investigations N (%)
Total Identified 1,039Evaluated 860 (83)TST 5mm 179 (21)Initiated treatment 135 (75)
Female 474 (53)Age <5 45 ( 5)
5-14 171 (20) 15-24 169 (19) 25 507 (57)
Black 390 (48)

Network Visualization

Network Key
Nodes
TB cases
TST(+) contacts
TST(-) contacts
TST status unknown
Links
Close contact
Casual contact

Are All TB Cases Associated?

Case-Patients
2515
4543
39
38
37
36
35
3433
32
30
29
22 21
20
19
18
17
16
14
13
12
11
10
9
8
7
6
5
4
3
2
1

What Does the Entire Network Look Like?

Entire Network

How Are Infected Contacts Related to the Cases?

Case-patients and LTBI
2162
2161
2159
2158
2153
2148
2136
2087
2044
1984
1953
1940
1939
1938
1922
1914
1890
1884
1866
1864
1836
1825
1817
1796
1763
1761
1760
1749
1742
1741
1730
1724
1718
1709
1694
16871686
1682
1662
1660
1657
1651
1649
1648
1636
1621
1620
1614
1612
1611
1610
1604
1603
1589
1578
15721558
1552
1544
1537
1533
1522
1518
1506
1502
1500
1494
1493
1484
1482
1469
1466
1463
1457
1450
1445
1442
1436
1435
1432
1423
1411
1407
1404
1393
1381
1377
1345
13371329
1324
1322
1316
1297
1296
1295
1290
1272
1262
1243
1233 1227
1225
1223
1216
1206
1205
1200
1196
1195
1184
1167
1160
1155
1152
1143
1128
1127
1126
1114
1112
1108
1107
1100
1095
1087
1082
1079
1075
1061
1059
1049
1033
1032
1019
1006
1002
45
43
39
38
37
36
35
34
33
32
30
29
25
22
21
20
19
18
17
16
15
14
13
12
11
10
9
8
7
6
5
4
3
2
1

Which Contacts Should We Pursue for More Information?

Network Core
2162
2112
2102
2034
1982
1939
1938
1929
1925
1924
1922
1919
1918
1910
1905
19041895
1893
1890
1889
18821870
1869
1868
1866
1861
1858
1857
18551853
1846
1833
1828
1817
1813
1806
1804
1800
1799
1798
1797
17931777
17661742
1741
1733
1716
1711
1693
1692
1690
1671
1662
1650
1649
1637
1627
1620
1618
1599
1587
1584
1582
1571
1553
1539
1536
1526
1523
1495
14691461
1457
1453
1451
1429
1425
1420
1413
1411
1405
1399
1393
1373
1366
1343
13271325
1324
1318
1268
1265
1260
1259
1254
1239
1227
1225
1218
1204
1196
1195
1193
1189
1187
1183
11731172
1164
1158
1157
1156
1135
1127
1108
1107
1095
1094
1087
1079
1078
1066
1048
1042
1040
1032
10311029
1028
1027
1020
1018
43
38
37
36
35
33
32
30
2922
21
20
19
18
17
16
15
14
13
12
11
10
8
7
6
5
4
3
2
1

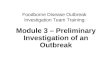
How Do You Prioritize?

Contacts Needing Evaluation
21422140
2139
2133
2132
2131
2130
21292126
2111
2092
2081
20732059
2043
2041 2037
2034
2011
1981
1980
1975
1974
1973
1972
1971
1970
1969
1968
1967
1966
1965
1964
19631962
1961
1948
1944
1935
1929
1926
1925
1924
1919
1910
1909
1905
1901
1900
1897
1893
1889
1886
1871
1869
1868
18671865
1863
1861
1856
1854
1849
1833
1814
1813
1810
1809
1807
1800
1799
1797
1793
1792
1788
1785
1784
1777
1768
1746
1738
1729
1728
1723
1713
1708
1679
1659
1654
1631
1624
1605
1597
1590
1588
1587
1580
1569
1557
1554
1551
1541
15391535
1531
1512
1511
1508
1507
15041503
1492
1455
1420
1419
1383
1372
1371
1359
1356
1353
1346
1328
13191307
1298
1294
1268
1258
1257
1253
1241
1239
1238
1236
1234
1231
1230
1226
1211
1210
1198
1185
1162
1151
1135
1134
1130
11021083
1074
1070
1069
1067
1060
1057
1053
1051
1045
1041
1039
1036
1025
1021
1017
10091008
45
43
39
38
37
36
35
34
33
32
30
29
25
22
21
20
19
18
17
1615
14
13
12
11
10 9
8
7
6
5
4
3
2
1

Conclusions

Conclusion: EPI Data
• Delayed diagnosis generated a large community outbreak in a low incidence area
• All case-patients were linked to index case-patient
• High TST reaction rate around the index case-patient

Conclusion: Network-Informed Approach
• Proved feasible in a low incidence setting
• Required no new data; based on routine contact investigations
• Facilitated discussions between state and county TB controllers

Acknowledgments
McKenzie Andre, MDEpidemic Intelligence Service OfficerDivision of TB EliminationCDC
Local and State TB Control Authorities
Valdis E. KrebsInFlow Software™http://www.orgnet.com