Embed Size (px)
Citation preview

1
Using Surveys to Assess Patient‐Centered Factors that May Affect Responses to Chronic Pain
Treatment
Carol Greco, PhD1; Lan Yu, PhD1; Paul Pilkonis, PhD1
1University of Pittsburgh, Pittsburgh, Pennsylvania
Original Project Title: Measuring the Context of Healing: Using PROMIS in Chronic Pain TreatmentPCORI ID: ME‐1402‐10114 HSRProj ID: 20152286 ClinicalTrials.gov ID: NCT02873429
_______________________________ To cite this document, please use: Greco V, Yu L, Pilkonis P.(2019). Using Surveys to Assess Patient‐Centered Factors that May Affect Responses to Chronic Pain Treatment. Washington, DC: Patient‐Centered Outcomes Research Institute (PCORI). https://doi.org/10.25302/4.2019.ME.140210114

2
Table of Contents ABSTRACT ........................................................................................................................................... 3 BACKGROUND .................................................................................................................................... 4 PATIENT AND STAKEHOLDER ENGAGEMENT ....................................................................................... 9 METHODS ........................................................................................................................................... 9
Study Overview and Study Design ....................................................................................................................... 9
Study cohort ......................................................................................................................................................... 9
Inclusion and Exclusion Criteria. ........................................................................................................................ 10
Data Collection................................................................................................................................................... 12
Outcome Measures for Aims 1 and 2 ................................................................................................................ 13
Baseline Computerized Assessment .................................................................................................................. 13
Follow‐up Computerized Assessments (2 Months and 4 Months) .................................................................... 18
Patient Baseline Cognitive Interview ................................................................................................................. 18
Patient Follow‐up Cognitive Interview ............................................................................................................. 18 Clinician Baseline Cognitive Interview. .............................................................................................................. 19 Clinician Follow‐up Cognitive Interview. ........................................................................................................... 19
Aim 1 utilized correlation and multiple linear regression (ordinary least squares estimation) to test the
proposed hypotheses ........................................................................................................................................ 19
Aim 2: Heterogeneity of Treatment Effects ....................................................................................................... 20
Aim 3 involved direct, in‐person feedback from
patients and clinicians and used patient voices in research. ........................................................................... 20
Study protocol ................................................................................................................................................... 21
RESULT .............................................................................................................................................. 21
Descriptive Information About the Study Participants. ..................................................................................... 21
Results of Analyses for Aim 1: Are baseline scores on HEAL measures predictive of outcomes? ..................... 27
HEAL and Clinical Global Impression.. ............................................................................................................... 27
HEAL and PROMIS Pain Intensity and Interference ........................................................................................... 30
Results of Analyses for Aim 2: Heterogeneity of Treatment Effects. ................................................................ 32
Results of Analysis of Aim 3. .............................................................................................................................. 38
DISCUSSION ........................................................................................................................... 41 Decisional context.............................................................................................................................................. 41
The study results in context ............................................................................................................................... 42
Implementation of study results ....................................................................................................................... 43
Generalizability .................................................................................................................................................. 44
Subpopulation Considerations ........................................................................................................................... 44
Study limitations ................................................................................................................................................ 45 Future research .................................................................................................................................................. 46
CONCLUSION ......................................................................................................................... 46
REFERENCES .......................................................................................................................... 48
APPENDIX .............................................................................................................................. 51

3
B. Abstract
Background: Nonspecific, contextual factors are seldom measured in research trials or clinics, yet they
can influence outcomes. This project evaluated the Healing Encounters and Attitudes Lists (HEAL) and
Patient‐reported Outcomes Measurement Information System (PROMIS) measures during pain
treatment. HEAL includes Patient‐Provider Connection, Healthcare Environment perceptions, Treatment
Expectancy (TEX), Positive Outlook (POS), Spirituality (SPT), and Attitudes Toward
Complementary/Alternative Medicine (CAM). We addressed heterogeneity of treatment effects (HTE),
the methods gap, by comparing outcomes in patient subgroups: persons receiving CAM versus
conventional treatments and, separately, patient subgroups who had higher and lower scores on HEAL
TEX.
Objective: Specific research questions:
1. Do nonspecific factors, assessed by HEAL, predict pain treatment outcomes?
2. Do the PROMIS and HEAL measures contribute to an understanding of which subgroups of
patients may benefit from pain treatments?
3. Do patients and clinicians find HEAL, PROMIS, and the American Chronic Pain Association (ACPA)
Pain Log to be useful in treatment?
Methods: In this prospective observational study, persons with chronic pain starting a CAM (eg,
acupuncture, chiropractic; n = 109) or a conventional medicine treatment (eg, physical therapy,
medication management; n = 100) completed HEAL and PROMIS measures online at baseline and at 2
and 4 months later. They rated clinical global improvement (CGI) at follow‐ups. Correlations and
multiple regression were the main analytic strategies. We compared CAM and conventional patients as
well as those with lower and higher HEAL TEX in order to evaluate HTE. A subset of patients (n = 44) and
clinicians (n = 13) completed interviews on the clarity and clinical utility of HEAL, PROMIS, and ACPA Pain
Log.
Results: Baseline HEAL TEX, POS, and CAM were correlated with follow‐up PROMIS Pain Intensity, and
baseline HEAL TEX, POS, CAM, and SPT were correlated with PROMIS Pain Interference. All baseline
HEAL scores except those for Spirituality were correlated with CGI at 2 and 4 months (Spearman rho, all
p value < 0.05). In final regression models, baseline HEAL TEX and baseline Pain Intensity accounted for
42% of the variance in 4‐month Pain Intensity, with HEAL TEX contributing 2% additional variance over
baseline Pain Intensity. Baseline HEAL CAM, SPT, and POS accounted for 2.1%, 1.7%, and 1.5%,
respectively, of 4‐month follow‐up Pain Interference variance beyond that accounted for by baseline
Pain Interference. Regarding subgroup comparisons based on receiving CAM versus conventional

4
treatments, the conventional treatment group had higher PROMIS Average Pain, Pain Interference, and
Pain Intensity; lower Physical Functioning; and poorer Overall Health compared with the CAM treatment
group at all time points. The lower TEX group had higher pain and poorer health and functioning than
the higher TEX group at all time points. In interviews, patients and clinicians reported HEAL and PROMIS
to be relevant to their treatment, and patients made suggestions for the ACPA Pain Log.
Conclusions: Several HEAL measures were correlated with later PROMIS Pain treatment outcomes.
Higher HEAL TEX and choosing CAM over conventional medicine were patient factors that positively
influenced outcomes. Patients and clinicians found HEAL and PROMIS measures as well as the ACPA Pain
Log to be potentially useful tools for enhancing communication in clinical settings.
Limitations: This study included only patients with chronic pain; however, HEAL and many PROMIS
measures apply to a broader range of patients and treatments.
C. Background
In both health care and research, there is a growing recognition that important contributors to
health and healing are the clinical context and patients’ own beliefs and attitudes.1,2 The 2011 Institute
of Medicine report Relieving Pain in America highlights the importance of the patient–provider bond,
stating that “the effectiveness of pain treatments depends greatly on the strength of the clinician‐
patient relationship.” The 2011‐2015 strategic plan of the National Institutes of Health (NIH) National
Center for Complementary and Alternative Medicine (NCCAM) notes that “better understanding of the
contributions of both specific and nonspecific effects influencing outcomes and the potential for insight
into exploitation of either or both to improve symptom management or general health and well‐being is
needed.” Nonspecific aspects of treatment include factors such as patients’ beliefs and expectations,
patients’ sense of connection or trust in the provider, and optimism and spirituality. These nonspecific,
or contextual, factors may interact with the direct effects of various types of treatments, such as
medication adjustment or physical therapy.
Historically, such complex and interactive factors have been unexamined or relegated to the
“black box” of placebo response.3,4 More recently, however, patient‐centered and contextual factors
have been the subject of investigation, particularly in studies of complementary and alternative
medicine (CAM). Factors that have been found to influence outcomes include patients’ beliefs or
expectations about treatment,5‐7 patients’ perceptions of the bond with a provider,8 negative affect,9,10
and spirituality.11‐13 For example, 2 studies of openly labeled placebos support the role of patient beliefs
and expectations. A study of more than 80 chronic low back pain patients assigned to treatment as usual
(TAU) or to openly labeled placebo pills that included a statement about mind–body influences found

5
statistically significant improvements in pain and pain‐ related disability in the placebo group compared
with TAU.14 A similarly designed study with irritable bowel syndrome patients showed that open‐label
placebo resulted in reduced symptom severity (p = .03) and adequate symptom relief (p = .03) compared
with an evaluation‐only control group.15 Furthermore, in a randomized, double‐blind placebo‐controlled
trial for gastroesophageal reflux disease, those randomly assigned to receive an expanded patient–
provider interaction (including questions about lifestyle and symptom details) were more likely to have
decreased gastroesophageal reflux disease (GERD) severity (p = .01) and were significantly more likely to
report a 50% or greater reduction in GERD symptoms than those who received the nonexpanded visit (p
= .01).16
Within‐patient (spirituality, outlook) and contextual factors (treatment expectations, patient–
provider connection) are often referred to as nonspecific factors, as they are not specific to a particular
treatment. Although nonspecific factors are known to be important in health outcomes, the issue
remains of how to measure these factors in a standardized and systematic way. Existing questionnaires
are often long, difficult for low literacy patients to understand, and disease‐ or treatment‐specific and
thus of little use in comparative effectiveness research or general medical settings. To address this gap,
our team developed a set of item banks to measure nonspecific factors in healing, the Healing
Encounters and Attitudes Lists (HEAL) (NCCAM R01 AT006453, The Healing Context in CAM: Instrument
Development and Initial Validation), using the rigorous methodology of the Patient‐reported Outcomes
Measurement Information System (PROMIS). PROMIS has developed and calibrated item banks
assessing a wide variety of domains17 and represents the most ambitious attempt to date to apply
models from item response theory to health‐related assessment.18,19 PROMIS tools confer 2 major
advantages: They are standardized to be comparable across diseases, treatments, and patients of
various ages and literacy levels, and they can be presented as computerized adaptive tests (CATs), in
which items are presented to test takers based on their responses to previously presented items. This
reduces the number of items (typically 3 to 6) needed to determine a patient’s score, thus minimizing
patient burden. The efficiency of the PROMIS and HEAL measures makes it feasible to generate a rich
health status profile and “snapshot” of the current treatment context at little cost.
We chose to evaluate the HEAL and PROMIS measures in the context of treatment for
chronic pain because pain is a widespread problem associated with considerable personal and
societal costs.2
Main Research Questions
Research Question 1: Do nonspecific factors, as assessed by our HEAL measures, predict

6
treatment outcomes?
We hypothesized that HEAL scores would predict significant variance in outcome on
measures such as global impression of improvement, pain intensity, and pain interference with
life activities.
Research Question 2: Do the HEAL and PROMIS health status measures contribute to an
improved understanding of the heterogeneity of patients and treatment effects?
Our person‐centered approach was to compare patients based on their preferences for
CAM versus conventional medicine. In addition, we wanted to evaluate the role of expectations
of patients about their treatment, comparing patients with lower and higher positive Treatment
Expectancy (TEX). We hypothesized that those with higher expectations of treatment would
have greater symptom reduction than those with lower expectations.
Research Question 3: Do patients and providers find the information provided by HEAL and
PROMIS measures to be clear, relevant, and useful in the treatment setting? Do patients find
the American Chronic Pain Association Pain (ACPA) Pain Log clear and helpful as a
communication tool in treatment?
To address these questions, we conducted cognitive interviews with patients and their
providers. We predicted that patients and clinicians would endorse the HEAL instruments, the
PROMIS health status instruments, and the ACPA Pain Log as useful tools to improve the quality
of care.
Significance
This project, Measuring the Context of Healing: Using PROMIS in Chronic Pain
Treatment, focuses on PROMIS health status measures of Pain Intensity and Interference,
Physical Function, Sleep, Depression, and Anxiety, and a set of new instruments developed
using PROMIS methods, HEAL. The HEAL measures include TEX, Patient‐Provider Connection
(PPC), Healthcare Environment perceptions (HCE), Positive Outlook (POS), Spirituality (SPT) and
Attitude Toward CAM (CAM). Regarding the patient‐centered questions that inspire PCOR, 2 are
most relevant to this study: “Given my personal characteristics, conditions, and preferences,
what should I expect will happen to me?” and “What can I do to improve the outcomes that are
most important to me?” The HEAL measures and other PROMIS health status instruments allow
us to document patient‐centered factors that may play a role in predicting outcomes of
treatment for chronic pain.20‐23 Our project also sought to inform the methodology gap

7
identified by PCORI: heterogeneity of treatment effects (HTE). In this project, we used HEAL
CATs and the selection of PROMIS health status CATs to better characterize individual
differences among patients and their views of clinicians and health care settings that contribute
to HTE. An equally important goal was to capture the patient voice in the development of
measures. In the development of the HEAL measures (NIH R01 AT006453), 6 patient focus
groups had helped identify important concepts in healing, and a diverse group of 48 community
members participated in cognitive interviews to determine clarity and content validity of items.
The qualitative review and cognitive interviewing led to enhanced ease of use, greater
simplicity and clarity, and decreased literacy demands. Because PROMIS and HEAL CATs are
relevant across medical conditions and treatments, including conventional medicine and
integrative medicine, we expect the current project to have broad impact on both research and
clinical treatment. When used clinically, HEAL instruments, in conjunction with other PROMIS
measures, are expected to enhance treatment relationships, provide information about
patients’ trajectories of healing, and promote understanding of HTE.
D. Patient and Stakeholder Engagement
Patient and clinician stakeholders were involved in this study from its inception. As we
were creating the study proposal, we interviewed patients about study questions and outcomes
that were important to them. This highlighted the significant outcomes of pain reduction and
improved function, and the importance of clinicians’ understanding of patients’ preferences
and everyday environment. We collaborated with patient advocacy organizations (American
Chronic Pain Association and Chronic Pain Research Consortium) and integrative and
conventional pain clinicians to shape the questions and methods.
Through these initial collaborations, we identified a set of stakeholders to serve on our
Patient/Stakeholder Advisory Panel (PSAP). Our PSAP included 2 patients, a patient advocacy
organization stakeholder, a pain research advocacy group organizer who is also a patient, and 4
clinician stakeholders. The PSAP met quarterly face to face as well as individually with
researchers or in subcommittees, as needed, to work on activities such as the following:
1. Formulating Research Questions and Study Design. PSAP members contributed to the
relevance of the study by expanding the list of pain conditions participants could endorse in

8
online assessments; adding questions regarding opioid pain medications, resulting in an
additional research exploration regarding satisfaction with opioids and the prescribing clinician;
and adding the Press‐Ganey Patient Satisfaction Questionnaire to our online assessment to
assess concurrent validity of our treatment‐related HEAL measures.
2. Participating in and Monitoring the Conduct of the Project. PSAP members monitored the
study at each of the quarterly meetings; one of the standing agenda items was updates on the
research progress. The PSAP also enhanced the rigor of the conduct of the project through
creative ideas for recruitment, providing recruitment assistance through placing flyers at new
locations and talking about the study at various community events, increasing the clarity of
instructions for the online assessments, and revising the layperson descriptions of HEAL and
PROMIS measures so that they could be easily understood in treatment settings by both
patients and clinicians.
3. Disseminating the Study’s Results/Facilitating Adoption of Research Evidence Into
Practice. Our PSAP was very active in creating dissemination plans and materials: We formed
subcommittees with unique skillsets to work on dissemination to such various groups as
patients/caregivers, researchers, clinicians, and health system leadership. For example, our
ACPA representative PSAP member helped create a PowerPoint presentation for patients was
shown at the Pain Day for consumers during the May 2017 American Pain Society annual
meeting. We had also been actively disseminating results at scientific meetings; one of our
clinician PSAP stakeholders won a prize for best poster from North America during the March
2017 research conference of the World Federation of Chiropractic and International Board of
Chiropractic Examiners. See Section M for a summary of presentations and adoption of the
HEAL measures by other researchers.
In addition to engaging with our PSAP, we engaged with patients and clinicians during
in‐depth cognitive interviews. We conducted cognitive interviews with 44 patients and 13
providers to determine their views on whether HEAL and PROMIS can help patients and
providers communicate and engage more fully in their treatment partnerships. We used
feedback from the patient interviews to modify the HEAL and PROMIS reports. We also asked
patients for feedback about the clarity and potential utility of the ACPA Pain Log items; their

9
suggestions will be shared with the ACPA.
E. Methods
The research questions include: 1) Do non‐specific factors, as assessed by our HEAL
measures, predict treatment outcomes? (2) Do the PROMIS health profile and HEAL measures
contribute to the understanding of HTE? and (3) Do patients and their providers find the HEAL
and PROMIS measures easy to understand and useful and relevant to their ongoing treatment?
Likewise, do patients consider the ACPA Pain Log to be clear and useful as a communication
tool in treatment?
Overview and Study Design. This PROMIS‐related project is a prospective cohort study.
Because our intention was to evaluate PROMIS and HEAL measures in clinical treatment for
chronic pain, we invited patients who were starting a new treatment to complete the HEAL and
PROMIS computerized assessments. Participants completed the online questionnaires at 3 time
points: baseline (within 1 month of starting treatment), 2 months after baseline, and 4 months
after baseline. For this study patients needed to have some experience with their provider and
some knowledge about the treatment so that they could rate these areas on HEAL TEX and PPC.
Therefore, the baseline was early in treatment rather than prior to treatment.
Participants received $30 for completing each of the 3 online assessments. Participants
in Pittsburgh were also invited to complete individual cognitive interviews, in which they “think
aloud” while reviewing HEAL, PROMIS, and ACPA Pain Log items, and rate items and summary
reports. Participants and their clinicians, many of whom also completed individual interviews,
received $40 for each interview. Enrollment began on July 10, 2015 and continued through
August 30, 2016. The final online assessments were completed by December 9, 2016.
Study Cohort. For recruitment, we used several methods for identifying potentially
eligible and interested individuals. We routinely spoke with practicing pain clinicians about the
study and supplied clinics with our flyers and information. In addition, clinicians at the Center
for Integrative Medicine in Pittsburgh introduced interested persons to our research staff
directly, in person. We regularly advertised electronically through university‐wide email
delivery systems (Read Green) and on electronic message boards in clinics. We utilized the
services of the University of Pittsburgh’s Clinical and Translational Science Institute’s (CTSI)

10
research registry. The CTSI research registry performed initial screening and provided contact
information for potentially eligible participants. In addition, our stakeholder panel members
helped by placing our recruitment flyers at their doctors’ offices, gyms, and other public
settings.
We enrolled patients who were seeking treatment in a variety of conventional medicine
settings (pain clinics, primary care settings, and rehabilitation services) or integrative/CAM
clinics. Institutional Review Board (IRB) approval was obtained from the University of
Pittsburgh. Our 2 external collaborating integrative medicine clinics—Venice Family Clinic at UCLA
and Allina Health System in Minneapolis—obtained IRB approval at their respective institutions.
We intentionally included a wide range of patients with many types of pain who
received diverse treatments, because (1) a broad range of patients and treatments is needed to
examine HTE, and (2) PROMIS and HEAL assessments are designed to apply broadly across
patients and treatments. Recruitment materials were distributed at each research site.
Interested patients who saw our advertisements or heard about the study at their health care
offices telephoned or emailed our study staff to learn about the study and undergo screening,
which required no more than 5 minutes of their time.
Inclusion and Exclusion Criteria. To be eligible to participate in the computerized
assessments, patients must have had pain of at least 3 months duration and had started a pain
treatment requiring at least monthly visits within the past month. They must have been 18
years of age or older and able to read and understand English as well as complete
questionnaires on a computer. Individuals were ineligible if they were currently diagnosed (self‐
reported) with a psychotic disorder (eg, schizophrenia, schizoaffective disorder) or a bipolar
disorder, or were unable to speak or read English.
Minimizing Attrition, and Reasons for Loss to Follow‐up. Informed consent
documentation as well as the main study questionnaires were completed online. Although
participants were welcome to complete the assessments at our research offices or at their pain
treatment sites, they could also complete them remotely. To minimize attrition, we tracked the
time when second and third assessments were due and contacted participants via email and
telephone, if necessary. In addition, the same research staff member contacted them across

11
the 3 time points of the study. We found that careful monitoring and friendly connection with
participants helped minimize attrition and loss to follow‐up.
Table 1. Assessment Measures
Baseline 2‐month Follow‐up
4‐month Follow‐up
HEAL Item Banks
Patient‐Provider Connection ■ ■ ■
Treatment Expectancy ■ ■ ■
Healthcare Environment ■ ■ ■
Positive Outlook ■ ■ ■
Attitude Toward Conventional/AlternativeMedicine
■ ■ ■
Spirituality ■ ■ ■
PROMIS Item Banks
Alcohol Usea ■ ■ ■
Anxiety ■ ■ ■
Average Pain Rating ■ ■ ■
Depression ■ ■ ■
Fatigue ■ ■ ■
Pain Intensity ■ ■ ■
Pain Interference ■ ■ ■
Physical Functioning ■ ■ ■
Sleep Disturbance ■ ■ ■
Clinical Characteristics
Height/weight (BMI; self‐report) ■
Charlson Comorbidity Index ■
Clinical Global Improvement ■ ■
Global Report of General Health ■ ■ ■
Press‐Ganey Survey (CAHPS v.5)a ■ ■ ■
Treatment/provider questions ■ ■ ■
Brief Opioid Prescription Historya ■ ■ ■
ACPA Pain Log (interview with patients) ■ ■
General Participant Information
Demographic questionnaire ■

12
Baseline 2‐month Follow‐up
4‐month Follow‐up
Stakeholder Interviews
Patient cognitive interview ■ ■
Clinician cognitive interview ■ ■
aAdded at the request of stakeholder advisory panel members.
Data Collection. The schedule for assessment measures is provided in Table 1. All HEAL
and PROMIS health status measures used in this project had been previously developed and
validated, and were not developed as part of this study.20,21,24‐27 The HEAL measures include the
following: PPC, which assesses patient views of the relationship with the provider; TEX, which
assesses patient expectations about whether the treatment will be helpful; HCE, which assesses
patient perceptions of the health care provider’s office and staff; POS, which assesses patient
level of confidence and optimism in general; CAM, which assesses patient views about
integrative medicine or CAM; and SPT, which assesses patient spiritual beliefs and experience of
spiritual support. The HEAL responses are scored on a 1‐to‐5 scale representing frequency
(“Never” to “Almost always”) or intensity (“Not at all” to “Very much”). Within each scale, raw
scores are summed and converted to T scores with mean of 50 and standard deviation of 10.
PROMIS health status measures in the assessments were Depression (DEP), Anxiety
(ANX), Fatigue (FAT), Sleep Disturbance (SLP), Alcohol Use, Physical Functioning (PHYS), Pain
Intensity (PINT), and Pain Interference (PI). The PROMIS measures listed previously are, like the
HEAL scales, scored on 1‐to‐5 scales of frequency or intensity, and raw scores are summed and
converted to T scores with mean of 50 and standard deviation of 10. In addition, we collected
PROMIS Average Pain Rating (AvePain), which is a single item rated from none (0) to very
severe (9‐10), and PROMIS Overall Health (Health), a single item rating from excellent (1) to
poor (5).
We administered the HEAL and PROMIS scales as CATs—except HEAL CAM, which is
available only as a 6‐item scale. CAT administration means that items are presented to the
patient based on his or her responses to previous items; this reduces the number of items that
a patient needs to answer.

13
Outcome Measures for Aims 1 and 2. The outcome measures for aim 1 were PROMIS
Pain Intensity and Pain Interference, and the single‐item rating of Clinical Global Improvement
(CGI),28 which asks the patient to report his or her current symptoms compared with when he
or she began treatment (eg, ranging from much worse to unchanged to much better). For aim
2, which evaluated heterogeneity of patient and treatment effects based on type of treatment
(CAM or conventional) and, in separate subgroup analyses, HEAL treatment expectations, the
outcome measures were PROMIS Pain Intensity, Pain Interference, Physical Function, overall
health, and Average Pain.
All measures used in this study were patient‐reported outcomes chosen because people
with chronic pain care about them. Thus, patients in treatment for chronic pain (along with
their clinicians) are the best source of information for reporting about their pain, pain
treatment, and the nonspecific factors assessed. We chose some of our measures, such as pain
intensity, pain interference with life activities,25 and physical function based on interviews with
patient stakeholders between February and April 2014.29 Our patient advocacy organization
stakeholder, ACPA, has a pain log communication tool that we also included in the subsample
of patients who participated in qualitative interviews, in order to document its clarity, ease of
use, and patient perceptions of its utility. The PROMIS and HEAL measures were developed and
tested using the rigorous instrument development procedures of the NIH PROMIS initiative,
with validation studies published and in preparation.23,26,30
Additional measures included in the study are noted in Table 1 (PROMIS Alcohol Use,
Press‐ Ganey Questionnaire, Opioid Prescription History). We included them based on specific
input from stakeholders following the initial PCORI project submission. Patients at the
conventional and integrative medicine sites completed the same online assessment protocol
(through Assessment Center, the platform used by PROMIS). Each participant was assigned a
study identification number. We used the identification number to link participants’ data across
the 3 online assessments (baseline, 2 months, and 4 months). We collected no medical record
data for this study.
Baseline Computerized Assessment. Eligible participants completed informed consent
procedures and were administered the CAT versions of HEAL measures, a selection of PROMIS

14
health status measures, and other demographic and clinical characteristics measures (see
Tables 2 and 3).

15
Table 2. Demographic Characteristics at Baseline, Overall, by Group, and by Low/High TEX
Total (N =
209)
CAM (n =
109)
nventional (n =
100)
P Valuea (CAM
Versus
Conventional)
Low TEX (n =
105)
High TEX (n =
104)
P Value
(Low
Versus
High)Categorical
Measure
Category
N (%)
n (%)
n (%)
n (%)
n (%)
Gender Male 52 (24.9) 27 (24.8) 25 (25.0) .96923 (21.9) 29 (27.9) .317
Female 157 (75.1) 82 (75.2) 75 (75.0) 82 78.1) 75 (72.1)
Race White 159 (76.1) 87 (79.8) 72 (72.0) .22875 (71.4) 84 (80.8) .201
Nonwhite 42 (20.1) 16 (14.7) 26 (26.0) 26 (24.8) 16 (15.4)
Multiracial 6 (2.9) 4 (3.7) 2 (2.0) 4 (3.8) 2 (1.9)
Missing 2 (0.96) 2 (1.8) 0 (0.0) 0 (0.0) 2 (1.9)
Hispanic/
Latino
Yes 14 (6.7) 11 (10.7) 3 (3.0) .0745 (4.8) 9 (8.7) .285
No 195 (93.3) 98 (89.9) 97 (97.0) 100 (95.2) 95 (91.3)
Education Less than 4‐year degree 101 (48.3) 54 (49.5) 47 (47.0) .76552 (49.5) 49 (47.1) .781
Greater than or equal to
4‐year degree
108 (51.7)
55 (50.5)
53 (53.0)
53 (50.5)
55 (52.9)
Age Mean + SD 47.5 ± 14.9 45.6 ± 14.5 49.5 ± 15.0 .05447.0 ± 15.0 47.9 ± 14.5 .645
aChi‐square test was used for categorical measures, independent samples t test for age.

16
Table 3. Clinical Characteristics at Baseline, Overall, by Group, and by Low/High TEX
Total (N =
209)
CAM (n =
109)
nventional (n =
100)
P Valuea
(CAM Versus
Conventional)
Low TEX (n
= 105)
High TEX (n =
104)
P Value
Low Versus
High)
Categorical
Measure Category
N (%)
n (%)
n (%)
n (%)
n (%)
Opioid use Only 1 55 (26.3) 21 (19.3) 34 (34.0) .001
40 (38.1) 15 (14.4) < .001
2 or more 12 (5.7) 2 (1.8) 10 (10.0) 7 (6.7) 5 (4.8)
Missing 2 (1.0) 0 (0.0) 2 (2.0) 1 (1.0) 0 (0.0)
Do not use 140 (67.0) 86 (78.9) 54 (54.0) 57 (54.3) 84 (80.8)
Satisfaction with
opioids taken
Not at all 6 (2.9) 2 (1.8) 4 (4.0) .4254 (3.8) 2 (1.9) .755
A little bit 12 (5.7) 6 (5.5) 6 (6.0) 10 (9.5) 2 (1.9)
Somewhat 30 (14.4) 11 (10.1) 19 (19.0) 21 (20.0) 9 (8.7)
Quite a bit 15 (7.2) 4 (3.7) 11 (11.0) 10 (9.5) 5 (4.8)
Very much 4 (1.9) 0 (0.0) 4 (4.0) 2 (1.9) 2 (1.9)
Missing 2 (1.0) 0 (0.0) 2 (2.0) 1 (1.0) 0 (0.0)
Not asked 140 (67.0) 86 (78.9) 54 (54.0) 57 (54.3) 84 (80.8)
CCI: 2+ health
conditions
Yes 50 (23.9) 25 (22.9) 25 (25.0) .72726 (24.8) 24 (23.1) .775
No 159 (76.1) 84 (77.1) 75 (75.0) 79 (75.2) 80 (76.9)
Abbreviation: CCI, Charlson Comorbidity Index. aChi‐square tests were used.

17
Table 3. Clinical Characteristics at Baseline, Overall, by Group, and by Low/High TEX (Cont’d)
Total (N =
209)
CAM (n =
109)
nventional (n
= 100)
P Valuea (CAM
Versus
Conventional)
Low TEX (n = 105)High TEX (n =
104)
P Value (Low
Versus High)
Categorical
Measure Category
N (%)
n (%)
n (%)
n (%)
n (%)
Pain on average Mild (1‐3) 21 (10.0) 16 (14.7) 5 (5.0) .0346 (5.7) 15 (14.4) .143
Moderate (4‐6) 92 (44.0) 49 (45.0) 43 (43.0) 45 (42.9) 47 (45.2)
Severe (7‐8) 85 (40.7) 41 (37.6) 44 (44.0) 48 (45.7) 37 (35.6)
Very severe (9‐10) 9 (4.3) 2 (1.8) 7 (7.0) 5 (47.6) 4 (3.8)
Missing 2 (1.0) 1 (0.9) 1 (1.0) 1 (1.0) 1 (1.0)
Overall health Excellent 9 (4.3) 5 (4.6) 4 (4.0) .4372 (1.9) 7 (6.7) .321
Very good 50 (23.9) 28 (25.7) 22 (22.0) 22 (21.0) 28 (26.9)
Good 73 (34.9) 41 (37.6) 32 (32.0) 38 (36.2) 35 (33.7)
Fair 56 (26.8) 23 (21.1) 33 (33.0) 31 (29.5) 25 (24.0)
Poor 21 (10.0) 12 (11.0) 9 (9.0) 12 (11.4) 9 (8.7)
aChi‐square tests were used.

18
Follow‐up Computerized Assessments (2 Months and 4 Months). Patients were eligible
for follow‐up assessments if they participated in treatment visits at least once after their
baseline assessment. The reason for this requirement is that we wanted to be sure that they
were actually in a treatment for their pain. We considered patients lost to follow‐up if they did
not complete any follow‐up evaluations. Patients who did not complete the first follow‐up (2
months) were still invited to complete the final (4 month) follow‐up.
Patient Baseline Cognitive Interview. We conducted “think aloud,” or cognitive,
interviews with a subset of patients to assess their understanding of the HEAL, PROMIS, and
ACPA Pain Log questions and to determine whether they found the questions to be clear,
relevant, and potentially useful for enhancing communication and understanding in clinical
encounters. We set the maximum number of cognitive interviews at 25% of the overall sample
(50 out of 200) based on guidelines that suggest that qualitative interviews should cease when
no new information is uncovered (saturation)31 and the report that saturation may take place
after approximately 20% of a sample has been interviewed.32 Participants in the assessment
study were invited to participate in the cognitive interviews immediately after they completed
their baseline assessment. We interviewed Pittsburgh participants and not participants from
external integrative medicine sites (Los Angeles and Minneapolis) for feasibility reasons. As a
part of the interview, both patients and clinicians rated the HEAL and PROMIS item banks on
their understanding of the concepts, relevance of the concepts for their treatment, and
usefulness of the information on a 0‐to‐4 ordinal scale (“Not at all,” “A little bit,” “Somewhat,”
“Quite a bit,” “Very much”; see Appendix A for the cognitive interview guide and survey
questions). Patients also completed the ACPA Pain Log and provided feedback on its content (at
initial interview only). Patients were provided with graphic representations of their HEAL and
selected PROMIS health status scores and were asked to provide feedback and suggestions to
the research team.
Patient Follow‐up Cognitive Interview. We conducted follow‐up interviews to assess
patient perspectives on the personal and clinical utility of reviewing changes over time on the
HEAL and PROMIS scales. The follow‐up cognitive interview mirrored the baseline interview,
including the same types of questions. Interviewees were encouraged to ask questions and

19
engage in critical dialogue about the uses and implications of this type of assessment in clinical
care settings. If the treatment was short term (eg, as with physical therapy, chiropractic
treatment, or acupuncture), we conducted the second interview at the 2‐month follow‐up
rather than at 4 months.
Clinician Baseline Cognitive Interview. We approached all clinicians of the Pittsburgh
patients who completed cognitive interviews to participate in clinician interviews. We enrolled
several types of health care providers, including physicians, acupuncturists, massage therapists,
and physical therapists. The clinicians were given their patients’ summary scores from the
online assessments and were encouraged to engage in a candid conversation about the
directions that computer assessment might take in the treatment environment and what
information is most beneficial for their purposes.
Clinician Follow‐up Cognitive Interview. At follow‐up interviews, the same clinicians
were provided with longitudinal HEAL and PROMIS summary scores, which were briefly
explained to them. The clinicians were asked to reflect on how the scores could potentially
influence the clinical encounter over time. The topics mirrored those in the baseline interview,
with additional attention paid to the potential value of having longitudinal health status
measures available.
Data Analysis Plan
Aim 1 utilized correlation and multiple linear regression (ordinary least squares
estimation) to test the proposed hypotheses. We predicted that correlations (Spearman’s rank
correlation) between HEAL scores and patients’ reports of CGI at 2‐month and 4‐month follow‐
ups would be moderate or larger (0.50 or greater). These 2 predictions regarding HEAL and CGI
at 2‐month and 4‐month follow‐ups represent hypotheses 1a and 1b, respectively. Similarly, for
hypotheses 1c and 1d (regarding HEAL and Pain outcomes), we predicted that correlations
(Pearson) between HEAL scores and PROMIS Pain Interference and Pain Intensity at 2‐month
and 4‐month follow‐ups would be moderate to large (.50 or greater). Regarding our hypotheses
about regressions, with pain as outcomes and HEAL as predictors, we expected that HEAL
scores would account for significant amounts of variance in PROMIS Pain Intensity and Pain
Interference outcomes in preliminary, unadjusted models and also in final regression models

20
that were adjusted for a baseline level of pain.
Aim 2: Heterogeneity of Treatment Effects. We specifically designed our study to
address whether subgroups of patients experience different treatment effects. The main goals
of aim 2 were to assess (1) the effect on treatment outcome of patients’ choice to engage in
CAM or conventional medicine, and, separately, (2) whether patients with higher and lower
HEAL TEX at baseline had different pain treatment outcomes. For aim 2, we used stepwise
multiple linear regression for each pain treatment outcome (ordinary least squares estimation),
then used mixed models (ie, multivariate mixed effect linear regression models) to examine the
cohort difference longitudinally. All predictors were fixed effects, and intercepts were random
effects. For regression analyses, we examined whether HEAL scores were significant predictors
of outcome in each model, with and without controlling for baseline status. For mixed models,
we modeled HEAL scores at baseline, different cohorts (CAM versus conventional; high TEX
versus low TEX), time, and baseline status simultaneously. In the series of mixed models, we
examined (1) HEAL scores and time only; (2) HEAL scores, time, and time squared; and 3) HEAL
scores, time, and baseline status. The outcome variables used in the models—and presented in
Tables 8 and 9—are PROMIS Average Pain, PROMIS Overall Health, PROMIS Physical Function,
PROMIS Pain Interference, and PROMIS Pain Intensity. With the final models, we used
backward selection by adding the significant (at p < .15) HEAL score predictors back to the
model after controlling for the baseline status of the outcome variable, and time. We designed
these analyses to increase understanding of the contributions of PROMIS and HEAL in the
different cohorts: (1) CAM and conventional medicine, and (2) higher and lower TEX. We used
SPSS and STATA software for data analyses.
Aim 3 involved direct, in‐person feedback from patients and clinicians, and used
patient voices in research. For aim 3, we conducted individual cognitive interviews with
patients and clinicians regarding clinical utility of the HEAL measures, PROMIS health status
measures, and the ACPA Pain Log. At each of the 2 cognitive interviews (baseline and 4‐month
follow‐up), we elicited several structured, evaluative ratings of clarity, relevance to the
patients’ treatment experience, and potential usefulness in the clinical setting, using 0‐to‐4
ordinal scales (eg, “Never” to “Very much”). We expected that patients and clinicians would

21
rate the PROMIS and HEAL highly on clarity of language (ie, means of 3.0 or higher on a 0‐to‐4
scale). We expected that the patients would rate the relevance and usefulness of treatment‐
related HEAL items (eg, their views of the Patient‐Provider Connection, their perceptions of the
Healthcare Environment, and their Treatment Expectancy) significantly higher than HEAL items
that reflect personal characteristics (eg, Positive Outlook, Spirituality) that may or may not be
pertinent to clinical treatment. We compared mean scores on relevance of treatment‐related
versus within‐patient HEAL measures using paired t tests.
Our data analysis plan for the aim 3 evaluation of the ACPA Pain Log included counts of
comments regarding clarity and confusion related to the log’s items, pictograms, response
scales, and relevance to chronic pain. Thus, we obtained descriptive data during the cognitive
interviews with patients with the intent to compile these data into charts with positive and
negative comments and specific suggestions.
Study Protocol. We implemented the study protocol outlined above as originally
contracted, based on our original proposal and the data analytic requests made by PCORI
scientific staff prior to the contract award. The protocol was approved by the University of
Pittsburgh IRB and the IRBs of our contracted external integrative medicine sites: Venice Clinic
in Los Angeles and Allina Health System in Minneapolis.
F. Results
To briefly reiterate our aims, this project assessed (1) whether nonspecific factors
assessed by HEAL measures predict pain treatment outcomes, (2) whether HEAL and PROMIS
measures contribute to understanding of HTE, and (3) whether patients and their providers find
HEAL and PROMIS measures, and the ACPA Pain Log, easy to understand and useful in their
ongoing treatment.
The first 2 aims were addressed through our main study, which included 209 persons
with chronic pain who were initiating a new treatment; the third question was addressed
through interviews with a subset of patients and their health care providers.
Descriptive Information About the Study Participants
Descriptions of study flow, participants, and assessments can be found in Tables 1‐3 and
Figure 1. The participants included 209 patients with chronic pain who had started a new

22
complementary/alternative treatment (n = 109) or conventional medicine treatment (n = 100)
during the previous month (Figure 1).

Figure 1. Participant Flow Diagram
Telephone Screening for eligibility (n=436)
Screened as ineligible (n=175)
• No new treatment for pain (n=99)• Mild pain/not chronic (n=18)• Excluded condition (n=20)• No frequent treatment/not continuing
treatment (n=30)• Not interested (n=8)
Not eligible for 2-mo follow up (n=4)
Completed 2-mo follow up (n=95) Missed 2-mo follow up (n=10)
Not eligible for 2-mo follow up (n=2)
Completed 2-mo follow up (n=97) Missed 2-mo follow up (n=1)
Complementary/Alternative (n=132)
Did not start treatment w/in window (n=19)
Consented ineligible/withdrew (n=4)
Eligible Baseline completed (n=109)
Conventional (n=128)
Did not start treatment w/in window (n=23)
Consented ineligible/withdrew (n=5)
Eligible Baseline completed (n=100)
Eligible Screens (n=260)
4-mo follow up complete (n=100)
Completed 2-mo follow up missed 4-mo follow up (n=2)
Lost to all follow up (n=3)
4-mo follow up complete (n=96)
Completed 2-mo follow up missed 4-mo follow up (n=2)
Lost to all follow up (n=0)
• Withdrew (n=2)• Ineligible – no
treatment (n=2)
• Withdrew (n=1)• Ineligible – no
treatment (n=3)• Ineligible
condition (n=1)
Baseline
4-mo Follow Up
2-mo Follow Up
23

24
In terms of study flow, eligibility issues, study enrollment, and loss to follow‐up, 42
eligible persons did not enroll or complete assessments. These 42 individuals were screened
eligible and expressed interest in participating and were then emailed the link to enroll;
however, they failed to complete enrollment after several contact attempts, apparently
because they were no longer interested in participating. In addition, 3 participants completed
the online consent and then withdrew without completing the questionnaires due to confusion
about the technology or loss of interest. Five participants consented and then were deemed
ineligible because they did not start treatment. One individual consented and completed the
questionnaire but was later found to be ineligible due to an excluded psychiatric condition. See
Figure 1 for details of eligibility, enrollment, and retention.
Regarding demographics, the participants’ average age was 47.5 years (SD = 15), 75%
were female, 23% were nonwhite or multiracial, and 7% were of Hispanic ethnicity; further
demographic and clinical characteristics can be found in Tables 2 and 3. CAM and conventional
medicine participants did not differ on demographic characteristics (Table 2). Regarding clinical
characteristics at baseline, CAM patients’ PROMIS Average Pain was less than that of
conventional medicine participants (p = .034).
Of our participants, 24% reported having 2 or more other medical comorbidities in
addition to their chronic pain (Table 3). We also explored subgroups of patients who were using
opioid medications and who were not (140 out of 209), as well as their satisfaction with these
prescriptions. Only 23 out of 109 CAM patients used opioids, whereas 44 of 100 conventional
medicine patients did (p = .001). Those in the high TEX group were less likely than low TEX
participants to be taking opioid medications (20 out of 104 versus 47 of 105; p < .001).

25
Table 4. Current Pain Treatment, Provider, and Pain Type, Self‐reported at Baseline
Total (N = 209) CAM (n = 109) nventional (n =
100)
Category N (%) n (%) n (%)
Treatment type Medication 41 (19.6) 5 (4.6) 36 (36.0)
Injection 15 (7.2) 3 (2.8) 12 (12.0)
Physical therapy 56 (26.8) 8 (7.3) 48 (48.0)
Chiropractic 29 (13.9) 27 (24.8) 2 (2.0)
Acupuncture 37 (17.7) 37 (33.9) 0
Massage/other body work 15 (7.2) 15 (13.8) 0
Meditation 6 (2.9) 6 (5.5) 0
Psychotherapy/counseling 1 (0.5) 1 (0.9) 0
Biofeedback/relaxation 2 (1.0) 2 (1.8) 0
Hypnosis/guided imagery 1 (0.5) 1 (0.9) 0
Occupational therapy 4 (1.9) 2 (1.8) 2 (2.0)
Nutritional counseling 2 (1.0) 2 (1.8) 0
Provider type Primary care doctor 33 (15.8) 18 (16.5) 15 (15.0)
Specialist doctor 50 (23.9) 9 (8.3) 41 (41.0)
Physical therapist 40 (19.1) 2 (1.8) 38 (38.0)
Chiropractor 33 (15.8) 31 (28.4) 2 (2.0)
Acupuncturist 23 (11.0) 23 (21.0) 0
Massage therapist/body worker 14 (6.7) 14 (12.8) 0
Psychotherapist/counselor 3 (1.4) 1 (0.9) 2 (2.0)
Biofeedback therapist 2 (1.0) 2 (1.8) 0
Nurse 1 (0.5) 1 (0.9) 0
Meditation teacher 5 (2.4) 5 (4.6) 0
Occupational therapist 2 (1.0) 1 (0.9) 1 (1.0)
Other health care provider 3 (1.4) 2 (1.8) 1 (1.0)

26
Table 4. Current Pain Treatment, Provider, and Pain Type, Self‐reported at Baseline (Cont’d)
Total (N = 209) CAM (n = 109) nventional (n =
100)
Category N (%) n (%) n (%)
Pain type Back pain 96 (45.9) 49(45.0) 47 (47.0)
Neck pain 16 (7.7) 9 (8.3) 7 (7.0)
Headaches/migraines 6 (2.9) 5 (4.6) 1 (1.0)
Arthritis or joint pain 25 (12.0) 10 (9.2) 15 (15.0)
Muscle pain 6 (2.9) 5 (4.6) 1 (1.0)
Nerve pain/neuropathy 14 (6.7) 7 (6.4) 7 (7.0)
Fibromyalgia 12 (5.7) 7 (6.4) 5 (5.0)
Cancer pain 3 (1.4) 1 (0.9) 2 (2.0)
Stomach or gastrointestinal pain 4 (1.9) 3 (2.8) 1 (1.0)
Pelvic/bladder pain 4 (1.9) 3 (2.8) 1 (1.0)
Other pain problems 23 (11.0) 10 (9.2) 13 (13.0)
Table 4 shows the variety of CAM and conventional treatments that participants
received. The most common pain condition was back pain, reported by 46% (96 out of 209) of
participants. The most frequently used CAM treatments were acupuncture (17.7%; 37 out of
209), chiropractic (13.9%; 29 out of 209), and massage/other body work (7.2%; 15 out of 209),
and the most frequently used conventional medicine treatments were physical therapy (26.8%;
56 out of 209), medication (19.6%; 41 out of 209), and injection (7.2%; 15 out of 209). In
addition to inquiring about current treatment, we asked participants to indicate number of
prior treatments they had received for their chronic pain, and the vast majority—92% (192 out
of 209)—had received 2 or more types of treatments previously for their pain.
We found that the participants had improvement in PROMIS Pain Intensity and PROMIS
Pain Interference from baseline to the 2‐month assessment and from baseline to the 4‐month
assessment (all p’s < 0.001). On the CGI, 63% of participants reported improvement

27
(“Somewhat better” or “Much better”) at both follow‐up assessments (see Table 5). Thus,
across multiple pain conditions and many types of conventional medicine and integrative
medicine treatments, the participants as a group showed improvement.
Results of Analyses for Aim 1: Are baseline scores on HEAL measures predictive of outcomes?
Our aim 1 research question addressed the issue of whether the HEAL nonspecific
factors scores at baseline were associated with later improvement in (1) CGI, (2) PROMIS Pain
Intensity, and (3) PROMIS Pain Interference with life activities.
1. HEAL and Clinical Global Impression. All HEAL baseline scores were significantly and
positively associated with CGI—except for HEAL Spirituality, which was not significantly
associated with CGI. However, the HEAL baseline scores were not as strongly associated with CGI
as we had hypothesized: The largest rho with CGI at 2 months was baseline HEAL PPC
(Spearman rho = 0.257, 2‐tailed p < 0.01), and the largest rho with 4‐month CGI was baseline
HEAL POS (Spearman rho = 0.252, 2‐tailed p < 0.01; see Table 6).

28
Table 5. HEAL, PROMIS, and CGI at Baseline, 2‐month, and 4‐month Assessments
Baseline 2‐month FU 4‐month FU
± SD ± SD ± SD
HEAL: Health Care Environment 50.7 ± 8.3 50.7 ± 8.2 50.5 ± 8.7
HEAL: Attitude Toward CAM 52.6 ± 9.4 52.9 ± 9.9 53.6 ± 10.3
HEAL: Positive Outlook 50.4 ± 10.4 50.6 ± 10.5 50.8 ± 11.0
HEAL: Patient‐Provider Connection 57.1 ± 7.9 58.1 ± 8.5 57.0 ± 9.7
HEAL: Spirituality 51.9 ± 12.0 51.1 ± 11.5 51.5 ± 11.9
HEAL: Treatment Expectations 51.4 ± 7.5 50.4 ± 9.7 51.0 ± 10.3
PROMIS: Anxiety 56.4 ± 9.1 56.1 ± 10.0 56.6 ± 10.7
PROMIS: Depression 54.8 ± 9.0 54.1 ± 9.7 54.1 ± 10.1
PROMIS: Fatigue 57.5 ± 9.1 57.4 ± 9.5 56.9 ± 10.1
PROMIS: Physical Function 39.7 ± 7.0 40.6 ± 8.4 41.3 ± 8.9
PROMIS: Pain Interference 63.5 ± 6.6 61.2 ± 7.6 61.2 ± 9.0
PROMIS: Pain Intensity 54.1 ± 5.9 51.5 ± 6.5 50.8 ± 7.5
PROMIS: Sleep 55.9 ± 8.7 55.3 ± 9.5 55.3 ± 9.7

29
Table 5. HEAL, PROMIS, and CGI at Baseline, 2‐month, and 4‐month Assessments (Cont’d)
aseline N (%) ‐month FU N (%)‐month FU N
(%)
PROMIS Average Pain None (0)
0 (0.0)
1 (0.5)
4 (1.9)
Mild (1‐3) 21 (10.0) 48 (23.0) 54 (25.8)
Moderate (4‐6) 92 (44.0) 79 (37.8) 70 (33.5)
Severe (7‐8) 85 (40.7) 56 (26.8) 57 (27.3)
Very severe (9‐10) 9 (4.3) 8 (3.8) 12 (5.7)
Missing 2 (1.0) 17 (8.1) 12 (5.7)
PROMIS Overall Health Excellent
9 (4.3)
8 (3.8)
9 (4.3)
Very good 50 (23.9) 48 (23.0) 50 (23.9)
Good 73 (34.9) 77 (36.8) 67 (32.1)
Fair 56 (26.8) 44 (21.0) 56 (26.8)
Poor 21 (10.0) 15 (7.2) 14 (6.7)
Missing 0 (0.0) 17 (8.1) 13 (6.2)
Clinical Global
Impression
Much better
25 (12.0)
32 (15.3)
Somewhat better 96 (45.9) 92 (44.0)
No change 43 (20.6) 35 (16.7)
Somewhat worse 14 (6.7) 24 (11.5)
Much worse 3 (1.4) 0 (0.0)
Missing 28 (13.4) 26 (12.4)

30
Table 6. Correlations Between HEAL Measures at Baseline, and CGI at 2 Months and 4 Months
CGI at 2 Months
CGI at 4 Months
Health Care Environment 0.232a 0.160b
Attitude Toward CAM 0.224a 0.245a
Positive Outlook 0.226a 0.252a
Patient‐Provider Connection 0.257a 0.202a
Spirituality –0.031 –0.051
Treatment Expectations 0.182b 0.227a
aSignificant at 0.01 level (2‐tailed). bSignificant at 0.05 level (2‐tailed).
Table 7. Significant Correlations Between HEAL Measures at Baseline and PROMIS Pain Interference and Pain Intensity at 2 Months and 4 Months
Pain Interference 2
Months
Pain Intensity 2 Months
Pain Interference 4
Months
Pain Intensity 4 Months
Health Care Environment NS NS NS NS
Attitude Toward CAM –0.144a NS –0.202a –0.151a
Positive Outlook –0.311a –0.181b –0.263a –0.246a
Patient‐Provider Connection NS NS NS NS
Spirituality 0.155b NS NS NS
Treatment Expectations –0.230a NS –0.232a –0.191a
aSignificant at 0.01 level (2‐tailed). bSignificant at 0.05 level (2‐tailed).
2. HEAL and PROMIS Pain Intensity and Interference. We found that several of the baseline
HEAL scores were significantly associated with PROMIS Pain Interference at 2‐months and 4‐

31
months follow‐up (see Table 7 for details): HEAL TEX, HEAL POS, and HEAL CAM. HEAL SPT was
associated with 2‐month ratings of Pain Interference but not with 4‐month ratings. Baseline
HEAL POS was associated with 2‐month and 4‐month PROMIS Pain Intensity. Baseline HEAL
Attitude toward CAM and Baseline HEAL TEX were associated with 4‐month PROMIS Pain
Intensity but not 2‐month Pain Intensity. Although the associations were statistically significant,
ranging from –0.16 to –0.31, they were not of the magnitude that we had hypothesized (0.50 or
greater). Thus, several of the HEAL measures were predictive of 2‐month and 4‐month pain
outcomes—but modestly so.
In the multiple regression analyses, one goal was to evaluate whether HEAL scores
predicted pain outcomes in the entire group of 209 patients. As a preliminary step to the final
models, we evaluated whether HEAL measures at baseline predicted pain outcomes at 2
months and 4 months, without adjusting for baseline levels of pain. In these unadjusted
models, we found that HEAL POS and HEAL SPT accounted for 17.7% of the variance in PROMIS
Pain Interference at 2 months, and 7.6% of the variance in PROMIS Pain Intensity at 2 months.
Together, HEAL POS, HEAL SPT, and HEAL Attitudes Toward CAM accounted for 15.8% of the
variance in PROMIS Pain Interference at 4 months, and HEAL POS and HEAL SPT accounted for
8.2% of the variance in PROMIS Pain Intensity at 4 months.
We adjusted the final regression models for baseline level of pain outcomes. This is
important because the severity of pain at the first assessment is a confounder in the association
of HEAL measures with pain outcomes. We adjusted the regression models by first entering the
baseline value of the outcome (eg, PROMIS Pain Intensity). Thus, these analyses provide
information about variance accounted for by HEAL over and above the influence of baseline
level of pain symptoms on follow‐up pain symptoms. Baseline PROMIS Pain Interference, HEAL
SPT, and HEAL POS accounted for 46.7% of the variance in 2‐month PROMIS Pain Interference,
but most of this was due to baseline status: HEAL SPT contributed an additional 1.8% of
variance beyond that accounted for by baseline Pain Interference. HEAL POS added an
additional 3.7% of variance beyond the effects of baseline Pain Interference and HEAL SPT.
When baseline Pain Intensity was added to the regression model predicting 2‐month PROMIS
Pain Intensity, we found that baseline Pain Intensity and HEAL TEX accounted for 47.5 % of the

32
PROMIS Pain Intensity outcome at 2 months, with just 1.2% of this due to the addition of
baseline HEAL TEX. The regression model predicting 4‐month PROMIS Pain Interference
adjusted for baseline Pain Interference resulted in a total of 46.2 % of the PROMIS Pain
Interference variance predicted by baseline Pain Interference (40.9%), Attitudes Toward CAM
(additional 2.1% of variance), HEAL SPT (additional 1.7% of variance), and HEAL POS (additional
1.5% of variance accounted for). The model predicting 4‐month PROMIS Pain Intensity with
baseline PROMIS Pain Intensity and HEAL scores as predictors resulted in a total of 41.2% of
variance accounted for: Baseline PROMIS Pain Intensity accounted for 39.2 % of the variance,
and an additional 2% of variance was accounted for by including HEAL TEX in the model.
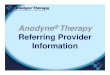
Figure 2. Observed Means of Outcome Measures by CAM and Conventional
Results of Analyses for Aim 2: Heterogeneity of Treatment Effects
For aim 2, we were interested in whether HEAL and PROMIS measures contribute to
Observed Mean
Abbreviations: AvePain, PROMIS Average Pain; Health, PROMIS Global Report of General Health (high
scores = worse health); PHYS, PROMIS Physical Function (higher scores = better function); PI, PROMIS
Pain Interference; PINT: PROMIS Pain Intensity.

33
understanding of HTE. The goal was to determine HTE based on the type of treatment patients
had chosen (subgroup analyses of patients receiving CAM/integrative medicine or conventional
medicine). An additional goal was to determine heterogeneity of pain treatment outcomes
based on the patients’ baseline HEAL TEX scores (subgroup analyses of patients with higher
versus lower TEX). In other words, the aim was to determine the effects on outcome of (1)
choosing a CAM or a conventional treatment, and, in a separate subgroup analysis, determine
effects of (2) initial treatment expectations (HEAL TEX). We conducted longitudinal analysis
using mixed models to capture HTE based on type of treatment and HEAL TEX scores at
baseline. For the CAM and the conventional medicine treatments, we plotted observed mean
scores at baseline, 2‐months follow‐up, and 4‐months follow‐up for each of the 5 outcome
variables: Average Pain, Overall Health (higher values = poorer health), PROMIS Physical
Functioning, PROMIS Pain Interference with life activities (PI), and PROMIS Pain Intensity (PINT).
The conventional group had a higher Average Pain score, poorer Overall Health, poorer Physical
Functioning, higher PI, and higher PINT than did the CAM group at each time point (see Figure
2). We used a series of mixed models to further examine these differences. We fitted the final
most parsimonious model using backward selection on HEAL scores after controlling for
baseline status. For Average Pain, the overall average across all time points for the CAM group
was 0.2444 (ie, the intercept, p < .001). The Average Pain in the conventional group was 0.215
(p = .062), which was higher than that of the CAM group after controlling for time, baseline
status, and baseline HEAL scores. A 1‐unit change in time made a 0.462 (p < .001) decrease in
Average Pain after controlling for other predictors in the model.

34
Table 8. Multivariable Regression Final Models With Pain and Health Status Variables as Outcomes, and Treatment Type, Time, Baseline HEAL
Scores, and Baseline Status as Predictors
Average Pain Health PHYS PI PINT
Treatment NS0.114 [0.038, 0.191] –0.979 [–1.695, –0.263] 1.011 [0.205, 1.817] 1.541 [0.788, 2.295]
Time –0.462 [–0.595, –0.329] NS0.847 [0.433, 1.261] –1.185 [–1.663, –0.707] –1.714 [–2.126, –1.301]
Baseline status 0.837 [0.772, 0.902] 0.815 [0.775, 0.854] 0.898 [0.843, 0.953] 0.781 [0.718, 0.844] 0.825 [0.766, 0.885]
HCE – – – NS –
PCAM – – – –0.058 [0.015, 0.101]
POS NS–0.010 [–0.014, –0.006] 0.064 [0.025, 0.102] –0.107 [–0.151, –0.063] –0.041 [–0.077, –0.006]
PPC – – – – –
SPT 0.013 [0.003, 0.023] ––0.058 [–0.090, –0.027] 0.091 [0.054, 0.127] –
TEX –0.035 [–0.048, –0.022] –0.073 [0.032, 0.115] –0.121 [–0.170, –0.072] –0.089 [–0.134, –0.045]
Intercept 2.444 [1.536, 3.351] 1.022 [0.748, 1.297] NS17.929 [12.441, 23.417] 11.978 [7.635, 16.321]
Notes: Treatment refers to CAM group (served as control) versus conventional group. NS stands for not significant at 0.05 level. – stands for not applicable: The variable was not entered in the model due to p > 0.15. For each cell, the estimated coefficient beta is followed by its corresponding 95% confidence interval. Baseline status = baseline value on the outcome variable. This was included in the prediction models.
Abbreviations: Average Pain, PROMIS Average Pain; CAM, HEAL Attitude Toward Conventional/Alternative Medicine; HCE, HEAL Health Care Environment; Health, PROMIS Overall Health; PHYS, PROMIS Physical Function; PI, PROMIS Pain Interference; PINT, PROMIS Pain Intensity; POS, HEAL Positive Outlook; PPC, HEAL Patient‐Provider Connection; SPT, HEAL Spirituality; TEX, HEAL Treatment Expectancy.

35
Also, a 1‐unit change in baseline status on Average Pain made a 0.837 (p < .001) increase
in Average Pain after controlling for other predictors in the model. Similarly, a 1‐unit change in
HEAL SPT scores at baseline made a 0.013 (p = .009) increase in Average Pain after controlling
for other predictors, and a 1‐unit change in HEAL TEX scores at baseline made a 0.035 decrease
in Average Pain after controlling for other predictors. These baseline variables, HEAL SPT and
HEAL TEX, were statistically significant predictors of Average Pain in the final model. See Table 8
for estimates for each of the 5 outcomes.
To examine the impact of Treatment Expectancy, we divided the sample into 2 groups
using a median split (low: < 51.5 versus high: 51.5+) of the HEAL TEX scores at baseline.
Observed mean score plots showed that the low HEAL TEX group had higher Average Pain,
Poorer Overall Health, poorer Physical Functioning, higher Pain Intensity, and higher Pain
Interference than did the high HEAL TEX (see Figure 3). The same series of mixed models was
fitted to each of the 5 outcomes for Treatment Expectancy as that used for type of treatment
(CAM versus conventional). The final most parsimonious model using backward selection on
HEAL scores, after controlling for baseline status, showed that the overall average across all
time points for the low TEX group was 2.590 (ie, the intercept, p < .001). The Average Pain in
the high TEX group was 0.237 (p = .053) lower than the low TEX group after controlling for time,
baseline status, and baseline HEAL scores. A 1‐unit change in time made a 0.448 decrease in
Average Pain after controlling for other predictors in the model; also, a 1‐unit change in
baseline status made a 0.851 increase in Average Pain after controlling for other predictors in
the model. Similarly, a 1‐unit change in HEAL SPT scores at baseline made a 0.016 increase in
Average Pain after controlling for other predictors. A 1‐unit change in HEAL PCAM scores at
baseline, HEAL POS scores at baseline, and HEAL PPC scores at baseline made a 0.016 decrease,
0.013 decrease, and 0.018 decrease, respectively, after controlling for other predictors in the
model. See Table 9 for estimates for each of the 5 outcomes.

36
Figure 3. Observed Means of Outcome Measures by Treatment Expectancy
Observed Mean by Low TEX vs. High TEX
Av ePain
PHYS
PI
Abbreviations: AvePain, PROMIS Average Pain; Health, PROMIS Global Report ofGeneral Health
(high scores = worse health); PHYS, PROMIS Physical Function (higher scores =
better function); PI, PROMIS Pain Interference; PINT, PROMIS Pain Intensity;
TEX, Treatment Expectancy.

37
Table 9. Multivariable Regression Final Models With Pain and Health status Variables as Outcomes, and High Versus Low Treatment
Expectancy, Time, Baseline HEAL Scores, and Baseline Status as Predictors
Average Pain Health PHYS PI PINT
Expectancy NS NS NS NS–0.844 [–1.571, –0.116]
Time –0.448 [–0.582, –0.314] NS0.795 [0.376, 1.214] –1.113 [–1.600, –0.625] –1.646 [–2.064, –1.229]
Baseline status 0.851 [0.785, 0.917] 0.805 [0.763, 0.847] 0.916 [0.861, 0.970] 0.796 [0.731, 0.861] 0.825 [0.764, 0.887]
HCE – – – –PCAM –0.016 [–0.028, –0.004] NS0.050 [0.012, 0.088] –0.054 [–0.098, –0.009] –
POS –0.013 [–0.025, –0.001] –0.010 [–0.015, –0.006] 0.078 [0.041, 0.116] –0.126 [–0.169, –0.083] –0.054 [–0.091, –0.016]
PPC –0.018 [–0.032, –0.004] – – ––0.047 [–0.090, –0.004] SPT 0.016 [0.006, 0.027] NS–0.067 [–0.099, –0.035] 0.101 [0.064, 0.139] 0.037 [0.006, 0.069]
Intercept 2.590 [1.570, 3.610] 1.185 [0.867, 1.503] NS16.795 [11.584, 22.005] 13.025 [8.730, 17.319]
Expectancy refers to low Treatment Expectancy group (served as control) versus high Treatment Expectancy group. NS stands for not significant at 0.05 level. – stands for not applicable: The variable was not entered in the model due to p > 0.15. For each cell, the estimated coefficient beta is followed by its corresponding 95% confidence interval. Baseline status = baseline value on the outcome variable. This was included in the prediction models.
Abbreviations: AvePain, PROMIS Average Pain; CAM: HEAL Attitude Toward Conventional/Alternative Medicine; HCE, HEAL Health Care Environment; Health, PROMIS Overall Health; PHYS, PROMIS Physical Function; PI, PROMIS Pain Interference; PINT, PROMIS Pain Intensity; POS, HEAL Positive Outlook; PPC, HEAL Patient‐Provider Connection; SPT, HEAL Spirituality; TEX, HEAL Treatment Expectancy

38
After we completed the mixed model analysis, we calculated post hoc power using
Average pain. We observed a 0.7 Average Pain difference between CAM and conventional
groups and a 0.5 difference across time points. Based on 100 simulations of a group sample of
100 participants, we achieved a 78% power to detect the difference of 0.7 between CAM and
conventional groups and a 75% power to detect a difference of 0.5 across time points, with
alpha level of .05.
Results of Analysis of Aim 3
Aim 3 evaluated patients’ and providers’ views of the utility of HEAL, PROMIS health
status measures, and the ACPA Pain Log in the treatment context. We conducted individual
interviews with 44 of the aim 1 and aim 2 participants, and 13 of their CAM and conventional
medicine practitioners. Of these 44 interview participants, 23% were male, 34% were nonwhite
or multiracial, 5% were of Hispanic/Latino ethnicity, and 34% had less than a 4‐year college
education. During the interview, patients and clinicians were asked to rate the clarity,
relevance, and usefulness of each of the HEAL and PROMIS measures on a scale of 0 (“Not at
all”) to 4 (“Very much”).

39
Figure 4. HEAL Short Form Itemsa
FACTOR 2: Health Care Environment
Item ID Item Stem
HCEn_2402 The staff was respectful.
HCEn_2403 The staff was friendly.
HCEn_2398 The staff was helpful.
HCEn_2446 My care was well organized.
HCEn_2448 The health care provider's office respected my privacy.
HCEn_2400 The waiting area was comfortable.
— —
FACTOR 3: Treatment Expectancy
Item ID Item Stem
TEC_6199 I am confident in this treatment.
TEC_6132 This treatment will be successful.
TEC_6082 I feel good about this treatment.
TEC_6221 I expect good outcomes from this treatment.
TEC_6160 This treatment is right for me.
TEC_6220 I value this treatment.

40
Table 10. Preliminary Summary of Patient Stakeholder Concerns With the American Chronic Pain Association Pain Log
Number of Concerns Reported by Conceptual Category
Item Content
Concerns Reported (N)a
Proportion of Reviews (%)
ondents (N) Pictures
Rating Scale Time Frame
rrelevant Content
omprehen sion/Ill‐ defined
Medication (taken as prescribed)
29 57.5% 23 18 8 0 2 1
Exercise (number of days per week)
18 35.0% 14 7 8 0 1 2
Overall activity level 17 35.0% 14 7 9 0 0 1
Sexual activity 15 30.0% 12 6 2 0 4 3
Alcohol (number of drinks)
9 22.5% 9 0 0 8 1 0
aFewer than 20% of interviewees expressed a concern for the following items: appetite, level of pain, stress level, fear of pain, side effects of medication, bowel irregularity, mood level, social interaction level, financial worries, sleep interference.
Note: The ACPA Pain Log is publicly available at https://theacpa.org/painLog/default.aspx .

41
Regarding clarity of the HEAL and PROMIS items, patients and providers found the items to be
clear and easy to understand (means ranged from 3.5 to 4.0 on a 0‐to‐4 scale). PROMIS pain‐
related measures were rated as highly relevant in the treatment context (means ranged from
3.8 to 4.0), and PROMIS Physical Function, Depression, Anxiety, and Sleep Disturbance were
also rated as clinically relevant (means ranged from 3.3 to 3.8). As we expected, the clinical
relevance of treatment‐related HEAL items (eg, TEX, PPC) were rated significantly higher than
within‐person HEAL items (POS and SPT). Paired t tests revealed TEX (mean = 3.5, SD = 0.8)
relevancy ratings were significantly higher than POS ratings (mean = 3.3, SD = 1.0) and SPT
ratings (mean = 2.3, SD = 1.4); t(79) = 2.31, p < .03 and t(79) = 6.54, p < .001, respectively, when
both patient and health care provider ratings were combined. PPC relevance ratings (mean =
3.5, SD = 0.7) were higher than those for POS and SPT (t(79) = 2.43, p < .02 and t(79) = 7.29, p <
.001, respectively) for the combined patient–provider sample. HCE was the only treatment‐
related HEAL item bank that did not significantly differ from the within‐person HEAL ratings of
POS and SPT. Overall, patients and HCPs were often in agreement of HEAL relevance to
treatment; however, health care providers rated the relevance of the TEX items and SPT items
lower than did patients (F[1, 79] = 9.90, p < .01, and F[1, 79] = 4.96, p < .03, respectively) (see
Figure 4 for HEAL Short Form items).
Our aim 3 intention regarding the ACPA Pain log was to collect in‐depth interview
information concerning the log’s graphic representations of symptoms and side effects, the
log’s response scales and verbal content, and the log’s general relevance for enhancing patient–
provider communication and understanding. Table 10 summarizes the types of comments
patients made about the ACPA Pain Log. Our research team will report these results in detail to
the ACPA along with any suggestions for changes to the log.
G. Discussion
Decisional Context. Our study evaluated the roles of patients’ perceptions, treatment‐
related beliefs, and personal characteristics in pain treatment outcomes. Of the patient‐
centered questions that inspire PCOR, 2 are relevant to the current study: “Given my personal
characteristics, conditions, and preferences, what should I expect will happen to me?” and
“What can I do to improve the outcomes that are important to me?” We found that nonspecific

42
factors as assessed by HEAL influenced pain treatment outcomes. The magnitude of baseline
HEAL scores’ influence on outcomes was small, although it was statistically significant for HEAL
POS, SPT, PCAM, and TEX. Having higher expectations regarding the value and personal
appropriateness of a particular treatment (eg, “This treatment is right for me”) was associated
with better outcomes at our 2‐month and 4‐month follow‐up. We also found that patients who
initiated CAM treatments had more positive outcomes than did those who chose conventional
medicine. Although the study design limits our ability to draw conclusions regarding the direct
causes of improvement, the study results may inspire patients to become familiar with and
educated about CAM treatments. And, if, once educated, they determine whether they could
personally expect benefits (ie, have high Treatment Expectancy), they may engage in CAM fully
and experience positive outcomes. Our results may also inform clinicians’ decisions. Clinicians
may be inspired in several ways: increased openness to CAM and increased recognition of the
importance of the patients’ beliefs about treatment and the connection between patient and
provider. In some settings and with some patients, providers may recognize the value of talking
about deeply personal factors such as spirituality. If health systems and payers recognize these
results, increase their openness to CAM for pain, and increase their focus on nonspecific factors
as important for outcomes, this could lead to decreasing the burden of pain in our society. It is
important to recognize, however, that not all patients have access to CAM due to lack of
availability and lack of insurance coverage for some CAM treatments. It is also important to
note that, in our study, CAM and conventional medicine patients differed from each other on
other factors, such as baseline average pain, and this may have also influenced the results.
The Study Results in Context. The study addresses the methods gap of heterogeneity of
patients and treatment effects, specifically evaluating how patient choices of CAM or
conventional treatment modify outcomes and assessing the modifying effects of initial
treatment expectations regarding pain treatment. To summarize what we have learned based
on the HTE analyses, 3 main patterns are worth noting. First, as a group, the chronic pain
patients in this study showed improvement over time in the following areas: Average Pain,
Physical Function, Pain Interference, and Pain Intensity. This was true for the group of
participants overall, regardless of type of treatment they received and whether their treatment

43
expectations were lower or higher than average. Second, participants’ characteristics and
treatment choices at baseline were strong predictors of their outcomes. Participants who
engaged in CAM treatments had less severe pain and better physical function at baseline than
did conventional medicine participants, and they also had greater improvements in these areas
over time. Likewise, those participants who had higher HEAL TEX at baseline showed greater
improvement in pain and function than those with lower HEAL TEX. Third, given the importance
of baseline HEAL TEX and patient choices about treatment types, and considering the impact of
time in predicting improvement, several other HEAL measures also emerged as contributing to
treatment outcomes. Although the additional outcome variance predicted was relatively small,
HEAL POS and HEAL SPT were statistically significant contributors to physical function and pain
outcomes, and HEAL CAM and HEAL PPC were statistically significant contributors to several
outcomes variables as well (see Tables 8 and 9).
There is growing recognition of the influence of nonspecific factors such as expectations,
beliefs, ritual, and perceptions of the patient–provider connection in the experience of pain.33
Some studies have evaluated open‐label placebo and found that patient beliefs and the ritual
involved with taking the placebo pills led to improvements in pain relative to patients receiving
usual care alone.14,34 A recent study used experimentally induced pain (a heat stimulus) and an
opioid or a placebo infusion, and manipulated treatment expectations and attention through
instructions to study participants. This study supported the role of expectations.35 Our study
adds to this literature by measuring reports of nonspecific factors from the patient’s
perspective and evaluating their role in real‐world pain treatment settings. In addition, we
obtained patients’ and clinicians’ perspectives on the utility of using HEAL and PROMIS to
enhance care in clinical settings.
Implementation of Study Results. Our aim 3 sought patients’ and clinicians’
perspectives on implementing PROMIS and HEAL assessments as part of clinical care. Patients
viewed treatment‐related assessments particularly favorably, rating them to be highly relevant.
Regarding HEAL, patients made statements such as, “Integration between mental and physical
is best” and “If I’m in a medical environment where people are spiritual, that adds another level
to me; there is more trust.” However, some patients felt that HEAL SPT questions were

44
irrelevant to their chronic pain condition, but “spirituality may be more relevant in a terminal
situation,” and some providers said that they would not be comfortable discussing the HEAL
PPC and HEAL HCE with their patients.
Conventional medicine providers also noted that the extra time required for viewing and
discussing HEAL and PROMIS reports with patients would be a barrier to implementation in
clinical settings. Thus, in implementing HEAL and PROMIS into clinical care in the future, it will
be important for the assessments to be completed online before visits and for automatically
generated summary reports to be easily available to clinicians as part of the medical record.
Ideally, clinicians should receive training in how to discuss the report with their patients. And,
preferably, patients and clinicians must have the freedom to choose which HEAL and PROMIS
measures to use as communication tools in their treatment. Similarly, many patients found the
ACPA Pain Log to be a potentially useful tool to enhance communication with their provider—
given that some confusing elements of the log can be modified. The research team will suggest
changes to the ACPA that should improve the log’s clinical utility.
Disseminating the results of this study and encouraging other researchers to adopt HEAL
into their studies were major activities of our research team and PSAP during recent months.
Publications and presentations are listed in Section M of this report. Our dissemination of HEAL
measures to other researchers is also provided in Section M.
Generalizability. We were able to recruit and retain a fairly diverse sample of persons with
chronic pain, including 23% nonwhite or multiracial persons, 25% males, and approximately
50% with less than a 4‐year college education; however, we had few persons of Hispanic/Latino
ethnicity in the study (14 out of 209). We increased the breath of our sample by including
patients from the Venice Clinic at UCLA, which is an integrative medicine clinic where patients
receive treatment free of charge. Our results have reasonable generalizability to US populations
seeking treatment for chronic pain. However, HEAL and many PROMIS measures are equally
relevant for patients with a broad range of medical conditions and treatments, and the choice
to study chronic pain limits the generalizability of our results to other patient populations.
Subpopulation Considerations. Our study included subpopulations of persons seeking

45
CAM treatment and conventional medicine treatment. Persons in CAM treatments tended to
have higher expectations about their new treatment and better self‐reported health and less
pain than those in conventional treatments, and fewer of the CAM patients were also using
opioid medications. Approximately one‐quarter of both CAM and conventional participants
reported having 2 or more medical comorbidities in addition to their chronic pain; thus
medically ill persons were represented. The questions regarding opioid use were suggested by a
clinician member of our PSAP to explore the potential role of opioids in treatment satisfaction
with pain treatment overall, which will require further study. We assessed the PROMIS health
status measures of depressive and anxiety symptoms; these psychosocial factors are important
to assess along with self‐reports of pain and physical function. Although depression can
contribute to poor pain treatment outcomes, our study found that, overall, in our diverse
sample of persons who freely select their pain treatments, depressive symptoms were not
significantly reduced over the 4‐month period of study; however, pain was reduced over time
to a statistically significant extent.
Study Limitations. This study focused broadly on the measuring contextual factors in
treatment using the HEAL and PROMIS health status instruments. We chose to study patients
with chronic pain during their routine, self‐chosen treatments. Thus, there are limits to the
generalizability of this study beyond pain. And, due to the diversity of treatments, from
acupuncture to physical therapy, we are unable to discern for which treatments contextual
factors may be most important. HEAL and many PROMIS measures are relevant on a broad
level to many types of medical conditions and treatments, however. In addition, in addressing
the HTE methods gap, we chose to evaluate subgroups of patients based on type of treatment
they had chosen (CAM or conventional medicine). In separate subgroup analyses, we also chose
to evaluate outcomes in subgroups of patients with lower and higher levels of HEAL TEX. These
treatment type and expectancy subgroupings were important factors in HTE; however, the
roles of other potentially important factors remain unknown. A limitation of this study is that
biases may be present in the analysis of HTE. Patients in the comparison groups of CAM versus
conventional medicine and those showing low versus high HEAL TEX may diverge in many ways.
Of note, CAM and conventional medicine patients did not differ on demographic grounds;

46
however, in terms of clinical variables, there were differences. CAM participants reported less
pain on average at baseline and were less likely to be taking prescription opioid medications.
Thus, there may be bias in our HTE results. We addressed this through controlling for baseline
level of Average Pain (and baseline levels of our other outcome variables) in our final
multivariate models.
Some of the limits to the conclusions that can be drawn from this study are based on our
chosen design. This study was a cohort study of patients who chose their pain treatments.
Factors that may contribute to those choices—such as preference for CAM methods, types of
pain, and severity of symptoms—were not controlled. The self‐selection of treatments, while of
real‐world significance, is a limitation of this study. In contrast, in randomized controlled trials
such potential sources of bias or confounding can be systematically addressed through
stratification and other methods. Another limitation is that, given our simple subgroup
analyses, we did not show that HEAL scores (such as TEX) identified a subpopulation for whom
CAM therapies were more effective than conventional therapies. That said, despite limitations
in the design, the study has value, as it was conducted in the real‐world settings in which
patients with chronic pain seek and obtain treatment.
Future Research. Recommendations for future research include evaluating HEAL and
PROMIS measures in populations with medical illnesses other than chronic pain to support
generalizability. Feasibility, acceptability, and outcomes associated with implementing HEAL
and PROMIS within the electronic medical record in real‐world clinical settings should also be a
focus of future research. In addition, HEAL measures could be a valuable addition to large
placebo‐controlled trials. In such a research design, investigators would be able to test, through
patient‐reported measures, the specific influences of treatment beliefs and personal
characteristics as contributors to the placebo effect.
H. Conclusions
We found that the patients’ perceptions of the treatment context and of themselves (eg,
positive outlook and spirituality), as assessed by the HEAL measures, are associated with
PROMIS pain treatment outcomes. This is consistent with recent literature on nonspecific and
placebo research in pain.14,35 Factors such as expectations about treatment and participation in

47
CAM versus conventional medical treatment were associated with significant differences in
symptoms throughout the 4 months of our study follow‐up. In interviews, patients and
clinicians reported that the HEAL and PROMIS measures were easy to understand and useful for
enhancing patient–provider communication during treatment. These results may be useful to
the following health care decision makers: patients, clinicians, and health system leaders who
are interested in enhancing treatment outcomes and fully engaging patients in treatment.

48
References
1. Barrett B, Muller D, Rakel D, Rabago D, Marchand L, Scheder JC. Placebo, meaning, and health. Perspect Biol Med. 2006;49(2):178‐198.
2. Institute of Medicine Committee on Advancing Pain Research, Care, and Education. Relieving Pain in America: A Blueprint for Transforming Prevention, Care, Education and Research. Washington, DC: National Academies Press; 2011.
3. Barrett B, Muller D, Rakel D, Rabago D, Marchand L, Scheder JC. Placebo, meaning, and health. Perspect Biol Med. 2006;49(2):178‐198.
4. Price DD, Finniss DG, Benedetti F. A comprehensive review of the placebo effect: recent advances and current thought. Annu Rev Psychol. 2008;59(1):565‐590.
5. Vase L, Robinson ME, Verne NG, Price DD. The contributions of suggestion, desire, and expectation to placebo effects in irritable bowel syndrome patients. Pain. 2003;105(1):17‐25.
6. Vase L, Robinson ME, Verne NG, Price DD. Increased placebo analgesia over time in irritable bowel syndrome (IBS) patients is associated with desire and expectation but not endogenous opioid mechanisms. Pain. 2005;115(3):338‐347.
7. Wasan AD, Kong J, Pham L‐D, Kaptchuk TJ, Edwards R, Gollub RL. The impact of placebo, psychopathology, and expectations on the response to acupuncture needling in patients with chronic low back pain. J Pain. 2010;11(6):555‐563.
8. Kaptchuk TJ, Kelley JM, Conboy LA, et al. Components of placebo effect: randomised controlled trial in patients with irritable bowel syndrome. BMJ. 2008;336(7651):999‐1003.
9. Karp JF, Yu L, Friedly J, Amtmann D, Pilkonis PA. Negative affect and sleep disturbance may be associated with response to epidural steroid injections for spine‐related pain. Arch Phys Med Rehabil. 2014;95(2):309‐315.
10. Jamison RN, Edwards RR, Liu X, et al. Relationship of negative affect and outcome of an opioid therapy trial among low back pain patients. Pain Pract. 2012;13(3):173‐181.
11. Hyland ME, Geraghty AWA, Joy OET, Turner SI. Spirituality predicts outcome independently of expectancy following flower essence self‐treatment. J Psychosom Res. 2006;60(1):53‐58.
12. Hyland ME, Whalley B. Motivational concordance: an important mechanism in self‐help therapeutic rituals involving inert (placebo) substances. J Psychosom Res. 2008;65(5):405‐413.
13. Jegindø E‐ME, Vase L, Skewes JC, et al. Expectations contribute to reduced pain levels during prayer in highly religious participants. J Behav Med. 2012;36(4):413‐426.
14. Carvalho C, Caetano JM, Cunha L, Rebouta P, Kaptchuk TJ, Kirsch I. Open‐label placebo treatment in chronic low back pain: a randomized controlled trial. Pain. 2016;157(12):2766‐2772.

49
15. Kaptchuk TJ, Friedlander E, Kelley JM, et al. Placebos without deception: a randomized controlled trial in irritable bowel syndrome. PLoS One. 2010;5(10):1‐7.
16. Dossett ML, Mu L, Davis RB, et al. Patient‐provider interactions affect symptoms in gastroesophageal reflux disease: a pilot randomized, double‐blind, placebo‐controlled trial. PLoS One. 2015;10(9):e0136855.
17. Cella D, Yount S, Rothrock N, et al. The Patient‐Reported Outcomes Measurement Information System (PROMIS). Med Care. 2007;45(suppl 1):S3‐S11.
18. Cella D, Gershon R, Lai J‐S, Choi S. The future of outcomes measurement: item banking, tailored short‐forms, and computerized adaptive assessment. Qual Life Res. 2007;16(suppl 1):133‐141.
19. Reeve BB, Hays RD, Bjorner JB, et al. Psychometric evaluation and calibration of health‐related quality of life item banks. Med Care. 2007;45(suppl 1):S22‐S31.
20. Greco CM, Glick RM, Morone NE, Schneider MJ. Addressing the "it is just placebo" pitfall in CAM: methodology of a project to develop patient‐reported measures of nonspecific factors in healing. Evid Based Complement Alternat Med. 2013;2013:1‐9.
21. Greco CM, Yu L, Johnston KL, et al. Measuring nonspecific factors in treatment: item banks that assess the healthcare experience and attitudes from the patient’s perspective. Qual Life Res. 2016;25(7):1625‐1634.
22. Cella D, Riley W, Stone A, et al. The Patient‐Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self‐reported health outcome item banks: 2005‐2008. J Clin Epidemiol. 2010;63(11):1179‐1194.
23. Pilkonis PA, Choi SW, Reise SP, et al. Item banks for measuring emotional distress from the Patient‐Reported Outcomes Measurement Information System (PROMIS): Depression, anxiety, and anger. Assessment. 2011;18(3):236‐283.
24. Pilkonis PA, Choi SW, Reise SP, et al. Item banks for measuring emotional distress from the Patient‐Reported Outcomes Measurement Information System (PROMIS): Depression, anxiety, and anger. Assessment. 2011;18(3):263‐283.
25. Amtmann D, Cook KF, Jensen MP, et al. Development of a PROMIS item bank to measure pain interference. Pain. 2010;150(1):173‐182.
26. Cella D, Riley W, Stone A, et al. The Patient‐Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self‐reported health outcome item banks: 2005‐2008. J Clin Epidemiol. 2010;63(11):1179‐1194.
27. Choi SW, Reise SP, Pilkonis PA, Hays RD, Cella D. Efficiency of static and computer adaptive short forms compared to full length measures of depressive symptoms. Qual Life Res. 2010;19:125‐135.
28. Guy W. Clinical global impressions. In: ECDEU Assessment Manual for Psychopharmacology. Rockville, MD: National Institute of Mental Health; 1976:218‐222.

50
29. Rose M, Bjorner JB, Becker J, Fries JF, Ware JE. Evaluation of a preliminary physical function item bank supports the expected advantages of the Patient‐Reported Outcomes Measurement Information System (PROMIS). Assessment. 2008;61(1):17‐33.
30. Greco CM, Glick RM, Morone NE, Schneider MJ. Addressing the “it is just placebo” pitfall in CAM: methodology of a project to develop patient‐reported measures of nonspecific factors in healing. Evid Based Complement Alternat Med. 2013;2013:1‐9.
31. Huston P, Rowan M. Qualitative studies: their role in medical research. Can Fam Physician. 1998;44:2453‐2458.
32. Guest G. How many interviews are enough? an experiment with data saturation and variability. Field Methods. 2006;18(1):59‐82.
33. Kelley JM, Lembo AJ, Ablon JS, et al. Patient and practitioner influences on the placebo effect in irritable bowel syndrome. Psychosom Med. 2009;71(7):789‐797.
34. Kaptchuk TJ, Friedlander E, Kelley JM, et al. Placebos without deception: a randomized controlled trial in irritable bowel syndrome. PLoS One. 2010;5(12):e15591.
35. Atlas LY, Wielgosz J, Whittington RA, Wager TD. Specifying the non‐specific factors underlying opioid analgesia: expectancy, attention, and affect. Psychopharmacology (Berl). 2014;231(5):813‐823.

51
APPENDIX

Appendix A: Cognitive Interview Materials
1. Patient Interview – Baseline2. Patient Interview – Assessment 23. Patient FAQ4. Clinician Interview – Baseline5. Clinician Interview – Assessment 26. Clinician FAQ7. HEAL definitions

PROMIS Patient Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Treatment Expectancy items are clear and easy to understand.
The Treatment Expectancy items are relevant to my treatment experience.
The Treatment Expectancy items provide useful information to my healthcare provider.
The Patient-Provider Connection items are clear and easy to understand.
The Patient-Provider Connection items are relevant to my treatment experience.
The Patient-Provider Connection items provide useful information to my healthcare provider.
The Healthcare Environment items are clear and easy to understand.
The Healthcare Environment items are relevant to my treatment experience.
The Healthcare Environment items provide useful information to my healthcare provider.
The Positive Outlook items are clear and easy to understand.
The Positive Outlook items are relevant to my treatment experience.
The Positive Outlook items provide useful information to my healthcare provider.
The Spirituality items are clear and easy to understand.
The Spirituality items are relevant to my treatment experience.
The Spirituality items provide useful information to my healthcare provider.
The CAM Attitudes items are clear and easy to understand.
The CAM Attitudes items are relevant to my treatment experience.
The CAM Attitudes items provide useful information to my healthcare provider.
The Pain Intensity items are clear and easy to understand.
The Pain Intensity items are relevant to my treatment experience.
The Pain Intensity items provide useful information to my practitioner.

PROMIS Patient Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Pain Interference items are clear and easy to understand.
The Pain Interference items are relevant to my treatment experience.
The Pain Interference items provide useful information to my healthcare provider.
The Limited Physical Function items are clear and easy to understand.
The Limited Physical Function items are relevant to my treatment experience.
The Limited Physical Function items provide useful information to my healthcare provider.
The Sleep Problems items are clear and easy to understand.
The Sleep Problems items are relevant to my treatment experience.
The Sleep Problems items provide useful information to my healthcare provider.
The Fatigue items are clear and easy to understand.
The Fatigue items are relevant to my treatment experience.
The Fatigue items provide useful information to my healthcare provider.
The Depression items are clear and easy to understand.
The Depression items are relevant to my treatment experience.
The Depression items provide useful information to my healthcare provider.
The Anxiety items are clear and easy to understand.
The Anxiety items are relevant to my treatment experience.
The Anxiety items provide useful information to my healthcare provider.

PROMIS Patient Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the graph and item report resulting from the questions you were asked on the computer.
Did the questions on the computer assessment make sense? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What do you like/dislike about the graphical and numerical formats? What could we do to improve these formats? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do the scores make sense? Do you understand from the graphs/item output which areas might be important to you and your provider? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Would this type of information help your treatment? In what way? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Patient Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
How comfortable would you be discussing this information during your treatment sessions? How should the assessments be used in treatment? How useful do you think this information would be in communicating with your healthcare provider?
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do you like the color?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Are the HEAL definitions helpful?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do you prefer paper-and-pencil questionnaires or computer questionnaires? Why?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do you have any overall comments about your experience completing the questionnaires? What other suggestions do you have for us?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Patient Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the “Live Better with Pain Log”
Did this questionnaire make sense? Why or why not? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
When you were making your ratings, did you refer to the pictures? Did the pictures accurately represent the questions? Would you change them in any way? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
On a scale of 1-10, with 1 being not at all helpful and 10 being extremely helpful, how helpful were the pictures when you were answering the questions? __________________________________________________________________________________________
How helpful were the numbers below each set of pictures when you were making your ratings?
______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What questions or suggestions do you have about this assessment? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Patient Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Treatment Expectancy items are clear and easy to understand.
The Treatment Expectancy items are relevant to my treatment experience.
The Treatment Expectancy items provide useful information to my healthcare provider.
The Patient-Provider Connection items are clear and easy to understand.
The Patient-Provider Connection items are relevant to my treatment experience.
The Patient-Provider Connection items provide useful information to my healthcare provider.
The Healthcare Environment items are clear and easy to understand.
The Healthcare Environment items are relevant to my treatment experience.
The Healthcare Environment items provide useful information to my healthcare provider.
The Positive Outlook items are clear and easy to understand.
The Positive Outlook items are relevant to my treatment experience.
The Positive Outlook items provide useful information to my healthcare provider.
The Spirituality items are clear and easy to understand.
The Spirituality items are relevant to my treatment experience.
The Spirituality items provide useful information to my healthcare provider.
The CAM Attitudes items are clear and easy to understand.
The CAM Attitudes items are relevant to my treatment experience.
The CAM Attitudes items provide useful information to my healthcare provider.
The Pain Intensity items are clear and easy to understand.
The Pain Intensity items are relevant to my treatment experience.
The Pain Intensity items provide useful information to my practitioner.

PROMIS Patient Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Pain Interference items are clear and easy to understand.
The Pain Interference items are relevant to my treatment experience.
The Pain Interference items provide useful information to my healthcare provider.
The Limited Physical Function items are clear and easy to understand.
The Limited Physical Function items are relevant to my treatment experience.
The Limited Physical Function items provide useful information to my healthcare provider.
The Sleep Problems items are clear and easy to understand.
The Sleep Problems items are relevant to my treatment experience.
The Sleep Problems items provide useful information to my healthcare provider.
The Fatigue items are clear and easy to understand.
The Fatigue items are relevant to my treatment experience.
The Fatigue items provide useful information to my healthcare provider.
The Depression items are clear and easy to understand.
The Depression items are relevant to my treatment experience.
The Depression items provide useful information to my healthcare provider.
The Anxiety items are clear and easy to understand.
The Anxiety items are relevant to my treatment experience.
The Anxiety items provide useful information to my healthcare provider.

PROMIS Patient Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the handouts titled “XXXXXXXX” (PROMIS/HEAL graph and items) and the questions you answered on the computer.
Did the questions on the computer assessment make sense? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Since taking the first assessment, have you and your treatment provider discussed the assessment or the results? If so, tell me more about that. Has the information been helpful? __________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Is it useful to see how your answers have changed over time? In what way? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What do you like/dislike about the graphical and numerical formats? What could we do to improve these formats? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do you like the color?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Patient Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Are the HEAL definitions helpful?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Do you understand that the presentation is over time?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
How comfortable would you be discussing this information during your treatment sessions? How should the assessments be used in treatment? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What other suggestions do you have for us?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PCORI Interview FAQ’s
Patient:
1. Can I have a hard copy of the graphs and items?We would like the opportunity to speak with your healthcare provider before we give you acopy or your results. Once we have spoken with them, you are free to ask them for a copy ofyour results, or you can contact our office at (412) 246-6972. In order it give us a chance toreach your healthcare provider, we ask that you wait at least 30 days after this interview tocontact us.
2. Can I have an electronic version (e.g. pdf) of the graphs and items?Yes, we can provide you with a secured pdf after we have contacted your healthcare provider.
3. What does a rating of 50 mean?A rating of 50 is considered “average” for the general population. These items were tested in asample of the US population which was balanced for age, race, gender, and education.
The numbers on the graphs are percentiles on a scale of 0-100 that tell us the percent of peoplein general who rate this item less than you. For example, the 20th percentile is the value (or“rating”) in which 20% of people score at or below.
4. Can you explain what the high ratings mean in the separate categories?In general, higher ratings indicate “more” of that category, and vice versa. A higher rating couldsometimes be more favorable, Patient Provider Connection, and sometimes less favorable, i.e.Pain Intensity.
5. Why are there only 4-6 questions in some of the categories?
All of the questions are presented in a Computerized Adaptive Test (CAT) format. Items are selected on the basis of the person’s responses to previous items. Each person only needs to answer a subset of items to accurately estimate what would have been obtained by administering the entire set of items.
6. What are all of the possible response options?For a majority of the questions, the possible responses are: Frequency: Never Rarely Sometimes Often Almost Always
Severity: Not at all A little bit Somewhat Quite a bit Very Much

Category Response Options
Treatment Expectancy Not at all, A little bit, … , Quite a bit, Very much
Patient-Provider Connection Never, Rarely, … , Often, Almost always Not at all, A little bit, … , Quite a bit, Very much
Healthcare Environment Never, Rarely, … , Often, Almost always Not at all, A little bit, … , Quite a bit, Very much
Positive Outlook Never, Rarely, … , Often, Almost always Not at all, A little bit, … , Quite a bit, Very much
Spirituality Never, Rarely, … , Often, Almost always Not at all, A little bit, … , Quite a bit, Very much
CAM Attitudes Not at all, A little bit, … , Quite a bit, Very much
Pain Intensity Had no pain, Mild, … , Severe, Very severe No pain, Mild, … , Severe, Very severe
Pain Interference Never, Rarely, … , Often, Always Not at all, A little bit, … , Quite a bit, Very much
Limited Physical Function Cannot do, Quite a lot, … , Very little, Not at all Can't do because of health, A lot of difficulty, … , A little bit of difficulty, No difficulty at all Unable to do, With much difficulty, … , With a little difficulty, Without any difficulty
Sleep Problems Never, Rarely, … , Often, Always Not at all, A little bit, … , Quite a bit, Very much Very good, Good, … , Poor, Very poor
Fatigue Never, Rarely, … , Often, Always Not at all, A little bit, … , Quite a bit, Very much None, Mild, … , Severe, Very severe None, 1 day, … , 4-5 days, 6-7 days
Depression Never, Rarely, … , Often, Always
Anxiety Never, Rarely, … , Often, Always

PROMIS Clinician Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Treatment Expectancy items are clear and easy to understand.
The Treatment Expectancy items are relevant to the care I provide.
The Treatment Expectancy items provide useful information.
The Patient-Provider Connection items are clear and easy to understand.
The Patient-Provider Connection items are relevant to the care I provide.
The Patient-Provider Connection items provide useful information.
The Healthcare Environment items are clear and easy to understand.
The Healthcare Environment items are relevant to the care I provide.
The Healthcare Environment items provide useful information.
The Positive Outlook items are clear and easy to understand.
The Positive Outlook items are relevant to the care I provide.
The Positive Outlook items provide useful information.
The Spirituality items are clear and easy to understand.
The Spirituality items are relevant to the care I provide.
The Spirituality items provide useful information.
The CAM Attitudes items are clear and easy to understand.
The CAM Attitudes items are relevant to the care I provide.
The CAM Attitudes items provide useful information.
The Pain Intensity items are clear and easy to understand.
The Pain Intensity items are relevant to the care I provide.
The Pain Intensity items provide useful information.

PROMIS Clinician Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Pain Interference items are clear and easy to understand.
The Pain Interference items are relevant to the care I provide.
The Pain Interference items provide useful information.
The Limited Physical Function items are clear and easy to understand.
The Limited Physical Function items are relevant to the care I provide.
The Limited Physical Function items provide useful information.
The Sleep Problems items are clear and easy to understand.
The Sleep Problems items are relevant to the care I provide.
The Sleep Problems items provide useful information.
The Fatigue items are clear and easy to understand.
The Fatigue items are relevant to the care I provide.
The Fatigue items provide useful information.
The Depression items are clear and easy to understand.
The Depression items are relevant to the care I provide.
The Depression items provide useful information.
The Anxiety items are clear and easy to understand.
The Anxiety items are relevant to the care I provide.
The Anxiety items provide useful information.
The Alcohol Use items are clear and easy to understand.
The Alcohol Use items are relevant to the care I provide.
The Alcohol Use items provide useful information.

PROMIS Clinician Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the handouts titled “XXXXXXXX” (PROMIS/HEAL graph and items).
Are the questions your patient answered easy to understand? What would you change about them? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Would this type of information affect your treatment decisions? In what way? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What do you like/dislike about the graphical and numerical formats? What could we do to improve these formats? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
How comfortable would you be discussing this information during your treatment sessions? How should the assessments be used in treatment? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Clinician Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Do you prefer paper-and-pencil questionnaires or computer questionnaires? Why?
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What barriers are there to implementing an assessment like this in your clinic?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What other suggestions do you have for us?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Clinician Interview – Baseline PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the “Live Better with Pain Log”
Do you feel this questionnaire will be easily understood by patients? Why or why not? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Did the pictures accurately represent the questions? Would you change them in any way? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
On a scale of 1-10, with 1 being not at all helpful and 10 being extremely helpful, how helpful is this information when formulating a treatment plan? __________________________________________________________________________________________
What questions or suggestions do you have about this assessment? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Clinician Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Treatment Expectancy items are clear and easy to understand.
The Treatment Expectancy items are relevant to the care I provide.
The Treatment Expectancy items provide useful information.
The Patient-Provider Connection items are clear and easy to understand.
The Patient-Provider Connection items are relevant to the care I provide.
The Patient-Provider Connection items provide useful information.
The Healthcare Environment items are clear and easy to understand.
The Healthcare Environment items are relevant to the care I provide.
The Healthcare Environment items provide useful information.
The Positive Outlook items are clear and easy to understand.
The Positive Outlook items are relevant to the care I provide.
The Positive Outlook items provide useful information.
The Spirituality items are clear and easy to understand.
The Spirituality items are relevant to the care I provide.
The Spirituality items provide useful information.
The CAM Attitudes items are clear and easy to understand.
The CAM Attitudes items are relevant to the care I provide.
The CAM Attitudes items provide useful information.
The Pain Intensity items are clear and easy to understand.
The Pain Intensity items are relevant to the care I provide.
The Pain Intensity items provide useful information.

PROMIS Clinician Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Please rate the following statements on a 5-point scale:
0 – Not at all 1 – A little bit 2 – Somewhat 3 – Quite a bit 4 – Very Much
The Pain Interference items are clear and easy to understand.
The Pain Interference items are relevant to the care I provide.
The Pain Interference items provide useful information.
The Limited Physical Function items are clear and easy to understand.
The Limited Physical Function items are relevant to the care I provide.
The Limited Physical Function items provide useful information.
The Sleep Problems items are clear and easy to understand.
The Sleep Problems items are relevant to the care I provide.
The Sleep Problems items provide useful information.
The Fatigue items are clear and easy to understand.
The Fatigue items are relevant to the care I provide.
The Fatigue items provide useful information.
The Depression items are clear and easy to understand.
The Depression items are relevant to the care I provide.
The Depression items provide useful information.
The Anxiety items are clear and easy to understand.
The Anxiety items are relevant to the care I provide.
The Anxiety items provide useful information.

PROMIS Clinician Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
For the following set of questions, we will be referring to the handouts titled “XXXXXXXX” (PROMIS/HEAL graph and items).
Are the questions your patient answered easy to understand? What would you change about them? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
Have you discussed the results of the first assessment with this patient? What affect has that had on your treatment plan? _______________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What do you like/dislike about the graphical and numerical formats? What could we do to improve these formats? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
How comfortable would you be discussing this information during your treatment sessions? How should the assessments be used in treatment? ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PROMIS Clinician Interview – Assessment 2 PCORI
ID# __ __ __ __ __ __ Initials __ . __ __ __ Date __ __ / __ __ / __ __
Is it useful to see how your patient’s answers have changed over time? In what way?
___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What barriers are there to implementing an assessment like this in your clinic?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
What other suggestions do you have for us?
________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________

PCORI Interview FAQ’s (Healthcare provider)
1. Can I make these items a part of my patient’s medical record/clinical file?**NO. Please do not add hard copies or electronic copies of these data into your patient’s files. If you would liketo document a discussion of the information, we suggest a general “as reported by [patient]…” approach, ratherthan stating the information was directly drawn from the computerized assessment study.
As a part of our NIH Certificate of Confidentiality, we are not permitted to include references or documentsrelated to this study in the patients’ medical records. Also, the current study is a pilot study and the graphs andformatting will be changing throughout the study.
2. Can I have a hard copy of the graphs and items?Yes, we will provide you with a hard copy of each. Feel free to provide your patient with a copy as well. (Thepatient has seen this info during his/her baseline interview, but was not provided a copy at that point.)
3. Can I have an electronic version (e.g. pdf) of the graphs and items?Yes, we can provide you with a secured pdf.
4. What does a score of 50 mean?A score of 50 is considered “average” for the general population.
These items were tested in a sample of the US population which was balanced for age, race, gender, and education.
5. What do scores between 40 and 60 mean?A score of 40 or 60 means that 40 or 60% of the population scored at the same level or below your patient.
6. Can you explain what the high scores mean in the separate categories?In general, higher scores indicate “more” of that category, and vice versa. Certain categories are more“negative” while others could be considered “positive”. For example, a higher than average score in the Angercategory would indicate “more” anger. On the other hand, a higher than average score in Social Satisfactionwould indicate “more” satisfaction.
7. Do you have definitions of each of the categories?Yes, we have definitions available for most of the categories if you are interested. They are also available on themain PROMIS website: http://www.nihpromis.org/measures/domainframework
8. Why are there only 4-6 questions in some of the categories?
All of the questions are presented in a Computerized Adaptive Test (CAT) format. CAT is a method of administering tests by computer, based on the psychometric framework of IRT (Item Response Theory). Items are selected on the basis of the examinee’s responses to previously administered items. This process uses an algorithm to estimate person "ability" and then chooses the best next item, enabling test administration based on specifications such as content coverage and test length. The capacity to rank all examinees on the same continuum, even if they have not been given any common items, allows for a test that is individually tailored to each examinee. With item banking, each patient need only answer a subset of items to obtain a measure that accurately estimates what would have been obtained by administering the entire set of items.

Helpful Definitions
Treatment Expectancy • Your expectations about whether the treatment will be helpful
Patient-Provider Connection • Your views of your relationship with your healthcare provider
Healthcare Environment • Your views about the healthcare provider’s office and staff
Positive Outlook • Your level of confidence and optimism, in general
Spirituality • Your spiritual beliefs and experience of spiritual support
Attitudes toward CAM (Complementary Alternative Medicine) • Your views about integrative medicine or CAM

Appendix B: Glossary of Terms
ABBREVIATIONREVIATI TERM
ACPA American Chronic Pain Association ANX PROMIS Anxiety AvePain PROMIS Average Pain BMI Body Mass Index CAM Complementary/Alternative Medicine CAM Attitudes Toward CAM (HEAL) CATs Computerized Adaptive Tests CCI Charlson Comorbidity Index CGI Clinical Global Improvement CON Conventional (medicine group) DEP PROMIS Depression FAQ Frequently Asked Questions FAT PROMIS Fatigue HCE Health Care Environment (HEAL) HEAL Healing Encounters and Attitudes Lists Health PROMIS Overall Health HTE Heterogeneity of Treatment Effects IOM Institute of Medicine IRB Institutional Review Board IRT Item Response Theory NCCAM National Center for Complementary and Alternative Medicine NIH National Institutes of Health NS Not significant OLS Ordinary Least Squares PHYS PROMIS Physical Function PI PROMIS Pain Interference PINT PROMIS Pain Intensity POS Positive Outlook (HEAL) PPC Patient-Provider Connection (PPC) PROMIS Patient Reported Outcomes Measurement Information System PROs Patient Reported Outcomes PSAP Patient Stakeholder Advisory Panel SD Standard Deviation SLP PROMIS Sleep SPT Spirituality (HEAL) TEX Treatment Expectancy (HEAL) UCLA University of California Los Angeles

Copyright© 2019. University of Pittsburgh. All Rights Reserved.
Disclaimer: The [views, statements, opinions] presented in this report are solely the responsibility of the author(s) and do not necessarily represent the views of the Patient‐Centered Outcomes Research Institute® (PCORI®), its Board of Governors or Methodology Committee.
Acknowledgement: Research reported in this report was [partially] funded through a Patient‐Centered Outcomes Research Institute® (PCORI®) Award (#ME‐1402‐10114) Further information available at: https://www.pcori.org/research-results/2014/using-surveys-assess-patient-centered-factors-may-affect-responses-chronic