Embed Size (px)
Citation preview
3/24/2015
1
©Pathway Health 2013
Using QAPI and PIPs for Accident and Fall
Prevention
Sue LaGrange, RN, BSN, NHA
Director of Education
Pathway Health
1
©Pathway Health 2013
Upon completion of this program, attendees will be able to:
1. Understand the falls risk assessment, principles of QAPI, and person-centered care
2. Review case study demonstrating practical application of investigation
techniques and current evidence-based interventions
3. Provide tools to develop an effective Falls Prevention Process Improvement Program
Objectives
2
©Pathway Health 2013
This process is a fluid process
• Change
– New Regulations
– Updates in Standards of Practice
– Culture of our buildings
– Learning is ongoing to meet the individualized quality and safe care for the residents!
– Continuous process of determining the best possible means of providing quality
QAPI
3
3/24/2015
2
©Pathway Health 2013
CMS has provided various tools on the website: http://cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/qapitools.html
• Self-Assessment
• Various Guides
• Goal setting
• Resources
QAPI Tools
4
©Pathway Health 2013
QA – Quality Assurance (F520 QA&A, Quality assessment & assurance)
– Identifies and corrects quality issues
– Retrospective
– Focus on outliers or individuals
– Efforts end once achieved
– DON, Physician and 3 staff members
– Meet quarterly
QAPI
5
©Pathway Health 2013
– Proactive approach
– Efforts are on-going
– Focus on system changes
– Plan involves input from staff representing all roles and disciplines within the organization
– Meet at more frequent intervals
Performance Improvement
6
PI - Performance Improvement
3/24/2015
3
©Pathway Health 2013
Because quality assurance is already in place in your nursing home, the added
emphasis is on Performance Improvement.
They compliment each other and are both key in successful outcomes.
QA is Already in Our SNF
7
©Pathway Health 2013
AIM, POINT OF VIEW-- • Old QA: Retrospective — looking backward,
PROBLEM TO SOLUTION • New QAPI: Proactive, Preventative — looking
forward SCOPE— • Old QA: Silo approach, department oriented • New QAPI: Facility wide, cooperation, support METHOD— • Old QA: Audits to inspect if standards are met • New QAPI: Systematic data-driven to identify PI
OLD QA & NEW QAPI
8
©Pathway Health 2013
FOCUS— • Old QA: Mistakes, Finding outliers; solving problems • New QAPI: Improving processes & systems,
Considering balance between quality of life & quality of care outcomes
EMPLOYEE/LEADERSHIP— • Old QA: Quality assurance coordinators & assigned QA
team; Very little direct involvement of senior leaders • New QAPI: Expectation of all staff (Front Line Staff)
involved in PI, some as PI leaders, Residents as Performance leaders
OLD QA & NEW QAPI
9
3/24/2015
4
©Pathway Health 2013
• QAPI (Quality Assurance & Performance Improvement)
– Systematic,
– Comprehensive,
– Data-driven,
– Proactive approach
10
QAPI
QAPI
System Changes
©Pathway Health 2013
A fluid CHANGE process supporting
– New Regulations & updates in Standards of Practice
– Culture of the facility
– Ongoing learning to meet individualized quality & safe care for residents – Continuously determining the best possible
means of providing quality
QAPI Characteristics
11
©Pathway Health 2013
QAPI is resident-centered yet built on systems thinking.
QAPI involves everyone who works in your facility.
12
3/24/2015
5
©Pathway Health 2013
Systemic Analysis and Systemic Action
Performance Improvement Projects
Feedback data systems and Monitoring
Design and Scope Governance and
Leadership
Elements for QAPI in SNFs
13
©Pathway Health 2013
• You can find the detailed descriptions of the 5 elements on the CMS website:
http://cms.gov/Medicare/Provider-Enrollment-and-
Certification/SurveyCertificationGenInfo/Downloads/fiveelementsqapi.pdf
5 Elements
14
©Pathway Health 2013
Performance Improvement Projects:
Key to Success
PIPs
15
3/24/2015
6
©Pathway Health 2013
Performance Improvement Projects examine performance & make improvements
• In any area needing attention
Or
• Found to be a high priority based on the needs of the residents.
PIP
16
©Pathway Health 2013
Define roles & agree on working ground rules
– Gather improvement ideas from the team
– Pick an idea to test & clearly define it
– Design a good test of the change you want to make from the idea
Work with the Team
17
©Pathway Health 2013
What do we want to do?
• For whom
• By when
• How can we make it happen
PIP Key Questions
18
3/24/2015
7
©Pathway Health 2013
Sources
• MDS - problem patterns
• Nursing Home Compare
• Recent state surveys
• Resident & family satisfaction
• Caregiver turnover & absence
• Patterns of ER & hospital use
Reviewing Your Data
19
©Pathway Health 2013
F323: Prevention of Accidents
20
©Pathway Health 2013
• Intent is that the facility provides an environment that is free from hazards over which the facility has control and
• Provides appropriate supervision to each
resident to prevent avoidable accidents.
F323
21
3/24/2015
8
©Pathway Health 2013
Accident occurred when:
• Environmental hazards had been identified
• Resident risks were identified
• Hazards & risks were assessed
• Interventions were implemented to decrease hazards and risk
• Effectiveness of interventions were being monitored and modified as needed
Definition: Unavoidable Accident
22
©Pathway Health 2013
Accident occurred related to failure to:
• Identify environmental hazard
• Identify individual resident risk factors
• Evaluate/analyze hazards & risks
• Implement interventions to reduce an accident
• Monitor and modify interventions as needed
Definition: Avoidable Accident
23
©Pathway Health 2013
• Resident Risk Identification
• Resident Assessment Risk Factors
• Resident Vulnerabilities
• Realistic Goals
• INVESTIGATION and Root Cause Analysis
• Accident Prevention
• Interventions – Creative – Individualized
Steps for System Overview:
24
3/24/2015
9
©Pathway Health 2013
• Assessment Process
• Assistance/Assistive Devices
• Environment/Resident Environment
– Rooms
– Unit Areas
– Common Use Areas
– Facility Grounds
**Alarms, Doors, Cameras, etc.
F323: PREVENTION IS KEY!!
25
©Pathway Health 2013
• Previous elopement attempts
• Cognitive Status
• Change in Cognition
• Change in Condition (infection, new meds, etc.)
• Behaviors (resistance to care, impulsive, agitation, wandering, etc.)
• Verbalizations of leaving the facility or going home, to work, etc.
• Past life experiences
Assessment Process
26
©Pathway Health 2013
On an ongoing basis and at least quarterly, the facility staff will want to reassess:
• Any increased behaviors
• Additional attempts to elope
• Decrease in risk for elopement
• Review and revision (if needed) of the care plan
Assessment Process-continued
27
3/24/2015
10
©Pathway Health 2013
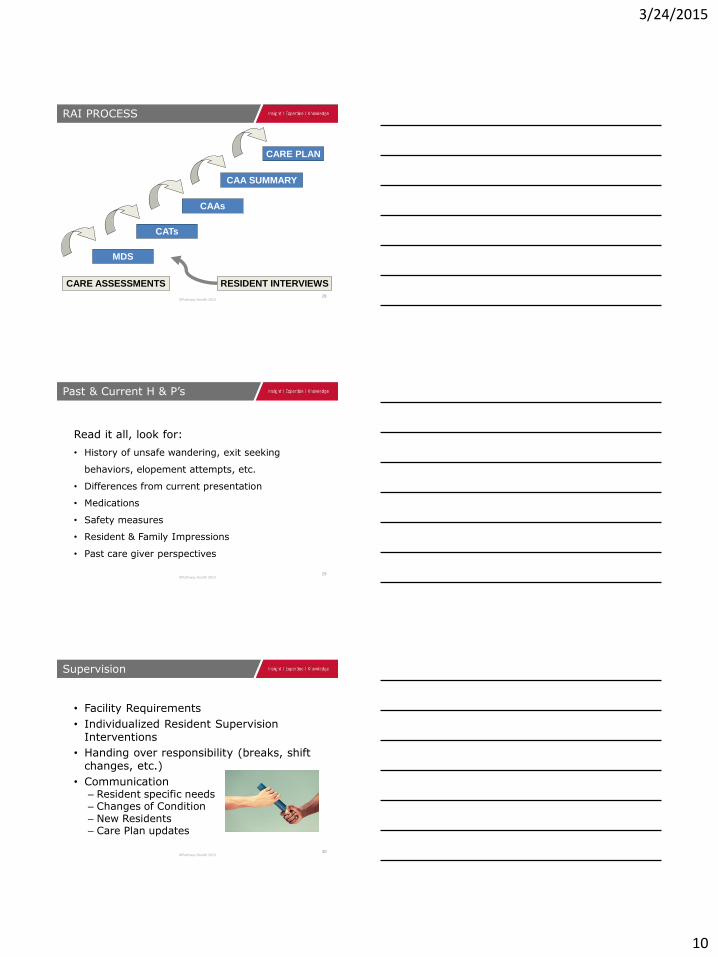
RAI PROCESS
28
MDS
CATs
CAAs
CARE PLAN
CAA SUMMARY
CARE ASSESSMENTS RESIDENT INTERVIEWS
©Pathway Health 2013
Read it all, look for:
• History of unsafe wandering, exit seeking
behaviors, elopement attempts, etc.
• Differences from current presentation
• Medications
• Safety measures
• Resident & Family Impressions
• Past care giver perspectives
Past & Current H & P’s
29
©Pathway Health 2013
• Facility Requirements
• Individualized Resident Supervision Interventions
• Handing over responsibility (breaks, shift changes, etc.)
• Communication – Resident specific needs – Changes of Condition – New Residents – Care Plan updates
Supervision
30
3/24/2015
11
©Pathway Health 2013
Falls Risk Assessment
31
©Pathway Health 2013
• Identification of a baseline in order for individualized precautions and care planning
• To achieve each resident’s highest level of functioning
• To prevent and/or reduce injuries related to falls
• To enhance dignity and self-worth for the resident
• To rehabilitate or restore function
Purpose of Falls Risk Assessment
32
©Pathway Health 2013
• On Admission
• On Re-Admission
• Quarterly
• With a Change in Condition
When to do a Fall Risk Assessment
33
3/24/2015
12
©Pathway Health 2013
• History of Falls/Accidents
• Diagnoses
– Cardiac, Neurological, Elimination concerns, Orthopedic, Perceptual, Cognitive, Psychological, etc.
• Physical Device Use
• Environment
• Medications
• Elopement or Wandering
• Behaviors or Cognitive Impairment – Safety Awareness
– Compliance
• Root Cause Analysis
Potential Areas to Assess
34
©Pathway Health 2013
• Residents with recent surgery or new admissions
• Psychotropic drug use
• Fall history
• Appropriate clothing and footwear
• Visual deficits
• Impaired mobility/functional
status
• Incontinence
• Change of environment
• Cognitive status
• Mood or behavior indicators
• Underlying illness and disease processes
• Sensory status
• Orthostatic hypotension
Other Considerations
35
©Pathway Health 2013
How Can We Develop a PIP (QAPI) for an Effective Falls Management Program?
36
3/24/2015
13
©Pathway Health 2013
• Put together a team
• Education
• Organizational Buy In!
• Identify a “Falls Champion”
• Promote an Interdisciplinary Approach
• Identify Team Responsibilities
Develop a PIP
37
©Pathway Health 2013
• Policies and Procedures
• All Staff Education
• Fall Culture
• Resident and Family Education
• Assessment Process
• Incident/Accident Process
• Forms and Documentation
• Follow Up
Review Your System
38
©Pathway Health 2013
After a Fall:
• Team Huddle
• Post Fall Investigation
• Root Cause Analysis
• Document Objective Findings
• Assess/Reassess
• Evaluate effectiveness of interventions
Post Fall Action
39
3/24/2015
14
©Pathway Health 2013
Early problem identification
• Examination of root causes
• Use of data & feedback from multiple sources • Understanding how systems of care affect quality
outcomes
• Systemic action
• Involvement of all staff in the quality mission
Required QAPI Components
40
©Pathway Health 2013
Commit to a culture of safety
• What do you look for?
• What do you reward?
• How can you tell when it’s in place?
Safety First
41
©Pathway Health 2013
If injured, it can take months to recover, often in a nursing facility, & mobility can be permanently changed.
• By offering effective fall prevention programs, we can reduce falls & help older adults live safer, happier, longer lives.
Resident Considerations
42
3/24/2015
15
©Pathway Health 2013
Establish your commitment to Independence and Safety
• Educate about fall risk factors & prevention strategies for older adults, families, & caregivers
• Environmental assessment & intervention including resident input
• Exercise must be offered as a way to promote independence!
An Effective Program
43
©Pathway Health 2013
Establish your commitment to Falls & Injury Prevention
• Pre-admission considerations
• Admission assessment
• ALWAYS include them in assessment findings & education if responsible, or with resident permission
Resident/Family Alliances
44
©Pathway Health 2013
Run a report of Current Mobility Status for this quarter and last quarter – walk in room, walk in corridor
• Compare it to report from last quarter
• Have there been changes, declines?
Use Your Data – MDS
45
3/24/2015
16
©Pathway Health 2013
By location, diagnosis, behaviors, and functional status – the more detailed your information is, the more effective your root cause analysis will be.
• Location - room, hallway, bathroom
• Devices in use, call lights, alarms etc.
What to Look For - Trending
46
©Pathway Health 2013
Getting to the reasons for the mobility decline and other risk factors is called Root Cause Analysis
• Interview direct care-giving staff, family, & resident for their perspectives regarding why the decline happened
• Document and analyze interview results
Questions
47
©Pathway Health 2013
• Poor lighting
• Loose rugs
• Poorly fitting shoes
• Beds or toilets without handrails
• Clutter
External Factors
48
3/24/2015
17
©Pathway Health 2013
• Unsteady gait
• Balance problems
• Weak muscles
• Poor vision/ hearing loss
• Medications
• Dementia (memory loss & confusion)
Internal Risk Factors
49
©Pathway Health 2013
• Are doors easy to open & close for those with mobility issues
• How long are the hallways? Are there are benches along the way to destinations
• Is there plenty of closet space & storage available to reduce clutter
Safety in Mind
50
©Pathway Health 2013
Remain in place, wait for direction?
• Get up to see what’s wrong?
• See what you can do to help?
Your Response to Alarms
51
3/24/2015
18
©Pathway Health 2013
* Risk assessment tools by themselves do not prevent patient falls - they predict them…
*National Patient Safety Foundation Professional Learning Series
Risk Assessment Tools
52
©Pathway Health 2013
Current Mobility Status
• Seating
• Standing
• Transfers
• Toileting Needs
• Footwear
Note resident & family response to immediate safety measures – cooperation is the key to
accident prevention!
Assessment - Mobility
53
©Pathway Health 2013
Problems with unsafe, uncomfortable seating can lead to restlessness and falls risk
• People slide into a position of comfort & support. However . . . everyone fatigues out of the ideal sitting posture
• Body type & disability often prevent ideal sitting posture
Seating Challenges
54
3/24/2015
19
©Pathway Health 2013
Do not wait until a fall happens to check for:
• Effects
• Side effects
• Interactions
Plan for Falls Prevention!
Anticipate Medication Risks
55
©Pathway Health 2013
Look at Medical Conditions for Risk:
• Hypertension
• Angina
• Parkinson's Disease Urine Output
• Constipation
• Heart Rate & Rhythm
• Pain
These Conditions = Risk
56
©Pathway Health 2013
• Involuntary movements
• Low blood pressure with position changes
• Heart rhythm changes
• Cause drowsiness, imbalance, incoordination, slowed reactions, dizziness, confusion.
• Poor impulse control
• Hyperglycemia
Psychotherapeutic Effects
57
3/24/2015
20
©Pathway Health 2013
Excessive decrease in ability to form blood clots can cause bleeding, leading to anemia, weakness & dizziness.
Watch for bruising easily, unusual bleeding around gums, blood in urine, or rectal bleeding.
Anticoagulants
58
©Pathway Health 2013
Effective Investigation
59
©Pathway Health 2013
To get the most out of critical times around an event
Staff on the scene must be coached in skills of observation and critical thinking
Begin Immediately
60
3/24/2015
21
©Pathway Health 2013
Delaying the investigation until morning or Monday, or whenever the DON or Risk
Manager gets around to it will not improve your outcomes or statistics.
Don’t Wait!
61
©Pathway Health 2013
Assigned nurse/care assistants/Others on duty
• Supervisor
• Dining Services Staff
• Housekeeping/Maintenance
• Administrator/Clinical Managers
More eyes & ears = more thorough perspectives
Assemble Key Players
62
©Pathway Health 2013
Placement of the person’s body at the time of the fall
• What was the person trying to do?
• Was it unusual or typical – has it happened before?
Observations + Questions
63
3/24/2015
22
©Pathway Health 2013
If they don’t, or didn’t wait – WHY?
what makes them unsafe to do it independently?
weakness, stiffness, dizziness…?
And Then What
64
©Pathway Health 2013
If they are known not to call for help, what are you doing to make it safer for them?
Strengthen, loosen up, address causes of
dizziness
Compensation VS Restriction
65
©Pathway Health 2013
• Watch them in action to assess correct use
• Therapies evaluation to identify modifications
• Do not let the device be a potential cause for falls
Use of Devices
66
3/24/2015
23
©Pathway Health 2013
Make immediate modifications based on causes
• Communicate interventions & rationales to everyone to reinforce safety as soon as possible
Critical Investigation Elements
67
©Pathway Health 2013
Leadership supports staff participation in all stages of problem solving, providing time & materials.
• Assure that full support is observable & positively viewed by your staff - Talk it up & follow up with actions
• Integrate the process with other efforts & find ways to make the most of times the team gets together
• Interview & ask how you can better help them participate
Leadership
68
©Pathway Health 2013
Residents, Family & Staff provide feedback regarding problem identification, intervention development, & goal setting.
• Get signatures on postings, meeting minutes & plans indicating participation
• Include QAPI in admission process (packet), staff explain and discuss with residents and families
• Include QAPI in orientation & other in-services, give opportunities for all to participate
Facility-wide Participation
69
3/24/2015
24
©Pathway Health 2013
On-going coaching & mentoring should accompany training to assure success.
• Lead by example, train department heads & supervisors to actively incorporate new information & changes into daily routine
• Be a cheerleader & maintain positive support (expect the same from the team)
• Be patient & consistent, ask how you can help
Coach & Mentor
70
©Pathway Health 2013
Test processes & changes on a small sample to work out the barriers & unforeseen issues before full roll out.
• Take suggestions supported by data (QM’s, QI’s, etc.)
• Solicit enthusiastic staff, ask for volunteers (one unit, one hallway, etc.)
• Use PDSA cycle to test, work out the bugs (retest till a smooth process is found, keep measuring results)
Small Sample Testing
71
©Pathway Health 2013
Monitor progress, maintain electronic records of projects.
• Showcase successes
• Stay organized, current & connected to the data
• Be able to pull out & review, revisit
Record Keeping
72
3/24/2015
25
©Pathway Health 2013
Establish QAPI as THE process for monitoring quality.
• Include QAPI discussions at every meeting, add agenda items to all routine meetings
• Be sure staff are fluent in answering questions about QAPI and any PIPs in the facility
• Remember, surveyors may be using the same process to review regulatory compliance
Use QAPI Format
73
©Pathway Health 2013
Implement QAPI to develop an effective way of planning, working, & problem-solving together
• Not only about meeting the minimum standards, but about continually aiming higher
• Not just about compliance, about inventing better ways of providing care & service
HOW CAN YOU DEMONSTRATE THIS MISSION?
The Problem-Solving Model
74
©Pathway Health 2013
Audit your system for success:
• F323 Rounds by the IDT
• Hazard Identification
• Fall Audits
• Incident/Accident Reports
* Use these audits to correct the system through your QA process for success!
Teach PIP Team to Audit
75
3/24/2015
26
©Pathway Health 2013
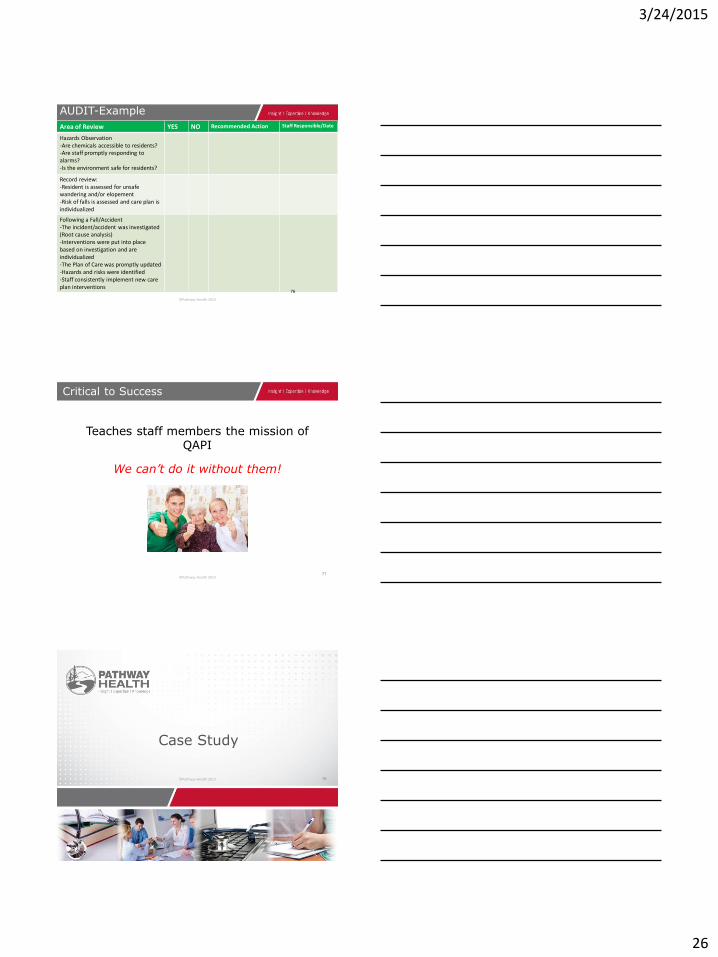
Area of Review YES NO Recommended Action Staff Responsible/Date
Hazards Observation -Are chemicals accessible to residents? -Are staff promptly responding to alarms? -Is the environment safe for residents?
Record review: -Resident is assessed for unsafe wandering and/or elopement -Risk of falls is assessed and care plan is individualized
Following a Fall/Accident -The incident/accident was investigated (Root cause analysis) -Interventions were put into place based on investigation and are individualized -The Plan of Care was promptly updated -Hazards and risks were identified -Staff consistently implement new care plan interventions
AUDIT-Example
76
©Pathway Health 2013
Teaches staff members the mission of QAPI
We can’t do it without them!
Critical to Success
77
©Pathway Health 2013
Case Study
78
3/24/2015
27
©Pathway Health 2013
On the Scene Investigation
79
alarmed chair
Alarmed
©Pathway Health 2013
Tools (Examples)
80
©Pathway Health 2013
Fishbone – Root Cause Analysis Tool
81
3/24/2015
28
©Pathway Health 2013
QAPI Action Plan (Tool Example)
82
©Pathway Health 2013
QAPI News Brief Volume1, 2013:
• http://www.cms.gov/Medicare/Provider-Enrollment-and-Certification/QAPI/Downloads/QAPINewsBrief.pdf
• http://www.ihi.org/knowledge/Pages/HowtoImprove/ScienceofImprovementHowtoImprove.aspx
– Langley GL, Nolan KM, Nolan TW, Norman CL, Provost LP. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance (2nd edition). San Francisco: Jossey-Bass Publishers; 2009.
Resources
83
©Pathway Health 2013
• http://psnet.ahrq.gov/primer.aspx?primerID=10
• http://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/downloads/som107ap_pp_guidelines_ltcf.pdf
• http://www.cdc.gov/HomeandRecreationalSafety/Falls/nursing.html
• https://www.nhqualitycampaign.org/goalDetail.aspx?g=mob
References and Helpful Websites
84
3/24/2015
29
©Pathway Health 2013
Advancing Excellence in America’s Nursing Homes:
https://www.nhqualitycampaign.org/
Stratis Health:
http://www.stratishealth.org/providers/QAPI.html
**The Plan-Do-Study-Act (PDSA) cycle was originally developed by Walter A. Shewhart as the Plan-Do-Check-Act (PDCA) cycle. W. Edwards Deming modified Shewhart's cycle to PDSA, replacing "Check" with "Study." [See Deming WE. The New Economics for Industry, Government, and Education. Cambridge, MA: The MIT Press; 2000.]
Resources
85
©Pathway Health 2013
• http://www.ncoa.org/improve-health/center-for-healthy-aging/falls-prevention/falls-prevention-awareness.html
• http://www.stopfalls.org/service_providers/sp_bm.shtml
• Veteran’s Administration projects
• http://www.visn8.va.gov/patientsafetycenter/fallsTeam/
• Institute for Person Centered Care
• http://ubipcc.com/
• http://www.seniorhomes.com/p/assisted-living-safety/
Resources
86
©Pathway Health 2013
Vibrant Living Concepts
http://blog.actionpact.com/2013/07/29/vibrant-living-prevents-falls-and-eliminates-need-for-alarms/
http://actionpact.com/index.php/product/eliminating-alarms-and-reducing-falls-by-engaging-with-life
Sue Ann Guildermann, RN, BA, MA. Effective Fall Prevention Strategies Without Physical Restraints or Personal Alarms Empira, 4/24/2012 Webinar for Stratis Health
Resources
87
3/24/2015
30
©Pathway Health 2013
Willy BA; Wheelchair Seating for Elders; On line pamphlet prepared under contract for Mountain Pacific Quality Health– Wyoming 2010. http//:www.mpqhf.com/WCSbooklet508.pdf
Illustrations by Chris Willy; Web publication by Mountain Pacific Quality – Wyoming’s 9th Scope of Work CMS; Wheelchair Seating for Elders by BA Willy. http://www.cdc.gov/homeandrecreationalsafety/images/cdc_guide-a.pdf
http://www.cdc.gov/homeandrecreationalsafety/images/cdccompendium_030508-a.pdf
88
Resources
©Pathway Health 2013
• Newsletter & CEUs – Initiatives in Safe Patient Care
• http://initiatives-patientsafety.org/Initiatives2%20.pdf
• www.cdc.gov/injury/STEADI
• http://www.npsf.org/wp-content/uploads/2013/03/PLS_1302_FallPrevention_LAG_MF.pdf
• http://www.cdc.gov/homeandrecreationalsafety/falls/adultfalls.html
Resources
89
©Pathway Health 2013
Questions
90
3/24/2015
31
©Pathway Health 2013
Thank You!
91





























