Embed Size (px)
Citation preview

Uterine Fibroid Embolization
(UFE)
Lukasz S. Babiarz, Harvard Medical School Year IVGillian Lieberman, MD
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
September 2008

2
Agenda
•
Uterine Fibroids: Background•
Case Presentation
•
Post-embolization
Complications/Issues•
Literature Review–
MRI Characteristics of Fibroids
–
Outcomes, UFE vs. Surgery
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

3
Uterine Fibroids: Epidemiology•
Uterine Fibroids are benign monoclonal tumors arising from the smooth muscle cells of the myometrium.
•
They are the most common benign neoplasm in females affecting 25% of white
and 50% of black
women during
their reproductive years.•
White women develop symptomatic fibroids in their 30s and 40s, whereas black women manifest disease at a younger age, even in their 20s.
•
The cumulative incidence of fibroids of any size by age 50 has been estimated as >80 percent for black women and almost 70 percent for white women.
•
Compared to white women, black women experience more severe disease
symptoms.
•
In most women uterine fibroids shrink at menopause.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

4
Uterine Fibroids: Risk Factors–
Parity ↓
–
Oral contraceptives ↓
(unless early exposure)–
Smoking ↓
–
Diet: red meats ↑
and vegetables ↓–
Early menarche ↑
–
Familial predisposition ↑–
Alcohol ↑
–
Hypertension ↑–
Uterine infection ↑
–
PCOS ↑
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

5
Uterine Fibroids: Symptoms•
Heavy
and/or prolonged menses
(menorrhagia)
•
Bulk-related symptoms–
Pelvic pressure resulting in urinary frequency, constipation, or hydronephrosis
–
Pelvic pain due to tumor degeneration or torsion
•
Reproductive dysfunction–
Infertility
–
Miscarriage–
Pregnancy complications (placental abruption, dysfunctional labor)
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

6
Our Patient: Presentation•
44 year-old G1P0 ♀, with a 2 year history of uterine fibroids and otherwise in good health, presented for uterine fibroid embolization
(UFE).
•
In last 2 months, she experienced increased pelvic clamping
and constant daily bloating, increased
urinary frequency, increased constipation, and one episode of urinary incontinence.
•
She denied having significant or irregular bleeding with or without her periods
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

7
US Imaging: Uterus
US revealed an enlarged fibroid uterusmeasuring 10.4 x 10.0 x 5.4 cm.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS BIDMC PACS

8
US Imaging: Right Fibroid
US revealed a large fibroid in the right fundusmeasuring 6.4 x 6.2 x 6.3 cm.
BIDMC PACS
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS

9
US Imaging: Left Fibroid
There is also a somewhat smaller fibroid in theleft fundus
measuring 5.4 x 4.3 x 4.5 cm.
BIDMC PACS
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS

10
MR Imaging: Coronal T2•
Coronal T2-weighted images (A-D; anterior to posterior).
•
The uterus is anteverted
and anteflexed
and measures 9.1 x 6.4 x 11.7
cm. Multiple fibroids are present (white oval).
•
The two largest fibroids are located in the right
lateral aspect (6.4 x 7.8 x 6.8 cm) and in the left
lateral aspect of the uterine body (5.4 x 4.3 x 4.2 cm) (white arrows).
•
Both fibroids have areas of heterogenous
T2 signal intensity.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS
ABIDMC PACS
B
BIDMC PACS
CBIDMC PACS
D

11
MR Imaging: Sagittal
and Axial T2•
Sagittal
(A-B; right to left) and axial (C-D; inferior to superior) T2-
weighted images.
•
The uterus is anteverted
and anteflexed
and measures 9.1 x 6.4 x 11.7
cm. Multiple fibroids
are present (white oval).
•
The two largest fibroids are located in the right
lateral aspect (6.4 x 7.8 x 6.8 cm) and in the left
lateral aspect of the uterine body (5.4 x 4.3 x 4.2 cm) (white arrows).
•
Both fibroids have areas of heterogenous
T2 signal intensity.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS
BIDMC PACSBIDMC PACS
BIDMC PACS
BA
DC

12
Uterine Fibroid Embolization: Indications/Relative Contraindications
•
Indications: To relieve bothersome bulk-related symptoms and/or abnormal bleeding due to fibroids
•
Relative contraindications:–
Postmenopausal status (natural regression of fibroids)–
GnRH
agonists use (decreased uterine artery caliber/blood flow)–
Pedunculated/submucosal
fibroids (myomectomy/hysteroscopic
resection is preferred)
–
Adenomyosis
(hysterectomy is the definitive treatment)–
Previous internal iliac artery ligation (vascular compromise)–
Large/numerous fibroids–
Future pregnancy plans
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

13
Uterine Fibroid Embolization: Absolute Contraindications
•
Absolute contraindications:–
GU infection–
Malignancy–
Immunosuppression–
Vascular disease limiting access–
Contrast allergy –
Pregnancy
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

14
UFE: Procedure Steps
•
Performed under local anesthesia with moderate sedation:1) Percutaneous
access
is obtained via femoral artery
(most
often right fem. a.).2) Arteriogram is performed for visualization. Uterine
artery, ovarian/vesical
artery
branches supplying fibroids, and anatomic variations
are identified.
3) Catheter is passed into the distal uterine artery under fluoroscopic guidance and the embolizing
agent is
infused. The infusion is continued until flow to the fibroid/s ceases. The procedure is then repeated on the contralateral
side.
4) If necessary and feasible, utero-ovarian branches are embolized
with superselective
catheterization.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

15
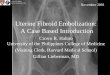
Patient’s UFE: Pre-embolization
Angiogram shows hypertrophy of the uterine arteries
with fibroid blush
(white arrows). No aberrant vessels or significant vesical/ovarian supply are seen.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD
BIDMC PACS
RIGHT
BIDMC PACS
LEFT

16
Patient’s UFE: Post-embolization•
Abdominal aortogram
demonstrates abrupt cut-off of the uterine arteries bilaterally
(white arrows), as expected. In addition, there is no evidence for any ovarian/vesical
arterial supply to the uterus.
BIDMC PACS
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

17
Post UFE Complications
•
Fever (2-4%)•
Readmission (2.4-3.5%)
•
Unplanned surgical procedure (1-2.5%)•
Allergic reaction (2.5%)
•
Hemorrhage (0.15-0.75%)•
Life-threatening event (0.2-0.5%)
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

18
Post-embolization
Issues•
Pain
–
related to fibroid/uterus ischemia; mild to severe with
variable duration; managed with PCA•
Vaginal discharge
–
bloody discharge can last ≥2 weeks
•
Postembolization
syndrome
–
occurs within 48 hrs and lasts up to 7 days; characterized by pelvic pain/cramping, nausea/vomiting, fever, fatigue, myalgias, and leukocytosis
•
Vaginal passage of fibroids
–
can occur up to a year post UFE
•
Undetected sarcoma
–
a handful of case reports of hysterectomies post UFE revealing low grade leiomyosarcoma
previously diagnosed as fibroids
•
Ovarian dysfunction
–
age-related transient or permanent loss of ovarian function; 1-2% risk in women <45, 15-20% risk in perimenopausal
women >45
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

19
UFE: Short-term Outcomes
•
Procedure is completed in
98-100%
of patients •
Improvement of abnormal bleeding in
85-94%
•
Improvement of dysmenorrhea
in
77-79%•
Significant improvement in quality of life in 95%
•
Additional invasive procedure in
14%•
Bulk-related symptoms controlled in 60-96%
•
Mean uterine volume reduced by 40-70%
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

20
MR Characteristics of Fibroids and Outcomes
•
Burn PR et al: –
18 women, 32 fibroids
–
On T1 pre and post
contrast compared fibroids with hyperintese
signal to those with hypointense
signal (relative to myometrium)–
Similarly, on T2
compared fibroids with
huperintense
signal to those with hypointense signal (relative to skeletal muscle)
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

21
Burn PR et al: Results
•
High T1
signal intensity before embolization was predictive of a poor response
to UFE (P
= .008)•
High T2
signal intensity was predictive of a
good response to UFE (P = .007)•
Contrast enhancement
signal characteristics
were not predictive
of post UFE uterine fibroid volume reduction
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

22
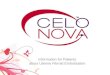
Burn PR et al: T1 MRI•
High signal
intensity
(relative to myometrium) seen on T1 MRI
results
from hemorrhagic necrosis
and the
presence of blood breakdown products. Thus, a fibroid that has outgrown its blood supply and degenerated
is
expected to show a poor response
to
UFE (black arrows).Burn PR et al. Radiology 2000 Mar;214(3):729-34
PRE UFE POST UFE
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

23
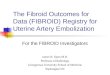
Burn PR et al: T2 MRI•
High signal
intensity
(relative to skeletal muscle) seen on T2 MRI
results from
increased cellularity and/or vascularity
(white arrows). This feature renders the fibroid susceptible to UFE. At times the T2 signal intensity is heterogeneous, which reflects the diverse histologic
composition
of fibroid.
Burn PR et al. Radiology 2000 Mar;214(3):729-34
PRE UFE POST UFE
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

24
UFE vs. Surgery•
Versus hysterectomy:–
Shorter procedure duration
(-16 minutes; 95% CI -26 to -7 minutes)–
Lower blood loss
(-405 mLs; 95% CI -512 to -298 mLs)–
Shorter hospitalization
(-3.3 d; 95% CI -3.8 to -2.8 d)–
Faster full recovery
(-27 d; 95% CI -36 to -17 d)–
MORE unscheduled visits (OR 1.8; 95% CI 0.98-3.30)–
HIGHER rate of readmission (OR 6.0; 95% CI 1.1-31.5) •
Versus myomectomy:–
Shorter procedure duration
(-34 minutes; 95% CI -49 to -20 minutes)–
Shorter hospitalization
(-1.6 d; 95% CI -2.5 to -0.7 d)–
Faster full recovery
(-16 d; 95% CI -21 to -12 d)–
HIGHER reintervention rate (OR 9; 95% CI 2-44)
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

25
References•
Huyck KL, Panhuysen CI, Cuenco KT, et al. The impact of race as a risk factor for symptom severity and age at diagnosis of uterine leiomyomata among affected sisters. Am J Obstet Gynecol 2008 Feb;198(2):168.e1-9.
•
Kjerulff KH, Langenberg P, Seidman JD, et al. Uterine leiomyomas. Racial differences in severity, symptoms and age at diagnosis. J Reprod Med 1996 Jul;41(7):483-90.
•
Day Baird D, Dunson DB, Hill MC, et al. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003 Jan;188(1):100-7.
•
Parazzini F, La Vecchia C, Negri E, et al. Epidemiologic characteristics of women with uterine fibroids: a case-control study. Obstet Gynecol 1988 Dec;72(6):853-7.
•
ACOG Committee Opinion. Uterine artery embolization. Obstet Gynecol 2004 Feb;103(2):403-4.•
SOGC clinical practice guidelines. Uterine fibroid embolization (UFE). Number 150, October 2004. Int J Gynaecol Obstet 2005 Jun;89(3):305-18.
•
Worthington-Kirsch R, Spies JB, Myers ER, et al. The Fibroid Registry for outcomes data (FIBROID) for uterine embolization: short-term outcomes. Obstet Gynecol 2005 Jul;106(1):52-9.
•
Spies JB, Spector A, Roth AR, et al. Complications after uterine artery embolization for leiomyomas. Obstet Gynecol 2002 Nov;100(5 Pt 1):873-80.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

26
•
Joyce A, Hessami S, Heller D. Leiomyosarcoma after uterine artery embolization. A case report. J Reprod Med 2001 Mar;46(3):278-80.
•
Goodwin SC, Spies JB, Worthington-Kirsch R, et al. Uterine Artery Embolization for Treatment of Leiomyomata: Long-Term Outcomes From the FIBROID Registry. Obstet Gynecol 2008 Jan;111(1):22-33.
•
Chrisman HB, Saker MB, Ryu RK, et al. The impact of uterine fibroid embolization on resumption of menses and ovarian function. J Vasc Interv Radiol 2000 Jun;11(6):699-703.
•
Burn PR, McCall JM, Chinn RJ, et al. Uterine fibroleiomyoma: MR imaging appearances before and after embolization of uterine arteries. Radiology 2000 Mar;214(3):729-34.
•
Kawakami S, Togashi K, Konishi I, et al. Red degeneration of uterine leiomyoma: MR appearances. J Comput Assist Tomogr 1994; 18:925-928.
•
Gupta J, Sinha A, Lumsden M, et al. Uterine artery embolization for symptomatic uterine fibroids. Cochrane Database Syst Rev 2006 Jan 25;(1):CD005073.
•
Edwards RD, Moss JG, Lumsden MA, et al. Uterine-artery embolization versus surgery for symptomatic uterine fibroids. N Engl J Med 2007 Jan 25;356(4):360-70.
•
Hehenkamp WJ, Volkers NA, Donderwinkel PF, et al. Uterine artery embolization versus hysterectomy in the treatment of symptomatic uterine fibroids (EMMY trial): peri- and postprocedural results from a randomized controlled trial. Am J Obstet Gynecol 2005 Nov;193(5):1618-29.
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD

27
Acknowledgements
•
Salomao
Faintuch, MD•
Gillian Lieberman, MD
•
Maria Levantakis•
Larry Barbaras
Lukasz S. Babiarz, HMS IVGillian Lieberman, MD