Embed Size (px)
Citation preview
Using Bar Code Technology to Improve Patient Safety
Objectives
Analyze the need for and benefits of a BPOC system for specimen collection.
State recommended guidelines for specimen collection including National Patient Safety Goals.
Evaluate technical requirements including hardware and software considerations.
Identify strategies for adoption of the technology.
Prepare metrics for measuring the impact of a bedside labeling program.
Case for Change
Joint Commission National Patient Safety Goal #1 requires two patient identifiers when providing care, treatment or services.
When collecting blood bank samples a two person process must be used or an automated ID technology.
All specimens must be labeled at the bedside and in front of the patient.
The College of American Pathologists recognizes patient identification as a cardinal safety goal.

The Impact of Identification Errors
Incidence of mislabeling errors found to be as high as 7%. (Howanitz, PJ, Renner SW, Walsh MK)
The American College of Pathologists has performed more than 130 studies on specimen errors.
34%-58% of total lab errors mislabeled specimens. (Bonini P, Plebani M, Ceriotti F, Rubboli F.)
Impact on Safety
1 of every 18 lab errors results
in an adverse event
Extrapolated to all the nation’s hospital-based laboratories:
160,900 adverse events per year as results of mislabeled specimens
(Valenstein PN, Raab SS, Walsh MK)
Good News
Interventions to increase awareness and emphasize patient ID can decrease errors
One institution decreased errors from 7% to 3% over two years. ( Howanitz PJ)
Tracking and immediate investigation decreased errors from 47% to 14% in another. (Quillen K, Murphy K)

Bar Code Technology
The Food and Drug Administration has proposed bar coding at the point of care for medication and blood product delivery
One institution was able to decrease identification errors by 77% after the implementation of bar code technology.
(Bolgna LJ, Mutter M)

Our Story

Howard County General Hospital
Where is Howard County General Hospital??

Joined Johns Hopkins Medicine in 1998.The only acute care medical facility in
Howard County, Maryland. Provided services to over 186,000 people
in 2009.227 beds
Who is Howard County General Hospital??

Cardiology Critical Care Gynecology Medicine Neonatology Obstetrics Orthopedics Pediatrics Perinatology Psychiatry Surgery
Inpatient Services

Anti-Coagulation Clinic Diagnostic Imaging Emergency Medicine Psychiatric Emergency Unit Rehabilitation Sleep Services Surgery Wellness/ Health Education Wound Care Center
Outpatient Services
Cardiology ObstetricsOncologyOrthopedicsPediatricsPsychiatrySurgery
Major Service Lines
Fifth largest private employer in Howard County
1,700+ full and part-time employees
60% live in Howard County
Employees
Fiscal Year 2009 Utilization Stats
74,653 Emergency Room Visits
17,425 Inpatient Admissions
3,084 Newborn Deliveries
13,309 Surgical Procedures
Our Laboratory
Receives over 500,000 specimens per year
Receives on average 1,400 specimens per day
Sends out on average 200 specimens per day
Our Blood bank
Transfusions per year
4,695 Packed Cells
645 Fresh Frozen Plasma
278 Pheresed Platelets
501 Rhogam doses
Our Story
All specimen collection decentralized and
performed by patient care technicians and
registered nurses.
PCTs and RNs receive extensive education on the
importance of patient ID
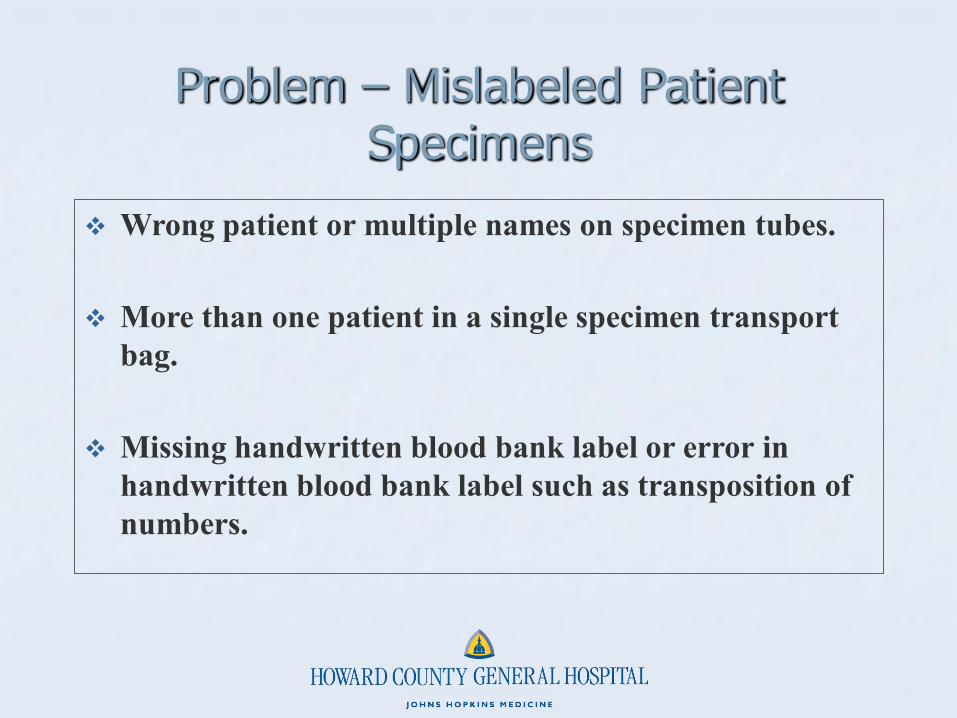
Problem – Mislabeled Patient Specimens
Wrong patient or multiple names on specimen tubes.
More than one patient in a single specimen transport bag.
Missing handwritten blood bank label or error in handwritten blood bank label such as transposition of numbers.

Problem Solving Approach Used – PDCA
PDCA (Plan–Do–Check–Act) - a four-step model for
carrying out change. Just as a circle has no end, the PDCA cycle should be repeated again and again for continuous improvement.
Problem Solving Approach Used – PDCA
PDCA Steps:
Plan - Plan a change, aimed at improvement.
Do – Carry out the change (preferably on a small
scale).
Check – Check the results – what was learned?
Act – Adopt the change, abandon it, or run through the
cycle again.
PDCA Cycle #1
Plan - Organized a focus group of Nurses and
Patient Care Technicians (PCTs) to analyze currentprocess.
Do – Made minor modifications to labels and
focused attention and staff education, accountability, anddisciplinary measures.
Check – Result - no measurable decrease in labeling
errors.
Act – Made decision to run process through a second
PDCA cycle.

PDCA Cycle #2
Plan - Organized a selection committee to
evaluate and ultimately select a phlebotomy positivepatient ID solution – a Request for Proposal (RFP)was distributed to five vendors.
Keys to system selection decision included: - bedside patient ID barcode scanning- bedside specimen label printing- real-time wireless communications
Committee unanimously agreed on the vendor and product of choice – contract was negotiated and signed.
PDCA Cycle #2 (continued)
Plan - Organized a Project Management Team
to develop the initial Phase 1 implementation planand a Project Implementation Team to execute thePhase 1 implementation plan. Phase 1 Project Scope: Six (6) inpatient units
Project Management Team – Included the Director of Nursing, applicable nurse managers, Clinical Education, IT, and the Laboratory’s LIS Coordinator.
Project Implementation Team – Included the above, plus a PCT from each inpatient unit.
PDCA Cycle #2 (continued)
Plan - Evaluated, selected, and deployed the
required hardware needed for the Phase 1implementation (PDA and COW deployment).
- Wireless PDAs- Wireless Printers- Computer on Wheels (COW)

PDCA Cycle #2 (continued)
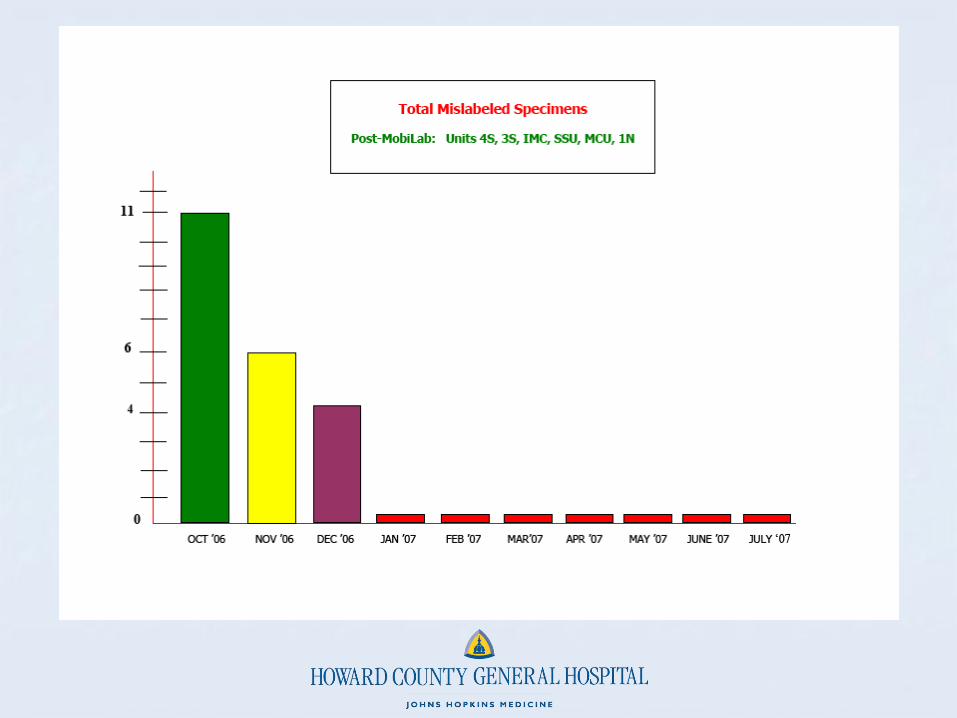
Do - Initially implemented the system on one pilot
inpatient unit – 3South (October 2006) and monitored results.
Once pilot unit was proven to be stable, proceeded with implementation in the remaining five (5) inpatient units – 1North, 4South, IMC, MCU, and SSU –monitoring results as well (October - December 2006).
Extensive staff training was required and was completed right before each unit’s Go LIVE date.
PDCA Cycle #2 (continued)
Check – Measured and compared mislabeled
specimen statistics before, during, and after Phase 1implementation of system.
PDCA Cycle #2 (continued)
Act – Continued monitoring results of the system’simpact on mislabeled specimens.
Implemented Phase2 and Phase 3 (final) implementations.
Phase 2 – Project scope included ICU (7/2007), NICU (7/2007), Pediatrics (12/2007), ED (2/2008), and Labor/Delivery (6/2008).
Phase 3 Project scope included Ambulatory Surgery and PACU (6/2009)

LABORATORY BENEFITS
FASTER RECEIVE PROCESS
NO MORE HANDWRITTEN INITIALS TO
DECIPHER
NO TRANSCRIPTION ERRORS ON
HANDWRITTEN BLOOD BANK LABELS
NO MORE SECOND SIGNATURE REQUIRED
ON BLOOD BANK LABELS

MEDITECH RECEIVE ROUTINE
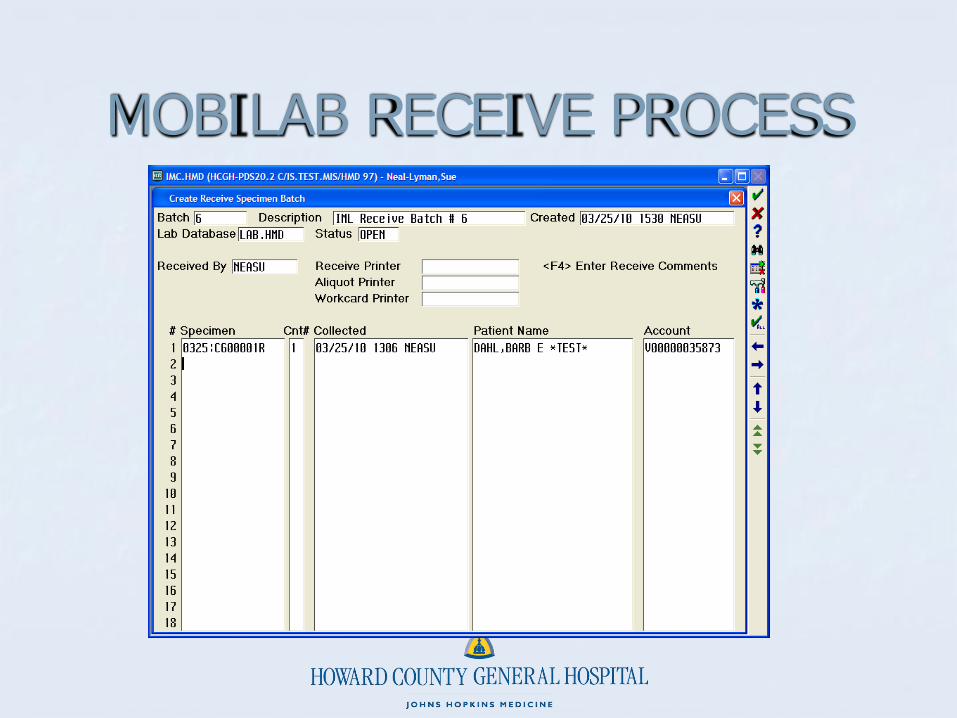
MOBILAB RECEIVE PROCESS
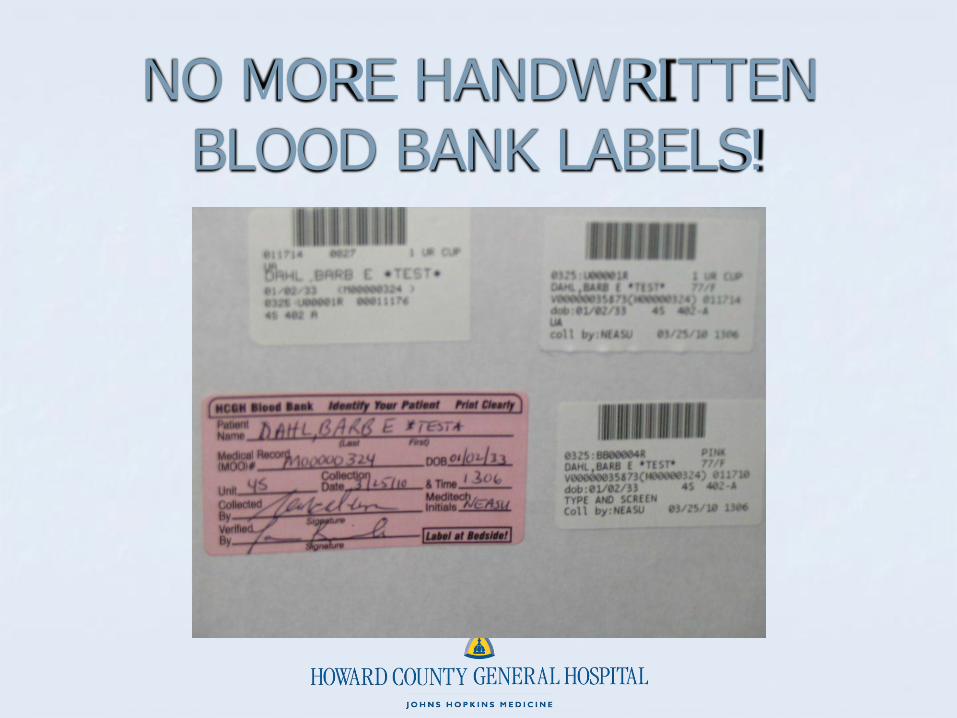
NO MORE HANDWRITTEN BLOOD BANK LABELS!

Results To Date
All Mislabelled Specimens
2007-2010
0
5
10
15
20
Month
Nu
mb
er
of
Sp
ec
ime
ns
Mislabelled Specimens 17 18 13 11 8 12 11 8 6 7 13 5 6 6 7 1 2 3 2 3 1 1 0 1 3 2 1 4 5 0 1 5 0 2 1 0 5
Ma
r
Ap
r
Ma
yJun Jul
Au
g
Se
pOct
No
v
De
c
Jan
08
Fe
b
Ma
r
Ap
r
Ma
yJun Jul
Au
g
Se
pOct
No
v
De
c
Jan
09
Fe
b
Ma
r
Ap
r
Ma
yJun Jul
Au
g
Se
ptOct
No
v
De
c
Jan
10
Fe
b
Ma
r
Sources of Errors
Training: new employees putting multiple
patients in one transport bag.
Technology not implemented: Dialysis
Wireless network down
Unable to scan wristband

Foundations of Success
Patient focused attitude leading to teamwork between
laboratory and nursing managers and staff
Committed IT department. Robust wireless network
KEY.
Investment in sufficient equipment.
Immediate follow up and accountability
Sharing of data and celebration of success with staff.

Thank you for listening!!
Presenters:
Nancy Smith, MAS, RN Senior Director Patient CareHoward County General Hospital(410) [email protected]
Sue Neal-Lyman BS MT (ASCP) LIS CoordinatorJohns Hopkins Hospital Laboratory at Howard County General(410) [email protected]

References
1. Bonini P, Plebani M, Ceriotti F, Rubboli F. Errors in laboratory medicine. Clin
Chem. 2002;48(5): 691-698
2. Bolgna LJ, Mutter M. Life after phlebotomy deployment; reducing major patient
and specimen identification errors. J Healthc Inf Manag. 2002;16(1):65-70
3. Howanitz, PJ. Errors in laboratory medicine. Arch Pathol Lab Med.
2005;(129):1252-1261
4. Howanitz, PJ, Renner SW, Walsh MK. Continuous wristband monitoring over 2
years decreases identification errors. Arch Pathol Lab Med. 2002;(126):809-815
5. Quillen K, Murphy K. Quality Improvement to decrease specimen mislabeling in
transfusion medicine. Arch Pathol Lab Med. 2006;(130):1196-1198
6. The Joint Commission. 2009 National patient safety goals hospital program.
Published October 31, 2008
7. Valenstein, PN, Raab SS, Walsh MK. Indentification errors involving clinical
laboratories. Arch Pathol Lab Med. 2006;(130):1106-1113.





























