-
7/17/2019 Vaccine HIV
1/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
Vaccine xxx (2014) xxxxxx
Contents lists available at ScienceDirect
Vaccine
j ournal homepage: www.elsevier .com/ locate /vaccine
Synthetic HIV-1 matrix protein p17-based AT20-KLH
therapeuticimmunization in HIV-1-infected patients receiving
antiretroviraltreatment: A phase I safety and immunogenicity
study
Maria Luisa Iaria a,1, Simona Fiorentinia,1, Emanuele Foc b,
Sonia Zicari a, Cinzia Giagulli a,Q1Francesca Caccuri a, Daniela
Francisci c, Giovanni Di Perri d, Francesco Castelli b,Franco
Baldelli c, Arnaldo Caruso a,
a Department of Molecular and Translational Medicine, University
of Brescia, Brescia, Italyb Department of Clinical and
ExperimentalSciences,University of Brescia, Brescia, Italyc Section
of Infectious Diseases,Department of Experimental Medicine and
Biochemical Sciences, University of Perugia, 06132 Perugia, Italyd
Department of Medical Sciences, University of Turin, Turin,
Italy
a r t i c l e i n f o
Article history:
Received 9 July 2013
Received in revised form
16 December 2013
Accepted 19 December 2013
Available online xxx
Keywords:
Therapeutic vaccine
HIV-1 matrix protein p17
Peptide-based-immunotherapy
a b s t r a c t
Background: Therapeutic vaccination is a promising novel
approach to treat HIV-1 infected people by
boosting or redirecting immune system to neutralize critical
HIV-1 antigens whose biological effects are
relevant in the context ofviral pathogenesis. With the aim to
induce neutralizing antibodies to the matrix
protein p17 we have developed a peptide-based immunogen
(AT20-KLH) and evaluated its safety and
immunogenicity.
Methodology: Twenty four asymptomatic HAART-treated HIV-1+
patients were enrolled in a phase I clin-
ical study and were randomized to three groups: 2 groups were
treated with five IM injection (Arm A:
25g/inoculation; Arm B: 100g/inoculation) at day (D) D0, D28,
D56, D84 and D112; the control group
(Arm C) were not injected. Safety was assessed by monitoring
local and systemic adverse events (AEs),
recorded till D168. Evaluation ofimmunogenicity was by titering
antibodies at D0, D35, D56, D63, D84,
D91, D112, D140 and D168 using ELISA.Results: In all, 105 local
and systemic AEs were reported across the three groups. Most were
mild and
resolved without sequelae. Also the few unsolicited events,
deemed unrelated to the study vaccines,
caused no problems. No significant changes in the routine
laboratory parameters, CD4 T-cell count or
HIV-1 viremia were found. At the time ofenrollment 23 out of24
patients had no anti-AT20 antibodies,
whereas 11 exhibited anti-p17 antibodies. Irrespective ofthe
presence ofpreimmunization antibodies,
all subjects developed high titers ofanti-AT20 antibodies (GM
9775) in response to both AT20-KLH doses.
These antibodies were also capable ofrecognizing AT20 within the
p17 framework.
Conclusions: The AT20 peptide-based approach has allowed to
redirect HAART-treated patients humoral
responses toward a previously untargeted hotspot of functional
activity. Overall, the tested AT20-KLH
doses were safe and well tolerated, supporting further
exploration ofAT20-KLH as an HIV-1 therapeutic
vaccine candidate.
2013 Elsevier Ltd. All rights reserved.
1. Introduction
Highly active antiretroviral therapy (HAART), suppressing
the
HIV-1 replication and ameliorating the immunologic response,
has
Clinical trial identifier MED-AT20-001. Corresponding author at:
Departmentof Molecular and Translational Medicine,Q2
Section of Microbiology, Piazzale Spedali Civili, 1, 25123
Brescia, Italy.
Tel.: +39 030 394491; fax: +39 030395258.
E-mail address: [email protected] (A. Caruso).1 These authors
contributed equally to thework.
led to reduced morbidity and mortality [13]. However, a
discord-ant response on HAART with virologic suppression but
impaired
immunologic reconstitution may be observed; in these
individuals
clinical disease progression is greater than in those with a
com-
plete response [4] and is an independent risk factor for
mortality
[5]. Moreover, multiclass drug resistance is a clinically
important
issue in patients who cannot benefitfrom two fully activedrugs
[6].
Therefore, lifelong adherence, side and long-termeffects of
HAART,
immune reconstitution and multiclass drug-resistant issues,
along
with cost, point for the need of novel therapeutic options.
The aim of therapeutic vaccination in HIV-1-infected
individ-
uals is to induce or better direct immune responses that are
0264-410X/$ seefront matter 2013 Elsevier Ltd. All rights
reserved.
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
21
22
23
24
25
26
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://www.sciencedirect.com/science/journal/0264410Xhttp://www.elsevier.com/locate/vaccinemailto:[email protected]://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051mailto:[email protected]://www.elsevier.com/locate/vaccinehttp://www.sciencedirect.com/science/journal/0264410Xhttp://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051
-
7/17/2019 Vaccine HIV
2/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
2 M.L. Iaria et al. / Vaccinexxx (2014) xxxxxx
effective, either more potent than those induced by the
natural
infection.
HIV-1 protein triggers chronic immunological deregulation
[7]
and, among them, several investigators have hypothesized an
important role of the matrix protein p17 that exhibits
different
immunomodulatory properties which may be relevant in the
con-
text of viral pathogenesis [811]. In addition, p17 is the target
of
neutralizing Abs which correlate with slower progression to
AIDS
[1215]. Thefinding that p17is exported from infected cells [16],
is
detected in serum of HIV-1-infected patients [11] and
accumulates
in lymph nodes of even successfully HAART-treated patients
[17]
makes the mechanisms observed in vitro also possible in
vivo.
P17 activities are all mediated by its binding to specific
cellular
receptors [1820] through a functional epitope, shaped as a
par-
tially unfolded-helix located at the p17 NH2-terminal region
[8].
Mice immunized with a 20 amino acids (aa)-long synthetic
pep-
tide (AT20) representative of the p17 functional region, coupled
to
the carrier protein Keyhole Limpet Hemocyanin (KLH),
developed
p17-neutralizingAbs capableof blockingp17/p17receptor(s)
inter-
action and,consequently, all biological activities of the viral
protein
[8,21]. Further, being that AT20 resides within a highly
conserved
conformational epitope immunization it induces Abs capable
of
neutralizing the p17 proteins derived from divergent strains
dis-
playing critical mutations within AT20 [22]. On the basis of
thesepreclinical data, AT20-KLH was selected as the active agent to
per-
form a therapeutic phase I clinical trial in HIV-1-infected
patients.
2. Materials and methods
2.1. Study product
A contractor for the good manufacturing practice (GMP) was
identified in Italy (Areta International S.r.l., Gerenzano),
pro-
duced and released the AT20-KLH vaccine according to current
regulations. The released product was obtained conjugating
the
GMP-grade AT20 peptide (OPC, Germany) with the GMP-grade
KLH (Byosin, CA, USA) as carrier protein. The final product
con-taining the drug substance and the excipients was packaged
as
ready-to-use vials (25g and 100g) and stored at 53 C. The
immunogenic product was emulsified extemporaneously with the
adjuvant (GMP-grade Montanide ISA-51, Seppic, France) in a
1:1
ratio and administered intramuscularly deeply in the
usualregions.
2.2. Study design
The therapeutic phase I study (MED-AT20-001, EudraCT n.
2008-001465-29) was a multi-centre, randomized, dose
escalation
clinical trial whose primary endpoint was safety assessment
and
the secondary endpoint was immunogenicity.
Studywas conducted in HIV-1-infected, clinically
asymptomatic
individuals, in HAART therapy for at least 1 year prior to
vacci-nation, with undetectable (
-
7/17/2019 Vaccine HIV
3/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
M.L. Iaria et al. / Vaccinexxx (2014) xxxxxx 3
binding as compared to NH4SCN-untreated wells (M1, low avid-
ity; 1< M< 2 medium avidity; M2 high avidity).
2.4. Statistical analysis
Even if this was not a remit of MED-AT20-001 study, enroll-
ment of 24 subjects provides a sufficient number of observed
AEs
to describe the safety endpoint by number, percentage and
con-
fidence interval (95%CI). Difference in Ab levels was evaluated
by
MannWhitney test. To determine whether Ab AI increases
during
treatments, we used Wilcoxon test.
3. Results
3.1. Demographics
The 24 enrolled individuals were subdivided into three arms:
Arm A (n =9) patients treated with the AT20-KLH lower dose
(25g/inoculation); Arm B (n =9), patients receiving the
AT20-
KLH higher dose (100g/inoculation); and Arm C (n = 6),
control
untreated patients. The mean age standard deviation (SD) of
study participants was 43.569.42in Arm A,40.009.38in Arm B
and 39.8310.59 in ArmC and95.8% were Caucasian(Table 1S). At
the time of enrolment, CD4 count (meanSD) was 760138.5 in
Arm A,802147.5 inArmB and 698188.2 in ArmC and CD4/CD8
ratio (meanSD) was 1.280.6 in Arm A, 1.331.1 in ArmB and
0.990.4 in Arm C. No difference in baseline demographics was
present. All 24 patients have completed the study. The
according-
to-protocol analysis for the presence of anti-p17 and
anti-AT20Abs
included a screening phase (D-15), a treatment phase of 112
days,
consisting in five vaccination (D0, D28, D56, D84, D112), five
visits
after one week to each vaccination (V4, V5, V7, V9, V11), and
a
post-vaccination follow-up period (V12) ending 56 days after
last
vaccination (V13) (Table 1).
3.2. Safety
Safety was assessed by monitoring local and systemic AEs andwere
reported according to the MedDRA Dictionary. No significant
alteration of clinical and laboratory assessments were
observed.
The number of patients with at least one local and/or non-local
AE
related or not to vaccination is reported in Table 2. A total
num-
ber of 105 AEs were observed. Notably, most of the
registered
AEs were mild [Arm A: 70/75, 94% (95%CI: 87.498.6%); Arm B:
23/25, 92% (95%CI: 81.7102%); Arm C: 2/5, 40% (95%CI: 083%)]
and recovered(71/75,95%,95%CI: 8999% in ArmA and 23/25,92%,
95%CI: 81.7102% in Arm B) in all groups of participants (Table
2S).
Moderate AEs were rare, being only 6.7% in Arm A (5/75,
95%CI:
811.2%), 8% in Arm B (2/25, 95%CI: 018.5%) and 40% in Arm C
(2/5,95%CI: 083%). No serious AEsoccurred in anypatients
receiv-
ing the AT20-KLH vaccine, whereas a severe AE (Phosphokinase
increase) was observed in one Arm C patient. The most
frequentAEs categorywas General disordersand administration site
condi-
tions (43/105, 41%, 95%CI: 3149%) with more widespread
events
of pyrexia (13/43, 30%, 95%CI: 16.543.5%), swelling (10/43,
23%,
95%CI: 10.535.5%) and pain (9/43, 21%, 95%CI: 9.132.9%). Most
of
these AEs were showed by patients in Arm A (39/43, 90%,
95%CI:
8198%).Moreover,inArmAthemajorityofAEs(53/75,71%,95%CI:
6079%) was related with the treatment while, in Arm B, just
20%
of them (5/25, 95%CI: 4.435.6%) were treatment-related AEs.
As a further safety parameter, assessment of CD4+ T-cell
count
and viral load was performed. Data collected during the
treatment
phase and at D168 are consistent with a remarkable
immunologic
and virologic safety of the vaccination. No variation of CD4+
T-cell
countwas observed throughout the whole study duration
(Fig.2A).
A comparative analysis between the individual level of
CD4T-cells, T
able
1
T
rialschedule;13visits,5administrations,168daysduration/subject.
Visitnumber
V1
V2
V3
V4
V5
V6
V7
V8
V9
V10
V11
V12
V13
Trialtimelines(indicative)
D-15a
D0
D7
D28
D35
D56
D63
D84
D91
D112
D119
D140
D168
Timewindows(day)
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
[3days]
Vaccinationdose
X
X
X
X
X
Anti-AT20Abtiterandavidityindex(ELISA)
X
X
X
X
X
X
X
X
X
X
X
X
X
Anti-p17proteinAbtiter(ELISA)
X
X
X
X
X
X
X
X
X
X
X
X
X
Cellularimmunityanalysisb
X
X
X
X
X
X
X
X
X
Local&systemicevents/reactions
X
X
X
X
X
X
X
X
X
X
X
X
Trialphase
SCREENING
PRIMING
FOLLOW-UP
aWithin1monthto1weekpriortodesign.
bForpatientsenrolledinclinicalcentertoBrescia.
A
llpatientshaveundergonealltheproceduresde
scribedunlessexplicitlyexplained.
137
138
139
140
141
142
143
144
145
146
147
148
149
150
151
152
153
154
155
156
157
158
159
160
161
162
163
164
165
166
167
168
169
170
171
172
173
174
175
176
177
178
179
180
181
182
183
184
185
186
187
188
189
190
191
192
193
194
195
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051
-
7/17/2019 Vaccine HIV
4/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
4 M.L. Iaria et al. / Vaccinexxx (2014) xxxxxx
Table 2
Incidence of AEs.
A r m A (n = 9) Arm B (n = 9) Arm C (n = 6)
Any system 9(100.0%) 6(66.7%) 3(50%)
Blood and lymphatic system disorders 1(11.1%) 2(22.2%)
0(0.0%)
Lymphadenopathy 1(11.1%) 2(22.2%) 0(0.0%)
Ear and labirinth disorders 2(22.2%) 1(11.1%) 0(0.0%)
Vertigo 2(22.2%) 1(11.1%) 0(0.0%)
Gastrointestinal disorders 2(22.2%) 4(44.4%) 0(0.0%)
Diarrhea 2(22.2%) 2(22.2%) 0(0.0%)
Costipation 0(0.0%) 1(11.1%) 0(0.0%)
Gastric ulcer 0(0.0%) 1(11.1%) 0(0.0%)
Tongue disorders 1(11.1%) 0(0.0%) 0(0.0%)
Toothache 0(0.0%) 1(11.1%) 0(0.0%)
General disorders and administration site conditions 8(88.9%)
2(22.2%) 1(16.7%)
Pain 5(55.6%) 1(11.1%) 0(0.0%)
Pyrexia 4(44.4%) 1(11.1%) 1(16.7%)
Swelling 4(44.4%) 0(0.0%) 0(0.0%)
Malaise 2(22.2%) 0(0.0%) 0(0.0%)
Asthenia 0(0.0%) 1(11.1%) 0(0.0%)
Influenza-like illness 1(11.1%) 0(0.0%) 0(0.0%)
Injection site pain 1(11.1%) 0(0.0%) 0(0.0%)
Nodule 1(11.1%) 0(0.0%) 0(0.0%)
Tenderness 1(11.1%) 0(0.0%) 0(0.0%)
Infections and infestations 6(66.7%) 4(44.4%) 1(16.7%)
Influenza 3(33.3%) 1(11.1%) 1(16.7%)
Nasopharyngitis 1(11.1%) 2(22.2%) 0(0.0%)
Pharingitis 1(11.1%) 0(0.0%) 1(16.7%)
Fungal infection 0(0.0%) 1(11.1%) 0(0.0%)
Gastroenteritis 1(11.1%) 0(0.0%) 0(0.0%)
Helicobacter infection 0(0.0%) 1(11.1%) 0(0.0%)
Oral Herpes 1(11.1%) 0(0.0%) 0(0.0%)
Investigations 0(0.0%) 1(11.1%) 1(16.7%)
Blood creatinine phosphokinase increase 0(0.0%) 0(0.0%)
1(16.7%)
HIV test positive 0(0.0%) 1(11.1%) 0(0.0%)
Musculoskeletal and connective tissue disorders 1(11.1%)
2(22.2%) 0(0.0%)
Arthralgia 1(11.1%) 1(11.1%) 0(0.0%)
Back pain 0(0.0%) 1(11.1%) 0(0.0%)
Nervous system disorders 1(11.1%) 2(22.2%) 1(16.7%)
Headache 1(11.1%) 2(22.2%) 0(0.0%)Sciatica 0(0.0%) 0(0.0%)
1(16.7%)
Psychiatric disorders 0(0.0%) 1(11.1%) 0(0.0%)
Insomnia 0(0.0%) 1(11.1%) 0(0.0%)
Respiratory, thoracic and mediastinal disorders 2(22.2%) 0(0.0%)
0(0.0%)
Cough 2(22.2%) 0(0.0%) 0(0.0%)
Oropharingeal pain 1(11.1%) 0(0.0%) 0(0.0%)
Skin and subcutaneous tissue disorders 3(33.3%) 0(0.0%)
0(0.0%)
Pruritus 3(33.3%) 0(0.0%) 0(0.0%)
Erithema 1(11.1%) 0(0.0%) 0(0.0%)
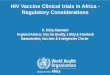
measured at D-15 and D168, confirmed that they did not
signifi-
cantly differ in 100% of subjects enrolled (Fig. 2B).
Preservation of
circulating CD4+ T cells was mirrored by the absence of
significant
plasma viremia rebounds.Based on data obtained, after a careful
evaluation of the AEs
IDSMB qualified the AT20-KLH vaccine candidate as safe and
well
toleratedboth locally and systemically.A report has
beendeposited
to the Italian Regulatory Agencies.
3.3. Immunogenicity
Serum samples were analyzed at the Brescia University core
laboratory. In agreement with previous observation, showing
that
during the natural course of HIV-1 infection the occurrence of
Ab
responseto AT20is rareand eventually ata verylowtiter
[7,24],
most patients (23/24, 95.9%, 95%CI: 94.895%) had not
detectable
anti-AT20 Abs at the time of enrolment. The only patient
posi-
tive for AT20 Abs (Ab titer: 100) was randomly enrolled in Arm
A.
Eleven out of 24 patients (45.8%, 95%CI: 25.464.6%) (5
random-
ized in Arm A, 3 in Arm B and 3 in Arm C) exhibiting p17 Abs
with titers ranging from 100 to 12,800 (Ab GMT = 852.4).
Subjects
immunized with AT20-KLH developed high titers of anti-AT20
Abscompared to untreatedpatients (p < 0.001). As a consequence
of the
rising level of anti-AT20 Abs, difference in sera reactivity
were no
more observed when patients samples were tested in ELISA
plates
coated withthe AT20peptide or withthe entire
recombinantnative
p17 protein (Fig. 3A). These results demonstrate that the Abs
gen-
erated to the synthetic AT20 peptide are capable to recognize
the
epitope within the viral protein framework. Moreover,sera
derived
from patients immunized with AT20-KLH were capable to
displace
thebinding between p17and p17receptor(s)whereas sera derived
from patients belonging to the control Arm did not (Figure
1S).
The clinical trial was designed as a dose escalation trial.
There-
fore, we evaluated if one of the two doses tested have elicited
a
better immune response. As shown in Fig. 4A, four weeks
after
the first dose of vaccine (D28), the rate of seroconversion to
AT20
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
2
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051
-
7/17/2019 Vaccine HIV
5/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
M.L. Iaria et al. / Vaccinexxx (2014) xxxxxx 5
Fig. 2. Profileof CD4+ T cell count along clinical trial. (A)
Diagrams representmean
(SD) absolute CD4+ T cell count of patients enrolled in Arm A,
Arm B and Arm C.
Datawere collectedat theindicatedvisits. Arrows indicatetime
foreach vaccination.
(B) Comparison between CD4+ T cell number, as measured in each
patient, at the
screening visit (V1) and during the follow up period (V13).
Pvalue was calculated
by MannWhitney test.
was 55% in Arm A (5/9) and 33% (3/9) in Arm B.
Seroconvertion
in 100% of vaccinated subjects was occurred from the second
dose
onward. Moreover, as soon as four weeks after the second dose
ofvaccine(D56), 22%of vaccinated persons (4/18; 3 belongingto
Arm
A andonebelonging toArm B)reachedtheiranti-AT20Ab titerpeak
(12,800). At D84, four weeks after the third vaccination, a
further
enhancement of Ab titers in 12 patients was observed (5
belong-
ing to Arm A and 7 belonging to Arm B). At this time 55% (n =
5)
of Arm A patients reached the highest titer (12,800) of
anti-AT20
IgG, whereas only 22% (n = 2) of Arm B subjects reached their
anti-
AT20 Ab peak (Ab titer 6400, n = 1; Ab titer 12,800, n = 1 ) (p
= 0.09).
At D112, in Arm A two patients (22.2%) had not reached yet
their
AT20Ab peakand showedan Abtiter of6400 (n =1)and800(n =1).
At this timepoint, 5 patients in Arm B showed a further
increment
in anti-AT20 Ab titer whereas three of them reached their Ab
peak
(Ab titer 12,800, n = 2; Ab titer 6400, n = 1). By the end of
vaccina-
tion, 100% of treated patients reached a plateau of anti-AT20
Abtiter that was maintained till the follow-up observation time
point.
The highest titer observed following this immunization
protocol
(12,800) was reached by 78% (n =7) patients from Arm A and
55%
(n = 5)patients fromArm B (Fig. 4A). However, as shown in Fig.
4B,
the anti-AT20 Abs GMT among vaccinated persons belonging to
Arm A and Arm B did not significantly differ at any time point.
To
investigate the possibility that AT20-specific memory B-cells
could
be recruited in response to AT20-KLH vaccination, anti-AT20
IgG
avidity was also evaluated (Fig. 4C). To this purpose, anti-AT20
IgG
AI was calculated when Abs first appeared andthe
follow-upphase
(D168). Abs with high avidity at the first appearance were
devel-
oped by 67% (n =6) of patients inArm A and 33%(n = 3) of
patients
in Arm B. At D168 all these patients showed Abs with an
avidity
grade 3. The remaining patients population (n = 9) showed
AT20
IgG at low(n = 2 in Arm A; n =3 inArm B)or mediumavidity (n =
1
in Arm A; n =3 in Arm B) when Abs were first detected.
Avidity
increased over time in 77% of these subjects (n = 7) reaching a
high
AI. Among them, 2 patients in Arm A and 4 patients in Arm B
dis-
played an AI> 3. Only two subjects (n = 1 in Arm A and n =1
in Arm
B) displayed anti-AT20 IgG at a medium AI.
In summary, these results attest for the capability of AT20-
KLH vaccine to elicit a de novo anti-AT20 Ab synthesis, as
well
as to trigger anti-AT20 Ab production from a pre-existing pool
of
B lymphocytes by retrieving an immunological memory. In both
cases, AIs reached at the follow-up phase was significantly
higher
(p =0.01inArmA,p =0.008inArmB)thantheAIobservedwhenAbs
first appeared. Furthermore, when anti-AT20 Abs were
produced
through a de novo induction, 77% of vaccinated patients (n
=7)were
enabled to develop anti-AT20 Abs with high avidity by the end
of
the study.
4. Discussion
This is a first-in-man evaluation of a synthetically
manufactured
vaccine consisting of a structurally conserved HIV-1 matrix
protein
region (AT20),functionallyinvolved in p17/p17receptor(s)
interac-
tion [8]. Being an exploratory study, patients received two
differentAT20-KLH doses. Notably, none of them caused major AEs and
the
most common mild AE was a dose-independent pain at the site
of injection, consistent with the presence of adjuvant in the
for-
mulation. Preservation of CD4+ T-cell number and the absence
of
plasma viremia rebounds attest for a remarkable immunologic
and
virologicsafety of the vaccine preparation.These results prove
that
AT20-KLH is safe and well tolerated.
All patients, except one, had no detectable anti-AT20 Abs at
the
time of enrolment. This is in line with previous studies
showing
that Abs to p17 NH2-terminal region are less common than
those
recognizingother p17epitopes,and thatthese Abs
disappearsignif-
icantly before than AIDS-related reduction in Ab titer occurs
[24].
All enrolled subjects immunized with AT20-KLH developed high
titers of anti-AT20 Abs. Such an immunogenic activity is
uncom-mon amongst HIV-1 vaccines, since results recorded up to
date
never reached 100%, even in HIV-1-seronegative volunteers
[25].
This finding points to a strong immunogenicity of the
AT20-KLH
molecule from one side, confirming the capability of HAART
to
fully restore patients humoral response on the other side.
Phe-
notypic and functional B cell abnormalities commonly observed
in
untreated HIV-1-infected patients are indeed completely
restored
by HAART [26].
Ourstudy have shown that Abs generated to the syntheticAT20
peptide recognize the epitope residing within the native p17
con-
firming that AT20, as immunogenic peptide, is presented in
vivo
in a conformation that mimics the structure it acquires within
the
viral protein. These data arestrengthenby theobservationthat
Abs
developed by AT20-KLH-vaccinated patients are able to
neutralizep17/p17receptor(s) interaction andp17 biological
activity[27]. The
latter results are in agreement with our preclinical data [21]
show-
ing that Abs elicited in mice by AT20-KLH injection possess
potent
p17 neutralizing activity.
The finding that Abs elicited by AT20-KLH recognizes both
lin-
ear and conformational epitopes on the viral protein [22],
makes
possible neutralization of p17 with major amino acid
substitutions
within this epitope. This opens to the opportunity of
evaluating
the efficacy of the peptide-based vaccine in patients infected
with
HIV-1 strains displaying divergent p17 proteins. Interestingly,
by
evaluating anti-AT20 Abs AI, we were able to discriminate de
novo
patients from individuals with a pre-existing pool of B-cells
that
can be triggered by AT20-KLH to recover a specific
immunological
memory. It will be interesting to investigate if
differentmodality of
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
249
250
251
252
253
254
255
256
257
258
259
260
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051
-
7/17/2019 Vaccine HIV
6/7
Please cite this article in press as: Iaria ML, et al. Synthetic
HIV-1 matrix protein p17-based AT20-KLH therapeutic immuniza-
tion in HIV-1-infected patients receiving antiretroviral
treatment: A phase I safety and immunogenicity study. Vaccine
(2014),
http://dx.doi.org/10.1016/j.vaccine.2013.12.051
ARTICLE IN PRESSGModel
JVAC 14964 17
6 M.L. Iaria et al. / Vaccinexxx (2014) xxxxxx
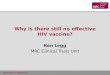
Fig. 3. Profile of the Ab response to AT20-KLH vaccination. (A)
Level of anti-AT20 Abs were evaluated by ELISA, using platescoated
with unconjugated AT20 peptide (filled
signs) or with the entire recombinant p17 protein (empty signs).
Circles represents data obtained from vaccine-treated patients,
squares are for untreated control patients.
Data are represented as Ab geometric mean (GM) titers(log
scale). Arrows indicate time for each vaccination (0, 28, 56, 84,
112 days).
Fig. 4. Quality of AT20-KLH-induced Ab response. (A) Diagram
represents titers of anti-AT20-Abs evaluated at the indicated day
of observation. Vaccinated subjects were
grouped by dose ofAT20-KLH received (Arm A, empty circles; ArmB,
filled circles).(B) Trend ofanti-AT20 Absincreasealong
theclinicaltrial. (C)Anti-AT20Abs avidity grade
(AI) in each AT20-KLH treated patient assessed at the time of
first anti-AT20 Ab appearance and at the follow-up phase (V13).
Each patient is represented with a different
symbol. If AI1, anti-AT20 IgG wereconsidered at low avidity; if
1< AI< 2, at medium avidity and if AI2 at high avidity.
Pvalue was calculated with Wilcoxon test.
Ab development (natural vs. induced) may reflect a different
capa-
bility of Abs to recognize linear and conformational epitopes
and
therefore, a differentresponseof patientsto
thetherapeuticvaccine
in terms of efficacy.
All data indicate the achievement of both the primary
(safety)
and the secondary (immunogenicity) endpoints of the study,
high-
lighting the effectiveness of our approach of using an
immunogen
incorporating a selected determinant in order to induce
potent
and specific Abs against a crucial p17 functional epitope,
rather
than the whole virus or viral subunits, which are known to
elicit
adverse immunosuppressive, immunoenhancing and autoimmune
responses [2830].
In conclusion, using a peptide-based approach for
therapeutic
vaccinationit has beenpossibleto redirect
HAART-treatedpatients
humoral responses toward a previously untargeted hotspot of
functional activity. The AT20-KLH-based clinical trial provides
an
incentive to expand present efforts in therapeutic
immunizations,
and to boost international partnerships with the aim to
speedy
achieve effective immune-based interventions for the
long-lasting
repair of HIV-1-related immune defects.
Acknowledgements
The therapeutic phase I study (MED-AT20-001, EudraCT n.
2008-001465-29) was a multi-centre, randomized, dose
escalation
clinical trial fully sponsored by Medestea Research &
Production
S.p.A., a privately owned biopharmaceutical company.
3
3
3
3
3
3
3
3
3
3
3
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1016/j.vaccine.2013.12.051
-
7/17/2019 Vaccine HIV
7/7
http://localhost/var/www/apps/conversion/tmp/scratch_4/dx.doi.org/10.1155/2012/829584http://dx.doi.org/10.1016/j.vaccine.2013.12.051http://dx.doi.org/10.1016/j.vaccine.2013.12.051