Embed Size (px)
Citation preview
Utah Medicaid Pharmacy and Therapeutics Committee
Drug Class Review
Vesicular Monoamine Transporter 2 Inhibitors and
Anticholinergic Agents for Movement Disorders
AHFS Classification: 28:56 Vesicular Monoamine Transporter 2 (VMAT2) Inhibitors
Deutetrabenazine (Austedo) Tetrabenazine (Xenazine, generic)
Valbenazine (Ingrezza)
AHFS Classification: 28:36.08 Anticholinergic Agents
Benztropine (Cogentin, generic) Trihexyphenidyl (generic)
Final Report
March 2018
Review prepared by: Elena Martinez Alonso, B.Pharm., Medical Writer Vicki Frydrych, B.Pharm., Pharm.D., Clinical Pharmacist Valerie Gonzales, Pharm.D., Clinical Pharmacist Joanita Lake, B.Pharm., MSc EBHC (Oxon), Research Assistant Professor, Clinical Pharmacist Michelle Fiander, MA, MLIS, Research Assistant Professor, Evidence Synthesis Librarian Joanne LaFleur, PharmD, MSPH, Associate Professor University of Utah College of Pharmacy University of Utah College of Pharmacy, Drug Regimen Review Center Copyright © 2018 by University of Utah College of Pharmacy Salt Lake City, Utah. All rights reserved

2
Contents Executive Summary ........................................................................................................................ 3
Introduction ..................................................................................................................................... 6
Table 1. FDA-Approved Movement Disorder Agents ........................................................... 6
Disease Overview and Guideline Recommendations ................................................................. 8
Table 2. Clinical Practice Guideline Recommendations ...................................................... 13
Pharmacology & Special Populations ........................................................................................... 17
Table 3. Pharmacokinetics for Movement Disorder Agents ................................................. 18
Table 4. Special Population Considerations for Movement Disorder Agents ...................... 19
Table 5. Labeled Drug Interactions for Movement Disorder Agents ................................... 21
Methods......................................................................................................................................... 22
Clinical Efficacy ........................................................................................................................... 24
Safety ............................................................................................................................................ 27
Table 6. Adverse Events and Warnings for Movement Disorder Agents ............................. 29
Summary ....................................................................................................................................... 31
References ..................................................................................................................................... 32
Appendix A ................................................................................................................................... 36
Table 1. Agents for the Management of Parkinsonism ......................................................... 36
Appendix B ................................................................................................................................... 37
Table 1. Medline Literature Search Strategy for SRs and RCTs .......................................... 37
Table 2. EMBASE Literature Search Strategy for SRs and RCTs ....................................... 38
Appendix C ................................................................................................................................... 41
Table 1. Placebo-Controlled Trials Including VMAT-2 Inhibitor Agents ........................... 41
Appendix D ................................................................................................................................... 43
Table 1. List of Excluded References ................................................................................... 43
3
Executive Summary
Introduction: Movement disorders are neurological syndromes characterized by abnormal hyperkinetic or hypokinetic movements. The movement disorder agents discussed in this report include 3 vesicular monoamine transporter 2 (VMAT-2) inhibitors (tetrabenazine, deutetrabenazine, and valbenazine) and 2 anticholinergic agents (benztropine and trihexyphenidyl). VMAT-2 inhibitors are indicated for the management of chorea associated with Huntington´s disease and tardive dyskinesia. Anticholinergic agents are approved for all forms of parkinsonism (including Parkinson’s disease), and drug-induced extrapyramidal disorders.
Each of the movement disorder agents is available as an oral formulation. Benztropine is additionally available as an injection for intramuscular or intravenous administration. Dosages should be individualized. The approach to treatment begins with an initial dose, followed by gradual dose adjustments to achieve a reduction of symptoms while maintaining tolerability.
Tetrabenazine approval was granted in 2008 for the treatment of chorea associated with Huntington’s disease. In 2017, two novel VMAT-2 inhibitors were approved: deutetrabenazine for both Huntington’s disease and tardive dyskinesia, and valbenazine for tardive dyskinesia.
For the treatment of chorea associated with Huntington´s disease, the 2012 American Academy of Neurology (AAN) guideline on chorea management in Huntington’s disease recommends tetrabenazine treatment as probably effective for this condition. Off-label use of tetrabenazine in patients with tardive dyskinesia is recommended in the 2013 AAN guideline for the treatment of tardive syndromes. Recommendations for deuterabenazine and valbenazine are not yet incorporated into clinical guidelines.
The anticholinergic agents, benztropine and trihexyphenidyl, have been available for decades to reduce tremor and dystonic symptoms associated with Parkinson´s disease (idiopathic parkinsonism), other forms of parkinsonism, and drug-induced extrapyramidal disorders. Although they are not considered first-line treatment options for Parkinson´s disease, the 1993 AAN practice parameters on initial therapy of Parkinson’s disease state that anticholinergic agents are frequently used to treat tremor in early-stages of Parkinson’s disease. The Food and Drug Administration (FDA) package inserts note that anticholinergic agents are usually used in combination with levodopa for the treatment of all forms of parkinsonism. For the management of drug-induced extrapyramidal disorders, the 2004 American Psychiatric Association guideline for the treatment of patients with schizophrenia recommends the short-term use of anticholinergic agents as a treatment option for antipsychotic-induced extrapyramidal side effects such as akathisia, dystonia, and parkinsonism. Recommendations against the use of anticholinergic agents in tardive dyskinesia are highlighted by various guidelines and FDA package inserts due to the lack of evidence or potential for worsening of tardive dyskinesia.
Efficacy and Pharmacokinetic Evidence: Following a systematic literature search, no head-to-head efficacy and safety comparisons among the movement disorder agents included in this

4
report were identified.
Regarding VMAT-2 inhibitors, literature reviews suggest the two novel VMAT-2 inhibitors (deutetrabenazine and valbenazine) have improved pharmacological and pharmacokinetic properties compared to tetrabenazine. Tetrabenazine exhibits a short plasma half-life and a rapid and variable metabolism. High peak plasma concentrations of active metabolites may occur and are usually associated with adverse events (somnolence, depression, akathisia, and parkinsonism). Deutetrabenazine, due to the presence of deuterium atoms, displays reduced metabolism variability, a longer plasma half-life, greater stability, and more resistance to drug metabolism compared to tetrabenazine. Its slow metabolism avoids high peak plasma concentrations of active metabolites and may improve tolerability. Genotyping for a genetic variant of the hepatic enzyme responsible for metabolizing tetrabenazine, the cytochrome P450 (CYP) 2D6 variant, is required for tetrabenazine doses above 50 mg daily. Labeling for deutetrabenazine does not require genotyping for CYP2D6; however, the maximum recommended dose should be reduced to 36 mg daily in poor CYP2D6 metabolizers. Tetrabenazine is usually administered two to three times daily, with daily doses ranging from 12.5 mg to 100 mg. Deutetrabenazine requires less frequent dosing (twice daily) and lower daily dosages (6 mg to 48 mg per day) than tetrabenazine.
In the absence of head-to-head randomized controlled trials in patients with Huntington´s disease, two indirect comparisons from placebo-controlled trials were identified. One network meta-analysis suggests similar efficacy and safety between deutetrabenazine and tetrabenazine, with a significant improvement in depression and somnolence scales with deutetrabenazine. The second indirect comparison evaluated tolerability profiles of deutetrabenazine compared to tetrabenazine. A significantly lower incidence of moderate to severe adverse events such as depression, somnolence, akathisia, parkinsonism, and insomnia was reported in favor of deutetrabenazine. This apparent favorable safety profile observed with deutetrabenazine should be interpreted cautiously as indirect comparisons provide low-quality evidence and no direct, head-to-head, evidence is available.
Valbenazine and its active metabolite possess high VMAT-2 selectivity and no affinity for other receptors (e.g. adrenergic, dopaminergic, muscarinic, etc.). Tetrabenazine and its two main active metabolites block VMAT-2 producing the desired effects; however, they also have affinity for other receptors, contributing to the occurrence of adverse events. No direct evidence from randomized controlled trials (RCTs) compares deutetrabenazine and valbenazine in the treatment of tardive dyskinesia. Valbenazine is taken once daily, while deutetrabenazine is administered twice daily.
Regarding anticholinergic agents, no head-to-head comparative evidence between benztropine and trihexyphenidyl was identified in patients with parkinsonism or drug-induced extrapyramidal disorders.
Adverse Events: In Huntington’s disease, VMAT-2 inhibitor use is associated with an increased risk of depression and suicidality. Tetrabenazine and deutetrabenazine labeling include a black box warning regarding depression and suicidal ideation in these patients. Other
5
reported adverse events include drowsiness, somnolence, fatigue, akathisia, parkinsonism, anxiety, insomnia, and gastrointestinal disturbances. In the setting of tardive dyskinesia, deutetrabenazine and valbenazine do not include depression and suicidal ideation as drug warnings. In placebo-controlled trials for tardive dyskinesia, somnolence was the most frequently reported adverse event with valbenazine treatment. Nasopharyngitis and insomnia were the most common adverse events reported for deutetrabenazine. The potential for risk for prolongation of the corrected QT (QTc) interval is described in the warning section of each VMAT-2 inhibitor product. In patients prescribed VMAT-2 inhibitors who are CYP2D6 poor metabolizers or who use strong CYP2D6 inhibitors concomitantly, recommended dosage should be reduced based on tolerability. Genotyping for polymorphisms in the CYP2D6 gene is required for tetrabenazine doses above 50 mg daily.
The anticholinergic agents, benztropine and trihexyphenidyl, are associated with anticholinergic side effects such as dry mouth, constipation, blurred vision, confusion, and urinary retention. They should be used with caution in the elderly.
Summary: No head-to-head comparisons were identified for the movement disorder agents included in this report. In patients with Huntington´s disease, deutetrabenazine shows advantages compared to tetrabenazine, including increased resistance to metabolism, longer half-life, reduced peak plasma concentrations, and a lower dosing frequency. Evidence from indirect comparisons suggests similar efficacy but a better safety profile with deutetrabenazine compared to tetrabenazine, probably due to pharmacokinetic differences. However, this theoretical safety advantage should be confirmed via randomized controlled head-to-head trials. For patients with tardive dyskinesia, comparative evidence between deutetrabenazine and valbenazine is lacking.
No comparative evidence is available for benztropine and trihexyphenidyl in parkinsonism or drug-induced extrapyramidal disorders. Guidelines do not specify a preference for one agent over another.
Overall, evidence is insufficient to confirm efficacy and safety differences between movement disorder agents. Well-conducted direct, head-to-head randomized controlled trials are needed.

6
Introduction
Movement disorders are neurological conditions characterized by abnormal voluntary and involuntary movements.1 These disorders can affect the work, leisure and activities of daily living of patients and their caregivers. Movement disorders include several diseases such as Huntington’s disease, drug-induced extrapyramidal disorders, tardive dyskinesia, parkinsonism, Parkinson’s disease, Wilson’s disease, tics, essential tremor, dystonia, and Tourette syndrome, among others.1-3 This report reviews the comparative efficacy and safety of 5 movement disorder agents approved by the Food and Drug Administration (FDA): 3 vesicular monoamine transporter 2 (VMAT-2) inhibitor agents (deutetrabenazine,4 tetrabenazine,5 and valbenazine6) and 2 anticholinergic agents (benztropine7,8 and trihexyphenidyl9,10). Deutetrabenazine and tetrabenazine are approved orphan drugs for the treatment of chorea associated with Huntington’s disease. Deutetrabenazine and valbenazine are the first drugs approved for tardive dyskinesia. The three VMAT-2 inhibitor agents have orphan drug designations for the treatment of Tourette syndrome in pediatric patients.11 Tetrabenazine has an additional orphan drug designation for the treatment of moderate/severe tardive dyskinesia.11 Benztropine and trihexyphenidyl are approved for all forms of parkinsonism and drug-induced extrapyramidal disorders.
Each of the movement disorder agents is available as an oral formulation. Benztropine is also available as an injection for intramuscular or intravenous use. Dosing should be individualized to each patient and gradually uptitrated based on a reduction of symptoms and tolerability.4-6,8-10
Table 1 provides specific information concerning labeled indications and dosing recommendations for the movement disorder agents included in this report. Appendix A contains a listing of all agents indicated for the management of parkinsonism.
Table 1. FDA-Approved Movement Disorder Agents Generic Name &
Brand Name (Approval Date)
Preparations (availability of
generic) Indication & Dosage
Vesicular Monoamine Transporter 2 Inhibitors
Deutetrabenazine4
Austedo
(April 2017)
Oral tablet: • 6 mg • 9 mg • 12 mg
Chorea associated with Huntington’s disease
• Patients not being switched from tetrabenazine: o Initial dose: 6 mg once daily; titrate up at weekly intervals by 6 mg per day up
to a maximum recommended daily dosage of 48 mg (24 mg twice daily) o Administer total daily dosages of 12 mg or above in two divided doses
• Switching patients from tetrabenazine to Austedo: Discontinue tetrabenazine and initiate Austedo the following day. (See recommended initial dosage in the full drug label information)
Tardive dyskinesia in adults
• Initial dose: 6 mg twice daily; may increase by 6 mg/day at weekly intervals to a maximun of 48 mg/day
• Administer total daily dosages of 12 mg or above in two divided doses

7
Tetrabenazine5
Xenazine
(August 2008)
Oral tablet: • 12.5 mg • 25 mg
Generic available
Chorea associated with Huntington’s disease
Dosing Recommendations Up to 50 mg per day
• 1st week: 12.5 mg daily • 2nd week, 25 mg daily (12.5 mg twice daily); then slowly titrate at weekly
intervals by 12.5 mg to a tolerated dose that reduces chorea • If daily doses of 37.5 mg to 50 mg are needed, they should be divided into 3
doses (maximum single dose: 25 mg)
Dosing Recommendations Above 50 mg per day
• Patients requiring doses >50 mg/day should be genotyped for CYP2D6: o Extensive/intermediate metabolizers: Maximum daily dose: 100 mg;
37.5mg/single dose o Poor metabolizers: Maximum daily dose: 50 mg; 25 mg/single dose
Unlabeled indications: Tardive dyskinesia
Valbenazine6
Ingrezza
(April 2017)
Oral capsule: • 40 mg • 80 mg
Tardive dyskinesia o Initial: 40 mg once daily o After 1 week, increase to 80 mg once daily o Dose adjustments due to drug interactions (see full package labeling)
Anticholinergic Agents
Benztropine mesylate7,8
Cogentin
(December 1959)
Oral tablet: • 0.5 mg • 1 mg • 2 mg
Generic only
Injection (IV or IM):
• 1mg/ml Generic available
Parkinsonism: Adjunct therapy of all forms of parkinsonism (idiopathic parkinsonism, post-encephalitic parkinsonism)
o Usual dose: 1 to 2 mg daily (range: 0.5 to 6 mg daily); maximum: 6 mg daily
Drug-induced extrapyramidal disorders: Aid in the control of extrapyramidal disorders (except tardive dyskinesia) due to neuroleptic drugs (e.g., phenothiazines)
o Usual dose: 1 to 4 mg once or twice daily up to a maximum daily dose of 6 mg
* Dosage must be individualized according to the need of the patient
Trihexyphenidyl hydrochloride9,10
Tremin (May 1949)- Discontinued
Oral elixir: • 2 mg/5 ml
Oral tablet: • 2 mg • 5 mg
Generic only
Parkinsonism: Adjunct therapy of all forms of parkinsonism (postencephalitic, arteriosclerotic, and idiopathic). It is often used with levodopa
o Initial dose: 1 mg/day, increase by 2 mg increments at intervals of 3 to 5 days; usual dose: 6 to 10 mg/day in 3 to 4 divided doses; doses of 12 to 15 mg/day may be required
Drug-induced extrapyramidal disorders:
o Initial dose: 1 mg/day; increase as necessary to usual range: 5 to 15 mg/day in 3 to 4 divided doses
Abbreviations: IM, intramuscular; IV, intravenous

8
Disease Overview and Guideline Recommendations
Movement disorders are neurological conditions caused by basal ganglia dysfunction.1 Basal ganglia are a group of subcortical gray matter nuclei, located in the brain, and principally responsible for motor control.1 The etiology of movement disorders includes certain drugs (e.g., antipsychotics), genetic factors, injuries, stroke, infections, and unknown origins.1,3,12,13
Movement disorders can be classified as hyperkinetic movement disorders (excessive involuntary movements and weakness) and hypokinetic disorders (reduced movements). Hyperkinetic movement disorders include tremor, dystonia, athetosis, chorea, myoclonus, and tics.3 Hypokinetic movement disorders, commonly called parkinsonism syndromes, include Parkinson’s disease and other subtypes of parkinsonims.1 Following is specific information regarding the disorders for which the agents in this report are FDA approved.
1) Hyperkinetic movement disorders
1.1. Huntington’s disease
Huntington’s disease, formerly known as Huntington’s chorea,3 is a fatal, progressive, autosomal dominant neurodegenerative disorder caused by a mutation in the huntingtin gene. It is characterized by motor, cognitive, and psychiatric impairment.1,3,14 Histopathologic abnormalities include striatal medium-sized spiny neuron loss, which may cause dopaminergic hyperactivity.14 Huntington’s disease onset is between 25 and 45 years old and typical early symptoms include rapid involuntary choreiform movements (chorea or “uncontrollable dance-like movements”14). Other symptoms, such as behavioral disturbances and dementia, appear as the disease progresses.3,14 Disease prevalence is estimated to be 5 cases per 100,000 worldwide.1 According to the Huntington Study Group, around 30,000 North Americans live with Huntington’s disease.15
Huntington’s disease is a chronic disease with no treatment to delay its progression. Current treatment strategies are aimed to treat movement impairment, but do not treat dementia. Tetrabenazine and deutetrabenazine are VMAT-2 inhibitors that decrease dopaminergic activity.1,4,5 They are currently approved for the treatment of chorea associated with Huntington’s disease.4,5 Quetiapine, olanzapine, or risperidone are used for behavioral impairments.1 The 2012 American Academy of Neurology (AAN) guideline for Huntington’s disease recommends the use of tetrabenazine for the treatment of choreic movements.16 Deutetrabenazine is not mentioned in the guideline, perhaps because it was approved after guideline publication. See Table 2 for a summary the guideline recommendations.
2) Hypokinetic movement disorders
2.1. Parkinsonism
Hypokinetic movement disorders are classified as parkinsonism syndromes. The estimated prevalence of parkinsonism in the United States and Western Europe, which increases with age, is 1-2 per 1,000 in the population.1 Symptoms of parkinsonism include rest tremor, rigidity, akinesia, slow movements or bradykinesia, and abnormal gait and posture.1

9
The several types of parkinsonism are classified depending on the etiology including the following: (1) idiopathic parkinsonism (e.g. Parkinson’s disease), (2) parkinsonism secondary to several causes such as postencephalitic parkinsonism due to a viral infection, drug or toxin-induced parkinsonism due to drugs (e.g. phenothiazines, butyrophenones, metoclopramide, reserpine, tetrabenazine) or toxins (e.g. environmental toxins), vascular parkinsonism, post-traumatic parkinsonism, familial/genetic parkinsonism, and (3) parkinsonism associated with other neurologic diseases (e.g. Lewy body disease, multisystem atrophy, progressive supranuclear palsy, corticobasal degeneration).1
The most common form of parkinsonism is Parkinson’s disease. Other parkinsonism syndromes are differentiated from Parkinson’s disease by the basal ganglia structures damaged, speed of disease progression, prognosis, etiology, and response to treatment.1,3 Symptoms of non-idiopathic parkinsonism are similar to those of Parkinson’s disease.1
Benztropine and trihexyphenidyl are currently approved as adjunct therapy of all forms of parkinsonism.7-10
Specific information about two forms of parkinsonism (Parkinson’s disease and drug-induced parkinsonism) is described below.
2.1.1. Idiopathic Parkinsonism or Parkinson’s Disease
Parkinson’s disease (PD) is second only to Alzheimer’s disease as the most common neurodegenerative disease.17 PD affects 10 million persons worldwide and approximately 1 million in the US.18 PD is predominantly a disease of the elderly. The prevalence is 1% in those over 65 years, although 4% of cases are identified in younger persons.18 Life expectancy is unchanged but quality of life is affected.18 Most patients are unable to continue full time work within 4-5 years of diagnosis.18 Risk factors include advanced age, male sex, low estrogen levels, agricultural work (presumed pesticide exposure), low folate levels, and head trauma (especially as a child). The genetic marker alpha-synuclein is associated with a 1.5-fold increased risk of PD. Evidence demonstrates a low correlation with disease and a positive family history.17,19,20
Parkinson’s disease symptoms arise from progressive degeneration of dopaminergic neurons in the substantia nigra of the midbrain, resulting in a deficiency of striatal dopamine.17,18 Many symptoms of Parkinson’s disease are the result of striatal dopaminergic deficiency resulting from a progressive loss of neurons.
The diagnosis of PD is a made clinically and requires the presence of the cardinal feature, bradykinesia, and one other cardinal manifestation; resting tremor, rigidity, bradykinesia or gait impairment/postural instability.18 Symptoms present asymmetrically.21 Other common features include disturbances in speech, mood, cognitive function, autonomic disturbances, sexual dysfunction, hyposomia (loss of smell), gastroparesis/constipation, insomnia, dream enactment and dementia.17
Clinical guidelines for the treatment of Parkinson’s disease include the 2017 National Institute for Health and Care Excellence (NICE) guideline on Parkinson’s disease in adults,22 the 2012 Canadian Guideline on Parkinson’s Disease,23 the 2011 European Academy of Neurology

10
Guideline on Early (uncomplicated) Parkinson’s Disease,24 and the 1993 practice parameters from the AAN on initial therapy of Parkinson’s disease.25 See Table 2 for a summary of guideline recommendations. In general, the guidelines recommend levodopa-carbidopa or a dopamine agonist (non-ergot class is preferred) as first-line therapy for treatment of motor symptoms, with some preference for use of levodopa in younger patients. Monoamine oxidase B (MAO- B) inhibitors are sometimes considered a first-line option. As the disease progresses, combination therapy with levodopa and dopamine agonists is recommended. Guidelines include further recommendations for managing on-off phenomena, wearing-off phenomena, freezing, and dystonias. Movement fluctuations are managed by adjustment of the levodopa dose, frequency of administration, addition of a catechol-o-methyl transferase (COMT) inhibitor agent or MAO-B medication. Off-time may be reduced with dopamine agonists. Dyskinesias may respond to amantadine therapy. Anticholinergics and beta-blockers are useful in the management of tremor. Anticholinergics, such as benztropine and trihexyphenidyl, may be used in patients at early-stage Parkinson’s disease with resting tremors and well-maintained cognitive function.26 Due to limited efficacy and high occurrence of gastrointestinal and neuropsychiatric adverse events,27 the use of anticholinergic agents should be used with caution or avoided in the elderly population.23-26 Most documents include recommendations for the treatment of non-motor problems; autonomic dysregulation, sleep, mood and cognitive changes. Surgical interventions are recommended when medication therapy has failed.
2.1.2. Drug-induced parkinsonism
Parkinsonism is a movement disorder that may be induced by drugs.1,3 It is characterized by tremor, rigidity, akinesia, bradykinesia, and abnormal gait and posture; as it is observed in a patient with Parkinson’s disease.28 Drug-induced parkinsonism is the most commonly described form of antipsychotic-induced extrapyramidal side effects.28
2.2. Drug-induced extrapyramidal disorders
Antipsychotic agents are generally prescribed for mental illnesses. The American Psychiatric Association (APA) Guideline Watch (2009) for the treatment of patients with schizophrenia recommends second-generation antipsychotic drugs as first line therapy for acute symptoms due to a lower incidence of extrapyramidal side effects (EPSE) compared to first-generation antipsychotic drugs.29 However, authors state that first-generation antipsychotic agents may be an adequate first-line choice for some patients.29 Antipsychotic agents improve neurologic symptoms by blocking dopamine receptors on the basal ganglia; however, this pharmacologic effect may also produce neurological adverse events such as extrapyramidal symptoms.28,30 The APA classifies extrapyramidal side effects as acute (parkinsonism, dystonia [uncontrolled muscular spasm], and akathisia [restlessness]), and chronic (tardive dyskinesia and tardive dystonia).1,28,30 Generally, symptoms appear within 3 months of the initiation of antipsychotic therapy and disappear weeks to months after drug withdrawal.1 Dystonia and akathisia frequently occur hours to weeks following antipsychotic therapy initiation; and parkinsonism may appear after a few days of antipsychotic therapy initiation or dose increase. Tardive dyskinesia usually occurs after years on antipsychotic treatment.30 Acute EPSE are dose-dependent and typically

11
remit after drug withdrawal or dose reduction,28 whereas tardive dyskinesia is not clearly dose-dependent and may not resolve after treatment discontinuation.28,30
Extrapyramidal side effects are more common with first generation or typical antipsychotics agents (e.g. phenothiazines, butyrophenones, and thioxanthenes) than second generation or atypical antipsychotics (e.g. risperidone, aripiprazole, olanzapine, etc.).1,28 Children and adolescents are at higher risk of developing EPSE than adults.28,31 The 2004 APA guideline reported EPSE (one form or several forms) in more than 60% of patients receiving first-generation antipsychotic therapy.28 A study in schizophrenia patients reported a cumulative incidence of EPSE ranging from 7.7% with olanzapine to 32.8% with depot first generation antipsychotic drugs.32
Trihexyphenidyl and benztropine have been shown to reduce extrapyramidal adverse events (e.g. acute dystonia and parkinsonism) and are currently approved for this purpose.8-10,12 However, anticholinergic drugs are not indicated for the chronic EPSE of tardive dyskinesia because they do not reduce and may aggravate symptoms of tardive dyskinesia.8-10,12 In addition, trihexyphenidyl and benztropine can cause anticholinergic adverse events and should not be administered at high doses or for extended periods of time.28 Other agents used for the management of drug-induced extrapyramidal symptoms include diphenhydramine, amantadine, or propranolol (off-label use).12
Clinical guidelines include the 2004 American Psychiatric Association Practice Guideline for the treatment of patients with schizophrenia28 and the 2009 Maudsley Prescribing Guidelines for psychotropic drugs.33 In patients with antipsychotic-induced extrapyramidal side effects, both guidelines recommend reducing the dose of antipsychotics, switching to other antipsychotics with lower risk of extrapyramidal effects, or adding short-term anticholinergic agents (e.g. trihexyphenidyl or benztropine).1,28,33 Trihexyphenidyl and benztropine are recommended for dystonia, akathisia, and parkinsonism; however, they are not recommended for tardive dyskinesia.27,32 A 2011 Canadian guideline including treatment recommendations for extrapyramidal side effects associated with second-generation antipsychotic use in children and youth is also available.
The 2013 American College of Gastroenterology guideline for the management of gastroparesis34 recommends metoclopramide as first-line prokinetic therapy in patients with gastroparesis. Metoclopramide should not be used longer than 3 months and should be discontinued if central nervous system side effects such as involuntary movements appear.34 In 2013, the European Medicines Agency evaluated the use of metoclopramide-containing products and recommended a maximum treatment duration of 5 days for all formulations (oral, parenteral and rectal) to reduce the risk of neurological side effects.35
2.2.1 Drug-induced tardive dyskinesia
Tardive dyskinesia (TD) is characterized by repeated and rapid involuntary movements of the body, including tongue, lips, jaw, eyes, face, trunk, and extremities.36,37 It typically occurs after prolonged use (months to years) of dopamine-receptor antagonists (e.g. antipsychotic agents, especially first generation drugs, or metoclopramide) and may be irreversible even after

12
treatment dicontinuation.1,28,38 Tardive dyskinesia appears more frequently in patients with schizophrenia and other mental illness disorders requiring chronic treatment with antipsychotic, dopamine receptor antagonist agents.1 Other risk factors associated with the occurrence of TD include advanced age, female sex, and an extended treatment duration of antipsychotic therapy.38 The prevalence of tardive dyskinesia reported in patients exposed to first generation antipsychotic drugs for more than 3 months is higher than 20%.37,38 An increased cumulative incidence of TD with extended duration of antipsychotic drug therapy has been documented in studies (5%, 27%, 43%, and 52% after 1 year, 5 years, 10 years, and 15 years with antipsychotic therapy, respectively).38 The incidence of TD is generally lower with atypical antipsychotic drugs compared with typical antipsychotic drugs.37
Prevention measures include avoiding prescribing metoclopramide for more than 3 months and monitoring patients receiving long-term antipsychotic drug therapy. Treatment approaches include antipsychotic dose reduction, switching to another antipsychotic agent, or drug therapy. Some patients (1%-62% depending on age, duration of treatment, etc.) may experience spontaneous remission of tardive dyskinesia after drug withdrawal,37 or may need extended supportive treatment.
The 2013 AAN guideline for the management of tardive syndromes,39 including tardive dyskinesias, considers tetrabenazine as a possible therapeutic option for tardive syndromes (off-label use). Regarding anticholinergic treatment, the authors state that data is insufficient to make a recommendation. Novel therapies, approved within the last year, for the treatment of tardive dyskinesia (i.e. deutetrabenazine and valbenazine), are not yet included in any guideline.
13
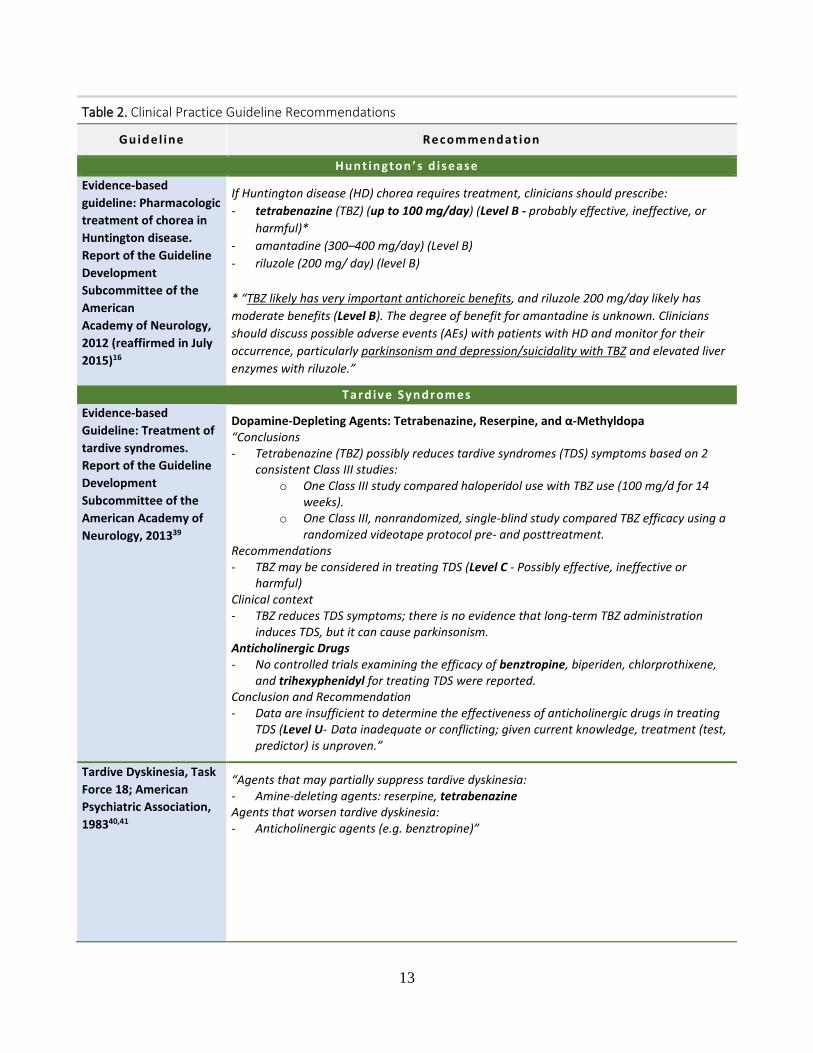
Table 2. Clinical Practice Guideline Recommendations
Gu id e l ine Recom mend at ion
Hu n t in gton ’s d isease Evidence-based guideline: Pharmacologic treatment of chorea in Huntington disease. Report of the Guideline Development Subcommittee of the American Academy of Neurology, 2012 (reaffirmed in July 2015)16
If Huntington disease (HD) chorea requires treatment, clinicians should prescribe: - tetrabenazine (TBZ) (up to 100 mg/day) (Level B - probably effective, ineffective, or
harmful)* - amantadine (300–400 mg/day) (Level B) - riluzole (200 mg/ day) (level B) * “TBZ likely has very important antichoreic benefits, and riluzole 200 mg/day likely has moderate benefits (Level B). The degree of benefit for amantadine is unknown. Clinicians should discuss possible adverse events (AEs) with patients with HD and monitor for their occurrence, particularly parkinsonism and depression/suicidality with TBZ and elevated liver enzymes with riluzole.”
Tar d ive Syn dr om es Evidence-based Guideline: Treatment of tardive syndromes. Report of the Guideline Development Subcommittee of the American Academy of Neurology, 201339
Dopamine-Depleting Agents: Tetrabenazine, Reserpine, and α-Methyldopa “Conclusions - Tetrabenazine (TBZ) possibly reduces tardive syndromes (TDS) symptoms based on 2
consistent Class III studies: o One Class III study compared haloperidol use with TBZ use (100 mg/d for 14
weeks). o One Class III, nonrandomized, single-blind study compared TBZ efficacy using a
randomized videotape protocol pre- and posttreatment. Recommendations - TBZ may be considered in treating TDS (Level C - Possibly effective, ineffective or
harmful) Clinical context - TBZ reduces TDS symptoms; there is no evidence that long-term TBZ administration
induces TDS, but it can cause parkinsonism. Anticholinergic Drugs - No controlled trials examining the efficacy of benztropine, biperiden, chlorprothixene,
and trihexyphenidyl for treating TDS were reported. Conclusion and Recommendation - Data are insufficient to determine the effectiveness of anticholinergic drugs in treating
TDS (Level U- Data inadequate or conflicting; given current knowledge, treatment (test, predictor) is unproven.”
Tardive Dyskinesia, Task Force 18; American Psychiatric Association, 198340,41
“Agents that may partially suppress tardive dyskinesia: - Amine-deleting agents: reserpine, tetrabenazine Agents that worsen tardive dyskinesia: - Anticholinergic agents (e.g. benztropine)”

14
Table 2. Clinical Practice Guideline Recommendations
Gu id e l ine Recom mend at ion
Par k in son ´s Disease (PD) Parkinson’s disease in adults: diagnosis and management. National Institute for Health and Care Excellence (NICE) guideline NG71. Methods, evidence and recommendations, July 201722
- Anticholinergics are most commonly used in “the earlier stages of Parkinson’s disease, with the aim of improving motor symptoms”
- “No studies assessed the effectiveness of anticholinergics in people with inadequate symptomatic control associated with Parkinson’s disease.” “Evidence to recommendations: Trade-off between benefits and harms: Although no evidence of benefit was identified for anticholinergics as an adjunct treatment to levodopa for people with Parkinson’s disease and inadequate symptomatic control, the Guideline Development Group (GDG) discussed and strongly agreed that anticholinergics have significant potential for causing adverse cognitive effects and hallucinations as well as increased risk of falls and/or urinary retention and should therefore not be offered to people with Parkinson’s disease who have developed dyskinesia and/or motor fluctuations.”
- “Do not offer anticholinergics to people with Parkinson’s disease who have developed dyskinesia and/or motor fluctuations
Canadian Guideline on Parkinson's Disease (2012)23
Motor Symptoms in Early PD • First-Line Pharmacological therapy
o Levodopa at the lowest possible dose. Avoid modified- release formulations o Dopamine agonists (DA), may try more than one agent
Non-ergot dopamine agonists are preferred. Ergot DA require testing renal function, erythrocyte sedimentation rate, chest radiograph
o MAO-B inhibitors (selegiline, rasagiline) Second-Line Pharmacological therapy
• Amantadine • Anticholinergics for symptomatic treatment* • Beta-adrenergic antagonists for postural tremor
* “Anticholinergics may be used as a symptomatic treatment typically in young people with early PD and severe tremor, but should not be drugs of first choice due to limited efficacy and the propensity to cause neuropsychiatric side effects. (level B - Probably effective, ineffective, or harmful for the given condition in the specified population)”
European Academy of Neurology: Early (uncomplicated) Parkinson's disease (2011)24
No uniform proposal for initiating therapy in symptomatic patients. Initial therapy may include:
- MAO-B inhibitors (e.g. selegiline or rasagiline) (level A - established as effective, ineffective, or harmful; requires at least one convincing class I study or at least two consistent, convincing class II studies)
o Effects more modest than levodopa but are easy to administer (one dose, once daily, no titration), and well tolerated (especially rasagiline).
- Amantadine or an anticholinergic (level B - probably effective, ineffective, or harmful; requires at least one convincing class II study or overwhelming class III evidence)
o Effects smaller than levodopa. They are poorly tolerated in the elderly and are best restricted to young patients.
- Levodopa is the most effective symptomatic antiparkinsonian (level A). Long-term use often leads to motor complications. It is recommended in older patients who are more sensitive to neuropsychiatric adverse effects and less prone to motor

15
Table 2. Clinical Practice Guideline Recommendations
Gu id e l ine Recom mend at ion
complications. Early use of controlled-release formulations, do not delay motor complications
- Dopamine agonist (pramipexole, piribedil, and ropinirole immediate- or controlled-release) are effective as monotherapy. Pramipexole and ropinirole have a lower risk of motor complications than levodopa. (level A) Lower class evidence, supports bromocriptine with no evidence suggesting they are less effective.
Neuroprotective strategies and alternative therapies for Parkinson disease (an evidence-based review): Report of the Quality Standards Subcommittee of the American Academy of Neurology (2006)42
* This guideline does not mention anticholinergic therapy - “Levodopa does not appear to accelerate disease progression. - No treatment has been shown to be neuroprotective. - There is no evidence that vitamin or food additives can improve motor function in PD. - Exercise may be helpful in improving motor function - Speech therapy may be helpful in improving speech volume. - No manual therapy has been shown to be helpful in the treatment of motor
symptoms, although studies in this area are limited. Further studies using a rigorous scientific method are needed to determine efficacy of alternative therapies.”
Quality Standards Subcommittee of the American Academy of Neurology. Practice parameters: initial therapy of Parkinson’s disease (summary statement). Neurology 199325
- The 1993 AAN Practice Parameter examined anticholinergics, amantadine, selegiline, dopamine agonists, and levodopa in the treatment of PD. The conclusions about anticholinergics were that:
o “Anticholinergic agents are commonly used as initial therapy, especially in cases where tremor is predominant, but there is no evidence that anticholinergic agents are better than levodopa for tremor (Class II - Evidence provided by one or more well-designed clinical studies such as case control, cohort studies, etc.).”
Dr u g- in du ced extr ap yr am id al d isord er s Treatment recommendations for extrapyramidal side effects associated with second-generation antipsychotic use in children and youth (CAMESA, 2011)43
- “Treatment recommendations for neuroleptic-induced acute dystonia: o Administer diphenhydramine (LOE high) or an anticholinergic (benztropine
and biperiden) (LOE very low). - Treatment recommendations for neuroleptic-induced acute akathisia or parkinsonism
o Anticholinergics or amantadine can be added for the treatment of parkinsonism (LOE high)
- Treatment recommendations for tardive dyskinesia: o Discontinue anticholinergic medication if patient is taking concurrently;
anticholinergics may exacerbate tardive dyskinesia (LOE high). - Treatment recommendations for tardive dystonia:
If the antipsychotic medication can be discontinued, taper off the medication and treat the dystonia with an anticholinergic such as trihexyphenidyl. There are case reports of adolescents with tardive dystonia who were successfully treated with anticholinergic therapy (LOE very low).”
The Maudsley Prescribing Guidelines (10th Edition). London:
- Guidelines recommend “reducing or switching antipsychotics or adding short-term anticholinergic medications as treatment for those presenting with antipsychotic-induced parkinsonism (dystonia, pseudo-parkinsonism)”

16
Table 2. Clinical Practice Guideline Recommendations
Gu id e l ine Recom mend at ion
Informa Healthcare, 200933
- “Dystonia can be treated with anticholinergic drugs given orally, intramuscularly or intravenously depending on the severity of symptoms”
- “Pseudo-parkinsonism: o Reduce or switch antipsychotics o Prescribe an anticholinergic. The majority of patients do not require long-
term anticholinergics. Use should be reviewed at least every 3 months. Do not prescribe at night (symptoms usually absent during sleep)”
- “Anticholinergics are generally unhelpful for akathisia (restlessness)” - ”Tardive dyskinesia: Stop anticholinergic if prescribed”
American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Second Edition, 200428 Note: In accordance with national standards, including those of the Agency for Healthcare Research and Quality’s National Guideline Clearinghouse, this guideline can no longer be assumed to be current.
- “The first approach to treatment of parkinsonism associated with first-generation antipsychotics should be to lower the antipsychotic dose to the extrapyramidal symptom threshold. If dose reduction does not sufficiently improve symptoms, then a switch to a second-generation antipsychotic should be considered. Medications with anticholinergic (e.g., benztropine) or dopamine agonist (e.g., amantadine) activity often reduce the severity of parkinsonian symptoms. However, dopamine agonists carry a potential risk of exacerbating psychosis, and anticholinergic drugs can cause anticholinergic side effects. Thus, excessive doses and chronic use of these agents should be avoided or minimized.”
- “Decisions to use medications to treat side effects are driven by the severity and degree of distress associated with the side effect and by consideration of other potential strategies, including lowering the dose of the antipsychotic medication or switching to a different antipsychotic medication”
- Medications that can be used to treat extrapyramidal side effects: o Benztropine: reduce akathisia, dystonia, parkinsonism o Trihexyphenidyl hydrochloride: reduce akathisia, dystonia, parkinsonism o Amantadine: reduce akathisia, parkinsonism o Propranolol: reduce akathisia o Lorazepam: reduce akathisia o Diphenhydramine: reduce akathisia, dystonia, parkinsonism
Abbreviations: AAN, American Academy of Neurology; LOE, level of evidence; PD, Parkinson’s disease;

17
Pharmacology & Special Populations
Tetrabenazine, deutetrabenazine and valbenazine are vesicular monoamine transporter type 2 (VMAT-2) inhibitors.4-6,12,13 They reversibly block VMAT-2 decreasing the uptake of dopamine into the presynaptic vesicles and causing dopamine depletion in the central nervous system.4-
6,12,13 Each agent is metabolized to active metabolites. The principal active metabolite for VMAT-2 inhibitors is dihydrotetrabenazine (HTBZ), which exhibits the major pharmacological effect.44
Tetrabenazine is rapidly metabolized and has short half-life.5,44 It requires a multiple daily administration schedule (2 to 3 times daily).5,44 Doses should be carefully individualized according to the observed benefits and adverse events.5 Tetrabenazine is rapidly metabolized to several metabolites by hepatic carbonyl reductase and its plasma concentrations are very low.5,45 The main active metabolites (α-HTBZ and β-HTBZ) have high bioavailability, show similar activity to tetrabenazine, and are primarily metabolized by cytochrome P450 2D6 (CYP2D6).5,13,45 High peak plasma concentrations of active metabolites may occur within 1 hour after tetrabenazine administration, probably contributing to the occurrence of adverse events.46 Tetrabenazine and its 2 main active metabolites block VMAT-2, producing the desired effects. However, they also have affinity for other receptors (e.g. adrenergic, dopaminergic, muscarinic),45 causing adverse events.47 Doses of tetrabenazine ranging from 12.5 mg to 100 mg daily are recommended; however, patients requiring doses higher than 50 mg daily should be genotyped for CYP2D6 to identify their CYP2D6 metabolizer status (extensive, intermediate, or poor).5 The recommended maximum daily dose should be reduced to 50 mg for poor metabolizers.5
Deutetrabenazine is an analog of tetrabenazine, with 6 hydrogen atoms substituted by deuterium atoms (nontoxic forms of hydrogen).13 Because deuterium atoms bind to carbon stronger than hydrogen, deutetrabenazine exhibits increased resistance to CYP2D6 metabolism and a prolonged plasma half-life.13,48 Less frequent administration and lower doses of deutetrabenazine are required to achieve the desired effect (6 to 46 mg daily) compared to tetrabenazine (12.5 to 100 mg daily).4,13 The slow metabolism of deutetrabenazine and lower peak plasma concentrations are associated with a reduction in the incidence of adverse events.13,48,49
Valbenazine has a longer plasma half-life than tetrabenazine and deutetrabenazine supporting once-daily administration.47 Valbenazine has high VMAT-2 selectivity. The results of a study comparing the pharmacological profile of tetrabenazine and valbenazine13 suggest that valbenazine has a “higher potency, selectivity, and specificity of VMAT2 binding”13 than tetrabenazine due to its principal, active metabolite, (+)-α- HTBZ. This metabolite is the most highly VMAT-2 selective when compared to tetrabenazine, valbenazine and other metabolites of these agents.13 Additionally, given the absence of affinity for other receptors a lower incidence of adverse events is expected.47
Benztropine and trihexyphenidyl are anticholinergic drugs.7-10 They inhibit acetylcholine action at central muscarinic receptors and block parasympathetic nervous system effects.12 Trihexyphenidyl also exhibits a direct relaxing effect in smooth muscles.9,10,12
18
According to the 2015 Beers criteria for potentially inappropriate medication use in older adults, benztropine and trihexyphenidyl should be used with caution or avoided in this population due to safety concerns.50 Anticholinergic side effects of particular concern in the elderly include to the development of dementia, cognitive impairment, and physical dysfunction.50
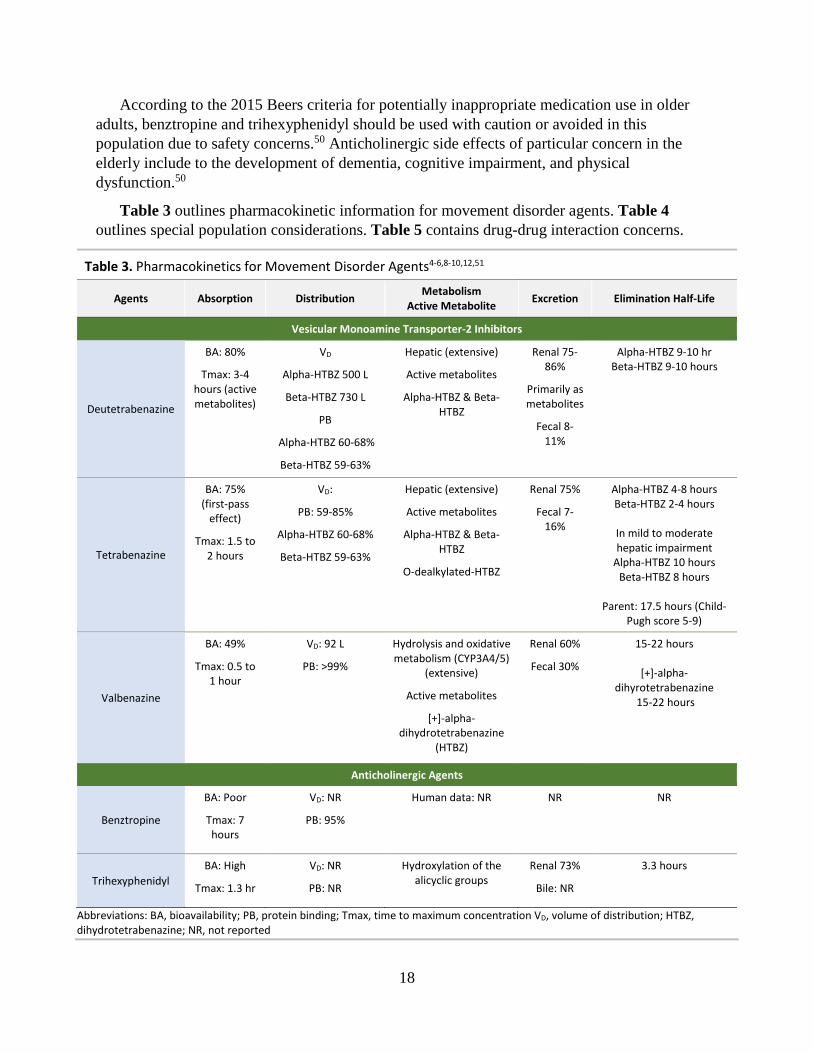
Table 3 outlines pharmacokinetic information for movement disorder agents. Table 4 outlines special population considerations. Table 5 contains drug-drug interaction concerns.
Table 3. Pharmacokinetics for Movement Disorder Agents4-6,8-10,12,51
Agents Absorption Distribution Metabolism Active Metabolite Excretion Elimination Half-Life
Vesicular Monoamine Transporter-2 Inhibitors
Deutetrabenazine
BA: 80%
Tmax: 3-4 hours (active metabolites)
VD
Alpha-HTBZ 500 L
Beta-HTBZ 730 L
PB
Alpha-HTBZ 60-68%
Beta-HTBZ 59-63%
Hepatic (extensive)
Active metabolites
Alpha-HTBZ & Beta-HTBZ
Renal 75-86%
Primarily as metabolites
Fecal 8-11%
Alpha-HTBZ 9-10 hr Beta-HTBZ 9-10 hours
Tetrabenazine
BA: 75% (first-pass
effect)
Tmax: 1.5 to 2 hours
VD:
PB: 59-85%
Alpha-HTBZ 60-68%
Beta-HTBZ 59-63%
Hepatic (extensive)
Active metabolites
Alpha-HTBZ & Beta-HTBZ
O-dealkylated-HTBZ
Renal 75%
Fecal 7-16%
Alpha-HTBZ 4-8 hours Beta-HTBZ 2-4 hours
In mild to moderate hepatic impairment
Alpha-HTBZ 10 hours Beta-HTBZ 8 hours
Parent: 17.5 hours (Child-
Pugh score 5-9)
Valbenazine
BA: 49%
Tmax: 0.5 to 1 hour
VD: 92 L
PB: >99%
Hydrolysis and oxidative metabolism (CYP3A4/5)
(extensive)
Active metabolites
[+]-alpha-dihydrotetrabenazine
(HTBZ)
Renal 60%
Fecal 30%
15-22 hours
[+]-alpha-dihyrotetrabenazine
15-22 hours
Anticholinergic Agents
Benztropine
BA: Poor
Tmax: 7 hours
VD: NR
PB: 95%
Human data: NR NR NR
Trihexyphenidyl BA: High
Tmax: 1.3 hr
VD: NR
PB: NR
Hydroxylation of the alicyclic groups
Renal 73%
Bile: NR
3.3 hours
Abbreviations: BA, bioavailability; PB, protein binding; Tmax, time to maximum concentration VD, volume of distribution; HTBZ, dihydrotetrabenazine; NR, not reported

19
Table 4. Special Population Considerations for Movement Disorder Agents4-6,8-10,12,51
Pediatric Geriatric Adjustment for Kidney Disease
Adjustment for Hepatic Disease Pregnancy & Lactation
Vesicular Monoamine Transporter-2 Inhibitors
Deutetrabenazine
Safety and efficacy not established in children
Refer to adult dosing; use with caution
Not studied Contraindicated in patients with
hepatic impairment
No AEs observed in animal reproduction
studies
Not evaluated in preclinical studies
Distribution to breast milk, unknown
Tetrabenazine
Safety and efficacy not established in children
No information No information No information Pregnancy: Category C
Crosses placenta: unknown
Distribution to breast milk: Unknown, infant
risk cannot be ruled out
Valbenazine
Safety and efficacy not established in children
No dosage adjustment recommended
CrCl 30-90 mL/min, no adjustment
CrCl < 30 mL/min, use
not recommended
Moderate or severe
impairment (Child-Pugh
score 7 to 15): recommended dose of 40 mg
once daily
Pregnancy: Fetal risk cannot be ruled out
Distribution to breast milk: unknown, infant
risk cannot be ruled out
Anticholinergic Agents
Benztropine
Use in contraindicated in children <3 years of
age
Drug-induced extrapyramidal
symptoms (age > 3 years):
1-4 mg once or twice daily
Parkinsonism (age > 3 years):
Initial 0.5-1 mg at bedtime; increase by
0.5 mg increments every 5-6 days
MAX DOSE: 6 mg/day MAINTENANCE: 1- mg
daily
Begin at the low end of the dosing range and
increase only as needed
Beers criteria: Use caution or avoid use as potentially
inappropriate in older adults
No information No information Safe use in pregnancy has not been established
Crosses placenta: unknown
Breastfeeding: Infant risk cannot be ruled out

20
Table 4. Special Population Considerations for Movement Disorder Agents4-6,8-10,12,51
Pediatric Geriatric Adjustment for Kidney Disease
Adjustment for Hepatic Disease Pregnancy & Lactation
Trihexyphenidyl
Safety and efficacy not established in children
Begin at the low end of the dosing range and
increase gradually
Concomitant use with levodopa: 3-6 mg daily, adjusted for side effects and degree of symptom
control
Concomitant use with other parasympathetic
inhibitors: partial substitution initially with progressive reduction in
other medication as dose of trihexphenidyl is
increased
Beers criteria: Use caution or avoid use as
potentially inappropriate in older adults
No dosage adjustment
required
No information Pregnancy Category C
Crosses placenta: unknown
Excretion in breast milk: unknown
Breastfeeding: may alter milk production or composition. Consider
alternate therapy and if used, monitor the infant for adverse
effects and/or adequate milk intake
Abbreviations: Crcl, creatinine clearance

21
Table 5. Labeled Drug Interactions for Movement Disorder Agents Agents Drug Interactions
Vesicular Monoamine Transporter-2 Inhibitors
Deutetrabenazine4
Do not use with: • Reserpine • MAOIs • Tetrabenazine, or valbenazine
Use caution with: • Drugs that cause QTc prolongation • Neuroleptic drugs (dopamine antagonists or antipsychotics) • Alcohol or other sedating drugs: May have additive sedation and somnolence
Dose adjustment with: • Strong CYP2D6 inhibitors (e.g. paroxetine, fluoxetine, quinidine, bupropion): Maximum recommended dose
of deutetrabenazine is 36 mg per day (18 mg twice daily)
Tetrabenazine5
Do not use with: • Reserpine: At least 20 days should elapse after stopping reserpine before starting tetrabenazine • MAOIs: or use within a minimum of 14 days of discontinuing therapy with an MAOI • Deutetrabenazine, or valbenazine
Use caution with: • Alcohol or Other Sedating Drugs: May have additive sedation and somnolence • Drugs that cause QTc prolongation: May have additive effect. Tetrabenazine causes a small prolongation of
QTc • Neuroleptic drugs (dopamine antagonists or antipsychotics): The risk for parkinsonism, neuroleptic
malignant syndrome, and akathisia may be increased
Dose adjustment with: • Strong CYP2D6 inhibitors (e.g. fluoxetine, paroxetine, quinidine): Do not exceed 50 mg/day and the
maximum single dose should not exceed 25 mg if administered in conjunction with a strong CYP2D6 inhibitor
Valbenazine6
Do not use with: • MAOIs • Strong CYP3A4 inducers
Dose adjustment with: • Strong CYP3A4 inhibitors: Reduce dose to 40 mg • Strong CYP2D6 inhibitors: Recommended dose reduction based on tolerability • Digoxin: Dosage adjustment of digoxin may be necessary
Anticholinergic Agents
Benztropine8
Use caution with: • Antipsychotic drugs, tricyclic antidepressants: patients should be advised to report gastrointestinal
complaints, fever or heat intolerance promptly. Paralytic ileus, hyperthermia and heat stroke, all of which have sometimes been fatal, have occurred.
• Hot weather: anhidrosis may occur
Trihexyphenidyl10 Use caution with: • Levodopa: Dose reduction recommended
Abbreviations: MAOI, monoamine oxidase inhibitors

22
Methods
Literature Search
Search strategies were developed by an informational scientist for OVID Medline and EMBASE. Strategies consisted of controlled vocabulary, such as MeSH, and keyword phrases. Two methodological filters were used, one for systematic reviews (ad hoc) and another for randomized controlled trials (RCT).52 Results were limited to English language. In EMBASE, we excluded conference abstracts. Searches were conducted in January 2018. The complete search strategies and terms are available in Appendix B.
We also screened the reference lists of related systematic reviews and other relevant websites for further information:
1. For guidelines addressing Huntington’s disease, parkinsonism, tardive dyskinesia, and drug-induced extrapyramidal disorders, websites of the National Guideline Clearinghouse, The American Academy of Neurology, The American Academy of Family Physicians, and The American Psychiatric Association
2. For prescribing information package inserts, the Food and Drug Administration website (Drugs@FDA: FDA Approved Drug Products): https://www.accessdata.fda.gov/scripts/cder/daf/)
3. Evidence-based drug information databases (Micromedex and Lexicomp)
Screening
At least 2 review authors screened titles and abstracts. Conflicts were resolved via discussion between reviewers and if necessary a third person as tie-breaker. The full texts for all citations receiving 2 inclusion votes were retrieved; final eligibility for inclusion was determined by the lead author. Figure 1 shows the PRISMA flow chart53 for the review process of systematic reviews and RCTs.
Inclusion and Exclusion Criteria
Systematic reviews/meta-analyses (SR/MA) of RCTs and RCTs providing head-to-head efficacy and/or safety comparisons among the movement disorder agents were included. For product comparisons where a systematic review provided robust data, we examined only those trials or systematic reviews published after the search date of the robust systematic review.
Excluded references met the following exclusion criteria:
• SR/MAs not synthesizing the results from RCTs separately from observational studies • SR/MAs of observational studies, registries, and retrospective studies. Only results from MA
of RCTs are considered for evaluation • Reviews not using a systematic method • Network meta-analyses, which according to the hierarchy of evidence, are considered to have
low quality because they include indirect comparisons • Studies comparing movement disorder agents versus placebo

23
• Single studies such as observational studies, pharmacodynamic studies, studies evaluating non-FDA approved doses, registries, pilot studies, and switching studies
A list containing the excluded references is provided in Appendix D.
Figure 1. PRISMA Flow Diagram of the selection process
Records identified through database searching (n = 946)
Scre
enin
g In
clud
ed
Elig
ibili
ty
Iden
tific
atio
n
Records after duplicates removed (n = 680)
Records screened (n = 681)
Records excluded (n =679)
Full-text articles assessed for eligibility
(n = 2)
Studies included in qualitative synthesis
(n = 0)
Full-text articles excluded, with reasons
(n =2)
• 2 network meta-analyses

24
Clinical Efficacy
After applying inclusion and exclusion criteria, no publications evaluating direct comparative efficacy and safety data for the movement disorder agents included in this report were identified.
Huntington’s disease - tetrabenazine versus deutetrabenazine
Tetrabenazine and deutetrabenazine were FDA approved based on two phase III, 12-week, placebo-controlled trials (TETRA-HD32 and FIRST-HD54 studies) for the management of chorea associated with Huntington’s disease.54,55 Tetrabenazine was approved in 2008 as the first drug with a positive effect on the chorea movements associated with Huntington’s disease (5-point reduction in chorea severity with tetrabenazine compared to 1.5- point reduction with placebo).55 Deutetrabenazine was approved in 2017. Clinical studies found a chorea severity reduction of 4.4 units with deutetrabenazine compared to 1.9 units with placebo.54 No other drugs are currently approved for the treatment of chorea in Huntington’s disease patients.
Direct Comparisons
No direct evidence comparing tetrabenazine and deutetrabenazine was identified.
Indirect Comparisons
In the absence of head-to-head studies, one indirect comparison involving tetrabenazine and deutetrabenazine was identified.56 Results from this study will be included as additional information. However, well-conducted head-to-head studies are needed to differentiate the effect of these drugs in patients with Huntington’s disease.
Rodrigues et al56 (2017) performed a network meta-analysis including 1 tetrabenazine placebo-controlled trial and 1 deutetrabenazine placebo-controlled trial. This network meta-analysis provided low-quality evidence as assessed by the authors based on GRADE (Grading of Recommendations, Assessment, Development and Evaluation) evaluation. Results suggested no efficacy differences between tetrabenazine and deutetrabenazine in reducing choreiform movements in Huntington’s disease. Regarding the odds of certain adverse events, no significant differences between groups were reported. A non-statistically significant reduction of depression and somnolence events was observed in favor of deutetrabenazine. Concerning the mean differences between treatment groups in depression and sleepiness scores (using rating scales), a significant improvement in both scales was reported with deutetrabenazine compared to tetrabenazine.
Tardive dyskinesia – deutetrabenazine versus valbenazine
Deutetrabenazine and valbenazine were recently approved by the FDA for tardive dyskinesia based on placebo-controlled trials.57
Direct Comparisons
No direct evidence comparing deutetrabenazine versus valbenazine was identified. No other drugs are currently approved for the treatment of tardive dyskinesia. Citrome et al48,58 opined in 2

25
systematic reviews published in 2017 that direct head-to-head comparisons between the two recently approved VMAT-2 inhibitors in patients with tardive dyskinesia are needed.48,58
Off-label use of tetrabenazine
Tetrabenazine has been historically used for hyperkinetic disorders such as dystonia, tics, and tardive dyskinesia, although it is not approved for these indications by the FDA.45 Support for off-label use in hyperkinetic disorders comes only from small studies; however, some authors consider tetrabenazine a therapeutic alternative for these indications based on limited, positive evidence.45
Tetrabenazine is used off-label for tardive dyskinesia. It is recommended by the American Academy of Neurology39 as possibly effective for tardive dyskinesia. Eight studies evaluating tetrabenazine for this indication were included in a systematic review.47 One study was a double-blind, cross-over study and the remaining 7 studies were open-label trials. Results indicate tetrabenazine improves tardive dyskinesia and is well-tolerated. Limitations of the evidence include the absence of randomized controlled trials, differences in population characteristics and dosing, and different outcome assessment tools. Higher-quality evidence is needed to adequately define the place in therapy of tetrabenazine.47
Appendix C outlines the efficacy results from placebo-controlled trials including VMAT-2 inhibitor agents.
Parkinsonism - Benztropine versus trihexyphenidyl
Direct Comparisons
Several guidelines indicate that anticholinergic agents, such as benztropine and trihexyphenidyl, are probably efficacious for resting tremors occurring during early-stage Parkinson’s disease, especially in the population below than 70 years old without cognitive dysfunction.26 However, no head-to-head comparative evidence between benztropine and trihexyphenidyl was identified in patients with parkinsonism.
Drug-induced extrapyramidal disorders - Benztropine versus trihexyphenidyl
Direct Comparisons
Clinical evidence available for this indication is limited. Anticholinergic agents seem to be effective for drug-induced acute extrapyramidal disorders such as dystonia and parkinsonism.8-
10,28 Acute akathisia is generally less responsive to anticholinergic medications.27,33 The use of anticholinergic agents may exacerbate chronic extrapyramidal disorders such as tardive dyskinesia and is not recommended.8-10,28 Anticholinergic agents are usually prescribed in patients with antipsychotic- or other drug-induced extrapyramidal disorders; however, no head-to-head comparisons between benztropine and trihexyphenidyl were identified.

26
Anticholinergic Drugs and Tardive Dyskinesia
A Cochrane review published in 201859 and a systematic review published in 201736 evaluated anticholinergic drugs, including benztropine and trihexyphenidyl for TD. Evidence was available only for comparisons of benztropine and trihexyphenidyl to other drugs (e.g. amantadine) for the treatment of antipsychotic-induced tardive dyskinesia or neuroleptic-induced parkinsonism.36,59 The AAN39 states there is insufficient information to make conclusions about the efficacy of anticholinergic agents in the treatment of tardive syndromes, including tardive dyskinesia. Moreover, evidence40,60 and package inserts8,10 highlight the potential for worsening of tardive dyskinesia with the use of benztropine and trihexyphenidyl.
27
Safety
Anticholinergic agents, such as benztropine and trihexyphenidyl, are broadly used to treat drug-induced movement disorders such as parkinsonism and dystonia; however, they are associated with many anticholinergic side effects such as dry mouth, constipation, blurred vision, confusion, and urinary retention.36 Benztropine and trihexyphenidyl do not carry any black box warning, but other warnings such as anhidrosis, hyperthermia, central nervous system effects, or anticholinergic effects in special population (e.g. patients with cardiovascular disease, hepatic or renal impairment, gastrointestinal obstruction, glaucoma, prostatic hyperplasia or urinary retention) should be considered.8-10 Anticholinergic agents should be used with caution in the elderly.50
The main safety concern related to VMAT-2 inhibitor use in patients with Huntington’s disease is the increased risk of depression and suicidal thoughts and behaviors.4,5 These serious adverse events were reported in placebo-controlled trials at different rates depending on the VMAT-2 inhibitor agent.4,5 Tetrabenazine and deutetrabenazine carry a black box warning regarding depression and suicidality in patients with Huntington’s disease.4,5 Both agents are contraindicated in patients with Huntington’s disease who have thoughts of suicide or in patients with untreated or uncontrolled depression.4,5 Other reported adverse events related to tetrabenazine and deutetrabenazine include drowsiness, somnolence, fatigue, akathisia, parkinsonism, anxiety, insomnia, and gastrointestinal disturbances.4,5 In the setting of tardive dyskinesia, deutetrabenazine and valbenazine do not include depression and suicidal ideation as drug warnings.4,6 In placebo-controlled trials for tardive dyskinesia, somnolence was the most frequently reported adverse event with valbenazine treatment.6,61 Nasopharyngitis and insomnia were the most common adverse events reported for deutetrabenazine.4
VMAT-2 inhibitor agents causes QTc prolongation. Co-administration with other drugs that prolongs the QTc should be avoided.4-6 Labeling for tetrabenazine and deutetrabenazine includes warnings concerning the risk of akathisia, agitation, restlessness, parkinsonism, and neuroleptic malignant syndrome.4,5 In patients prescribed VMAT-2 inhibitors who are CYP2D6 poor metabolizers or who use strong CYP2D6 inhibitors concomitantly, recommended dosage should be reduced based on tolerability.4-6
A recent pooled analysis concerning the cardiovascular profile of valbenazine demonstrated no differences in the cardiovascular risk with valbenazine compared to placebo.62 Potential safety nuances between VMAT-2 inhibitor agents need to be confirmed in head-to-head randomized controlled trials.
An approved Risk Evaluation and Mitigation Strategy (REMS) is available for tetrabenazine. This program is intended to inform healthcare professional about the risk of depression and suicide thoughts, appropriate dose titration and dosing, and potential for drug interactions with strong CYP2D6 inhibitors.63

28
Indirect comparison in patients with Huntington’s Disease
Claassen et al.64 (2017) conducted indirect tolerability comparisons between tetrabenazine and deutetrabenazine in patients with Huntington’s disease. Results suggested a significantly lower incidence of overall adverse events, moderate to severe adverse events, and neuropsychiatric adverse events such as agitation, akathisia, depression, drowsiness/somnolence, insomnia, and parkinsonism for deutetrabenazine compared to tetrabenazine. Significantly lower rates of dose reduction and dose reduction/suspension due to adverse events were reported with deutetrabenazine compared to tetrabenazine. Authors explained the apparent favorable safety profile of deutetrabenazine may be related to its pharmacokinetic profile. Indirect comparisons are considered low-quality evidence and should be interpreted cautiously. Well-conducted head-to-head studies are needed to confirm the safety differences between these two agents.
Table 6 includes adverse events, warnings, and contraindications for movement disorder agents.

29
Table 6. Adverse Events and Warnings for Movement Disorder Agents4-6,8-10,12,51 Generic Name Contraindications/Warnings Adverse Events
Vesicular Monoamine Transporter 2 Inhibitors Deutetrabenazine Contraindications:
• Patients who are actively suicidal, or in patients with untreated or inadequately treated depression
• Hepatic impairment • See table 5 for drug interaction- related
contraindications Black box warning: Depression and suicidality in patients with Huntington disease: • Deutetrabenazine or tetrabenazine can
increase the risk of depression and suicidal thoughts and behavior (suicidality) in patients with Huntington disease
• Particular caution should be exercised in treating patients with a history of depression or prior suicide attempts or ideation
Other warnings: • Akathisia • CNS depression • Hyperprolactinemia • Neuroleptic malignant syndrome • Ophthalmic effects • Parkinsonism • QTc prolongation • CYP2D6 poor metabolizers • Huntington disease: May worsen mood,
cognition, rigidity, and functional capacity in patients
Additional warnings for tetrabenazine • Esophageal dysmotility/aspiration • Orthostatic hypotension
>10%: CNS: Drowsiness (11%)
1% to 10%: CNS: Fatigue (9%), insomnia (4% to 7%), anxiety (4%), depression (≤4%), agitation (≤4%), akathisia (≤4%), restlessness (≤4%), suicidal ideation (2%) GI: Diarrhea (9%), xerostomia (9%), constipation (4%) GU: Urinary tract infection (7%) Hema&onco: Bruise (4%) Resp: Nasopharyngitis (4%)
Tetrabenazine >10%:
CNS: Drowsiness (≤17% to ≤57%), sedation (≤17% to ≤57%), depression (19% to 35%), extrapyramidal reaction (15% to 33%), fatigue (22%), insomnia (22%), akathisia (19% to 20%), anxiety (15%), falling (15%)
GI: Nausea (13%)
Resp: Upper respiratory tract infection (11%)
1% to 10%:
CNS: Drug-induced Parkinson's disease (3% to 10%), equilibrium disturbance (9%), irritability (9%), abnormal gait (4%), dizziness (4%), dysarthria (4%), headache (4%), obsessive rumination (4%)
GI: Dysphagia (4% to 10%), vomiting (6%), decreased appetite (4%), diarrhea (2%)
GU: Dysuria (4%)
Hema&onco: Bruise (6%)
NMS: Bradykinesia (9%)
Resp: Bronchitis (4%), dyspnea (4%) Miscellaneous: Laceration (6%, head)
Valbenazine No contraindications No black box warnings Other warnings: • Somnolence • QT Prolongation • Use with caution in patients with
moderate/severe hepatic impairment • Use not recommended in patients with severe
renal impairment • CYP2D6 poor metabolizers
>10%: CNS: Drowsiness (≤11%), fatigue (≤11%), sedation (≤11%) 1% to 10%: CNS: Abnormal gait (≤4%), dizziness (≤4%), equilibrium disturbance (≤4%), falling (≤4%), akathisia (≤3%), restlessness (≤3%), anxiety (≥1% to <2%), drooling (≥1% to <2%), extrapyramidal reaction (≥1% to <2%), insomnia (≥1% to <2%) Endo&meta: Increased serum glucose (≥1% to <2%), weight gain (≥1% to <2%) GI: Vomiting (3%) NMS: Arthralgia (2%), dyskinesia (≥1% to <2%) Resp: Respiratory tract infection (≥1% to <2%)

30
Table 6. Adverse Events and Warnings for Movement Disorder Agents4-6,8-10,12,51 Generic Name Contraindications/Warnings Adverse Events
Anticholinergic Agents Benztropine Contraindications:
• Children <3 years of age No black box warnings Other warnings: • Anhidrosis/hyperthermia • Anticholinergic effects (constipation,
xerostomia, blurred vision, urinary retention) • CNS effects • Weakness • Use with caution in children >3 years of age
due to its anticholinergic effects, and in patients with CV disease, GI obstruction, glaucoma, prostatic hyperplasia/urinary stricture or retention
• Patients with tardive dyskinesia
Frequency not defined.
CV: Tachycardia
CNS: Confusion, depression, disorientation, heatstroke, hyperthermia, lethargy, memory impairment, nervousness, numbness of fingers, psychotic symptoms (exacerbation of pre-existing symptoms), toxic psychosis, visual hallucination
Derma: Skin rash
GI: Constipation, nausea, paralytic ileus, vomiting, xerostomia
GU: Dysuria, urinary retention
Ophth: Blurred vision, mydriasis
Trihexyphenidyl Contraindications: • Narrow angle glaucoma No black box warnings Other warnings: • Anhidrosis/hyperthermia • Anticholinergic effects (constipation,
xerostomia, blurred vision, urinary retention) • CNS effects • Ocular effects • Psychiatric effects • Use with caution in children >3 years of age
due to its anticholinergic effects, and in patients with CV disease, hepatic or renal impairment, GI obstruction, glaucoma, prostatic hyperplasia/ urinary stricture or retention
• Patients with tardive dyskinesia • Abrupt discontinuation of therapy: acute
exacerbations or adverse events
Frequency not defined: CV: Tachycardia CNS: Agitation, confusion, delusions, dizziness, drowsiness, euphoria, hallucination, headache, nervousness, paranoia, psychiatric disturbance Derma: Skin rash GI: Constipation, intestinal obstruction, nausea, parotitis, toxic megacolon, vomiting, xerostomia GU: Urinary retention NMS: Weakness Ophth: Blurred vision, glaucoma, increased intraocular pressure, mydriasis
Abbreviations: CNS, central nervous system; CV, cardiovascular; Derma, dermatologic; endo&meta: endocrine & metabolic; GI, gastrointestinal; GU, genitourinary; hema&onco; hematologic & oncologic; NMS, neuromuscular & skeletal; Ophth, Ophthalmic; Resp, respiratory

31
Summary
Movement disorder agents included in this report are indicated for the management of chorea associated with Huntington´s disease (tetrabenazine and deutetrabenazine), tardive dyskinesia (deutetrabenazine and valbenazine), all forms of parkinsonism (benztropine and trihexyphenidyl), and drug-induced extrapyramidal disorders (benztropine and trihexyphenidyl).
Following a systematic literature search for direct head-to-head comparisons among the movement disorder agents included in this report, no publications were identified. Evidence findings are highlighted below:
- Tetrabenazine versus deutetrabenazine for Huntington´s disease: No direct evidence comparing both agents was identified. Only placebo-controlled trials are available. Theoretical differences in pharmacokinetics and safety between tetrabenazine and deutetrabenazine are described in literature reviews and indirect comparisons. Tetrabenazine exhibits a short half-life, is rapidly metabolized to active metabolites, and may cause adverse events related to high peak plasma concentrations. Deutetrabenazine is more resistant to drug metabolism and has a prolonged half-life, which helps minimize high peak plasma concentrations, improves tolerability, and decreases dosing frequency. Genotyping for CYP2D6 is required for tetrabenazine doses above 50 mg daily. Labeling for deutetrabenazine does not require genotyping for CYP2D6; however, the maximum recommended dose should be reduced to 36 mg daily in poor CYP2D6 metabolizers. Tetrabenazine is usually administered 2 to 3 times daily with daily doses ranging from 12.5 mg to 100 mg, whereas deutetrabenazine is administered twice daily at lower daily dosing (6 mg to 48 mg). Evidence from indirect comparisons suggests similar efficacy but a better safety profile with deutetrabenazine compared to tetrabenazine, probably due to pharmacokinetic differences.
- Deutetrabenazine versus valbenazine for tardive dyskinesia: Deutetrabenazine and valbenazine are the first drugs approved for the treatment of tardive dyskinesia and have not been compared head-to-head in an RCT. Only placebo-controlled trials are available. Valbenazine is administered once daily, while deutetrabenazine is taken twice daily.
- Benztropine versus trihexyphenidyl for parkinsonism and drug-induced extrapyramidal disorders: no head-to-head comparative evidence was identified. Guidelines do not specify a preference for one agent over another.
Tetrabenazine and deutetrabenazine include a black box warning regarding depression and suicidal ideation in patients with Huntington disease. Other reported adverse events in these patients include drowsiness, somnolence, fatigue, akathisia, parkinsonism, anxiety, insomnia, and gastrointestinal disturbances. In the setting of tardive dyskinesia, somnolence was the most frequently reported adverse event with valbenazine treatment. Nasopharyngitis and insomnia were the most common adverse events reported for deutetrabenazine. Benztropine and trihexyphenidyl are associated with many anticholinergic side effects such as dry mouth, constipation, blurred vision, confusion, and urinary retention, and should be used cautiously in the elderly.
Overall, evidence is insufficient to confirm efficacy and safety differences between movement disorder agents. Well-conducted head-to-head RCTs are needed.
32
References 1. Simon RP, Aminoff MJ, Greenberg DA. Movement Disorders. In: Clinical Neurology, 10e. New
York, NY: McGraw-Hill Education; 2017. 2. Kasper DL, Fauci AS, Hauser SL, Longo DL, Jameson JL, Loscalzo J. Tremor and Movement
Disorders. In: Harrison's Manual of Medicine, 19e. New York, NY: McGraw-Hill Education; 2016.
3. Olanow CW, Schapira AHV, Obeso JA. Parkinson’s Disease and Other Movement Disorders. In: Kasper D, Fauci A, Hauser S, Longo D, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medicine, 19e. New York, NY: McGraw-Hill Education; 2015.
4. Austedo (deutetrabenazine) oral tablets [package insert]. North Wales, PA: Teva Pharmaceuticals USA, Inc; revised August, 2017.
5. Xenazine (tetrabenazine) oral tablets. Deerfield, IL: Lundbeck; revised September 2017. . 6. Ingrezza (valbenazine) oral tablets. San Diego, CA: Neurocrine Biosciences, Inc.; revised April
2017. 7. Benztropine mesylate injection. West-Ward Pharmaceutical Corp; revised May 2014. 8. Benztropine mesylate oral tablets. Par Pharmaceutical; revised June 2017. 9. Trihexyphenidyl hydrochloride oral solution. VersaPharm Incorporated; revised May 2013. 10. Trihexyphenidyl hydrochloride oral tablets. Kaiser Foundation Hospitals; revised December
2017. 11. U.S. Food & Drug Administration. Search Orphan Drug Designations and Approvals.
https://www.accessdata.fda.gov/scripts/opdlisting/oopd/listResult.cfm. Accessed February 12, 2018.
12. Lexicomp. Wolters Kluwer; 2018. http://online.lexi.com/action/home. Accessed January 29, 2018.
13. Bashir H, Jankovic J. Treatment options for chorea. Expert review of neurotherapeutics. 2018;18(1):51-63.
14. Cepeda C, Murphy KP, Parent M, Levine MS. The role of dopamine in Huntington's disease. Progress in brain research. 2014;211:235-254.
15. Huntington Study Group. Living with HD. http://huntingtonstudygroup.org/. Accessed January 30, 2018.
16. Armstrong MJ, Miyasaki JM. Evidence-based guideline: pharmacologic treatment of chorea in Huntington disease: report of the guideline development subcommittee of the American Academy of Neurology. Neurology. 2012;79(6):597-603.
17. Olanow CW, Schapira AHV. Chapter 372. Parkinson's Disease and Other Movement Disorders. In: Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison's Principles of Internal Medicine, 18e. New York, NY: The McGraw-Hill Companies; 2012.
18. Rudolph JN, Walker RH. Chapter 211. Parkinson Disease and Related Disorders. In: McKean SC, Ross JJ, Dressler DD, Brotman DJ, Ginsberg JS, eds. Principles and Practice of Hospital Medicine. New York, NY: The McGraw-Hill Companies; 2012.
19. Goetz CG. The history of Parkinson's disease: early clinical descriptions and neurological therapies. Cold Spring Harbor perspectives in medicine. 2011;1(1):a008862.
20. Parkinson's Disease Risk Factors. 2016. http://www.parkinsons.org/parkinsons-risk-factors.html. 21. Galifianakis NB, Ghazinouri A. Parkinson Disease & Essential Tremor. In: Williams BA,
Chang A, Ahalt C, et al., eds. Current Diagnosis & Treatment: Geriatrics, 2e. New York, NY: McGraw-Hill Education; 2014.
22. National Institute for Health and Care Excellence (NICE) guideline NG71. Parkinson’s disease in adults: diagnosis and management. Methods, evidence and recommendations, July 2017.

33
23. Grimes D, Gordon J, Snelgrove B, et al. Canadian Guidelines on Parkinson's Disease. The Canadian journal of neurological sciences Le journal canadien des sciences neurologiques. 2012;39(4 Suppl 4):S1-30.
24. Oertel WH, Berardelli A, Bloem BR, et al. Early (Uncomplicated) Parkinson's Disease. In: European Handbook of Neurological Management. Wiley-Blackwell; 2010:217-236.
25. Practice parameters: initial therapy of Parkinson's disease (summary statement). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 1993;43(7):1296-1297.
26. Rao SS, Hofmann LA, Shakil A. Parkinson's disease: diagnosis and treatment. American family physician. 2006;74(12):2046-2054.
27. Tonda ME, Guthrie SK. Treatment of acute neuroleptic-induced movement disorders. Pharmacotherapy. 1994;14(5):543-560.
28. American Psychiatric Association Practice Guideline for the Treatment of Patients With Schizophrenia Second Edition, 2004.
29. American Psychiatric Association Guideline Watch (September 2009): Practice Guideline for the Treatment of Patients with Schizophrenia.
30. Pereira SR, Albert M. Anticholinergic discontinuation for antipsychotic-induced extra-pyramidal symptoms. Cochrane Database of Systematic Reviews. 2017;2017(3).
31. National Collaborating Centre for Mental H. National Institute for Health and Clinical Excellence: Guidance. In: Psychosis and Schizophrenia in Children and Young People: Recognition and Management. Leicester (UK): British Psychological Society Copyright (c) The British Psychological Society & The Royal College of Psychiatrists.; 2013.
32. Novick D, Haro JM, Bertsch J, Haddad PM. Incidence of extrapyramidal symptoms and tardive dyskinesia in schizophrenia: thirty-six-month results from the European schizophrenia outpatient health outcomes study. Journal of clinical psychopharmacology. 2010;30(5):531-540.
33. Taylor D, Paton C, Kapur S. The Maudsley Prescribing Guidelines (10th Edition). London: Informa Healthcare, 2009.
34. Camilleri M, Parkman HP, Shafi MA, Abell TL, Gerson L. Clinical guideline: management of gastroparesis. The American journal of gastroenterology. 2013;108(1):18-37; quiz 38.
35. European Medicines Agency. European Medicines Agency recommends changes to the use of metoclopramide. 26 July 2013 (EMA/443003/2013).
36. Bergman H, Walker DM, Nikolakopoulou A, Soares-Weiser K, Adams CE. Systematic review of interventions for treating or preventing antipsychotic-induced tardive dyskinesia. Health technology assessment (Winchester, England). 2017;21(43):1-218.
37. El-Sayeh HG, Rathbone J, Soares-Weiser K, Bergman H. Non-antipsychotic catecholaminergic drugs for antipsychotic-induced tardive dyskinesia. The Cochrane database of systematic reviews. 2018;1:Cd000458.
38. Tarsy D, Lungu C, Baldessarini RJ. Epidemiology of tardive dyskinesia before and during the era of modern antipsychotic drugs. Handbook of clinical neurology. 2011;100:601-616.
39. Bhidayasiri R, Fahn S, Weiner WJ, Gronseth GS, Sullivan KL, Zesiewicz TA. Evidence-based guideline: treatment of tardive syndromes: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology. 2013;81(5):463-469.
40. American Psychiatric Association. Tardive dyskinesia: a task force report of the American Psychiatric Association. Washington DC: American Psychiatric Association, 1980.
41. Tardive dyskinesia: summary of a Task Force Report of the American Psychiatric Association. By the Task Force on Late Neurological Effects of Antipsychotic Drugs. The American journal of psychiatry. 1980;137(10):1163-1172.
42. Suchowersky O, Gronseth G, Perlmutter J, Reich S, Zesiewicz T, Weiner WJ. Practice Parameter: neuroprotective strategies and alternative therapies for Parkinson disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2006;66(7):976-982.

34
43. Pringsheim T, Doja A, Belanger S, Patten S. Treatment recommendations for extrapyramidal side effects associated with second-generation antipsychotic use in children and youth. Paediatrics & child health. 2011;16(9):590-598.
44. Yero T, Rey JA. Tetrabenazine (Xenazine), An FDA-Approved Treatment Option For Huntington's Disease-Related Chorea. P & T : a peer-reviewed journal for formulary management. 2008;33(12):690-694.
45. Chen JJ, Ondo WG, Dashtipour K, Swope DM. Tetrabenazine for the treatment of hyperkinetic movement disorders: a review of the literature. Clinical therapeutics. 2012;34(7):1487-1504.
46. Jankovic J. Dopamine depleters in the treatment of hyperkinetic movement disorders. Expert opinion on pharmacotherapy. 2016;17(18):2461-2470.
47. Caroff SN, Aggarwal S, Yonan C. Treatment of tardive dyskinesia with tetrabenazine or valbenazine: a systematic review. Journal of comparative effectiveness research. 2017.
48. Citrome L. Deutetrabenazine for tardive dyskinesia: A systematic review of the efficacy and safety profile for this newly approved novel medication-What is the number needed to treat, number needed to harm and likelihood to be helped or harmed? International journal of clinical practice. 2017;71(11).
49. Coppen EM, Roos RA. Current Pharmacological Approaches to Reduce Chorea in Huntington's Disease. Drugs. 2017;77(1):29-46.
50. American Geriatrics Society 2015 Updated Beers Criteria for Potentially Inappropriate Medication Use in Older Adults. Journal of the American Geriatrics Society. 2015;63(11):2227-2246.
51. Micromedex (electronic version). Truven Health Analytics; 2018. http://www.micromedexsolutions.com/. Accessed January 30, 2018.
52. Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
53. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS medicine. 2009;6(7):e1000097.
54. Group HS, Frank S, Testa CM, et al. Effect of Deutetrabenazine on Chorea Among Patients With Huntington Disease: A Randomized Clinical Trial. Jama. 2016;316(1):40-50.
55. Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial. Neurology. 2006;66(3):366-372.
56. Rodrigues FB, Duarte GS, Costa J, Ferreira JJ, Wild EJ. Tetrabenazine Versus Deutetrabenazine for Huntington's Disease: Twins or Distant Cousins? Movement disorders clinical practice. 2017;4(4):582-585.
57. Anderson KE, Stamler D, Davis MD, et al. Deutetrabenazine for treatment of involuntary movements in patients with tardive dyskinesia (AIM-TD): a double-blind, randomised, placebo-controlled, phase 3 trial. The lancet Psychiatry. 2017;4(8):595-604.
58. Citrome L. Valbenazine for tardive dyskinesia: A systematic review of the efficacy and safety profile for this newly approved novel medication-What is the number needed to treat, number needed to harm and likelihood to be helped or harmed? International journal of clinical practice. 2017;71(7).
59. Bergman H, Soares-Weiser K. Anticholinergic medication for antipsychotic-induced tardive dyskinesia. The Cochrane database of systematic reviews. 2018;1:Cd000204.
60. Yassa R. Tardive dyskinesia and anticholinergic drugs. A critical review of the literature. L'Encephale. 1988;14 Spec No:233-239.
61. Hauser RA, Factor SA, Marder SR, et al. KINECT 3: A Phase 3 Randomized, Double-Blind, Placebo-Controlled Trial of Valbenazine for Tardive Dyskinesia. The American journal of psychiatry. 2017;174(5):476-484.

35
62. Thai-Cuarto D, O'Brien CF, Jimenez R, Liang GS, Burke J. Cardiovascular Profile of Valbenazine: Analysis of Pooled Data from Three Randomized, Double-Blind, Placebo-Controlled Trials. Drug safety. 2017.
63. NDA 21-894 Xenazine® (tetrabenazine). Risk Evaluation and Mitigation Stategy (REMS). Revised August 2014. https://www.fda.gov/downloads/Drugs/DrugSafety/PostmarketDrugSafetyInformationforPatientsandProviders/ucm129514.pdf. Accessed February 7, 2018.
64. Claassen DO, Carroll B, De Boer LM, et al. Indirect tolerability comparison of Deutetrabenazine and Tetrabenazine for Huntington disease. Journal of clinical movement disorders. 2017;4:3.
65. Frank S. Tetrabenazine as anti-chorea therapy in Huntington disease: an open-label continuation study. Huntington Study Group/TETRA-HD Investigators. BMC neurology. 2009;9:62.
66. O'Brien CF, Jimenez R, Hauser RA, et al. NBI-98854, a selective monoamine transport inhibitor for the treatment of tardive dyskinesia: A randomized, double-blind, placebo-controlled study. Movement disorders : official journal of the Movement Disorder Society. 2015;30(12):1681-1687.
67. Factor SA, Remington G, Comella CL, et al. The Effects of Valbenazine in Participants with Tardive Dyskinesia: Results of the 1-Year KINECT 3 Extension Study. The Journal of clinical psychiatry. 2017;78(9):1344-1350.
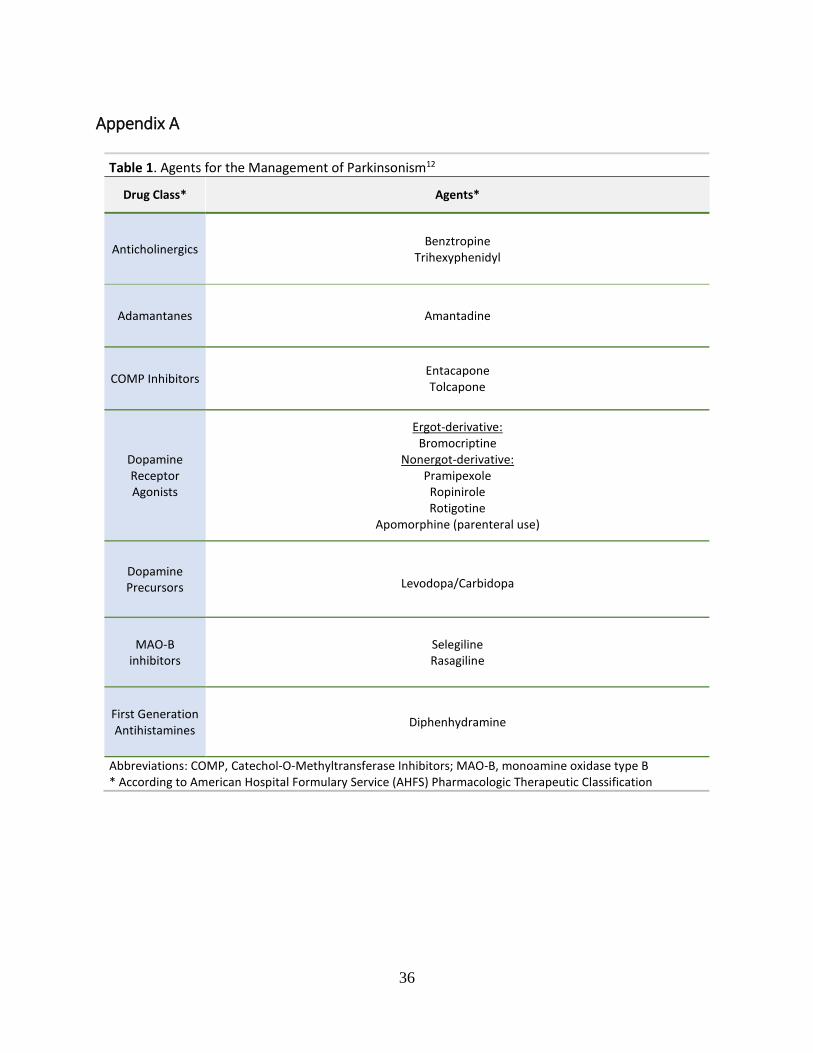
36
Appendix A
Table 1. Agents for the Management of Parkinsonism12
Drug Class* Agents*
Anticholinergics Benztropine Trihexyphenidyl
Adamantanes Amantadine
COMP Inhibitors Entacapone Tolcapone
Dopamine Receptor Agonists
Ergot-derivative: Bromocriptine
Nonergot-derivative: Pramipexole
Ropinirole Rotigotine
Apomorphine (parenteral use)
Dopamine Precursors Levodopa/Carbidopa
MAO-B inhibitors
Selegiline Rasagiline
First Generation Antihistamines Diphenhydramine
Abbreviations: COMP, Catechol-O-Methyltransferase Inhibitors; MAO-B, monoamine oxidase type B * According to American Hospital Formulary Service (AHFS) Pharmacologic Therapeutic Classification

37
Appendix B Table 1. Medline Literature Search Strategy for SRs and RCTs
Ovid MEDLINE(R) without Revisions 1996 to January Week 4 2018, Ovid MEDLINE(R) Epub Ahead of Print February 02, 2018, Ovid MEDLINE(R) In-Process & Other Non-Indexed Citations February 02, 2018, Ovid MEDLINE(R) Daily Update February 02, 2018 Search Date: February 6, 2018
# Searches Results
1 Meta-Analysis/ 80779
2 (metaanaly$ or meta-analy$).ti,ab,kw,kf. 119168
3 ((systematic adj3 review) or (overview adj4 review)).ti,kw,kf. 81213
4 (cochrane$ or systematic review?).jw. 14955
5 (or/1-4) and English.la. [SR Filter] 179990
6 (randomized controlled trial or controlled clinical trial).pt. or randomized.ab. or placebo.ab. or clinical trials as
topic.sh. or randomly.ab. or trial.ti. 888590
7 exp animals/ not humans.sh. 2169217
8 (6 not 7) and English.la. [Cochrane RCT Filter 6.4.d Sens/Precision Maximizing] 763621
9 Benztropine/ or Tetrabenazine/ or Trihexyphenidyl/ 809
10 (valbenazin$ or valbenazin$ or benztropin$ or deutetrabenazin$ or tetrabenazin* or
trihexyphenidy).ti,ab,kw,kf. 708
11 or/9-10 [Drugs of Interest] 1191
12 exp Movement Disorders/ 82408
13 parkinsonian disorders/ or parkinson disease/ 47338
14 Tardive Dyskinesia/ or Dyskinesia, Drug-Induced/ 3364
15 (parkinsonian* or (parkinson* adj2 (disease? or disorder* or syndrome* or symptom*))).ti,ab,kw,kf. 72566
16 (chorea$ adj3 (chronic or disease? or disorder? or hereditary or progressiv$ or rheumatic$ or senile or
sydenham$ or syndrom$)).ti,ab,kw,kf. 955
17 extrapyramidal$.ti,ab,kw,kf. 6125
18 ((medication? or drug?) adj2 (related or induced) adj2 (chorea$ or tremor? or (impaired adj2 (motor or
movement?)) or muscl* rigidity)).ti,ab,kw,kf. 65
19 (movement? adj2 (abnormal or involuntar* or disorder? or paroxysmal$ or syndrome? or
disease?)).ti,ab,kw,kf. 15855
20 Dyskinesi*.ti,ab,kw,kf. 9487

38
21 Huntington Disease/ 7152
22 (huntington? adj10 chorea$).ab,kw,kf. or (huntington? and (chorea$ or disease? or disorder? or syndrom$)).ti. 6048
23 or/12-22 [Indications] 125360
24 Vesicular Monoamine Transport Proteins/ 934
25 Cholinergic Antagonists/ 3811
26 ((anticholinergic? or anti-cholinergic?) adj2 (agent? or drug?)).ti,ab,kw,kf. 2236
27 (cholinergic? adj2 (antagonist? or blocker or inhibitor?)).ti,ab,kw,kf. 927
28 (Vesicular Monoamine Transport$ adj2 (inhibitor? or blocker?)).ti,ab,kw,kf. 51
29 ((VMAT or VMAT2 or VMAT-2) adj2 (inhibitor? or antagonist? or blocker?)).ti,ab,kw,kf. 98
30 or/24-29 [Drug Classes] 7102
31 and/5,11 [Drugs & SR ] 19
32 and/5,23,30 [Drug Class & Indications & SR] 29
33 and/8,11 [Drugs & RCT--1996-] 117
34 and/8,23,30 [Drug Classs & Indications & RCT 1996-] 104
35 31 or 32 42
36 remove duplicates from 35 38
37 33 or 34 195
38 remove duplicates from 37 [RCTs to export] 192
Table 2. EMBASE Literature Search Strategy for SRs and RCTs Databases: EMBASE.COM; Search Date: Feb. 6, 2018 No. Query
Results 46
#36 #6 AND #35 OR (#11 AND #25 AND #35)
175,497 #35 (cochrane*:jt OR 'systematic review*':jt OR 'meta analysis'/mj OR 'systematic review'/mj OR ((systematic NEAR/3 review):ti) OR 'meta analys*':ti,ab,kw OR metaanalys*:ti,ab,kw OR ((overview NEAR/4 (review OR reviews)):ti)) NOT ('conference abstract'/it OR 'conference review'/it) AND [english]/lim
134 #34 #32 AND #33
20,636,499 #33 1996:py OR 1997:py OR 1998:py OR 1999:py OR 2000:py OR 2001:py OR 2002:py OR 2003:py OR 2004:py OR 2005:py OR 2006:py OR 2007:py OR 2008:py OR 2009:py OR 2010:py OR 2011:py OR 2012:py OR 2013:py OR 2014:py OR 2015:py OR 2016:py OR 2017:py OR 2018:py
344 #32

39
#30 OR #31 144
#31 #11 AND #25 AND #29
236 #30 #6 AND #29
608,384 #29 #26 NOT (#27 OR #28)
2,600,211 #28 animal*:ti OR beaver*:ti OR beef:ti OR bovine:ti OR breeding:ti OR canine:ti OR castoris:ti OR cat:ti OR cattle:ti OR cats:ti OR chicken*:ti OR cow:ti OR dog:ti OR dogs:ti OR equine:ti OR foal:ti OR foals:ti OR fish:ti OR insect*:ti OR livestock:ti OR mice:ti OR mouse:ti OR murine:ti OR plant:ti OR plants:ti OR pork:ti OR porcine:ti OR protozoa*:ti OR purebred:ti OR rabbit*:ti OR rat:ti OR rats:ti OR rodent*:ti OR sheep:ti OR thoroughbred:ti OR veterinar*:ti,ab,de
6,398,399 #27 ('animal'/exp OR 'invertebrate'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'animal tissue'/exp OR 'animal cell'/exp OR 'nonhuman'/de) NOT (('animal'/exp OR 'invertebrate'/exp OR 'animal experiment'/exp OR 'animal model'/exp OR 'animal tissue'/exp OR 'animal cell'/exp OR 'nonhuman'/de) AND ('human'/exp OR 'human cell'/de))
640,712 #26 ('clinical study'/mj OR 'clinical trial'/mj OR 'controlled clinical trial'/mj OR 'controlled study'/mj OR 'major clinical study'/mj OR 'randomized controlled trial'/mj OR 'control group'/mj OR (((clinical OR randomi* OR controlled OR multicentre OR multicenter OR 'multi centre' OR 'multi center') NEAR/3 (study OR trial)):ti,ab) OR placebo:ab,ti OR 'head to head':ti,ab) AND [english]/lim NOT ('conference abstract'/it OR 'conference review'/it)
166,616 #25 #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 OR #24
3,857 #24 ((chorea* OR extrapyramid*) NEAR/3 (disease* OR disorder* OR syndrom*)):ti,ab,kw
2,229 #23 (huntington* NEAR/10 chorea):ti,ab,kw
21,089 #22 dyskinesi*:ti,ab,kw
26,128 #21 (disorder* NEAR/2 ('motor function*' OR 'motor skill*' OR movement*)):ti,ab,kw
140 #20 (('medication* related' OR 'medication induced' OR 'drug related' OR 'drug induced') NEAR/2 (chorea* OR tremor*)):ti,ab,kw
15,062 #19 ((chorea* NEAR/3 (chronic OR disease* OR disorder* OR progressiv* OR senile OR syndrom*)):ti,ab,kw) OR extrapyramidal*:ti,ab,kw
6,581 #18 (parkinson* NEAR/2 symptom*):ti,ab,kw
9,125 #17 (parkinson* NEAR/2 syndrom*):ti,ab,kw
15,508 #16 'parkinson* disease*':ti,ab,kw
22,439 #15

40
'parkinsonism':ti,ab,kw 22,202
#14 'motor dysfunction'/mj
5,262 #13 'tardiv* dyskines*':ti,ab,kw
110,483 #12 'parkinson disease'/exp/mj OR 'extrapyramidal symptom'/mj OR 'akathisia'/mj OR 'chorea'/mj OR 'tardive dyskinesia'/mj OR 'dyskinesia'/exp/mj OR 'motor dysfunction'/mj
19,391 #11 #7 OR #8 OR #9 OR #10
10,614 #10 'cholinergic receptor blocking agent'/mj
1,272 #9 'vesicular monoamine transporter 2'/de
195 #8 (('vesicular monoamine transport*' NEAR/2 (inhibitor* OR blocker*)):ti,ab,kw) OR (((vmat OR vmat2 OR 'vmat-2') NEAR/2 (inhibitor* OR antagonist* OR blocker*)):ti,ab,kw)
9,975 #7 anticholinergics:ti,ab,kw OR 'anti-cholinergics':ti,ab,kw OR parasympathicolytics:ti,ab,kw OR (((cholinolytic OR anticholinergic OR 'anti-cholinergic' OR parasympathetic) NEAR/3 (agent OR agents OR drug OR drugs)):ti,ab,kw) OR (((acetycholine OR atropinic*) NEAR/3 (agent OR agents OR antagonist* OR blocker* OR blocking OR drug OR drugs OR inhibitor OR inhibitors)):ti,ab,kw) OR 'achr inhibitor':ti,ab,kw OR 'achr inhibitors':ti,ab,kw
4,750 #6 #1 OR #2 OR #3 OR #4 OR #5
81 #5 'valbenazine'/de OR valbenazin*:ti,ab,kw
2,607 #4 'trihexyphenidyl'/mj OR trihexyphenidyl*:ti,ab,kw OR artane:ti,ab,kw
1,783 #3 'tetrabenazine'/mj OR tetrabenazin*:ti,ab,kw
104 #2 'deutetrabenazine'/de OR deutetrabenazin*:ti,ab,kw
362 #1 'benzatropine'/mj OR benzatropin*:ti,ab,kw

41
Appendix C Table 1. Placebo-Controlled Trials Including VMAT-2 Inhibitor Agents
Clinical Studies Study Design Study Duration/ Participants Results for Primary Endpoint
Huntington’s Disease
Tetr
aben
azin
e
TETRA-HD, HSG (2006)55
Randomized, double-blind, placebo controlled
12 weeks N=84
Primary efficacy endpoint: : Total Maximal Chorea Score, an item of the Unified Huntington's Disease Rating Scale (UHDRS)a Treatment effect: • 3.5-unit reduction in UHDRS chorea score
(Significant differences between groups) TETRA-HD Extension (2009)65
Open-label randomized controlled study
80 weeks N= 75
Primary efficacy endpoint: UHDRS total Maximal Chorea Score • 4.6-unit reduction in UHDRS chorea Score (Significant improvement in favor of TBZ)
Deut
etra
bena
zine FIRST-HD,
HSG (2016)54 Randomized, double-blind, placebo controlled
12 week N=90
Primary efficacy endpoint: UHDRS total Maximal Chorea Score • 2.5 unit reduction in UHDRS chorea score
(p<0.0001) (Significant differences between groups)
Tardive Dyskinesia
Deut
etra
bena
zine
Study 1 (AIM-TD, 2017)57
Randomized, double-blind, placebo-controlled, multi-center trial
12 weeks N=224
Primary efficacy endpoint: Abnormal Involuntary Movement Scale (AIMS)b to assess TD severity • Deu 36 mg: -1.9 unit reduction
(-3.09, -0.79) (Significant improvement in favor of Deu)
• Deu 24 mg: -1.8 unit reduction (-3.00, -0.63) (Significant improvement in favor of Deu)
• Deu 12 mg: -0.7 unit reduction (-1.84, 0.42)
Study 24 Randomized, double-blind, placebo-controlled, multi-center trial
12 weeks N= 113
Primary efficacy endpoint: AIMS total score • 1.4 unit reduction in AIMS (3.0 units of
improvement in Deu vs. 1.6 placebo) (Significant improvement in favor of Deu)
Valb
enaz
ine
KINECT 266 Randomized, double-blind, placebo-controlled (Phase II study)
6 weeks N= 100
Primary efficacy endpoint: AIMS total score, LS mean change from baseline to week 6: • -0.2 placebo, -2.6 valbenazine (p = 0.001)
(Significant improvement in favor of valbenazine)

42
KINECT 3 (2017)61 Randomized, double-blind, placebo-controlled
6 weeks N= 227
Primary efficacy endpoint: AIMS total score, LS mean change from baseline to week 6: • -0.1 placebo, -3.2 valbenazine 80 mg
(p< 0.001) (Significant improvement in favor of valbenazine)
KINECT 3 Extension (2017)67
Double-blind extension of KINECT 3
Up to 48 weeks plus 4-week Washout N=198
Primary efficacy endpoint: AIMS total score, LS mean change from baseline to week 48: • -4.8 valbenazine 80 mg, -3.0 valbenazine 40 mg
(statistically significant improvements relative to baseline in both dose groups)
Abbreviation: AIMS, Abnormal Involuntary Movement Scale; Deu, deutetrabenzazine; LS, least square; TD, tardive dyskinesia; TBZ, tetrabenazine; UHDRS, Unified Huntington's Disease Rating Scale Notes: a UHDRS: scale where chorea is rated from 0 to 4 (with 0 representing no chorea) for 7 different parts of the body. The total score ranges from 0 to 28. b AIMS: 12-item scale; items 1 to 7 assess the severity of involuntary movements across body regions and these items were used in this study. Each of the 7 items was scored on a 0 to 4 scale, rated as: 0=not present; 1=minimal, may be extreme normal (abnormal movements occur infrequently and/or are difficult to detect); 2=mild (abnormal movements occur infrequently and are easy to detect); 3=moderate (abnormal movements occur frequently and are easy to detect) or 4 =severe (abnormal movements occur almost continuously and/or of extreme intensity).
43
Appendix D
Table 1. List of Excluded References Wrong study design: Indirect Comparisons 1. Claassen DO, Carroll B, De Boer LM, et al. Indirect tolerability comparison of Deutetrabenazine and
Tetrabenazine for Huntington disease. Journal of clinical movement disorders. 2017;4:3. 2. Rodrigues FB, Duarte GS, Costa J, Ferreira JJ, Wild EJ. Tetrabenazine Versus Deutetrabenazine for
Huntington's Disease: Twins or Distant Cousins? Movement disorders clinical practice. 2017;4(4):582-585.





























