Embed Size (px)
Citation preview

UTAH MEDICAID DUR REPORT NOVEMBER 2018
MACROLIDE ANTIBIOTICS Azithromycin (Zithromax including Tri-Pak and Z-Pak, Generic)
Clarithromycin (Generic) Erythromycin (Erythrocin, E.E.S., EryPed, Ery-Tab, Generic)
Drug Regimen Review Center Joanita Lake B.Pharm, MSc EBHC (Oxon), Research Assistant Professor Valerie Gonzales, Pharm.D., Clinical Pharmacist Elena Martinez Alonso, B.Pharm., MSc MTSI, Medical Writer Joanne LaFleur, Pharm.D., MSPH, Associate Professor Data support Jacob Crook, MStat
Acknowledgement We acknowledge, with thanks, Adam L. Hersh, MD, PhD, Pediatric Infectious Diseases, Department of Pediatrics, University of Utah, for his expertise and guidance.
University of Utah College of Pharmacy Copyright © 2018 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved

2
Contents Background ........................................................................................................................................................... 4
Methodology ......................................................................................................................................................... 5
Macrolide uses ...................................................................................................................................................... 5
Conditions that may require chronic or prophylactic antibiotic use or alternate care plans .......................... 5
Inappropriate antibiotic use ................................................................................................................................. 6
Macrolide resistance ............................................................................................................................................. 7
Select macrolide safety information ..................................................................................................................... 9
Evidence (Clinical Guidelines, FDA approval, Systematic Reviews, and expert opinion) ..................................... 9
Table 1. Tiered Classification of Diagnoses by Macrolide Treatment Recommendations and FDA approval 11
Table 2. Evidence used for classification of diagnoses into 3 tiers mapped against current evidence .......... 19
Cochrane Systematic Reviews .................................................................................................................... 25
Noted reasons why macrolides may be chosen in clinical practice .................................................................... 26
Utah Medicaid Utilization Data ........................................................................................................................... 27
A. Utah macrolide prescribing rates ............................................................................................................... 27
Table 3. Utah Medicaid macrolide prescribing rates compared to CDC rates for the United States ........ 27
B. Sick visits that resulted in macrolide prescribing ....................................................................................... 28
Table 4. Utah Medicaid macrolide ............................................................................................................. 28
C. Macrolide utilization: Number of claims and patients ............................................................................... 29
Table 5. All (FFS and ACO) UT Medicaid macrolide utilization .................................................................. 30
Table 6. FFS UT Medicaid macrolide utilization) ....................................................................................... 31
Table 7. ACO UT Medicaid macrolide utilization ....................................................................................... 32
D. Age and Sex of FFS patients that received macrolides .............................................................................. 33
E. Potential inappropriate macrolide prescribing ........................................................................................... 34
Table 8a. Number of macrolide prescriptions and patients by tiered classification ................................. 34
Table 8b. Number of macrolide agent prescriptions by tiered classification ............................................ 34
Table 9. Revised number of macrolide prescriptions and patients by tiered classification ...................... 35
Table 10a. Number of prescriptions and patients with a Cystic Fibrosis (CF) diagnosis code ................... 36
Table 10b. Type of macrolide used in patients with CF diagnosis code ..................................................... 36
Table 10c. Prescribers of macrolide prescriptions in patients with CF ...................................................... 36
Table 11a. Number of prescriptions and patients with an acne diagnosis code ....................................... 37
Table 11b. Type of macrolide used in patients with an acne diagnosis code ............................................ 37
Table 11c. Prescribers of macrolide prescriptions in patients with acne diagnosis codes submitted ....... 37
F. Prescribers of all macrolide prescriptions .................................................................................................. 37
Table 12a. Prescriber type .......................................................................................................................... 37
Table 12b. Prescriber specialty .................................................................................................................. 38
3
G. Prescribers of macrolides by tiered classification (recommended firstline, not firstline, unnecessary) ... 39
Table 13. Prescribers of macrolides by tiered classification ...................................................................... 40
Conclusions ......................................................................................................................................................... 42
Appendix 1 .......................................................................................................................................................... 43
Table 1. Tiered Classification of Diagnoses by Macrolide treatment recommendations (adapted from Sanchez et al.) with newly defined ICD10 definitions .................................................................................... 43
Appendix 2 – Diagnosis codes of FFS macrolides not after sick visit .................................................................. 47
Appendix 3 .......................................................................................................................................................... 51
References .......................................................................................................................................................... 52

4
Background Inappropriate antibiotic use (overuse and misuse) leads to antibiotic resistance which has been described by world health leaders as “nightmare bacteria” that pose “a catastrophic threat”. The mechanisms of bacterial resistance include “decreased penetration to or increased efflux from the target site; alteration of the target site; and inactivation of the antibiotic by a bacterial enzyme.”1-3 In addition, it is important to avoid unnecessary antibiotic use because antibiotics cause disruption of the gut microbiome (intestinal flora); contribute to overgrowth infections such as Clostridium difficile infections (C.difficile) or vaginal yeast infections; and they are responsible for adverse drug events.4 The effect on the intestinal flora may also cause an imbalance in the immune system, resulting in immune dysregulation and inflammation.5-7 Recent studies have indicated a possible association between antibiotic exposure and chronic diseases including inflammatory bowel disease, obesity, and juvenile idiopathic arthritis (JIA).5,8-11 Antibiotic resistance is a growing global problem attributed to overuse and misuse of antibiotics and it is associated with significant morbidity and mortality.5,12 In 2013, the Centers for Disease Control and Prevention (CDC) reported at least 2 million annual patient cases of antibiotic resistant infections in the United States (U.S.) with at least 23,000 directly related deaths. They report that these estimates are based on conservative assumptions (underestimate) and that actual numbers are certainly higher. In addition, they report that “Many more people die from other conditions that were complicated by an antibiotic-resistant infection.” About 250,000 people are hospitalized annually because of C.difficile infections and about 14,000 patients die as a result of these infections. One out of five emergency department (ED) visits for adverse drug events are attributed to antibiotics. Antibiotics are the most common cause of adverse event related ED visits in children under 18 years old.4 The 2013 CDC report states that “…up to 50% of antibiotic prescribing is not needed or not optimally effective as prescribed.”4 Improving antibiotic prescribing/stewardship is core in preventing antibiotic resistance. Antibiotic stewardship is described as a “commitment to always use antibiotics appropriately and safely—only when they are needed to treat disease, and to choose the right antibiotics and to administer them in the right way in every case.”4 The 2017 CDC report on “Antibiotic use in the United States Progress and Opportunities” states that the numbers of antibiotic prescriptions given to children and adults remain high across the U.S.13 Medicaid-insured children are particularly more vulnerable to inappropriate antibiotic use. A recent study found that misconceptions about antibiotics are more prevalent among parents of Medicaid-insured children.14 Macrolides inhibits RNA-dependent protein synthesis by binding to the 50S ribosomal subunit, causing blockage of transpeptidation at the chain elongation step.15,16 They have moderately broad spectrum of activity (most gram-positive, some gram-negative, and Mycoplasma spp.,Chlamydia spp. and Legionella spp).17 Azithromycin and clarithromycin are newer derivatives of erythromycin and have a broader spectrum of antibacterial activity than erythromycin (enhanced gram-negative activity).15 Macrolides are commonly prescribed worldwide for a variety of infections and, because of their anti-inflammatory and immunomodulatory activity (reducing interleukin-8 and tumor necrosis factor-alpha), are also used in the treatment of some chronic conditions.15,17 “Macrolides are frequently the drug of choice in patients allergic to penicillin.”17 In the United States, macrolides and penicillins were the most commonly prescribed outpatient antibiotic classes prescribed during 2010, and azithromycin was the most frequently prescribed antibiotic.17,18 It is particularly important to specifically look at pneumonia because it remains a common, serious, and costly infection.19 The purpose of this review is to present utilization data of macrolide antibiotics in Utah Medicaid patients and to identify potential misuse or overuse. This report will focus on basic principles of antibiotic stewardship and Utah Medicaid drug utilization data to help identify inappropriate use. This information can be used to

5
help identify interventions to ensure appropriate antibiotic use in this population. This is not intended to be a drug class review. This report does not include fidaxomicin which is indicated in the treatment of Clostridium difficile infection (CDI).20
Methodology The Centers for Disease Control and prevention (CDC), Agency for Healthcare Research and Quality (AHRQ), the FDA website, Micromedex, Lexicomp, UpToDate, University of Utah Health website,21 Intermountain Healthcare website,22 Cochrane Library and Pubmed were searched for specific information to help inform the drug utilization extraction and presentation of data to assist the DUR Board with decisions about antibiotic prescribing and stewardship. Local experts were contacted as well. Methods for Utah Medicaid antibiotic utilization data extracted have been described in the Utah Medicaid Utilization Data section. Data is included in this report for oral antibiotics with utilization data.
Macrolide uses Macrolides are used for a variety of infections as shown below, but use is only appropriate when the antibiotic is employed according to the sequence (i.e., first-line, second-line, etc.) specified in treatment guidelines for the respective indication. Examples of inappropriate antibiotic use is covered in the ‘Inappropriate antibiotic use’ section and appropriate versus inappropriate use of macrolides is covered in the ‘Evidence’ section. In general, common uses (not necessarily appropriate) found in the literature include community-acquired respiratory tract infections (acute upper and lower), skin and soft tissue infections, Helicobacter pylori (H. pylori) eradication, some chronic conditions such as cystic fibrosis or acne, and various miscellaneous conditions including gastroparesis, trachoma, typhoid fever, and prevention of Mycobacterium avium complex infection in patients with HIV infection (primarily clarithromycin and azithromycin)15,17
Conditions that may require chronic or prophylactic antibiotic use or alternate care plans
A. Sickle cell disease (SCD) These patients are highly susceptible to infections (damaged spleen) including Streptococcus pneumonia (30-100 times higher rates of infection), and meningitis, pneumonia, and sepsis which are major causes of death in these children. Guidelines recommend daily prophylactic penicillin as soon as possible until they are 5 years old (the highest rate of infection occurs in those under 3 years old).23
B. Cystic Fibrosis Cystic fibrosis (CF) is a complex genetic disease characterized by thick viscous secretions leading to recurrent lung infections, bronchiectasis, and progressive deterioration in lung function.24 Patients may experience frequent lung infections including pneumonia and bronchitis (most commonly caused by Pseudomonas aeruginosa or Staphylococcus aureus). Patients with CF receive various treatments to manage the disease on a daily basis. This includes antibiotics, chronic use of inhaled tobramycin or inhaled aztreonam or chronic use of azithromycin (please refer to guidelines for specific recommendations).25-27 Mortality is typically (85%) attributable to lung disease.26
C. Acne Patients with moderate to severe inflammatory acne or those resistant to topical treatment may be receiving oral antibiotics to inhibit the growth of C. acnes. Tetracycline has anti-inflammatory action.

6
Erythromycin has less anti-inflammatory action and is recommended only if tetracyclines are contraindicated, because C. acnes often develops resistance to erythromycin. Nonetheless, patients often experience intolerable gastrointestinal (GI) effects with erythromycin. Azithromycin may be used, but concerns about resistance limit its use. Other antibiotics used in the treatment of acne include trimethoprim-sulfamethoxazole, clindamycin, and cephalexin, but their routine use is discouraged. Oral antibiotics should be used for the shortest duration possible (ideally three to four months; avoid use as maintenance therapy) to limit the emergence of antibiotic resistance, and it should not be used as monotherapy. Antibiotics should be used in combination with a topical retinoid to facilitate discontinuation of the antibiotic.28,29 According to experts “No consensus exists regarding whether oral antibiotics should be tapered or abruptly stopped,” and patients on long courses should be closely monitored “that antibiotic therapy is given for the shortest duration necessary.”28,30
D. Cancer Patients receiving cancer chemotherapy31
E. Chronic (> 30 days) “high dose” corticosteroids31 F. Transplants
Patients that have received solid organ, bone marrow or stem cell transplants31
G. Immunodeficiency Patients with immunodeficiency (congenital or acquired) or HIV infected (with CD4 count < 350/mm3)31
Inappropriate antibiotic use The 2017 CDC report on “Antibiotic use in the United States Progress and Opportunities” states that “Numerous studies have found that antibiotics are being prescribed for illnesses which do not require antibiotics, and the incorrect type of antibiotic, dose, or duration are often prescribed across all healthcare settings.”13 Inappropriate antibiotic use includes any treatment outside guideline recommendations such as the following: A. Viral infections or other infections for which antibiotics are not indicated
Many common infections are viral infections and should not be treated with antibiotics including colds, flu, most sore throats/viral pharyngitis, most coughs and bronchitis, many sinus infections, many ear infections, and asymptomatic urinary tract infection.12 One of the reasons for the increase in macrolide resistance in Utah is thought to be related to Z-Pak (azithromycin) prescribing for chest colds and sinus infections.19
B. “Conditions which antibiotics might be indicated but are over diagnosed, such as a condition that is diagnosed without fulfilling diagnostic criteria”32 A strep test (group A Streptococcus) is required before prescribing antibiotics for pharyngitis. Diagnosis of pneumonia requires a chest radiograph or CT and clinical features, but Nathan C. Dean, MD, Section Chief of Pulmonary and Critical Care Medicine Intermountain Medical Center and LDS Hospital, reports that according to 2014 Utah Instacare data, 40% of patients diagnosed and treated for pneumonia did not

7
have chest radiography.31 According to a presentation by Dr. Dean, absence of infiltrates rules out community-acquired pneumonia (CAP) in most cases and antibiotics are not indicated in the treatment of acute bronchitis.31
C. Wrong/inappropriate antibiotic (class/agent) D. Use of a broader-spectrum antibiotic than recommended
Using the narrowest spectrum agent that is active against the targeted pathogens is recommended.12 E. Inappropriate dose or duration
Note that historically it was recommended that patients should complete the entire course of antibiotics to prevent relapse and limit antibiotic resistance. This was emphasized regardless of symptoms whereas more experts are currently saying “shorter is better.” The rationale is that “Longer courses are actually MORE likely to lead to resistance...partly by increasing our normal flora's exposure to antibiotics. Plus shorter courses often work as well for many infections.” The Pharmacist’s Letter states individualized considerations are necessary for each patient including the type and severity of the infection and the antibiotic choice. They also recommend to “discourage the idea of using longer courses ‘just in case’." However, strep throat is highlighted as an exception where the full course of antibiotics (10-day course of penicillin or amoxicillin) is needed to “eradicate the bug...and possibly prevent rheumatic fever.”33 Examples of infections where shorter courses of antibiotics may be given to children include the following:
Many uncomplicated skin or kidney infections: 5 days of antibiotics can be given instead of 10 to 14 days33
Community-acquired pneumonia: “…it's usually okay to stop antibiotics after just 5 days if the patient hasn't had a fever for 2 to 3 days and is otherwise stable.”33
Bladder infections in most school-age kids without a fever: “2 to 4 days is often all that's needed to treat...instead of the traditional 7 to 14 days.”33
F. Prolonged use without supporting guideline/evidence of benefit
Antibiotic-associated adverse effects are common and prolonged use increases the risk of an adverse drug event.34,35
Inappropriate antibiotic prescribing in specific settings According to a 2017 CDC report, inappropriate prescribing mainly occurs with acute respiratory infections in outpatient settings, whereas in nursing homes and hospitals inappropriate prescribing is common with urinary tract infections and pneumonia. They also highlight that thousands of patients may die due to C.difficile infections caused by antibiotic overuse.13 More inappropriate antibiotic prescribing may also be seen in emergency departments because clinicians have to make rapid decisions with limited diagnostic information. UpToDate mentions the key role that pharmacists can play in ensuring appropriate prescribing in this setting is by assisting the clinician with decisions about appropriate antibiotic choice and dosing, guideline development, and ensuring that patients received adequate follow-up and verification of microbiology data.32
Macrolide resistance
Macrolide resistance is a growing problem and macrolides may not always be effective in treating common infections such as community-acquired pneumonia.17

8
There is cross-resistance between erythromycin, azithromycin, and clarithromycin for gram-positive organisms. Erythromycin-resistant gram-negative organisms may be sensitive to azithromycin or clarithromycin because of the enhanced gram-negative activity.15 Treponema pallidum (T. pallidum) Syphilis macrolide resistance Azithromycin is a second-line alternative to penicillin for the treatment of syphilis, but resistant strains have emerged that could result in treatment failure.15 Alternative second-line agents (tetracyclines or ceftriaxone) are preferred due to this reason.36 Azithromycin should only be considered if no other options are available.36 University of Utah Health The University of Utah Health website was searched for information on local macrolide resistance. No information was found apart from a paper on “Variation in Outpatient Antibiotic Prescribing for Acute Respiratory Infections in the Veteran Population” in which researchers found variations in antibiotic prescribing where “10 percent of health care providers write an antibiotic prescription for nearly every patient (95 percent or more) who walks in with a cold, bronchitis or other acute respiratory infection (ARI).” There were variations in the middle and “At the low end, 10 percent of providers prescribe antibiotics during 40 percent or fewer patient visits.”37 The variation appeared to be mainly due to habits of providers. They also found a 10 percent increase in the proportion of broad-spectrum antibiotics (macrolides) prescribed even though it is not recommended first line for most respiratory infections (data of 130 VA medical centers (VAMCs) across the U.S. from 2005 – 2012).37 As suggested by this study, understanding and improving provider decision-making is an important step going forward and may be what we is needed to help address macrolide overuse in the Utah Medicaid population. The researchers state that “We’d like to use this research to start a conversation among providers and patients about antibiotic prescribing for ARIs, and share the approaches of providers who are prescribing antibiotics less frequently with those who may be prescribing too often.” and this may be a good strategy in general going forward.37,38 Intermountain A search was conducted on the Intermountain website for macrolide resistance information. A document entitled “Diagnosis and management of Community-Acquired Pneumonia (CAP) June 2016 Update” was identified, which is a care process model (CPM) intended for immunocompetent patients ≥ 18 years. The CPM is maintained by Intermountain Healthcare’s Lower Respiratory Tract Infection Team, a subgroup of the Intensive Medicine Clinical Program.19 The authors state that recommendations are based on recent local susceptibility data and practice patterns, along with the most recent consensus guidelines of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS).19 According to this document, pneumonia accounts for more than 1% of adults seen in Intermountain emergency departments (EDs), and 60% of these patients are admitted to the hospital.19 The authors report that increased macrolide resistance appeared in 2013 and 2014.
“Macrolide resistance (azithromycin, erythromycin, and clarithromycin) among Streptococcus pneumoniae isolates has increased at all Utah Intermountain hospital microbiology labs. Resistance has increased among respiratory pneumococcal isolates to 60% in northern Utah and 32% in St. George. Among blood isolates from adults, resistance is now 15% to 35% in northern Utah and 21% in St. George.”19
The reason for the increase in macrolide resistance is thought to be related to Z-Pak (azithromycin) prescribing for chest colds and sinus infections and possibly under-vaccination with PCV13 (Prevnar) in children.19 “Children vaccinated with PCV13 have greatly reduced carriage of most multi-drug-resistant pneumococcal strains. Pneumococcus remains the most common and deadly bacteria that causes pneumonia.”19 In a separate presentation, Nathan C. Dean, MD, Section Chief of Pulmonary and Critical Care

9
Medicine Intermountain Medical Center and LDS Hospital, reports that “despite considerable clinician and public education, about 70% of adults with acute bronchitis get antibiotics – usually a Z-Pak” and that “Multiple randomized trials show no benefit from antibiotics.”31 The authors include a section called “What antibiotics provide coverage?’. “Pneumococcal activity remains very high for ceftriaxone and amoxicillin. (Clavulanate in Augmentin contributes nothing against streptococci.) Azithromycin remains effective for treatment of other pathogens that cause pneumonia, such as Mycoplasma, Chlamydia, Haemophilus influenzae, and Moraxella.” In the presentation, Dr. Dean states for pneumococcal resistance, ceftriaxone, ampicillin/amoxicillin, and levofloxacin or moxifloxacin remain highly active. It is also important to note that they recommend “Quinolones should NOT be used as first-line therapy due to documented immune-modulating effects of macrolides and lower mortality with combined therapy versus quinolone monotherapy in sicker patients. Overuse of quinolones has led to increased resistance. If a quinolone is used, the recommended dose of levofloxacin (Levaquin) remains at 750 mg for 5 days; adjust subsequent doses if creatinine clearance less than 30. Longer courses increase cost, drive resistance, and increase the likelihood of secondary C. difficile.”19 A tool called DRIP scoring is used to identify patients with pneumonia at risk for infection with MRSA, Pseudomonas, and other bacteria resistant to usual community-acquired pneumonia (CAP) therapy.19 A table is provided with scores for risk factors (Major=2 points: antibiotic use <60 days, long-term care resident, tube feeding, prior drug-resistant pneumonia [1 year] OR Minor=1 point: Hospitalization < 60 days, chronic pulmonary disease, poor functional status, gastric acid suppression, wound care, MRSA colonization [1 year]) and if a patient has a score ≥ 4 indicates they are considered at increased risk of drug-resistant pneumonia in which case it is recommended to consider using an antipseudomonal betalactam (cefepime or piperacillin-tazobactam) plus a macrolide (azithromycin), and an antiMRSA agent (vancomycin or linezolid).19
Select macrolide safety information
The macrolide antibiotics have been associated with gastrointestinal side effects, hepatotoxicity, and cardiovascular events including QT prolongation.15
Azithromycin is generally better tolerated than clarithromycin and erythromycin.15
Many of the drug-interactions involving erythromycin and clarithromycin are related to inhibition of hepatic cytochrome CYP (P450) 3A enzymes. Fewer hepatic enzyme- related drug interactions are reported for azithromycin, because it does not appear to affect hepatic enzymes significantly.15
Evidence (Clinical Guidelines, FDA approval, Systematic Reviews, and expert opinion)
Sanchez et al. studied outpatient macrolide antibiotic prescribing in the United States, 2008-2011.39 The authors classified diagnoses by macrolide treatment recommendations into three mutually exclusive categories (1) Macrolide first-line, (2) Macrolide not first-line, and (3) Antibiotics unnecessary or antibiotic indications are unclear (eg, acute bronchitis).39 The classification can be seen in the first and second columns of table 1 below. The guidance that they based this on have been included in table 2 (first column). They have used the 2012 Johns Hopkins Antibiotic guide40 for conditions where guidance was lacking.

10
We first (1) reviewed whether the diagnoses are FDA approved or not which is indicated in the last three columns of table 1, then (2) identified and reviewed current guidelines, (3) mapped the evidence against the Sanchez et al. supportive evidence for the tiered classification in table 2 (second column), and finally (4) indicated in table 1 below (third column) whether the classification is still appropriate based on current evidence. The classification by Sanchez et al39 were done by experts in the field. Any evidence findings suggesting a different classification were therefore carefully considered and experts in the field were contacted i.e. for Cystic Fibrosis. Their expert opinions were included after the evidence in table 2 (column 3).

Table 1. Tiered Classification of Diagnoses by Macrolide Treatment Recommendations and FDA approval
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
Macrolides first-line [1, 3–10]
Pneumonia (including atypical pneumonia)
Macrolide is recommended if previously healthy and no risk factors for drug-resistant S. pneumoniae infection.46 “For children older than 3 months suspected or known to have atypical CAP, erythromycin is an acceptable alternative to the preferred macrolide (azithromycin) in outpatient and inpatient settings.”42
Yes, CAP due to Chlamydophila pneumoniae, H. influenzae, Legionella pneumophila, Moraxella catarrhalis, Mycoplasma pneumoniae, or S. pneumoniae
Yes, CAP due to susceptible Mycoplasma pneumoniae, S. pneumoniae, or Chlamydophila pneumoniae (adult and pediatric patients) and H. influenzae, H. parainfluenzae, or M. catarrhalis (adults).
Respiratory tract infections Some S. pneumoniae, some S. aureus, M. pneumoniae, Legionella pneumophila, Off-label in CAP in children
Nontuberculosis mycobacteria disease
Azithromycin (in combination with other antimicrobials) is recommended for Mycobacterium abscessus pulmonary, skin, soft tissue, and bone infection.47
Yes for Mycobacterium avium complex (MAC): Prevention and treatment in patients with advanced HIV infection No for Mycobacterium abscessus infection (off-label use)
Yes for Mycobacterium avium complex (MAC): Prevention and treatment in patients with advanced HIV infection
Not stated
Pertussis Recommended (azithromycin, clarithromycin)48
No (off-label use) No (off-label use) Yes
Cat scratch disease (Bartonella) Cutaneous bacillary angiomatosis (not in Sanchez et al. classification)
Recommended (azithromycin49; clarithromycin alternative50) Erythromycin is recommended for treatment of bacillary angiomatosis, peliosis hepatis, bacteremia, osteomyelitis, and other severe infections (excluding CNS infections or endocarditis) due to Bartonella in adolescent and adult HIV-infected patients.42 Erythromycin may be considered (appears effective but it has not been systematically examined and based on limited data and expert experience)49
No (off-label use) No (off-label use) No (off-label use)

12
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
Cervicitis and endocervicitis, urethritis, and other gonococcal or chlamydia infection
Recommended (azithromycin)51,52 Refer to 2015 Centers for Disease Control and Prevention (CDC) sexually transmitted diseases treatment guidelines51,52 section below for infection and combination with other antibiotic details.
Yes, cervicitis and urethritis due to C. trachomatis or N. gonorrhoeae
No (off-label use) Chlamydia, N. gonorrhoeae, syphilis and nongonococcal urethritis
Chancroid (H. ducreyi) Azithromycin is recommended51,52 Erythromycin (base) is effective and recommended for the treatment of chancroid due to H. ducreyi (consider resistance when initiating therapy; intermediate resistance to erythromycin has been reported in several isolates)42
Yes, genital ulcer disease (in men) due to Haemophilus ducreyi
No (off-label use) No (off-label use)
Granuloma inguinale, and other sexually transmitted infections
Azithromycin is recommended, and erythromycin (base) is effective and recommended when azithromycin is not appropriate.51,52
No (off-label use) No (off-label use) No (off-label use)
Babesiosis Recommended (azithromycin in combination with atovaquone)53
No (off-label use) No (off-label use) Not stated
Infectious diarrhea/traveler’s diarrhea, Shigellosis
Traveler’s diarrhea: Azithromycin may be firstline54-56 (due to increased levels of resistance to fluoroquinolones), especially in regions with a high prevalence of Campylobacter (eg, Southeast Asia, India) or in geographical areas with suspected Campylobacter resistance or enterotoxigenic Escherichia coli.16
No (off-label use) No (off-label use) E. histolytica (causing Amebiasis) Off-label: Enteric campylobacteriosis Listeriosis

13
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
Shigellosis: Azithromycin as alternative to ciprofloxacin, but limited data54
Peptic ulcer disease, H. pylori infection Requested resistance information for UT from local experts. No further information available at this stage.
“therapy must be chosen empirically based on regional bacterial resistance patterns, local recommendations, and drug availability.” Standard triple therapy is preferred firstline and considered a reasonable initial therapy where clarithromycin resistance is low. Standard triple therapy: PPI, amoxicillin 1 g, and clarithromycin 500 mg (Biaxin) twice daily OR PPI, clarithromycin 500 mg, and metronidazole 500 mg (Flagyl) twice daily)
No (off-label use) Yes, component of triple therapy for eradication of Helicobacter pylori to reduce the risk of duodenal ulcer recurrence in adults with H. pylori infection and duodenal ulcer disease (active or 5 year history of duodenal ulcer). Not for use as single antibacterial agent as it increases the risk of clarithromycin resistance.
Campylobacter gastroenteritis; used in conjunction with neomycin for decontaminating the bowel
Chronic obstructive pulmonary disease exacerbation
Recommended (azithromycin)57 Yes, acute bacterial exacerbations of chronic obstructive pulmonary disease (COPD) due to Haemophilus influenzae, Moraxella catarrhalis, or Streptococcus pneumoniae
No (off-label use) Not stated
Macrolides not first-line [2-4, 11-16]
Cystic Fibrosis
The Sanchez et al. classification does not specifically list cystic fibrosis in this category, but reference a Cochrane review (Southern et al58 2012 [11 of Sanchez et al] about macrolide antibiotics for cystic fibrosis in this category. The same review was identified in the systematic review section of this report. This SR included 5 azithromycin studies. The authors
No (off-label use) Dosing information is included in Lexicomp for “Cystic fibrosis, anti-inflammatory (off-label use)” Evidence is based on 3 double-blind RCTs60-62 “Note: Patients should be screened for nontuberculous mycobacterial infection prior to
No (off-label use) No (off-label use)
14
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
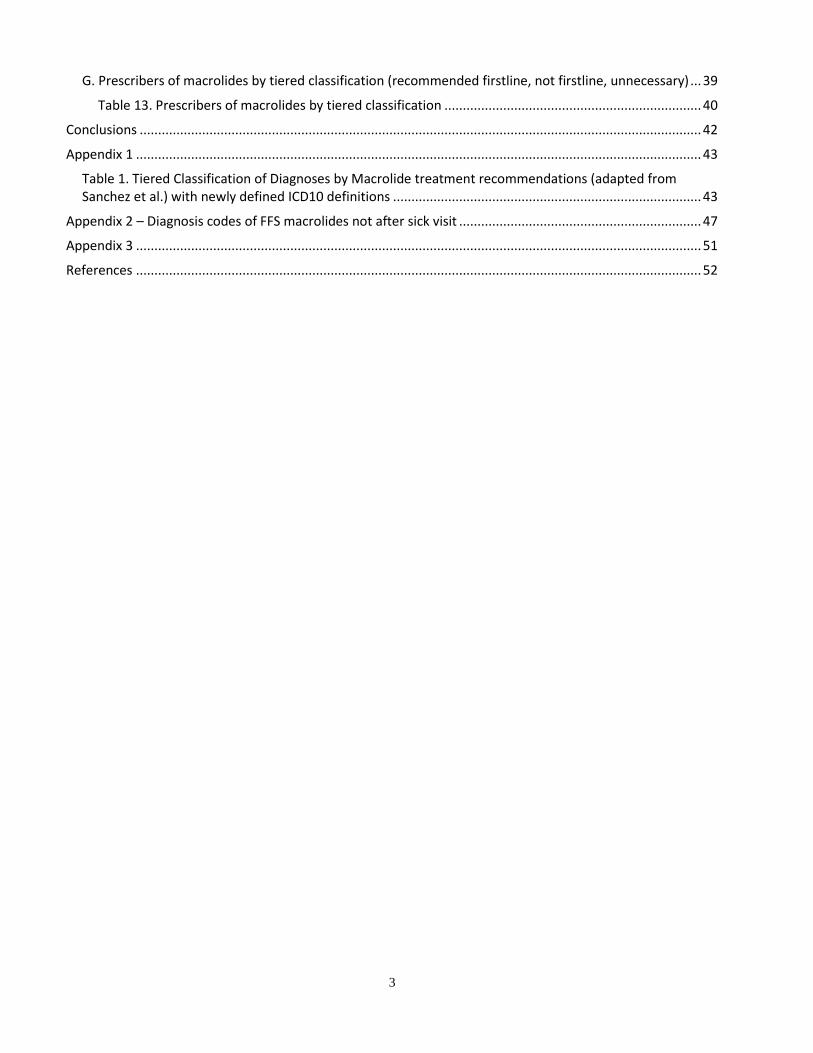
reported evidence of improved respiratory function after six months of azithromycin. Data on longer use was unclear, but they did find that reduction in pulmonary exacerbation was sustained. Due to the emergence of macrolide resistance, they suggest that there is a need for a multi-center trial examining long-term effects.58 The 2013 Cystic Fibrosis Pulmonary Guidelines Chronic Medications for Maintenance of Lung Health59 recommend azithromycin is an effective and recommended agent to improve lung function and reduce exacerbations According to a colleague, Professor Dave Young, who is an expert in Cystic Fibrosis “Chronic azithromycin is considered standard of care (first line) for CF patients with and w/o chronic pseudomonas for their anti-inflammatory benefits which leads to reduced exacerbations and improved lung function.”
treatment and azithromycin should not be given if present (Mogayzel 2013; Saiman 2003).”
Acne
Acne: Azithromycin and erythromycin may be considered for moderate and severe acne that are resistant to topical treatments in patients who cannot receive a tetracycline (ie, pregnant women or children <8 years of age) only for a course, then topical should be continued29
No (off-label use) No (off-label use) No (off-label use)

15
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
Pharyngitis, Strep throat, Scarlet fever (as a result of a group A streptococcus infection)
CDC pediatric recommendations63 for pharyngitis based on Hersh et al64, and Shulman et al65: Amoxicillin and penicillin V remain first-line therapy, and clarithromycin, or azithromycin amongst other options are recommended in those hypersensitive to penicillin.
Yes, pharyngitis/tonsillitis due to S. pyogenes as an alternative to first-line therapy
Yes, pharyngitis/tonsillitis due to susceptible Streptococcus pyogenes (alternative agent).
Yes S. pyogenes
Sinusitis Although included as an FDA-approved use in the clarithromycin manufacturer’s prescribing information, it is not recommended due to increased resistance in Streptococcus pneumoniae66 CDC pediatric recommendations63 based on Wald et al.67 and Chow et al.(IDSA)66: Amoxicillin or amoxicillin/clavulanate remain first-line therapy.63
Yes, acute bacterial sinusitis (adults).
Yes, acute maxillary sinusitis due to susceptible H. influenzae, S. pneumoniae, or M. catarrhalis
Not specifically stated
Acute otitis media Macrolides not recommended. CDC pediatric recommendations63 based on Lieberthal et al68, Hersh et al64, and Coker et al69: amoxicillin first-line; amoxicillin/clavulanate if amoxicillin has been taken within the past 30 days; non-type 1 hypersensitivity to penicillin: 2nd and 3rd generation cephalosporins like cefdinir, cefuroxime, or cefpodoxime. The American Academy of Pediatrics guidelines68: “Macrolides, such as erythromycin and azithromycin, have limited efficacy against both H influenza and S pneumoniae.”68
Yes, acute otitis due to H. influenzae, M. catarrhalis, or S. pneumoniae
Yes, acute otitis media in pediatric patients due to susceptible H. influenzae, M. catarrhalis, or S. pneumoniae.
Erythromycin Ethylsuccinate: Off-label Yes, fixed-combination preparation containing erythromycin ethylsuccinate and sulfisoxazole acetyl for AOM in children caused by susceptible Haemophilus influenza.

16
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
Pneumococcal surveillance studies indicated substantial resistance to erythromycin-sulfisoxazole and therefore not appropriate for patients that fail to improve on amoxicillin.
Urinary tract infections CDC pediatric recommendations63 based on White70 and UTI guidance71: “Initial antibiotic treatment should be based on local antimicrobial susceptibility patterns. Suggested agents include TMP/SMX, amoxicillin/clavulanate, cefixime, cefpodoxime, cefprozil, or cephalexin in children 2-24 months.”
No (off-label use) No (off-label use) Nongonococcal urethritis (adults)
Gastrointestinal infections (excluding Shigellosis)
No (off-label use) No (off-label use) Infection due to Entamoeba histolytica - Intestinal infectious disease Listeriosis
Pelvic inflammatory disease
“Although included as an FDA-approved use in the manufacturer’s prescribing information as an indication for IV azithromycin, the medication has largely been studied in patients with mild PID (Bevan 2003; Savaris 2007) and is not listed as an alternative parenteral regimen in the CDC guidelines”16,51 2017 Cochrane SR (Savaris et al72): no conclusive evidence that one regimen of antibiotics was safer or more effective than any other; one study which they rated as moderate-quality at low risk of bias, “suggested that a macrolide
No (off-label use) No (off-label use) Female gonococcal pelvic inflammatory disease

17
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
(azithromycin) may be more effective than a tetracycline (doxycycline) for curing mild-moderate PID.”72
Skin and mucosal infections
Cutaneous bacillary angiomatosis: Erythromycin may be considered, because it appears effective but it has not been systematically examined and based on limited data and expert experience.49
Yes, uncomplicated skin and skin structure infections due to Staphylococcus aureus, Streptococcus pyogenes, or Streptococcus agalactiae
Yes, uncomplicated skin/skin structure infection due to susceptible Staphylococcus aureus or S. pyogenes
Yes Impetigo Erythrasma (long-term skin infection caused by Corynebacterium minutissimum73) Infection of skin AND/OR subcutaneous tissue (Mild to Moderate), Caused by S. pyogenes or S. aureus
Other miscellaneous bacterial infections (eg, syphilis, tuberculosis, Lyme disease)
Primary and secondary syphilis: Azithromycin is a recommended alternative for patients who are unable to receive penicillin or doxycycline (should be used with caution and should not be used to treat syphilis in patients with HIV, pregnant women, or in the MSM population).51,52 Lyme disease: Azithromycin and clarithromycin are recommended as alternatives.53 Prophylaxis of infective endocarditis: Clarithromycin is a recommended alternative in patients with certain cardiac conditions who are allergic to penicillins or ampicillin and undergoing dental or respiratory tract procedures.74
No (off-label use) Lyme disease: No (off-label) Primary syphilis, In penicillin allergic patients Off-label: Lyme disease
Antibiotics unnecessary [1, 3, 16–20]
All other conditions, including allergic rhinitis, asthma, acute bronchitis and bronchiolitis, influenza, nonsuppurative otitis
CDC pediatric recommendations63 based on Hersh et al64 and Fashner et al75: “Management of the common cold, nonspecific URI, and acute cough illness should focus on symptomatic relief. Antibiotics
Acute bacterial exacerbation of chronic bronchitis (adults) Others No (off-label use)
Yes, acute bacterial exacerbation of chronic bronchitis in adults due to susceptible Haemophilus influenzae, H. parainfluenzae, Moraxella catarrhalis, or Streptococcus pneumoniae.
Not stated

18
Category Assigned Diagnoses Updated guidance Azithromycin FDA approved16 Clarithromycin FDA approved41 Erythromycin FDA approved42-45*
media, and viral upper respiratory infection
should not be prescribed for these conditions.” Based on Ralston et al76: Antibiotics are not helpful for the treatment of bronchiolitis and should not be used.
Others, No (off-label use)
* Lexicomp states (erythromycin): Bacterial infections: Treatment of susceptible bacterial infections, including S. pyogenes, some S. pneumoniae, some S. aureus, M. pneumoniae, Legionella pneumophila, diphtheria, pertussis, Chlamydia, erythrasma, N. gonorrhoeae, E. histolytica, syphilis and nongonococcal urethritis, and Campylobacter gastroenteritis; used in conjunction with neomycin for decontaminating the bowel. These were matched to categories above based on knowledge and experience.
19
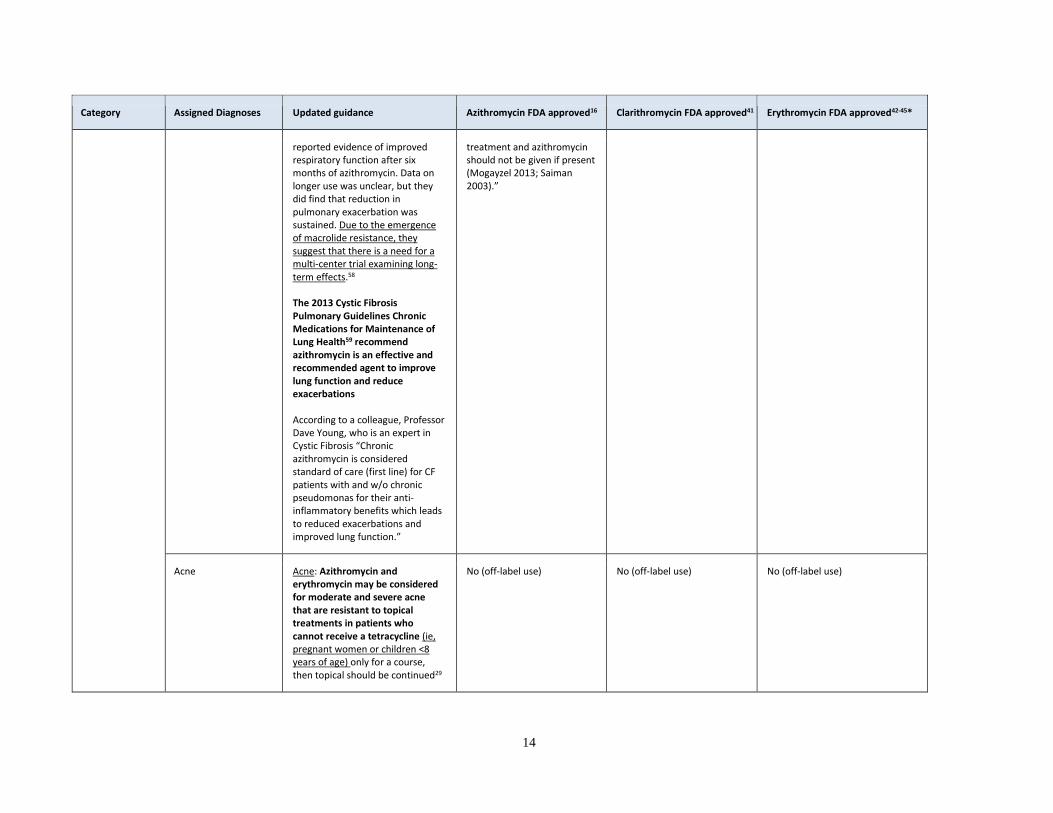
Table 2. Evidence used by Sanchez et al for classification of diagnoses into 3 tiers39 mapped against current evidence
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
1. Irwin RS. Introduction to the diagnosis and management of cough: ACCP evidence-based clinical practice guidelines. Chest 2006; 129(1 Suppl):25S–7S.
Laopaiboon et al. 2015 Cochrane SR: Acute lower respiratory tract infections “ranging from acute bronchitis and acute exacerbations of chronic bronchitis to pneumonia”77; small studies with unclear methodological quality. This evidence indicate that “In patients with acute bronchitis of a suspected bacterial cause, azithromycin tends to be more effective in terms of lower incidence of treatment failure and adverse events than amoxycillin or amoxyclav.”77
2. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis 2012; 55(10):1279–82.
Covered below
3. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015; 64(Rr-03):1–137.
Covered below
Macrolides Firstline
4. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med 2007; 175(4):367–416.
2007 American Thoracic Society (ATS) and IDSA Guideline for the Diagnosis, Treatment, and Prevention of Nontuberculosis Mycobacterial Disease47 British Thoracic Society (BTS) Guidelines for the Management of Non-Tuberculous Mycobacterial Pulmonary Disease US Cystic Fibrosis (CF) Foundation and European CF Society Consensus Recommendations for the Management of Nontuberculous Mycobacteria in Individuals with Cystic Fibrosis Mycobacterium abscessus pulmonary, skin, soft tissue, and bone infection: Azithromycin (in combination with other antimicrobials) is effective and recommended
5. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007; 44(suppl 2):S27–72.46
2007 Consensus Guideline on Management of Community-Acquired Pneumonia in Adults (Mandell et al46) Outpatient treatment (pneumonia): “Previously healthy and no risk factors for drug-resistant S. pneumoniae (DRSP) infection: A macrolide (azithromycin, clarithromycin, or erythromycin) (strong recommendation; level I evidence)”46
6. Bradley J, Byington C, Shah S, et al. The management of community-acquired pneumonia in infants and children older than 3 months of age: clinical practice guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. Clin Infect Dis 2011; 53(7):e25–76.
“For children older than 3 months suspected or known to have atypical CAP, erythromycin is an acceptable alternative to the preferred macrolide (azithromycin) in outpatient and inpatient settings.”42
7. Krause PJ, Lepore T, Sikand VK, et al. Atovaquone and azithromycin for the treatment of babesiosis. N Engl J Med 2000; 343(20):1454–8.
2006 Infectious Diseases Society of America (IDSA) guidelines for the clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis53 Babesiosis: Azithromycin is effective and recommended in combination with atovaquone
8. Global Strategy for the Diagnosis, Management, and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease (GOLD). 2017. http://www.goldcopd.org Accessed 13 June 2017).
2018 Global Initiative for Chronic Obstructive Lung Disease guidelines for the diagnosis, management, and prevention of chronic obstructive pulmonary disease57 Prevention of COPD exacerbations: azithromycin is effective and recommended Herath SC and Poole P, 2013 Cochrane SR: Some patients such as those with frequent exacerbations may benefit from continuous prophylactic macrolide antibiotics, but benefits to individual patients and harms including potential adverse effects and antibiotic resistance due to antibiotic overuse should be considered.78

20
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
9. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015; 64(Rr-03):1–137.51 Cervicitis and endocervicitis, urethritis, and other gonococcal or chlamydia infection Chancroid (H. ducreyi) Granuloma inguinale, and other sexually transmitted infections
2015 Centers for Disease Control and Prevention (CDC) sexually transmitted diseases treatment guidelines51,52 Chlamydia and Gonococcal: Chlamydia trachomatis infection of the cervix, urethra, or pharynx: Azithromycin is an effective and recommended agent Chlamydia in heterosexual partners of infected patients (if permitted by law): Azithromycin is an effective and recommended treatment Disseminated gonococcal infections including arthritis, arthritis-dermatitis syndrome, meningitis, and endocarditis: Azithromycin in combination with ceftriaxone is an effective and recommended treatment Gonorrhea in heterosexual partners of infected patients (if permitted by law): Azithromycin in combination with cefixime is an effective and recommended treatment Uncomplicated gonococcal infections of the rectum or pharynx, or conjunctivitis: Azithromycin in combination with ceftriaxone is an effective and recommended treatment Other sexually transmitted Prophylaxis against sexually transmitted infections following sexual assault in adolescents and adults: Azithromycin in combination with ceftriaxone (plus metronidazole or tinidazole) is a recommended regimen M. genitalium: Azithromycin is more effective and preferred over doxycycline (the extended 5-day regimen may be slightly more effective than single-dose therapy and be less likely to select for macrolide resistance of M. genitalium) Granuloma inguinale: Azithromycin is an effective and recommended agent, and erythromycin (base) if azithromycin is not appropriate. Chancroid: Azithromycin is an effective and recommended agent. Erythromycin (base) is effective and recommended for the treatment of chancroid due to H. ducreyi (consider resistance when initiating therapy; intermediate resistance to erythromycin has been reported in several isolates)42 Romero L, et al. 2017 Cochrane SR: Insufficient low quality evidence for macrolides in the treatment of H ducreyi infection. “Low quality evidence suggests that azithromycin could be considered as the first therapeutic alternative, based on their mono-dose oral administration, with a similar safety and effectiveness profile, when it is compared with long-term erythromycin use.”79 In their background section they explain the rationale of the CDC and other guideline development groups for recommending the use of mono-dose as first therapeutic alternative to treat sexually transmitted infections (STIs). It is effective and for adherence reasons. Macrolides are also suitable for pregnant or nursing women or patients who are allergic to cephalosporins.51,79,80
Pertussis listed in this tier, but no link to reference found. 2005 CDC guidelines: Recommended Antimicrobial Agents for the Treatment and Postexposure Prophylaxis of Pertussis48 Pertussis: Azithromycin and clarithromycin are effective and recommended.
Cat scratch disease listed in this tier, but no link to reference found in the section for macrolide first-line references (evidence). However, one reference is provided in another tier (maybe should have been included in the section stating evidence supporting multiple tiers):
2014 IDSA guidelines for the diagnosis and management of skin and soft tissue infections (SSTI) (Stevens et al49) Cat scratch disease: Azithromycin is an effective and recommended 2015 US Department of Health and Human Services (HHS) Guidelines for Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents41,50

21
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
10. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014; 59(2):e10–52.49
Treatment of or as long-term suppressive therapy of bartonellosis infection: Clarithromycin is an effective and recommended alternative agent in the management of this condition. Alternative Therapy for Bartonella Infections (Not for Endocarditis or CNS Infections): Azithromycin or clarithromycin Erythromycin is a recommended and effective agent for treatment of bacillary angiomatosis, peliosis hepatis, bacteremia, osteomyelitis, and other severe infections (excluding CNS infections or endocarditis) due to Bartonella in adolescent and adult HIV-infected patients.42
Infectious diarrhea/traveler’s diarrhea and Shigellosis listed in this tier, but no link to reference found.
2005 World Health Organization (WHO) guidelines for the control of shigellosis81 2017 IDSA Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea54 CDC Yellowbook55 2016 American College of Gastroenterology (ACG) Guideline for the Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults56 Shigellosis: Alternative to ciprofloxacin: Azithromycin (may be used to treat this condition although there is limited data on efficacy) Travelers' diarrhea (e.g. caused by : Azithromycin is effective and may be recommended firstline (due to increased levels of resistance to fluoroquinolones), especially in regions with a high prevalence of Campylobacter (eg, Southeast Asia, India) or in geographical areas with suspected Campylobacter resistance or enterotoxigenic Escherichia coli.16
Peptic ulcer disease and H. pylori listed in this tier. 2015 American Academy of Family Physicians (AAFP) Diagnosis and Treatment of Peptic Ulcer Disease and H. pylori Infection82 “therapy must be chosen empirically based on regional bacterial resistance patterns, local recommendations, and drug availability.” Standard triple therapy is preferred firstline and considered a reasonable initial therapy where clarithromycin resistance is low.82 Standard triple therapy: PPI, amoxicillin 1 g, and clarithromycin 500 mg (Biaxin) twice daily OR PPI, clarithromycin 500 mg, and metronidazole 500 mg (Flagyl) twice daily)82 Other treatment choices82
Sequential therapy (needs validation in US)
Quadruple therapy: PPI, amoxicillin 1 g, clarithromycin 500 mg, and tinidazole 500 mg or metronidazole 500 mg twice daily OR Bismuth subsalicylate 525 mg or subcitrate 300 mg, metronidazole 250 mg, and tetracycline 500 mg, four times daily; and PPI twice daily
Levofloxacin-based triple therapy (needs validation in US) Requested resistance information for UT from local experts. No further information available at this stage.
Not covered in tiered classification table by Sanchez et al. 2012 American College of Gastroenterology (ACG) guidelines for the management of gastroparesis83 Gastroparesis: Erythromycin is effective in improving gastric emptying and recommended (Strong recommendation, moderate level of evidence). “However, the long-term effectiveness of oral therapy is limited by tachyphylaxis.”83

22
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
Macrolides Not Firstline
Acne listed in this tier. 2016 American Academy of Dermatology guidelines of care for the management of acne vulgaris29 Acne: May be 1st line for moderate and severe acne and forms of inflammatory acne that are resistant to topical treatments: Azithromycin or erythromycin may be considered, but in combination with topical therapy (benzoyl peroxide or a retinoid). It should only be used in patients who cannot receive a tetracycline (ie, pregnant women or children <8 years of age) due to due to an increased risk of bacterial resistance. Topical therapy should be continued for maintenance after the antibiotic course is completed.
10. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014; 59(2):e10–52.49
2014 IDSA guidelines for the diagnosis and management of skin and soft tissue infections (SSTI) (Stevens et al49) Cutaneous bacillary angiomatosis: Erythromycin may be considered, because it appears effective but it has not been systematically examined and based on limited data and expert experience
11. Southern KW, Barker PM, Solis-Moya A, Patel L. Macrolide antibiotics for cystic fibrosis. Cochrane database Syst Rev 2012; 11:Cd002203.
2013 Cystic Fibrosis Pulmonary Guidelines Chronic Medications for Maintenance of Lung Health59 Cystic fibrosis: Azithromycin is an effective and recommended agent to improve lung function and reduce exacerbations The Southern et al58 2012 Cochrane SR [11 of Sanchez et al] was identified in the systematic review section of this report. The authors of this SR that includes 5 studies with low risk of bias (according to the authors), reported evidence of improved respiratory function after six months of azithromycin. Data on longer use was unclear, but they did find that reduction in pulmonary exacerbation was sustained. They also reported on some secondary outcomes that included some positive outcomes for azithromycin (“significant reduction in need for oral antibiotics and greater weight gain” and “reduced identification of Staphylococcus aureus on respiratory culture”), but some adverse events with the use of a higher once-weekly dose of azithromycin (gastrointestinal adverse events), and “a significant increase in macrolide resistance.” Due to the emergence of macrolide resistance, they suggest that there is a need for a multi-center trial examining long-term effects.43
12. Gupta K, Hooten TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the Infectious Diseases Society of America and the European Society for Microbiology and Infectious Diseases. Clin Infect Dis 2011; 52(5):e103–20.
CDC pediatric recommendations63 based on White70 and UTI guidance71: “Initial antibiotic treatment should be based on local antimicrobial susceptibility patterns. Suggested agents include TMP/SMX, amoxicillin/clavulanate, cefixime, cefpodoxime, cefprozil, or cephalexin in children 2-24 months.”
13. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics 2013; 131(3):e964–99.68
CDC pediatric recommendations63 based on Lieberthal et al68, Hersh et al64, and Coker et al69: amoxicillin first-line; amoxicillin/clavulanate if amoxicillin has been taken within the past 30 days; non-type 1 hypersensitivity to penicillin: 2nd and 3rd generation cephalosporins like cefdinir, cefuroxime, or cefpodoxime. The American Academy of Pediatrics guidelines (Lieberthal et al68): “Macrolides, such as erythromycin and azithromycin, have limited efficacy against both H influenza and S pneumoniae.”68 “Although trimethoprim-sulfamethoxazole and erythromycin-sulfisoxazole had been useful as therapy for patients with AOM, pneumococcal surveillance studies indicated that resistance to these 2 combination agents is substantial. Therefore, when patients fail to improve while receiving amoxicillin, neither trimethoprim-sulfamethoxazole nor erythromycin-sulfisoxazole is appropriate therapy.” Multiple antibiotics failure: The guidelines recommend that tympanocentesis should be

23
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
considered, and culture of middle ear fluid should be performed for bacteriologic diagnosis and susceptibility testing.68
14. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (updated): adult sinusitis. Otolaryngol Head Neck Surg 2015; 152(2 suppl):S1–39. 15. Chow AW, Benninger MS, Itzhak B, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis 2012; 54(8):e72–112.
“Although included as an FDA-approved use in the manufacturer’s prescribing information, given increased resistance in Streptococcus pneumoniae, azithromycin is not recommended for the treatment of bacterial sinusitis (AAO-HNS [Rosenfeld 2015]; IDSA [Chow 2012]).”16 CDC pediatric recommendations63 based on Wald et al.67 and Chow et al.(IDSA)66: Amoxicillin or amoxicillin/clavulanate remain first-line therapy.63 Authors of a 2016 Cochrane SR (Head et al84) found very little evidence that systemic antibiotics are effective in patients with chronic rhinosinusitis.84 Please refer to SR section for more information.
Other miscellaneous bacterial infections (eg, syphilis, tuberculosis, Lyme disease) FROM: Evidence Supporting Multiple Tiers 3. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep 2015; 64(Rr-03):1–137. Lyme disease and pelvic inflammatory disease listed in this tier.
2015 Centers for Disease Control and Prevention (CDC) sexually transmitted diseases treatment guidelines51,52 Chlamydia and Gonococcal: Conjunctivitis due to Chlamydia trachomatis in infants: Azithromycin is an effective and recommended alternative agent if erythromycin is not appropriate. Other sexually transmitted Primary and secondary syphilis: Azithromycin is a recommended alternative for patients who are unable to receive penicillin or doxycycline (should be used with caution and should not be used to treat syphilis in patients with HIV, pregnant women, or in the MSM population). 2006 Infectious Diseases Society of America (IDSA) guidelines for the clinical assessment, treatment, and prevention of Lyme disease, human granulocytic anaplasmosis, and babesiosis53 Lyme disease: Azithromycin is an effective and recommended alternative agent for the treatment of early localized or disseminated lyme disease (erythema migrans or borrelial lymphocytoma) in patients who are unable to take or who are intolerant of tetracyclines, penicillins, or cephalosporins. Clarithromycin is effective and recommended as an alternative in the management of this condition. 2007 American Heart Association (AHA) guidelines for the prevention of infective endocarditis74 Prophylaxis of infective endocarditis: Azithromycin and clarithromycin are effective and recommended alternative antibiotics for patients with certain cardiac conditions who are allergic to penicillins or ampicillin and undergoing dental or respiratory tract procedures. Pelvic inflammatory disease Authors of a 2017 Cochrane SR (Savaris et al72) found no conclusive evidence that one regimen of antibiotics was safer or more effective than any other for the cure of PID, and one study which they rated as moderate-quality at low risk of bias, “suggested that a macrolide (azithromycin) may be more effective than a tetracycline (doxycycline) for curing mild-moderate PID.”72
FROM: Evidence Supporting Multiple Tiers 2. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis 2012; 55(10):1279–82.65
CDC pediatric recommendations63 for pharyngitis based on Hersh et al64, and Shulman et al65: Amoxicillin and penicillin V remain first-line therapy, and clarithromycin, or azithromycin amongst other options are recommended in those hypersensitive to penicillin.

24
Evidence Supporting Multiple Tiers August 2018 Review of guidelines and Cochrane SRs
Not covered in tiered classification table by Sanchez et al. Perletti et al. 2013 Cochrane review on chronic bacterial prostatitis: Oral fluoroquinolones for the treatment of chronic bacterial prostatitis (traditional pathogens) appear compararable in terms of efficacy and safety, and no conclusive evidence was found for alternative agents (co-trimoxazole, beta-lactams and tetracyclines). Macrolides appeared to be more effective compared to fluoroquinolones in the treatment of CBP caused by obligate intracellular pathogens.85
Antibiotics Unnecessary
16. Gonzales R, Bartlett JG, Besser RE, et al. Principles of appropriate antibiotic use for treatment of uncomplicated acute bronchitis: background. Ann Intern Med 2001; 134(6):521–9. 17. Albert RH. Diagnosis and treatment of acute bronchitis. Am Fam Physician 2010; 82(11):1345–50. 18. Pratter MR. Cough and the common cold: ACCP evidence-based clinical practice guidelines. Chest 2006; 129(1 suppl):72S–4S. 19. National Asthma Education and Prevention Program, Third Expert Panel on the Diagnosis and Management of Asthma. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma. Bethesda, MD: National Heart, Lung, and Blood Institute (US); 2007 Aug. https://www.ncbi.nlm.nih.gov/books/NBK7232/ 20. Ralston, SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics 2014; 134(5): e1474–502.
CDC pediatric recommendations63 based on Hersh et al64 and Fashner et al75: “Management of the common cold, nonspecific URI, and acute cough illness should focus on symptomatic relief. Antibiotics should not be prescribed for these conditions.” Based on Ralston et al76: Antibiotics are not helpful for the treatment of bronchiolitis and should not be used. Chronic Asthma: Authors of a 2015 Cochrane SR (Kew et al86) found that the currently available evidence “is of very low quality due to heterogeneity among patients and interventions, imprecision and reporting biases.”86 Macrolides do not appear to be effective in improving most clinical outcomes based on their findings, but better quality evidence is need. Asthma exacerbations: Authors of a 2018 Cochrane SR (Normansell et al87) found limited evidence that antibiotics given at the time of an asthma exacerbation may improve symptoms and PEFR at follow-up, but findings were inconsistent and the studies had several limitations so the authors report limited confidence in the results and did not form conclusion due to insufficient evidence.87 Diffuse panbronchiolitis (DPB): According to authors of a 2015 Cochrane SR (Lin et al88) current guidelines suggest that “it may be reasonable to use low-dose macrolides soon after diagnosis is made and to continue this treatment for at least six months.” However, they found little evidence for macrolides in the treatment of DPB in their SR and could not make any new recommendations.88

Cochrane Systematic Reviews Cystic Fibrosis Authors of a Cochrane systematic review (SR) published in 2012 that includes 5 studies with low risk of bias (according to the authors), reported evidence of improved respiratory function after 6 months of azithromycin. Data on longer use was unclear, but they did find that reduction in pulmonary exacerbation was sustained. They also reported on some secondary outcomes that included positive outcomes for azithromycin (“significant reduction in need for oral antibiotics and greater weight gain” and “reduced identification of Staphylococcus aureus on respiratory culture”), but some adverse events with the use of a higher once-weekly dose of azithromycin (gastrointestinal adverse events), and “a significant increase in macrolide resistance.” Due to the emergence of macrolide resistance, they suggest that there is a need for a multi-center trial examining long-term effects.58 Chronic Rhinosinusitis Authors of Cochrane SR published in 2016 found very little evidence that systemic antibiotics are effective in patients with chronic rhinosinusitis. “We did find moderate quality evidence of a modest improvement in disease-specific quality of life in adults with chronic rhinosinusitis without polyps receiving three months of a macrolide antibiotic. The size of improvement was moderate (0.5 points on a five-point scale) and only seen at the end of the three-month treatment; by three months later no difference was found.” Limitations included small studies and few adverse events reported, and the authors suggest that more research is needed.84 Chronic Asthma Authors of Cochrane SR published in 2015 found that the currently available evidence “is of very low quality due to heterogeneity among patients and interventions, imprecision and reporting biases.”86 Macrolides do not appear to be effective in improving most clinical outcomes based on their findings, but better quality evidence is needed.86 Asthma exacerbations Authors of a recently published Cochrane SR (2018) found limited evidence that antibiotics given at the time of an asthma exacerbation may improve symptoms and PEFR at follow-up, but findings were inconsistent and the studies had several limitations so the authors report limited confidence in the results and did not form conclusion due to insufficient evidence.87 Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD) Authors of Cochrane SR published in 2013 that included trials of patients with COPD who were frequent exacerbators (and “needed treatment with antibiotics or systemic steroids, or who were on supplemental oxygen”), including older individuals (mean age of 66 years), found that use of continuous prophylactic macrolide antibiotics results in a clinically significant benefit in reducing exacerbations in COPD patients. It is important to note that the authors state “Because of concerns about antibiotic resistance and specific adverse effects, consideration of prophylactic antibiotic use should be mindful of the balance between benefits to individual patients and the potential harms to society created by antibiotic overuse.”78 Pelvic inflammatory disease (PID) Authors of a recently published Cochrane SR (2017) found no conclusive evidence that one regimen of antibiotics was safer or more effective than any other for the cure of PID, and one study which they rated as moderate-quality at low risk of bias, “suggested that a macrolide (azithromycin) may be more effective than a tetracycline (doxycycline) for curing mild-moderate PID.”72

26
Diffuse panbronchiolitis (DPB) According to authors of Cochrane SR published in 2015, current guidelines suggest that “it may be reasonable to use low-dose macrolides soon after diagnosis is made and to continue this treatment for at least six months.” However, they found little evidence for macrolides in the treatment of DPB in their SR and could not make any new recommendations.88 Acute lower respiratory tract infections “ranging from acute bronchitis and acute exacerbations of chronic bronchitis to pneumonia”77 Authors of Cochrane SR published in 2015 found small studies with unclear methodological quality. This evidence indicate that “In patients with acute bronchitis of a suspected bacterial cause, azithromycin tends to be more effective in terms of lower incidence of treatment failure and adverse events than amoxycillin or amoxyclav.”77 Chancroid (genital ulcerative disease caused by Haemophilus ducreyi) Authors of Cochrane SR published in 2017 found insufficient low quality evidence for macrolides in the treatment of H ducreyi infection (risk of bias due to poor methods, drop-out rate, and pharmaceutical sponsored studies). “Low quality evidence suggests that azithromycin could be considered as the first therapeutic alternative, based on their mono-dose oral administration, with a similar safety and effectiveness profile, when it is compared with long-term erythromycin use.”79 Chronic bacterial prostatitis Authors of a 2013 Cochrane review found that oral fluoroquinolones appear comparable for the treatment of chronic bacterial prostatitis (traditional pathogens) in terms of efficacy and safety, and no conclusive evidence was found for alternative agents (co-trimoxazole, beta-lactams and tetracyclines). Macrolides appeared to be more effective compared to fluoroquinolones in the treatment of CBP caused by obligate intracellular pathogens.85
Noted reasons why macrolides may be chosen in clinical practice
Dosing and adherence advantages: effective mono-dose for example in the treatment of chancroid51,79
Suitable for pregnant or nursing women51,79 Pregnancy Risk Factor B16 (no adverse events observed in animal reproduction studies) Current guidelines recommend azithromycin for the treatment of several infections, including chlamydia, gonococcal infections, and Mycobacterium avium complex (MAC) in pregnant patients. 16,51 Azithromycin is excreted in breast milk, but the relative infant dose (RID) is acceptable (below the generally acceptable RID of <10%). Caution is advised by the manufacturer when administered to breast-feeding women due to the potential for causing potential adverse events in infants including GI disturbances, rash, somnolence, and infantile hypertrophic pyloric stenosis (IHPS).16 Current CDC guidelines recommend azithromycin in the treatment of granuloma inguinale in lactating women, and as an alternative for lymphogranuloma venereum.16,51
Suitable for patients who are allergic to other antibiotics such as cephalosporins.51,79,80

27
Utah Medicaid Utilization Data All the data shown below is for a one year timeframe; August 1, 2017 to July 31, 2018.
A. Utah macrolide prescribing rates According to the CDC in 2015, the Outpatient Antibiotic Prescriptions per 1,000 Population for Utah ranged from 769-845, which falls somewhere in the middle of ranges nationally (highest: 1,018-1,319; lowest: 511-668).89,90 Macrolides were prescribed as 154 prescriptions per 1000 population.90 There were 430,726 Utah Medicaid eligible patients during our timeframe (August 1, 2017 to July 31, 2018), but they were not all eligible for the entire period. We adjusted this for time-of-eligibility, resulting in 345,393.1 patient years. There were 27,362 macrolide prescriptions during this period, and 25,519 azithromycin prescriptions. 20,872 patients received a macrolide, and 20,024 received azithromycin. (27,362/345,393.1)x1000=79.22 macrolide prescriptions per 1,000 person/years eligible for Medicaid (25,519/345,393.1)x1000=73.88 azithromycin prescriptions per 1,000 person/years eligible for Medicaid In the previous DUR report for antibiotics in the Utah pediatric population, the rates also appeared lower than expected. At the time, it was thought that there could be a few possible explanations for this including an underestimate of claims or a potential overestimate of the eligible population because they may not have been eligible for the whole year. The above calculation for the rate of macrolide prescribing considers the patient’s time of eligibility, and the best possible attempt was made to ensure inclusion of all macrolide claims. It is possible that macrolide prescribing is lower in the Utah Medicaid population compared to the CDC 2015 rates for the U.S.90 Another reason may include: focus and push for appropriate antibiotic prescribing by big organizations over the years perhaps making it likely that prescribing practices have changed over time as there have been national efforts to address this issue.
Table 3. Utah Medicaid macrolide prescribing rates (2017/2018) compared to CDC rates for the United States (2015)90
United States, 2015 Utah Medicaid,
August 2017 through July 2018
ANTIBIOTIC PRESCRIPTIONS PER
1,000 PERSONS, RATE
Not calculated for this project
Age group
<20 yearsa 778
≥20 yearsa 850
Sex
Female 1,005
Male 663
Antibiotic class
Macrolides 154 79.22
Top agent
Azithromycin 144 73.88
Note: Similar to CDC comment, these totals may not add all oral prescriptions due to missing data
28
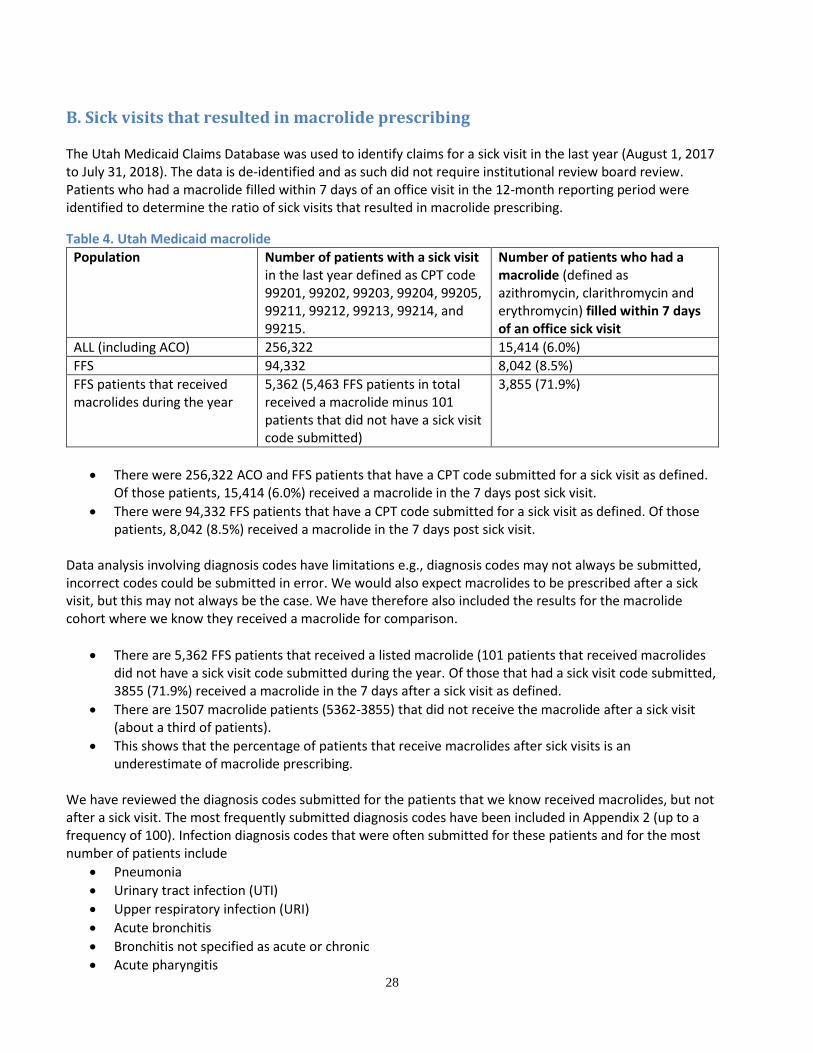
B. Sick visits that resulted in macrolide prescribing The Utah Medicaid Claims Database was used to identify claims for a sick visit in the last year (August 1, 2017 to July 31, 2018). The data is de-identified and as such did not require institutional review board review. Patients who had a macrolide filled within 7 days of an office visit in the 12-month reporting period were identified to determine the ratio of sick visits that resulted in macrolide prescribing.
Table 4. Utah Medicaid macrolide Population Number of patients with a sick visit
in the last year defined as CPT code 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, and 99215.
Number of patients who had a macrolide (defined as azithromycin, clarithromycin and erythromycin) filled within 7 days of an office sick visit
ALL (including ACO) 256,322 15,414 (6.0%)
FFS 94,332 8,042 (8.5%)
FFS patients that received macrolides during the year
5,362 (5,463 FFS patients in total received a macrolide minus 101 patients that did not have a sick visit code submitted)
3,855 (71.9%)
There were 256,322 ACO and FFS patients that have a CPT code submitted for a sick visit as defined. Of those patients, 15,414 (6.0%) received a macrolide in the 7 days post sick visit.
There were 94,332 FFS patients that have a CPT code submitted for a sick visit as defined. Of those patients, 8,042 (8.5%) received a macrolide in the 7 days post sick visit.
Data analysis involving diagnosis codes have limitations e.g., diagnosis codes may not always be submitted, incorrect codes could be submitted in error. We would also expect macrolides to be prescribed after a sick visit, but this may not always be the case. We have therefore also included the results for the macrolide cohort where we know they received a macrolide for comparison.
There are 5,362 FFS patients that received a listed macrolide (101 patients that received macrolides did not have a sick visit code submitted during the year. Of those that had a sick visit code submitted, 3855 (71.9%) received a macrolide in the 7 days after a sick visit as defined.
There are 1507 macrolide patients (5362-3855) that did not receive the macrolide after a sick visit (about a third of patients).
This shows that the percentage of patients that receive macrolides after sick visits is an underestimate of macrolide prescribing.
We have reviewed the diagnosis codes submitted for the patients that we know received macrolides, but not after a sick visit. The most frequently submitted diagnosis codes have been included in Appendix 2 (up to a frequency of 100). Infection diagnosis codes that were often submitted for these patients and for the most number of patients include
Pneumonia
Urinary tract infection (UTI)
Upper respiratory infection (URI)
Acute bronchitis
Bronchitis not specified as acute or chronic
Acute pharyngitis

29
Acute sinusitis
Chronic sinusitis
Strep pharyngitis
Sepsis Many patients had diagnosis codes submitted for nicotine dependence and chronic obstructive pulmonary disease (COPD) which highlights the need to continue and improve efforts to help patients with smoking cessation.
C. Macrolide utilization: Number of claims and patients (August 1, 2017 to July 31, 2018) The Utah Medicaid Claims Database was used to identify claims for oral macrolide prescriptions including azithromycin, clarithromycin, and erythromycin, regardless of sick visit codes submitted. This was done in order to include all claims for macrolides, because sick visit diagnosis codes may not always precede macrolide fills.
The tables below show the number of claims and patients that received macrolides during the last year (All fills, FFS fills and ACO fills in 3 tables)
The majority of claims were for azithromycin (25519=93%)
Claims for clarithromycin and erythromycin accounted for approximately 7% of the macrolide claims (clarithromycin 932=3.4% and erythromycin 911=3.3%)

Table 5. All (FFS and ACO) UT Medicaid macrolide utilization (number of patients and claims); August 1, 2017 to July 31, 2018 ALL FILLS
2017 2018 Total
Claims Patients Claims Patients Claims Patients
Azithromycin AZITHROMYCIN POW 1GM PAK 37 34 29 28 66 62
Azithromycin AZITHROMYCIN SUS 100/5ML 850 772 1048 949 1898 1622
Azithromycin AZITHROMYCIN SUS 200/5ML 3230 2943 4040 3619 7270 6053
Azithromycin AZITHROMYCIN TAB 250MG 6200 5438 7505 6463 13705 10985
Azithromycin AZITHROMYCIN TAB 500MG 1063 919 1400 1189 2463 2022
Azithromycin AZITHROMYCIN TAB 600MG 43 15 73 18 116 22
Azithromycin ZITHROMAX POW 1GM PAK 1 1 _ _ 1 1
Clarithromycin CLARITHROMYC SUS 125/5ML 7 7 6 6 13 13
Clarithromycin CLARITHROMYC SUS 250/5ML 30 26 33 32 63 58
Clarithromycin CLARITHROMYC TAB 250MG 10 9 16 14 26 23
Clarithromycin CLARITHROMYC TAB 500MG 349 331 453 415 802 730
Clarithromycin CLARITHROMYC TAB 500MG ER 12 11 16 15 28 24
Erythromycin Base ERY-TAB TAB 250MG EC 26 10 22 6 48 11
Erythromycin Base ERY-TAB TAB 333MG EC 6 1 10 2 16 2
Erythromycin Base ERY-TAB TAB 500MG EC 6 5 _ _ 6 5
Erythromycin Base ERYTHROMYCIN CAP 250MG EC 6 3 16 7 22 9
Erythromycin Base ERYTHROMYCIN TAB 250MG BS 26 18 27 13 53 27
Erythromycin Base ERYTHROMYCIN TAB 500MG BS 25 15 25 15 50 28
Erythromycin Ethylsuccinate E.E.S. GRAN SUS 200/5ML 73 11 3 1 76 12
Erythromycin Ethylsuccinate ERYPED SUS 200/5ML 28 7 13 6 41 10
Erythromycin Ethylsuccinate ERYPED SUS 400/5ML 68 17 70 16 138 23
Erythromycin Ethylsuccinate ERYTHROM ETH SUS 200/5ML 151 39 273 58 424 78
Erythromycin Ethylsuccinate ERYTHROM ETH TAB 400MG 12 3 7 2 19 3
Erythromycin Stearate ERYTHROCIN TAB 250MG 5 1 13 6 18 6
Total Total 12264 10359 15098 12539 27362 20872
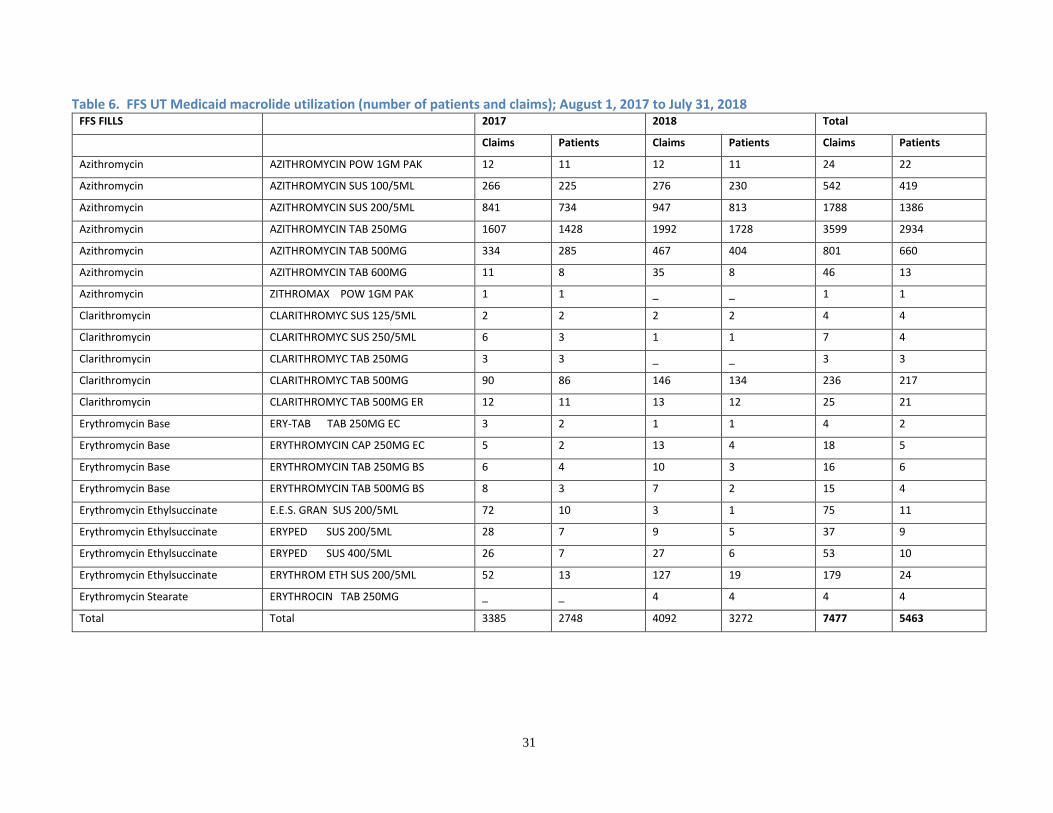
31
Table 6. FFS UT Medicaid macrolide utilization (number of patients and claims); August 1, 2017 to July 31, 2018 FFS FILLS
2017 2018 Total
Claims Patients Claims Patients Claims Patients
Azithromycin AZITHROMYCIN POW 1GM PAK 12 11 12 11 24 22
Azithromycin AZITHROMYCIN SUS 100/5ML 266 225 276 230 542 419
Azithromycin AZITHROMYCIN SUS 200/5ML 841 734 947 813 1788 1386
Azithromycin AZITHROMYCIN TAB 250MG 1607 1428 1992 1728 3599 2934
Azithromycin AZITHROMYCIN TAB 500MG 334 285 467 404 801 660
Azithromycin AZITHROMYCIN TAB 600MG 11 8 35 8 46 13
Azithromycin ZITHROMAX POW 1GM PAK 1 1 _ _ 1 1
Clarithromycin CLARITHROMYC SUS 125/5ML 2 2 2 2 4 4
Clarithromycin CLARITHROMYC SUS 250/5ML 6 3 1 1 7 4
Clarithromycin CLARITHROMYC TAB 250MG 3 3 _ _ 3 3
Clarithromycin CLARITHROMYC TAB 500MG 90 86 146 134 236 217
Clarithromycin CLARITHROMYC TAB 500MG ER 12 11 13 12 25 21
Erythromycin Base ERY-TAB TAB 250MG EC 3 2 1 1 4 2
Erythromycin Base ERYTHROMYCIN CAP 250MG EC 5 2 13 4 18 5
Erythromycin Base ERYTHROMYCIN TAB 250MG BS 6 4 10 3 16 6
Erythromycin Base ERYTHROMYCIN TAB 500MG BS 8 3 7 2 15 4
Erythromycin Ethylsuccinate E.E.S. GRAN SUS 200/5ML 72 10 3 1 75 11
Erythromycin Ethylsuccinate ERYPED SUS 200/5ML 28 7 9 5 37 9
Erythromycin Ethylsuccinate ERYPED SUS 400/5ML 26 7 27 6 53 10
Erythromycin Ethylsuccinate ERYTHROM ETH SUS 200/5ML 52 13 127 19 179 24
Erythromycin Stearate ERYTHROCIN TAB 250MG _ _ 4 4 4 4
Total Total 3385 2748 4092 3272 7477 5463

32
Table 7. ACO UT Medicaid macrolide utilization (number of patients and claims); August 1, 2017 to July 31, 2018 ACO FILLS
2017 2018 Total
Claims Patients Claims Patients Claims Patients
Azithromycin AZITHROMYCIN POW 1GM PAK 25 24 17 17 42 41
Azithromycin AZITHROMYCIN SUS 100/5ML 584 549 772 719 1356 1207
Azithromycin AZITHROMYCIN SUS 200/5ML 2389 2216 3093 2812 5482 4686
Azithromycin AZITHROMYCIN TAB 250MG 4593 4028 5513 4753 10106 8126
Azithromycin AZITHROMYCIN TAB 500MG 729 640 933 790 1662 1375
Azithromycin AZITHROMYCIN TAB 600MG 32 10 38 10 70 13
Clarithromycin CLARITHROMYC SUS 125/5ML 5 5 4 4 9 9
Clarithromycin CLARITHROMYC SUS 250/5ML 24 23 32 31 56 54
Clarithromycin CLARITHROMYC TAB 250MG 7 6 16 14 23 20
Clarithromycin CLARITHROMYC TAB 500MG 259 245 307 282 566 516
Clarithromycin CLARITHROMYC TAB 500MG ER _ _ 3 3 3 3
Erythromycin Base ERY-TAB TAB 250MG EC 23 8 21 5 44 9
Erythromycin Base ERY-TAB TAB 333MG EC 6 1 10 2 16 2
Erythromycin Base ERY-TAB TAB 500MG EC 6 5 _ _ 6 5
Erythromycin Base ERYTHROMYCIN CAP 250MG EC 1 1 3 3 4 4
Erythromycin Base ERYTHROMYCIN TAB 250MG BS 20 14 17 11 37 22
Erythromycin Base ERYTHROMYCIN TAB 500MG BS 17 13 18 13 35 25
Erythromycin Ethylsuccinate E.E.S. GRAN SUS 200/5ML 1 1 _ _ 1 1
Erythromycin Ethylsuccinate ERYPED SUS 200/5ML _ _ 4 2 4 2
Erythromycin Ethylsuccinate ERYPED SUS 400/5ML 42 12 43 10 85 16
Erythromycin Ethylsuccinate ERYTHROM ETH SUS 200/5ML 99 26 146 40 245 55
Erythromycin Ethylsuccinate ERYTHROM ETH TAB 400MG 12 3 7 2 19 3
Erythromycin Stearate ERYTHROCIN TAB 250MG 5 1 9 3 14 3
Total Total 8879 7660 11006 9311 19885 15572

D. Age and Sex of FFS patients that received macrolides
46% of FFS patients that received macrolide prescriptions were <18 years old.
In the adult population, it seems like more patients that received macrolides were in the 25-34 year old and the 35-44 year old categories.
The sex distribution seem appropriate given the demographics of the Utah Medicaid population (mainly women and children).
0
500
1000
1500
2000
2500
<18 18-24 25-34 35-44 45-54 55-64
count 2561 434 786 693 516 452
Nu
mb
er
of
pat
ien
ts
Age
Number of FFS patients in different age categories that received macrolides
0
500
1000
1500
2000
2500
3000
3500
Female Male
count 3377 2086
Nu
mb
er
of
pat
ien
ts
Sex of FFS patients that received macrolides
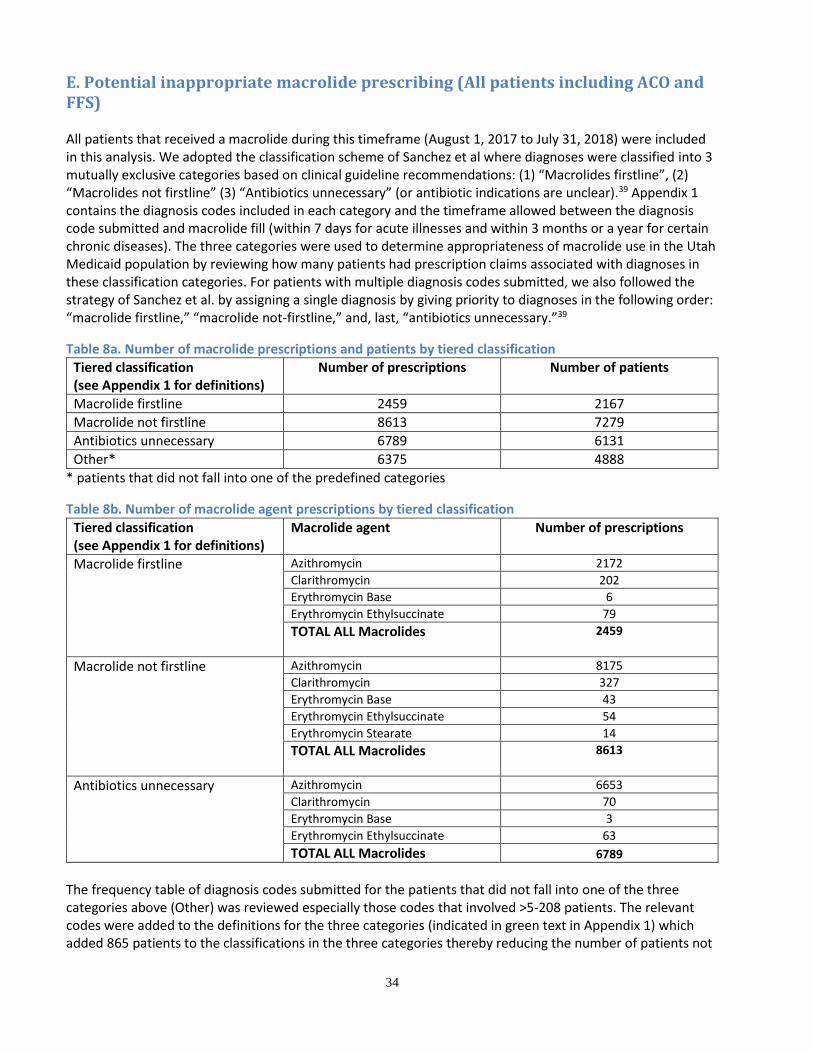
34
E. Potential inappropriate macrolide prescribing (All patients including ACO and FFS) All patients that received a macrolide during this timeframe (August 1, 2017 to July 31, 2018) were included in this analysis. We adopted the classification scheme of Sanchez et al where diagnoses were classified into 3 mutually exclusive categories based on clinical guideline recommendations: (1) “Macrolides firstline”, (2) “Macrolides not firstline” (3) “Antibiotics unnecessary” (or antibiotic indications are unclear).39 Appendix 1 contains the diagnosis codes included in each category and the timeframe allowed between the diagnosis code submitted and macrolide fill (within 7 days for acute illnesses and within 3 months or a year for certain chronic diseases). The three categories were used to determine appropriateness of macrolide use in the Utah Medicaid population by reviewing how many patients had prescription claims associated with diagnoses in these classification categories. For patients with multiple diagnosis codes submitted, we also followed the strategy of Sanchez et al. by assigning a single diagnosis by giving priority to diagnoses in the following order: “macrolide firstline,” “macrolide not-firstline,” and, last, “antibiotics unnecessary.”39
Table 8a. Number of macrolide prescriptions and patients by tiered classification Tiered classification (see Appendix 1 for definitions)
Number of prescriptions Number of patients
Macrolide firstline 2459 2167
Macrolide not firstline 8613 7279
Antibiotics unnecessary 6789 6131
Other* 6375 4888
* patients that did not fall into one of the predefined categories
Table 8b. Number of macrolide agent prescriptions by tiered classification
Tiered classification (see Appendix 1 for definitions)
Macrolide agent Number of prescriptions
Macrolide firstline Azithromycin 2172 Clarithromycin 202 Erythromycin Base 6 Erythromycin Ethylsuccinate 79 TOTAL ALL Macrolides 2459
Macrolide not firstline Azithromycin 8175 Clarithromycin 327 Erythromycin Base 43 Erythromycin Ethylsuccinate 54 Erythromycin Stearate 14 TOTAL ALL Macrolides 8613
Antibiotics unnecessary Azithromycin 6653 Clarithromycin 70 Erythromycin Base 3 Erythromycin Ethylsuccinate 63 TOTAL ALL Macrolides 6789
The frequency table of diagnosis codes submitted for the patients that did not fall into one of the three categories above (Other) was reviewed especially those codes that involved >5-208 patients. The relevant codes were added to the definitions for the three categories (indicated in green text in Appendix 1) which added 865 patients to the classifications in the three categories thereby reducing the number of patients not

35
belonging to one of the three categories and likely inappropriate use to 4023. Please refer to table 10 below for adjusted numbers.
Table 9. Revised number of macrolide prescriptions and patients by tiered classification Tiered classification (see Appendix 1 for definitions)
Number of prescriptions ALL ACO+FFS (FFS)
Number of patients ALL ACO+FFS (comparison to before revision)
(FFS)
Macrolide firstline 2666 (789) 2354 (8.6% more) (620)
Macrolide not firstline 10083 (2724) 8430 (15.8% more) (2202)
Antibiotics unnecessary 6201 (1617) 5658 (7.7% fewer) (1447)
Other* 5335 (1329) 4023 (17.7% fewer) (1085)
*patients that did not fall into one of the predefined categories. Additionally, not all patients (n=407) have a dx in the Medicaid database. Macrolide not firstline and prior other antibiotic fills Patients in the macrolide not firstline category that received another antibiotic within 14 days prior to receiving a macrolide were identified, because these patients could or could not be receiving appropriate therapy. These would require individual review on a case by case basis to determine diagnoses, antibiotics received and the appropriateness of the type, dose, duration and order of antibiotics received. The remaining patients did not receive another antibiotic within 14 days prior to the macrolide and the assumption is that these patients received a macrolide first line for indications in which macrolide therapy is not recommended firstline. Of the 8430 patients that fall into the macrolide not firstline category,
3848 (45.6% of the not firstline) patients filled “any other antibiotic” within 14 days before filling a prescription for a macrolide indicating potential appropriate/inappropriate use. Any other antibiotic is defined in appendix 3.
4582 (54.4% of the not firstline) patients did not fill a prescription for another antibiotic within 14 days prior to filling a prescription for a macrolide indicating highly likely inappropriate use.
Antibiotics unnecessary: In addition, 5658 patients were in the antibiotics not necessary category. TOTAL INAPPROPRIATE USE Likely to highly likely (number of patients): 4023 + 5658 + 4582 = 14,263/20,465 = ~70% of patients receiving macrolides Potential (number of patients): 3848/20,465 = ~19% (and 407 patients unknown/without dx codes) Limitations and potential future analyses It is important to remember that any assessment using diagnosis codes (designed for billing purposes) relies on accurate diagnosing and diagnosis code submission (diagnosis codes are often under submitted, or coding errors may occur as these are not entered by physicians), and billing coding may not reflect the more complete documentation that the doctor has executed among the patient’s chart housed in the clinic. Also, identifying and defining diagnosis codes for data extraction is a tedious task and omissions and errors are possible as there are a plethora of possible codes for the variety of forms an illness may manifest. The additional analysis hereafter was based on the numbers/data in tables 8a and 8b above prior to revising diagnosis codes of patients that did not fall into one of the categories. Patients could be receiving a macrolide as third line in which case maybe more than 14 days since their original diagnosis code needs to be considered. Also, patients could have been hospitalized prior to receiving the macrolide in which case prior antibiotic use may not be shown in the pharmacy data.

36
Patients with certain conditions (such as cancer, sickle cell disease, immunodeficiency or transplants), hospitalized patients or those in care facilities may be more vulnerable to infections especially resistant infections. Future work should explore particular patient and clinician characteristics associated with macrolide selection through multivariable logistic regression. Given that this is a local claims database, appropriate local characteristics should be identified to explore which may be different from the National characteristics explored by Sanchez et al.39 Cystic Fibrosis The macrolide not firstline include cystic fibrosis, and based on current evidence and expert opinion, macrolide is appropriate as firstline therapy for patients with cystic fibrosis. We are therefore including a breakdown in the table below of how many patients had diagnosis codes for cystic fibrosis in this tier.
Table 10a. Number of prescriptions and patients associated with a Cystic Fibrosis diagnosis code* Tiered classification Number of prescriptions Number of patients
Macrolide not firstline 8613 7279
Cystic fibrosis (CF)* 238 39
CF* after adding additional codes as definitions to tiers
230 38 (12 FFS)
*Without a dx code for another infection in the firstline category
Table 10b. Type of macrolide used in patients with CF diagnosis code
Type of macrolide for CF Number of prescriptions
Azithromycin 223 Erythromycin Ethylsuccinate 3 Erythromycin Stearate 12
Table 10c. Prescribers of macrolide prescriptions in patients with CF
Type Rx_count
Physician 159
Unknown\Missing 45
Nurse Practitioner 31
Physician Assistant 2
Osteopath 1
Specialty Rx_count
Pulmonary Diseases 148
Unknown/Missing 46
Pediatrics 29
Family Practice 10
Gastroenterology 4
Otorhinolaryngology 1
Acne Another use that may require additional review for appropriateness is acne so we have included the potential number of patients that may require additional review to ensure appropriate use. This additional review could include:
(1) The type of macrolide and whether the patient has received a tetracycline before with any evidence of a contraindication (whether pregnant or <8 yrs) Erythromycin is recommended only if tetracyclines are contraindicated. Erythromycin is not a firstline treatment for acne because C. acnes often develops resistance to erythromycin. Also, it has less anti-inflammatory action and patients often experience intolerable GI effects with erythromycin. Azithromycin may also be used, but concerns about resistance limit its use.28,29
(2) Whether patients received macrolide for >3 months

37
Oral antibiotics should be used for the shortest duration possible (ideally three to four months; avoid use as maintenance therapy) to limit the emergence of antibiotic resistance, and it should not be used as monotherapy. Antibiotics should be used in combination with a topical retinoid to facilitate discontinuation of the antibiotic.28,29
Table 11a. Number of prescriptions and patients associated with an acne diagnosis code* Tiered classification Number of prescriptions Number of patients
Macrolide not firstline 8613 7279
Acne* 241 196
Acne* after after adding additional codes as definitions to tiers
240 195 (33 FFS)
*Without a dx code for another infection in the firstline category
Table 11b. Type of macrolide used in patients with an acne diagnosis code
Type of macrolide for acne Number of prescriptions
Azithromycin 218
Clarithromycin 8
Erythromycin Base 13
Erythromycin Stearate 2
Table 11c. Prescribers of macrolide prescriptions in patients with acne diagnosis codes submitted
Type Rx_count
Physician 120
Unknown\missing 42
Physician Assistant 26
Osteopath 22
Nurse Practitioner 17
Dentist 12
Certified Nurse Midwife
1
Podiatrist 1
Specialty Rx_count
Family Practice 93
Unknown/Missing 63
Pediatrics 32
Dermatology 24
Emergency Medicine 8
Internal Medicine 8
Obstetrics-Gynecology 5
General Preventive Medicine 2
Otorhinolaryngology 2
Nephrology 1
Pulmonary Diseases 1
Psychiatry 1
Plastic Surgery 1
F. Prescribers of all macrolide prescriptions
Table 12a. Prescriber type
Prescriber Type Prescription count
Physician 12369
Unknown\Missing 5397
Physician Assistant 4172
Nurse Practitioner 2577
Osteopath 2194
Prescriber Type Prescription count
Dentist 398
Certified Nurse Midwife 103
Nurse Practitioner 86
GROUP PRACTICE 32
Optometrist 24
Podiatrist 10
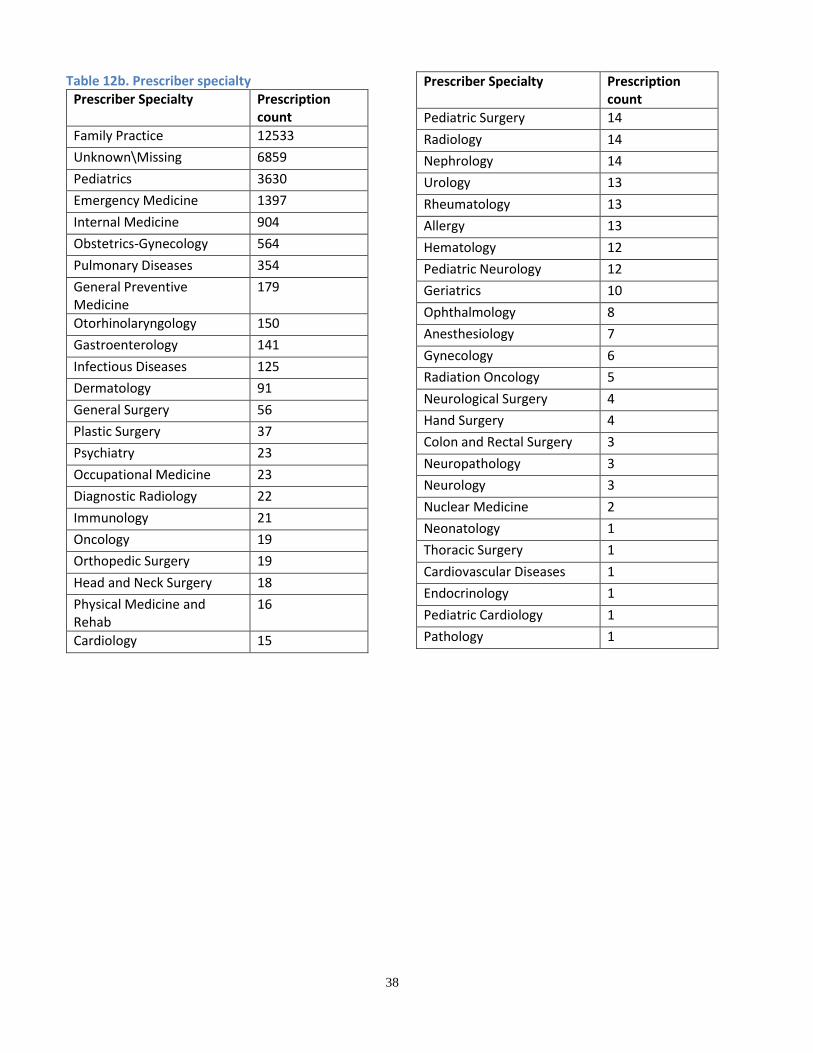
38
Table 12b. Prescriber specialty Prescriber Specialty Prescription
count
Family Practice 12533
Unknown\Missing 6859
Pediatrics 3630
Emergency Medicine 1397
Internal Medicine 904
Obstetrics-Gynecology 564
Pulmonary Diseases 354
General Preventive Medicine
179
Otorhinolaryngology 150
Gastroenterology 141
Infectious Diseases 125
Dermatology 91
General Surgery 56
Plastic Surgery 37
Psychiatry 23
Occupational Medicine 23
Diagnostic Radiology 22
Immunology 21
Oncology 19
Orthopedic Surgery 19
Head and Neck Surgery 18
Physical Medicine and Rehab
16
Cardiology 15
Prescriber Specialty Prescription count
Pediatric Surgery 14
Radiology 14
Nephrology 14
Urology 13
Rheumatology 13
Allergy 13
Hematology 12
Pediatric Neurology 12
Geriatrics 10
Ophthalmology 8
Anesthesiology 7
Gynecology 6
Radiation Oncology 5
Neurological Surgery 4
Hand Surgery 4
Colon and Rectal Surgery 3
Neuropathology 3
Neurology 3
Nuclear Medicine 2
Neonatology 1
Thoracic Surgery 1
Cardiovascular Diseases 1
Endocrinology 1
Pediatric Cardiology 1
Pathology 1

39
G. Prescribers of macrolides by tiered classification (recommended firstline, not firstline, unnecessary)
0 500 1000 1500 2000 2500 3000 3500 4000
Physician
Unknown\Missing
Physician Assistant
Nurse Practitioner
Osteopath
Dentist
Certified Nurse Midwife
GROUP PRACTICE
Podiatrist
Optometrist
PhysicianUnknown\
MissingPhysicianAssistant
NursePractitioner
Osteopath DentistCertified
NurseMidwife
GROUPPRACTICE
PodiatristOptometris
t
Unnecessary 2924 1306 1222 680 611 24 10 9 1 2
Not firstline 3800 1674 1469 983 625 32 17 6 5 2
Firstline 1059 790 205 166 230 3 4 2 0 0
Prescriber types by diagnosis categories
Unnecessary Not firstline Firstline
0 500 1000 1500 2000 2500 3000 3500 4000 4500
Family Practice
Pediatrics
Emergency Medicine
Unknown/Missing
Internal Medicine
Pulmonary Diseases
Obstetrics-Gynecology
Dermatology
Gastroenterology
Otorhinolaryngology
Predominant prescriber specialties by diagnosis categories
Unnecessary Not firstline Firstline

40
Table 13. Prescribers of macrolides by tiered classification
Number of prescriptions
Specialty Firstline Not firstline Unnecessary
Family Practice 844 3845 3503
Pediatrics 245 1432 930
Emergency Medicine 246 520 363
Unknown/Missing 924 317 1626
Internal Medicine 97 234 182
Pulmonary Diseases 24 152 19
Obstetrics-Gynecology 30 59 37
Dermatology 0 40 4
Gastroenterology 9 35 9
Otorhinolaryngology 2 35 25
General Surgery 7 17 8
Infectious Diseases 8 13 3
Diagnostic Radiology 0 10 1
General Preventive Medicine 2 9 13
Head and Neck Surgery 0 8 1
Occupational Medicine 0 8 10
Plastic Surgery 2 8 13
Physical Medicine and Rehab 0 6 4
Psychiatry 4 6 2
Oncology 0 5 5
Hand Surgery 0 4 0
Cardiology 1 3 5
Pediatric Surgery 0 3 3
Colon and Rectal Surgery 0 2 0
Hematology 1 2 0
Nephrology 2 2 3
Orthopedic Surgery 0 2 1
Radiation Oncology 0 2 0
Radiology 0 2 0
Allergy 0 1 6
Endocrinology 0 1 0
Immunology 0 1 0
Neurological Surgery 0 1 2
Neuropathology 0 1 1
Rheumatology 0 1 2
Thoracic Surgery 0 1 0
Urology 2 1 1
Anesthesiology 1 0 1
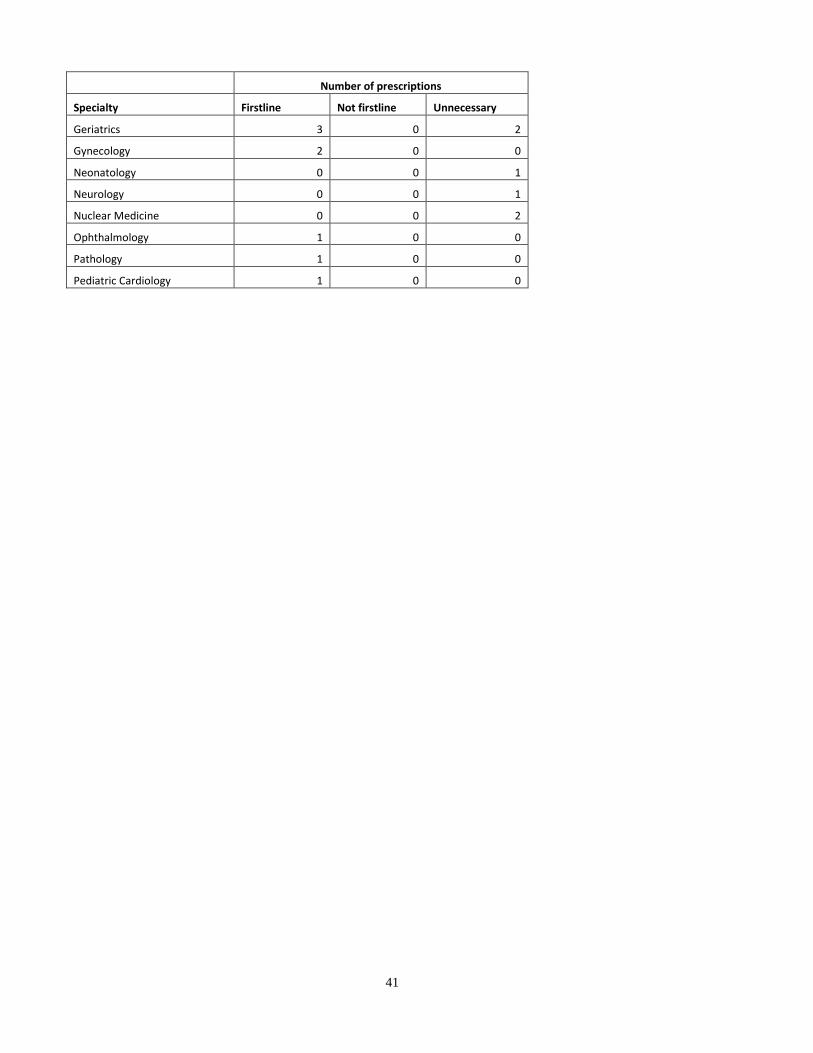
41
Number of prescriptions
Specialty Firstline Not firstline Unnecessary
Geriatrics 3 0 2
Gynecology 2 0 0
Neonatology 0 0 1
Neurology 0 0 1
Nuclear Medicine 0 0 2
Ophthalmology 1 0 0
Pathology 1 0 0
Pediatric Cardiology 1 0 0

Conclusions It is important to find strategies to ensure accurate diagnosis of infections (especially respiratory tract infections) and adherence to evidence-based recommendations for macrolide use to help prevent antimicrobial resistance. The overall macrolide and more specifically azithromycin prescribing rates in the Utah Medicaid population appears lower than the CDC 2015 rates for the U.S. (~79 vs. 154 and ~73 vs. 144).90 Our data shows that macrolides were used by 20,872 patients and accounted for 27,362 claims in one year, which is mainly azithromycin use (93%). About a third of Utah Medicaid patients that received macrolides did not receive these after a sick visit and reviewing only the percentage of patients that receive macrolides after sick visits is an underestimate of macrolide prescribing. It does however provide useful information on the extent of macrolide prescribing during sick visits. In our FFS population, 8.5% of patients that had a sick visit code submitted received a macrolide within 7 days. Review of the diagnosis codes of those patients that received a macrolide, but not after a sick visit indicated that many of these patients had diagnosis codes submitted for nicotine dependence and chronic obstructive pulmonary disease (COPD) which highlights the need to continue and improve efforts to help patients with smoking cessation. The age and sex distribution of macrolide use appear related to the demographics of the Utah Medicaid population (mainly women and children); FFS macrolide use for example include 62% females and 46% were under 18 years old. Review of macrolides used in the Utah Medicaid population indicate potential inappropriate use for indications in which macrolides are not recommended firstline as well as indications in which antibiotics are considered unnecessary. Approximately 70% of patients that received macrolides appear likely or highly likely to be inappropriate, and an additional 19% could be potentially inappropriate (only about 11-30% appear appropriate). However, the limitations for using diagnosis codes to determine inappropriate use should be considered. We cannot capture sound professional judgment that might have been made based on bacteria culture for susceptibility/resistance, previous antibiotic treatment in hospital, or other special population circumstance (immunocompromised, prophylaxis of M.avium in HIV) where it is difficult to extract from ICD10 coding whether use is appropriate or not. Nonetheless, this number (70%) is so high that there is probably plenty of misuse remaining. The not firstline category include patients that received another antibiotic within 14 days prior to receiving a macrolide and potential inappropriate use needs to be reviewed further in these patients (the 19%) potentially via individual patient reviews. Macrolide use in the treatment of acne require additional review to ensure appropriate use (I.e., prescribers, type of macrolide, duration of use, and prior tetracycline use and contraindications such as being pregnant or <8years old). Review of prescriber types and specialties involved with inappropriate macrolide prescribing indicate opportunities for targeted educational interventions. We need to continue efforts to “ensure patients receive the right antibiotic, at the right time, with the right dose and duration.”13 To consider:
Identify top macrolide prescribers (per prescription frequencies) that fall into potentially inappropriately prescribing to send an educational letter to them in general (not patient specific).
Identify patients that have potentially been receiving inappropriate macrolides for individual patient review and send recommendation(s) to prescribers
Continue and improve efforts to help patients with smoking cessation

Appendix 1
Table 1. Tiered Classification of Diagnoses by Macrolide treatment recommendations (adapted from Sanchez et al.) with newly defined ICD10 definitions
Macrolides firstline Timeframe for dx code submission ICD-9 ICD-10 (Used ICD-9data.com for mapping to ICD-10)
Pneumonia (including atypical) Within 7 days prior
481 Pneumococcal pneumonia [Streptococcus pneumoniae pneumonia], 482 Other bacterial pneumonia, 483 Pneumonia due to other specified organism, 484 Pneumonia in infectious diseases classified elsewhere, 485 Bronchopneumonia, organism unspecified, 486 Pneumonia, organism unspecified
J13* Pneumonia due to Streptococcus pneumoniae; J18.1 Lobar pneumonia, unspecified organism;J14 Pneumonia due to Hemophilus influenzae; J15.0 Pneumonia due to Klebsiella pneumoniae; J15.1 Pneumonia due to Pseudomonas; J15.3 Pneumonia due to streptococcus, group B; J15.4 Pneumonia due to other streptococci; J15.5 Pneumonia due to Escherichia coli; J15.6 Pneumonia due to other Gram-negative bacteria; J15.7 Pneumonia due to Mycoplasma pneumoniae; J15.8 Pneumonia due to other specified bacteria; J15.9 Unspecified bacterial pneumonia; J15.20 Pneumonia due to staphylococcus, unspecified; J15.211 Pneumonia due to Methicillin susceptible Staphylococcus aureus; J15.212 Pneumonia due to Methicillin resistant Staphylococcus aureus; J15.29 Pneumonia due to other staphylococcus; J16.0 Chlamydial pneumonia; J16.8 Pneumonia due to other specified infectious organisms; J17 Pneumonia in diseases classified elsewhere; J18.0 Bronchopneumonia, unspecified organism; J18.9 Pneumonia, unspecified organism; A22.1 Pulmonary anthrax; A37.91 Whooping cough, unspecified species with pneumonia; A48.1 Legionnaires' disease; B25.0 Cytomegaloviral pneumonitis; B44.0 Invasive pulmonary aspergillosis after reviewing dx frequency include J200 Acute bronchitis due to mycoplasma pneumonia; J188 Other pneumonia, unspecified organism
Nontuberculosis mycobacteria disease Within 7 days prior
031.0 Pulmonary diseases due to other mycobacteria A31.0 Pulmonary mycobacterial infection
Pertussis Within 7 days prior 033.9 A37.90 Whooping cough, unspecified species without pneumonia
Cat scratch disease (Bartonella) Within 7 days prior 078.3 A28.1 Cat scratch disease, A44.9 Bartonellosis, unspecified
Cervicitis and endocervicitis, urethritis, and other gonococcal or chlamydia infections, chancroid (H. ducreyi), granuloma inguinale (characterized by genital ulcers), and other sexually transmitted infections Within 7 days prior
073.0 Ornithosis with pneumonia; 073.7 Ornithosis with other specified complications; 073.8 Ornithosis with unspecified complication; 073.9 Ornithosis, unspecified 597.80 Urethritis, unspecified; 076 Chronic infection of the conjunctiva and cornea caused by chlamydia trachomatis; 077 Other diseases of conjunctiva due to viruses and chlamydiae; 616.0 Cervicitis and endocervicitis
A54* Gonococcal infection; A55* Chlamydial lymphogranuloma (venereum); A56* Other sexually transmitted chlamydial diseases; A57* Chancroid; A58* Granuloma inguinale; A59* Trichomoniasis; A63* Other predominantly sexually transmitted diseases, not elsewhere classified; A64* Unspecified sexually transmitted disease; A70* Chlamydia psittaci infections; J17* Pneumonia in diseases classified elsewhere; N34.1 Nonspecific urethritis, N34.2 Other urethritis; A70-A74 Other diseases caused by chlamydiae; N72 Inflammatory disease of cervix uteri Add Z202 Contact w and exposure to infect w a sexl mode of (from dx freq found this)
Babesiosis (mostly spread by ticks) Within 7 days prior B60.0 Babesiosis
Infectious diarrhea/traveler’s diarrhea Within 7 days prior 009.2 Infectious diarrhea A09* Infectious gastroenteritis and colitis, unspecified
Shigellosis Within 7 days prior 004 Shigellosis A03* Shigellosis
Peptic ulcer disease, H. pylori infection Within 7 days prior
533 Peptic ulcer site unspecified, 041.86 Helicobacter pylori [H. pylori] infection
K27* Peptic ulcer, site unspecified, B96.81 Helicobacter pylori [H. pylori] as the cause of diseases classified elsewhere
Chronic obstructive pulmonary disease exacerbation Within 7 days prior J44.1 Chronic obstructive pulmonary disease with (acute) exacerbation

44
Macrolides not firstline Timeframe for dx code submission ICD-9 ICD-10 (Used ICD-9data.com for mapping to ICD-10)
Cystic Fibrosis Anytime during the year 277 E84*
Pharyngitis Within 7 days prior 462 Acute pharyngitis J02.9 Acute pharyngitis after reviewing dx frequency include all J02* Acute pharyngitis; J060 Acute laryngopharyngitis
Strep throat Within 7 days prior 034.0 J02.0
Acute tonsillitis Within 7 days prior 463 Acute tonsillitis
J03.90 Acute tonsillitis after reviewing dx frequency: include J0300 Acute streptococcal tonsillitis, unspecified, but J03* Acute tonsillitis so include all J03*
Scarlet fever Within 7 days prior 034.1 Scarlet fever A38 Scarlet fever
Urinary Tract Infection (UTI) Within 7 days prior
590.1, 590.2, 590.8, 590.9, 595.0, 595.9, 599.0: Acute puelonephritis, renal abscess, other pyelonephritis
N10* Acute pyelonephritis, N15.1 Renal and perinephric abscess, N12* Tubulo-interstitial nephritis, not specified as acute or chronic, N16* Renal tubulo-interstitial disorders in diseases classified elsewhere, N15.9 Renal tubulo-interstitial disease, unspecified, N30.00 Acute cystitis without hematuria, N30.01 Acute cystitis with hematuria, N39.0 Urinary tract infection, site not specified
Sinusitis Within 7 days prior 461.9 Acute sinusitis, unspecified, 473.9 Unspecified Sinusitis (Chronic)
J01.90 Acute sinusitis, unspecified; Include all J01* after reviewing dx frequency found this was not included; J320 Chronic maxillary sinusitis; J321 Chronic frontal sinusitis; Include all J32* J32.9 Unspecified Sinusitis (Chronic)
Acute otitis Media Within 7 days prior 382 Suppurative and unspecified otitis media H66- Suppurative and unspecified otitis media
Gastrointestinal infections (excluding shigellosis) Within 7 days prior
001 Cholera 002 Typhoid and paratyphoid fevers 003 Other salmonella infections 005 Other food poisoning (bacterial) 006 Amebiasis 007 Other protozoal intestinal diseases 008 Intestinal infections due to other organisms 787 Symptoms involving digestive system 002 Typhoid and paratyphoid fevers 027.0 Listeriosis
A00* Cholera A01* Typhoid and paratyphoid fevers; A02* Other salmonella infections; A05* Other bacterial foodborne intoxications, not elsewhere classified; A06* Amebiasis; A07* Other protozoal intestinal diseases; A04* Other bacterial foodborne intoxications, not elsewhere classified R11* Nausea and vomiting, R10* Abdominal and pelvic pain R19* Other symptoms and signs involving the digestive system and abdomen Nausea and vomiting A01* Typhoid and paratyphoid fevers A32* Listeriosis
Pelvic inflammatory disease Within 7 days prior 614.9 Unspecified inflammatory disease of female pelvic organs and tissues N73.9 Female pelvic inflammatory disease, unspecified
Skin and mucosal infections Within 7 days prior
680 Carbuncle and furuncle 681 Cellulitis and abscess of finger and toe 682 Other cellulitis and abscess 683 Acute lymphadenitis 684 Impetigo 685 Pilonidal cyst 686 Other local infections of skin and subcutaneous tissue 035 Eryspelas; 110 Dermatophytosis 111 Dermatomycosis other and unspecified 704.8 Other specified diseases of hair and hair follicles; 728.0 Infective myositis, 611.0 Inflammatory disease of breast, 771.5 Neonatal infective mastitis, 728.86 Necrotizing fasciitis, 380.0 Perichondritis and chondritis of pinna, 380.1 Infective otitis externa (680-686, 035, 110-111, 704.8, 728.0, 611.0, 771.5, 728.86, 380.0-380.1
L00-L08* Infections of the skin and subcutaneous tissue (L00 Staphylococcal scalded skin syndrome, L01 Impetigo, L02 Cutaneous abscess, furuncle and carbuncle, L03 Cellulitis and acute lymphangitis, L04 Acute lymphadenitis, L05 Pilonidal cyst and sinus, L08 Other local infections of skin and subcutaneous tissue), A46* Erysipelas, B35* Dermatophytosis, B36* Other superficial mycoses, L66.3 Perifolliculitis capitis abscedens, L73.8 Other specified follicular disorders, M60.009 Infective myositis, unspecified site, N61.0 Mastitis without abscess, N61.1 Abscess of the breast and nipple, P39.0 Neonatal infective mastitis, M72.6 Necrotizing fasciitis, H61.009 Unspecified perichondritis of external ear, unspecified ear, H61.019 Acute perichondritis of external ear, unspecified ear, H61.029 Chronic perichondritis of external ear, unspecified ear, H61.039 Chondritis of external ear, unspecified ear, H60.00 Abscess of external ear, unspecified ear, H60.10 Cellulitis of external ear, unspecified ear, H60.319 Diffuse otitis externa, unspecified ear, H60.329 Hemorrhagic otitis externa, unspecified ear, H60.399 Other infective otitis externa, unspecified ear, H61.93 Disorder of external ear, unspecified, bilateral, H61.93 Disorder of external ear, unspecified, bilateral, H62.40 Otitis externa in

45
Includes cellulitis, carbuncle/furuncle, impetigo, lymphadenitis, erysipelas, dermatophytosis, folliculitis, myositis, mastitis, necrotizing fasciitis, infective otitis externa)
other diseases classified elsewhere, unspecified ear, H60.20 Malignant otitis externa, unspecified ear, H62.8X1 Other disorders of right external ear in diseases classified elsewhere, H62.8X1 Other disorders of right external ear in diseases classified elsewhere
Other miscellaneous bacterial infections (eg, syphilis, tuberculosis, Lyme disease) Within 7 days prior 010-018 Tuberculosis
A50-A53* Syphilis A15-A19* Tuberculosis A69.20 Lyme disease, unspecified
Acne Within 3 months prior 706.0, 706.1 L70.0 Acne vulgaris L70.2 Acne varioliformis
Miscellaneous bacterial infections not specifically described in macrolide tier, but included in eTable2 of Fleming-Dutra et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-201191 Within 7 days prior
030 Leprosy 032 Diphtheria 036 Meningococcal infection 037 Tetanus 038 Septicemia 039 Actinomycotic infections 040 Other bacterial diseases 041 Bacterial infection in conditions classified elsewhere and of unspecified site 130 Toxoplasmosis 131 Trichomoniasis 132 Pediculosis and phthirus infestation 133 Acariasis 134 Other infestation 135 Sarcoidosis 136 Other and unspecified infectious and parasitic diseases 137 Late effects of tuberculosis 138 Late effects of acute poliomyelitis 139 Late effects of other infectious and parasitic diseases 320 Bacterial meningitis 321 Meningitis due to other organisms 322 Meningitis of unspecified cause 323 Encephalitis myelitis and encephalomyelitis 383 Mastoiditis and related conditions, 475 Peritonsillar abscess
A30* Leprosy [Hansen's disease] A36* Diphtheria A39* Meningococcal infection A35* Other Tetanus A41* Other sepsis, A40* Streptococcal sepsis L08.1 Erythrasma, A42.0 Pulmonary actinomycosis, A42.1 Abdominal actinomycosis, B47.9 Mycetoma, unspecified, A42.81 Actinomycotic meningitis, A42.81 Actinomycotic meningitis, A42.89 Other forms of actinomycosis, A43.8 Other forms of nocardiosis A48.0 Gas gangrene, A48.8 Other specified bacterial diseases, K90.81 Whipple's disease, A48.8 Other specified bacterial diseases, A48.51 Infant botulism, A48.52 Wound botulism, M60.009 Infective myositis, unspecified site, A48.3 Toxic shock syndrome, A48.8 Other specified bacterial diseases B95* Streptococcus, Staphylococcus, and Enterococcus as the cause of diseases classified elsewhere B96* Other bacterial agents as the cause of diseases classified elsewhere B58* Toxoplasmosis; A59* Trichomoniasis; B85* Pediculosis and phthiriasis B86* Scabies; B87* Myiasis; B88 Other infestations B89* Unspecified parasitic disease D86* Sarcoidosis L94.6 Ainhum, M35.2 Behçet's disease, B60.11 Meningoencephalitis due to Acanthamoeba (culbertsoni), B60.19 Other acanthamebic disease, B60.2 Naegleriasis, B59 Pneumocystosis, B60.8 Other specified protozoal diseases, A07.8 Other specified protozoal intestinal diseases, B60.8 Other specified protozoal diseases, B99.8 Other infectious disease, B89 Unspecified parasitic disease, B89 Unspecified parasitic disease B90.9 Sequelae of respiratory and unspecified tuberculosis B91 Sequelae of poliomyelitis, G14 Postpolio syndrome B94.1 Sequelae of viral encephalitis, B94.0 Sequelae of trachoma, B94.8 Sequelae of other specified infectious and parasitic diseases, B94.9 Sequelae of unspecified infectious and parasitic disease G00* Bacterial meningitis, not elsewhere classified, G01* Meningitis in bacterial diseases classified elsewhere B45.1 Cerebral cryptococcosis G02 Meningitis in other infectious and parasitic diseases classified elsewhere G03.0 Nonpyogenic meningitis G04* Encephalitis, myelitis and encephalomyelitis G05* Encephalitis, myelitis and encephalomyelitis in diseases classified elsewhere G92* Toxic encephalopathy H70* Mastoiditis and related conditions, J36* Peritonsillar abscess

46
Antibiotics unnecessary, All other conditions including
Asthma Within 3 months prior 493 Asthma, 995.3 Allergy, unspecified J45* Asthma, T78.40XA Allergy, unspecified, initial encounter
Allergic rhinitis Within 3 months prior 477 Allergic rhinitis
J30.9 Allergic rhinitis, unspecified; Add after reviewing fx table: J302 Other seasonal allergic rhinitis; J301 Allergic rhinitis due to pollen
Nonsuppurative otitis media Within 7 days prior 381: Non-suppurative otitis media and Eustachian tube disorders H65* Nonsuppurative otitis media
Acute bronchitis and bronchiolitis Within 7 days prior
490 Bronchitis, not specified as acute or chronic, 466 Acute bronchitis and bronchiolitis
J40* Bronchitis, not specified as acute or chronic, J20.9 Acute bronchitis, unspecified, Add after reviewing fx table: J219 Acute bronchiolitis, unspecified; J210 Acute bronchiolitis due to respiratory syncytial v
Influenza Within 7 days prior 487 Influenza, 488 Influenza due to identified avian influenza virus
J09.X1 Influenza due to identified novel influenza A virus with pneumonia J09.X2 Influenza due to identified novel influenza A virus with other respiratory manifestations J09.X3 Influenza due to identified novel influenza A virus with gastrointestinal manifestations J09.X9 Influenza due to identified novel influenza A virus with other manifestations J10* Influenza due to other identified influenza virus J11* Influenza due to unidentified influenza virus
Viral upper respiratory infection,Viral pneumonia/common cold Within 7 days prior
480: Viral pneumonia, 460: Acute nasopharyngitis [common cold], 464 Acute laryngitis and tracheitis, 465 Acute upper respiratory infections of multiple or unspecified sites, 786.2 Cough
J12* Viral pneumonia, not elsewhere classified J00* Acute nasopharyngitis [common cold], J06.9 Acute upper respiratory infections of multiple or unspecified sites, R05 Cough Add after reviewing fx table: J050 Acute obstructive laryngitis (croup); J040 Acute laryngitis; B349 Viral infection, unspecified

Appendix 2 – Diagnosis codes of FFS macrolides not after sick visit
I. Diagnosis codes submitted during the year by diagnosis frequency
Dx Code Diagnosis Name Freq Patients
I10 ESSENTIAL (PRIMARY) HYPERTENSION 1636 211
F17210 NICOTINE DEPENDENCE, CIGARETTES, UNCOMPLICATED 1294 237
J449 CHRONIC OBSTRUCTIVE PULMONARY DISEASE, UNSPECIFIED 1123 90
R0902 HYPOXEMIA 1099 135
F1120 OPIOID DEPENDENCE, UNCOMPLICATED 1014 58
E119 TYPE 2 DIABETES MELLITUS WITHOUT COMPLICATIONS 990 95
R05 COUGH 909 372
J189 PNEUMONIA, UNSPECIFIED ORGANISM 851 156
R109 UNSPECIFIED ABDOMINAL PAIN 839 216
F1520 OTHER STIMULANT DEPENDENCE, UNCOMPLICATED 787 25
F419 ANXIETY DISORDER, UNSPECIFIED 771 192
E860 ACC POISON-ALCOHOL NEC 762 106
E860 DEHYDRATION 762 106
Z87891 PERSONAL HISTORY OF NICOTINE DEPENDENCE 729 144
K219 GASTRO-ESOPHAGEAL REFLUX DISEASE WITHOUT ESOPHAGIT 722 163
M545 LOW BACK PAIN 711 165
Z23 ENCOUNTER FOR IMMUNIZATION 652 354
F329 MAJOR DEPRESSIVE DISORDER, SINGLE EPISODE, UNSPECI 636 170
G8929 OTHER CHRONIC PAIN 621 129
N390 URINARY TRACT INFECTION, SITE NOT SPECIFIED 607 113
R0602 SHORTNESS OF BREATH 562 201
R633 FEEDING DIFFICULTIES 559 26
E876 HYPOKALEMIA 552 52
E876 MED MISADVENTURE NEC/NOS 552 52
R112 NAUSEA WITH VOMITING, UNSPECIFIED 546 126
J9601 ACUTE RESPIRATORY FAILURE WITH HYPOXIA 530 50
R51 HEADACHE 526 169
R079 CHEST PAIN, UNSPECIFIED 518 126
J069 ACUTE UPPER RESPIRATORY INFECTION, UNSPECIFIED 506 220
J45909 UNSPECIFIED ASTHMA, UNCOMPLICATED 502 135
G4733 OBSTRUCTIVE SLEEP APNEA (ADULT) (PEDIATRIC) 493 71
R509 FEVER, UNSPECIFIED 491 199
N186 END STAGE RENAL DISEASE 473 7
Z794 LONG TERM (CURRENT) USE OF INSULIN 469 55
J441 CHRONIC OBSTRUCTIVE PULMONARY DISEASE W (ACUTE) EX 450 62
A419 SEPSIS, UNSPECIFIED ORGANISM 444 48
E871 HYPO-OSMOLALITY AND HYPONATREMIA 438 41
E871 POST-OP FOREIGN BODY 438 41
R1310 DYSPHAGIA, UNSPECIFIED 416 60
G40909 EPILEPSY, UNSP, NOT INTRACTABLE, WITHOUT STATUS EP 409 49
J209 ACUTE BRONCHITIS, UNSPECIFIED 400 155

48
Dx Code Diagnosis Name Freq Patients
R69 ILLNESS, UNSPECIFIED 395 25
Z79899 OTHER LONG TERM (CURRENT) DRUG THERAPY 391 123
E1165 TYPE 2 DIABETES MELLITUS WITH HYPERGLYCEMIA 390 42
Z00129 ENCNTR FOR ROUTINE CHILD HEALTH EXAM W/O ABNORMAL 380 183
E039 HYPOTHYROIDISM, UNSPECIFIED 379 98
J029 ACUTE PHARYNGITIS, UNSPECIFIED 373 184
F319 BIPOLAR DISORDER, UNSPECIFIED 371 45
Z79891 LONG TERM (CURRENT) USE OF OPIATE ANALGESIC 359 37
F411 GENERALIZED ANXIETY DISORDER 353 96
F1420 COCAINE DEPENDENCE, UNCOMPLICATED 352 5
F17200 NICOTINE DEPENDENCE, UNSPECIFIED, UNCOMPLICATED 350 126
E875 CONTAMINATION 344 16
E875 HYPERKALEMIA 344 16
E840 CYSTIC FIBROSIS WITH PULMONARY MANIFESTATIONS 342 7
E840 TAKEOFF/LANDING ACCIDENT 342 7
I2510 ATHSCL HEART DISEASE OF NATIVE CORONARY ARTERY W/O 332 33
J9621 ACUTE AND CHRONIC RESPIRATORY FAILURE WITH HYPOXIA 328 29
J9620 ACUTE AND CHR RESP FAILURE, UNSP W HYPOXIA OR HYPE 323 12
F71 MODERATE INTELLECTUAL DISABILITIES 320 7
D649 ANEMIA, UNSPECIFIED 317 66
R197 DIARRHEA, UNSPECIFIED 315 108
E6601 MORBID (SEVERE) OBESITY DUE TO EXCESS CALORIES 303 74
K5900 CONSTIPATION, UNSPECIFIED 295 98
Z5189 ENCOUNTER FOR OTHER SPECIFIED AFTERCARE 290 8
Z931 GASTROSTOMY STATUS 286 29
Q251 COARCTATION OF AORTA 285 3
G800 SPASTIC QUADRIPLEGIC CEREBRAL PALSY 285 14
F332 MAJOR DEPRESSV DISORDER, RECURRENT SEVERE W/O PSYC 284 20
R531 WEAKNESS 284 84
R5383 OTHER FATIGUE 283 117
Z720 TOBACCO USE 282 95
R0600 DYSPNEA, UNSPECIFIED 276 94
R918 OTHER NONSPECIFIC ABNORMAL FINDING OF LUNG FIELD 274 101
G809 CEREBRAL PALSY, UNSPECIFIED 273 13
I509 HEART FAILURE, UNSPECIFIED 273 42
M549 DORSALGIA, UNSPECIFIED 272 99
F89 UNSPECIFIED DISORDER OF PSYCHOLOGICAL DEVELOPMENT 268 32
F1020 ALCOHOL DEPENDENCE, UNCOMPLICATED 267 22
R1013 EPIGASTRIC PAIN 266 73
G4700 INSOMNIA, UNSPECIFIED 262 86
R102 PELVIC AND PERINEAL PAIN 262 84
Z3490 ENCNTR FOR SUPRVSN OF NORMAL PREGNANCY, UNSP, UNSP 254 83
R569 UNSPECIFIED CONVULSIONS 253 57
E872 ACIDOSIS 250 30
Z431 ENCOUNTER FOR ATTENTION TO GASTROSTOMY 250 16
E872 FAILURE STERILE PROCEDRE 250 30
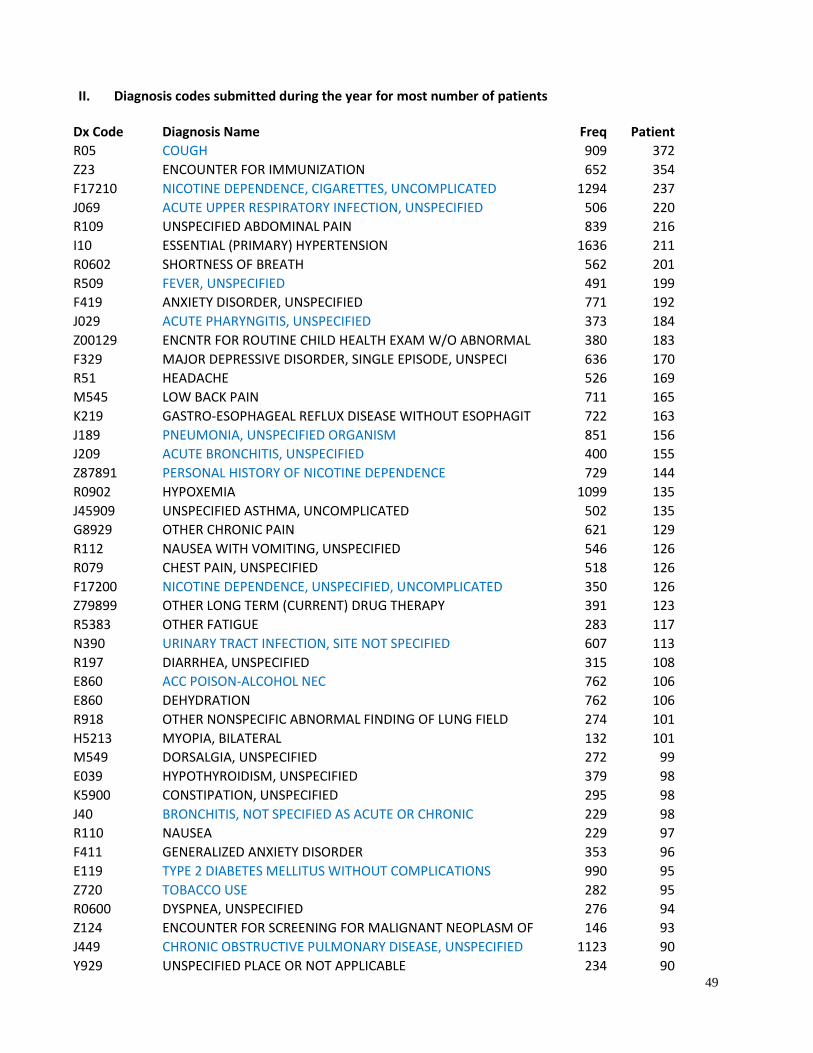
49
II. Diagnosis codes submitted during the year for most number of patients
Dx Code Diagnosis Name
Freq
Patient
R05 COUGH 909 372
Z23 ENCOUNTER FOR IMMUNIZATION 652 354
F17210 NICOTINE DEPENDENCE, CIGARETTES, UNCOMPLICATED 1294 237
J069 ACUTE UPPER RESPIRATORY INFECTION, UNSPECIFIED 506 220
R109 UNSPECIFIED ABDOMINAL PAIN 839 216
I10 ESSENTIAL (PRIMARY) HYPERTENSION 1636 211
R0602 SHORTNESS OF BREATH 562 201
R509 FEVER, UNSPECIFIED 491 199
F419 ANXIETY DISORDER, UNSPECIFIED 771 192
J029 ACUTE PHARYNGITIS, UNSPECIFIED 373 184
Z00129 ENCNTR FOR ROUTINE CHILD HEALTH EXAM W/O ABNORMAL 380 183
F329 MAJOR DEPRESSIVE DISORDER, SINGLE EPISODE, UNSPECI 636 170
R51 HEADACHE 526 169
M545 LOW BACK PAIN 711 165
K219 GASTRO-ESOPHAGEAL REFLUX DISEASE WITHOUT ESOPHAGIT 722 163
J189 PNEUMONIA, UNSPECIFIED ORGANISM 851 156
J209 ACUTE BRONCHITIS, UNSPECIFIED 400 155
Z87891 PERSONAL HISTORY OF NICOTINE DEPENDENCE 729 144
R0902 HYPOXEMIA 1099 135
J45909 UNSPECIFIED ASTHMA, UNCOMPLICATED 502 135
G8929 OTHER CHRONIC PAIN 621 129
R112 NAUSEA WITH VOMITING, UNSPECIFIED 546 126
R079 CHEST PAIN, UNSPECIFIED 518 126
F17200 NICOTINE DEPENDENCE, UNSPECIFIED, UNCOMPLICATED 350 126
Z79899 OTHER LONG TERM (CURRENT) DRUG THERAPY 391 123
R5383 OTHER FATIGUE 283 117
N390 URINARY TRACT INFECTION, SITE NOT SPECIFIED 607 113
R197 DIARRHEA, UNSPECIFIED 315 108
E860 ACC POISON-ALCOHOL NEC 762 106
E860 DEHYDRATION 762 106
R918 OTHER NONSPECIFIC ABNORMAL FINDING OF LUNG FIELD 274 101
H5213 MYOPIA, BILATERAL 132 101
M549 DORSALGIA, UNSPECIFIED 272 99
E039 HYPOTHYROIDISM, UNSPECIFIED 379 98
K5900 CONSTIPATION, UNSPECIFIED 295 98
J40 BRONCHITIS, NOT SPECIFIED AS ACUTE OR CHRONIC 229 98
R110 NAUSEA 229 97
F411 GENERALIZED ANXIETY DISORDER 353 96
E119 TYPE 2 DIABETES MELLITUS WITHOUT COMPLICATIONS 990 95
Z720 TOBACCO USE 282 95
R0600 DYSPNEA, UNSPECIFIED 276 94
Z124 ENCOUNTER FOR SCREENING FOR MALIGNANT NEOPLASM OF 146 93
J449 CHRONIC OBSTRUCTIVE PULMONARY DISEASE, UNSPECIFIED 1123 90
Y929 UNSPECIFIED PLACE OR NOT APPLICABLE 234 90
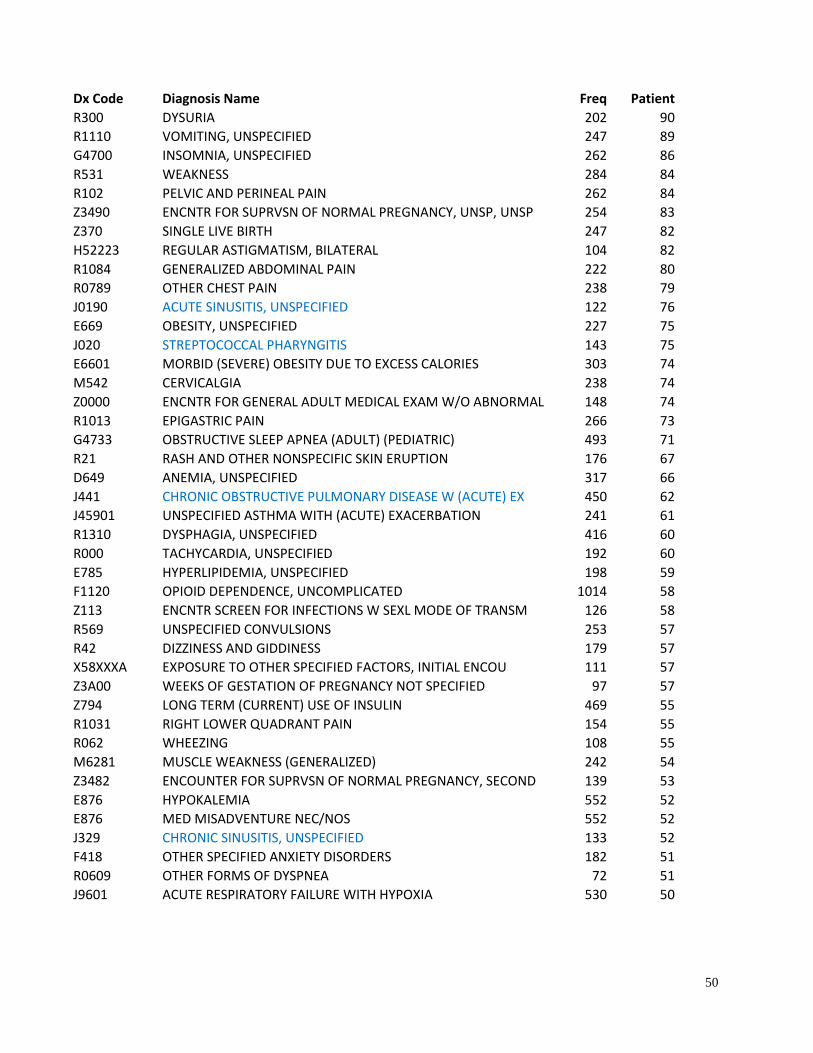
50
Dx Code Diagnosis Name
Freq
Patient
R300 DYSURIA 202 90
R1110 VOMITING, UNSPECIFIED 247 89
G4700 INSOMNIA, UNSPECIFIED 262 86
R531 WEAKNESS 284 84
R102 PELVIC AND PERINEAL PAIN 262 84
Z3490 ENCNTR FOR SUPRVSN OF NORMAL PREGNANCY, UNSP, UNSP 254 83
Z370 SINGLE LIVE BIRTH 247 82
H52223 REGULAR ASTIGMATISM, BILATERAL 104 82
R1084 GENERALIZED ABDOMINAL PAIN 222 80
R0789 OTHER CHEST PAIN 238 79
J0190 ACUTE SINUSITIS, UNSPECIFIED 122 76
E669 OBESITY, UNSPECIFIED 227 75
J020 STREPTOCOCCAL PHARYNGITIS 143 75
E6601 MORBID (SEVERE) OBESITY DUE TO EXCESS CALORIES 303 74
M542 CERVICALGIA 238 74
Z0000 ENCNTR FOR GENERAL ADULT MEDICAL EXAM W/O ABNORMAL 148 74
R1013 EPIGASTRIC PAIN 266 73
G4733 OBSTRUCTIVE SLEEP APNEA (ADULT) (PEDIATRIC) 493 71
R21 RASH AND OTHER NONSPECIFIC SKIN ERUPTION 176 67
D649 ANEMIA, UNSPECIFIED 317 66
J441 CHRONIC OBSTRUCTIVE PULMONARY DISEASE W (ACUTE) EX 450 62
J45901 UNSPECIFIED ASTHMA WITH (ACUTE) EXACERBATION 241 61
R1310 DYSPHAGIA, UNSPECIFIED 416 60
R000 TACHYCARDIA, UNSPECIFIED 192 60
E785 HYPERLIPIDEMIA, UNSPECIFIED 198 59
F1120 OPIOID DEPENDENCE, UNCOMPLICATED 1014 58
Z113 ENCNTR SCREEN FOR INFECTIONS W SEXL MODE OF TRANSM 126 58
R569 UNSPECIFIED CONVULSIONS 253 57
R42 DIZZINESS AND GIDDINESS 179 57
X58XXXA EXPOSURE TO OTHER SPECIFIED FACTORS, INITIAL ENCOU 111 57
Z3A00 WEEKS OF GESTATION OF PREGNANCY NOT SPECIFIED 97 57
Z794 LONG TERM (CURRENT) USE OF INSULIN 469 55
R1031 RIGHT LOWER QUADRANT PAIN 154 55
R062 WHEEZING 108 55
M6281 MUSCLE WEAKNESS (GENERALIZED) 242 54
Z3482 ENCOUNTER FOR SUPRVSN OF NORMAL PREGNANCY, SECOND 139 53
E876 HYPOKALEMIA 552 52
E876 MED MISADVENTURE NEC/NOS 552 52
J329 CHRONIC SINUSITIS, UNSPECIFIED 133 52
F418 OTHER SPECIFIED ANXIETY DISORDERS 182 51
R0609 OTHER FORMS OF DYSPNEA 72 51
J9601 ACUTE RESPIRATORY FAILURE WITH HYPOXIA 530 50

51
Appendix 3
Aminopenicillins
Amoxicillin
Ampicillin
Beta-Lactamase Inhibitors
Amoxicillin-Clavulanate
First-Generation Cephalosporins
Cefadroxil
Cephalexin
Folate Antagonists
Trimethoprim
Lincomycin Derivatives
Clindamycin
Miscellaneous Antibiotics
Linezolid
Vancomycin
Natural Penicillins
Penicillin V Potassium
Penicillinase-Resistant Penicillins
Dicloxacillin
Quinolones
Ciprofloxacin
Levofloxacin
Moxifloxacin
Second-Generation Cephalosporins
Cefaclor
Cefprozil
Cefuroxime
Sulfonamides
Sulfamethoxazole-Trimethoprim
Tetracyclines
Doxycycline
Minocycline
Tetracycline
Third-Generation Cephalosporins
Cefdinir
Cefixime
Cefpodoxime
52
References 1. UpToDate. Beta-lactam antibiotics: Mechanisms of action and resistance and adverse effects.
https://www-uptodate-com.ezproxy.lib.utah.edu/contents/beta-lactam-antibiotics-mechanisms-of-action-and-resistance-and-adverse-effects?source=machineLearning&search=antibiotic%20side%20effects&selectedTitle=1~150§ionRank=1&anchor=H9#H9. Accessed 25 September 2017.
2. Gold HS, Moellering RC, Jr. Antimicrobial-drug resistance. N Engl J Med. 1996;335(19):1445-1453. 3. Pitout JD, Sanders CC, Sanders WE, Jr. Antimicrobial resistance with focus on beta-lactam resistance
in gram-negative bacilli. Am J Med. 1997;103(1):51-59. 4. Centers for Disease Control and prevention (CDC). Antibiotic Resistance Threats in the United States,
2013. https://www.cdc.gov/drugresistance/threat-report-2013/. 5. Goldman JL, Jackson MA. Tip of the Iceberg: Understanding the Unintended Consequences of
Antibiotics. Pediatrics. 2015;136(2):e492-493. 6. Dethlefsen L, Huse S, Sogin ML, Relman DA. The pervasive effects of an antibiotic on the human gut
microbiota, as revealed by deep 16S rRNA sequencing. PLoS Biol. 2008;6(11):e280. 7. Wu HJ, Ivanov, II, Darce J, et al. Gut-residing segmented filamentous bacteria drive autoimmune
arthritis via T helper 17 cells. Immunity. 2010;32(6):815-827. 8. Bailey LC, Forrest CB, Zhang P, Richards TM, Livshits A, DeRusso PA. Association of antibiotics in
infancy with early childhood obesity. JAMA Pediatr. 2014;168(11):1063-1069. 9. Kronman MP, Zaoutis TE, Haynes K, Feng R, Coffin SE. Antibiotic exposure and IBD development
among children: a population-based cohort study. Pediatrics. 2012;130(4):e794-803. 10. Saari A, Virta LJ, Sankilampi U, Dunkel L, Saxen H. Antibiotic exposure in infancy and risk of being
overweight in the first 24 months of life. Pediatrics. 2015;135(4):617-626. 11. Horton DB, Scott FI, Haynes K, et al. Antibiotic Exposure and Juvenile Idiopathic Arthritis: A Case-
Control Study. Pediatrics. 2015;136(2):e333-343. 12. Centers for Disease Control and prevention (CDC). Get Smart: Know When Antibiotics Work in
Doctor’s Offices https://www.cdc.gov/getsmart/community/index.html. Accessed 20 September 2017.
13. Centers for Disease Control and prevention (CDC). 2017 Antibiotic use in the United States Progress and opportunities. https://www.cdc.gov/getsmart/pdf/stewardship-report.pdf.
14. Vaz LE, Kleinman KP, Lakoma MD, et al. Prevalence of Parental Misconceptions About Antibiotic Use. Pediatrics. 2015;136(2):221-231.
15. UpToDate. Graziani, A.L. et al. Azithromycin, clarithromycin, and telithromycin. Literature review current through: Jun 2018. This topic last updated: Jun 04, 2018.
16. Azithromycin (Systemic) (Lexi-Drugs). http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/1768824#f_pharmacology-and-pharmacokinetics. Accessed 1 August 2018.
17. Hansen MP, Thorning S, Aronson JK, et al. Adverse events in patients taking macrolide antibiotics versus placebo for any indication. Cochrane Database of Systematic Reviews. 2015(8).
18. Hicks LA, Taylor TH, Jr., Hunkler RJ. U.S. outpatient antibiotic prescribing, 2010. N Engl J Med. 2013;368(15):1461-1462.
19. Intermountain Care Process Model. Diagnosis and management of Community-Acquired Pneumonia (CAP). June 2016 Update. https://intermountainhealthcare.org/ext/Dcmnt?ncid=520102603. Accessed 6 August 2018.
20. Fidaxomicin (Lexi-Drugs). http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/3451543. Accessed 1 August 2018.
21. University of Utah Health. https://healthcare.utah.edu/. 22. Intermountain Healthcare. https://intermountainhealthcare.org/.

53
23. National Quality Measures Clearinghouse (NQMC). Measure summary: Sickle cell disease (SCD): percentage of children in a state between the ages of 3 months and 5 years diagnosed with SCD who received appropriate antibiotic prophylaxis for at least 350 days during the measurement year. In: National Quality Measures Clearinghouse (NQMC) [Web site]. Rockville (MD): Agency for Healthcare Research and Quality (AHRQ); 2013 Dec 13. [cited 2017 Sep 21]. Available: https://www.qualitymeasures.ahrq.gov.
24. O'Reilly R, Elphick HE. Development, clinical utility, and place of ivacaftor in the treatment of cystic fibrosis. Drug design, development and therapy. 2013;7:929-937.
25. Diseases and Conditions - Cystic fibrosis - Treatments and drugs By Mayo Clinic Staff. http://www.mayoclinic.org/diseases-conditions/cystic-fibrosis/basics/treatment/con-20013731. Accessed 19 August 2015.
26. Understanding the complexities of treatment - Cystic Fibrosis, Andrea Peterson, PharmD. http://www.freece.com/FreeCE/Cal_Details.aspx?ID=32f98560-5651-4798-8008-0d01a1293413.
27. Mogayzel PJ Jr, Naureckas ET, Robinson KA, Mueller G, Hadjiliadis D, Hoag JB, Lubsch L, Hazle L, Sabadosa K, Marshall B, Pulmonary Clinical Practice Guidelines Committee. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013 Apr 1;187(7):680-9. [90 references]. http://www.guideline.gov/content.aspx?id=45307.
28. UpToDate. Treatment of acne vulgaris. https://www-uptodate-com.ezproxy.lib.utah.edu/contents/treatment-of-acne-vulgaris?source=search_result&search=antibiotic&selectedTitle=34~150#H24. Accessed 25 September 2017.
29. Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. Journal of the American Academy of Dermatology. 2016;74(5):945-973 e933.
30. Del Rosso JQ, Kim G. Optimizing use of oral antibiotics in acne vulgaris. Dermatol Clin. 2009;27(1):33-42.
31. Dean, N.C. Diagnosis and management of acute respiratory tract infections. . https://intermountainphysician.org/intermountaincme/Documents/Dean%2010.25.16%20CME-LRTIfall2016.pdf.
32. UpToDate. Antimicrobial stewardship in outpatient settings. https://www-uptodate-com.ezproxy.lib.utah.edu/contents/antimicrobial-stewardship-in-outpatient-settings?source=search_result&search=antibiotic%20resistance&selectedTitle=3~150. Accessed 21 September 2017.
33. Pharmacist's Letter. Expect to See Shorter Antibiotic Courses to Help Limit Resistance. November 2016. https://pharmacist.therapeuticresearch.com/Content/Articles/PL/2016/Nov/Expect-to-See-Shorter-Antibiotic-Courses-to-Help-Limit-Resistance.
34. Antibiotic-Associated Adverse Events Common - Medscape - Jun 12, 2017. http://www.medscape.com/viewarticle/881459.
35. Tamma PD, Avdic E, Li DX, Dzintars K, Cosgrove SE. Association of adverse events with antibiotic use in hospitalized patients. JAMA Internal Medicine. 2017;177(9):1308-1315.
36. UpToDate. Hicks, C.B. et al. Syphilis: Treatment and monitoring. Literature review current through: Jun 2018. | This topic last updated: May 21, 2018. https://www-uptodate-com.ezproxy.lib.utah.edu/contents/syphilis-treatment-and-monitoring?topicRef=474&source=see_link.
37. Health Care Home. News & Announcements 2015 July. Health Care Providers A Major Contributor to Problem of Antibiotic Overuse. https://healthcare.utah.edu/publicaffairs/news/2015/07/072015_Health-care-providers-major-contributor-to-antibiotic-overuse.php.
38. Jones BE, Sauer B, Jones MM, et al. Variation in Outpatient Antibiotic Prescribing for Acute Respiratory Infections in the Veteran Population: A Cross-sectional Study. Ann Intern Med. 2015;163(2):73-80.
54
39. Sanchez GV, Shapiro DJ, Hersh AL, Hicks LA, Fleming-Dutra KE. Outpatient Macrolide Antibiotic Prescribing in the United States, 2008-2011. Open Forum Infect Dis. 2017;4(4):ofx220.
40. Bartlett JG, Auwaerter PG, Pham PA.The Johns Hopkins Antibiotic Guide: Diagnosis and Treatment of Infectious Diseases . 3rd ed. Sudbury, MA: Jones and Bartlett Publishers; 2012.
41. Clarithromycin (Lexi-Drugs) http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/6628?hl=Antibiotic, Macrolide#f_uses. Accessed 8 August 2018.
42. Erythromycin (Systemic) (Lexi-Drugs). http://online.lexi.com/lco/action/doc/retrieve/docid/patch_f/1831759#f_uses. Accessed 8 August 2018.
43. Micromedex. Erythromycin Ethylsuccinate http://www.micromedexsolutions.com/micromedex2/librarian/CS/6A8C8F/ND_PR/evidencexpert/ND_P/evidencexpert/DUPLICATIONSHIELDSYNC/9B8106/ND_PG/evidencexpert/ND_B/evidencexpert/ND_AppProduct/evidencexpert/ND_T/evidencexpert/PFActionId/evidencexpert.DoIntegratedSearch?SearchTerm=Erythromycin+Ethylsuccinate&fromInterSaltBase=true&false=null&false=null&=null#close. Accessed 8 August 2018.
44. Micromedex. Erythromycin Stearate http://www.micromedexsolutions.com/micromedex2/librarian/CS/94481D/ND_PR/evidencexpert/ND_P/evidencexpert/DUPLICATIONSHIELDSYNC/36EECD/ND_PG/evidencexpert/ND_B/evidencexpert/ND_AppProduct/evidencexpert/ND_T/evidencexpert/PFActionId/evidencexpert.DoIntegratedSearch?SearchTerm=Erythromycin+Stearate&fromInterSaltBase=true&false=null&false=null&=null#. Accessed 8 August 2018.
45. Erythromycin (Systemic) (AHFS Essentials (Adult and Pediatric)). http://online.lexi.com/lco/action/doc/retrieve/docid/essential_ashp/6444249#uses-nested. Accessed 22 August 2018.
46. Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44 Suppl 2:S27-72.
47. Griffith DE, Aksamit T, Brown-Elliott BA, et al. An official ATS/IDSA statement: diagnosis, treatment, and prevention of nontuberculous mycobacterial diseases. Am J Respir Crit Care Med. 2007;175(4):367-416.
48. Tiwari T, Murphy TV, Moran J. Recommended antimicrobial agents for the treatment and postexposure prophylaxis of pertussis: 2005 CDC Guidelines. MMWR Recomm Rep. 2005;54(RR-14):1-16.
49. Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis. 2014;59(2):e10-52.
50. HHS Guidelines for the Prevention and Treatment of Opportunistic Infections in HIV-Infected Adults and Adolescents. Bartonellosis. Last Updated: May 7, 2013. https://aidsinfo.nih.gov/guidelines/brief-html/4/adult-and-adolescent-opportunistic-infection/329/bartonellosis.
51. Workowski KA. Centers for Disease Control and Prevention Sexually Transmitted Diseases Treatment Guidelines. Clin Infect Dis. 2015;61 Suppl 8:S759-762.
52. Workowski KA, Bolan GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137.
53. Wormser GP, Dattwyler RJ, Shapiro ED, et al. The clinical assessment, treatment, and prevention of lyme disease, human granulocytic anaplasmosis, and babesiosis: clinical practice guidelines by the Infectious Diseases Society of America. Clin Infect Dis. 2006;43(9):1089-1134.
54. Shane AL, Mody RK, Crump JA, et al. 2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea. Clin Infect Dis. 2017;65(12):1963-1973.

55
55. CDC Yellowbook. Chapter 2 The Pretravel Consultation. Self-Treatable Conditions. https://wwwnc.cdc.gov/travel/yellowbook/2018/the-pre-travel-consultation/travelers-diarrhea. Accessed 8 August 2018.
56. Riddle MS, DuPont HL, Connor BA. ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults. Am J Gastroenterol. 2016;111(5):602-622.
57. Global Initiative for Chronic Obstructive Lung Disease 2018 Report. https://goldcopd.org/wp-content/uploads/2017/11/GOLD-2018-v6.0-FINAL-revised-20-Nov_WMS.pdf. Accessed 8 August 2018.
58. Southern KW, Barker PM, Solis-Moya A, Patel L. Macrolide antibiotics for cystic fibrosis. Cochrane Database of Systematic Reviews. 2012(11).
59. Mogayzel PJ, Jr., Naureckas ET, Robinson KA, et al. Cystic fibrosis pulmonary guidelines. Chronic medications for maintenance of lung health. Am J Respir Crit Care Med. 2013;187(7):680-689.
60. Equi A, Balfour-Lynn IM, Bush A, Rosenthal M. Long term azithromycin in children with cystic fibrosis: a randomised, placebo-controlled crossover trial. Lancet. 2002;360(9338):978-984.
61. Saiman L, Marshall BC, Mayer-Hamblett N, et al. Azithromycin in patients with cystic fibrosis chronically infected with Pseudomonas aeruginosa: a randomized controlled trial. Jama. 2003;290(13):1749-1756.
62. Wolter J, Seeney S, Bell S, Bowler S, Masel P, McCormack J. Effect of long term treatment with azithromycin on disease parameters in cystic fibrosis: a randomised trial. Thorax. 2002;57(3):212-216.
63. Centers for Disease Control and Prevention (CDC). Antibiotic Prescribing and Use in Doctor’s Offices. Outpatient Healthcare Professionals. Pediatric Treatment Recommendations. https://www.cdc.gov/antibiotic-use/community/for-hcp/outpatient-hcp/pediatric-treatment-rec.html. Accessed 22 August 2018.
64. Hersh AL, Jackson MA, Hicks LA, American Academy of Pediatrics Committee on Infectious D. Principles of judicious antibiotic prescribing for upper respiratory tract infections in pediatrics. Pediatrics. 2013;132(6):1146-1154.
65. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55(10):1279-1282.
66. Chow AW, Benninger MS, Brook I, et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54(8):e72-e112.
67. Wald ER, Applegate KE, Bordley C, et al. Clinical practice guideline for the diagnosis and management of acute bacterial sinusitis in children aged 1 to 18 years. Pediatrics. 2013;132(1):e262-280.
68. Lieberthal AS, Carroll AE, Chonmaitree T, et al. The diagnosis and management of acute otitis media. Pediatrics. 2013;131(3):e964-999.
69. Coker TR, Chan LS, Newberry SJ, et al. Diagnosis, microbial epidemiology, and antibiotic treatment of acute otitis media in children: a systematic review. Jama. 2010;304(19):2161-2169.
70. White B. Diagnosis and treatment of urinary tract infections in children. Am Fam Physician. 2011;83(4):409-415.
71. Subcommittee on Urinary Tract Infection SCoQI, Management, Roberts KB. Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics. 2011;128(3):595-610.
72. Savaris RF, Fuhrich DG, Duarte RV, Franik S, Ross J. Antibiotic therapy for pelvic inflammatory disease. Cochrane Database of Systematic Reviews. 2017(4).
73. Erythrasma. https://medlineplus.gov/ency/article/001470.htm. Accessed 22 August 2018. 74. Wilson W, Taubert KA, Gewitz M, et al. Prevention of infective endocarditis: guidelines from the
American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality

56
of Care and Outcomes Research Interdisciplinary Working Group. Circulation. 2007;116(15):1736-1754.
75. Fashner J, Ericson K, Werner S. Treatment of the common cold in children and adults. Am Fam Physician. 2012;86(2):153-159.
76. Ralston SL, Lieberthal AS, Meissner HC, et al. Clinical practice guideline: the diagnosis, management, and prevention of bronchiolitis. Pediatrics. 2014;134(5):e1474-1502.
77. Laopaiboon M, Panpanich R, Swa Mya K. Azithromycin for acute lower respiratory tract infections. Cochrane Database of Systematic Reviews. 2015(3).
78. Herath SC, Poole P. Prophylactic antibiotic therapy for chronic obstructive pulmonary disease (COPD). Cochrane Database of Systematic Reviews. 2013(11).
79. Romero L, Huerfano C, Grillo-Ardila CF. Macrolides for treatment of Haemophilus ducreyi infection in sexually active adults. Cochrane Database of Systematic Reviews. 2017(12).
80. O'Farrell N, Lazaro N. UK national guideline for the management of chancroid 2014. International Journal of STD & AIDS 2014;25(14):975‐83.
81. World Health Organization. Guidelines for the control of shigellosis, including epidemics due to Shigella dysenteriae type 1. http://apps.who.int/iris/bitstream/handle/10665/43252/924159330X.pdf;jsessionid=22043002F7FC0FF4035BE12F8B59E31E?sequence=1. Accessed 8 August 2018.
82. Fashner J, Gitu AC. Diagnosis and Treatment of Peptic Ulcer Disease and H. pylori Infection. Am Fam Physician. 2015;91(4):236-242.
83. Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical guideline: management of gastroparesis. Am J Gastroenterol. 2013;108(1):18-37; quiz 38.
84. Head K, Chong LY, Piromchai P, et al. Systemic and topical antibiotics for chronic rhinosinusitis. Cochrane Database of Systematic Reviews. 2016(4).
85. Perletti G, Marras E, Wagenlehner FME, Magri V. Antimicrobial therapy for chronic bacterial prostatitis. Cochrane Database of Systematic Reviews. 2013(8).
86. Kew KM, Undela K, Kotortsi I, Ferrara G. Macrolides for chronic asthma. Cochrane Database of Systematic Reviews. 2015(9).
87. Normansell R, Sayer B, Waterson S, Dennett EJ, Del Forno M, Dunleavy A. Antibiotics for exacerbations of asthma. Cochrane Database of Systematic Reviews. 2018(6).
88. Lin X, Lu J, Yang M, Dong BR, Wu HM. Macrolides for diffuse panbronchiolitis. Cochrane Database of Systematic Reviews. 2015(1).
89. U.S. Department of Health and Human Services Centers for Disease Control and Prevention (CDC). CDC Public Health Grand Rounds. Be antibiotic aware: Smart Use, Best Care. May 15, 2018. https://www.cdc.gov/grand-rounds/pp/2018/20180515-presentation-antibiotics-aware-H.pdf. Accessed 8 August 2018.
90. Centers for Disease Control and Prevention (CDC). Outpatient Antibiotic Prescriptions — United States, 2015. https://www.cdc.gov/grand-rounds/pp/2018/20180515-presentation-antibiotics-aware-H.pdf. Accessed 8 August 2018.
91. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of Inappropriate Antibiotic Prescriptions Among US Ambulatory Care Visits, 2010-2011. Jama. 2016;315(17):1864-1873.