Embed Size (px)
Citation preview

Karen Blackman, MDKaren Blackman, MDAmy Odom, DOAmy Odom, DO
Primary Care CollaborationPrimary Care CollaborationTraverse City, MI 8/28/10Traverse City, MI 8/28/10
Using and Managing Using and Managing AntipsychoticsAntipsychotics
In the Primary Care In the Primary Care SettingSetting

ObjectivesObjectives
Identify the potential needs for prescribing Identify the potential needs for prescribing antianti--psychotics in a primary care settingpsychotics in a primary care setting
Use a systematic approach to following Use a systematic approach to following patients on antipatients on anti--psychotics to improve psychotics to improve safetysafety
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

AgendaAgenda
Review of antipsychotic nomenclatureReview of antipsychotic nomenclatureTour of antipsychotic use in the primary Tour of antipsychotic use in the primary care settingcare settingRisk profiles of antipsychoticsRisk profiles of antipsychoticsSafety tool for monitoring patients on Safety tool for monitoring patients on antipsychoticsantipsychotics
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
HandoutsHandoutsBipolar dosing charts Bipolar dosing charts Materials for dosing of Materials for dosing of APsAPs in dementia with in dementia with agitation or psychosisagitation or psychosis–– Cover of APA Quick Reference Guide to Cover of APA Quick Reference Guide to
treating patients with Alzheimertreating patients with Alzheimer’’s Disease and s Disease and other dementiasother dementias
–– Copy of page #21 from guide Copy of page #21 from guide -- dosing dosing atypical atypical APsAPs
TRUStTRUSt Big Big BeLtSBeLtS–– Antipsychotic Monitoring FormAntipsychotic Monitoring Form–– Antipsychotic Patient Education FormAntipsychotic Patient Education Form

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Why Learn About AntipsychoticsWhy Learn About Antipsychotics
Primary care providers are prescribing Primary care providers are prescribing themthemA great deal of psychiatry is done in the A great deal of psychiatry is done in the primary care officeprimary care office–– Patients may not have psychiatry accessPatients may not have psychiatry access–– Patients may avoid psychiatry even if they do Patients may avoid psychiatry even if they do
have accesshave access
These drugs can be a blessing and a curseThese drugs can be a blessing and a curse

Antipsychotic NomenclatureAntipsychotic NomenclatureFirst Generation (FGA) First Generation (FGA)
==TypicalsTypicals==ConventionalsConventionals–– Examples:Examples:–– Chlorpromazine (Chlorpromazine (thorazinethorazine) )
““Low potencyLow potency””
–– PerphenazinePerphenazine ((TrilafonTrilafon))““Medium potencyMedium potency””
–– Haloperidol (Haloperidol (HaldolHaldol))““High potencyHigh potency””
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Second Generation Antipsychotics Second Generation Antipsychotics (SGA)=(SGA)=AtypicalsAtypicals
AripiprazoleAripiprazole ((AbilifyAbilify))AsenapineAsenapine ((SaphrisSaphris))ClozapineClozapine ((ClozarilClozaril))IloperidoneIloperidone ((FanaptFanapt))OlanzapineOlanzapine ((ZyprexaZyprexa))QuetiapineQuetiapine ((SeroquelSeroquel))RisperidoneRisperidone ((RisperdalRisperdal))ZiprasidoneZiprasidone ((GeodonGeodon))
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

CATIECATIE
Clinical Clinical Antipsychotic Trials of Intervention Antipsychotic Trials of Intervention EffectivenessEffectiveness–– Published in NEJM in 2005Published in NEJM in 2005
Compared Compared efficacy and tolerability of FGA efficacy and tolerability of FGA perphenazineperphenazine ((TrilafonTrilafon) with several ) with several SGAsSGAs in in schizophreniaschizophrenia
Majority Majority discontinued their assigned medications discontinued their assigned medications ((~~1000/~15001000/~1500))
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

CATIE continuedCATIE continued
OlanzapineOlanzapine ((ZyprexaZyprexa) most efficacious?) most efficacious?–– Longest Longest time to all cause time to all cause discontinuationdiscontinuation–– Refuted laterRefuted later
OlanzapineOlanzapine worst weight gain, glucose, lipidsworst weight gain, glucose, lipids
PerphenazinePerphenazine worst re: neurologic side effectsworst re: neurologic side effects
Efficacy Efficacy and tolerability more similar than and tolerability more similar than expectedexpected
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

When do YOU use When do YOU use Antipsychotic Antipsychotic medications?medications?

When to Consider AP UseWhen to Consider AP UseBipolar DisorderBipolar DisorderDepression Depression –– Augmentation in treatment resistant depressionAugmentation in treatment resistant depression–– Psychotic depressionPsychotic depression
PsychosisPsychosis–– AcuteAcute–– ChronicChronic
Dementia with psychosis or agitationDementia with psychosis or agitationDeliriumDeliriumSpecial casesSpecial cases
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotics in Bipolar Antipsychotics in Bipolar DisorderDisorder
Nearly all atypical antipsychotics are efficacious Nearly all atypical antipsychotics are efficacious in mania, FDA approved and work quicklyin mania, FDA approved and work quickly–– Iloperidone not FDA approved for bipolarIloperidone not FDA approved for bipolar
Can also be effective for bipolar depressionCan also be effective for bipolar depression–– FDA approval for quetiapine (Seroquel) FDA approval for quetiapine (Seroquel) –– FDA approval for olanzapine with fluoxetine FDA approval for olanzapine with fluoxetine
(Symbyax)(Symbyax)
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

How to Approach Bipolar How to Approach Bipolar DisorderDisorder
Determine phase patient is in Determine phase patient is in –– 22ndnd and 3and 3rdrd rows in page 1 of Bipolar rows in page 1 of Bipolar
Medication Chart give FDA indicated phase Medication Chart give FDA indicated phase and other efficacy informationand other efficacy information
Judge how ill the patient isJudge how ill the patient is–– Urgent vs. nonUrgent vs. non--urgenturgent–– Row labeled Row labeled ““acuityacuity”” in charts addresses time in charts addresses time
till onset of actiontill onset of action
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

How to Approach Bipolar Disorder, cont.How to Approach Bipolar Disorder, cont.
Then look at the patient (and yourself) in Then look at the patient (and yourself) in light of side effects and ease of monitoring light of side effects and ease of monitoring medicationmedication
If using antipsychotic, consider another If using antipsychotic, consider another product (like an anticonvulsant mood product (like an anticonvulsant mood stabilizer) to take its place over time!stabilizer) to take its place over time!
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotics in Treatment Antipsychotics in Treatment Resistant DepressionResistant Depression
59 year old female59 year old femaleElderly demented Elderly demented mothermotherFinancial ruin due to Financial ruin due to divorcedivorceMoved out of Moved out of ““dreamdream””home to small home to small apartment apartment
Recurred on Recurred on citalopramcitalopram 60/d, 60/d, fluoxetinefluoxetine, , venlafaxinevenlafaxine, , sertralinesertraline, , Failed Failed bupropionbupropion and and buspironebuspironeaugmentationaugmentation
••Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team••20102010

Antipsychotics as Adjuncts to Antipsychotics as Adjuncts to Antidepressants in DepressionAntidepressants in Depression
Aripiprazole (Abilify) FDA approved as Aripiprazole (Abilify) FDA approved as augmenting agent augmenting agent Quetiapine (Seroquel) FDA approved as Quetiapine (Seroquel) FDA approved as augmenting agentaugmenting agentOlanzapine/fluoxetine (Symbyax) FDA approved Olanzapine/fluoxetine (Symbyax) FDA approved for treatment resistant depressionfor treatment resistant depressionOther augmenting agents may pose less dangersOther augmenting agents may pose less dangers–– Direct to consumer advertising, look out!Direct to consumer advertising, look out!–– Patients may be desensitized to danger statementsPatients may be desensitized to danger statements
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotics in Psychotic Antipsychotics in Psychotic DepressionDepression
55 year old female teacher55 year old female teacherSeverely depressed and not responding to Severely depressed and not responding to multiple antidepressant trialsmultiple antidepressant trialsWhen psychiatrist closes blinds, she asks if When psychiatrist closes blinds, she asks if psychiatrist is afraid of psychiatrist is afraid of ““himhim”” too too –– Reveals paranoiaReveals paranoia

Antipsychotics in Antipsychotics in Psychotic DepressionPsychotic Depression
Add antipsychotic to antidepressant Add antipsychotic to antidepressant regimenregimen–– WonWon’’t remit without thist remit without this–– Start low, go slow till symptoms addressedStart low, go slow till symptoms addressed
Treat for at least 3 months with the APTreat for at least 3 months with the AP–– Then can consider discontinuingThen can consider discontinuing
Treat depression long term to help Treat depression long term to help prevent further episodesprevent further episodes
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotics in Acute Antipsychotics in Acute PsychosisPsychosis
45 year old woman45 year old womanBrought in by her sisterBrought in by her sisterMaking no senseMaking no senseMoved recently from another stateMoved recently from another stateStopped medications she was onStopped medications she was onThinks she is important part of a Thinks she is important part of a government strategy to stop terrorism; government strategy to stop terrorism; suspects neighborssuspects neighbors

Antipsychotics in Acute Antipsychotics in Acute PsychosisPsychosis
Patient does not seem depressed, but Patient does not seem depressed, but distresseddistressedDiagnosis Diagnosis per per se not knownse not knownConsider hospitalization, psychiatry Consider hospitalization, psychiatry referral, trying to get back story (talk to referral, trying to get back story (talk to previous treating provider if possible)previous treating provider if possible)This is the individual for whom This is the individual for whom antipsychotics were designed!antipsychotics were designed!
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Antipsychotics in Chronic PsychosisAntipsychotics in Chronic Psychosis
48 yo male seen for 48 yo male seen for annual physical examannual physical examLives in AFCLives in AFCSchizophrenia since Schizophrenia since age 26age 26Goes to CMH for Goes to CMH for psychiatric carepsychiatric careOn olanzapineOn olanzapineFBS 160, TG 400FBS 160, TG 400

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Antipsychotics in Chronic PsychosisAntipsychotics in Chronic Psychosis
PCPs often provide care for chronically PCPs often provide care for chronically mentally illmentally illMay not be the prescriber of APMay not be the prescriber of AP’’s in these s in these casescasesNeed to monitor side effects and take Need to monitor side effects and take action when necessaryaction when necessaryCommunication with CMH to decide plan Communication with CMH to decide plan of actionof action

Antipsychotics in DementiaAntipsychotics in Dementia
91 year old retired professor91 year old retired professorAlzheimerAlzheimer’’s Diseases DiseaseAt home with ill, 88 year old wifeAt home with ill, 88 year old wifeUp much of the night agitated and Up much of the night agitated and seemingly responding to people who are seemingly responding to people who are not therenot there

Antipsychotics in Dementia Antipsychotics in Dementia With Psychosis or AgitationWith Psychosis or Agitation
Non pharmacology first!Non pharmacology first!–– If can calm psychosis, agitation no need to treatIf can calm psychosis, agitation no need to treat
Re: pharmacology: data best support atypical Re: pharmacology: data best support atypical antipsychotic efficacyantipsychotic efficacy–– though side effects minimize benefit potential!though side effects minimize benefit potential!
Less evidence that benzodiazepines, Less evidence that benzodiazepines, antidepressants, cholinesterase inhibitors, antidepressants, cholinesterase inhibitors, anticonvulsants benefitanticonvulsants benefitOnce controlled, try to taper off antipsychoticsOnce controlled, try to taper off antipsychotics
APA Practice Guideline for the Treatment of Patients With AlzheiAPA Practice Guideline for the Treatment of Patients With Alzheimermer’’s Disease and Other Dementias, s Disease and Other Dementias, Second Edition, December 2007Second Edition, December 2007
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Use of Atypical Antipsychotics for Use of Atypical Antipsychotics for Dementia Related Psychosis and AgitationDementia Related Psychosis and Agitation
APA Practice Guideline for the Treatment of Patients With AlzheiAPA Practice Guideline for the Treatment of Patients With Alzheimermer’’s Disease and Other s Disease and Other Dementias, Second Edition, December 2007Dementias, Second Edition, December 2007

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Antipsychotics in DeliriumAntipsychotics in Delirium
84 yo male has an 84 yo male has an acute mental status acute mental status change change Discovered to have a Discovered to have a UTIUTIIs aggressive with Is aggressive with staff and familystaff and familyNot responding to Not responding to redirection redirection

Antipsychotics in DeliriumAntipsychotics in Delirium
DeliriumDelirium–– Medical emergencyMedical emergency–– Evaluate and treat medicallyEvaluate and treat medically–– Haloperidol 1 Haloperidol 1 --10 mg every 210 mg every 2--4 hours 4 hours
Often 5 mg per dose is neededOften 5 mg per dose is neededHaloperidol 0.25 mg to 0.5 mg every 4 hours in Haloperidol 0.25 mg to 0.5 mg every 4 hours in elderlyelderly
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Special CasesSpecial CasesTransferred to primary care or discharged back Transferred to primary care or discharged back to us on antipsychoticsto us on antipsychotics–– What do we do when that patient is a child?What do we do when that patient is a child?–– What do we do when patient depressed, just out of What do we do when patient depressed, just out of
hospital, no diagnosis in papers of psychosis?hospital, no diagnosis in papers of psychosis?
Patient carries diagnosis of autism Patient carries diagnosis of autism –– Care transferred to Care transferred to pcppcp, stable on , stable on aripiprazolearipiprazole
((AbilifyAbilify) for last year) for last year
TouretteTourette Syndrome Syndrome
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

AgendaAgenda
√√ When to consider antipsychotic use in the When to consider antipsychotic use in the Primary Care settingPrimary Care setting
Review risk profiles of antipsychoticsReview risk profiles of antipsychotics
Safety tool for monitoring patients on Safety tool for monitoring patients on antipsychoticsantipsychotics
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
Antipsychotic RisksAntipsychotic Risks
CardiovascularCardiovascularNeurologicNeurologicMetabolicMetabolicOtherOther

Antipsychotics: Cardiovascular RisksAntipsychotics: Cardiovascular Risks

AntipsychoticsAntipsychoticsCardiovascular RisksCardiovascular Risks
2005 analysis of Tennessee Medicaid 2005 analysis of Tennessee Medicaid program reveals risk typicals = atypicalsprogram reveals risk typicals = atypicals
Recent study shows sudden cardiac death Recent study shows sudden cardiac death increased by about twofold amongst increased by about twofold amongst patients on APs, regardless of age*patients on APs, regardless of age*
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
*Ray WA, Chung CP, Murray KT, Hall K, Stein CM. (2009) Atypical antipsychotic drugs and the risk of sudden cardiac death.N Engl J Med. 2009 Jan 15;360(3):225-35

Antipsychotic RisksAntipsychotic RisksNeurologicNeurologic
Neuroleptic Malignant SyndromeNeuroleptic Malignant Syndrome–– Incidence with atypicals .2%Incidence with atypicals .2%–– Fever, encephalopathy, autonomic instability, Fever, encephalopathy, autonomic instability,
elevated CPK, rigid muscleselevated CPK, rigid muscles
Acute dystoniaAcute dystoniaE.g., torticollis E.g., torticollis E.g., oculogyric crisisE.g., oculogyric crisis
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotic RisksAntipsychotic RisksNeurologic (cont.)Neurologic (cont.)
AkathisiaAkathisia–– Unpleasant sensations of "inner" restlessnessUnpleasant sensations of "inner" restlessness–– inability to sit still or remain motionlessinability to sit still or remain motionless
DrugDrug--induced Parkinsonisminduced Parkinsonism–– Tremor (resting)Tremor (resting)–– Rigidity in movement, carriageRigidity in movement, carriage–– Postural instabilityPostural instability
Tardive DyskinesiaTardive Dyskinesia–– Drug induced abnormal involuntary movements of Drug induced abnormal involuntary movements of
face/jaw/mouth, trunk, limbsface/jaw/mouth, trunk, limbs–– Incidence on atypicals 0.8%, typicals 5.4%Incidence on atypicals 0.8%, typicals 5.4%
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

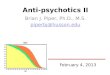
Shades of Neurologic ImpactShades of Neurologic Impact
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010
• Most typicals• Risperidone (Risperdal) especially
as dose increases• Note: Akathisia reported on
aripiprazole (Abilify) even at low doses
Higher Risk
• Quetiapine (Seroquel)
• Clozapine (Clozaril)
Lower Risk

Following Patients on Antipsychotics Following Patients on Antipsychotics for Neurologic Riskfor Neurologic Risk
TRUSt Big BeLtS TRUSt Big BeLtS
T T remorremor
R R estlessnessestlessness
U U nwanted movementsnwanted movements
St St iffnessiffness
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotics Risks Antipsychotics Risks MetabolicMetabolic
Increased weightIncreased weightIncreased blood sugar and frank DMIncreased blood sugar and frank DMIncreased lipidsIncreased lipids–– TriglyceridesTriglycerides–– CholesterolCholesterol–– LDL cholesterolLDL cholesterol–– ((⇓⇓ HDL cholesterol)HDL cholesterol)Increased BP as part of metabolic Increased BP as part of metabolic syndromesyndrome
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Shades of Metabolic ImpactShades of Metabolic Impact
• Clozapine (Clozaril)• Olanzapine (Zyprexa)
Higher Risk
• Quetiapine (Seroquel)• Risperidone (Risperdal)
Medium Risk
• Aripiprazole (Abilify)• Ziprasidone (Geodon)
Lower Risk
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Following Patients on Antipsychotics Following Patients on Antipsychotics for Metabolic Riskfor Metabolic Risk
TRUSt Big BeLtS TRUSt Big BeLtS
BigBig = BMI (weight, waist circumference)= BMI (weight, waist circumference)
B B lood pressurelood pressureee
L L ipidsipidstt
S S ugarugar
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

AntipsychoticsAntipsychoticsOther RisksOther Risks
SomnolenceSomnolenceDizzinessDizzinessHypotensionHypotensionSexual dysfunctionSexual dysfunctionDry mouthDry mouthLowering of seizure thresholdLowering of seizure thresholdHyperprolactinemiaHyperprolactinemiaLeukopenia Leukopenia –– agranulocytosis with Clozapine (Clozaril)agranulocytosis with Clozapine (Clozaril)
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Given the RisksGiven the RisksDonDon’’t Prescribe Lightlyt Prescribe Lightly
Make sure patients need the AP medicationMake sure patients need the AP medication–– Discover prior diagnoses by phoning hospitals, Discover prior diagnoses by phoning hospitals,
psychiatrists, CMHs, therapistspsychiatrists, CMHs, therapists–– Do NOT use for sleep when no other Do NOT use for sleep when no other
psychiatric diagnosis requiring AP existspsychiatric diagnosis requiring AP exists–– Consider other treatments for disruptive Consider other treatments for disruptive
behaviors in children without a firm behaviors in children without a firm psychiatric diagnosispsychiatric diagnosis
Partner with patient in making decision to usePartner with patient in making decision to use–– Risk/benefit discussionRisk/benefit discussion
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Given the RisksGiven the RisksWhat Do We Do When We Prescribe APs?What Do We Do When We Prescribe APs?
Track neurologic and metabolic Track neurologic and metabolic parametersparametersRespond to neurologic and metabolic Respond to neurologic and metabolic changeschanges–– Change antipsychotic or doseChange antipsychotic or dose–– Address metabolic changes medicallyAddress metabolic changes medically
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

AgendaAgenda
√√ When to consider antipsychotic use in the When to consider antipsychotic use in the Primary Care settingPrimary Care setting
√√ Review risk profiles of antipsychoticsReview risk profiles of antipsychotics
Safety tool for monitoring patients on Safety tool for monitoring patients on antipsychoticsantipsychotics
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotic Monitoring Form Antipsychotic Monitoring Form and Patient Education Handoutand Patient Education Handout
TRUSt Big BeLtSTRUSt Big BeLtS

Following Patients Following Patients on Antipsychotics: TRUSt Big BeLtSon Antipsychotics: TRUSt Big BeLtS
TT remorremorRR estlessnessestlessnessUU nwanted movementsnwanted movementsStSt iffnessiffnessBigBigBBlood pressurelood pressureeeLLipidsipidsttSSugarugar
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Following Patients Following Patients on Antipsychotics: TRUSt Big BeLtSon Antipsychotics: TRUSt Big BeLtS
TTremor: Ask, observe, remor: Ask, observe, documentdocument
RRestlessness: Ask, observe, estlessness: Ask, observe, documentdocument
UUnwanted movements: Ask, nwanted movements: Ask, observe walking, ask if observe walking, ask if others have noticed, others have noticed, documentdocument
StStiffness: Ask, observe, iffness: Ask, observe, check for cogwheeling, check for cogwheeling, documentdocument
BigBig = BMI (weight, waist = BMI (weight, waist circumference)circumference)
BBlood pressurelood pressureeeLLipidsipidsttSSugarugar
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

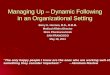
BaselineBaseline 4 4 weeksweeks
8 8 weeksweeks
12 12 weekweek
ssQuarterlyQuarterly AnnuallyAnnually
Every Every 5 5
yearsyears
PersonalPersonal/family /family historyhistory ++ ++Weight Weight (BMI)(BMI) ++ ++ ++ ++ ++Waist Waist circumcircum--ferenceference ++ ++BloodBloodpressurepressure ++ ++ ++FastingFastingplasma plasma glucoseglucose ++ ++ ++Fasting Fasting lipid lipid profileprofile ++ ++ ++
American Diabetes Association et al. Consensus Statement. Diabetes Care 2004.

Antipsychotics in Primary Care: Antipsychotics in Primary Care: SummarySummary
Appropriate usesAppropriate usesRemember risksRemember risks–– NeurologicNeurologic–– MetabolicMetabolic–– CardiovascularCardiovascular–– OtherOther
Can be a blessing when used appropriately, Can be a blessing when used appropriately, though these are serious drugsthough these are serious drugsSystematize monitoring for safer useSystematize monitoring for safer use
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotic ReferencesAntipsychotic ReferencesAdverse effects of antipsychotic medications.Adverse effects of antipsychotic medications.Muench J, Hamer AM. Am Fam Physician. Muench J, Hamer AM. Am Fam Physician. 2010 Mar 1;81(5):6172010 Mar 1;81(5):617--22.22.
Effectiveness of atypical antipsychotic drugs in patients with AEffectiveness of atypical antipsychotic drugs in patients with Alzheimer's disease.lzheimer's disease. Schneider Schneider LS, Tariot PN, Dagerman KS, Davis SM, Hsiao JK, Ismail MS, LebowLS, Tariot PN, Dagerman KS, Davis SM, Hsiao JK, Ismail MS, Lebowitz BD, Lyketsos CG, itz BD, Lyketsos CG, Ryan JM, Stroup TS, Sultzer DL, Weintraub D, Lieberman JA; CATIERyan JM, Stroup TS, Sultzer DL, Weintraub D, Lieberman JA; CATIE--AD Study Group.N AD Study Group.N Engl J Med. 2006 Oct 12;355(15):1525Engl J Med. 2006 Oct 12;355(15):1525--38.38.
Effectiveness of antipsychotic drugs in patients with chronic scEffectiveness of antipsychotic drugs in patients with chronic schizophrenia.hizophrenia.Lieberman JA, Lieberman JA, Stroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, KeefeStroup TS, McEvoy JP, Swartz MS, Rosenheck RA, Perkins DO, Keefe RS, Davis SM, Davis RS, Davis SM, Davis CE, Lebowitz BD, Severe J, Hsiao JK; Clinical Antipsychotic TriaCE, Lebowitz BD, Severe J, Hsiao JK; Clinical Antipsychotic Trials of Intervention ls of Intervention Effectiveness (CATIE) Investigators.N Engl J Med. 2005 Sep 22;35Effectiveness (CATIE) Investigators.N Engl J Med. 2005 Sep 22;353(12):12093(12):1209--23. Epub 23. Epub 2005 Sep 192005 Sep 19
Randomized controlled trial of the effect on Quality of Life of Randomized controlled trial of the effect on Quality of Life of secondsecond-- vs firstvs first--generation generation antipsychotic drugs in schizophrenia: Cost Utility of the Latestantipsychotic drugs in schizophrenia: Cost Utility of the Latest Antipsychotic Drugs in Antipsychotic Drugs in Schizophrenia Study (CUtLASS 1).Schizophrenia Study (CUtLASS 1).Jones PB, Barnes TR, Davies L, Dunn G, Lloyd H, Jones PB, Barnes TR, Davies L, Dunn G, Lloyd H, Hayhurst KP, Murray RM, Markwick A, Lewis SW. Arch Gen PsychiatrHayhurst KP, Murray RM, Markwick A, Lewis SW. Arch Gen Psychiatry. 2006 y. 2006 Oct;63(10):1079Oct;63(10):1079--87.87.
Atypical antipsychotic drugs and the risk of sudden cardiac deatAtypical antipsychotic drugs and the risk of sudden cardiac death.h. Ray WA, Chung CP, Ray WA, Chung CP, Murray KT, Hall K, Stein CM. N Engl J Med. 2009 Jan 15;360(3):22Murray KT, Hall K, Stein CM. N Engl J Med. 2009 Jan 15;360(3):2255--35. Erratum in: N Engl 35. Erratum in: N Engl J Med. 2009 Oct 29;361(18):1814.J Med. 2009 Oct 29;361(18):1814.
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010

Antipsychotic ReferencesAntipsychotic References
StahlStahl’’s Essential Psychopharmacology: s Essential Psychopharmacology: NeuroscientificNeuroscientific Basis and Practical Applications; Basis and Practical Applications; Third EditionThird Edition–– OnOn--line version at line version at neiglobal.comneiglobal.com
Sparrow/MSU FMRP Behavioral. Science TeamSparrow/MSU FMRP Behavioral. Science Team20102010