Embed Size (px)
Citation preview

07/03/2014
1
VACCINES AFFECTING HCW SAFETY
Kent A. Sepkowitz, MDMemorial Sloan-Kettering Cancer Center
Disclosure
Completely Free of All Human and Financial Conflict

07/03/2014
2
Are Hospitals Safe?
SARS, MERS, and Swine flu have demonstrated the risk to HCWs of caring for the contagious
How do healthcare workers prevent occupationally acquired infections?

07/03/2014
3
Diphtheria
Diphtheria etymology: “pair of leather scrolls”
Diphtheria
In early 1900s, diphtheria and scarlet fever accounted for half of all ID admissions
Occupational transmission to 5%
Gauze masks to prevent scarlet fever and vaccinations for diphtheria instituted
First attempts to protect HCW

07/03/2014
4

07/03/2014
5
Strongly Recommended
Dead
Influenza
HBV
Pertussis
Alive
MMR
Varicella
Recommended: Specific Circumstances Only
Dead
Meningococcus (micro lab)
Typhoid (micro lab)
Polio (micro lab)
Alive
Smallpox
BCG
Typhoid oral (ditto)

07/03/2014
6
Not Specifically Recommended
Dead
Pneumococcus
Tetanus
Diphtheria
Hepatitis A
Alive
Shingles
LAIV (Flumist)
Occupationally-Acquired Infections in HCWVaccine Available
• BloodborneHIV, hepatitis B, hepatitis C, CMV
• Airborne or DropletTB, measles, varicella, pertussis, mumps, influenza, RSV, parvovirus B19, rubella, variola, SARS, MERS,meningococcus
• Fecal-Oralsalmonella, hepatitis A, helicobacter, Norwalk
• Directscabies, lice, herpes simplex

07/03/2014
7
Are Live Vaccines Safe to Give?
MMR
Varivax / Zostrix
Flumist
BCG
Vaccinia
Occupationally-Acquired Infections in HCW
Bloodborne
• HIV
• Hepatitis B
• Hepatitis C
• CMV

07/03/2014
8
How Long Does HBV Vaccine Work?
US does not recommend routine re-vaccination
Many countries re-vaccinate every 5-10 years or when titers fall below a certain level
What About Non-Converters?
Excellent data from Eskimo/Inuit cohort followed since 1981-2 after vaccine
Hyperendemic for HBV
Non-converters had no serious cases of acute HBV, though 3 had new HBcAb over 10 years
Non-converters may be protected

07/03/2014
9
Who Does Not Seroconvert?
Overall rate about 90+%
Overweight smoking older males have lower rates --60+%
Repeat 3-dose
series X 1 adds
30-50% conversion
Generation of vaxed
infants now of age
Dealing with Non-Convertors (if second series fails)
Intradermal series
Double-dose vaccination in a standard 3-dose series of combination hepatitis A and hepatitis B vaccine Among 44 nonresponders, protective anti-HBs levels
were found in 26 (59%) after the first dose and in 42 (95%) after the third dose. (Cardell, JID 2008)

07/03/2014
10
Scenario #1
You are called because a nurse stuck himself with a needle used to draw blood from a patient with HBsAg
The nurse “thinks he was vaccinated for the last job” 7 years ago
Scenario #1: You should
1. Initiate a 3-vaccine series
2. Give HBIG
3. Start vaccine AND give HBIG
4. Check the nurse’s serostatus
5. Turn off your beeper and go back to sleep

07/03/2014
11
Scenario #1: You should
1. Initiate a 3-vaccine series
2. Give HBIG
3. Start vaccine AND give HBIG
4. Check the nurse’s serostatus
5. Turn off your beeper and go back to sleep
What Do You DoPost HBsAg Exposure?
If established vaccine responder: Nothing
If unvaccinated or serostatus unknown: Vaccine and HBIG
Check serostatus
If vaccine non-responder: HBIG X 2 or vaccine and HBIG X 1

07/03/2014
12
Occupationally-Acquired Infections in HCW
TB
Measles*
Varicella
Pertussis
Mumps
Influenza*
RSV
Parvovirus B19
Rubella
Variola*
SARS
Meningococcus*

07/03/2014
13
Pertussis
‘100-day cough’
20% of adult population estimated to be susceptible
12-30% of all prolonged coughing illnesses in adults are pertussis
Our immunity is waning: Outbreaks reported every year
Pertussis, US: 1922-2005

07/03/2014
14
Mayo OutbreakICHE 2009, 30:467
Mayo OutbreakICHE 2009, 30:467

07/03/2014
15

07/03/2014
16
Pertussis (Tdap)ACIP Recommendation, 2005
HCWs should receive Tdap every 10 years instead of Td Do not confuse Tdap with DTaP which has higher
concentrations of D and T (given to children)
ER’s often confuse these
Tdap hurts due to the toxoid part of the preparation
Acellular Pertussis Vaccine Combined with Tetanus and Diphtheria Toxoids
In the United States, there are two Tdap products ADACEL® licensed on June 10, 2005, for use in persons aged 11--64
years as a single dose active booster vaccination against tetanus, diphtheria, and pertussis.
Another Tdap product, BOOSTRIX® is just licensed for use in 10-64 year olds
Pediatric DTaP is DAPTACEL®
ADACEL® and DAPTACEL® contain the same five pertussis antigens

07/03/2014
17
Pertussis PEP Dosing
Azithromycin: 500mg day 1, then 250 for 4 more days (the Z-pack)
Erythromycin: 2 gms/d for 14d
Clarithromycin: 1gm/d for 7d
Bactrim: DSB BID for 14d
MMWR Dec 9, 2005;54 (RR14)
Scenario #2
The same nurse transferred to a pediatrics ward
He is exposed to a child with pertussis who had been treated for routine pneumonia in a non-isolation room
He was vaccinated with Tdap 2 years ago

07/03/2014
18
Scenario #2: You Should:
1. Not worry – he’s vaccinated
2. Give him PEP regardless of vaccine status
3. Give Tdap again
4. Check his pertussis serostatus
5. Turn off your beeper and go back to sleep
Scenario #2: You Should:
1. Not worry – he’s vaccinated
2. Give him PEP regardless of vaccine status
3. Give Tdap again
4. Check his pertussis serostatus
5. Turn off your beeper and go back to sleep

07/03/2014
19
Occupationally-Acquired Infections in HCW
TB
Measles
Varicella
Pertussis
Mumps
Influenza
RSV
Parvovirus B19
Rubella
Variola
SARS
Meningococcus
Meningococcus

07/03/2014
20

07/03/2014
21
Meningococcus Vaccine
6 serogroups cause almost all human disease (different antigen on capsule)
Current MCV4 Prevents A, C, W-135, and Y
Does not prevent B or X
MCV4 covers 70% of cases seen in college students pre-vaccination rec
Mening belt is 80%+ Group A
Meningococcus Vaccine
HCWs without a spleen or with complement deficiency
Clinical and research microbiologists including technicians “who might be exposed routinely to N meningitidis”
Boost every 5 years

07/03/2014
22
Princeton, UCSB and B Vaccine
Occupationally-Acquired Infections in HCW
TB
Measles
Varicella
Pertussis
Mumps
Influenza
RSV
Parvovirus B19
Rubella
Variola
SARS
Meningococcus

07/03/2014
23
Measles
It’s 3-D and starts in “dandruff distribution”

07/03/2014
24
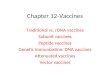
Measles: Koplik’s Spots
They appear opposite the molars as red spots with blue white centers

07/03/2014
25

07/03/2014
26
Occupationally-Acquired Infections in HCW
TB
Measles
Varicella
Pertussis
Mumps
Influenza
RSV
Parvovirus B19
Rubella
Variola
SARS
Meningococcus
Influenza

07/03/2014
27
Influenza: Model for the Worst Possible Vaccine
Needs to be given annually
Covers anticipated strains only
Only 60-80%+ effective against selected strains
Hurts but does not cause influenza
Does not prevent other URI
© 2013 Lippincott Williams & Wilkins, Inc. Published by Lippincott Williams & Wilkins, Inc. 2
Table 2

07/03/2014
28
Scenario #3
The same nurse transferred to the emergency room
He is exposed to a series of persons with influenza who were not isolated
Per EHS records, he was vaccinated for seasonal flu 2 months ago
Scenario #3: You Should:
1. Not worry – he’s vaccinated
2. Give him antiviral PEP regardless of vaccine status
3. Give him flu vaccination again
4. Check his influenza serostatus
5. Turn off your beeper and go back to sleep

07/03/2014
29
Scenario #3: You Should:
1. Not worry – he’s vaccinated
2. Give him antiviral PEP regardless of vaccine status
3. Give him flu vaccination again
4. Check his influenza serostatus
5. Turn off your beeper and go back to sleep
Occupationally-Acquired Infections in HCW
TB
Measles
Varicella
Pertussis
Mumps
Influenza
RSV
Parvovirus B19
Rubella
Variola
SARS
Meningococcus

07/03/2014
30
Vaccinia

07/03/2014
31
Benjamin Jesty62

07/03/2014
32
MyocarditisMilitary and civilian experience
About 1 per 1500 vaccinations
All male primary vaccinees in military Rate at 1 in 800
Mostly female revaccinees in civilian program
Most have recovered
Long-term consequences not known
Case definition remains very difficult
Vaccination Needs in HCW, 2012
• BloodborneHIV, hepatitis B, hepatitis C, CMV, Ebola
• Airborne or DropletTB, measles, varicella, pertussis, mumps, influenza, RSV, parvovirus B19, rubella, variola, SARS, meningococcus
• Fecal-Oralsalmonella, hepatitis A, helicobacter, Norwalk
• Directscabies, lice, herpes simplex

07/03/2014
33
Work Restrictions for HCW’s Exposed to or Infected with Vaccine-Preventable Diseases
Problem Restriction DurationMumpsActive Exclude 9 days after onset of parotitisExposure (Ab-) Exclude 12th day after initial exposure till
26thday after last exposure PertussisActive Exclude Beginning of catarrhal stage
through 3rd week after onsetof paroxysms or until 5 daysafter start of effective Abx
Exposure (Ab-)Symptoms Exclude 5 days after start of effective AbxNo symptom None If on Abx
Work Restrictions for HCW’s Exposed to or Infected with Vaccine-Preventable Diseases
Problem Restriction DurationRubellaActive Exclude 5 days after rash appears Exposure (Ab-) Exclude 7th day after initial exposure till 21st
day after last exposure VaricellaActive Exclude Until all lesions crust/dry Exposure (Ab-) Exclude 10th day after exposure till 21st day
(extend to 28d if VZIG used) ZosterActive Cover; no “high Same as varicella
-risk” patients Exposure (Ab-) Exclude Same as varicella

07/03/2014
34
Conclusions
Hospitals remain slightly unsafe places to work in
Healthcare workers do not avail themselves of useful vaccinations
There will always be another disease with potential risk