Embed Size (px)
Citation preview

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Early neurological delopment, growth and nutrition in very preterm infants
Maas, Y.G.H.
Link to publication
Citation for published version (APA):Maas, Y. G. H. (1999). Early neurological delopment, growth and nutrition in very preterm infants.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: https://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 18 Aug 2019

CHAPTER 6
Qualitative assessment of general movements in very preterm infants: relation to neonatal cranial ultrasound and neurological outcomes
Yolanda G.H. Maas, Majid Mirmiran, Augustinus A.M. Hart, Janna G. Koppe and Henk Spekreijse
6.1 Abstract
6.2 Introduction
6.3 Subjects and methods
6.3.1 Subjects
6.3.2 Overall cerebral ultrasound
6.3.3 Neurological examination at term
6.3.4 Spontaneous general movements
6.3.5 Statistical analysis
6.4 Results
6.5 Discussion
6.6 References
Submitted

106 Chapter 6

107
Qualitative assessment of general movements in very preterm infants: relation to neonatal cranial ultrasound and neurological outcome Yolanda G.H. Maas1, Majid Mirmiran3, Augustinus A.M. Hart2, Janna G. Koppe' and Henk Spekreijse4
'Department of Neonatology and
department of Clinical Epidemiology and Biostatistics Academical Medical Center, University of Amsterdam, Emma Childrens' Hospital Netherlands Institute for Brain Research "The Netherlands Ophthalmic Research Institute and Laboratory of Medical Physics
6.1 Abstract
Background An early diagnostic tool highly predictive of preterm babies at risk of long-
term neurological disorders is still needed in neonatology. We wanted to test the
applicability of a new method to detect early brain damage in newborn infants, based on the
observation of quality of spontaneous movements.
Methods We have examined longitudinally the quality of general movements (GMs) in a
group of 96 preterm infants born at < 30 weeks gestational age. These infants were
enrolled in a randomized trial studying early diet and thyroxine supplementation
Results Repeated measures of GM quality were stable over time and did not show
significant changes till corrected term age. No effects were found of early diet and/or
thyroxine supplementation. No significant differences in GM quality were found in infants
scored normal and abnormal based on repeated cranial ultrasound made before term age or
on neurological examination at term age.
Conclusions We conclude that the quality of GM is an easy and reliable measurement to be
carried out even in the neonatal intensive care unit in very preterm infants. Since it is stable
over time in the preterm period (from 30 to 40 weeks postconceptional age) one
observation would be sufficient for evaluation before term age. Diet and thyroxine
intervention effects were not found assessing preterm GM quality.
When applied before term age the agreement of this method with the results of preterm

108 Chapter 6
cranial ultrasound or conventional neurological outcome at corrected term age is very poor.
6.2 Introduction
In the United States alone approximately 50,000 infants are born yearly with a birth weight
< 1500g. Because of major advances in neonatal intensive care, 85% of these infants
survive (1,2). However 5-15% may develop major neurological abnormalities and an
additional 25-50% may exhibit minor neurodevelopmental disabilities (3). An early
diagnostic tool to identify babies at risk is needed. Prechtl and collaborators developed a
new and noninvasive assessment technique for the early detection of brain injury (4-8). This
new method is based on the observation of spontaneous motility assessing the quality of
general movement (GM) in preterm and term infants (4,9-14). This technique applied till 3-
4 months post term appears to have good predictive value for neurological dysfunction and
is superior to conventional neurological examination and cranial ultrasound (7,15-22). We
were interested to study the applicability of this test in our neonatal intensive care unit
(NICU) as an early diagnostic tool to detect neurological abnormalities in a group of 96
infants born before 30 weeks gestation. Each infant was examined longitudinally from 30
weeks postmenstrual age (PMA) till corrected term age. The reliability of this new method
was tested and its agreement with the results of repeated cranial ultrasound during the same
period and with those of conventional neonatal neurological examination at corrected term
age were validated. The infants were also enrolled in a randomized, double-blind, placebo
controlled trial on the early effects of diet and thyroxine supplementation on neurological
development.
6.3 Subjects and methods
6.3.1 Subjects
This study is based on 160 infants born in 1991 and 1992, who participated in a
randomized, double-blind, placebo controlled trial of early diet and T4 administration (23).
The study protocol was approved by the Medical Ethical Committee of the Academical
Medical Center, Amsterdam. All infants born at a gestational age of less than 30 weeks and
admitted to the Intensive Care Unit of the Academical Medical Center, were entered into

General body movements in preterm infants 109
this trial if after full explanation informed consent from at least one parent was obtained
within 24 hours after birth. Babies were excluded if they had a major congenital
abnormality known to influence growth or neurological development or when the mother
had an endocrinological disease or was an illicit drug user. Of the 160 infants enrolled 11
infants died within 72 hours after birth leaving us with 149 infants to study (24). These
infants were stratified (before diet randomization) according to mother's choice to
breastfeed her infant(s). Of the 149 infants, 120 entered into the "maternal milk (MM)
group" and 29 into the "only formula feeding (FF) group". The small number of mothers
that chose not to express breast milk for their infant(s) resulted in too small a number of
infants in the "only" formula feeding group" for reliable statistics. Therefore we further
analysed only the data of the maternal milk group. From these 120 infants 24 were never
observed; 11 because they died within 3 weeks after birth; 4 (of which 3 died) because of
the severity of their illness in the first 7 postnatal weeks, 1 because she was transferred to
another hospital 6 days postpartum, 2 (twins) because the parents withdrew their informed
consent and 6 because of absence of the researchers. This resulted in a total of 96 infants,
48 in the thyroxine and 48 in the placebo group. Fifty four infants were given standard
formula and 42 preterm formula, resulting in four groups (26 in the thyroxine/STF, 22 in
the thyroxine/PTF, 28 in the placebo/STF, 20 in the placebo/PTF group). Extensive data
were collected on obstetric, fetal and neonatal variables.
Infants started enteral feeding between 24 hours and several days after birth, depending on
their clinical condition. Enteral feeding was increased thereafter till a full enteral intake of
125 ± 15 kcal/kg/day had been achieved. Each infant was randomly assigned to STF or
PTF. Diet and macronutrient composition of the standard and preterm formula used and of
our weekly collected maternal milk samples are described in detail and discussed in Maas et
al. submitted and Maas, et al, BJN (24,25).
For each infant entering the study a numbered 'blind' set of ampoules, containing 25 /xg/ml
T4 or placebo, was prepared. Thyroxine supplementation once a day was started 12-24
hours after birth, in a dose of 8 ng per kilogram birth weight. This dose was chosen on the
basis of results of a pilot study (26) and given via an intravenous injection as long as
intravenous nutrition was given (mean period of 14 days) or enterally thereafter. The
treatment lasted 6 weeks.

110 Chapter 6
Gestational age was determined by the first day of the last menstrual period of the mother.
This was confirmed either by an ultrasound examination during early pregnancy or a
maturational assessment of the preterm infant with the help of the Dubowitz score (27).
Data concerning patient characteristics and clinical outcome within 24 hour after birth are
shown in table 6.1. Neonatal clinical data were collected until discharge (table 6.2).
Table 6.1 Clinical characteristics of the infants within 24h after birth
Thyroxine Placebo STF PTF STF PTF
(n= 26) (n=22) (n=28) (n=20
gestation (days), mean ± SD 194 ± 9 198 ± 8 196 + 9 195 + 9
birth weight (g), mean + SD 1108 ± 247 1038 ± 213 1044 ± 189 1077 ± 274
sex, male/female 11/15 15/7 11/17 8/12
Multiplets n 6 13 14 8
Birth weight < 10th centile n 1 4 3 2
antenatal glucocorticoids n 18 17 15 17
Caesarian section n 2 6 6 2
APGAR score at 5', mean + 8.5 ± 1.5 8.0 ± 1.7 8.0 ± 1.7 8.6 ± 2.2
SD
intubation at birth n 5 9 13 4
respiratory distress syndrome n 12 13 13 12
surfactant rescue therapy n 8 9 7 6
intrauterine infection n 2 2 1 2
cerebral haemorrhage (day 1) n 7 4 6 3

General body movements in preterm infants 111
Table 6.2 Clinical data until discharge
Thyroxine Placebo
STF PTF STF PTF
(n = 26) (n = 22) (n = 28) (n = 20)
Deaths n 0 1 1 0
Oxygen suppl. at 36 w n 4 3 3 6
Patent Ductus Arteriosus n 8 1 10 7
Necrotising Enterocolitis n 1 0 1 0
Septicaemia n 7 4 8 5
Days of intubation, mean ± SD 4 ± 4 5 ± 5 5 ± 7 6 ± 7
Days of 02 therapy, mean ± 27 ± 28 30 ± 33 32 ± 46 33 ± 33
SD
PMA at discharge home (days), 269 ± 16 279 ± 21 275 ± 17 276 ± 20
mean + SD
Cerebral ultrasound findings
Normal n (%) 12(46%) 9(41%) 13 (46%) 8 (40%)
Moderately abnormal n (%) 11 (42%) 9(41%) 15 (54%) 7(35%)
Severely abnormal n (%) 3 (12%) 4(18%) 0(0%) 5(25%)
Patent ductus arteriosus was diagnosed when clinical symptoms were confirmed by a
cardiac ultrasound. Necrotizing enterocolitis was diagnosed by pneumatosis on an
abdominal radiograph and/or by findings during surgery. Cranial ultrasounds were carried
out, using a 7.5 MHz transducer, within 24 h after birth and on days 5, 14, 28 and 42 or
more often if clinically indicated. Classification of haemorrhage was done as described by
Volpe (28). Haemorrhagic venous infarction followed by cysts were classified as
parenchymal haemorrhages. Ischaemic lesions were classified according to De Vries et al.
(29). Classification of ventriculomegaly was performed according to Levene (30).
6.3.2 Overall cerebral ultrasound
An overall cranial ultrasound classification was made judged on the basis of all repeated
ultrasound scans made of each infant in our unit. For better comparison with GM quality

112 Chapter 6
and the Prechtl neonatal neurological test, ultrasound data were also divided into three
groups, namely normal, suspect and abnormal. Classification was made as follows:
Normal: no haemorrhage and no ischaemia and no ventricular dilatation; Moderately
abnormal: a grade 1 or 2 haemorrhage and/or a grade 1 ischaemia and or a grade 1
ventricular dilatation; Severely abnormal: a grade 3 or 4 haemorrhage and/or a grade 2 or 3
ischaemia and/or a grade 2 ventricular dilatation.
6.3.3 Neurologic examination at term
At term age neurodevelopment was assessed using the method described by Prechtl (31).
This test was scored as normal, suspect or abnormal, using the classification as described
by Jurgens-van der Zee et al. (32).
6.3.4 Spontaneous General Movements
Observation and recording procedure
Two-hour video recordings were made of each infant. The recordings were started as soon
as the clinical condition of the infant was stabilized, usually at 1 - 2 weeks after birth and
continued every 2 weeks thereafter. The infants were studied until they left our neonatal
unit (discharged home or transferred to another hospital) or reached the expected date of
delivery (term age) in our unit. When infants left the hospital before 38 weeks of post-
menstrual age an additional video recording was made at term age (38 - 42 weeks' PMA).
All recordings were made in the hospital between noon and 6 p.m.. The infants were
recorded in the incubator or under a radiant warmer. All infants were undressed before the
start of each recording, wearing only a diaper, in the supine or semi-lateral position and
allowed some time to adjust. The video camera was positioned laterally, at an angle of 45°
degrees above the infant.
Assessment of the quality of general movements (GMs)
Video tapes were replayed and three representative general movements were selected from
each recording (total of about 10 minutes), excluding crying, fussing and sucking periods.
For each infant a collection of these selected GMs at different ages was then assembled and
stored on a separate tape, documenting the developmental trajectory of the GMs from birth

General body movements in preterm infants 113
to term age. The quality of the GM was assessed independently from these tapes by 2
observers (YGHM, MHA), both unaware of treatment and clinical and neurological
outcome of the infants.
The GMs were analysed according to Hadders et al. (1997) (8), a detailed method based on
the principles of Prechtl to assess the quality of GMs (4). This resulted in a classification of
normal, mildly abnormal or definitely abnormal GMs. Normal GMs consist of variable
movements of arms, legs, head and trunk. They wax and wane in intensity, speed and their
onset and offset are gradual. These movements are complex with many superimposed
rotations and with many changes in direction. This complexity and variability make the
movements fluent and elegant. Mildly abnormal GMs lack this fluency but are still
complex. Definitively abnormal GMs lack both fluency and complexity. Besides the global
assessment of GM quality, the Ferrari Optimality score was applied (5), judging 8 different
elements of movement this score distinguishes, such as movement character, sequence and
fluency. Inter-observer agreement was 100% for both scoring methods, based on the
independent assessment of GM quality of 24 recordings.
We have collected a total of 334 video recordings of 96 infants. The recordings were
divided per 2 weeks PMA and were divided over the four treatment groups (see table 6.3
and below).
Table 6.3 Number of observations made of the infants studied in the four different
treatment groups
Thyroxine Placebo
postmenstrual age ALL STF PTF STF PTF
(n=96) (n=26) (n=22) (n=28) (n = 20)
30-31 85 24 20 27 14
32-33 82 23 21 21 17
34-35 55 12 14 14 15
36-37 29 4 8 11 6
38-42 83 25 17 24 17

114 Chapter 6
6.3.5 Statistical analysis
To evaluate the effect of age, early diet and thyroxine administration on the development of
the quality of GM unbalanced repeated measurements analysis of covariance with structured
covariance matrices was performed on the optimality score of Ferrari (5) using program 5V
of the statistical package BMDP 7.0 (33). This technique allows for missing values which
are estimated implicitly from the available data. The model contained the main effects of
Thyroxine (yes/no), supplemented Formula (standard/preterm) and the within-infant grou
ping factor postmenstrual age (PMA) as well as all possible interactions between these 3
factors. In addition covariables (gestational age, gender, APGAR score at 5 minutes,
surfactant rescue therapy, antenatal glucocorticoids, cerebral haemorrhage on day 1
postpartum, weightpercentiles at birth) were included as well as their interactions with time
(postmenstrual age in weeks). To adjust for differences in PMA within each category an
additional covariable was introduced, defined by the difference between the actual PMA
and the lowest (30,32,34,36) value or the midvalue (40) of the categories. In order to
simplify the interpretation of the results we used a backward elimination of the three factors
and their interactions, taking the hierarchical structure into account. This means that no
main effect or interaction can be eliminated as long as it is included in a higher order
interaction in the model.
To test the assumptions of the model and to check on outliers, analysis of residuals was per
formed from the unbalanced repeated measurements analysis. To adjust for the missing
values in the data all figures presented here are based on the estimated values of the
regression parameters resulting from the unbalanced repeated measurements analysis of
covariance. Additional analysis to find whether there was a relation between overall
preterm cerebral ultrasound findings and the developmental course of GM quality was
performed using ANOVA. Analysis of the agreement of global GM quality assessment at
corrected term age for neonatal neurological outcome examined at the same age was done
using the Pearson X2 test for 3x3 tables (BMDP program 4F (33)).
6.4 Results
In this study first a global assessment of GM quality was done, followed by a more detailed
analysis using the Ferrari optimality score. The findings of both scoring methods were

General body movements in preterm infants 115
highly correlated (p< 0.0001; Pearson X2). On statistical grounds the optimality score can
be expected to provide the higher power. Therefore only the results of the analysis of
optimality score data are described here. Abnormal GM (n= 148) corresponded with
scoring an optimality score of 8, mildly abnormal GM (n=168) corresponded with a score
of 10-11, while normal GM (n=13) had a score of 12-16.
Table 6.4 Estimated optimality score (+ SE) of Ferrari et al. (1990), of all infants studied, and of the Thyroxine and Placebo treatment groups per postmenstrual age group
postmenstrual All Thyroxine Placebo age n (n = 96) n (n=48) n (n=48)
30-31 83 9.5 ± 0.2 44 9.5 + 0.2 39 9.4 ± 0.2
32-33 79 9.5 ± 0.2 42 9.0 ± 0.2 37 9.8 ± 0.2
34-35 55 9.4 ± 0.2 26 9.5 + 0.2 29 9.4 ± 0.2
36-37 29 9.1 ± 0.3 12 9.4 ± 0.3 17 9.0 + 0.3
38-42 83 9.3 ± 0.2 42 9.3 ± 0.2 41 9.1 ± 0.2
The optimality score did not change between 30 weeks PMA and term age (table 6.4). We
found a difference in developmental trajectory for the infants receiving Thyroxine versus
Placebo (p = 0.0089), the main difference being found at 32-33 weeks PMA. When we
removed the T4xtime interaction from the analysis, no effects were found for diet
(p=0.45), thyroxine (p = 0.73) or time (p=0.070). Of the covariables we corrected for in
our analysis, gender and weight percentiles at birth showed evidence of an effect on GM
quality. The relation of gender and weightpercentiles at birth with the development
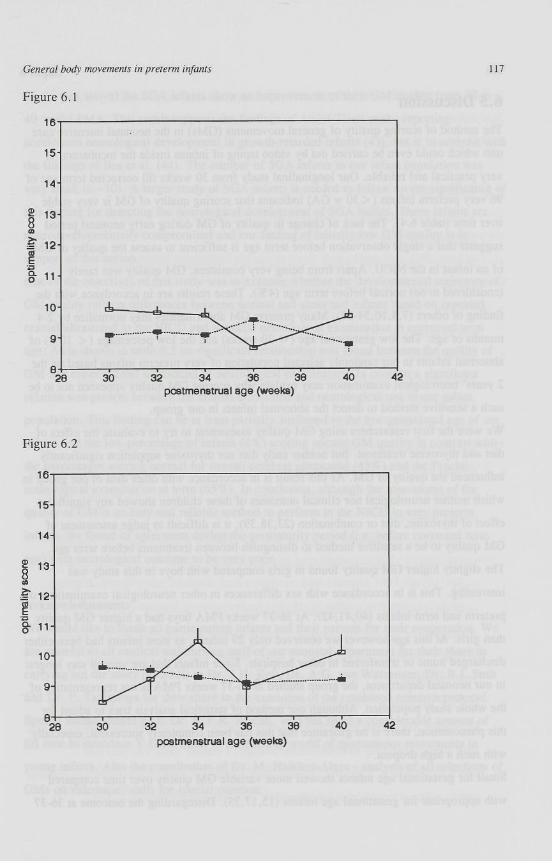
trajectory of the quality of GM are presented in figure 6.1 and 6.2. Except for 36-37 weeks
PMA, girls (n=51 (53%)) had a consistently higher optimality of GMs than boys (n=45
(47%)) (p = 0.0093). Infants who were growth retarded under the 10th weightpercentile
(SGA) (n= 10) had a different developmental trajectory from infants born with an
appropriate weight for their age (AGA) (n=86 (90%)) (p< 0.0001) with an initially poorer
GM quality but a clear improvement in time.
No relation was found between cerebral haemorrhage on postpartum day 1 and the
development of GM quality (p=0.45), nor could we find any significant relation between

116 Chapter 6
the overall cerebral ultrasound findings (based on all measurements done in our unit before
discharge) and development of GM quality (p=0.47) with low sensitivity and specificity of
50 and 51% respectively. No relation was found between global GM quality at corrected
term age and the outcome of the neonatal neurological examination (p=0.51) (table 6.5).
The low sensitivity and specificity were 60 and 52% respectively, while on the other hand
overall cranial ultrasound and neonatal neurological test were highly correlated(p = 0.0049).
Table 6.5 Results of GM quality assessment at corrected term age in 83 infants, per group of infants with a normal, suspect and abnormal overall cerebral ultrasound diagnoses, and per group of infants with a normal, suspect and abnormal outcome of the Prechtl neonatal neurological examination
Global GM quality score at corrected term age
normal suspect abnormal
normal (n=36)
(n=3) (n=39) (n = 41)
Overall normal (n=36) 1 (3%) 18 (50%) 17 (47%)
Cerebral suspect (n=37) 1 (3%) 17 (46%) 19(51%) Ultrasounds
abnormal (n=10) 1 (10%) 4 (40%) 5 (50%)
Prechtl normal (n = 54) 2 (4%) 25 (46%) 27 (50%)
score suspect (n=19) 0 (0%) 11 (58%) 8 (42%)
abnormal (n=10) 1 (10%) 3 (30%) 6(60%)
Legend to figures
Figure 6.1 Quality of General Movements (mean + SE) for girls (-Ö-) and boys (•••••) for
PMA week 30 to term age.
Figure 6.2 Quality of General Movements (mean ± SE) for infants with a birth weight <
plO (-O-) and infants with a birth weight > plO (•••••) for PMA week 30 to term age.
General body movements in preterm infants
Figure 6.1
117
28 30 32 34 36 36 postmenstrual age (weeks)
Figure 6.2
postmenstrual age (weeks)

118 Chapter 6
6.5 Discussion
The method of scoring quality of general movements (GMs) in the neonatal intensive care
unit which could even be carried out by video taping of infants inside the incubators, is
very practical and reliable. Our longitudinal study from 30 weeks till corrected term age of
96 very preterm infants ( < 30 w GA) indicates that scoring quality of GM is very stable
over time (table 6.4). The lack of change in quality of GM during early neonatal period
suggests that a single observation before term age is sufficient to assess the quality of GM
of an infant in the NICU. Apart from being very consistent, GM quality was rarely
(considered to be) normal before term age (4%). These results are in accordance with the
finding of others (7,8,10,34-37). Many preterm GM abnormalities may normalize by 2-4
months of age. The low gestational age (< 30 weeks) and the low percentage (< 10%) of
abnormal infants in our randomly selected population of very preterm infants based on the
2 years' neurological examination may explain why scoring GM quality appeared not to be
such a sensitive method to detect the abnormal infants in our group.
We were the first researchers using GM quality assessment to try to evaluate the effect of
diet and thyroxine treatment. But neither early diet nor thyroxine suppletion significantly
influenced the quality of GM. As this result is in accordance with other data of our group in
which neither neurological nor clinical outcomes of these children showed any significant
effect of thyroxine, diet or combination (23,38,39), it is difficult to judge assessment of
GM quality to be a sensitive method to distinguish between treatments before term age.
The slightly higher GM quality found in girls compared with boys in this study was
interesting. This is in accordance with sex differences in other neurological examinations of
preterm and term infants (40,41,42). At 36-37 weeks PMA boys had a higher GM quality
than girls. At this age however we observed only 29 infants, as most infants had been either
discharged home or transferred to other hospitals. Since infants that are very ill stay longest
in our neonatal department, the group studied at 36-37 weeks PMA is not representative of
the whole study population. Although our method of statistical analysis tries to adjust for
this phenomenon, there is no guarantee that this has been completely successful, especially
with such a high dropout.
Small for gestational age infants showed more variable GM quality over time compared
with appropriate for gestational age infants (15,17,35). Disregarding the outcome at 36-37

General body movements in preterm infants 119
weeks (see above) the SGA infants show an improvement of their GM quality from 30 to
40 weeks PMA. This result supports the findings of Amiel-Tison et al., reporting
accelerated neurological development in growth-retarded infants (43), but is in contrast with
the findings of Bos et al. (44). The number of SGA infants in our infant population was
very small (n= 10). A larger study of SGA infants is needed to follow on the significance of
this finding for detecting the neurological development of SGA babies. These infants are
neurodevelopmentally compromised and our finding of initially low GM quality is in
support of this notion.
One of the objectives of this study was to examine whether the developmental trajectory of
GM quality reflects differences between normal and abnormal infants based on repeated
cranial ultrasound in the NICU and neonatal neurological examination at corrected term
age. As is shown in table 6.5 no significant relationship was found between the quality of
GM and either cranial ultrasound or neurological examination. In contrast a significant
relation was present between the cranial ultrasound and neurological test in our infant
population. This finding can be at least partially attributed to the low gestational age of our
infants and the low percentage of infants (4%) scoring normal GM quality in contrast with
the percentages scoring normal for overall cerebral ultrasound (43%) and the Prechtl
neurological examination at term (65%). In conclusion, although the assessment of the
quality of GM is an easy and reliable method to perform in the NICU in very preterm
infants, we found its agreement during the prematurity period (i.e. before corrected term
age) with neurological outcome to be very poor.
Acknowledgements
We would like to thank all participating infants and their parents for their cooperation. We
are grateful to all medical and nursing staff of our neonatal department for their share in
carrying out the study protocol; to Dr. J.H. Kok, Dr. A.G. van Wassenaer, Dr. B.J. Smit
and Dr. P. Tamminga for their share in the execution of the combined research protocol.
Special thanks should go to Dr. H.F.R. Prechtl, who has spent a considerable amount of
his time to introduce Y.G.H. Maas to the exciting world of spontaneous movements in
young infants. Also the contribution of Dr. M. Hadders-Algra - analysis of all selections of
GMs on videotape - calls for special mention.
120 Chapter 6
Y.G.H. Maas was financially supported by Nutricia, The Netherlands.
This report is part of a study in fulfilment of the Degree in Philosophy in Science for
Y.G.H. Maas.
6.6 References
1. Volpe JJ (ed.) Neurology of the Newborn, 3rd edition, W.B. Saunders Company,
Philadelphia, 1995
2. Hack M, Friedman H, Avery A, Fanaross MB. Outcomes of extremely low birth
weight infants. Pediatrics 1996;98:931-937
3. Volpe JJ. Brain injuries in preterm infants - from pathogenesis to prevention. Brain
and development 1997;19:519-534
4. Prechtl, HFR. Qualitative changes of spontaneous movements in fetus and preterm
infant are a marker of neurological dysfunction (Editorial). Early Hum Dev
1990;23:151-158.
5. Ferrari F, Cioni G, Prechtl HFR. Qualitative changes of general movements in
preterm infants with brain lesions. Early Hum Dev 1990;23:193-231.
6. Hadders-Algra, M. The assessment of general movements is a valuable technique for
the detection of brain dysfunction in young infants. A review. Acta Paediatr Suppl
1996;416:39-43.
7. Prechtl HFR, Einspieler C, Cioni G, Bos AF, Ferrari F, Sontheimer D. An early
marker for neurological deficits after perinatal brain lesions. Lancet 1997;349:1361-
1363.
8. Hadders-Algra, M, Klip-Van den Nieuwendijk AWJ, Martijn A, Van Eykern LA.
Assessment of general movements: towards a better understanding of a sensitive
method to evaluate brain function in young infants. Dev Med Child Neurol
1997;39:89-99.
9. Bos AF, Martijn A, Van Asperen RM, Hadders-Algra M, Okken A, Prechtl HFR.
Qualitative assessment of general movements in high-risk preterm infants with chronic
lung disease requiring dexamethasone therapy. J Pediatr 1998;132:300-306.
10. Bos AF, Martijn A, Okken A, Prechtl HFR. Quality of general movements in preterm
infants with periventricular echodensities. Acta Paediatr 1998;87:328-335.

General body movements in preterm infants 121
11. Prechtl HFR, Nolte R. Motor behaviour of preterm infants. In: Prechtl HFR, editor.
Continuity of neural functions from prenatal to postnatal life, Clinics in
Developmental Medicine No 94. Blackwell Scientific Publications Ltd. Oxford, UK,
1984:79-92.
12. Cioni G, Prechtl HFR. Preterm and early postterm motor behaviour in low-risk
premature infants. Early Hum Dev 1990;23:159-191.
13. Hadders-Algra M, Prechtl HFR. Developmental course of general movements in early
infancy. I. Descriptive analysis of change in form. Early Hum Dev 1992;28:201-213.
14. Einspieler C, Prechtl HFR, Ferrari F, Cioni G, Bos AF. The qualitative assessment of
general movements in preterm, term and young infants - review of the methodology.
Early Hum Dev 1997;50:47-60.
15. Bekedam DJ, Visser GHA, Vries JIP de, Prechtl HFR. Motor behaviour in the
growth retarded fetus. Early Hum Dev 1985;12:155-165.
16. Geerdink JJ, Hopkins B. Qualitative changes in general movements and their
prognostic values in preterm infants. Eur J Paediatr 1993;152:362-367.
17. Sival DA, Visser GHA, Prechtl HFR. The effect of intrauterine growth retardation on
the quality of general movements in the human fetus. Early Hum Dev 1992;28:119-
132.
18. Prechtl HFR, Ferrari F, Cioni G. Predictive value of general movements in
asphyxiated fullterm infants. Early Hum Dev 1993;35:91-120.
19. Albers S, Jorch G. Prognostic significance of spontaneous motility in very immature
preterm infants under intensive care treatment. Biol Neonate 1994;66:182-187.
20. Einspieler C. Abnormal spontaneous movements in infants with repeated sleep
apnoeas. Early Hum Dev 1994;36:31-48.
21. Einspieler C, Prechtl HFR, van Eykern L, de Roos B. Observation of movements
during sleep in ALTE and apnoeic infants. Early Hum Dev 1994;40:39-50.
22. Droit S, Boldrini A, Cioni G. Rhythmical leg movements in low-risk and brain
damaged preterm infants. Early Hum Dev 1996;44:201-213.
23. Van Wassenaer AG, Kok JH, de Vijlder JJM, et al. Effects of thyroxine
supplementation on neurologic development in infants born at less than 30 weeks'
gestation. N Engl J Med 1997;336:21-26.

122 Chapter 6
24. Maas YGH, Gerritsen J, Hart AAM, Mirmiran M, Koppe JG, Spekreijse H. Physical
development in very preterm infants: influence of early diet and thyroxine
supplementation. Submitted.
25. Maas YGH, Gerritsen J, Hart AAM, et al. Development of macronutrient
composition of very preterm human milk. Br J Nutr 1998;80:35-40.
26. Van Wassenaer AG, Kok JH, Endert E, Vulsma T, de Vijlder JJM. Thyroxine
supplementation to infants of less than 30 weeks gestational age does not increase
plasma triiodothyronine concentrations. Acta Endocrinol 1993;129:139-146.
27. Dubowitz LMS, Dubowitz V, Goldberg C. Clinical assessment of gestational age in
newborn infants. J Pediatr 1970;77:1-10.
28. Volpe JJ. Neurology of the newborn. 2nd ed. W.B. Saunders Company ;1987:p331.
29. De Vries LS, Eken P, Dubowitz LMS. The spectrum of leukomalacia using cranial
ultrasound. Behav Brain Res 1992;49:1-6.
30. Levene MI. Measurements of the lateral ventricles in preterm infants with real-time
ultrasound. Arch Dis Child 1981;56:900-904.
31. Prechtl H. The neurological examination of the full term newborn infant. 2nd. Edn.
Clinics in Developmental Medicine No 63. William Heinemann medical books Ltd.
London, UK, 1977.
32. Jurgens-van der Zee AD, Bierman-van Eendenburg MEC, Fidler VJ, et al. Preterm
birth, growth retardation and acidemia in relation to neurological abnormality of the
newborn. Early Hum Dev 1979;3/2:141-154.
33. Dixon WJ, ed. BMDP statistical software manual. Berkeley, Los Angeles, Oxford:
University of California Press, 1992.
34. Vies J, Kingma H, Caberg H, Duniels H, Casaer P. Posture and motility of lowrisk
preterm infants: a study from 32-36 weeks of postconceptional age. Dev Med Child
Neurol 1989;31:191-195.
35. Geerdink JJ, Hopkins B. Effects of birthweight status and gestational age on the
quality of general movements in preterm newborns. Biol Neonate 1993;63:215-224.
36. Van Kranen-Mastenbroek VHJM, Folmer KB, Kingma H, et al. The influence of
head position and head position change on spontaneous body posture and motility of
fullterm AG A and SGA newborn infants. Brain Dev 1997;19:104-110.

General body movements in preterm infants 123
37. Kalkebeeke TH, Siebenthal KV, Largo RH. Movement quality in preterm infants
prior to term. Biol Neonate 1998;73:145-154.
38. Smit BJ, Kok HJ, de Vries LS, van Wassenaer AG, Dekker FW, Ongerboer de
Visser BW. Motor nerve conduction velocity in very preterm infants in relation to L-
thyroxine supplementation. J Pediatr 1998;132:64-69.
39. Smit BJ, Kok HJ, de Vries LS, van Wassenaer AG, Dekker FW, Ongerboer de
Visser BW. Somatosensory evoked potentials in very preterm infants in relation to L-
thyroxine supplementation. Pediatrics 1998;101:865-869.
40. Dubowitz L and Dubowitz V, (eds) The neurological assessment of the preterm and
full-term newborn infants. Clinics in Developmental Medicine No 79, William
Heinemann medical books Ltd. London, UK, 1981.
41. Amiel-Tison C. A method for neurological evaluation within the first year of life.
Current Problems in Pediatrics 1976;7:1-50.
42. Amiel-Tison C and Grenier A, (eds). Neurological Assessment during the First Year
of Life. Oxford University Press, Oxford, 1986.
43. Amiel-Tison C. Developmental outcome and follow-up of the small-for-gestational
age infant. Am J Obstet Gynecol 1980;138:303-306.
44. Bos AF, Van Loon AJ, Hadders-Algra M, Martijn A, Okken A, and Prechtl HFR.
Spontaneous motility in preterm, small-for-gestational age infants. II Qualitative
aspects. Early Hum Dev 1997; in press.

124 Chapter 6