Embed Size (px)
Citation preview

Radiation Therapy Workshop:Current knowledge on fraction size
Josep IsernHospital de la Santa Creu i Sant Pau, Barcelona

Current standard (outside prospective clinical trials):
1.8-2 Gy per fraction once-daily50-50.4Gy total doseIMRT highly preferred for most cases 5-6 weeks overall treatment time
FROM:NCIC SR-2
For preoperative RT

1.8-2 Gy per fraction once-daily50-50.4Gy total doseIMRT highly preferred for most cases 5-6 weeks overall treatment time
“several” weeks delay / rest
FROM:NCIC SR-2
1.8-2 Gy per fraction once-daily50-50.4Gy total doseIMRT highly preferred for most cases 5-6 weeks overall treatment time
“several” weeks delay / rest
definitive surgery
FROM:NCIC SR-2

1.8-2 Gy per fraction once-daily50-50.4Gy total doseIMRT highly preferred for most cases 5-6 weeks overall treatment time
“several” weeks delay / rest
definitive surgery
From AP data: boost ?¿?¿?
FROM:NCIC SR-2

If you want different results, do not do the same things

Current challenges in sarcoma radiation:
1. NO RADIATION

Current challenges in sarcoma radiation:
1. NO RADIATION2. FRACTION SIZE, DOSE and OVERALL TREATMENT

Current challenges in sarcoma radiation:
1. NO RADIATION2. FRACTION SIZE, DOSE and OVERALL TREATMENT3. COMBINED MODALITY REGIMENS
1. CONVENTIONAL CHEMOTHERAPY2. TARGETED AGENTS, IMMUNOLOGICAL …..

Current challenges in sarcoma radiation:
1. NO RADIATION2. FRACTION SIZE, DOSE and OVERALL TREATMENT3. COMBINED MODALITY REGIMENS
1. CONVENTIONAL CHEMOTHERAPY2. TARGETED AGENTS, IMMUNOLOGICAL …..

FRACTION SIZE

FRACTION SIZE,

Fraction size
.

Fraction size
However, no long-term follow up data on late functional sequelae are available from these 3 studies.
FRACTION SIZE

Fraction size
.
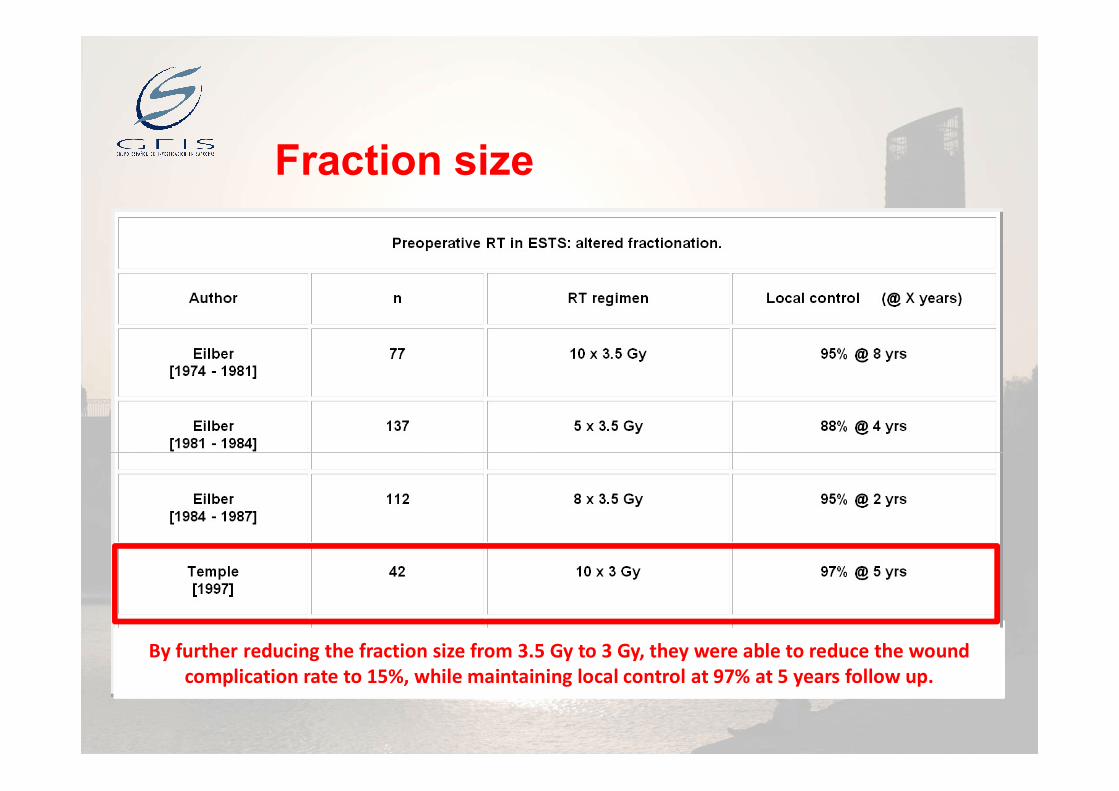
Fraction size
.By further reducing the fraction size from 3.5 Gy to 3 Gy, they were able to reduce the wound complication rate to 15%, while maintaining local control at 97% at 5 years follow up.
FRACTION SIZE, TOTAL DOSE and OVERALL TREATMENT
FRACTION SIZE, TOTAL DOSE and OVERALL TREATMENT

Fraction size

Fraction size
Phase II clinical trial: which may be on the lower level of acceptable local control.

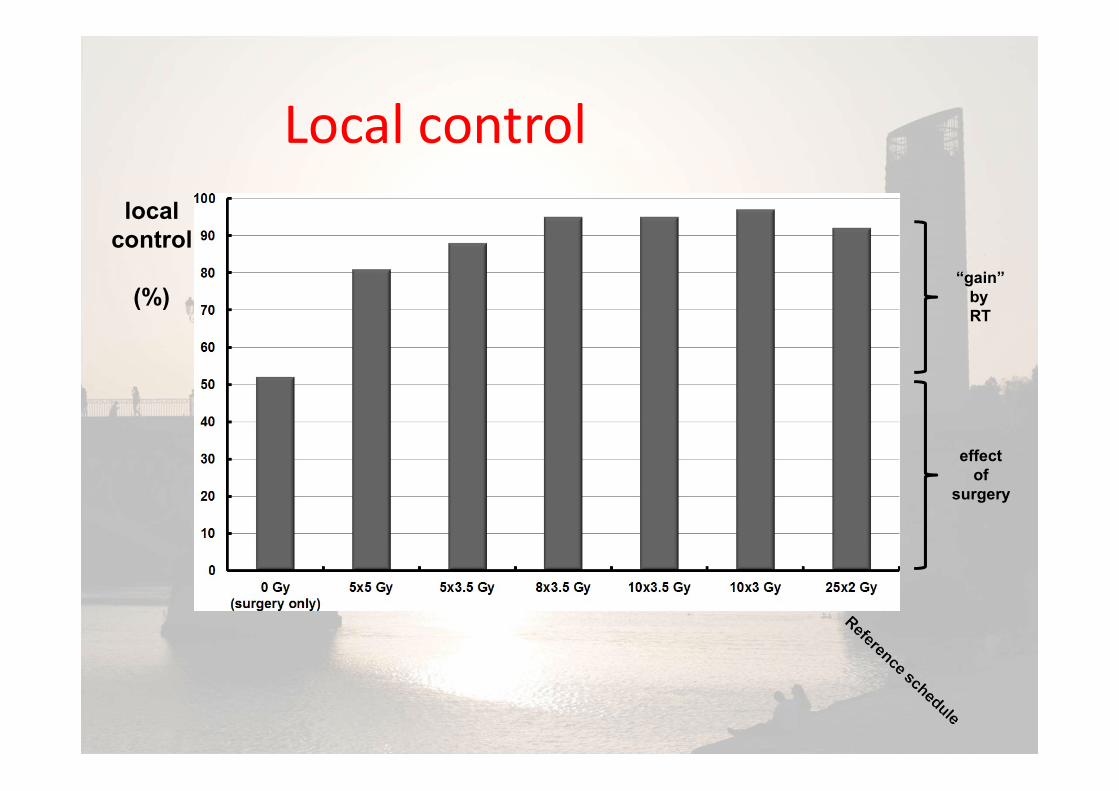
Local controllocal
control
(%)

Local controllocal
control
(%)

Local controllocal
control
(%)
effect of
surgery
Local controllocal
control
(%)
effect of
surgery
“gain” by RT

Local controllocal
control
(%)

Local controllocal
control
(%)

Local controllocal
control
(%)

:
SOME RADIOBIOLOGICAL CONSIDERATIONS ARISE FROM THE RESULTS OF THE STUDIES PREVIOUSLY EXPOSED:
*

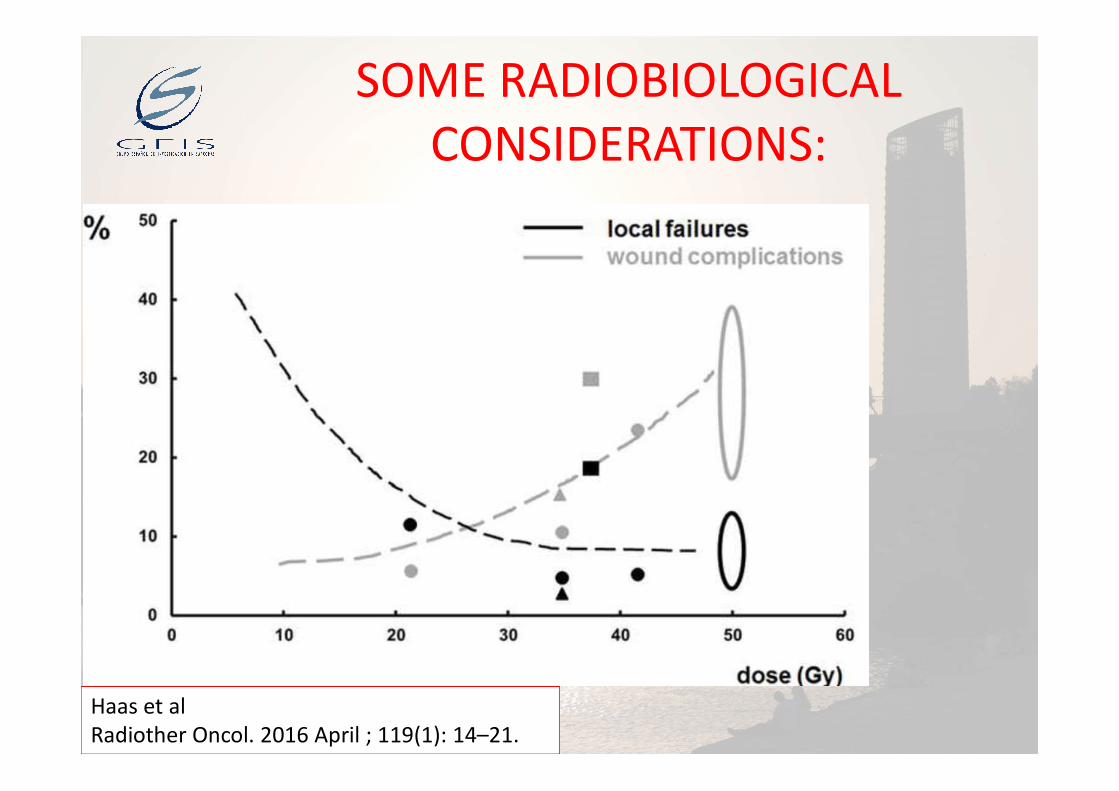
SOME RADIOBIOLOGICAL CONSIDERATIONS:
• Although the α/β ratio for the different sarcoma subtypes is unknown, it is possible that the value is below 10 Gy .
• One of the biological characteristics of sarcoma cells is their relatively low (-0.5 to 5.4) α/β ratio*. (most accepted 4 α/β ratio)
• This ratio, theoretically, may justify the use of larger-than-standard fractionation in order to achieve significant cell kill by RT.
*Joiner MC, Van der Kogel AJ. The linearquadratic approach to fractionation and calculation of isoeffect relationships. In: Steel GG, ed. Basic clinical radiobiology. New York,NY: Oxford University Press; 1997. pp. 106–12.

SOME RADIOBIOLOGICAL CONSIDERATIONS:
• BED DOSES.
*

SOME RADIOBIOLOGICAL CONSIDERATIONS:
Haas et alRadiother Oncol. 2016 April ; 119(1): 14–21.
.
A hypothetical local control probability curve, for simplification, calculated by: S = exp(− [αD + βD2]).
SOME RADIOBIOLOGICAL CONSIDERATIONS:
Haas et alRadiother Oncol. 2016 April ; 119(1): 14–21.
.

New approach....

• Ryan and colleagues reported on a series of 25 patients treated with the University of California Los Angeles:
• Hypofracctionated RT regimen (3.5Gy × 8) and dose-intense epirubicin and ifosfamide for three preoperative and three postoperative cycles

Results: • Local control: 88% (95% CI, 71–100%)• 95% pathologic necrosis rate of 40% (95% CI, 21–
59%).• The estimated 2-year rate for overall DFS was
62% (95%CI, 37–86%).• However, the regimen was too toxic, with 84%
predominantly hematologic grade 4 toxicities.• But, 20% wound complications actual rate who is
consistent with SR-2 Trial rates

• Investigators from the University of Calgary in Alberta, Canada, have published their experience with a “modified Eilber” protocol in 52 consecutive patients:
• Sequential intravenous doxorubicin for 3 days with 3 Gy × 10 (30 Gy) starting on the last day of chemotherapy.
Results
• They showed a 13.5% major wound complication rate and very good functional outcomes.
• No results about local control or survival


And adjuvant ?


• 21 elderly patients were treated with a short course of adjuvant RT
• Hypofractionated i regimen of 39–48 Gy in 13–16 fractions.( 3 G/fr)

Results:
• At a mean 26 months of follow-up.• Local control: 86 %• The hypofractionated radiation was well
tolerated with minimum long-term side effects.

CONCLUSIONS• Hypofractionated regimens delivered in eight
to 10 fractions, of 3-3,5 Gy, compared with conventional RT delivered in 25 fractions are the patient convenience of fewer treatments and associated reduced treatment cost.
• Although not yet proven, there are the potential appeals of increased treatment efficacy and/or decreased wound complication rates.







![Opening of Schools PLAN-Site Specific - Meadows$&.12:/('*(0(176 7KDQN \RX WR WKH IROORZLQJ 0DGLVRQ FRPPXQLW\ PHPEHUV DQG RXWVLGH RUJDQL]DWLRQV IRU WKHLU FRQWULEXWLRQ ZLWK WKLV SODQ](https://img.pdfslide.net/doc/110x75/6097e06fef8cc0084f2bb505/opening-of-schools-plan-site-specific-meadows-120176-7kdqn-rx-wr.jpg)

![RXU *UHHQ VHQVRUV WKDW DUH DYDLODEOH DW 0+] DQG …...wkh xvhu ri dq\ uhdglqjv wkdw duh rxwvlgh wkh dffhswdqfh udqjh iru wkdw sduwlfxodu surgxfw wkdw lv ehlqj prqlwruhg 7kh &06 skrqhv](https://img.pdfslide.net/doc/110x75/5e3a34f44852a145e44fbf40/rxu-uhhq-vhqvruv-wkdw-duh-dydlodeoh-dw-0-dqg-wkh-xvhu-ri-dq-uhdglqjv-wkdw.jpg)


![Tome 2 ACO SJLG Charté Vdef - Modernisation · 7udqvirupdwlrq qxppultxh ghvvlqrqv ohv ppwlhuv sxeolfv gh ghpdlq ewxgh survshfwlyh ± od vxlwh _ -xlq 3dupl fhv vhl]h idploohv gh](https://img.pdfslide.net/doc/110x75/5e8bf1ed01ce5705cc00fa5b/tome-2-aco-sjlg-chartf-vdef-modernisation-7udqvirupdwlrq-qxppultxh-ghvvlqrqv.jpg)

![Bold C1 Manual-EN-Web · +d]dugrxv :dvwh ± %dwwhu\ 'lvsrvdo :duqlqj 'r qrw wkurz dzd\ edwwhulhv zlwk xqfrqwuroohg gdlo\ zdvwh 7kh pdunlqj lq wklv pdqxdo lqglfdwhv wkdw wkh edwwhulhv](https://img.pdfslide.net/doc/110x75/5f9e6dc5e6c289383b065315/bold-c1-manual-en-web-ddugrxv-dvwh-dwwhu-lvsrvdo-duqlqj-r-qrw-wkurz-dzd.jpg)


![PBL-books Road-Trip text - Microsoft Publishertoolboxforteachers.s3.amazonaws.com/Core/PBL... · %ulhio\ vxppdul]h wkh surmhfw wkdw vwxghqwv zloo gr rxwvlgh ri vfkrro 5hphpehu lw](https://img.pdfslide.net/doc/110x75/5fb4e082e755193928497318/pbl-books-road-trip-text-microsoft-publishertoolboxforteacherss3-ulhio-vxppdulh.jpg)











