Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Burnout among dentists: Identification and prevention
Gorter, R.C.
Link to publication
Citation for published version (APA):Gorter, R. C. (2000). Burnout among dentists: Identification and prevention.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 27 Jan 2021

INTERVENTIONN STUDY 145 5
CHAPTERR 9
AA BURNOUT COUNSELLING PROGRAM FOR DENTISTS: EFFECTSS OF INTERVENTION
9.11 Introduction
Professionall burnout is considered a possible outcome of chronic inadequate copingg with occupational stress. As a metaphor, burnout refers to draining of energy;; more energy is lost than is replenished, similar to the dynamics of a car batteryy losing power.1 Generally, five core elements are recognised2: a) the individuall experiences symptoms of fatigue, exhaustion and depression; b) the emphasiss is on mental or behavioural rather than physical symptoms; c) burnout iss work related; d) the symptoms are exhibited in persons not previously known too suffer from mental health problems; and e) work performance is reduced. As aa topic of scientific study, burnout is usually defined as by Maslach3, consisting off emotional exhaustion, depersonalisation, and (diminished) personal accomplishment.. For a more comprehensive description of burnout and its currentt status in scientific perspective, one is referred to other authors.1"4
Burnoutt is regarded as a serious threat to the dental profession.5"6
Remarkably,, however, among all that was written about dentists and burnout, to thee best of our knowledge, no well-controlled empirical study on burnout interventionn among dentists was published. Moreover, empirical studies on burnoutt in dentistry, regardless of prevention, are very sparse. Nevertheless, the needd for preventive attention is well-understood.
9.1.11 Burnout prevention
Fromm studies among a variety of professions, not too much can be concluded aboutt the effects of burnout intervention. One author counted about ten studies thatt evaluate burnout intervention programs for human service professionals.7
Otherss categorised about thirty approaches to burnout intervention among a varietyy of professions.1 Yet another author states that there is no univocal answer too the question about what kind of intervention is most effective in reducing burnout.88 The general conclusion of these reviews is that the outcomes of evaluationn studies differ greatly. Training in coping skills, such as cognitive restructuringg and relaxation techniques, and facilitating social support have shownn some effect. However, methodological shortcomings of the evaluation studies,, such as lack of control groups, rather small numbers of subjects, or high

146 6 INTERVENTIONN STUDY
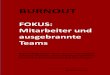
mortalityy in the sense of drop out at post-test stage, prevent firm conclusions aboutt the intervention effects. Moreover, the studies available are characterised byy a variety of samples, procedures, time frames, measurement instruments, and theoreticall approaches. Therefore, much about burnout intervention effects still needss to be explored. Without extensively discussing the available literature -thee sources above-mentioned provide for that very satisfactory - for our purposee Figure 9.1 may suffice to offer a short overview of the categorisation of approachess to burnout intervention.
Withh regard to the effectiveness of prevention at the three levels depicted in Figuree 9.1, the following was concluded.8 Most information is available on interventionss at the individual level, where relaxation techniques in combination withh cognitive coping techniques seem to have been most effective. On the effectivenesss of primary prevention at an individual level not much can be said withh certainty. At the organisational level, hardly anything can be said with confidence,, mainly because systematic research in a burnout context is lacking. Ass primary prevention, there is some indication that job-redesign and company fitnessfitness training do influence stress and job satisfaction positively, but generalisationn to burnout is not possible. As secondary prevention, there is some evidencee from one study that organisation development programs had a temporaryy burnout reducing effect. At the organisation - individual interface, timee management, interpersonal skill development, expectancy evaluation, assertivenesss training, and balancing work and private life often are part of primaryy prevention and seem to have positive results. Nevertheless, there is no informationn on the separate effectiveness of the specific contributors. As secondaryy prevention, there is an indication that establishing social support has bufferingg effects on the development of burnout, as well as relaxation techniques,, cognitive restructuring, and assertiveness training seem to influence burnoutt positively. Also individual psychotherapy, consisting of several of the above-mentionedd ingredients, is believed to give positive results, although so far onlyy case-based evidence exists.
Accordingg to Schaufeli & Enzmann, in burnout workshops several of the techniquess as depicted in Figure 9.1 are combined.1 Due to methodological shortcomingss and the lack of specificity of intervention, valid effect studies are hardd to identify. Nevertheless, effects on the burnout dimension emotional exhaustionn seem to have been established by multifaceted burnout workshops.
Att this point, one issue needs some clarification: the distinction between preventionn and intervention. Given the process character of burnout, and the fact thatt clinical validation has not yet been established satisfactory, distinguishing betweenn "burnout risk", "burning out", and "burned out" seems arbitrary. Subsequently,, the distinction between prevention, intervention, or treatment is arbitraryy too. Maslach recognised this dilemma before and prefers not to discriminatee between prevention and intervention too rigidly. Schaufeli &

o o
o o
e e
V)
V)
o o
3 3
O O
CQ
Q
O)
) 3.
. 5'
' a
a r*
r*
5' '
3 3
Stresss audit
Psychosociall check-up
Improvingg the job contentt and environment t
Timee scheduling
Management t development t
CareerCareer management
Retraining g
Corporatee fitness and wellnesss programs
Anticipatory y socialisation n
Conflictt management, communication,, and decision-making g
Organisational l development t
Institutionalisationn of Occupationall Health andd Safety Services
Employeee Assistance Programs s
O O
c
c _
_ 0>
>
O O
CD
D
3 3
CD D
3
3
Focu ss on individua l -organisationa l l interfac e e
-0 0
CD
D
CO O
0
0 3
3 EL L
CO
O
q q
CD D
CD
D
3 3
3' '
C
Q Q
Time-management t
Interpersonall skills training g
Promotingg a realistic imagee of the job
BalancingBalancing work and privatee life
Peer-supportt groups
Individuall peer-support
Coachingg and consultation n
Careerr planning
Specialisedd counselling
Psychotherapy y
Referral l
Individuall guidance andd assistance
Changee jobs
Tl l
O
O
O O
C
C
0)
)
0 0
3 3 5" "
Q
. .
<" "
ai
. ai.
c c
S)
)
Self-monitoring g
Self-assessment t
Didacticc stress management t
Promotingg a healthy lifestyle e
Cognitive-behavioural l techniques s
Relaxation n
0' '
I' '
3» »
-̂ ^
<
<
3 3 1 1
5' '
CD
D
c-j j
0
0
§ s s
0' '
Ï
Ï CD
D
3 3
=0 0
CD
D
S" "
0' '

148 8 INTERVENTIONN STUDY
Enzmann11 solve the dilemma by speaking of prevention when it concerns people stilll at work, to be called "at risk", and treatment when people are on sick-leave, too be called "actually burned out". Apparently, they consider burnout as the final stagee of a process. In line with this opinion, in the present study the phrasing "prevention"" wil l be used, because the subjects under study are active general dentall practitioners.
9.1.22 Burnout prevention among Dutch dentists
Although,, as mentioned above, no controlled empirical studies on burnout preventionn among dentists could be identified, in The Netherlands, some experiencee in this field exists. Comparing with previous five-year periods, Movirr Insurance4 noticed an increase in claims for disability over the years 1985-1990,, especially among physicians, veterinarians, and dentists. In many cases,, demotivation, job dissatisfaction, and burnout seemed to play a crucial role.. Subsequently, Movir initiated the development of a program, specially designedd for dentists. The aim of the program was to preventively pay attention too the pitfall of demotivation, and possibly burnout, in a dentist's career.10"13
Thee experiences with prevention programs for dentists can be summarised ass follows.b In a pilot version in 1993 fourteen dentists (7% of the invited) actuallyy participated. The central themes of the program - raising awareness of one'ss core capacities and talents, and taking first practical steps to give these capacitiess more emphasis in professional life - seemed to answer to the needs of thosee participating. The general conclusion of the participants was that the programm had helped them increase sense of control over private and professional life,, that self-awareness with regard to the central themes had grown, that the structuree of the program had helped in implementing changes, and that work motivationn was triggered positively. Even after several years, as evaluation reportss up to 1998 indicate, the majority of the participants of the pilot group keptt contact yearly by own initiative.
Afterr the pilot stage, between 1994 and 1998 a total of about sixty dentists participatedd in the programs, now labelled: "Practice on second thoughts". The basicc structure of the programs was: nine to twelve months period, monthly afternoonn group meetings, and individual counselling sessions throughout the program.. Invitations to participate were based on age group (around forty years off age), and final participation rate was, despite considerable financial support byy the insurance company, meanwhile maintaining anonymity, usually low (3-6%).. Reasons to not participate as often mentioned were: too much time consuming,, program too personal by nature, finances. When asked to
aa Movir Insurance is a Dutch mutual insurance company for disability among free entrepreneurss where, in 1997, more than 90% of the Dutch dentists were insured.
Unpublishedd internal reports by Van Ede Consulting, the Dutch resourcement and career developmentt agency that developed and organised the programs.

INTERVENTIONN STUDY 149 9
characterisee the long-term effects of the program, participants showing up at evaluationn meeting mentioned: more feelings of control, more self-consciousness,, feeling more free to ask for help, better time management, learningg to make choices, considering a sabbatical leave, or fully or partly implementedd career changes. In conclusion, in-company evaluations, as describedd in internal reports, sketch a positive image of the effects of participationn in the prevention programs, although participation among those whoo received invitations are very small.0
9.1.33 Prevention among dentists in a theoretical perspective
Whenn put into theoretical perspective, a few things must be noted about the programs.. First, the programs consist of a variety of the techniques depicted in Figuree 9.1. The focus is both on a purely individual level, as well as on the individuall - organisational interface. Furthermore, both identification, primary, andd secondary prevention are part of the program. The formula chosen goes well beyondd workshops, given the amount of meetings over time, and intensive individuall counselling. Second, it must also be noted that burnout prevention is nott explicitly the core of the program; personal and professional growth seems too be a more appropriate label. There is also no pre- or post-program assessment off burnout.
9.1.44 Aim of the study
Inn the present study, the aim was to examine the effect of the intervention as implementedd by the consulting agency. It was hypothesised that dentists who participatedd in the program would afterwards show lower levels of emotional exhaustionn and depersonalisation, and higher levels of personal accomplishment, whereass among non-participants this was not to be expected. Furthermore, it wass hypothesised that the percentage of dentists in burnout risk categories wouldd diminish most strongly among program participants.
9.22 Methods
9.2.11 Subjects
Inn April 1998 Dutch dentists who had participated in a national survey the year beforee received personal feedback on their burnout score as measured by Maslachh Burnout Inventory - Dutch version (MBI-NL ) (see chapter 5 of this thesis).. Dentists who were considered to form a "burnout risk group" (those with relativelyy unfavourable scores by median on all three subscales) also received
cc More detailed information about the programs and the evaluations is obtainable on request byy first author.

150 0 INTERVENTIONN STUDY
thee invitation to participate in a burnout prevention program. (The full risk groupp consisted of 144 dentists, 21% of all survey respondents; 13 of them were nott sent feedback or an invitation because they had indicated to prefer it this way;; which left a total of 131 dentists, or 18% of all respondents). In line with thee assumption that emotional exhaustion and depersonalisation are considered decisivee elements in the development of burnout2, dentists with unfavourable scoress on the scales EE and D, only not on PA, were also offered the possibility too participate. This concerned another 40 dentists or 6% of all survey respondents. .
9.2.22 Program
Togetherr with the invitation to participate in a prevention program, a brochure wass sent (Box 9.1 shows a translation). In comparison with the programs mentionedd in the introduction of this paper, some changes were implemented. Duee to time limits, a six months period had to be chosen instead of the nine to twelvee months time span. The program started in May / June 1998 with the first intakee sessions, and ended in November of the same year. At the same time, the characterr of the group meetings was intensified: instead of one monthly afternoonn session of approximately four hours, each group meeting now took 24 hours,, including overnight stay. Given the smaller number of individual and groupp sessions, some parts of the original program had to be skipped. However, thee themes discussed, the build up of the program, and the trainers and counsellorss remained the same.
9.2.33 Measures and design of study
Burnoutt was measured by the MBI-NL 15, which psychometric qualities among dentistss have been described in chapter 4 of this thesis.
Apartt from dentists who chose to participate in the program, those who decidedd not to participate were also followed. Since no ad random selection took place,, the design of the study is quasi experimental, with a pretest - posttest nonequivalentt control group design.15 As pretest the data from a national survey inn 1997 were taken, the posttest took place one month after the last group session.. Since non-participants could very well have undertaken preventive measuress individually, this was checked in the posttest questionnaire. Two groupss of non-participants were thus created: one group indicating to have taken thee initiative for preventive steps themselves, one group indicating to not have donee so.

INTERVENTIONN STUDY 151
Boxx 9.1 Program description "Practicee on second thoughts"
PROGRAM M
DesignedDesigned for: dentists who participated in the ACTA survey on work circumstances
Objective:Objective: to restore the balance by obtaining insight in one's own situation and workingg with a personal plan of action.
Contents: Contents:
(April/May) ) -- Intake: introduction to the agency and information on the program. After the
introductionn one is free to decide whether or not to participate;
(May) ) -- Brief biography: participants receive a questionnaire in order to prepare oneself
forr the program; answering the questions is estimated to take a two-weeks period; ;
(June) ) -- Individual counselling consult;
(September) ) WorkshopWorkshop I (3 half-days: Thursday evening - Friday afternoon) -- Development of vision: (re-) discovering personal talents and motivation;
transferencee towards a new vision and how to further develop this vision in personall and professional life;
-- Individual counselling consult;
(October) ) WorkshopWorkshop II (3 half-days: Thursday evening - Friday afternoon) -- Enterpreneurship with talents: vision on one's own practice, leisure t ime, and
personall development; how to deal with dilemma's and obstacles; how to make choices,, set priorities, and act inspired and effectively;
-- Individual counselling consult;
(November) ) WorkshopWorkshop III (3 half-days: Thursday evening - Friday afternoon) -- Communication and action: how to balance personal and professional life to
preventt losing energy; how to improve communication; how to deal wi th conflictingg interests; how to receive support; training of communication skills;
-- Conclusion wi th a personal plan of action; -- Individual counselling consult.
Thee program is suited to the individual's needs; the workshops facilitate individual differencess in development.

1522 INTERVENTION STUDY
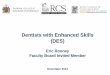
Inn Figure 9.2 the groups and measures are summarised:
Programm participants
Self-initiative e
Noo initiative
o. .
o3 3
o5 5
x. .
Y, ,
o2 2
o4 4
0 6 6
Figuree 9.2 Research design
Inn this design, Oi to 06are the MBI-measurements within the three groups, X] is thee "treatment" of the prevention program, and Y| is the non-specified "treatment"" of self-initiative by those who decided to not participate in the program.. The contents of this self-induced "treatment" is highly varied, and consistss of changes such as: having begun to work less hours, hiring more staff, takingg more breaks, or simply indicating to have become more aware of the problemm after the pretest and since then paying attention to one's own reaction too stressful situations.
9.2.44 Analyses
Pretestt and posttest results of the three MBI-NL scales were compared using Student'ss t (paired comparison) for testing differences between means. Given thee hypothesis that the prevention program or self-initiated activities wil l diminishh burnout levels, the program participants and the self-initiative group weree tested at a 0.05 significance level one-tailed; the no initiative group was testedd two-tailed since no clear diminishment or increase in burnout was expected.. Also, per scale a comparison was made with manual norm scores to indicatee possible changes in risk categories. Additionally, the frequencies of decreasee or increase on the MBI-NL scales were compared among the three groups.. Because of the small number of female participants, no gender differencess were calculated.
9.33 Results
9.3.11 Subjects
Off the 171 dentists invited to participate in the program, 45 (26%) appeared at thee agency for an intake session. Above that, a considerable number contacted thee agency by telephone. Three criteria were used by the agency to exclude a dentistt from participation: alcohol addiction or other substance dependency; interferencee with psychotherapy; and advise from the agency's psychologist. Afterr the intake sessions, one dentist was advised to seek help elsewhere, and twoo were advised to follow an alternative, individual program. All in all, 19

INTERVENTIONN STUDY 153 3
dentistss signed up for the program (11% of the invited). Of these, thirteen participatedd in the program as described in Box 9.1, and six chose to join a simultaneouslyy running regular program. Of the participants, four were females andd fifteen were males.
9.3.22 Response
Pretestt data were available of all subjects, since they were selected on basis of theirr scores at that time. Posttest data were gathered one month after the last groupp session of the program participants. Of the 19 program participants, who receivedd a questionnaire by mail, 17 responded within six weeks (89%). Of one respondent,, data were not usable.
Off those invited, but not participating in the program, 103 dentists received aa questionnaire; 88 men and 15 women. These were the original 171, minus the 199 program participants, the one dentist not accepted by the agency, and the two dentistss following individual counselling. Also, the 40 dentists with unfavourablee scores only on EE and D were not sent a posttest questionnaire sincee no one had responded. Finally, some dentists preferring to no longer participatee in the study were also kept from the posttest. Three questionnaires appearedd undeliverable. Within six weeks, 75 dentists responded (75%; 76% of thee men and 69% of the women). After the response period, another 3 dentists respondedd (3%), but their data were excluded from analyses.
9.3.33 Burnout levels
EmotionalEmotional exhaustion (EE): In an absolute sense, EE mean scores at the posttest weree lower for all three groups. For the program participants and the self-initiativee group, however, the difference between pretest and posttest was statisticallyy significant, while for the no initiative group the difference did not reachh statistical significance (Table 9.1).
Fromm the pretest - posttest correlations it can be learned that the direction of individuall subjects' change in scores was more or less similar within all groups. Standardd deviations of the program participants indicated that this group started moree homogeneously on EE when compared with the other two. The effect size Cohen'ss dd shows that among program participants almost 60% of the area coveredd by both pre- and posttest did not overlap, to be interpreted as a large
Thee effect size index Cohen's d gives an indication for the percentage of the area covered in pre-- and posttest that is not overlapped: d = 0, full overlap; d = 0.1, 7.7% not overlapped; d = 0.2,, 14.7% not overlapped; d = 0.5, 33% not overlapped; d = 0.8,47.4% not overlapped; d = 1.0,, 58.9% not overlapped; d = 2.0, 81.1% not overlapped; d = 4, 97.7% not overlapped.20 In otherr words, the higher the index, the larger the effect. In the context of behavioural science, Cohenn defined d values of 0.8 as being large differences.

1544 INTERVENTION STUDY
difference.. For the self-initiative group this was well over one third, meaning a mediumm difference, and for the no initiative group almost one third, meaning a smalll difference.
Tablee 9.1 Emotional exhaustion (EE): Mean scores, standard deviations, product moment coefficientt correlations, and Student's / tests
EE E
Pretestt -Meann (SD)
Posttestt -Meann (SD)
Pmcc c
Student'ss f test (pairedd samples)
Effectt size
ProgramProgram participants (N=(N= 16)
19.500 (4.76)
16.699 (5.03)
rr = 0.67, pp < 0.005
ff (15)= 2.83, pp = 0.006 (one-tailed)
dd = 1.00
Self-initiativeSelf-initiative group (N(N = 35)
21.377 (6.92)
18.299 (8.39)
rr = 0.55, pp = 0.001
ff (34)= 2.47, pp < 0.01 (one-tailed)
dd = 0.59
NoNo initiative group (N=31) (N=31)
23.455 (8.81)
20.877 (8.74)
rr = 0.59, pp < 0.001
ff (30)= 1.81, pp = 0.08 (two-tailed)
dd = 0.46
Apartt from testing differences in means also a comparison was made with norm scoress as described in the MBI-NL manual. For EE, the following categories are valid:: very low (scores less than 4), low (scores 4 to 9), moderate (scores 10 to 20),, high (scores 21 to 28), very high (scores higher than 28). In Table 9.2 the percentagess within each category are given at pretest and at posttest time for the threee groups. The most important shift, the shift from categories high / very high too lower categories was strongest among the program participants: from 42.1% att the pretest to 18.7% at the posttest. In the self-initiative group this shift was fromfrom 43.2% to 31.4%, while in the no initiative group this shift was from 51.4% too 46.7%. Among the program participants, the category very high was empty at thee posttest, while in the self-initiative group half the number of subjects, and in thee no initiative group two-thirds remained in this category.

INTERVENTIONN STUDY 155 5
Tablee 9.2 Emotional exhaustion (EE): Frequencies in MBI-NL manual norm score categories (inn percentages)
EE E
Veryy low Low w Moderate e High h Veryy high
Program Program participants participants
Pretest t N=19 9
0.0 0 0.0 0
57.9 9 31.6 6 10.5 5
Posttest t N=16 6
0.0 0 6.3 3
75.0 0 18.7 7 0.0 0
Self-Self-initiative initiative
group group Pretest t N=37 7
0.0 0 0.0 0
56.8 8 27.0 0 16.2 2
Posttest t N=35 5
0.0 0 14.3 3 54.3 3 22.8 8 8.6 6
NoNo initiative group group
Pretest t N=35 5
0.0 0 0.0 0
48.6 6 20.0 0 31.4 4
Posttest t N=30 0
0.0 0 6.7 7
46.6 6 26.7 7 20.0 0
DepersonalizationDepersonalization (D): All groups had lower posttest mean scores on D in an absolutee sense. However, only among the program participants the difference betweenn pre-and posttest scores reached statistical significance (Table 9.3).
Tablee 9.3 Depersonalisation (D): Mean scores, standard deviations, product moment coefficientt correlations, and Student's t tests
D D
Pretestt -Meann (SD)
Posttestt -Meann (SD)
Pmcc c
Student'ss t test (pairedd samples)
Effectt size
ProgramProgram participants (N=(N= 16)
10.633 (3.88)
8.50(3.06) )
rr = 0.04, n.s. .
ff (15)= 1.76, pp = 0.05 (one-tailed)
dd = 0.62
Self-initiative Self-initiative groupgroup (N = 35)
10.033 (2.90)
9.033 (5.18)
rr = 0.37, pp = 0.03
M 3 5 ) == 1.22, n.s.. (one-tailed)
dd = 0.29
NoNo initiative group (N(N = 31)
11.00(4 .02) )
10.066 (5.02)
rr = 0 . 6 1 , pp = 0.001
ff (30)= 1.27, n.s.. (two-tailed)
dd = 0.32
Amongg the program participants, the low pretest -posttest correlation indicated ann irregular pattern; some subjects increased in score, while other's scores diminished.. Further inspection showed that four subjects had higher scores at the posttest,, while also a large variation in amount of change among the other programm participants was noticed. The correlation within the other two groups wass more regular; all subjects more or less moved in the same direction. Standardd deviations showed that at pretest time, the self-initiative group was

156 6 INTERVENTIONN STUDY
mostt homogeneous, while at posttest time this group was most heterogeneous. Thee effect size Cohen's d shows that among the program participants well over onee third of the area covered by both measures did not show overlap, meaning a mediumm effect. Among both the self-initiative group, and the no initiative group thiss area was about 20%, meaning a small effect.
Again,, a comparison was made with norm scores as described in the MBI-NL manual-- For D, the following categories are valid: very low (scores equal to 0), loww (scores 1 to 3), moderate (scores 4 to 10), high (scores 11 to 14), very high (scoress higher than 14). In Table 9.4 the percentages within each category are givenn at pretest and at posttest time for the three groups. The most important shift,, the shift from categories high / very high to lower categories was strongest amongg both the program participants and the self-initiative group: from 47.3% at thee pretest to 18.7% at the posttest among the program participants, and from 43.2%% at the pretest to 13.9% at the posttest in the self-initiative group. In the no initiativee group there was no shift, or more accurately, a minor increase: from 45.7%% to 46.7%. Among the program participants, the category very high was reducedd up to about one-third of the subjects at the posttest, while in the self-initiativee group this category remained stable, and in the no initiative group two-thirdss remained in this category.
Tablee 9.4 Depersonalisation (D): Frequencies in MBI-NL manual norm score categories (inn percentages)
D D
Veryy low Low w Moderate e High h Veryy high
Program Program participants participants
Pretest t NN = 19
0.0 0 0.0 0
52.6 6 21.1 1 26.3 3
Posttest t NN = 16
0.0 0 6.3 3
75.0 0 12.5 5 6.2 2
Self-Self-initiative initiative
group group Pretest t NN = 37
0.0 0 0.0 0 56.8 8 32.4 4 10.8 8
Posttest t NN = 36
0.0 0 8.3 3
77.8 8 2.8 8 11.1 1
No No initiative initiative
group group Pretest t NN = 35
0.0 0 0.0 0
54.3 3 25.7 7 20.0 0
Posttest t NN = 30
0.0 0 6.7 7
46.6 6 33.4 4 13.3 3
PersonalPersonal Accomplishment (PA): In comparison with the pretest, on the posttest alll groups had higher mean scores on PA in an absolute sense. (Contrary to EE andd D, on PA a higher score is more favourable). Both among the program participantss and in the self-initiative group this difference reached statistical significance,, whereas in the no initiative group it did not (Table 9.5). Correlationss indicated a more or less regular change in the same direction within alll groups. Standard deviations indicated that the program participants were mostt homogeneous at the pretest, and even more so at the posttest. The effect sizee Cohen's d shows that both among the program participants and the self-

INTERVENTIONN STUDY 157 7
initiativee group about 60% of the area covered by both measures did not show overlap,, indicating a large effect. Among the no initiative group this area was closee to 20%, indicating a small effect.
Tablee 9.5 Personal Accomplishment (PA): Mean scores, standard deviations, product momentt coefficient correlations, and Student's t tests
PA A
Pretestt -Meann (SD)
Posttestt -Meann (SD)
Pmcc c
Student'ss t test (pairedd samples)
Effectt size
ProgramProgram participants (N=(N= 16)
26.311 (3.77)
29.388 (3.81)
rr = 0.52, pp < 0.05
ff (15)= -3.30, pp = 0.003 (one-tailed)
dd = 1.17
Seif-initiativeSeif-initiative group (N=35) (N=35)
25.344 (4.32)
28.777 (3.91)
rr = 0.53, pp = 0.001
ff (35)= -5.04, pp < 0.001 (one-tailed)
dd = 1.20
NoNo initiative groupgroup (N = 31)
24.711 (4.46)
25.711 (6.30)
rr = 0.63, pp < 0.001
ff (30)= -1.13, n.s.. (two-tailed)
dd = 0.29
AA comparison was made with norm scores as described in the MBI-NL manual. Forr PA, the following categories are valid: very low (scores equal to or less than 18),, low (scores 19 to 24), moderate (scores 25 to 30), high (scores 31 to 35), veryy high (scores higher than 35). In Table 9.6 the percentages within each categoryy are given at pretest and at posttest time for the three groups. The most importantt shift, the shift from categories low / very low to higher categories was strongestt among both the program participants and the self-initiative group: fromfrom 31.6% at the pretest to 18.8% at the posttest among the program participants,, and from 32.4% at the pretest to 17.1% at the posttest in the self-initiativee group. In the no initiative group there was only a small diminishment fromfrom this category: from 45.7% to 40.0%. Among the program participants, the categoryy very low was empty both at pretest and at posttest time, while in the self-initiativee group the 10% at pretest time had disappeared at posttest time. Remarkably,, in the no initiative group the percentage in the very low category wass about four times higher at posttest time compared to the pretest.

158 8 INTERVENTIONN STUDY
Tablee 9.6 Personal Accomplishment (PA)*: Frequencies in MBI-NL manual norm score categoriess (in percentages)
PA A
Veryy low Low w Moderate e High h Veryy high
Program Program participants participants
Pretest t N=19 9
0.0 0 31.6 6 52.6 6 15.8 8 0.0 0
Posttest t N=16 6
0.0 0 18.8 8 43.7 7 37.5 5 0.0 0
Self-Self-initiative initiative group group Pretest t N=37 7
10.8 8 21.6 6 62.2 2 5.4 4 0.0 0
Posttest t N=35 5
0.0 0 17.1 1 54.3 3 28.6 6 0.0 0
NoNo initiative group group
Pretest t N=35 5
5.7 7 40.0 0 45.7 7 8.6 6 0.0 0
Posttest t N=30 0
20.0 0 20.0 0 36.7 7 20.0 0 3.3 3
** Contrary to EE and D, on PA a higher category is more favourable
Ass an additional way of analysing, apart from the level of scores, or the magnitudee of change, the direction of individual changes was taken as an indicationn of differences between the three groups (Table 9.7).
Tablee 9.7 Frequencies of decrease, increase and equal levels on MBI-NL, pretestt - posttest comparison
EE: : Decrease e Increase e Equal l D: : Decrease e Increase e Equal l PA: : Decrease e Increase e Equal l
Program Program participants participants
8 1 % % 19% % 0 % %
6 9 % % 2 5 % % 6 % %
1 3 % % 8 1 % % 6 % %
Self-initiative Self-initiative groupgroup (*)
5 9 % % 3 5 % % 3% %
5 3 % % 2 9 % % 18% %
18% % 7 9 % % 3% %
NoNo initiative groupgroup (*)
52% % 4 2 % % 0% %
6 1 % % 32% % 6% %
35% % 4 8 % % 16% %
N.B.:: Decrease on EE and D, and increase on PA is indicative for a diminishing burnout level (*)) On EE, one, respectively two, cases were missing in the self- and no initiative group
Thee program participants showed highest percentages in the desired direction on alll three scales (which is: decrease on EE and D, and increase on PA). On the EEE scale, four out of five of the program participants changed in the desired direction,, while this was about one out of two in the no initiative group. The self-initiativee group was somewhere in between. On the D scale, the differences betweenn the three groups were smallest, with two-thirds of the program participantss improving, and half of the self-initiative group. This time, the no

INTERVENTIONN STUDY 159 9
initiativee group was somewhere in between. On the PA scale, four out of five of bothh the program participants and the dentists in the self-initiative group changedd in the desired direction, while this was one out of two for the dentists in thee no initiative group.
9.44 Conclusion and discussion
Thee hypothesis that participation in a prevention program would diminish burnoutt among dentists was confirmed: mean levels of emotional exhaustion andd depersonalisation were lower, while mean levels of personal accomplishmentt were higher after following the program. For those who were invitedd for the program but did not participate, changes were more diverse. Dentistss who somehow initiated preventive measures themselves showed a decreasee in burnout with regard to emotional exhaustion and personal accomplishment.. Dentists who did not initiate prevention of some kind did not changee in burnout level in a statistical sense. On all burnout scales, the effect sizee of change was largest among the program participants. Also, the percentage off dentists remaining in risk categories of burnout scales is about nil only among programm participants. Finally, the direction of positive change is most frequent amongg program participants. Therefore, the effects for those who have chosen to participatee in the prevention program, have been more beneficial than for those whoo decided not to participate.
Theree are several comments to be made at this place. In a sense, it is remarkablee that, despite small group size, effects were visible among the programm participants. Given the time span between intake and final group session,, five or six months, the main purpose of the program was to increase awarenesss of one's own talents or capacities and how they were, or were not met inn the current professional situation. The transition from awareness to actual implementationn of changes is not likely to have progressed much at that stage. Nevertheless,, burnout levels did diminish at this point in time already. Repeated measurementt after a more prolonged period wil l have to give more insight in the robustnesss of the changes. Furthermore, it must not be forgotten that the programm was not explicitly constructed as a "beating burnout" - project as such, ass the program contents in Box 9.1 show, but seemed to aim at demotivation and balancingg one's career and personal wishes in a broader sense.
Withh regard to the depersonalisation dimension, among the program participantss there is no correlation between pre- and posttest scores. Strangely enough,, although both the mean score level of all participants, and the percentagee in the category "very high" has decreased, some participants appear too have increased considerably in D-score after the program. Apparently, the programm gives room for contradictory effects, although it must be noted that percentagess of increase in D-score were even slightly higher in the other two groups.. Some dentists indicated to feel that they should be more assertive, better

160 0 INTERVENTIONN STUDY
safeguardd their own boundaries, and keep more distance from the patient emotionallyy as a means to reduce their own emotional exhaustion. This is in line withh how prominent burnout theorists regard the process sequence of burnout, in whichh depersonalisation is seen as self-protection in order to prevent from becomingg emotionally exhausted.3 Other dentists wish to allow themselves to createe more possibilities for personal contact with patients, because they feel it wil ll bring more job satisfaction. In fact, these two themes are part of the programm and may give a possible explanation for the opposite movement in depersonalisationn scores. Possibly, keeping more distance and being distant are sometimess quite close. It is an interesting theoretical point to what extent learningg to be more assertive and a tendency towards depersonalisation can be distinguished,, and whether the MBI-NL is capable to differentiate between these twoo developments in a construct validity sense. Apart from the validity question, givenn these diverging reactions, the program needs to emphasise the individual needss more closely and subsequently has to be geared to these individual differences. .
Thee present study's design is quasi-experimental since the subjects were nott randomly allocated to conditions. Although all were invited on the same groundss - unfavourable MBI-NL pretest scores - it must be assumed that self selectionn took place among those who did participate in the program and those whoo did not. A further exploration of features of the dentists that participated mayy give interesting information about for whom a program as such appears to bee a valuable solution. From the standard deviations on the MBI-NL scales it cann be concluded that the program participants were more homogeneous on the burnoutt dimensions than the two comparison groups.
Whatt strikes most when inspecting the data, is that mean scores of all groupss shift in the preferred direction on the three burnout scales. Although neverr reaching statistical significance, even the group with no initiative for preventionn shows this shift. One explanation for this shift among all groups is thee fact that all have received personal feedback on their pretest scores. The dentistss with self-initiative for prevention clearly took notice of this feedback, as thee program participants did. Although the no initiative group indicated to not havee taken special preventive measures, the possibility cannot be excluded that too some extent the message did have effect. The effect of feedback on a regular basiss as a preventive measure on its own is well-worth further investigating. Besides,, a positive change, regardless of statistical significance, in control groupss of other burnout prevention program studies is described more often.16
Onee other important aspect to be mentioned with regard to the positive shift in alll groups, is the possibility of regression towards the mean. In case of extreme pretestt scores, as in the present study, it is to be expected that on a repeated measuree with the same instrument scores wil l shift towards the population mean.177 This explanation cannot be excluded.

INTERVENTIONN STUDY 161 1
Fromm several comments expressed, it appeared that some dentists from the noo initiative group were in disagreement with the unfavourable pretest score and feedbackk given, and subsequently had very favourable posttest scores. This couldd be an example of "demand characteristics": a bias in posttest scores as a resultt of knowledge about the actual research purposes.18 One way or the other, thee fact that certain dentists indicated to have not taken initiatives for preventive action,, must lead to a reflection on how these dentists might be reached. Lookingg at their MBI-NL scores, there certainly is a risk for burnout among thesee dentists. A further inspection of what characterises this group may give moree information on what is needed to also offer these dentists well-tailored preventivee tools. A suggestion could be to lower the threshold for participation. Inn its present form, the program emphasises personal changes and includes groupp meetings with other dentists. These are two aspects that may be regarded ass too intrusive by dentists. From further comments it could be learned that the reasonss most often mentioned to decide not to participate were, apart from havingg taken self-initiative with regard to burnout prevention: too much time consuming,, reluctance to group sessions, contents of program, financial costs tooo high, and too large geographical distance from agency. By also offering a programm that starts with an emphasis on the dental practice, and by starting with ann individual path, those who are reluctant to participate in its present form may veryy well be reached. An intake counsellor at the agency could play an importantt role in matching one of the programs available to the individual's needs. .
Notwithstandingg the fact that most of the invited did not participate, the presentt mailing resulted in a considerably higher percentage of dentists subscribingg for the program, when compared with response percentages on previouss regular programs. In previous mailings, dentists were selected because theyy fell in a certain age group. In the present study, all were addressed because off an unfavourable personal burnout score, which, apparently, was a more valid argumentt than mere age. Therefore, one more conclusion to be drawn from this studyy is that personal feedback does have an extra value for the individual dentistt with regard to prevention.
Apartt from personal feedback, recognition is a valuable moment in the processs of preventive action. A possible instrument to intervene preventively is too offer profiles of dentists with burnout related complaints. It is the authors' experiencee that by publishing case histories in dental journals, unusually high numberss of reactions from dentists reached their office.19 Recognition of the describedd dentist appeared to be the onset to reflect upon one's professional lif e forr many dentists. There is a challenge in research to further explore typical profiless of dentists with burnout risk as a tool in preventive strategies.
Finally,, prevention cannot be regarded as a cure to be taken once. Those whoo did participate expressed the need to keep in touch from time to time with colleaguess from the program and their counsellors. The possibility of expressing

162 2 INTERVENTIONN STUDY
one'ss experiences and receiving feedback had become too valuable to miss. In thee introduction of this paper, burnout was metaphorically described as an empty carr battery. A battery has to be recharged regularly in order to function, and so doess a dentist. Speaking in the same figurative language, a regular check-up is essentiall for reliable functioning of a car. In the same way, a regular self-check instrumentt could be a valuable tool in burnout prevention. From the present study,, it is likely to conclude that personal feedback resulted in higher percentagess of preventive action than general information did. If this appears to bee true, another valuable entrance for prevention is discovered. Furthermore, in Thee Netherlands and, as far as the authors could identify, in other countries as well,, career planning and attention for personal expectancies in professional life iss not part of any dental curriculum. Real prevention should start before first symptomss show. Therefore, dental schools, dental organisations, and the individuall dentist have to be aware of a large vacuum in current supply of "continuouss education".

INTERVENTIONN STUDY 163 3
References s
1.. Schaufeli WB, Enzmann D. The burnout companion to study and practice: A critical analysis.. London, UK: Taylor & Francis, 1998.
2.. Schaufeli WB, Buunk BP. Professional burnout. In: MJ Schabracq, JAM Winnubst, CL Cooperr (Eds.). Handbook of work and health psychology (pp. 311-346). Chicester, UK: Johnn Wiley & Sons Ltd., 1996.
3.. Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual, 3rd edition. Paloo Alto, CA: Consulting Psychologists Press, Inc., 1996.
4.. Schaufeli WB, Maslach C, Marek T (Eds.). Professional burnout: Recent developments inn theory and research. London, UK: Taylor & Francis, 1993.
5.. Osborne D, Croucher R. Levels of burnout in general dental practitioners in the south-eastt of England. Brit Dent J 1994; 177: 372-7.
6.. Humphris G. A review of burnout in dentists. Dent Update 1998; 25: 392-96. 7.. van Dierendonck D. Balancing give and take: An equity approach to burnout. Thesis.
Utrecht,, The Netherlands: Utrecht University, 1997. 8.. Pastor C. Opbranden of uit de brand helpen. Doctoral thesis. Amsterdam, The
Netherlands:: Department of Psychological Methods, University of Amsterdam, 1998. 9.. Maslach C, Goldberg J. Prevention of burnout: New perspectives. Appl Prevent Psychol
1998;; 7: 63-74. 10.. Berkel E. Movir wil begeleidingsprogramma ter preventie van "burnout". NT 1994; 49:
592-5. . 11.. Berkel E. Movir schaft herkeuring af. Ned Tandartsenblad 1995; 50: 736-9. 12.. Kreyns JM. Instrument in handen van jezelf. TP 1996; 17 (3): 22-3. 13.. Vos J. Burnout-preventie krijgt structuur: In Zeist worden tandartsen weer "als nieuw".
NTT 1997; 52: 500-5. 14.. Schaufeli WB, van Dierendonck. Maslach Burnout Inventory, Dutch version (MBI-NL) .
Preliminaryy manual. Utrecht, The Netherlands: Research School Psychology & Health, Utrechtt University, 1995.
15.. Judd CM, Smith ER, Kidder LH. Research methods in social relations. Fort Worth, TX: Holt,, Rinehart & Winston, Inc., 1991.
16.. van Dierendonck D, Koot T, Garssen B, Visser A, Ketelaar M. De uitdaging tot innerlijkk meesterschap. Evaluatie van een burnout preventieprogramma voor ondernemingen.. Rotterdam, The Netherlands: Helen Dowling Instituut, 1999.
17.. van den Brink WP, Koele P. Statistiek - Deel 1. Meppel, The Netherlands: Boom, 1985. 18.. Hoogstraten J. De machteloze onderzoeker. Meppel, The Netherlands: Boom, 1979. 19.. Gorter RC. Tandarts en burnout: Begeleiding bij mentale belasting in ergonomisch
perspectief.. TP 1997; 18 (1): 17-23. 20.. Brunette DM. Critical thinking: Understanding and evaluating dental research. Chicago,
IL:: Quintessence Publishing Co, Ine, 1996.