Embed Size (px)
Citation preview

Dr. Wernham discloses that hehas received financial supportfrom Pfizer Animal Health Group,New Zealand, and Boehringer-Ingelheim.
icipital tenosynovitis is defined as inflamma-tion of the biceps brachii tendon and itsenveloping synovial sheath.1–3 Although the
condition has been reported as a common cause offorelimb lameness in dogs, its true prevalence isunknown.1–5 Bicipital tenosynovitis has beendescribed as a difficult and frustrating disease todiagnose, and the diagnosis is often made by elim-inating all other causes of lameness referable tothe shoulder joint.1,2 Likewise, definitive recom-mendations regarding the treatment and manage-ment of bicipital tenosynovitis have not been fullyevaluated. This article discusses the pertinentanatomy, signalment, history, etiology, pathophysi-ology, and diagnosis of bicipital tenosynovitis.Medical and surgical treatment options, including
postoperative rehabilitation, arealso reviewed.
ANATOMYThe biceps brachii muscle originates from thesupraglenoid tubercle via a long tendon thatcourses distally through the intertuberculargroove of the humerus6 (Figure 1). Distal to thegroove, the tendon blends into the spindle-shaped biceps brachii muscle.6 The joint capsulereflects around the tendon of origin at the cranialaspect of the scapulohumeral joint, forming asynovial tendon sheath that contains the bloodvessels and nerves supplying the tendon. Bicipitaltenosynovitis affects this intracapsular, extrasyn-ovial region of the tendon.1 The joint capsuleprojects distally along the tendon, through theintertubercular groove, and for a short distancedistal to the transverse humeral ligament.2 Thetransverse humeral ligament spans the greaterand lesser tubercles of the humerus and acts tomaintain the tendon and its sheath within theintertubercular groove. The capsule blends withthis ligament craniomedially, with thesupraspinatus and infraspinatus tendons laterally,and with the subscapularis tendon medially.
October 2008 537 COMPENDIUM
BicipitalTenosynovitis in DogsBenjamin G. J. Wernham, BVScRichard M. Jerram, BVSc, DACVSChristopher G. A. Warman, BVSc, MVS, MACVScVeterinary Specialist GroupAuckland, New Zealand
B
ABSTRACT:Bicipital tenosynovitis is a common cause of forelimb lameness in dogs. It typically
occurs in medium-sized or large, middle-aged or older animals.A history of chronic, progressive or
intermittent, moderate to severe weight-bearing lameness that is exacerbated by exercise is often
reported, and in most instances, an inciting cause is not identified. Diagnosis requires a planned and
systematic approach and is often challenging. Medical and surgical therapies exist, but definitive
recommendations regarding the optimum treatment modalities have not been fully established.The
prognosis for dogs with bicipital tenosynovitis is generally good to excellent in animals that undergo
surgical therapy; however, long-term follow-up of clinical patients is limited.
RelatedContent onCompendiumVet.com• Arthroscopy in Dogs: ForelimbJoint Diseases (August 2005)
Article #1CE

Medially and laterally, the joint capsule is irregularlythickened to form the medial and lateral glenohumeralligaments, which, in combination with the joint capsuleand periarticular musculature, are primarily responsiblefor shoulder stability.7 The tendon of insertion of thebiceps brachii muscle divides into two parts at the regionof the elbow joint. The stronger part inserts on the ulnartuberosity, and the weaker part inserts on the radialtuberosity.6
The biceps brachii muscle acts to flex the elbow andextend the shoulder joint.The biceps tendon contributesto passive shoulder joint stability, particularly in theneutral and flexed positions, and provides medial stabil-ity of the shoulder joint during extension.7
SIGNALMENT AND HISTORYBicipital tenosynovitis primarily occurs in medium-sized to large, middle-aged or older dogs.1,3,5,8 No breed
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs538 CE
• Direct trauma/rupture (e.g., collision injury)• Chronic overuse activities (e.g., digging, agility
exercises)• Mechanical injury secondary to medial displacement
of the biceps brachii tendon• Mechanical injury secondary to irritation of the
biceps brachii tendon and sheath by joint mice orosteophytes
• Mechanical injury secondary to calcifyingtendinopathy of the supraspinatus tendon
• Mechanical injury secondary to glenohumeralinstability
Box 1.Causes of BicipitalTenosynovitisin Dogs
Figure 1. Medial view of the shoulder joint illustratingthe relevant anatomy.Reproduced with permission fromJohnston SA, Biery DN, eds. Pfizer Atlas of Common PainfulConditions in Dogs and Cats.The Gloyde Group; 2003:24.
or sex predilection has been reported.1 Brinker and col-leagues9 reported that poorly conditioned or sedentaryanimals may be more prone to bicipital tenosynovitisthan physically fit animals. However, other reports havesuggested that active and athletic dogs are more suscep-tible to developing the disease.1,3,5
Affected dogs typically have a history of chronic, pro-gressive or intermittent, moderate to severe weight-bearing lameness that is exacerbated by exercise.1,3,5,8–12
There may be a history of an inciting traumatic inci-dent, but often, the onset of clinical signs is slow. Inmany cases, lameness has been evident for severalmonths before presentation.1,3,5
ETIOLOGY AND PATHOPHYSIOLOGYInflammation of the biceps tendon and its associatedsheath has been reported to be due to a variety ofcauses1–5,7–16 (Box 1). However, in many cases, an incitingcause is not established, and the disease is consideredprimary.1,12
It is suspected that repeated stress or trauma to thebiceps tendon results in hemorrhage and edema of thetendon and its surrounding synovium.1,2 The resultinginflammatory response leads to a predominantly lympho-cytic–plasmacytic cellular infiltration of the tendon andsynovium.1,12 Progression of the disease leads to synovialvillous hyperplasia and tendon fibrosis.1,2,9 In synovial vil-lous hyperplasia, the synovium proliferates and developsfolds, and vascularization subsequently increases.3 Densefibrous adhesions form between the tendon and its sheath,tending to limit motion.17 Continual movement of theseinflamed tissues within the intertubercular groove causespain and additional inflammation.2 Hypoxia of the tendonas a result of damaged blood supply can promote chon-
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs540 CE
droid metaplasia and calcification of the biceps tendon(biceps brachii calcifying tendinopathy).1,12,18 Calcificationof the tendon is thought to result from chondrocyte-mediated osteogenesis, resembling the early stages ofendochondral ossification. However, fibrocartilage trans-formation is not an essential step for calcification todevelop within the biceps brachii tendon.18
DIAGNOSISOrthopedic ExaminationA thorough and systematic orthopedic examination isessential when bicipital tenosynovitis is suspected.Details of the canine orthopedic examination are
described elsewhere.19 A complete orthopedic examina-tion allows the veterinarian to isolate the pain to theshoulder joint and aids in the diagnosis of any concur-rent orthopedic conditions. After localizing the pain tothe shoulder, the veterinarian should create a differentialdiagnosis19,20 (Box 2). A detailed neurologic examinationmay also be warranted, as conditions affecting thebrachial plexus (e.g., peripheral nerve sheath tumor) andcaudal cervical spine (e.g., intervertebral disk extrusion)often mimic shoulder pain.20
Dogs generally bear weight on the affected limbbecause pain occurs only when the diseased tendon isgliding within the intertubercular groove.1 Animals arevisually lame during ambulation, and this lameness isexacerbated with exercise.1–3,5,8–12 Affected animals mayguard against flexion and extension of the shoulderjoint, which can limit the swing phase of the gait.2,9
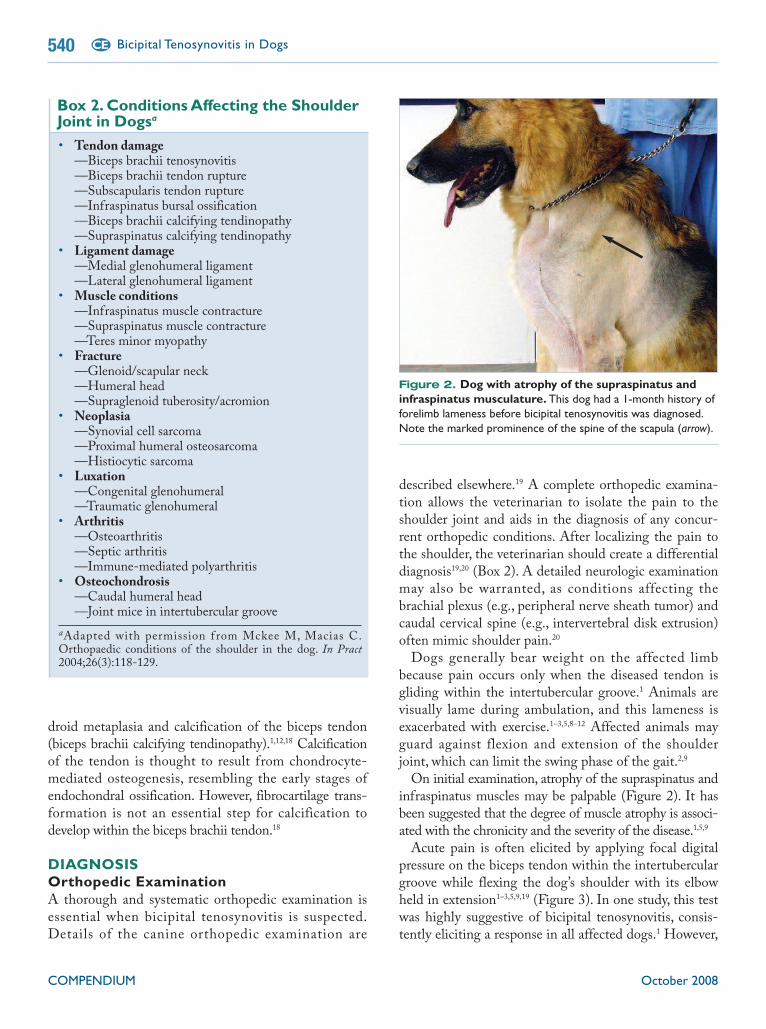
On initial examination, atrophy of the supraspinatus andinfraspinatus muscles may be palpable (Figure 2). It hasbeen suggested that the degree of muscle atrophy is associ-ated with the chronicity and the severity of the disease.1,5,9
Acute pain is often elicited by applying focal digitalpressure on the biceps tendon within the intertuberculargroove while flexing the dog’s shoulder with its elbowheld in extension1–3,5,9,19 (Figure 3). In one study, this testwas highly suggestive of bicipital tenosynovitis, consis-tently eliciting a response in all affected dogs.1 However,
• Tendon damage—Biceps brachii tenosynovitis—Biceps brachii tendon rupture—Subscapularis tendon rupture—Infraspinatus bursal ossification—Biceps brachii calcifying tendinopathy—Supraspinatus calcifying tendinopathy
• Ligament damage—Medial glenohumeral ligament—Lateral glenohumeral ligament
• Muscle conditions—Infraspinatus muscle contracture—Supraspinatus muscle contracture—Teres minor myopathy
• Fracture—Glenoid/scapular neck—Humeral head—Supraglenoid tuberosity/acromion
• Neoplasia—Synovial cell sarcoma—Proximal humeral osteosarcoma—Histiocytic sarcoma
• Luxation—Congenital glenohumeral—Traumatic glenohumeral
• Arthritis—Osteoarthritis—Septic arthritis—Immune-mediated polyarthritis
• Osteochondrosis—Caudal humeral head—Joint mice in intertubercular groove
aAdapted with permission f rom Mckee M, Macias C.Orthopaedic conditions of the shoulder in the dog. In Pract2004;26(3):118-129.
Box 2.ConditionsAffecting the ShoulderJoint in Dogsa
Figure 2. Dog with atrophy of the supraspinatus andinfraspinatus musculature.This dog had a 1-month history offorelimb lameness before bicipital tenosynovitis was diagnosed.Note the marked prominence of the spine of the scapula (arrow).

October 2008 COMPENDIUM
Bicipital Tenosynovitis in Dogs 541CE
failure to detect pain in the biceps brachii tendon doesnot rule out disease.19
It has been reported that the biceps retraction testmay be used to differentiate painful conditions of thebiceps tendon from other shoulder conditions.5 How-ever, in a study by Bardett,7 85% (40 of 47) of dogsdiagnosed with glenohumeral instability were also posi-tive for the biceps retraction test. Thus, a positive bicepsretraction test result appears to be an indicator of shoul-der joint pain rather than a pathognomonic sign ofbiceps tendon disease. The biceps retraction test is con-ducted with the dog standing or in lateral recumbency.The examiner’s hand is passed medial to the elbow sothat the olecranon rests in the palm of the hand (Figure4).The index finger is curled around the insertion of thebiceps tendon and pulled caudally. The presence of painis noted and compared with the contralateral limb.
RadiographyRadiographic evaluation of the shoulder joint shouldinclude standard lateral and craniocaudal views and cran-ioproximal–craniodistal (“skyline”) views of both shoul-ders. Radiographic findings may include sclerosis of theintertubercular groove, periarticular osteophyte forma-tion on the caudal aspect of the humeral head and gle-noid cavity (Figure 5), osteophyte formation at theintertubercular groove, enthesiophyte formation at the
supraglenoid tuberosity, and mineralization of the bicepsbrachii and supraspinatus tendons.1–3,5,9,21 Only sclerosisof the intertubercular groove has been reported as a spe-cific radiographic feature of bicipital tenosynovitis.22
However, a study by Lechleitner and Mayrhofer23 reported
that 60 of 100 dogs with no history of forelimb lamenesshad radiographic evidence of sclerosis within the intertu-bercular groove. Others have suggested that enthesio-phyte formation at the supraglenoid tuberosity andmineralization of the biceps brachii tendon are morespecific radiographic features of bicipital tenosynovitis.2,18
The cranioproximal–craniodistal radiographic viewcan be obtained by placing the animal in sternal recum-bency. The affected shoulder and elbow are hyperflexed
Figure 3. Position of the flexed shoulder and extendedelbow when applying focal digital pressure to the bicepsbrachii tendon within the intertubercular groove.
Figure 4. Position of the examiner’s hand whenconducting the biceps retraction test in a standing dog.
A thorough and systematic orthopedic examination is essentialwhen bicipital tenosynovitis is suspected.

COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs542 CE
while the radius and ulna are placed adjacent to the tho-racic wall.24 The animal’s head is positioned away fromthe affected limb. The cassette is positioned over theantebrachium and parallel with the table. It is essentialthat the humeral head is positioned over the film andnot obliquely so that distortion of the intertuberculargroove is minimized.24 Once the correct positioning hasbeen obtained, the x-ray beam is centered over the cra-nial aspect of the shoulder (Figure 6). This view assistsin the identification of calcification of the biceps brachiitendon and subtle irregularities in the intertuberculargroove1,14 (Figure 7). Radiographic imaging of the con-tralateral limb can be useful for direct comparison.
ArthrocentesisArthrocentesis should be performed to rule out otherpotential causes of shoulder pain, such as septic arthritisand immune-mediated polyarthritis.9 The shoulder
region is clipped and surgically prepared. A 1.5-inch,22-gauge spinal needle is used. The joint is enteredabout 1 cm distal to the acromion process of thescapula, with the needle directed toward the glenoid9
(Figure 8). If fluid is not found, the needle should be“walked” in different directions from the same skinpuncture site. Synovial fluid is aspirated, and its turbid-ity and viscosity are assessed. Synovial fluid should besubject to complete laboratory analysis and culture if anyabnormalities are suspected.
Cytologic analysis of synovial fluid from dogs withbicipital tenosynovitis tends to show changes consistentwith degenerative joint disease.1 In one study, 82%1 (14 of17) of dogs diagnosed with bicipital tenosynovitis showedelevations in monocyte, macrophage, and vacuolatedphagocyte concentrations, which were indicative ofdegenerative joint disease. However, these synovial fluidchanges are not specific for bicipital tenosynovitis, and
Figure 5. Mediolateral radiograph of a dog with a 1-month history of forelimb lameness before diagnosis ofbicipital tenosynovitis and shoulder osteoarthritis.Notethe marked sclerosis (Sc) within the intertubercular groove andthe osteophytosis (Os) associated with the caudal aspect of theglenoid and humeral head.
Figure 6. Correct position to obtain the cranioproximal–craniodistal view of the shoulder.Note that the x-ray beam(red outline) is centered over the cranial aspect of the shoulder.This view gives the veterinarian the clearest image of theintertubercular groove because it avoids superimposition of theintertubercular groove and the proximal end of the humerus.

not all cases of bicipital tenosynovitis exhibit synovialfluid abnormalities.1,5
Positive-Contrast ArthrographyPositive-contrast arthrography has been described as auseful diagnostic modality for identifying abnormalitiesassociated with bicipital tenosynovitis in dogs.2,3,5,10,15,21
The details and application of the procedure are describedelsewhere.25 Because the tendon sheath is continuouswith the scapulohumeral joint, a normal arthrogramshould fill the tendon sheath.9 The column of contrastagent should be continuous and have a lobulated appear-ance distally.9 Common abnormal findings include absentor incomplete filling (“filling defects”) of the tendonsheath with contrast agent, irregularities in the appear-ance of the tendon sheath, widening of the distal aspectof the tendon sheath, narrowing of the biceps tendonproximal to the transverse humeral ligament, and leakageof the contrast agent from the tendon sheath.1,3,5,9,10,15,21
Filling defects along the tendon may correspond to prolif-erative synovium, inflammation and adhesions betweenthe tendon and sheath, or joint mice.9,15,21 Leakage of con-trast agent from the tendon sheath is consistent with ten-don sheath rupture. However, iatrogenic tendon sheathrupture caused by overdistention of the sheath duringarthrography must also be considered.25
Because the synovium of the biceps tendon sheath is
contiguous with that of the scapulohumeral joint cap-sule, effusion and, hence, filling defects within thebiceps brachii tendon sheath can be due to other condi-tions that cause effusion within the scapulohumeraljoint.22 Negative findings on arthrography in dogs withbicipital tenosynovitis have also been described.2,9
Therefore, abnormal findings associated with positive-contrast arthrography should complement clinical, radi-ographic, and ultrasonographic findings and should notbe used as the sole means of diagnosing bicipitaltenosynovitis in dogs.1,10,22,26
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs544 CE
Figure 7. Cranioproximal–craniodistal radiographs.
Radiograph of a dog diagnosed with bicipital tenosynovitis andconcurrent supraspinatus tendon avulsion. Note the increasedcalcification of the biceps brachii tendon (B) and the sclerosis (Sc)of the intertubercular groove.The veterinarian must be cautiouswhen interpreting the finding of calcification adjacent to theintertubercular groove as being within the biceps tendon. Moreoften, increased radiopacity in this area is the result ofcalcification of the supraspinatus tendon of insertion orsupraspinatus tendon avulsion (S).
Radiograph of a normal canine shoulder. The biceps tendontravels along the intertubercular groove (ITG), which is locatedbetween the greater (GT) and lesser tubercles (LT) of thehumerus. Note the sharp outline of the intertubercular groovecompared with the image on the left.
Figure 8. Anatomic landmarks used when performingarthrocentesis on the left shoulder joint of a dog.Theright index finger is placed on the acromion of the spine of thescapula, and the left index finger is placed on the greatertuberosity of the humerus.The surgical draping has been removedfor illustration.
UltrasonographyDebate still exists over the benefits of using ultrasonog-raphy versus arthrography to evaluate bicipital tendondisease in dogs. Rivers et al21 reported that ultrasonogra-phy was less sensitive for diagnosing bicipital tenosyn-ovitis compared with arthrography. However, morerecent reports have suggested that ultrasonography ismore accurate, particularly in identifying intratendinous
or tendon sheath pathology.1,5,26–28 This is consistentwith findings in humans, in whom ultrasonography isoften used as the modality of choice in biceps tendonimaging, with magnetic resonance imaging (MRI) beingused in cases in which ultrasonography is inconclusive.29
Ultrasonography of the canine biceps apparatus has beendescribed in detail.26–28,30 The biceps tendon is easily recog-nized by its dense, linear, hyperechoic fiber pattern, whichis oriented with its long axis28,30 (Figure 9). The compact,
hyperechoic appearance of the biceps tendon is rapidlyreplaced by the coarse, hypoechoic biceps muscle fibers atthe musculotendinous junction.28,30 Above and below thetendon, the tendon sheath appears as a hyperechoic line,and its oval shape is readily recognized on cross-section.26A small amount of joint fluid is seen within the tendonsheath at its origin, represented by a thin anechoic halosurrounding the tendon on cross-section.28 Scanning the
transverse plane allows broad visualization of the entireintertubercular groove around the tendon, which is typi-cally smooth and uniformly reflective.28
Changes associated with bicipital tenosynovitis onultrasonographic examination may include the follow-ing26–28,30 (Figure 9):
• A hypoechoic to anechoic area around the biceps tendonconsistent with excess fluid within the tendon sheath
October 2008 COMPENDIUM
Bicipital Tenosynovitis in Dogs 545CE
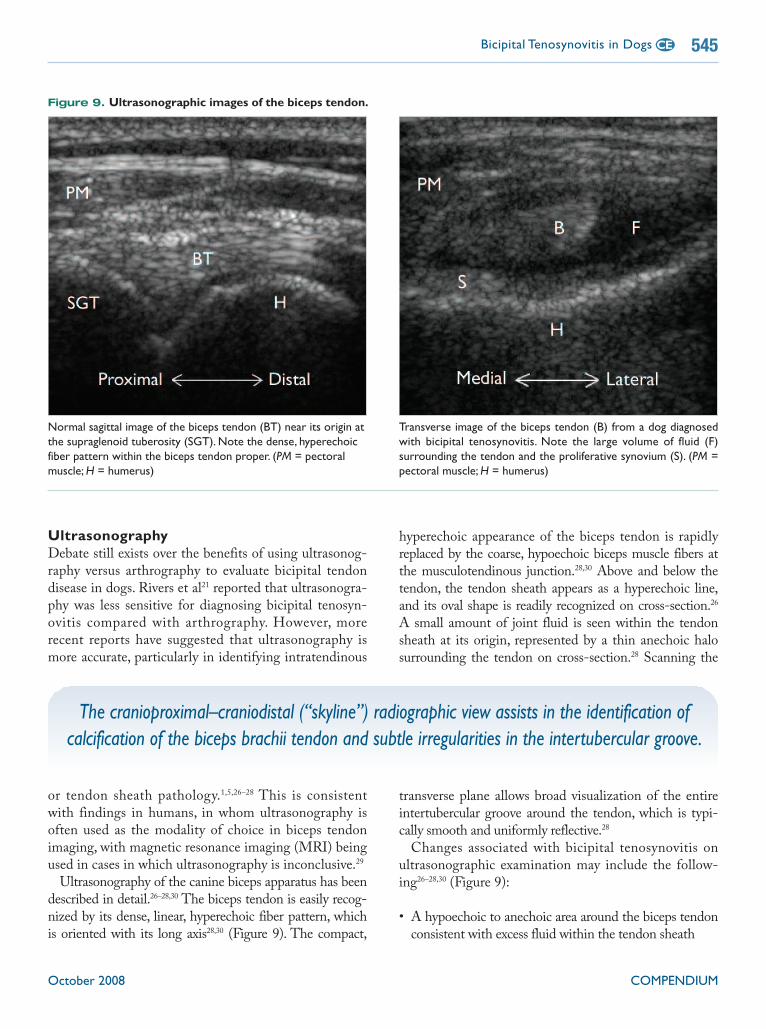
Figure 9. Ultrasonographic images of the biceps tendon.
Normal sagittal image of the biceps tendon (BT) near its origin atthe supraglenoid tuberosity (SGT). Note the dense, hyperechoicfiber pattern within the biceps tendon proper. (PM = pectoralmuscle;H = humerus)
Transverse image of the biceps tendon (B) from a dog diagnosedwith bicipital tenosynovitis. Note the large volume of fluid (F)surrounding the tendon and the proliferative synovium (S). (PM =pectoral muscle;H = humerus)
The cranioproximal–craniodistal (“skyline”) radiographic view assists in the identification ofcalcification of the biceps brachii tendon and subtle irregularities in the intertubercular groove.

• A hypoechoic, thickened tendon with possible fiberpattern disruption
• An irregular or proliferative synovial lining• Mineralization within the biceps tendon• An irregular intertubercular groove (in chronic cases)
Joint mice within the tendon sheath may be seen asirregular hyperechoic structures; joint mice larger than 2 to3 mm in diameter commonly result in distal acousticshadowing.27 As with arthrography, identification of exces-sive fluid within the tendon sheath during ultrasonogra-phy is not a specific finding for bicipital tenosynovitis.30
The advantages of ultrasonography are that it (1) is afast, noninvasive procedure that does not require generalanesthesia; (2) allows the exact location and extent ofthe lesion to be determined; (3) allows dynamic studiesto be conducted to assess abnormal tendon glidingmotion; and (4) allows serial examinations to be easilyperformed to assess tendon healing after therapy.5,26,28
The major disadvantage of ultrasonography is that the
information obtained is highly operator dependent. Ahigh level of experience with orthopedic ultrasonogra-phy and the use of standardized examination proceduresare essential for correct ultrasonographic evaluation anddiagnosis of bicipital tenosynovitis.26
ArthroscopyArthroscopy has significantly advanced the diagnosticinvestigation of intraarticular conditions of the shoulderjoint. It has become an extremely useful modality fordiagnosing bicipital tenosynovitis in dogs.3,20 Shoulderarthroscopy allows thorough, minimally invasive visualassessment of the intraarticular, extrasynovial componentof the biceps tendon and provides a potential avenue fortreatment.31 The type of arthroscope required, necessaryinstruments, and arthroscopic techniques for evaluationof the shoulder joint have been described elsewhere.3Arthroscopic examination may show synovial hyperemiaand proliferation, partial tearing of biceps tendon fibers,mineralization and hypertrophy of the biceps tendon,and osteophyte production within the intertuberculargroove3,32 (Figure 10).
Most cases of bicipital tenosynovitis occur at the originand midsubstance level of the tendon. However, carefulevaluation of the entire intraarticular portion of the ten-don is recommended to avoid diagnostic error.31 Probingthe tendon with a blunt instrument may be necessary inorder to evaluate integrity and detect partial tears.20
Magnetic Resonance Imaging andArthrographyStudies investigating the use of MRI and magnetic reso-nance arthrography in the diagnosis of bicipital tenosyn-ovitis in dogs are lacking. A recent study by Schaefer and
Forrest33 aimed to evaluate specific MRI acquisitionsequences and planes for observing diagnostic structuresof interest in the canine shoulder. They found that theT2*-weighted gradient echo sequence was preferred forevaluation of tendons and ligaments. They concludedthat the sagittal plane was most useful for evaluating thebiceps tendon in the longitudinal/long oblique view andthat both the transverse and dorsal planes provided the
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs546 CE
Figure 10. Arthroscopic image of the biceps tendon in adog diagnosed with bicipital tenosynovitis.Note the severesynovial proliferation and partial tearing of biceps tendon fibers.(Image courtesy of Drs. James Cook and JamesTomlinson,University of Missouri)
Arthrocentesis should be conducted to rule out other causes of shoulder pain,such as septic arthritis and immune-mediated polyarthritis.

best views for evaluating the relationship between thesupraspinatus and biceps tendons. Ultrasonography andMRI have been shown to have comparable accuracy fordetecting partial tears of the rotator cuff in humans.34
However, MRI enables better evaluation of the extent,location, and classification of lesions as well as detectionof associated pathologies of the shoulder.34 Magnetic res-onance arthrography has been shown to be more accu-rate than conventional MRI in evaluating rotator cuffsize and morphologic features in humans.35 Nevertheless,MRI is still limited by its cost and accessibility andshould therefore be used to complement rather thanreplace other diagnostic modalities.
MEDICALTHERAPYThe primary objective of medical therapy is to reduceinflammation of the biceps tendon and sheath.2,9
Intraarticular methylprednisolone acetate therapy isadvocated if no known mechanical causes (e.g., jointmice) are associated with the disease.9 Arthrocentesisand a complete examination of the synovial fluid shouldbe conducted before corticosteroid injection to confirmthat the joint is not septic.9 Injection of methylpred-nisolone acetate (20 to 40 mg) into the joint should befollowed by strict confinement for 6 weeks.5,9 If lame-ness is markedly improved but still persists, a secondinjection may be given after the 6-week confinementperiod. Direct injection of corticosteroids into the ten-don has been associated with collagen necrosis and ten-don rupture and is therefore contraindicated.36
The use of systemic NSAID or corticosteroid therapyin the medical management of bicipital tenosynovitis hasnot been scientifically evaluated. One report showed res-olution of lameness in six of seven dogs diagnosed withtraumatic bicipital tenosynovitis that were treated with a3-week course of carprofen (2 to 4 mg/kg/day PO) andstrictly confined for 6 weeks.5 It has been reported thatstrict confinement and NSAID or intraarticular steroidtherapy is often sufficient in acute or traumatic cases ofbicipital tenosynovitis.5,9 In one study, lameness resolvedin 11 of 13 dogs diagnosed with traumatic bicipitaltenosynovitis after administration of intraarticularsteroids (five of six dogs) or systemic nonsteroidal (six ofseven dogs) antiinflammatories and 6 weeks of strictconfinement followed by another 6 weeks of exerciserestriction.5 In contrast, Stobie et al1 reported that onlyseven of 16 dogs responded favorably to intratendinoussteroid therapy followed by 2 weeks of exercise restric-tion. It has been proposed that adequate confinement of
October 2008 COMPENDIUM
Bicipital Tenosynovitis in Dogs 547CE

at least 3 months’ duration may be required in determin-ing a favorable outcome in cases of traumatic bicipitaltenosynovitis.5 Reintroduction of uncontrolled exercisetoo early in the repair phase can disrupt tissue healing,slow recovery, and incite chronic lameness.5
It has been shown that corticosteroids can impair thebiomechanical properties and metabolic activities ofarticular cartilage.37 Therefore, prolonged medical ther-apy should be avoided in dogs with bicipital tenosynovi-tis, and surgery should be considered for dogs that donot improve after one or two doses of corticosteroids.1
The use of antiinflammatory medications in combina-tion with physical rehabilitation has not been fully evalu-ated as a treatment for bicipital tenosynovitis in dogs.Intraarticular methylprednisolone acetate, shoulder stabi-lization/stretching exercises,38 and pulse mode 3.3-MHztherapeutic ultrasound are used as initial treatmentmodalities in our hospital, with good success. Therapeu-tic ultrasound has thermal (mechanical) and nonthermal(biomechanical) effects on tissues.39 The deep heatingproduced by ultrasound can produce increases in collagenextensibility, pain threshold, blood flow, and macrophageand enzyme activity while decreasing muscle spasms.39
Nonthermal effects (i.e., the effects resulting from soundwaves causing molecules to vibrate) include stimulationof collagen deposition, angiogenesis, and fibroblast pro-liferation.39 The use of therapeutic ultrasound, including
its indications and treatment guidelines, has beendescribed in detail elsewhere.39
SURGICALTHERAPYSurgical treatment is often recommended for dogs thatdo not respond to medical therapy or for dogs in whicha mechanical cause is found initially.9,12 It is hypothe-sized that motion of the inflamed biceps tendon andsheath within the intertubercular groove is the cause ofpain; therefore, eliminating movement of the biceps ten-don through the intertubercular groove is the goal ofsurgical treatment.1,2,9 This goal may be achieved byeither tenodesis or tenotomy of the origin of the bicepsbrachii tendon.1,2,9,12,20
Biceps TenodesisClinical reports of biceps tenodesis show good to excellentresults.1, 40 Biceps tenodesis involves transferring the originof the biceps tendon from the supraglenoid tubercle to theproximal humerus. The procedure may be performed viaan open9 or arthroscopically assisted40 approach. There arethree methods of open biceps tenodesis:
• Screw and spiked plastic washer technique.9 Thismethod involves transecting the biceps tendon near itsattachment at the supraglenoid tuberosity. An appropri-ately sized bone screw and spiked plastic washer arethen used to attach the tendon to the proximalhumerus9 (Figure 11). Redundant tendon proximal tothe screw is removed and submitted for histopathology.9
• Passage of the transected biceps tendon through atunnel drilled in the greater tubercle of the humerus,followed by suturing the tendon laterally to thesupraspinatus muscle or the infraspinatus tendon.9
• Placement of a double Bunnell-Meyer suture pattern,using number 1 nonabsorbable suture material, in theproximal biceps muscle. Two parallel holes are thenmade in the greater tubercle of the humerus adjacentto the proximal biceps muscle. The two ends of suturematerial are passed through the holes and tied later-ally with the shoulder extended.9
The use of arthroscopy-assisted biceps tenodesis in sixdogs diagnosed with bicipital tenosynovitis wasreported.40 Although technically demanding, the tech-nique was minimally invasive and resulted in good toexcellent outcomes in all six dogs. The authors of thestudy concluded that further studies were required tofully assess the feasibility and results of the technique.
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs548 CE
Figure 11. Biceps tenodesis using the screw and spikedplastic washer technique in a dog.Craniomedial view of theleft shoulder joint. (B = biceps brachii tendon;GT = greatertubercle of the humerus; TH = transverse humeral ligament[transected])

Biceps TenotomyBiceps tenotomy involves transecting the biceps tendonfrom its origin, thereby preventing movement of theinflamed tissue within the intertubercular groove. Theprocedure may be performed through an open approachor arthroscopically.20 Arthroscopic tenotomy may beperformed using a scalpel, motorized shaver, or bipolarradiofrequency and is typically associated with fewerpostoperative complications, less tissue trauma, and sub-sequently less postoperative pain than tenodesis.3,12,31
The optimum location for tenotomy has yet to be deter-mined.31 Some surgeons cut the tendon as close to itsorigin as possible, while others cut below the lesion andattempt to remove the diseased tissue.31
Esterline and colleagues11 described the use of ultra-sound-guided percutaneous biceps brachii tenotomy asan alternative to arthroscopic tenotomy or surgical ten-odesis in 11 dogs. They concluded that this techniquewas a quick, easy, and accurate method of providingbiceps tendon release.11
The effect of biceps tenodesis and tenotomy on shoul-der and elbow function has not been adequately deter-mined in dogs. Early studies showed that the bicepstendon does not contribute significantly to scapulo-humeral stability.7 However, a more recent in vitro studyshowed that transection of the biceps tendon resulted ina small but significant increase in shoulder joint insta-bility.41 Some authors suggest that after tenotomy, thebrachialis muscle acts to maintain normal elbow flexionwhile the biceps brachii tendon slowly forms adhesionsto the proximal humerus, essentially producing a naturaltenodesis.12
The indications for, and long-term functional out-comes of, biceps tenotomy versus tenodesis have notbeen determined in dogs.40 Tenodesis is typically recom-mended over tenotomy in athletic humans.42 Someauthors have suggested that this finding, in addition tothe canine forelimb’s weight-bearing function, favors theuse of biceps tenodesis, especially in athletic and work-ing dogs.40 Long-term studies are required to determinethe effects of tenotomy versus tenodesis on muscle,elbow, and limb function before definitive recommenda-tions can be made.1,12,31,40
POSTOPERATIVE CAREPostoperative care must be tailored to the individualpatient, and recovery times may vary. As is true for themanagement of any orthopedic condition, weight man-agement, physical rehabilitation, use of antiinflamma-
October 2008 COMPENDIUM
Bicipital Tenosynovitis in Dogs 549CE

tory medications, and owner compliance are critical forobtaining the most successful outcome when treatingbiceps tenosynovitis using any modality.40
We have found the following postoperative regimeneffective in many patients treated surgically:
• Use ice in the early postoperative period to decreasethe pain originating from the shoulder region, localinflammation, and edema formation.
• Apply a Velpeau or modified Velpeau sling andstrictly confine the patient for 3 weeks.9,43 The slingshould be changed weekly, at which time, 45 minutesof passive range of motion (PROM) exercises shouldbe performed on the affected limb.
• After 3 weeks of confinement, remove the sling andplace the dog on exercise restriction for a further 5weeks.1
• During the 5 weeks of exercise restriction, the ownershould massage the surrounding musculature and per-
form gentle PROM exercises and flexion/extensionexercises of the shoulder joint up to three times a dayto assist with joint motion and prevent disuse muscleatrophy. In our hospital, a registered animal physicaltherapist teaches the owner how to perform theseexercises.
• Eight weeks after surgery, start the dog on a 6-weekcontrolled exercise program. Initially, heat therapy,shoulder flexion/extension exercises, and 10-minuteleash walking sessions are performed up to three timesa day.3 Between sessions, the dog is confined to asmall area and is allowed no free activity.3 The flex-ion/extension exercises can be varied and may includewalking through tall grass, controlled swimming, useof an exercise ball, or walking in shallow water; all ofthese increase the range of joint motion and theendurance of the surrounding musculature.3 Theduration of the leash walks is gradually increased. Bythe sixth week, the dog should be able to walk on aleash for 20 minutes followed by free activity for afurther 10 minutes.3 Normal activity may resume afterthe end of the 6-week exercise program.
PROGNOSISThe prognosis for normal limb function with bicipitaltenosynovitis depends on several variables, including thedegree of pathology and associated degenerative jointdisease, weight control, physical rehabilitation, andowner compliance.3 In the few studies published, resultsof biceps tenodesis and tenotomy are comparable, withgood to excellent return to limb function reported forboth techniques.1,3,5,12,40 Most dogs regain normal limbfunction 2 to 3 months after surgery.1,3 However, returnto function may be prolonged in some dogs, and up to 9months may be required before full recovery is seen.1
CONCLUSIONThe diagnosis of bicipital tenosynovitis requires a planned,methodical approach. Advances in arthroscopy and ultra-sound evaluation of the biceps brachii tendon have led to agreater understanding of biceps tendon pathology andhave revolutionized the diagnostic accuracy in these cases.Studies evaluating long-term outcomes of medical and
surgical therapy in the treatment of bicipital tenosynovitisare lacking. Prospective, randomized, controlled studiescomparing treatment options for bicipital tenosynovitis arerequired before recommendations regarding the optimumtreatment modality can be made.
ACKNOWLEDGMENTThe authors acknowledge Pfizer Animal Health Group, New Zealand, for its sup-port of Dr. Benjamin Wernham’s internship program.
REFERENCES1. Stobie D, Wallace LJ, Lipowitz AJ, et al. Chronic bicipital tenosynovitis in
dogs: 29 cases (1985-1992). JAVMA 1995;207:201-207.2. Lincoln JD, Potter K. Tenosynovitis of the biceps brachii tendon in dogs.
JAAHA 1984;20:385-392.3. Beale BS, Hulse DA, Schulz KS, Whitney WO. Arthroscopically assisted
surgery of the shoulder joint. In Beale BS, Hulse DA, Schulz KS, WhitneyWO, eds. Small Animal Arthroscopy. Philadelphia: WB Saunders; 2003:38-41.
4. Bardett JF. Lesions of the biceps tendon—diagnosis and classification. VetComp Orthop Traumatol 1999;12:188-195.
5. Bruce WJ, Burbidge HM, Bray JP, Broome CJ. Bicipital tendinitis andtenosynovitis in the dog: a study of 15 cases. N Z Vet J 2000;48:44-52.
6. Hermanson JW, Evans HE. The muscular system. In: Evans HE, ed. Miller’sAnatomy of the Dog. Philadelphia: WB Saunders; 1993:330.
7. Bardett JF. Diagnosis of shoulder instability in dogs and cats: a retrospectivestudy. JAAHA 1998;34:42-54.
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs550 CE
Eliminating movement of the biceps tendon through the intertubercular grooveis the goal of surgical treatment.

8. Davidson EB, Griffey SM, Vasseur PB, Shields SL. Histopathological, radi-ographic, and arthrographic comparison of the biceps tendon in normal dogsand dogs with biceps tenosynovitis. JAAHA 2000;36:522-530.
9. Brinker WO, Piermattei DL, Flo GL.The shoulder joint. In: Piermattei DL,Flo GL, eds. Handbook of Small Animal Orthopedics and Fracture Repair. 3rded. Philadelphia: WB Saunders; 1997:252-258.
10. Barthez PY, Morgan JP. Bicipital tenosynovitis in the dog—evaluation withpositive contrast arthrography. Vet Radiol Ultrasound 1993;34:325-330.
11. Esterline ML, Armburst L, Roush JK. A comparison of palpation guided andultrasound guided percutaneous biceps brachii tenotomy in dogs. Vet CompOrthop Traumatol 2005;18:135-139.
12. Wall CR, Taylor R. Arthroscopic biceps brachii tenotomy as a treatment forcanine bicipital tenosynovitis. JAAHA 2002;38:169-175.
13. Gilley RS, Wallace LJ, Hayden DW. Clinical and pathologic analyses ofbicipital tenosynovitis in dogs. Am J Vet Res 2002;63:402-407.
14. Muir P, Johnson KA. Supraspinatus and biceps brachii tendinopathy in dogs.J Small Anim Pract 1994;35:239-243.
15. LaHue TR, Brown SG, Roush JC,Ticer JW. Entrapment of joint mice in thebicipital tendon sheath as a sequela to osteochondritis dissecans of the proxi-mal humerus in dogs: a report of six cases. JAAHA 1988;24:99-105.
16. Boemo CM, Eaton-Wells RD. Medial displacement of the tendon of originof the biceps brachii muscle in 10 greyhounds. J Small Anim Pract1995;36:69-73.
17. Carb A, Halliwell WH. Nodular tenosynovitis of the flexor tendon in twodogs. JAAHA 1982;18:867-871.
18. Muir P, Goldsmid SE, Rothwell TL, Bellenger CR. Calcifying tendinopathyof the biceps brachii in a dog. JAVMA 1992;201:1747-1749.
19. Muir P. Physical examination of lame dogs. Compend Contin Educ Pract Vet1997;19(10):1149-1160.
20. Mckee M, Macias C. Orthopaedic conditions of the shoulder in the dog. InPract 2004;26(3):118-129.
21. Rivers B, Wallace L, Johnston GR. Biceps tenosynovitis in the dog: radi-ographic and sonographic findings. Vet Comp Orthop Traumatol 1992;5:51-57.
22. Todoroff JR. Biceps tendon disease and injuries: arthrographic and surgicalexperience [abstract]. Proc Sixth Annu Am Coll Vet Surg Symp 1996:107-109.
23. Lechleitner E, Mayrhofer E. Tendovaginopathien der Ursprungssehns desM. biceps brachii beim Hund. Röntgenologische, pathoanatomische undpathohistologische Befunde. Kleintierpraxis 1993;38:161-178.
24. Meier HT, Biller DS, Lora-Michiels M, Hoskinson JJ. Additional radi-ographic views of the thoracic limb in dogs. Compend Contin Educ Pract Vet2001;23(09):818-825.
25. Suter PF, Carb AV. Shoulder arthrography in dogs—radiographic anatomyand clinical application. J Small Anim Pract 1969;10:407-413.
26. Kramer M, Gerwing M, Sheppard C, Schimke E. Ultrasonography for thediagnosis of diseases of the tendon and tendon sheath of the biceps brachiimuscle. Vet Surg 2001;30:64-71.
27. Kramer M, Gerwing M, Sheppard C, et al. Sonography of the musculoskele-tal system in dogs and cats. Vet Radiol Ultrasound 1997;38(2):139-149.
28. Long CD, Nyland TG. Ultrasonographic evaluation of the canine shoulder.Vet Radiol Ultrasound 1999;40(4):372-379.
29. Jacobson JA. Musculoskeletal sonography and MRI. A role for both imagingmethods. Radiol Clin North Am 1999;37:713-735.
30. Samii VF, Long CD. Musculoskeletal system. In: Nyland TG, Mattoon JS,eds. Small Animal Diagnostic Ultrasound. 2nd ed. Philadelphia: WB Saunders;2002:267-284.
31. Holsworth IG, Schulz KS, Ingel K. Cadaveric evaluation of canine arthro-scopic bicipital tenotomy. Vet Comp Orthop Traumatol 2002;15:215-222.
32. Adamiak Z, Szalecki P. Treatment of bicipital tenosynovitis with double ten-odesis. J Small Anim Pract 2003;44:539-540.
33. Schaefer SL, Forrest LJ. Magnetic resonance imaging of the canine shoulder:an anatomic study. Vet Surg 2006;35:721-728.
34. Kenn W, Hufnagel P, Muller T, et al. Arthrography, ultrasound and MRI inrotator cuff lesions: a comparison of methods in partial lesions and smallcomplete ruptures. Rofo 2000;172(3):260-266.
35. Toyoda H, Ito Y, Nakao Y, et al. Evaluation of rotator cuff tears with mag-netic resonance arthrography. Clin Orthop Relat Res 2005;439:109-115.
36. Balasubramaniam P, Prathap K.The effect of injection of hydrocortisone intorabbit calcaneal tendons. J Bone Joint Surg 1972;54:729-734.
October 2008 COMPENDIUM
Bicipital Tenosynovitis in Dogs 551CE
37. Clark DM. Current concepts in the treatment of degenerative joint disease.Compend Contin Educ Pract Vet 1991;13:1439-1446.
38. Marcellin-Little DJ. Conservative treatment of shoulder conditions withphysical therapy. Proc Annu Am Coll Vet Surg Symp 2006:429-430.
39. Steiss JE, Levine D. Physical agent modalities. Vet Clin Small Anim2005;35:1317-1333.
40. Cook JL, Kenter K, Fox DB. Arthroscopic biceps tenodesis: technique andresults in six dogs. JAAHA 2005;41:121-127.
41. Sidaway BK, McLaughlin RM, Elder SH, et al. Role of the tendons of thebiceps brachii and infraspinatus muscles and the medial glenohumeral liga-ment in the maintenance of passive shoulder joint stability in dogs. Am J VetRes 2004;65(9):1216-1222.
42. Patton WC, McCluskey GM. Biceps tendinitis and subluxation. Clin SportsMed 2001;20:505-529.
43. Jerram RM, Herron MR. Scapular fractures in dogs. Compend Contin EducPract Vet 1998;20(11):1254-1260.
1. Which of the following statements regarding bicipi-tal tenosynovitis in dogs is false?a. Affected dogs are primarily medium sized to large.b. Male dogs are overrepresented.c. A history of a chronic, progressive or intermittent, mod-
erate to severe, weight-bearing lameness is oftenrecorded.
d. The disease typically affects middle-aged to older dogs.
2. Which of the following is not a reported cause ofbicipital tenosynovitis in dogs?a. mechanical injury secondary to calcifying tendinopathy
of the supraspinatus tendonb. mechanical injury secondary to glenohumeral instabilityc. infraspinatus muscle contractured. direct trauma
3. Which of the following statements regarding thebiceps retraction test is true?a. It may be performed with the dog standing or in lateral
recumbency.b. A positive result is pathognomonic for biceps tendon
disease.c. Direct comparison should be made with the contralat-
eral limb.d. a and c
4. Radiographic changes that may occur with bicipitaltenosynovitis includea. sclerosis of the intertubercular groove.
b. enthesiophyte formation at the supraglenoid tuberosity.c. mineralization of the biceps tendon.d. all of the above
5. The advantages of ultrasonographic assessment inthe diagnosis of bicipital tenosynovitis do notincludea. the ability to determine the exact location of the lesion
within the biceps tendon.b. the independence of the results from operator experi-
ence and skill.c. the ability to perform dynamic studies to assess abnor-
mal tendon gliding motion.d. its speed and noninvasiveness.
6. Medical treatment of canine bicipital tenosynovitisshould involve injection of methylprednisoloneacetate into the affected joint followed by ___weeks of strict confinement.a. 2 b. 3 c. 4 d. 6
7. Which of the following statements regarding theanatomy of the canine shoulder joint is false?a. The transverse humeral ligament spans the greater and
lesser tubercles of the humerus.b. The biceps brachii muscle acts to flex the elbow and the
shoulder joint.c. Medially and laterally, the joint capsule is irregularly
thickened to form the medial and lateral glenohumeralligaments, respectively.
d. The biceps tendon contributes to passive shoulder jointstability, particularly in the neutral and flexed positions.
8. Biceps tenodesisa. involves transferring the origin of the biceps tendon
from the supraglenoid tuberosity to the proximalhumerus.
b. typically produces good to excellent results regardlessof the duration of lameness.
c. may be performed via an arthroscopically assisted tech-nique.
d. all of the above
9. Which of the following statements regarding arthro-scopic biceps tenotomy is false?a. The procedure should only be reserved for acute cases
of bicipital tenosynovitis.b. The procedure is typically associated with fewer post-
operative complications than an open approach.c. The optimum location for tenotomy has not been
established.d. The procedure may be performed using a scalpel, a
motorized shaver, or bipolar radiofrequency.
10. What factors may influence an animal’s recoveryfrom biceps tendon surgery?a. obesity c. owner complianceb. physical rehabilitation d. all of the above
COMPENDIUM October 2008
Bicipital Tenosynovitis in Dogs552 CE
ARTICLE #1 CETESTThe Auburn University College of Veterinary Medicineapproves this article for 2 contact hours of continuingeducation credit.Subscribers may take individual CEtests or sign up for our annual CE program. Those whowish to apply this credit to fulfill state relicensure requirementsshould consult their respective state authorities regarding theapplicability of this program. CE subscribers can take CE testsonline and get real-time scores at CompendiumVet.com.
CE





























