Embed Size (px)
Citation preview

Using video to explore behavioural skills in the consultation
The Calgary-Cambridge approach

The MRCGP criteria - tear them up?

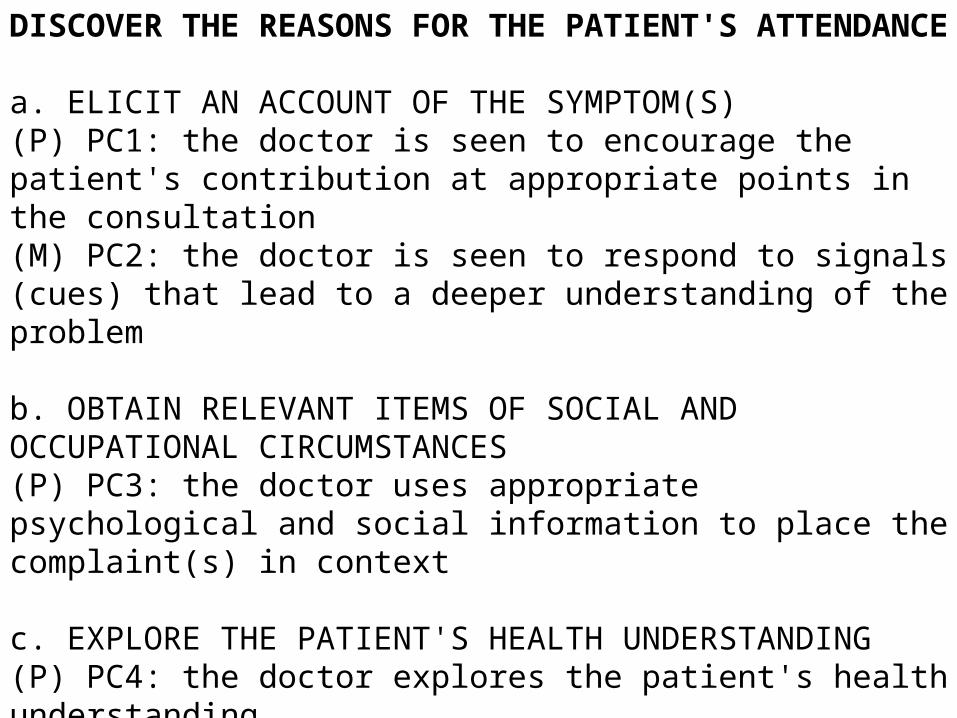
DISCOVER THE REASONS FOR THE PATIENT'S ATTENDANCE
a. ELICIT AN ACCOUNT OF THE SYMPTOM(S)(P) PC1: the doctor is seen to encourage the patient's contribution at appropriate points in the consultation(M) PC2: the doctor is seen to respond to signals (cues) that lead to a deeper understanding of the problem
b. OBTAIN RELEVANT ITEMS OF SOCIAL AND OCCUPATIONAL CIRCUMSTANCES(P) PC3: the doctor uses appropriate psychological and social information to place the complaint(s) in context
c. EXPLORE THE PATIENT'S HEALTH UNDERSTANDING(P) PC4: the doctor explores the patient's health understanding

DEFINE THE CLINICAL PROBLEM(S)
a. OBTAIN ADDITIONAL INFORMATION ABOUT THE SYMPTOMS, AND OTHER DETAILS OF MEDICAL HISTORY
(P) PC5: the doctor obtains sufficient information to include or exclude likely relevant significant conditions
b. ASSESS THE PATIENT BY APPROPRIATE PHYSICAL AND MENTAL EXAMINATION
(P) PC6: the physical/mental examination chosen is likely to confirm or disprove hypotheses that could reasonably have been formed OR is designed to address a patient's concern
c. MAKE A WORKING DIAGNOSIS
(P) PC7: the doctor appears to make a clinically appropriate working diagnosis

EXPLAIN THE PROBLEM(S) TO THE PATIENT
a. SHARE THE FINDINGS WITH THE PATIENT
(P) PC8: the doctor explains the problem or diagnosis in appropriate language
(M) PC9: the doctor's explanation incorporates some or all of the patient's health beliefs
b. ENSURE THAT THE EXPLANATION IS UNDERSTOOD AND ACCEPTED BY THE PATIENT
(M) PC10: the doctor specifically seeks to confirm the patient's understanding of the diagnosis
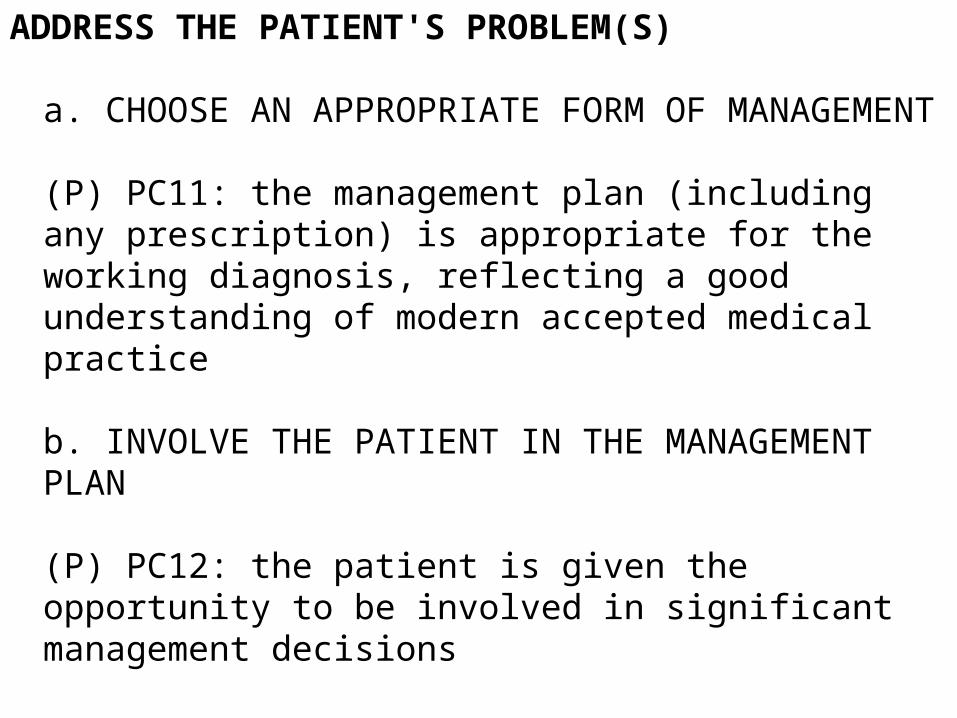
ADDRESS THE PATIENT'S PROBLEM(S)
a. CHOOSE AN APPROPRIATE FORM OF MANAGEMENT
(P) PC11: the management plan (including any prescription) is appropriate for the working diagnosis, reflecting a good understanding of modern accepted medical practice
b. INVOLVE THE PATIENT IN THE MANAGEMENT PLAN
(P) PC12: the patient is given the opportunity to be involved in significant management decisions

MAKE EFFECTIVE USE OF THE CONSULTATION
a. MAKE EFFECTIVE USE OF RESOURCES
(M) PC13: in prescribing the doctor takes steps to enhance concordance, by exploring and responding to the patient’s understanding of the treatment
(P) PC14: the doctor specifies the conditions and interval for follow-up or review
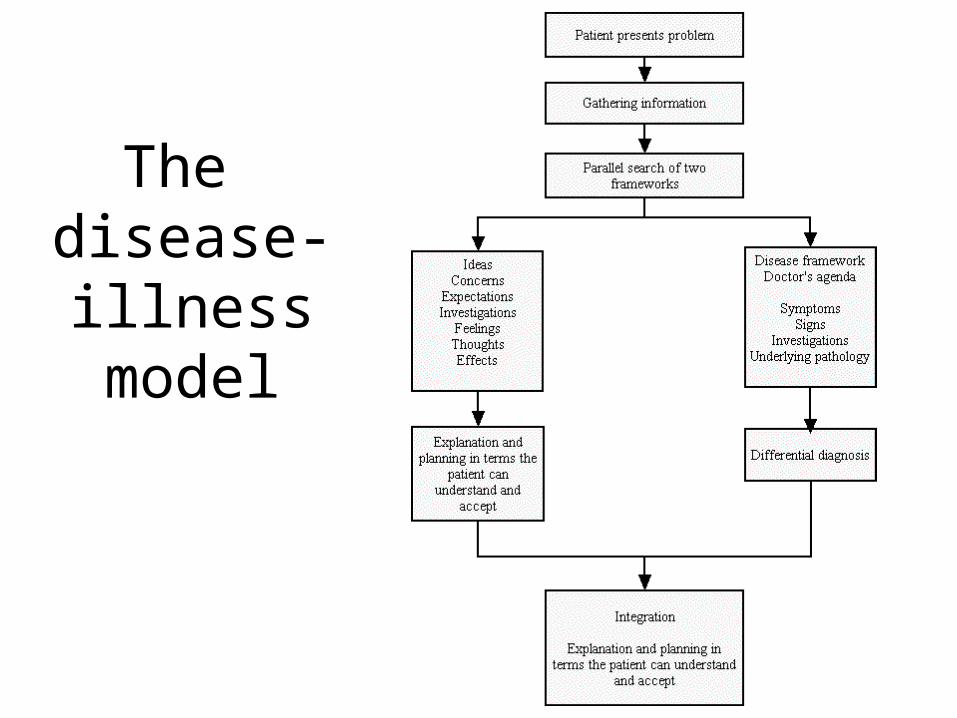
The disease- illness model

Evidence to support listeningBeckman and Frankdll (1984)
• Doctors frequently interrupted patients before they had completed their opening statement — after a mean time of only 18 seconds!
• Only 23% of patients completed their opening statement • in only one of 51 interrupted statements was the patient
allowed to complete their opening statement later • 94% of all interruptions concluded with the doctor obtaining
the floor • The longer the doctor waited before interruption, the more
complaints were elicited • Allowing the patient to complete the opening statement led
to a significant reduction in late-arising problems

Evidence to support listeningBeckman and Frankdll (1984)
• Clarifying or closed questions were the most frequent cause of interruption but any utterance by the doctor that specifically encouraged the patient to give further information about any one problem could also cause disruption: this, perhaps surprisingly, included echoing of the patient’s words
• In 34 our of 51 visits, the doctor interrupted the patient after the initial concern, apparently assuming that the first complaint was the chief one
• The serial order in which the patients presented their problems was not related to their clinical importance
• Most patients who were allowed to complete their opening statement without interruption took less that 60 seconds and none took longer the 150 seconds, even when encouraged to continue.
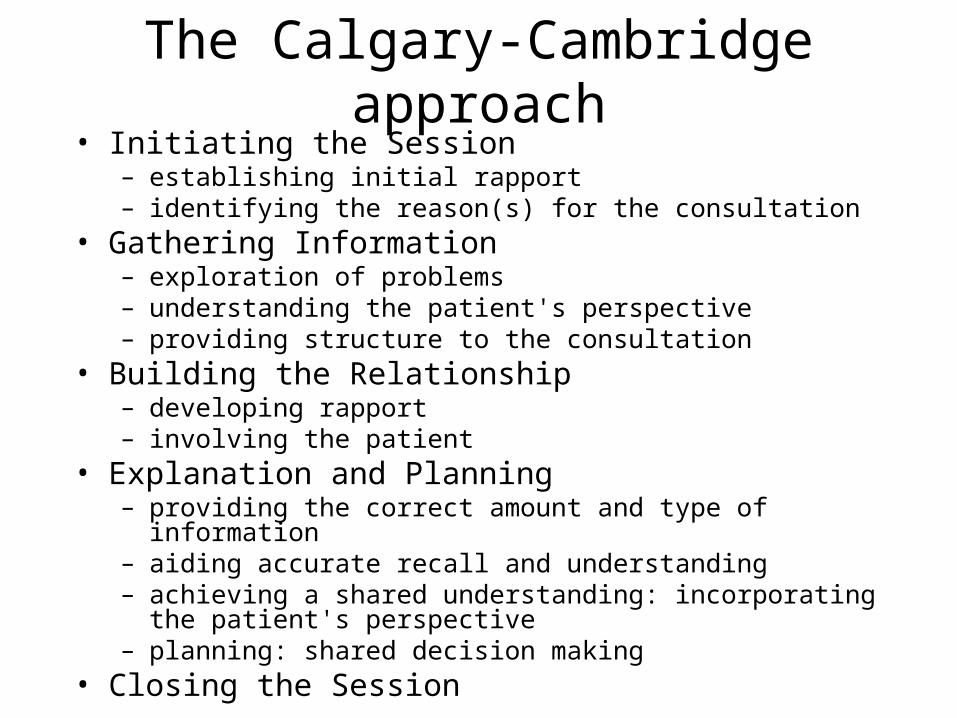
The Calgary-Cambridge approach• Initiating the Session
– establishing initial rapport – identifying the reason(s) for the consultation
• Gathering Information – exploration of problems – understanding the patient's perspective – providing structure to the consultation
• Building the Relationship – developing rapport – involving the patient
• Explanation and Planning – providing the correct amount and type of information – aiding accurate recall and understanding – achieving a shared understanding: incorporating the patient's
perspective – planning: shared decision making
• Closing the Session

ProvidingStructure
Initiating the Session
Closing the Session
Physical Examination
Explanation and planning
Gathering information
Building the relationship

Providing
Structure
Initiating the Session
preparation
establishing initial rapport
identifying the reason(s) for the consultation
providing the correct amount and type of information
aiding accurate recall and understanding
achieving a shared understanding: incorporating the patient’sillness framework
planning: shared decision making
Closing the Session
Building therelationship
••
•
••
•
•
•
•
•
Gathering information
Physical examination
Explanation and planning
making organisation overt
attending to flow
• exploration of the patient’s problems to discover the:
biomedical perspective the patient’s perspective
background information - context
• ensuring appropriate point of closure• forward planning
using appropriate non-verbal behaviour
developing rapport
involving the patient
•
•

So what are your needs?
• Have a look at the Calgary Cambridge behavioural skills – which do you think you need to work on most?
• Discuss for a few minutes in pairs then we will collate on a flipchart

The group process• Volunteer describes any background information s/he had before the
consultation• One person volunteers to view the consultation from the patient’s
perspective• Video is shown as raw material for work – group notes issues and
time on tape• Volunteer defines what s/he wants to get out of the session (flagging
up good and exploring developmental) onto flipchart then group adds their agenda too
• Volunteer chooses what agenda item to go with first – review that portion of the tape– how could it be done differently?
• Roleplay with patient volunteer, group ideas, further roleplay (rehearsal)
• Summary of learning points

Good feedback centres on the fundamental rule of communication
that it is outcome based – therefore…
• What were you trying to achieve then,
• what were you aiming for,
• what did you try to do to get there,
• what could you have done differently to help you get there?

Rules for feedback
• “What I saw was…”– Descriptive– Specific– Non judgmental
• “What I might try is…”– Owning statements
• Non-judgmental • Specific • Directed towards
behaviour rather than personally
• Checked with the recipient • Outcome based • Problem solving In the
form of suggestions rather than prescriptive comments

The group process• Volunteer describes any background information s/he had before the
consultation• One person volunteers to view the consultation from the patient’s
perspective• Video is shown as raw material for work – group notes issues and
time on tape• Volunteer defines what s/he wants to get out of the session (flagging
up good and exploring developmental) onto flipchart then group adds their agenda too
• Volunteer chooses what agenda item to go with first – review that portion of the tape– how could it be done differently?
• Roleplay with patient volunteer, group ideas, further roleplay (rehearsal)
• Summary of learning points





























