Embed Size (px)
Citation preview

AcknowledgementsTheauthoracknowledges Anita Moore, PT, DPT,ATC forsupervision, guidance, andassistance with patientcare,and thepatient forbeingawilling andhelpfulparticipant in this casereport.Contact [email protected] . Eng JJ, Tang P F.Gai t train in gstrategies to op timize walkin g ab i l i ty in p eop lewith stro ke: a syn thesis o f th eevid en ce. Exp ert RevNeu ro th er.
2 0 0 7 ;7 (1 0 ):1 4 1 7 -1 4 3 6 .d o i :1 0.1 5 8 6/1 4 7 3 7 17 5 .7 .1 0 .1 41 7 .Accessed June2 6 ,2 0 1 6 .2 . Lewek MD,Feasel J, Wen tz E, B rooks FP ,Wh itton MC .Useo fvi su al and p rop rio cep tive feedback to imp rove gai t sp eed and sp atio tempo ral
symmetry fo l lowin gch ron ic stro ke: acase series. Ph ysTh er. 2 0 1 2 ;9 2 (5 ):7 4 8 -7 5 6 .d o i:1 0 .2 52 2 /p tj .2 01 1 0 2 06 .Accessed June1 5 ,2 0 1 6 .3 . 5 .Salb ach NM ,Mayo NE, Wood -Dauph inee S, Han ley JA,R ich ard s C L,Cô té R .A task-o rien ted in terven tion enhan ces walkin g d istan ce and speed in
th e fi rstyear po st stro ke: a randomized con tro l led trial . C l in Reh ab i l . 2 0 0 4 ;1 8 :5 09 -5 1 9 .d o i :10 .1 1 9/0 2 6 9 2 15 5 0 4 cr7 6 3 oa.Accessed June2 7 ,2 0 1 6 .4 . Andersson P ,Fran zen E.Effects o fweigh t-sh i ft train in g on walkin g ab i l i ty, ambu lation , and weigh t d istrib u tion in in d ividualswith ch ron ic stro ke: a
p i lo t stud y.To p Stro ke Reh a b i l . 2 0 1 5 ;2 2 (6 ):4 3 7 -4 3 .d o i :1 0 .1 17 9 /1 0 7 49 3 5 7 15 Z.0 0 0 0 00 0 0 0 52 .Accessed Ju ly9 , 2 0 1 6 .5 . Jo a K L,Kwon SY, Cho i JW,HongSE,K imCH, Jun gHY.C lassi fi cation o fwalkin g ab i l i tyo fh ou seho ld walkers versu s commun ity walkers b ased on K -
BBS,gai t velo ci ty and up righ tmo to r con tro l . Eu r JP h ysReh a b i l Med . 2 0 1 5 ;5 1 (5 ):6 1 9 -2 5 .Avai lab leat:
h ttp ://www.minervam ed ic a.i t/ en /jou rnals /eu rop a- med icophy sic a/ articl e.php?cod =R3 3 Y2 0 1 5N0 5A0 6 1 9 . Accessed Sep tember 1 8 ,2 0 1 6 .2 .Rehab Measu res: Fuel -Meyer Assessmen t, Activi ties-Speci fic Balan ce Con fid en ce Scale, Disab i l i ties o f th eArm, Shou lder,and Hand , SixM inu teWalkTest, Ten Meter Walk Test, Five Times Si t to Stand . Rehab Measu res web si te. Avai lab le at:h ttp ://www.rehabmea su re s.o rg /r ehab web / al l me asu r es. asp x?P ag eVi ew =Sh ar ed . Accessed Ju ly2 4 ,2 0 1 6
Utilization of Postural Control Training to Improve Gait Symmetry and Walking Ability in a Patient Following a Lacunar Stroke: A Case Report
Hannah C.Wilder, BS,DPT Student andAmyLitterini, PT, DPTDepartment of Physical Therapy, University ofNew England, Portland, Maine
Observations
Conclusion
Purpose
Withconsiderationofthemanyuniquefactorscontributingtothepatientasawhole,physicaltherapyinterventionsaddressedthepatient'sownmobilitygoalstoallowhimtoparticipatemorefullyinhisenvironmentandhaveagreateroverallqualityoflife.
Tooutlinephysicaltherapyrehabilitationthatutilizedposturalcontroltraining,task-orientedtraining,andvisualfeedbacktoimprovewalkingabilityandfunctionalcapacityinapatientfollowingalacunarstrokeaffectingtheinternalcapsule,basalganglia,andcerebellum.
FollowingtenvisitsofoutpatientPT,thepatientdemonstratedimprovementsinmobilityandfunction. Basedonhisself-reports,heperceivedagreater abilitytonegotiatestairsandaccesshistractortomowhisappleorchard.Thisplanofcaremaybebeneficialwhenappliedtootherpatientswithasimilarpresentation;however,furtherinvestigationiswarranted.
PTinterventionsprimarilyfocusedonimprovingthepatient'sfunctionalmobility,ambulationinparticular,throughposturalcontroltrainingandtask-orientedtraining. Aftertenoutpatientvisits,thepatientdemonstratedimprovementsingaitandposturalsymmetryonobservation.WithcontinuedPTinterventionoverthenexteightvisits,thepatient’simprovementsingaitallowedhimtosafelyaccesshisyardandorchardsathome,advancinghimfromalimitedhouseholdambulationability,toanunlimitedhouseholdambulationability.5
Foundation• Alterationsingaitisoneofthemostnotedimpairments
followingstroke1• Improvingwalkingabilityisoneofthemostcommongoals
amongstpatientswithstrokeundergoingrehabilitation1• Currentliterature describesvisualandproprioceptivefeedback
andtask-orientedtrainingaseffectiveinimprovinggaitspeed,mechanics,strength,andbalancefollowingstroke.2,3
• Basedontheresearch,posturalcontroltrainingmayimprovewalkingabilityfollowingstroke.4
http://www.intechopen.com/source/html/41746/media/image1.jpeg
Description• 67-year-oldmale• Appleorchardowner• Pastmedicalhistoryofatrialfibrillation• Co-morbidities:
• Intermittentclaudication,chronicleft(L)shouldersubluxation,andright(R)shoulderimpingementsyndrome
• Referred tooutpatientPTthreemonthspostalacunarischemicstrokeaffectingtheposteriorlimboftheinternalcapsule,thebasalganglia,andpartofthecerebellum
• HemiparesisofhisdominantsideLupperandlowerextremities• Resultantactivitylimitationsandparticipationrestrictions• Physicaltherapygoals
• Improvemobilityandendurance• Increasefunctionalindependentwithgait• Returntowork-relatedactivitiessuchascaringforhisappleorchard.
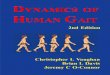
Figure1:Use of resistancebandasa walking aidtoassistwithcontrolattheleftankle,knee, andhipA: active hipextensiontoinitiateLLEswingphase of gait B:use of tapeforvisualcueof stepwidth
A. B.
•Verbal and visual cuing to increase speed, steplength, and stepwidth•Swing phase facilitation with band wrap•Ambulation with decreasing support overincreasing distance
GaitTraining
•Break up lower extremityextensor spasticpatternwith positioning and activemovement•Improve weight bearing ability through leftupper and lower extremities
NeuromuscularRe-Education
•Hamstring and hip abduction strengthening toimprove gaitmechanics and reduce lowerextremityextensor spasticity•Bilateral shoulder strengthening topreventfurther injury
TherapeuticExercise
•Proper transfermechanics•Recommendation forright heel liftand leftAFOadjustments•Home exercise program
Patient/FamilyEducation
Interventions
Unique