Embed Size (px)
Citation preview
Isabel Esteves Unidade de Infecciologia Pediátrica
Departamento de Pediatria, Hospital de Santa Maria – CHLN, EPE Directora: Maria do Céu Machado
Lisbon, Portugal
VACCINE-PREVENTABLE OUTBREAKS IN PORTUGAL:
HEPATITIS A AND MEASLES
May 12-13th, 2017 EAP SPRING MEETING
FARO, PORTUGAL

OUTBREAKS IN PORTUGAL
HEPATITISA§ Introduc*on–thevirusandthedisease§ Na*onalandeuropeanprevalencedata§ OutbreakinPortugalandEUcountries2016-2017§ ManagementbyNa*onalHealthAuthori*es
§ DiscussionMEASLES§ Introduc*on–thevirusandthedisease§ Na*onalandeuropeanprevalencedata§ OutbreakinPortugal§ ManagementbyNa*onalHealthAuthori*es
§ Discussion
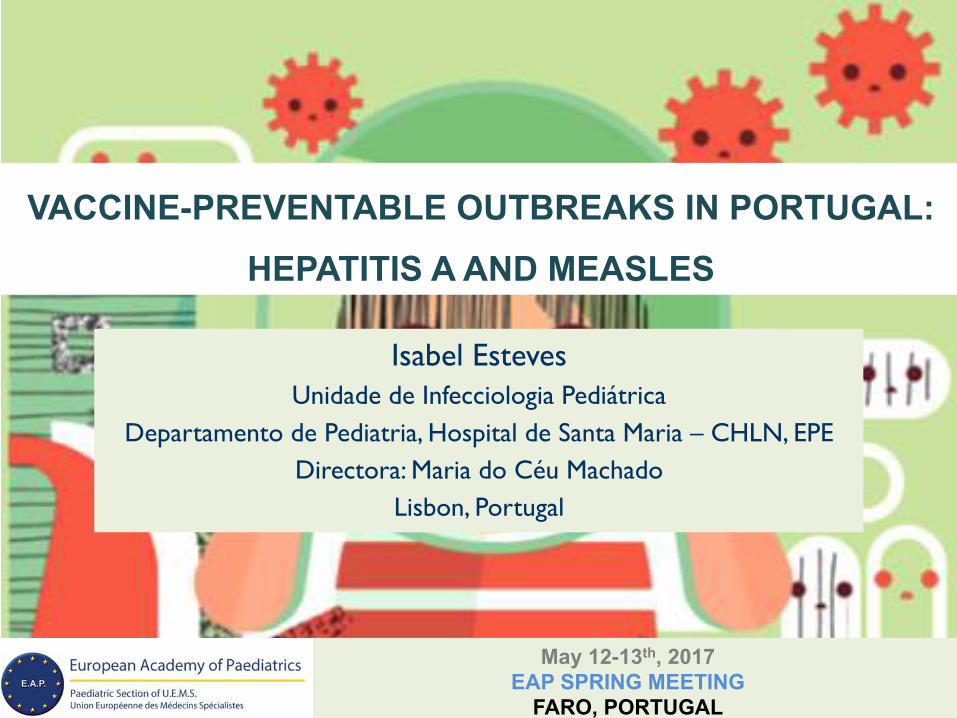
hGp://wwwnc.cdc.gov/travel/yellowbook/2012/
HEPATITIS A – GLOBAL SEROPREVALENCE
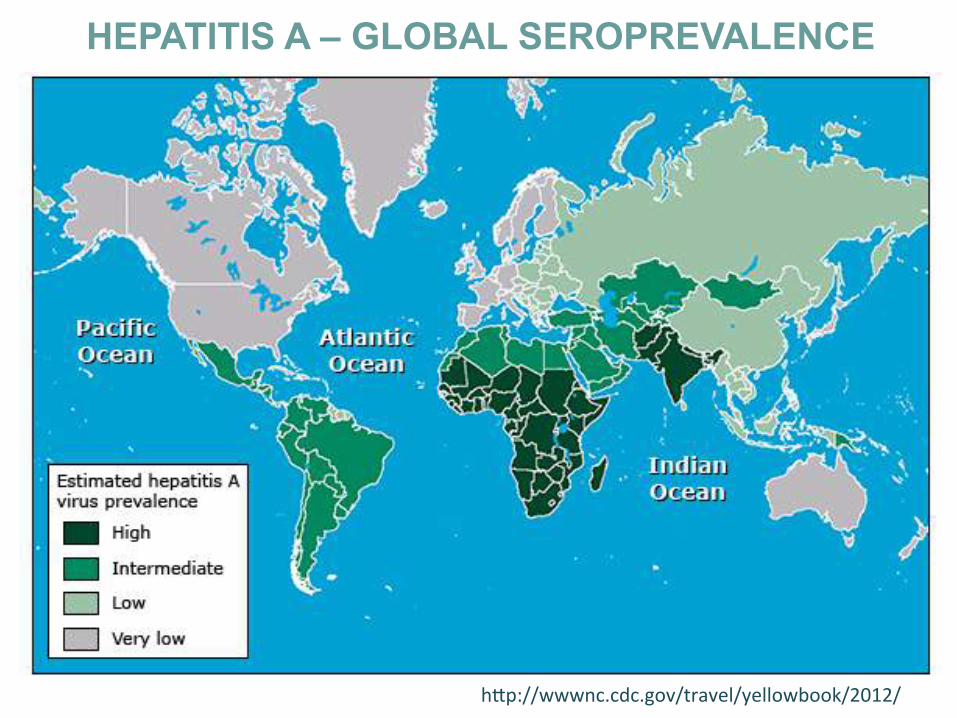
HEPATITIS A
§ Non-envelopedRNAhepatovirus(Picornaviridae)-1975§ 1serotype,severalgenotypes§ Resistanttoinac*va*on(Temp.60°cor≤4°c,eter,acid,anionic
substances)
VaughanGetal,InfectGenetEvol2014,227-43PintoRM,FutureMicrobiol2012,331-46
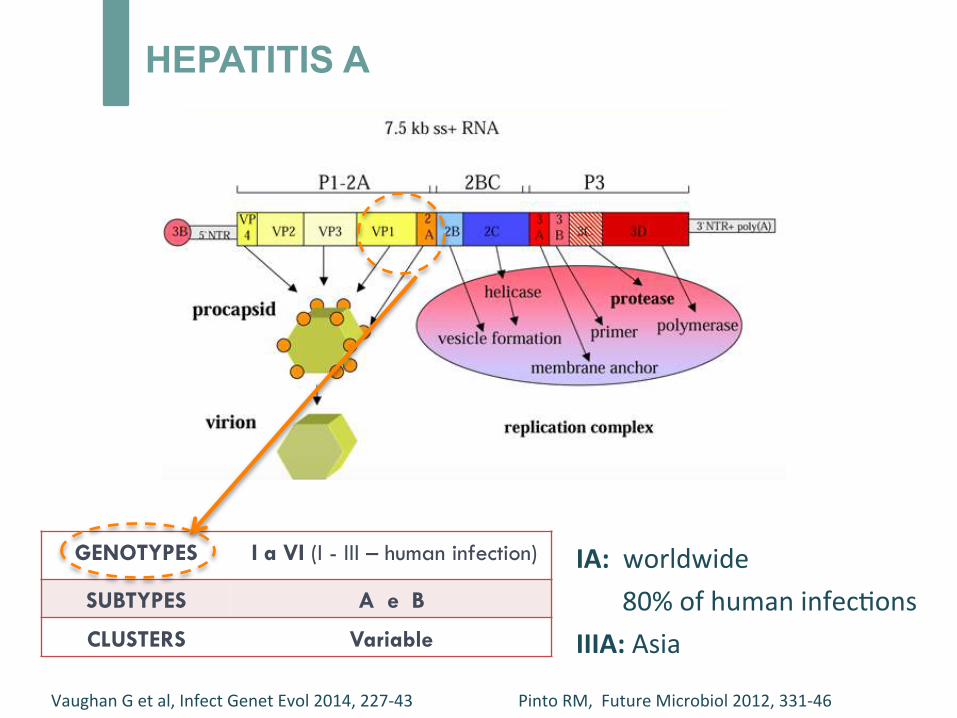
HEPATITIS A
GENOTYPES I a VI (I - III – human infection)
SUBTYPES A e B
CLUSTERS Variable
IA:worldwide80%ofhumaninfec*onsIIIA:Asia
VaughanGetal,InfectGenetEvol2014,227-43PintoRM,FutureMicrobiol2012,331-46
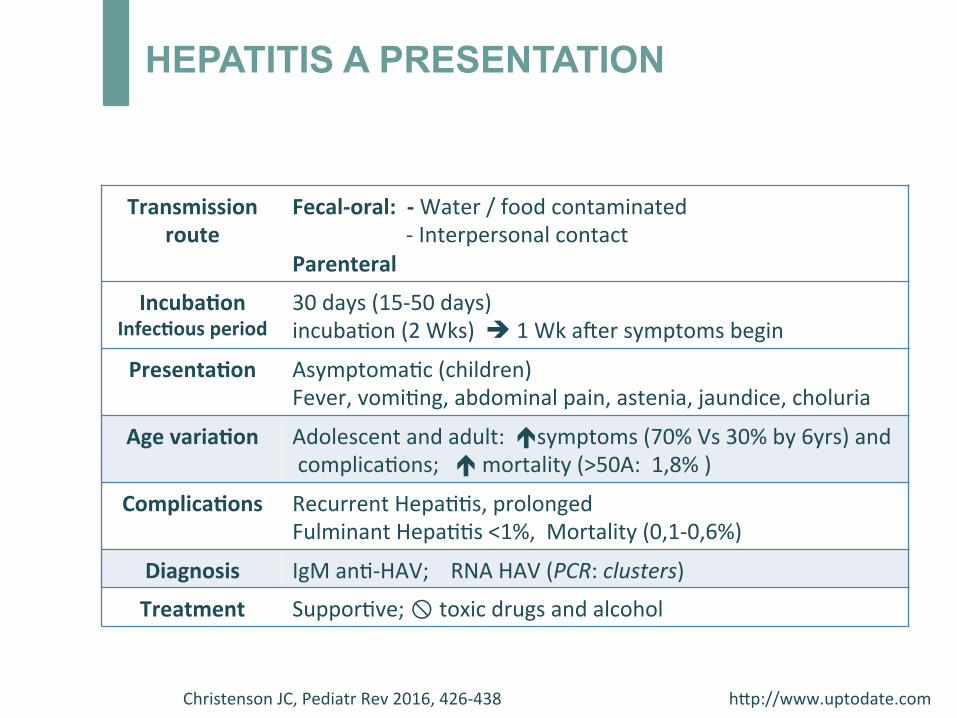
Transmissionroute
Fecal-oral:-Water/foodcontaminated-InterpersonalcontactParenteral
Incuba;onInfec;ousperiod
30days(15-50days)incuba*on(2Wks)è1Wka^ersymptomsbegin
Presenta;on Asymptoma*c(children)Fever,vomi*ng,abdominalpain,astenia,jaundice,choluria
Agevaria;on Adolescentandadult:ésymptoms(70%Vs30%by6yrs)andcomplica*ons;émortality(>50A:1,8%)
Complica;ons RecurrentHepa**s,prolongedFulminantHepa**s<1%,Mortality(0,1-0,6%)
Diagnosis IgMan*-HAV;RNAHAV(PCR:clusters)
Treatment Suppor*ve;!toxicdrugsandalcohol
ChristensonJC,PediatrRev2016,426-438hGp://www.uptodate.com
HEPATITIS A PRESENTATION
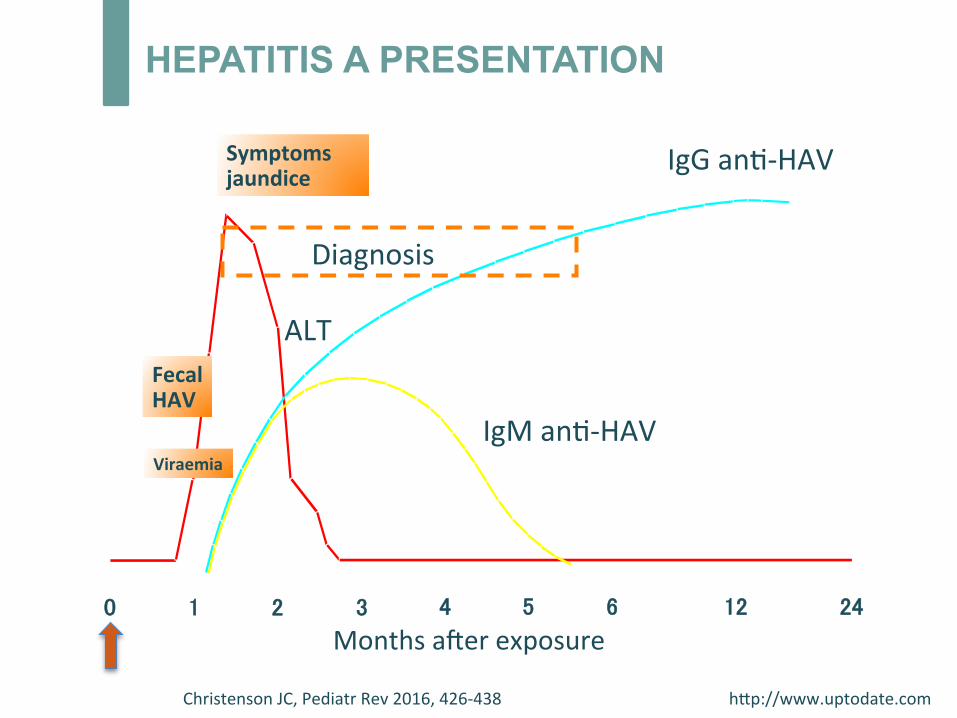
HEPATITIS A PRESENTATION
FecalHAV
Symptomsjaundice
0 1 2 3 4 5 6 12 24
IgGan*-HAV
ALT
IgMan*-HAV
Monthsa^erexposure
Viraemia
Diagnosis
ChristensonJC,PediatrRev2016,426-438hGp://www.uptodate.com
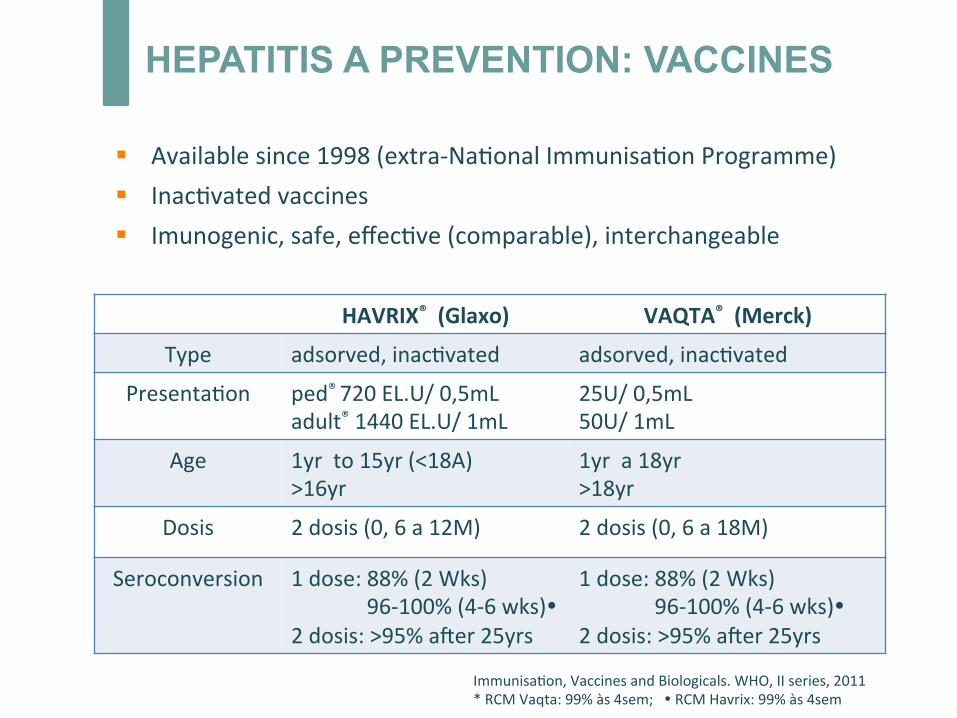
§ Availablesince1998(extra-Na*onalImmunisa*onProgramme)§ Inac*vatedvaccines§ Imunogenic,safe,effec*ve(comparable),interchangeable
HAVRIX®(Glaxo) VAQTA®(Merck)
Type adsorved,inac*vated adsorved,inac*vated
Presenta*on ped®720EL.U/0,5mLadult®1440EL.U/1mL
25U/0,5mL50U/1mL
Age 1yrto15yr(<18A)>16yr
1yra18yr>18yr
Dosis 2dosis(0,6a12M) 2dosis(0,6a18M)
Seroconversion 1dose:88%(2Wks)96-100%(4-6wks)�2dosis:>95%a^er25yrs
1dose:88%(2Wks)96-100%(4-6wks)�2dosis:>95%a^er25yrs
Immunisa*on,VaccinesandBiologicals.WHO,IIseries,2011*RCMVaqta:99%às4sem;�RCMHavrix:99%às4sem
HEPATITIS A PREVENTION: VACCINES
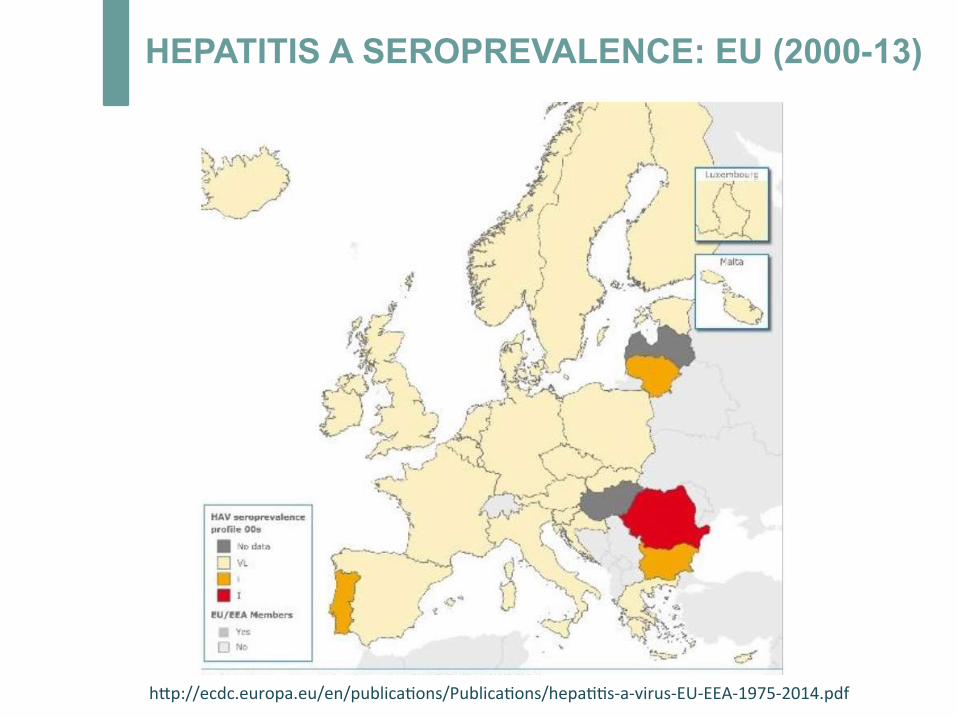
hGp://ecdc.europa.eu/en/publica*ons/Publica*ons/hepa**s-a-virus-EU-EEA-1975-2014.pdf
HEPATITIS A SEROPREVALENCE: EU (2000-13)
hGp://ecdc.europa.eu/EU-EEA-1975-2014
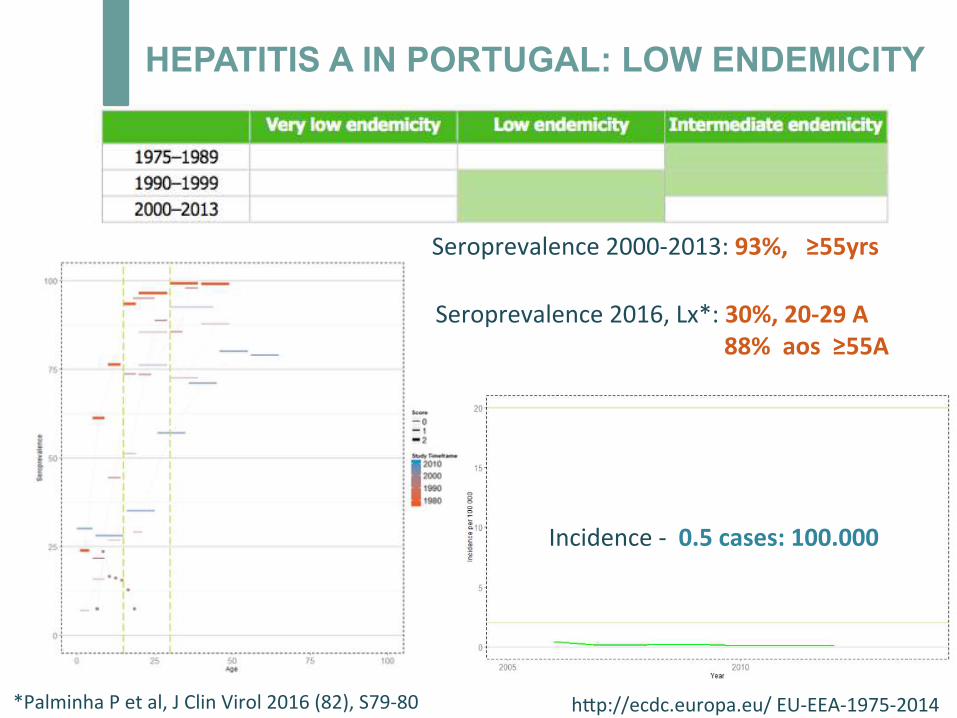
Incidence-0.5cases:100.000
Seroprevalence2000-2013:93%,≥55yrs
Seroprevalence2016,Lx*:30%,20-29A88%aos≥55A
*PalminhaPetal,JClinVirol2016(82),S79-80
HEPATITIS A IN PORTUGAL: LOW ENDEMICITY
hGp://ecdc.europa.eu/EU-EEA-1975-2014
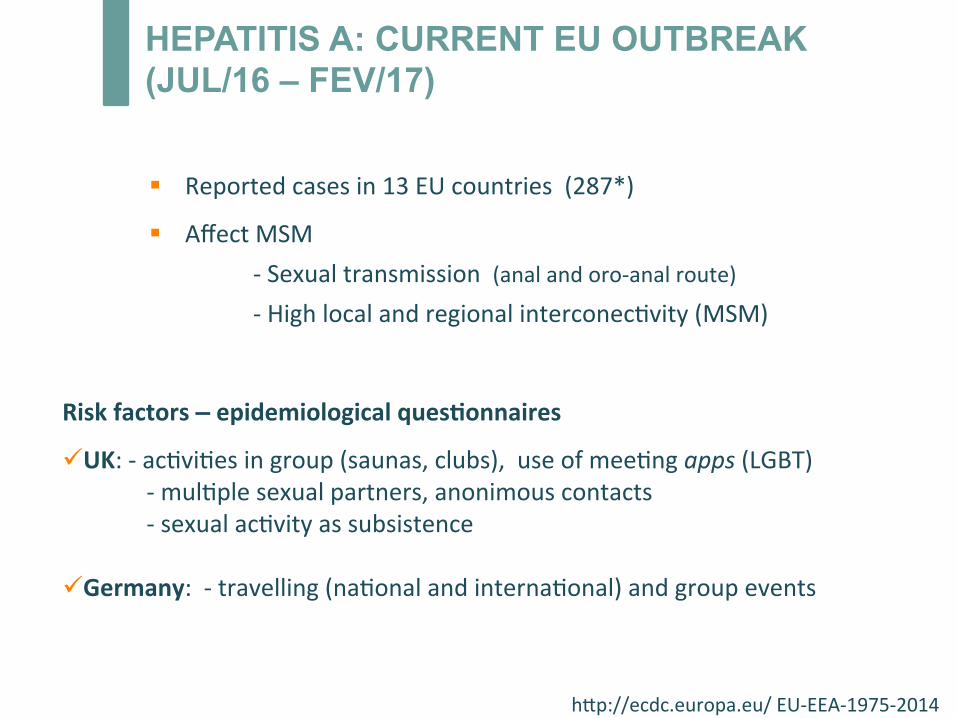
HEPATITIS A: CURRENT EU OUTBREAK (JUL/16 – FEV/17)
§ Reportedcasesin13EUcountries(287*)
§ AffectMSM-Sexualtransmission(analandoro-analroute)-Highlocalandregionalinterconec*vity(MSM)
Riskfactors–epidemiologicalques;onnaires
ü UK:-ac*vi*esingroup(saunas,clubs),useofmee*ngapps(LGBT)-mul*plesexualpartners,anonimouscontacts-sexualac*vityassubsistenceü Germany:-travelling(na*onalandinterna*onal)andgroupevents
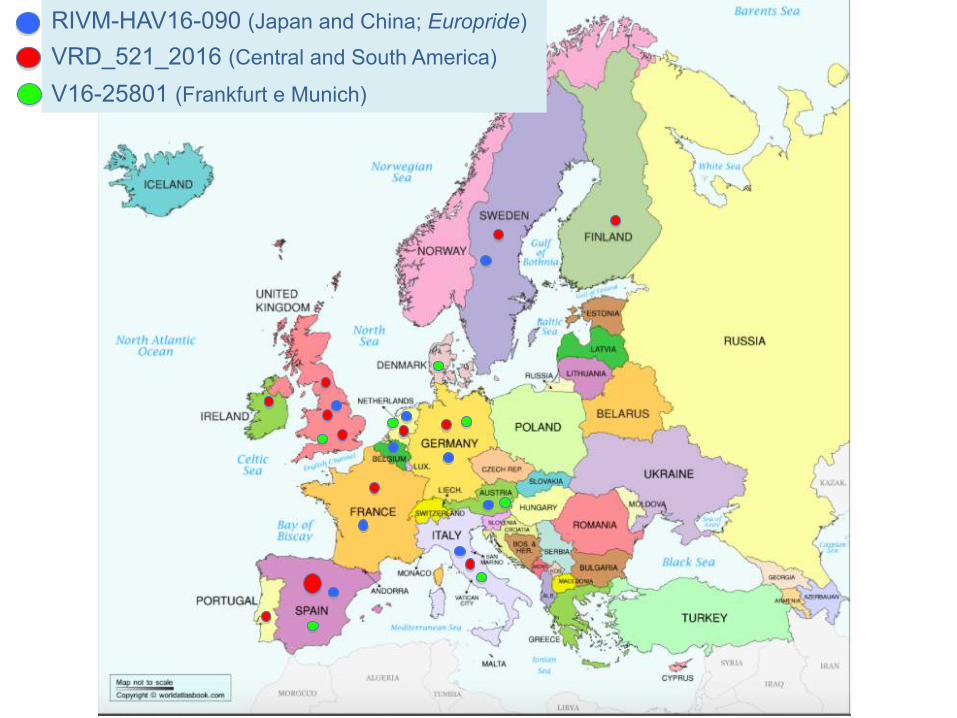
RIVM-HAV16-090 (Japan and China; Europride)
VRD_521_2016 (Central and South America)
V16-25801 (Frankfurt e Munich)
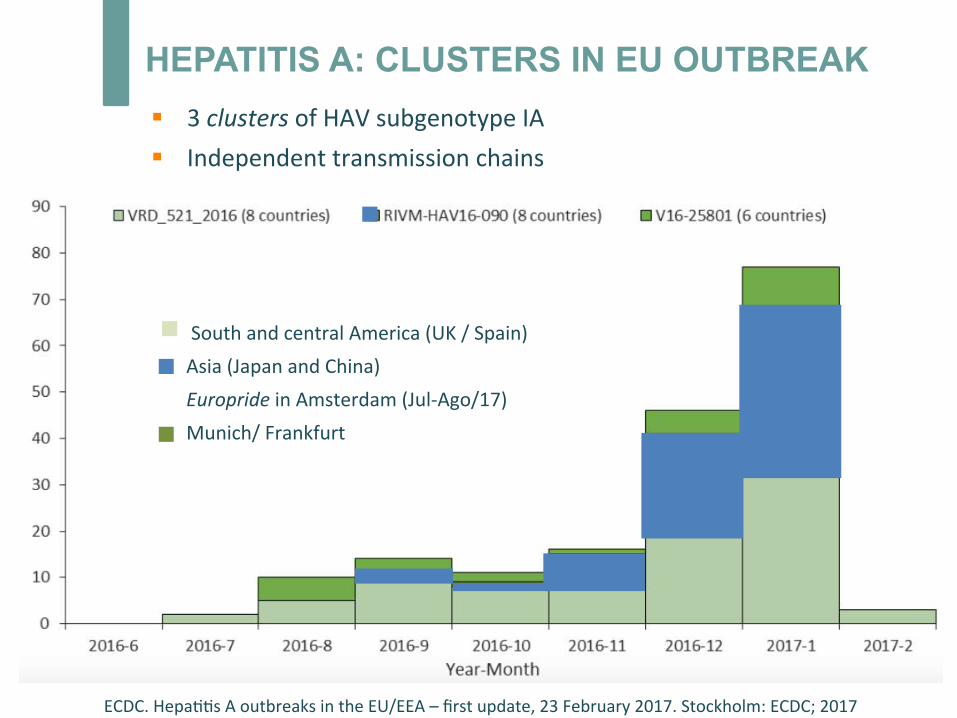
HEPATITIS A: CLUSTERS IN EU OUTBREAK
SouthandcentralAmerica(UK/Spain)Asia(JapanandChina)EuroprideinAmsterdam(Jul-Ago/17)Munich/Frankfurt
ECDC.Hepa**sAoutbreaksintheEU/EEA–firstupdate,23February2017.Stockholm:ECDC;2017
§ 3clustersofHAVsubgenotypeIA§ Independenttransmissionchains
HEPATITIS A: CLUSTER VRD_521_2016 (Portugal)
§ 1/Janthrough24/Apr/2017:242cases*no*fied§ 93%areyoungadultmen°
§ 79%liveinLisbon°§ 50%admiGedtohospital°
Na*onalGuidelinesforOutbreakControl-DGS(09-04-17)OutbreakinPortugal/EU
Globalvaccinerestric*ons(EU)
°Source:Hepa**sA,Na*onalGuidelines,08/05/2017,Na*onalHealthDirec*on*Source:DGS
§ ControlofvaccinesbyNa*onalHealthAuthori*es§ Specificloca*onsforvaccineadministra*on
Hepa*teA,Normano003/2017de09/04/2017,DireçãoGeraldeSaúde
§ OUTBREAKCONTROL:- IMMUNISATIONisthemaincontrolmeasure- Alertabouthygieneandsanitarypreven*vemeasures- Educa*onandcommunica*on(LGBTcommunity)
HEPATITIS A OUTBREAK: MANAGEMENT IN PORTUGAL
§ Vaccina*on:preandpost-exposurecondi*onsü Target:MSM;iden*fica*onofcontactsü 1doseofan;-HAVvaccine:freeofchargeü Thosewhohave1doseofvaccineareconsideredprotected
Travelers???
HEPATITIS A PREVENTION: IMMUNOGLOBULIN
§ Immunoglobulin:post-exposure(2wks)ü IGIM0,02mL/kg;protec*onin80-90%through3M
- Immunodeficiencywithvaccinefailure- Children<12Mofage- Chronichepa*cdisease- Vaccinecontraindica*ons
Hepa*teA,Normano003/2017de09/04/2017,DireçãoGeraldeSaúde
§ IGIMpre-exposure:0,02mL/KgIM(dura*on<3M)
0,06mL/KgIM(dura*on3-5M)
HEPATITIS A OUTBREAK: DISCUSSION
§ ControversiesaboutNa*onalHealthAuthorithiesguidelines:ü Travelersandotherriskgroupsneglectedü Efficacyofhealtheduca*onefforts?ü Pediatricvaccineinpre-exposureprophylaxis?Evidence?
§ Outbreakac*vity:ü Numberofcases/week?Severity?
§ Managementguidelines:ü Nºofadministeredvaccinesin1month?(1149)ü Nºofsecondarycases/contacts?Pediatriccases?ü Nºofavailablevaccines?

MEASLES
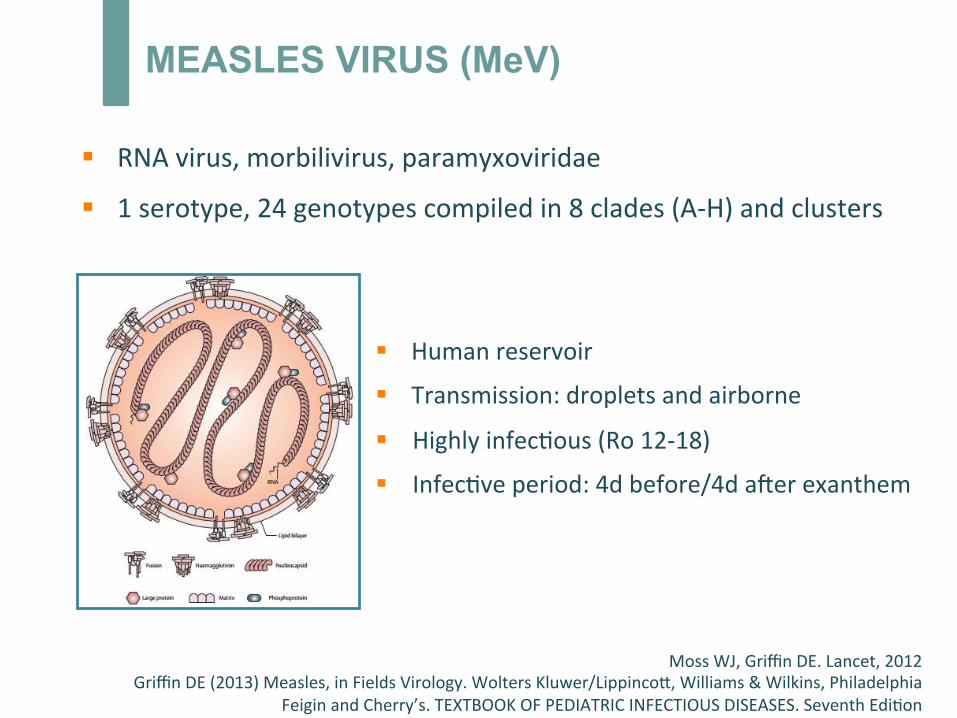
MEASLES VIRUS (MeV)
§ RNAvirus,morbilivirus,paramyxoviridae
§ 1serotype,24genotypescompiledin8clades(A-H)andclusters
MossWJ,GriffinDE.Lancet,2012GriffinDE(2013)Measles,inFieldsVirology.WoltersKluwer/LippincoG,Williams&Wilkins,Philadelphia
FeiginandCherry’s.TEXTBOOKOFPEDIATRICINFECTIOUSDISEASES.SeventhEdi*on
§ Humanreservoir
§ Transmission:dropletsandairborne
§ Highlyinfec*ous(Ro12-18)
§ Infec*veperiod:4dbefore/4da^erexanthem
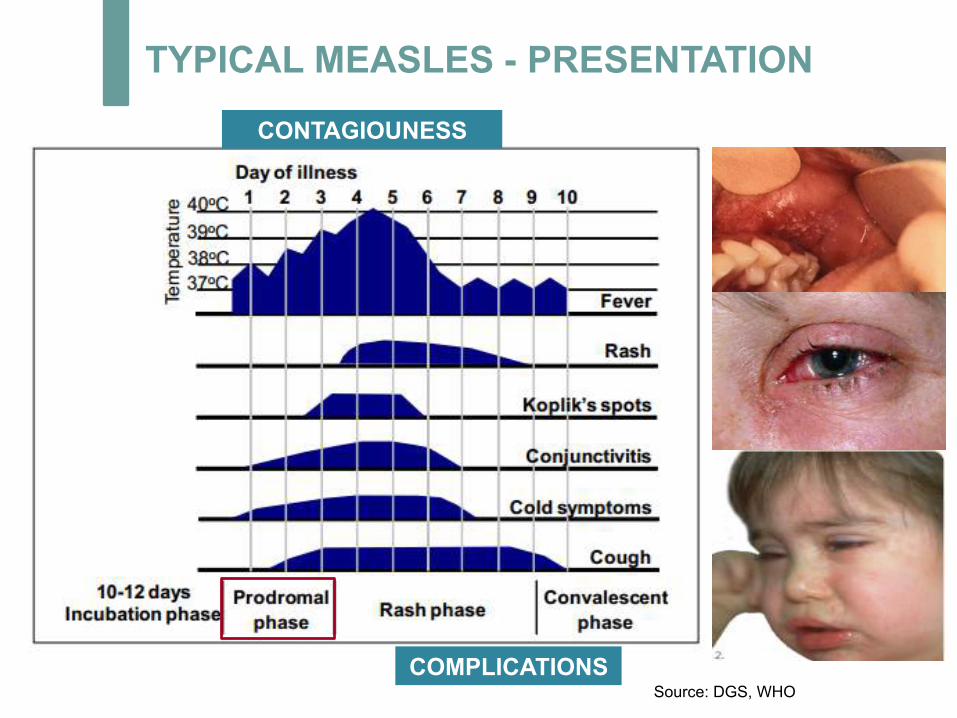
TYPICAL MEASLES - PRESENTATION
COMPLICATIONS Source: DGS, WHO
CONTAGIOUNESS
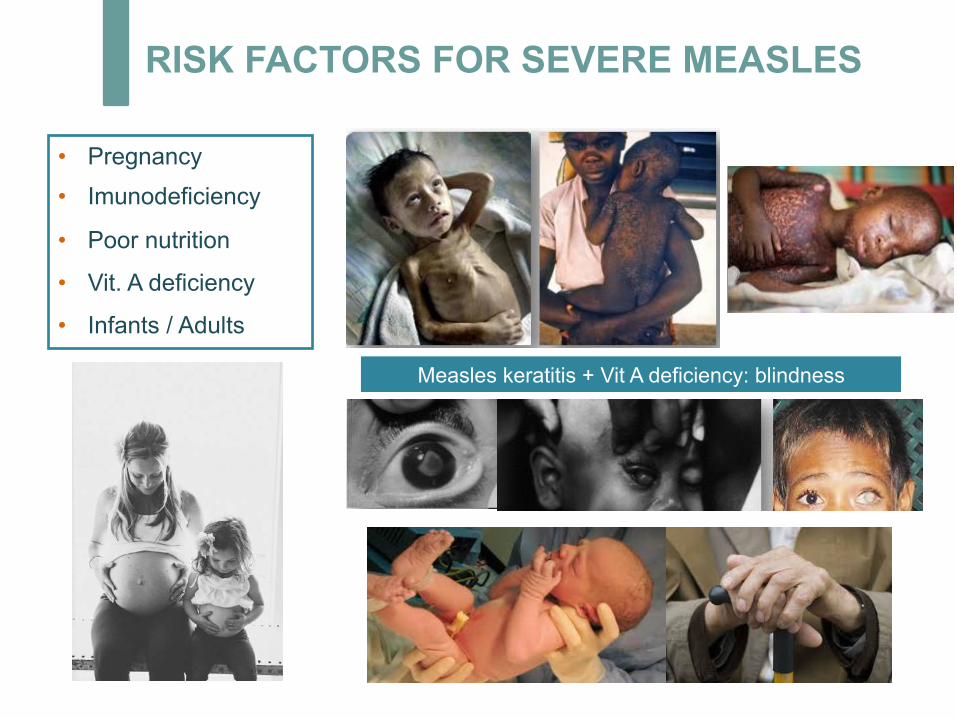
RISK FACTORS FOR SEVERE MEASLES
• Pregnancy
• Imunodeficiency
• Poor nutrition
• Vit. A deficiency
• Infants / Adults
Measles keratitis + Vit A deficiency: blindness
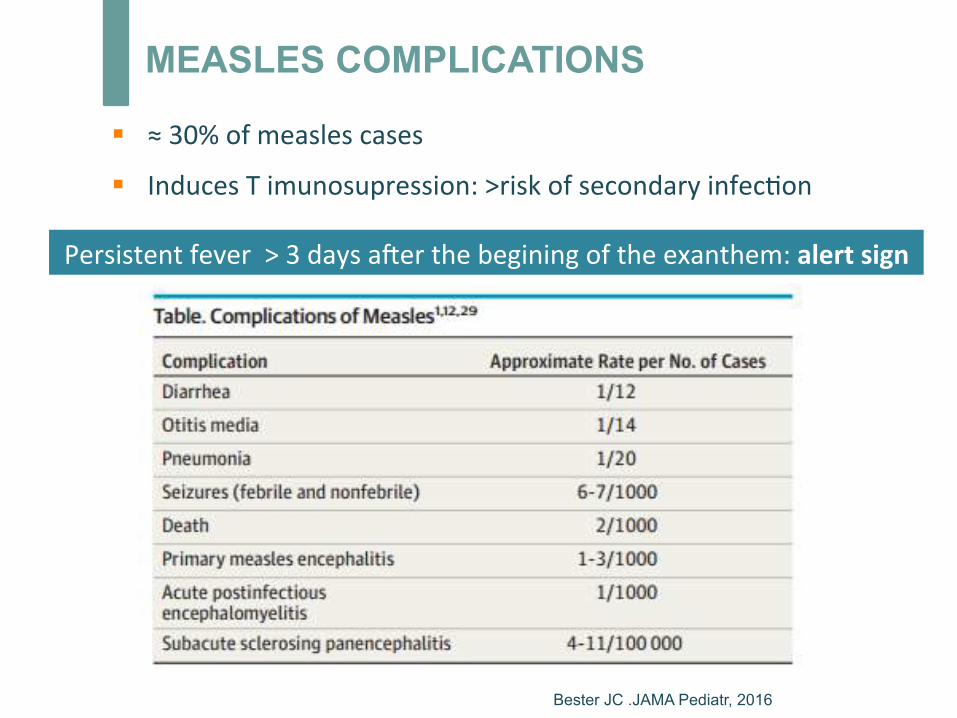
MEASLES COMPLICATIONS
§ ≈30%ofmeaslescases
§ InducesTimunosupression:>riskofsecondaryinfec*on
Persistentfever>3daysa^erthebeginingoftheexanthem:alertsign
Bester JC .JAMA Pediatr, 2016
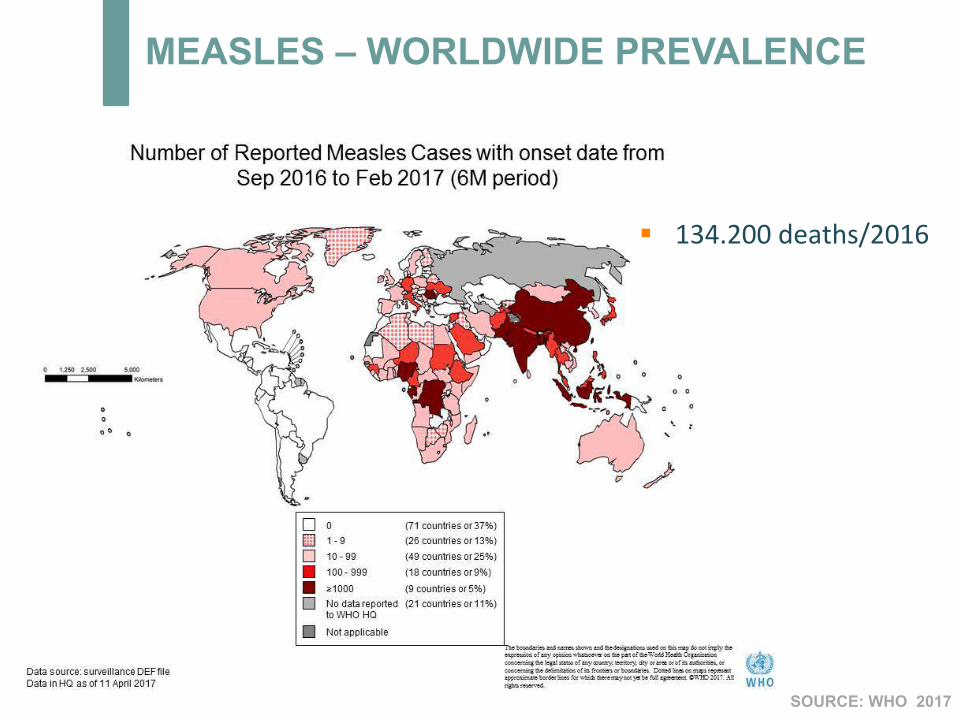
MEASLES – WORLDWIDE PREVALENCE
SOURCE: WHO 2017
§ 134.200deaths/2016
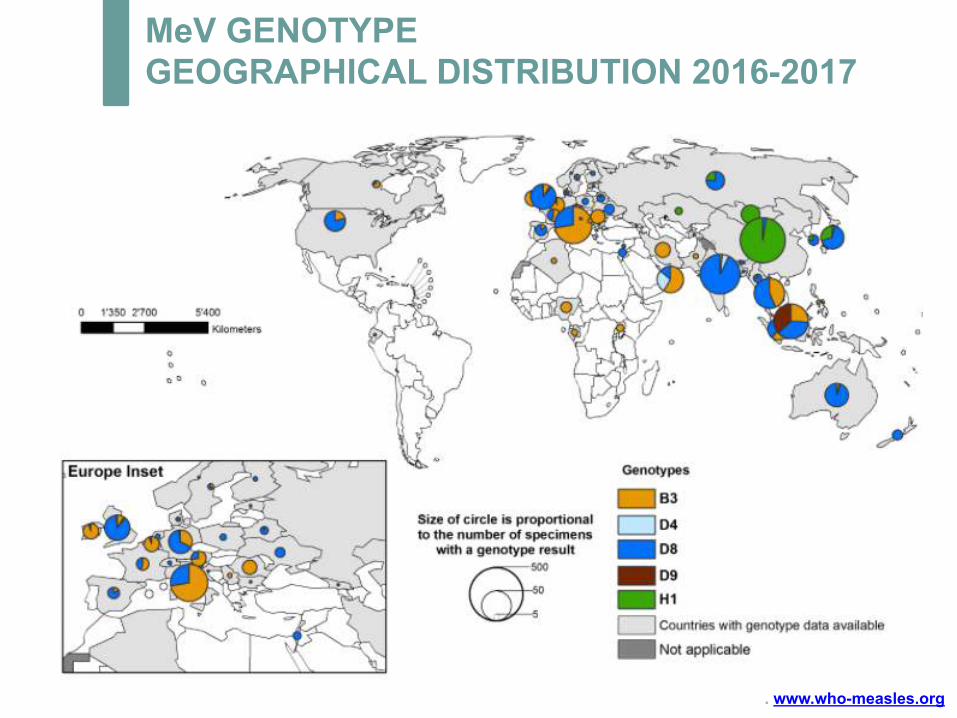
MeV GENOTYPE GEOGRAPHICAL DISTRIBUTION 2016-2017
. www.who-measles.org
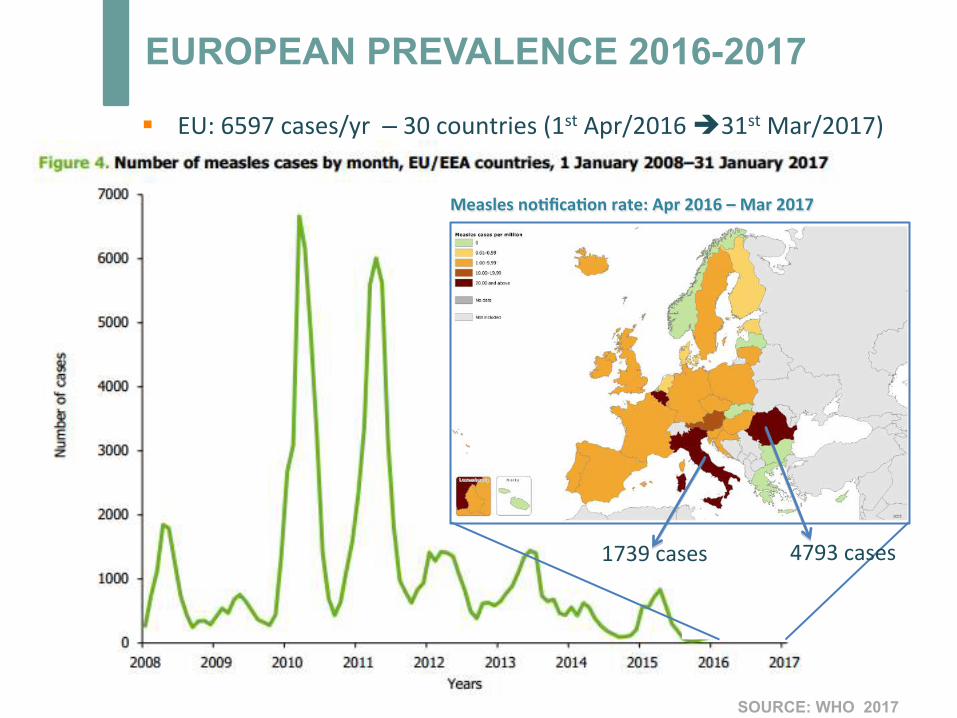
EUROPEAN PREVALENCE 2016-2017
SOURCE: WHO 2017
Measlesno;fica;onrate:Apr2016–Mar2017
§ EU:6597cases/yr–30countries(1stApr/2016è31stMar/2017)
4793cases1739cases
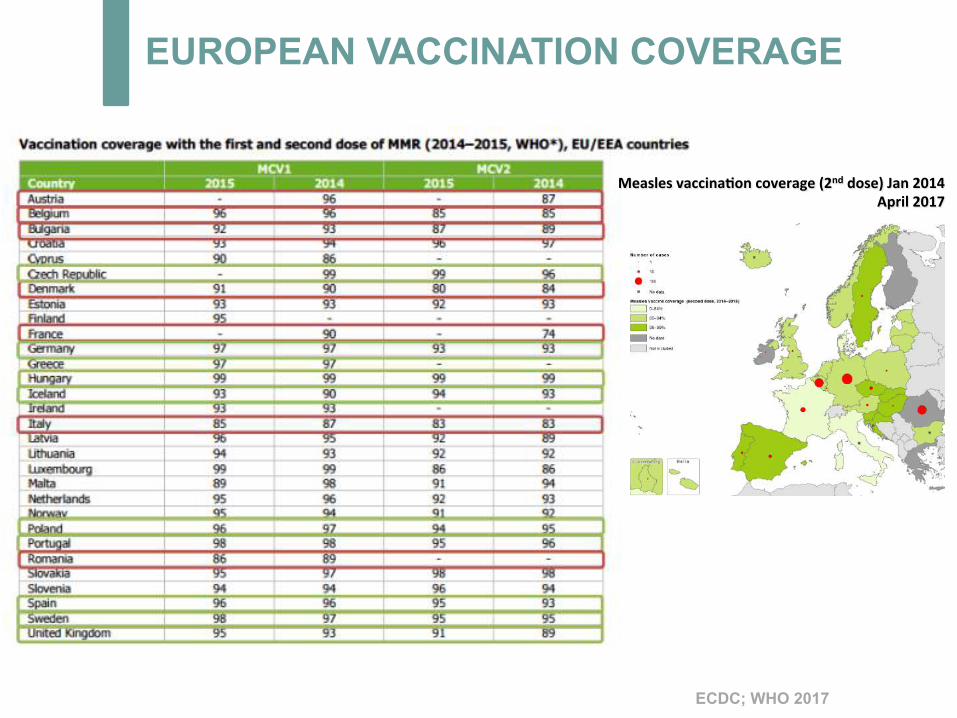
EUROPEAN VACCINATION COVERAGE
ECDC; WHO 2017
Measlesvaccina;oncoverage(2nddose)Jan2014April2017
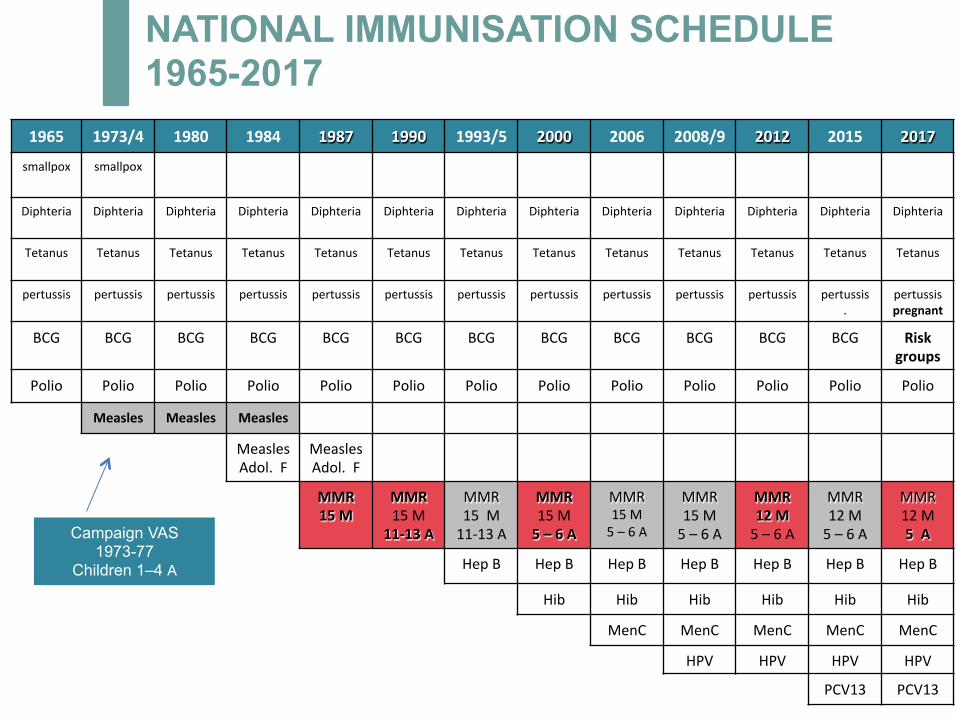
NATIONAL IMMUNISATION SCHEDULE 1965-2017
1965 1973/4 1980 1984 1987 1990 1993/5 2000 2006 2008/9 2012 2015 2017
smallpox smallpox
Diphteria Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Diphteria
Tetanus Tetanus Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
Tetanus
pertussis pertussis pertussis
pertussis
pertussis
pertussis
pertussis
pertussis
pertussis
pertussis
pertussis
pertussis.
pertussispregnant
BCG BCG BCG BCG BCG BCG BCG BCG BCG BCG BCG BCG Riskgroups
Polio Polio Polio Polio Polio Polio Polio Polio Polio Polio Polio Polio Polio
Measles Measles Measles
MeaslesAdol.F
MeaslesAdol.F
MMR15M
MMR15M
11-13A
MMR15M11-13A
MMR15M5–6A
MMR15M5–6A
MMR15M5–6A
MMR12M5–6A
MMR12M5–6A
MMR12M5A
HepB HepB HepB HepB HepB HepB HepB
Hib Hib Hib Hib Hib Hib
MenC MenC MenC MenC MenC
HPV HPV HPV HPV
PCV13 PCV13
Campaign VAS 1973-77
Children 1–4 A
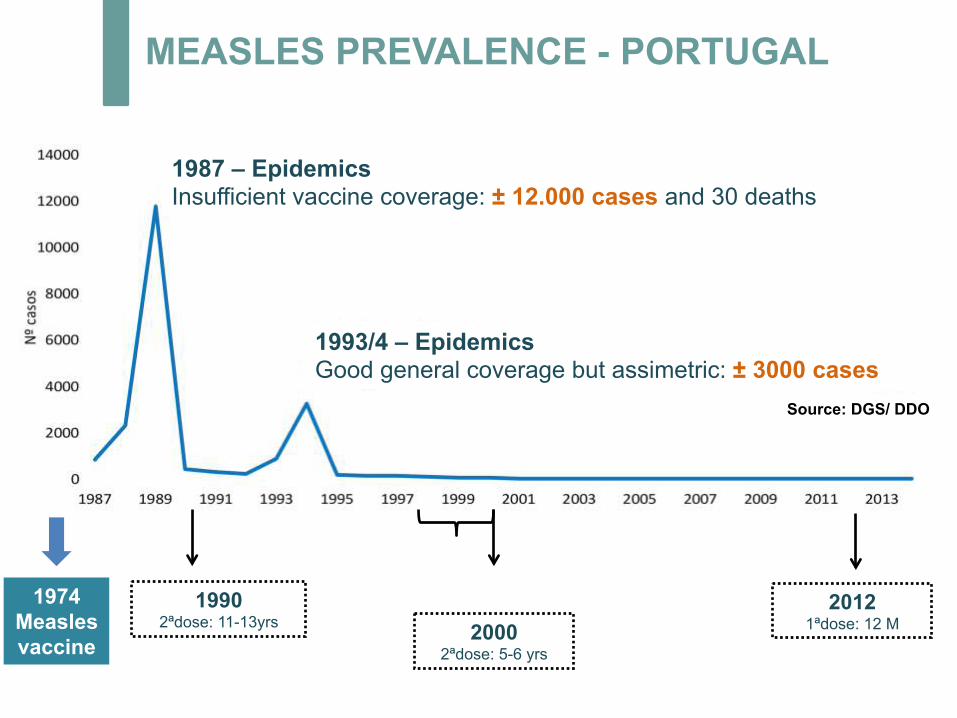
MEASLES PREVALENCE - PORTUGAL
1974 Measles vaccine
1990 2ªdose: 11-13yrs 2000
2ªdose: 5-6 yrs
Source: DGS/ DDO
2012 1ªdose: 12 M
1987 – Epidemics Insufficient vaccine coverage: ± 12.000 cases and 30 deaths
1993/4 – Epidemics Good general coverage but assimetric: ± 3000 cases
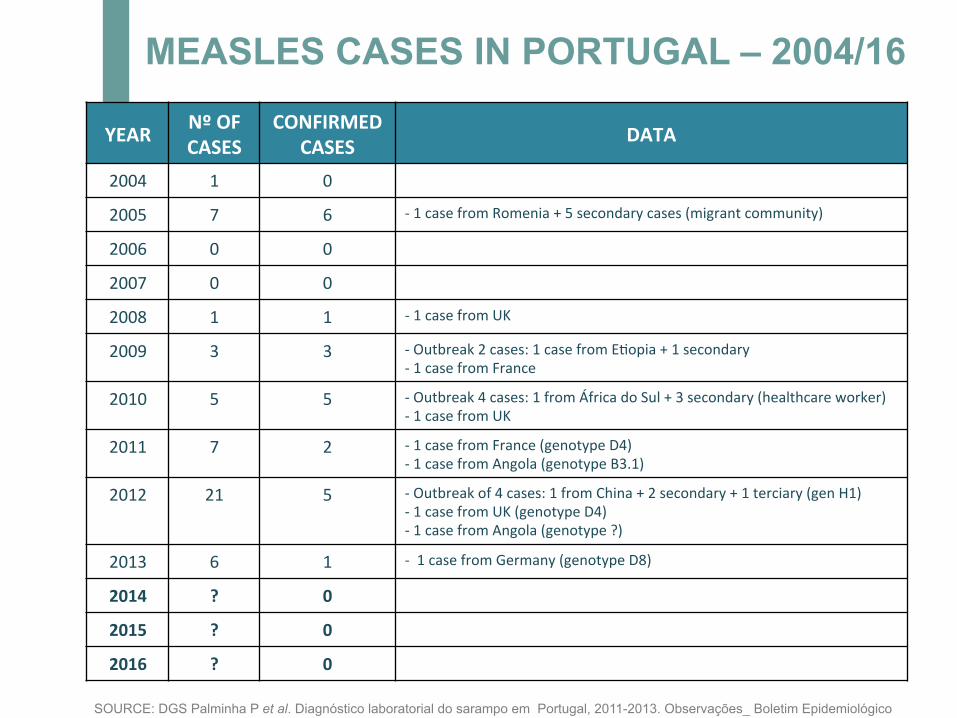
YEAR NºOFCASES
CONFIRMEDCASES DATA
2004 1 0
2005 7 6 -1casefromRomenia+5secondarycases(migrantcommunity)
2006 0 0
2007 0 0
2008 1 1 -1casefromUK
2009 3 3 -Outbreak2cases:1casefromE*opia+1secondary-1casefromFrance
2010 5 5 -Outbreak4cases:1fromÁfricadoSul+3secondary(healthcareworker)-1casefromUK
2011 7 2 -1casefromFrance(genotypeD4)-1casefromAngola(genotypeB3.1)
2012 21 5 -Outbreakof4cases:1fromChina+2secondary+1terciary(genH1)-1casefromUK(genotypeD4)-1casefromAngola(genotype?)
2013 6 1 -1casefromGermany(genotypeD8)
2014 ? 0
2015 ? 0
2016 ? 0
SOURCE: DGS Palminha P et al. Diagnóstico laboratorial do sarampo em Portugal, 2011-2013. Observações_ Boletim Epidemiológico
MEASLES CASES IN PORTUGAL – 2004/16
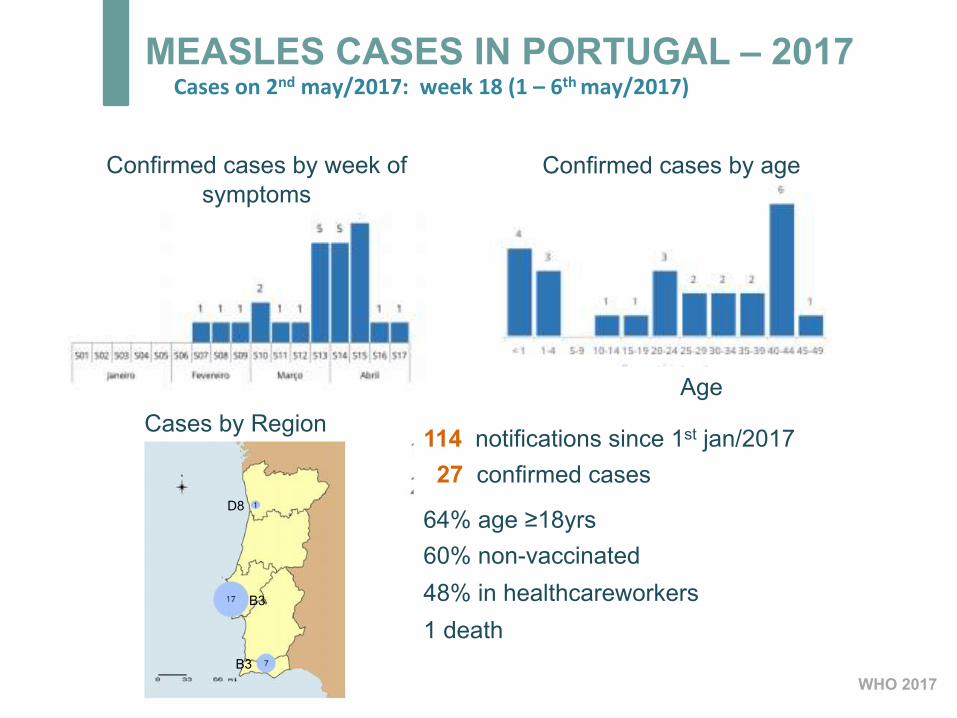
MEASLES CASES IN PORTUGAL – 2017 Caseson2ndmay/2017:week18(1–6thmay/2017)
ECDC; WHO 2017
Confirmed cases by week of
symptoms
Confirmed cases by age
D8
B3
B3
Cases by Region 114 notifications since 1st jan/2017 27 confirmed cases
64% age ≥18yrs 60% non-vaccinated 48% in healthcareworkers 1 death
Age
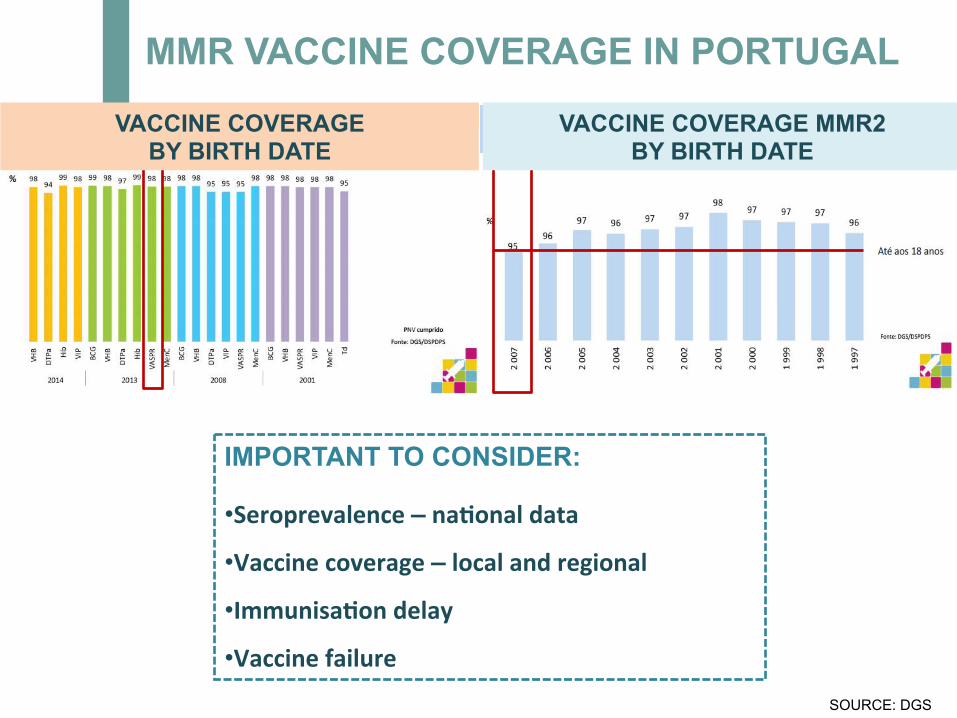
MMR VACCINE COVERAGE IN PORTUGAL
IMPORTANT TO CONSIDER:
• Seroprevalence–na;onaldata
• Vaccinecoverage–localandregional
• Immunisa;ondelay
• VaccinefailureSOURCE: DGS
VACCINE COVERAGE BY BIRTH DATE
VACCINE COVERAGE MMR2 BY BIRTH DATE
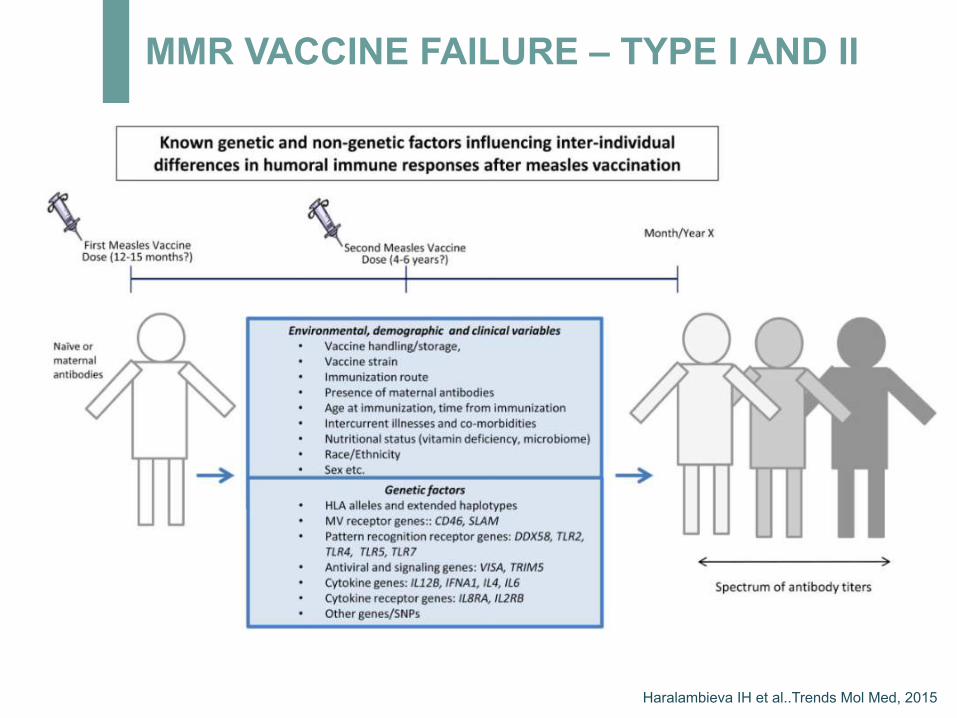
MMR VACCINE FAILURE – TYPE I AND II
Haralambieva IH et al..Trends Mol Med, 2015
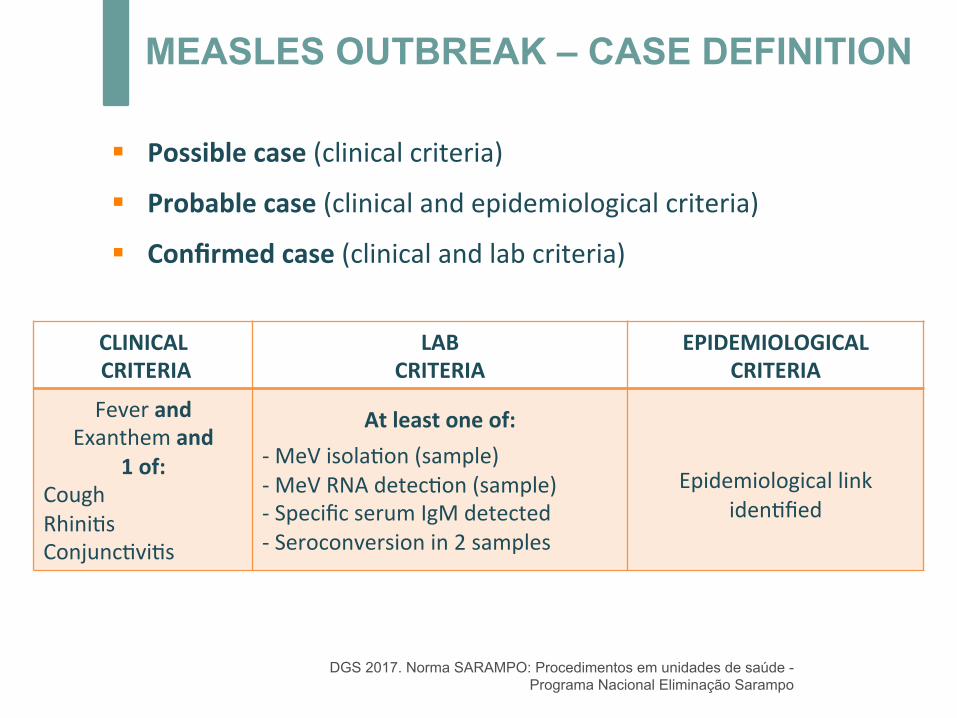
MEASLES OUTBREAK – CASE DEFINITION
§ Possiblecase(clinicalcriteria)§ Probablecase(clinicalandepidemiologicalcriteria)
§ Confirmedcase(clinicalandlabcriteria)
DGS 2017. Norma SARAMPO: Procedimentos em unidades de saúde - Programa Nacional Eliminação Sarampo
CLINICALCRITERIA
LABCRITERIA
EPIDEMIOLOGICALCRITERIA
FeverandExanthemand
1of:CoughRhini*sConjunc*vi*s
Atleastoneof:-MeVisola*on(sample)-MeVRNAdetec*on(sample)-SpecificserumIgMdetected-Seroconversionin2samples
Epidemiologicallink
iden*fied
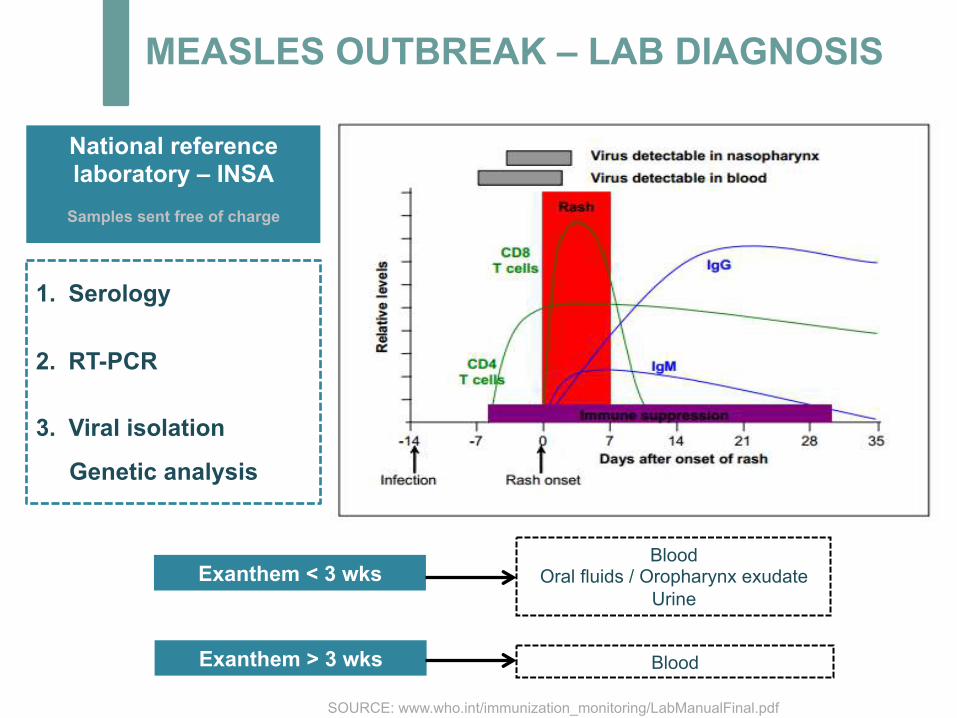
MEASLES OUTBREAK – LAB DIAGNOSIS
SOURCE: www.who.int/immunization_monitoring/LabManualFinal.pdf
1. Serology
2. RT-PCR
3. Viral isolation
Genetic analysis
Exanthem < 3 wks
Exanthem > 3 wks
Blood Oral fluids / Oropharynx exudate
Urine
Blood
National reference laboratory – INSA
Samples sent free of charge
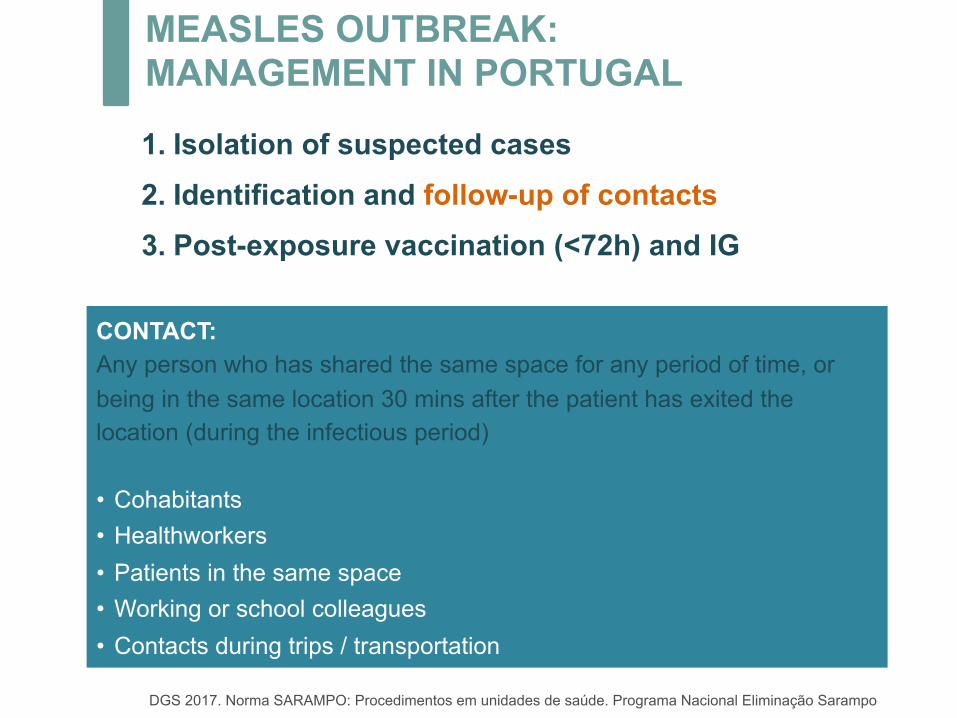
MEASLES OUTBREAK: MANAGEMENT IN PORTUGAL
1. Isolation of suspected cases 2. Identification and follow-up of contacts 3. Post-exposure vaccination (<72h) and IG
CONTACT: Any person who has shared the same space for any period of time, or being in the same location 30 mins after the patient has exited the location (during the infectious period) • Cohabitants • Healthworkers • Patients in the same space • Working or school colleagues • Contacts during trips / transportation
DGS 2017. Norma SARAMPO: Procedimentos em unidades de saúde. Programa Nacional Eliminação Sarampo
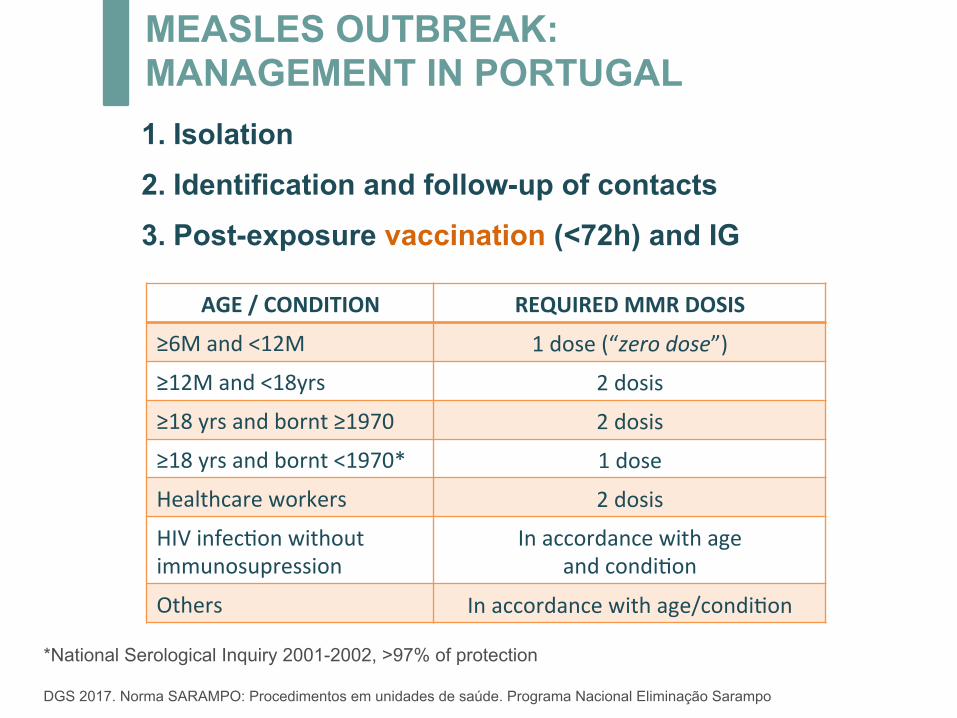
*National Serological Inquiry 2001-2002, >97% of protection DGS 2017. Norma SARAMPO: Procedimentos em unidades de saúde. Programa Nacional Eliminação Sarampo
1. Isolation 2. Identification and follow-up of contacts 3. Post-exposure vaccination (<72h) and IG
AGE/CONDITION REQUIREDMMRDOSIS
≥6Mand<12M 1dose(“zerodose”)
≥12Mand<18yrs 2dosis
≥18yrsandbornt≥1970 2dosis
≥18yrsandbornt<1970* 1dose
Healthcareworkers 2dosis
HIVinfec*onwithoutimmunosupression
Inaccordancewithageandcondi*on
Others Inaccordancewithage/condi*on
MEASLES OUTBREAK: MANAGEMENT IN PORTUGAL
DGS 2017. Norma SARAMPO: Procedimentos em unidades de saúde. Programa Nacional Eliminação Sarampo
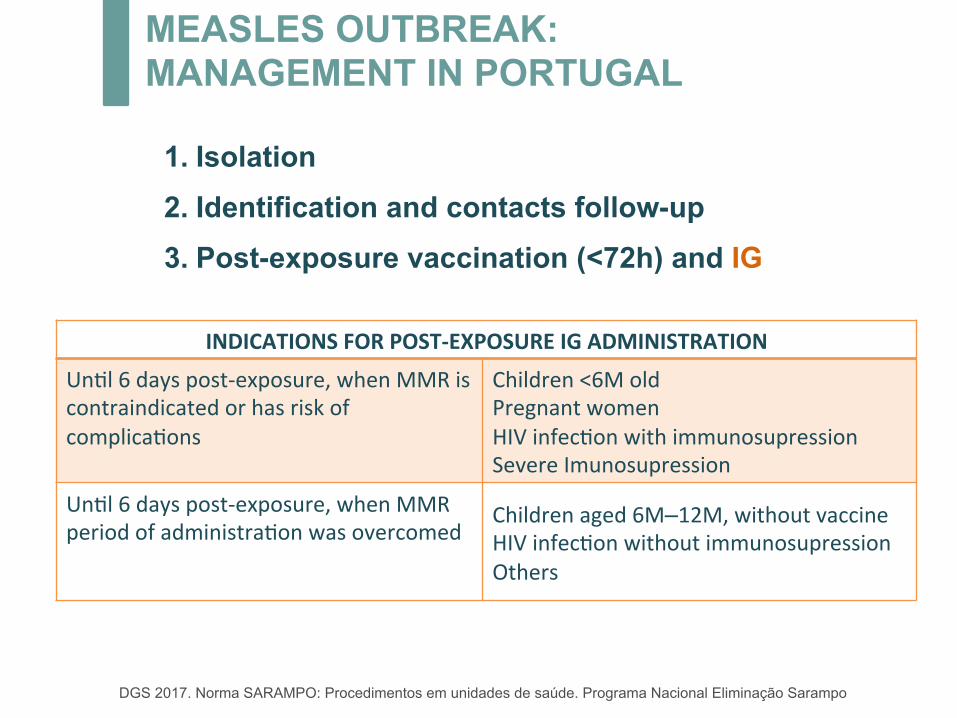
1. Isolation 2. Identification and contacts follow-up 3. Post-exposure vaccination (<72h) and IG
INDICATIONSFORPOST-EXPOSUREIGADMINISTRATION
Un*l6dayspost-exposure,whenMMRiscontraindicatedorhasriskofcomplica*ons
Children<6MoldPregnantwomenHIVinfec*onwithimmunosupressionSevereImunosupression
Un*l6dayspost-exposure,whenMMRperiodofadministra*onwasovercomed
Childrenaged6M–12M,withoutvaccineHIVinfec*onwithoutimmunosupressionOthers
MEASLES OUTBREAK: MANAGEMENT IN PORTUGAL
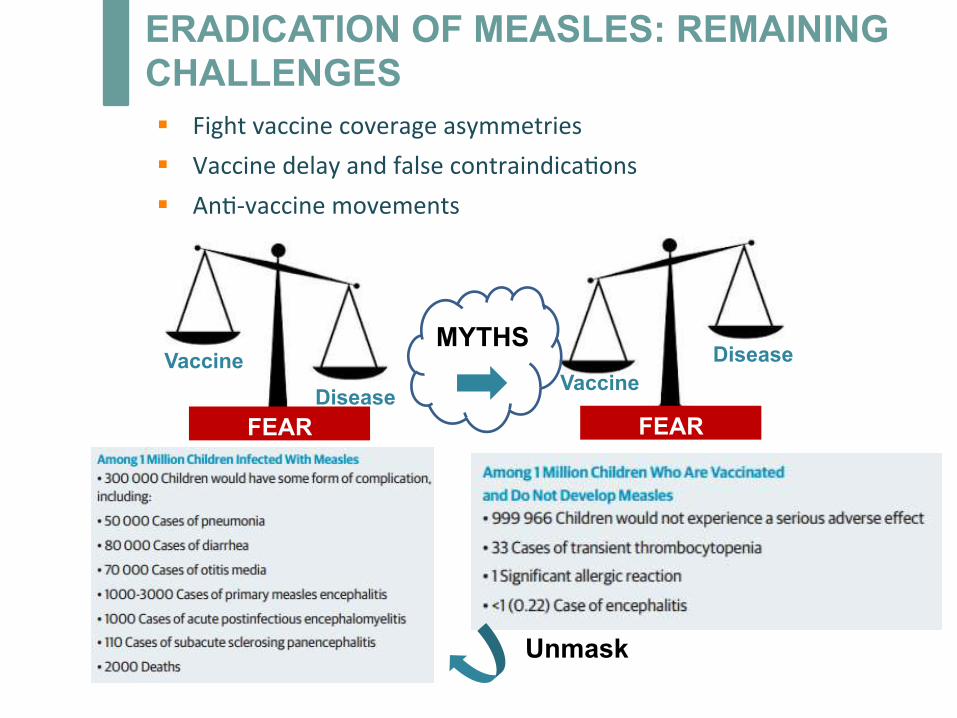
ERADICATION OF MEASLES: REMAINING CHALLENGES
Unmask
FEAR FEAR
Vaccine Disease
MYTHS Disease
Vaccine
§ Fightvaccinecoverageasymmetries§ Vaccinedelayandfalsecontraindica*ons§ An*-vaccinemovements
§ Elimina*on/Eradica*onispossible
ü Exclusivehumantransmission
ü Effec*vevaccine
§ Managementplan:transmissioninterrupted(south)andê(Lisbon)in2months
§ Fightvaccinehesitancy:teaching(notcoercion/obliga*on)
ERADICATION OF MEASLES: REMAINING CHALLENGES
ThankyouJ!
isabel.castro.menezes@gmail.comAcknowledgmentsfordataandpptonMeaslesoutbreak:DrDianaMoreira
HEPATITIS A NAD MEASLES OUTBREAK: DISCUSSION