Embed Size (px)
DESCRIPTION
Varicella zoster virus (VZV), the pathogen responsible for herpes zoster, belongsto the herpesvirus family and is sensitive to the antiviral drug aciclovir. However,the low oral bioavailability of aciclovir has to some extent limited its efficacy inthe treatment of herpes zoster and has prompted the development of the morereadily absorbed oral prodrug valaciclovir
Citation preview
ValaciclovirA Review of its Use in the Management of Herpes Zoster
Douglas Ormrod and Karen GoaAdis International Limited, Auckland, New Zealand
Various sections of the manuscript reviewed by: A.M. Arvin, Division of Pediatric Infectious Diseases, Stanford University, Stanford, California, USA; J.Colin, Department of Ophthalmology, Hospital Morvan, Brest, France; R.H. Dworkin, Department ofAnesthesiology, University of Rochester Medical Center, Rochester, New York, USA; B.G. Gazzard, Chelseaand Westminster Hospital, London, England; C.F. Grose, Division of Pediatric Infectious Diseases, Universityof Iowa Hospitals, Iowa City, Iowa, USA; D.P. Langston, Department of Ophthalmology, Harvard MedicalSchool, Boston, Massachusetts, USA; P. Ljungman, Department of Internal Medicine, Huddinge UniversityHospital, Huddinge, Sweden; M. Niimura, Department of Dermatology, Jikei University School of Medicine,Tokyo, Japan; R.J. Whitley, Department of Pediatrics, Microbiology and Medicine, University of Alabamaat Birmingham, Birmingham, Alabama, USA.
ContentsSummary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13181. Overview of Varicella and Herpes Zoster . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13212. Overview of Pharmacodynamic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1323
2.1 Antiviral Activity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13232.2 Viral Resistance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1323
3. Pharmacokinetic Properties . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13243.1 Absorption and Distribution . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13243.2 Metabolism and Elimination . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1326
4. Therapeutic Efficacy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13274.1 Assessment of Pain in Herpes Zoster . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13274.2 Compared with Aciclovir, Famciclovir and/or Placebo . . . . . . . . . . . . . . . . . . . . . 1327
4.2.1 Herpes Zoster . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13274.2.2 Herpes Zoster Ophthalmicus . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1330
4.3 Prognostic Factors for Outcome of Long Term Pain . . . . . . . . . . . . . . . . . . . . . . . . 13314.4 Exploratory Dose Regimens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13324.5 Pharmacoeconomic Issues . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1333
ADIS DRUG EVALUATION Drugs 2000 Jun; 59 (6): 1317-13400012-6667/00/0006-1317/$25.00/0
© Adis International Limited. All rights reserved.
Data Selection
Sources: Medical literature published in any language since 1983 on Valaciclovir, identified using AdisBase (a proprietary database of AdisInternational, Auckland, New Zealand), Medline and EMBASE. Additional references were identified from the reference lists of publishedarticles. Bibliographical information, including contributory unpublished data, was also requested from the company developing the drug.Search strategy: AdisBase search terms were ‘Valaciclovir’ or ‘Valtrex’ or ‘BW256U’ or ‘256U87’ or ‘Valacyclovir’ and ‘Herpes-Zoster’.Medline search terms were ‘Valaciclovir’ or ‘Valtrex’ or ‘BW256U’ or ‘256U87’ or ‘Valacyclovir’ and ‘Herpes-Zoster’. EMBASE search termswere ‘Valaciclovir’ or ‘Valtrex’ or ‘BW256U’ or ‘256U87’ or ‘Valacyclovir’ and ‘Herpes-Zoster’. Searches were last updated 20 May 2000.Selection: Studies in patients with herpes zoster who received valaciclovir. Inclusion of studies was based mainly on the methods sectionof the trials. When available, large, well controlled trials with appropriate statistical methodology were preferred. Relevant pharmacodynamicand pharmacokinetic data are also included.Index terms: Valaciclovir, varicella zoster virus, shingles, herpes zoster, zoster ophthalmicus, pharmacodynamics, pharmacokinetics,therapeutic use.

4.6 Quality of Life . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13335. Tolerability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13336. Dosage and Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13357. Place of Valaciclovir in the Management of Herpesvirus Infections . . . . . . . . . . . . . . . . . . 1335
SummaryAbstract Varicella zoster virus (VZV), the pathogen responsible for herpes zoster, belongs
to the herpesvirus family and is sensitive to the antiviral drug aciclovir. However,the low oral bioavailability of aciclovir has to some extent limited its efficacy inthe treatment of herpes zoster and has prompted the development of the morereadily absorbed oral prodrug valaciclovir.In a large comparative study valaciclovir, (1000mg 3 times daily for 7 days)
was at least as effective as aciclovir (800mg5 times daily for 7 days) in controllingthe symptoms of acute herpes zoster. Importantly, valaciclovir alleviated zoster-associated pain and postherpetic neuralgia significantly faster than aciclovir. A14-day regimen of valaciclovir showed no significant advantage over the 7-dayregimen. A smaller trial in Japanese patients focusing primarily on the cutaneous(rash) signs of herpes zoster confirmed the similar efficacy of valaciclovir andaciclovir in the 7-day regimen. This study did not follow all patients for a formalanalysis of postherpetic neuralgia. Valaciclovir and aciclovir demonstrated sim-ilar efficacy for the control of cutaneous lesions and ocular complications inpatients with zoster ophthalmicus.Preliminary results of a large controlled trial indicate that valaciclovir 1000mg
3 times daily and famciclovir (the prodrug of penciclovir) 500mg 3 times dailyare of similar efficacy in speeding resolution of acute herpes zoster rash andshortening the duration of postherpetic neuralgia.Starting treatment later than 72 hours after rash onset did not significantly
reduce the beneficial effect of valaciclovir on duration of zoster-associated pain(a continuum of pain that encompasses both acute pain and postherpetic neural-gia) in a large observational study, suggesting that valaciclovir might be effectivewhen given later than previously thought. However, valaciclovir should ideallybe given as soon as possible after symptoms appear.With the recommended regimen for the treatment of herpes zoster (1000mg 3
times daily for 7 days) valaciclovir was well tolerated, with nausea and headachebeing the most commonly reported adverse events. The adverse events profile ofthe agent was similar to that seen with aciclovir or famciclovir.Conclusion: The efficacy of valaciclovir for the treatment of herpes zoster
has been confirmed and extended by follow-up studies in herpes zoster op-hthalmicus, in Japanese patients, and in the wider primary care setting. Vala-ciclovir is at least equivalent to, and better in certain parameters than, aciclovirand appears to have similar efficacy to famciclovir 500mg 3 times daily.Valaciclovir is a well tolerated first-line therapy with an established place in thetreatment of immunocompetent patients with herpes zoster.
PharmacodynamicProperties
Primary infection with varicella zoster virus (VZV) causes varicella (chicken-pox). When VZV reactivates from its latent state in sensory ganglia, it causesherpes zoster (shingles). Like other herpesviruses VZV is sensitive to aciclovir.The therapeutic benefit of valaciclovir in herpes zoster is based on establishingsufficiently high aciclovir concentrations in the blood for rapid penetration to
1318 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
sensory nerve tissue and skin for inhibition of VZV replication. After oral admin-istration and absorption valaciclovir is hydrolysed to aciclovir and L-valine.Aciclovir is then converted to aciclovir monophosphate by VZV-encoded thym-idine kinase and then to the active triphosphate form by cellular enzymes.Aciclovir triphosphate inhibits VZV (and other herpesvirus) DNA polymerase,terminating viral DNA chain elongation and preventing viral replication.Aciclovir triphosphate inhibits replication of a range of herpesviruses includ-
ing, in descending order of in vitro susceptibility, herpes simplex virus (HSV)-1,HSV-2, VZV, Epstein-Barr virus, human herpesviruses 6, 8 and 7 and cytomeg-alovirus. The concentration of aciclovir resulting in 50% inhibition of VZV invitro is 0.12 to 10.8 mg/L.VZV resistance in response to treatment with aciclovir is extremely rare in
immunocompetent patients, but continued surveillance is required to determinethe true incidence. The profile of VZV resistance to aciclovir after oral adminis-tration of valaciclovir is expected to be the same as after administration ofaciclovir. Although still rare, aciclovir-resistant strains of VZV do occur morefrequently in HIV-positive patients and transplant recipients.
PharmacokineticProperties
In healthy volunteers and patients with herpes zoster, valaciclovir is readily ab-sorbed from the gastrointestinal tract and undergoes rapid and extensive first-passmetabolism to yield aciclovir. In patients with herpes zoster treated with oralvalaciclovir 1000mg 3 times daily the estimated bioavailability of aciclovir wasapproximately 4 times greater than after oral aciclovir 800mg 5 times daily in acomparator group.In healthy adult volunteers after single 100 to 1000mg doses of valaciclovir,
the peak plasma concentrations (Cmax) and area under the plasma aciclovir con-centration-time curve (AUC) values of aciclovir increased in a slightly less thandose-proportional manner. However, more marked dose proportionality was ob-served in a phase I study in healthy Japanese male volunteers who received oralvalaciclovir 250 to 2000mg. In a population pharmacokinetic analysis of patientswith herpes zoster treated with valaciclovir 1000mg 3 times daily the Cmax was5.73 mg/L (range 2.76 to 16.1 mg/L) and the estimated daily mean AUC foraciclovir was 88.6 mg/L • h.Aciclovir is mainly eliminated via the renal route, but is also excreted in the
faeces. In healthy volunteers who received a single dose of valaciclovir 1000mg,themean renal clearance of aciclovir (15.3 L/h) exceeded the creatinine clearance,indicating that renal tubular secretion is actively involved in the elimination ofthe drug. Thus, dosage adjustment is required for patients with renal impairment.In healthy Japanese men who received valaciclovir 250 to 2000mg as a singledose the renal clearance was similar regardless of dose.After single valaciclovir doses of 100 to 1000mg or multiple doses of 1000 to
8000 mg/day for 6 to 11 days, the plasma elimination half-life (t1⁄2) of aciclovirranged from 2.76 to 3.3 hours; for single doses of valaciclovir 250 to 2000mg thet1⁄2 in healthy Japanese men was very similar (2.9 to 3.59 hours).No clinically significant interactions between valaciclovir and coadministered
drugs (including cimetidine, probenecid, digoxin, antacids or thiazide diuretics)have been reported. Valaciclovir may be administered with food.
Therapeutic Efficacy The efficacy of valaciclovir for the treatment of herpes zoster has been investi-gated in a large number of immunocompetent patients. Trials have compared
Valaciclovir in Herpes Zoster: A Review 1319
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

valaciclovir with placebo, aciclovir and famciclovir. A large noncomparativestudy has also been published.Valaciclovir was reported in an abstract to be significantly more effective than
placebo in reducing the duration of new lesion formation in patients aged between18 and 50 years. In a pivotal study of 1141 patients ≥50 years of age with herpeszoster, valaciclovir 1000mg 3 times daily for 7 or 14 days was as effective asaciclovir 800mg 5 times daily for 7 days in speeding resolution of rash. Impor-tantly, valaciclovir was significantly more effective than aciclovir in shorteningthe duration of both zoster-associated pain and postherpetic neuralgia: medianduration of pain after treatment with valaciclovir for 7 or 14 days was 38 and 44days, respectively, compared with 51 days for aciclovir, while median durationof postherpetic neuralgia was 30, 35 and 39 days for valaciclovir 7 and 14 daysand aciclovir, respectively. There was no statistical difference between the ben-eficial effects of 7 or 14 days’ valaciclovir treatment. The 7-day regimens ofvalaciclovir and aciclovir have also been compared in 200 Japanese patients andthe 2 treatments were similarly effective in the acute (rash) stage of the disease.Follow-up was not sufficient for statistical analysis of postherpetic neuralgia.Valaciclovir and aciclovir have also demonstrated comparable efficacy for theacute symptoms and long term complications of zoster ophthalmicus in a con-trolled trial in 110 patients.Preliminary results (abstract) of a double-blind study in 597 patients aged ≥50
years indicate that valaciclovir 1000mg 3 times daily and famciclovir 500mg 3times daily have similar efficacy in speeding resolution of zoster-associated pain,the primary end-point. Furthermore, no statistical differences were detected be-tween the 2 drugs in rash healing rates or in postherpetic neuralgia.Retrospective analysis of a fully published pivotal study showed that vala-
ciclovir treatment was similarly effective whether initiated within 48 or between48 and 72 hours of onset of rash. A large noncomparative study (n = 1897) ofvalaciclovir for the treatment of herpes zoster examined the influence of timingof treatment on therapeutic outcomes. Starting treatment later than 72 hours afterrash onset did not significantly affect the duration of zoster-associated pain.Therefore the therapeutic window of valaciclovir may be wider than previouslythought. However, valaciclovir should ideally be given as soon as possible aftersymptoms appear. These and other studies also examined prognostic factors as-sociated with resolution of postherpetic neuralgia and found that patients ≥50years of age and those experiencing more intense prodromal or acute pain, irre-spective of age, were at increased risk of prolonged pain.Quality of life (QOL) is significantly affected by herpes zoster and the influ-
ence of valaciclovir for 7 or 14 days and aciclovir for 7 days on QOLwas reportedas part of the large pivotal trial. QOL scores in valaciclovir-treated patients weregenerally improved compared with patients treated with aciclovir. The power ofthis trial was not sufficient for formal statistical analysis of QOL. Pharma-coeconomic issues have also been investigated and valaciclovir was found to bemore cost effective than aciclovir. While this differential benefit may erode withthe introduction of generic aciclovir, valaciclovir itself would still be consideredcost effective in terms of the direct medical costs of managing zoster-associatedpain.
Tolerability Oral valaciclovir is well tolerated with an adverse event profile qualitatively andquantitatively similar to that of oral aciclovir. In immunocompetent patients
1320 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
treated with valaciclovir 1000mg 3 times daily for 7 days (the recommended dosagefor the treatment of herpes zoster) adverse events were infrequent and generallymild, and similar to those seen in a comparator group treatedwith aciclovir 800mgfor 5 days. The only events reported bymore than 10%of patients receiving eitherdrug were nausea and headache.Trials comparing valaciclovir and aciclovir for the treatment of herpes zoster
in Japanese patients, and for herpes zoster ophthalmicus, reported a similar rangeand frequency of mild gastrointestinal events and headache to that documentedin the large pivotal study. No significant change from baseline in clinical chem-istry or haematological parameters, and no effect on renal function was observedin either the valaciclovir- or aciclovir-treated groups in either of these compara-tive studies.A similar pattern of mild events was reported in the large noncomparative trial
of valaciclovir for herpes zoster carried out in a number of clinical settings, includingprimary care. However, the incidence of adverse events was lower than that seenin the controlled clinical studies: headache and nausea occurred, respectively, in3 and 3.3% of patients overall.The comparative tolerability profiles of valaciclovir and famciclovir in pa-
tients with herpes zoster were reported in an abstract and found to be similar, withheadache and nausea being the most common adverse events.
Dosage andAdministration
The recommended dosage of valaciclovir for the treatment of herpes zoster inimmunocompetent patients is 1000mg 3 times daily for 7 days. Ideally treatmentshould be started as soon as possible after the onset of rash, but recent data suggestthat treatment initiated later than 72 hours may also be efficacious. The dosageof valaciclovir should be reduced in patients with moderate or severe renal im-pairment.Valaciclovir has not been specifically studied in immunocompromised pa-
tients, although some patients with mild impairment of immunity were permittedin the Japanese studies of valaciclovir for herpes zoster. In immunocompromisedindividuals the exposure to aciclovir after valaciclovir (1000mg 3 times daily) isequivalent to that after intravenous aciclovir (5 mg/kg 3 times daily), thereforethe use of valaciclovir in patients with mildly impaired immunity may be consid-ered. No data are available on valaciclovir use for VZV infection in children orpregnant women.
1. Overview of Varicella and Herpes Zoster
Varicella zoster virus (VZV) is a member of theAlphaherpesviridae subfamily of herpesviruseswhich also includes herpes simplex virus (HSV)types 1 and 2. VZV has the potential to cause 2different clinical syndromes: varicella (chicken-pox) and herpes zoster (shingles).[1] The latter dis-ease is the result of reactivation of latent virus that
follows primary infection. Varicella is primarily adisease of childhood and 90% of chickenpox casesoccur in children less than 10 years of age. In trop-ical regions primary varicella infection occurslater, with highest VZV seroconversion rates oc-curring during teenage years.[2] Varicella in olderadolescents and adults is associated with increasedmorbidity and mortality from complications suchas varicella pneumonia and varicella infection ofthe central nervous system.[1] Herpes zoster, on the
Valaciclovir in Herpes Zoster: A Review 1321
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

other hand, primarily affects people older than 50years of age.[3] In immunocompetent individualsneither varicella or herpes zoster is usually lifethreatening; however, in immunocompromised pa-tients (those with HIV, transplant recipients or pa-tients with cancer undergoing chemotherapy or ra-diotherapy) disseminated VZV infection can causeserious disease or death.[1]In children, varicella is characterised by a rash
which rapidly progresses to papules, vesicles, pus-tules and finally crusts. The lesions are primarilyconfined to the central region of the trunk and theproximal upper extremities; they are not usuallypainful, but are pruritic. The illness is usually ac-companied by low grade fever and malaise, andonce cutaneous signs appear the illness generallylasts about 1 week. In adults with primary varicellainfection, more skin lesions are usually present andthe fever and constitutional symptoms are more se-vere.[1] Varicella in adults usually resolves within1 to 3 weeks. VZV persists by a latent infection ofthe dorsal root ganglia.[4]Individuals who have had varicella can experi-
ence reactivation of the virus, leading to herpeszoster.[1] The trigger for reactivation is not known,but is likely to result from immunological senes-cence associated with aging or with immune sup-pression caused by therapy for other medical con-ditions, or HIV infection.[1,5] It has been suggestedthat the increasing age of the population in mostcountries will give rise to an increasing incidenceof herpes zoster over the next 20 years.[3]Unlike primary VZV infection herpes zoster is
restricted to 1 or 2 unilateral dermatomes. In 70 to90% of patients rash is preceded by pain (prodro-mal pain).[6-8] The acute rash of herpes zoster startsas an erythematous area that increases in sizewithin the dermatome(s). Maculopapular lesionsthen appear which develop into vesicles or fluidfilled blisters. These then collapse, forming ulcersthat crust over before healing and complete re-epithelialisation of the skin. In the majority of pa-tients, the zoster rash is accompanied by moderateto severe pain.[5] About 15% of patients developherpes zoster ophthalmicus from VZV reactivation
in the trigeminal ganglion, with release of virusparticles along the ophthalmic (first) branch. In ad-dition to pain, VZVmay penetrate ocular tissue andcause complications such as keratitis, uveitis andscleritis.[9,10]The lesions of herpes zoster usually resolve and
heal in 1 to 3 weeks. However, pain is often severeduring the acute rash phase and may persist formonths or years after rash healing. It is this post-herpetic neuralgia that is the most serious and de-bilitating complication of herpes zoster.[11] Theskin may also become unusually sensitive to touchand temperature. The pathophysiology of posther-petic neuralgia is not completely understood, butmay involve both peripheral and central degenera-tive changes as a result of earlier viral replica-tion.[12] The preferential destruction of nerve fibresinvolved in inhibitory pain modulating systems, fi-brosis and atrophy of dorsal horn and root ganglia,and ectopic activity in damaged afferent noci-ceptors have all been implicated.[12] VZVDNAandprotein have been found in blood mononuclearcells months to years after initial rash in patientsexperiencing postherpetic neuralgia. In patientswho do have postherpetic neuralgia, VZV DNA isonly present for a few weeks. Thus, a chronic in-flammatory response to infection is also a possiblecontributor to postherpetic neuralgia.[12] The sever-ity and duration of pain in herpes zoster appear tobe associated with increasing age and are thereforean escalating problem in the elderly.[3] The reduc-tion of pain during herpes zoster, and more impor-tantly prevention of persisting pain and post-herpetic neuralgia, are the primary goals of therapyin this disease.The mainstay of treatment for herpes zoster un-
til the mid 1990s was aciclovir. Although the sever-ity of the rash and pain of the acute phase of thedisease was improved with aciclovir therapy, theduration of postherpetic neuralgia was not signifi-cantly altered in clinical trials[13,14] (althoughmeta-analyses of up to 5 trials did report some ben-efit.[15-17]). The most likely reason for this lack ofsubstantial effect on postherpetic neuralgia is thatat the recommended dose (800mg 5 times daily) the
1322 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

serum concentrations of aciclovir are only just ad-equate to inhibit replication of VZV.[18] This in turnwould limit the potential for aciclovir to stop VZVreplication in the sensory nervous system, which ismore important for an impact on pain. Therefore,the rationale for developing newer antiviral drugs,such as the aciclovir prodrug valaciclovir and thepenciclovir prodrug famciclovir, is to produce muchhigher serumconcentrations of active antiviral agentswith the aim of reducing the duration and severityof postherpetic neuralgia.Valaciclovir is an antiviral agent with efficacy
against herpesvirus infections including those causedby HSV, Epstein-Barr virus (EBV), cytomegalovirus(CMV) andVZV.[19,20] Of these, HSV and VZV arethe most sensitive and CMV the least.Although there is interest in the potential use of
valaciclovir in immunocompromised children andadults with varicella,[21,22] this review focuses onthe efficacy and tolerability of valaciclovir in thetreatment of herpes zoster in immunocompetentadults.
2. Overview of Pharmacodynamic Properties
After oral administration valaciclovir is rapidlyhydrolysed (>99% hydrolysed) to the active moi-ety aciclovir and L-valine, a naturally occurringessential amino acid.[19] After valaciclovir admin-istration metabolites of aciclovir are produced atlow concentrations (<10%) and are pharmacolog-ically inactive (see section 3).[19,23] The pharmaco-dynamic properties of valaciclovir are the same asthose for aciclovir.[19,24] These properties have beenextensively reviewed in previously published arti-cles in Drugs[19,20,24] and the following brief dis-cussion focuses on the activity of aciclovir (fromvalaciclovir) against VZV.
2.1 Antiviral Activity
Aciclovir is phosphorylated by virus-encodedVZV or HSV thymidine kinase within the infectedhost cell to aciclovir monophosphate. Aciclovirmonophosphate preferentially accumulates in her-pesvirus-infected cells, where it undergoes further
phosphorylation by cellular enzymes to its activetriphosphate form.[19,23,24] This moiety competeswith 2′-deoxyguanosine as a substrate for the viralDNApolymerase, terminating enzyme activity im-mediately and also becoming incorporated (as aci-clovir monophosphate) into the viral DNA chain.Chain elongation is terminated upon incorporationof aciclovir triphosphate as it lacks the 3′-hydroxylgroup necessary for further nucleotide addi-tion.[19,25,26]The selective inhibition by aciclovir triphosphate
of the DNA polymerases of a range of herpes-viruses includes, in descending order of in vitrosusceptibility, HSV-1, HSV-2, VZV, EBV, humanherpesviruses 6, 8 and 7 and CMV.[24,27-30] Theconcentration of aciclovir needed for 50% inhibi-tion (IC50) of VZV in vitro is 0.12 to 10.8 mg/L.[26]According to IC50 values obtained in plaque re-
duction assays aciclovir triphosphate is a 100- to160-fold more potent inhibitor of VZV and HSVDNApolymerases in vivo than penciclovir triphos-phate (the active antiviral metabolite of famci-clovir, the prodrug of penciclovir).[19,31] In contrast,the affinity of aciclovir for the virus thymidinekinase is low compared with that of penciclovir.[32]Although aciclovir triphosphate has a shorter intra-cellular half-life and achieves lower concentra-tions in VZV- and HSV-infected cells than pen-ciclovir triphosphate, intracellular concentrationsof aciclovir triphosphate in cultured cells reached20 to 38 times the concentrations required for in-hibition of HSV DNApolymerase and remained inexcess of inhibitory levels for 4 to 6 hours.[19,23]In vitro studies have confirmed that the mecha-
nism of action of aciclovir involves the highly se-lective inhibition of herpesvirus DNApolymerase,but not cellular DNA polymerase, and that there isonly minimal phosphorylation of aciclovir by cel-lular enzymes.[19,23] Thus, aciclovir, and thereforevalaciclovir, has minimal effects on non-infectedhost cells.
2.2 Viral Resistance
The profile of VZV resistance to aciclovir afteradministration of valaciclovir is expected to be the
Valaciclovir in Herpes Zoster: A Review 1323
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

same as after administration of the parent drug(aciclovir).[19] VZV resistance in response to treat-ment with aciclovir is extremely rare in immuno-competent patients. Although still rare, there is anincreased incidence of aciclovir-resistant strains ofVZV in immunocompromised patients, most com-monly in HIV-infected individuals,[33-35] and morerarely in bone marrow transplant recipients.[35,36]The majority of VZV isolates with reduced sen-
sitivity to aciclovir are thymidine kinase defi-cient.[34,35,37] In these mutants, the virus-specificconversion of aciclovir to aciclovir monophos-phate by viral thymidine kinase is reduced or pre-vented.The extent of cross-resistance to other antiviral
agents is dependent upon the mode of action of theagent and nature of the mutations conferring resis-tance. In general, thymidine kinase-deficient vi-ruses are also resistant to other antiherpes agents(e.g. penciclovir) that are dependent on thymidinekinase for phosphorylation to the active form.[19,38]One in vitro study has examined the emergence ofviral resistance after exposure to aciclovir and pen-ciclovir.[37] Cultured human cells were infectedwith the Kawaguchi or Oka varicella vaccine strain,or a clinical isolate from a patient with herpes zoster,and exposed to 2, 4 or 6 mg/L of aciclovir or pen-ciclovir. In 11 of 12 experiments resistant viruseswere recovered only from aciclovir-treated cul-tures (p < 0.0001). The authors speculate that thedifference may be due to the shorter intracellularhalf-life of aciclovir triphosphate (0.8 hours) com-pared with penciclovir triphosphate (7 to 14 hours),which may result in a difference in selective pres-sure on VZV replication.[37] The hypothesis is thatprolonged growth in the presence of an antiviralagent increases the likelihood of resistant strainsarising. Because penciclovir may have suppressedviral growth more strongly than aciclovir underthese experimental conditions aciclovir might havepermitted the selection of thymidine kinase-resistantviruses. It is quite possible that strains resistant topenciclovir would also occur if the experimentalconditions were adjusted to allow prolonged growthin the presence of this agent. It should also be noted
that only 1 of the 3 strains tested was a clinicalisolate.It is also important to bear in mind that aciclovir
has been available for clinical use for nearly 20years, compared with about 5 years for pencicloviror famciclovir. The shorter resistance surveillanceprogramme for penciclovir may mean that therehas been insufficient opportunity to characterise itsresistance profile.While the lack of emergence of aciclovir-resistant
strains of VZV in immunocompetent patients is en-couraging, it is only with even further usage of val-aciclovir and aciclovir may the true incidence ofaciclovir-resistant VZV viruses in this group be es-timated. Continued surveillance for herpesvirusresistance to aciclovir and penciclovir is ongoingthrough theTaskForceonHerpesvirusResistance.[39]
3. Pharmacokinetic Properties
The pharmacokinetic properties of oral valaci-clovir in healthy volunteers and in various patientgroups (e.g. patients with advanced HIV disease,elderly patients and transplant recipients) havebeen reviewed previously inDrugs.[19] This sectionprovides a summary of some of these data togetherwith results of more recent studies. Most informationon the pharmacokinetics of valaciclovir relates toits single dose absorption profile. Ageneral summaryof the pharmacokinetic properties of valaciclovir(and aciclovir) is shown in table I. The pharmaco-kinetics of valaciclovir in healthy elderly volun-teers,[47] patients with HIV infection,[48,49] patientswith liver disease[26] and transplant recipients[50]are broadly similar to those in healthy volunteers.No clinically significant interactions between val-aciclovir and coadministered drugs (including ci-metidine, probenecid, digoxin, antacids or thiazidediuretics) have been reported.[19] Valaciclovir canbe administered with food.[19]
3.1 Absorption and Distribution
Valaciclovir is well absorbed after oral admin-istration and undergoes first-pass intestinal and/orhepatic metabolism to produce aciclovir, the anti-
1324 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
viral metabolite, and L-valine, an essential aminoacid.[42,43,51]After oral administration, valaciclovir is better
absorbed through the wall of the gastrointestinaltract than oral aciclovir. This may be because trans-port-mediated uptake of aciclovir into intestinalmembranes occurs more rapidly with valaciclovirthan with aciclovir (reviewed previously[19]). Im-portantly, the absolute bioavailability of aciclovirafter oral administration of oral valaciclovir ismarkedly greater than that achieved after oralaciclovir (54% for aciclovir after valaciclovir ver-sus 12 to 20% for aciclovir after aciclovir).[40,42] Inpatients with herpes zoster treated with oralvalaciclovir 1000mg 3 times daily the estimatedbioavailability of aciclovir was approximately 4times greater than after aciclovir 800mg 5 timesdaily in a comparator group.[7]Mean maximum plasma aciclovir concentra-
tions (Cmax) and area under the plasma aciclovirconcentration-time curve (AUC) values increasedin a less than dose-proportional (non-linear) man-ner in healthy adult volunteers who received oralaciclovir as single 100 to 1000mg doses ormultipledoses of 250 to 2000mg 4 times daily for 11days.[42] After single 100 to 1000mg doses of vala-ciclovir, aciclovir Cmax values ranged from 0.83 to
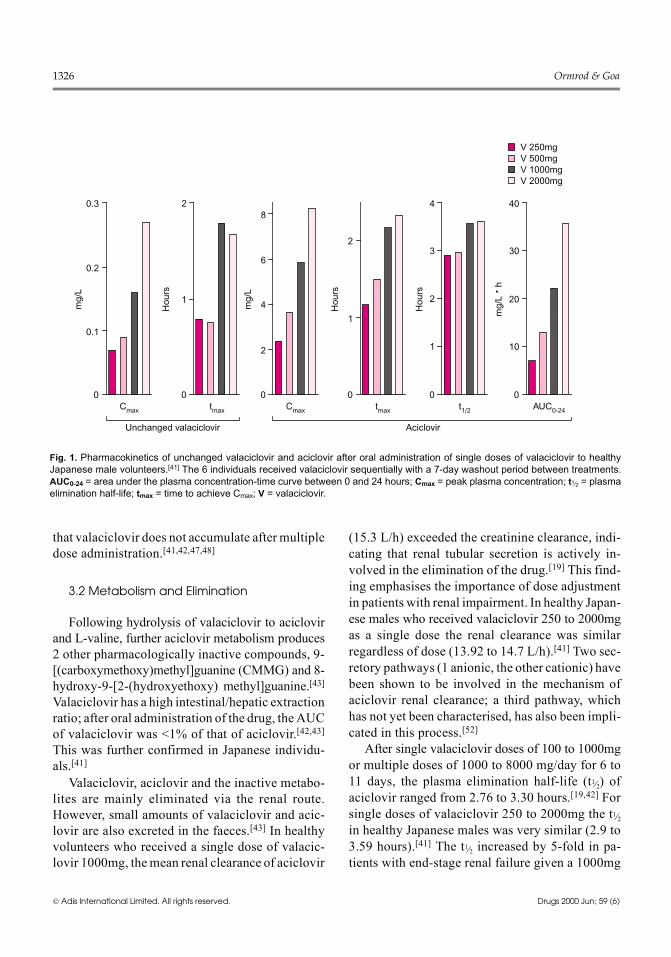
5.65mg/L; mean time to achieve Cmax (tmax) rangedfrom 0.88 to 1.75 hours; AUC values ranged from2.28 to 19.52 mg/L • h. The aciclovir AUC to 24hours (systemic exposure) achieved with vala-ciclovir 250mg 4 times daily was similar to thatachieved with oral aciclovir 800mg 5 times daily(23 vs 24 mg/L • h).[42] A phase I study in healthyJapanese male volunteers also demonstrated non-linear kinetics over the dose range 250 to 2000mg(fig. 1).[41] In a population pharmacokinetic analy-sis of patients with herpes zoster treated withvalaciclovir 1000mg 3 times daily the Cmax was5.73 mg/L (range 2.76 to 16.1 mg/L) and the esti-mated dailymeanAUC for aciclovir was 88.6mg/L• h.[7] These values were 2.5- and 2-fold higher, re-spectively, than in patients given aciclovir 800mg5 times daily.Valaciclovir and aciclovir bind to plasma pro-
teins only to a limited extent (table I).[26,44] Thevolume of distribution of aciclovir was similar inadults with normal renal function and those withrenal impairment.[44] In patients with cirrhosis therate, but not the extent, of conversion of valacic-lovir to aciclovir was reduced.[40] There is strongevidence from the extensive series of pharmacoki-netic studies conducted in the USA, UK and Japan,in healthy adult volunteers or patient populations,
Table I. Summary of some of the pharmacokinetic parameters of valaciclovir (and aciclovir after administration of valaciclovir) in adult Japaneseor Western volunteers who received a single oral dose of valaciclovir 1000mg; mean values ± standard error from n = 6 to 38 individualspresented[40-46]
Valaciclovir Aciclovir
Japanese Western
Absorption and distribution
Bioavailability (%) 54
Cmax (mg/L) 0.16±0.03 5.84±1.08 5.65±2.37
tmax (h) 1.79±0.90 2.17±0.61 1.75±0.63
AUC (mg/L • h) 22.07±5.71 19.52±6.04
Plasma protein binding (%) 13.5 - 17.9 22.0 - 33.0
Metabolism and elimination
Vd (L/1.73m2) 49.7
CLR (L/h) 13.92±1.56 15.32±5.15
t1⁄2 in volunteers with normal renal function (h) 3.55±0.27 3.03±0.13
t1⁄2 in ESRD (h) 14.4
AUC = area under the plasma concentration-time curve; CLR = renal clearance from the plasma; Cmax = maximum plasma concentration;ESRD = end stage renal disease; t1⁄2 = plasma elimination half-life; tmax = time to Cmax; Vd = volume of distribution.
Valaciclovir in Herpes Zoster: A Review 1325
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
that valaciclovir does not accumulate after multipledose administration.[41,42,47,48]
3.2 Metabolism and Elimination
Following hydrolysis of valaciclovir to aciclovirand L-valine, further aciclovir metabolism produces2 other pharmacologically inactive compounds, 9-[(carboxymethoxy)methyl]guanine (CMMG) and 8-hydroxy-9-[2-(hydroxyethoxy) methyl]guanine.[43]Valaciclovir has a high intestinal/hepatic extractionratio; after oral administration of the drug, theAUCof valaciclovir was <1% of that of aciclovir.[42,43]This was further confirmed in Japanese individu-als.[41]Valaciclovir, aciclovir and the inactive metabo-
lites are mainly eliminated via the renal route.However, small amounts of valaciclovir and acic-lovir are also excreted in the faeces.[43] In healthyvolunteers who received a single dose of valacic-lovir 1000mg, themean renal clearance of aciclovir
(15.3 L/h) exceeded the creatinine clearance, indi-cating that renal tubular secretion is actively in-volved in the elimination of the drug.[19] This find-ing emphasises the importance of dose adjustmentin patients with renal impairment. In healthy Japan-ese males who received valaciclovir 250 to 2000mgas a single dose the renal clearance was similarregardless of dose (13.92 to 14.7 L/h).[41] Two sec-retory pathways (1 anionic, the other cationic) havebeen shown to be involved in the mechanism ofaciclovir renal clearance; a third pathway, whichhas not yet been characterised, has also been impli-cated in this process.[52]After single valaciclovir doses of 100 to 1000mg
or multiple doses of 1000 to 8000 mg/day for 6 to11 days, the plasma elimination half-life (t1⁄2) ofaciclovir ranged from 2.76 to 3.30 hours.[19,42] Forsingle doses of valaciclovir 250 to 2000mg the t1⁄2in healthy Japanese males was very similar (2.9 to3.59 hours).[41] The t1⁄2 increased by 5-fold in pa-tients with end-stage renal failure given a 1000mg
0
0.1
0.2
0.3
mg/
L
0
1
2
Hou
rs
0
2
4
6
8
mg/
L
0
1
2
Hou
rs
0
1
2
3
4
Hou
rs
0
10
20
30
40
mg/
L ·
h
Cmax tmax Cmax tmax t1/2 AUC0-24
Unchanged valaciclovir Aciclovir
V 250mgV 500mgV 1000mgV 2000mg
Fig. 1. Pharmacokinetics of unchanged valaciclovir and aciclovir after oral administration of single doses of valaciclovir to healthyJapanese male volunteers.[41] The 6 individuals received valaciclovir sequentially with a 7-day washout period between treatments.AUC0-24 = area under the plasma concentration-time curve between 0 and 24 hours; Cmax = peak plasma concentration; t1⁄2 = plasmaelimination half-life; tmax = time to achieve Cmax; V = valaciclovir.
1326 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

dose of valaciclovir.[40] Thus, dosage adjustmentproportionate to renal impairment is required[26,53,54](see section 6).
4. Therapeutic Efficacy
The worldwide approval of valaciclovir for thetreatment of herpes zoster in immunocompetentadults was based on the results of 2 randomiseddouble-blind clinical trials involving a total of1538 patients with localised herpes zoster.[7,55,56]One of these compared valaciclovir with pla-cebo[55,56] and the other valaciclovir with acic-lovir.[7] Since then a number of follow-up studieshave reinforced the conclusion that valaciclovir isan effective agent for the management of herpeszoster. These include noncomparative and phase II,III studies in Japanese patients,[57-60] a large inter-national observational study in a wide range ofclinical settings,[61] a preliminary investigation oftwice daily administration of valaciclovir,[62] and acomparison of valaciclovir versus aciclovir forherpes zoster ophthalmicus.[63] Additionally, sup-plementary analyses of the original 2 studies havebeen published and these examined pharmaco-economic outcomes,[64] prognostic factors to iden-tify those patients at increased risk of prolongedpain and postherpetic neuralgia,[61,65] and timing oftherapy in relation to time to resolution of pain.[66]Finally, the results of a large study comparingvalaciclovir and famciclovir in herpes zoster havebeen published in abstract form.[67]
4.1 Assessment of Pain in Herpes Zoster
As outlined in section 1, pain invariably accom-panies acute herpes zoster and in some patients itextends well beyond rash healing. This is knownas postherpetic neuralgia, and shortening the dura-tion of this pain should be the primary objective ofstudies of treatment of herpes zoster. From the pa-tient’s point of view, for those developing post-herpetic neuralgia, the pain is a continuum.[19,68]Therefore many studies have also used the totalduration of pain from rash onset as an end point(known as zoster-associated pain). While zoster-associated pain in herpes zoster clinical trials is a
statistically more robust end-point, therapeuticoutcome is more meaningful in clinical terms if itrelates to postherpetic neuralgia. Therefore, the mostuseful trials present analyses of both end points.For a detailed discussion of issues surrounding as-sessment of zoster-associated pain and postherpeticneuralgia, the reader is referred to the papers byDworkin et al.[69] and Wood et al.[68]
4.2 Compared with Aciclovir, Famciclovirand/or Placebo
4.2.1 Herpes ZosterOne pivotal trial of oral valaciclovir in herpes
zoster was a multicentre, double-blind, random-ised placebo-controlled comparison of valacic-lovir 1000mg 3 times daily for 7 days with placebo.To date the results of this trial have been publishedonly in abstract form[55,56] or included in a meta-analysis.[65] 400 immunocompetent patients agedbetween 18 and 50 years were enrolled. Vala-ciclovir was more effective than placebo in reduc-ing the duration of new lesion formation (p =0.009), a surrogate measure of ongoing VZV rep-lication.[56] The trial protocol also specified thetime to ≥50% crusting or healing of lesions andduration of zoster-associated pain as primary end-points,[55] but these data have not yet been re-ported.The second multicentre, randomised, double-
blind trial has been published in full.[7] This studycompared oral valaciclovir 1000mg 3 times dailyfor 7 or 14 days with a standard dose of oral aci-clovir (800mg 5 times daily for 7 days) in 1141 im-munocompetent patients (≥50 years of age) withherpes zoster. Therapy was initiated within 72hours of the appearance of zoster rash. Primaryend-points were time to the complete cessation ofzoster-associated pain, time to cessation of new le-sion formation and/or increase in lesion area, andtime to ≥50% crusting or healed rash. Pain wasquantified and recorded by the patient daily ondays 1 to 30 and weekly thereafter. Cessation ofpain was defined as ≥28 days without pain and nosubsequent pain recurrence during the 24-weekfollow-up period. All patients were followed up for
Valaciclovir in Herpes Zoster: A Review 1327
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

24 weeks in order to conduct formal statisticalanalyses of the duration of zoster-associated painand postherpetic neuralgia.Results show that, although effects on rash were
similar for all treatments, both regimens of vala-ciclovir alleviated pain significantly faster thanaciclovir. The median duration of rash after initia-tion of treatment was 3 days for all 3 groups, andthe median time to ≥50% crusting or healed rashwas 5 days regardless of treatment. The hazard ra-tios were close to 1 for these acute (rash) end-points.[7]Of clinical importance is that treatment with va-
laciclovir significantly hastened the resolution ofzoster-associated pain compared with aciclovir. Onthe basis of hazard ratio analysis, zoster-associatedpain resolved 34 and 22% more quickly in patientstreated with valaciclovir for 7 (p = 0.001) and 14(p = 0.03) days, respectively, than in those receiv-ing aciclovir.[7] The median duration of pain was38, 44 and 51 days, respectively, for valaciclovir 7and 14 days and aciclovir. There was no statisticaldifference between valaciclovir for 7 or 14 days onthe duration of zoster-associated pain. Median du-ration of postherpetic neuralgia was 30, 35 and 39days for valaciclovir 7 and 14 days and aciclovir,respectively. At the end of the study (week 24) theprevalence of postherpetic neuralgia was lower af-ter valaciclovir treatment than after aciclovir: 25.7%of patients who had received aciclovir were stillexperiencing pain versus 19.9% of those who re-ceived valaciclovir for 7 days (p = 0.08 vs aciclovir)and 18.6% of those treated with valaciclovir for 14days (p = 0.02 vs aciclovir). When data from the 7-and 14-day valaciclovir-treated patientswerepooled,19.3% of patients were still experiencing pain ver-sus 25.7% of aciclovir recipients (p = 0.02).[7,19]The duration of abnormal sensations, e.g. hyper-
sensitivity, numbness and allodynia, was also shorterin valaciclovir recipients. The duration of abnor-mal sensations was 45 and 38 days, respectively,for valaciclovir 7 and 14 days, and 57 days for aci-clovir.[7]Two indices of postherpetic neuralgia were used
in this study: pain which persisted after resolution
of rash and pain which persisted from 30 days afterrash onset. When the former was analysed, painresolved significantly faster in both valaciclovir-treated groups compared with the aciclovir-treatedgroup (p = 0.002 and 0.03 for valaciclovir 7 and 14days, respectively). For pain which persisted from30 days after rash onset valaciclovir was again bet-ter than aciclovir, and was significant for the 7-daytreatment group (p = 0.001). Treatment-relatedtrends for pain intensity were not detected.[7] Theincidence of complications was low and similar forall groups.[7]A series of trials has also been carried out in
Japanese patients with herpes zoster. A noncom-parative study[59] and 2 phase II studies[57,58] estab-lished the tolerability and a suitable dosage of val-aciclovir in this group of patients. The optimumvalaciclovir dosage regimen identified in thesedose-ranging studies (1000mg 3 times daily for 7days) was then compared in a randomised, double-blind, multicentre study with aciclovir 800mg 5times daily for 7 days.[60] 202 patients were en-rolled in the study and 200 of these were includedin the intent-to-treat (ITT) analysis (102 receivedvalaciclovir and 98 aciclovir). Patients were mon-itored for 2 weeks after completion of therapy, butif pain persisted follow-up examinations were con-ducted (where possible) at monthly intervals untilpain disappeared, or up to 6 months after studycommencement. The severity and progression ofskin rash were defined in terms of erythema/papule, vesicle/pustule, erosion/ulcer and crust andscored on a 5-point grade system where 0 indicated‘none’ for a particular symptom and 4 indicated‘very severe’. Overall improvement of lesions wasquantified using a similar, but 6-point, system. Themethodology was not described for the analysis ofzoster-associated pain and postherpetic pain. ‘Effi-cacy’ and ‘usefulness’ were also measured andquantified using 6-point scales where 1 equated to‘excellent’ for ‘efficacy’, or to ‘very useful’ for‘usefulness’. The presence of virus in skin lesionswas assessed by immunofluorescence using amonoclonal antibody against VZV.
1328 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
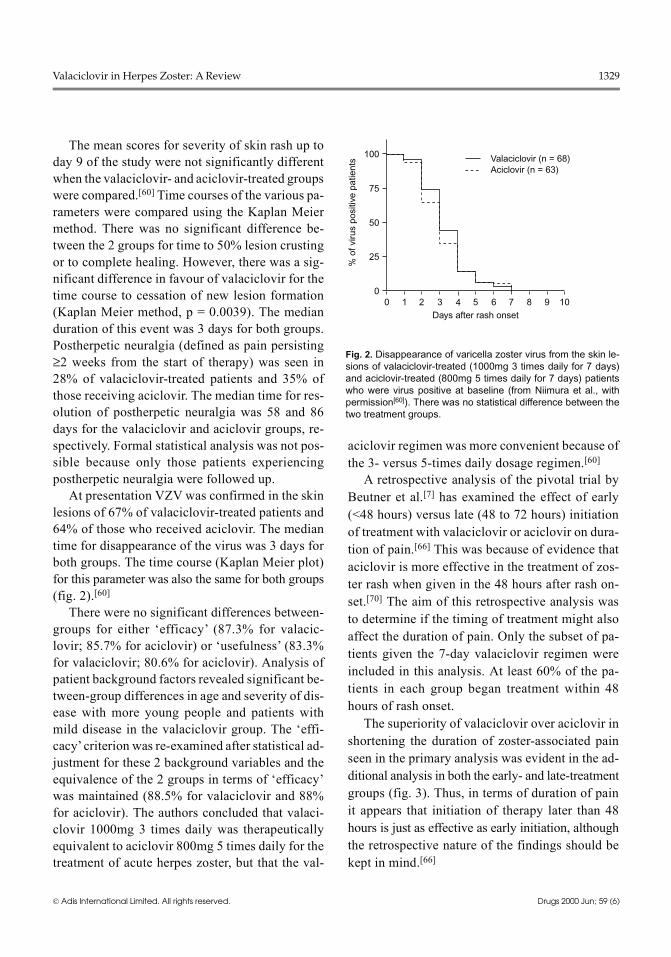
The mean scores for severity of skin rash up today 9 of the study were not significantly differentwhen the valaciclovir- and aciclovir-treated groupswere compared.[60] Time courses of the various pa-rameters were compared using the Kaplan Meiermethod. There was no significant difference be-tween the 2 groups for time to 50% lesion crustingor to complete healing. However, there was a sig-nificant difference in favour of valaciclovir for thetime course to cessation of new lesion formation(Kaplan Meier method, p = 0.0039). The medianduration of this event was 3 days for both groups.Postherpetic neuralgia (defined as pain persisting≥2 weeks from the start of therapy) was seen in28% of valaciclovir-treated patients and 35% ofthose receiving aciclovir. The median time for res-olution of postherpetic neuralgia was 58 and 86days for the valaciclovir and aciclovir groups, re-spectively. Formal statistical analysis was not pos-sible because only those patients experiencingpostherpetic neuralgia were followed up.At presentation VZV was confirmed in the skin
lesions of 67% of valaciclovir-treated patients and64% of those who received aciclovir. The mediantime for disappearance of the virus was 3 days forboth groups. The time course (Kaplan Meier plot)for this parameter was also the same for both groups(fig. 2).[60]There were no significant differences between-
groups for either ‘efficacy’ (87.3% for valacic-lovir; 85.7% for aciclovir) or ‘usefulness’ (83.3%for valaciclovir; 80.6% for aciclovir). Analysis ofpatient background factors revealed significant be-tween-group differences in age and severity of dis-ease with more young people and patients withmild disease in the valaciclovir group. The ‘effi-cacy’criterion was re-examined after statistical ad-justment for these 2 background variables and theequivalence of the 2 groups in terms of ‘efficacy’was maintained (88.5% for valaciclovir and 88%for aciclovir). The authors concluded that valaci-clovir 1000mg 3 times daily was therapeuticallyequivalent to aciclovir 800mg 5 times daily for thetreatment of acute herpes zoster, but that the val-
aciclovir regimen was more convenient because ofthe 3- versus 5-times daily dosage regimen.[60]A retrospective analysis of the pivotal trial by
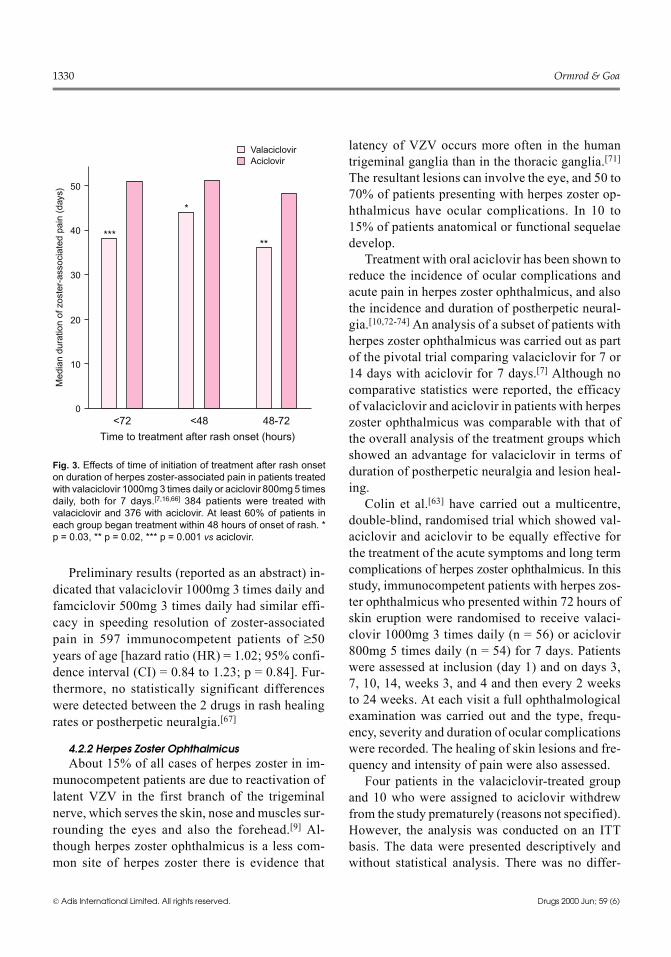
Beutner et al.[7] has examined the effect of early(<48 hours) versus late (48 to 72 hours) initiationof treatment with valaciclovir or aciclovir on dura-tion of pain.[66] This was because of evidence thataciclovir is more effective in the treatment of zos-ter rash when given in the 48 hours after rash on-set.[70] The aim of this retrospective analysis wasto determine if the timing of treatment might alsoaffect the duration of pain. Only the subset of pa-tients given the 7-day valaciclovir regimen wereincluded in this analysis. At least 60% of the pa-tients in each group began treatment within 48hours of rash onset.The superiority of valaciclovir over aciclovir in
shortening the duration of zoster-associated painseen in the primary analysis was evident in the ad-ditional analysis in both the early- and late-treatmentgroups (fig. 3). Thus, in terms of duration of painit appears that initiation of therapy later than 48hours is just as effective as early initiation, althoughthe retrospective nature of the findings should bekept in mind.[66]
% o
f viru
s po
sitiv
e pa
tient
s
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10Days after rash onset
Valaciclovir (n = 68)Aciclovir (n = 63)
Fig. 2. Disappearance of varicella zoster virus from the skin le-sions of valaciclovir-treated (1000mg 3 times daily for 7 days)and aciclovir-treated (800mg 5 times daily for 7 days) patientswho were virus positive at baseline (from Niimura et al., withpermission[60]). There was no statistical difference between thetwo treatment groups.
Valaciclovir in Herpes Zoster: A Review 1329
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
Preliminary results (reported as an abstract) in-dicated that valaciclovir 1000mg 3 times daily andfamciclovir 500mg 3 times daily had similar effi-cacy in speeding resolution of zoster-associatedpain in 597 immunocompetent patients of ≥50years of age [hazard ratio (HR) = 1.02; 95% confi-dence interval (CI) = 0.84 to 1.23; p = 0.84]. Fur-thermore, no statistically significant differenceswere detected between the 2 drugs in rash healingrates or postherpetic neuralgia.[67]
4.2.2 Herpes Zoster OphthalmicusAbout 15% of all cases of herpes zoster in im-
munocompetent patients are due to reactivation oflatent VZV in the first branch of the trigeminalnerve, which serves the skin, nose and muscles sur-rounding the eyes and also the forehead.[9] Al-though herpes zoster ophthalmicus is a less com-mon site of herpes zoster there is evidence that
latency of VZV occurs more often in the humantrigeminal ganglia than in the thoracic ganglia.[71]The resultant lesions can involve the eye, and 50 to70% of patients presenting with herpes zoster op-hthalmicus have ocular complications. In 10 to15% of patients anatomical or functional sequelaedevelop.Treatment with oral aciclovir has been shown to
reduce the incidence of ocular complications andacute pain in herpes zoster ophthalmicus, and alsothe incidence and duration of postherpetic neural-gia.[10,72-74] An analysis of a subset of patients withherpes zoster ophthalmicus was carried out as partof the pivotal trial comparing valaciclovir for 7 or14 days with aciclovir for 7 days.[7] Although nocomparative statistics were reported, the efficacyof valaciclovir and aciclovir in patients with herpeszoster ophthalmicus was comparable with that ofthe overall analysis of the treatment groups whichshowed an advantage for valaciclovir in terms ofduration of postherpetic neuralgia and lesion heal-ing.Colin et al.[63] have carried out a multicentre,
double-blind, randomised trial which showed val-aciclovir and aciclovir to be equally effective forthe treatment of the acute symptoms and long termcomplications of herpes zoster ophthalmicus. In thisstudy, immunocompetent patients with herpes zos-ter ophthalmicus who presented within 72 hours ofskin eruption were randomised to receive valaci-clovir 1000mg 3 times daily (n = 56) or aciclovir800mg 5 times daily (n = 54) for 7 days. Patientswere assessed at inclusion (day 1) and on days 3,7, 10, 14, weeks 3, and 4 and then every 2 weeksto 24 weeks. At each visit a full ophthalmologicalexamination was carried out and the type, frequ-ency, severity and duration of ocular complicationswere recorded. The healing of skin lesions and fre-quency and intensity of pain were also assessed.Four patients in the valaciclovir-treated group
and 10 who were assigned to aciclovir withdrewfrom the study prematurely (reasons not specified).However, the analysis was conducted on an ITTbasis. The data were presented descriptively andwithout statistical analysis. There was no differ-
0
10
20
30
40
50
Med
ian
dura
tion
of z
oste
r-as
soci
ated
pai
n (d
ays)
***
*
**
<72 <48 48-72
Time to treatment after rash onset (hours)
ValaciclovirAciclovir
Fig. 3. Effects of time of initiation of treatment after rash onseton duration of herpes zoster-associated pain in patients treatedwith valaciclovir 1000mg 3 times daily or aciclovir 800mg 5 timesdaily, both for 7 days.[7,16,66] 384 patients were treated withvalaciclovir and 376 with aciclovir. At least 60% of patients ineach group began treatment within 48 hours of onset of rash. *p = 0.03, ** p = 0.02, *** p = 0.001 vs aciclovir.
1330 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
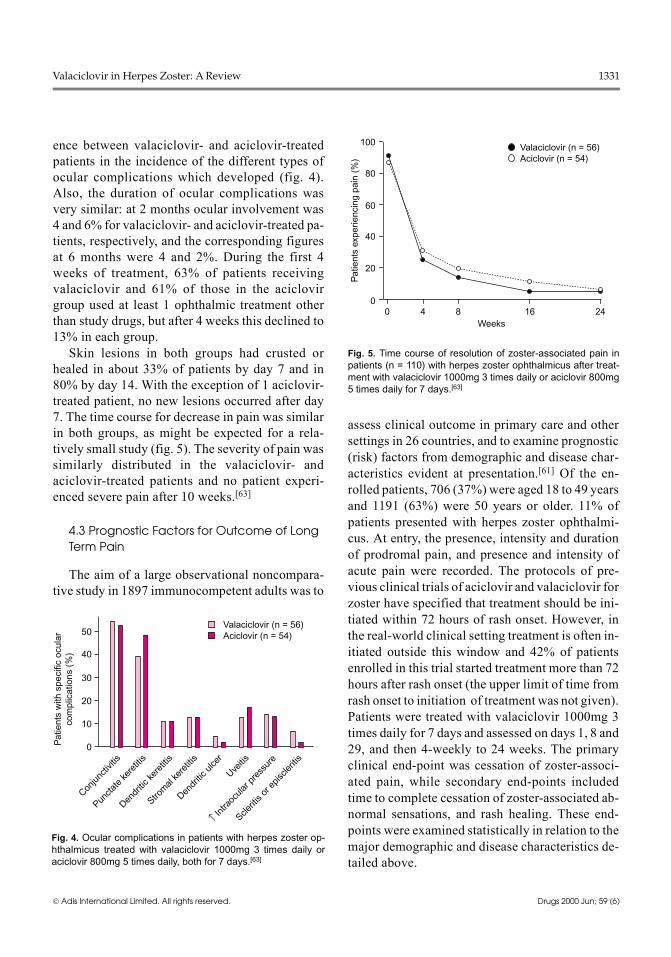
ence between valaciclovir- and aciclovir-treatedpatients in the incidence of the different types ofocular complications which developed (fig. 4).Also, the duration of ocular complications wasvery similar: at 2 months ocular involvement was4 and 6% for valaciclovir- and aciclovir-treated pa-tients, respectively, and the corresponding figuresat 6 months were 4 and 2%. During the first 4weeks of treatment, 63% of patients receivingvalaciclovir and 61% of those in the aciclovirgroup used at least 1 ophthalmic treatment otherthan study drugs, but after 4 weeks this declined to13% in each group.Skin lesions in both groups had crusted or
healed in about 33% of patients by day 7 and in80% by day 14. With the exception of 1 aciclovir-treated patient, no new lesions occurred after day7. The time course for decrease in pain was similarin both groups, as might be expected for a rela-tively small study (fig. 5). The severity of pain wassimilarly distributed in the valaciclovir- andaciclovir-treated patients and no patient experi-enced severe pain after 10 weeks.[63]
4.3 Prognostic Factors for Outcome of LongTerm Pain
The aim of a large observational noncompara-tive study in 1897 immunocompetent adults was to
assess clinical outcome in primary care and othersettings in 26 countries, and to examine prognostic(risk) factors from demographic and disease char-acteristics evident at presentation.[61] Of the en-rolled patients, 706 (37%) were aged 18 to 49 yearsand 1191 (63%) were 50 years or older. 11% ofpatients presented with herpes zoster ophthalmi-cus. At entry, the presence, intensity and durationof prodromal pain, and presence and intensity ofacute pain were recorded. The protocols of pre-vious clinical trials of aciclovir and valaciclovir forzoster have specified that treatment should be ini-tiated within 72 hours of rash onset. However, inthe real-world clinical setting treatment is often in-itiated outside this window and 42% of patientsenrolled in this trial started treatment more than 72hours after rash onset (the upper limit of time fromrash onset to initiation of treatment was not given).Patients were treated with valaciclovir 1000mg 3times daily for 7 days and assessed on days 1, 8 and29, and then 4-weekly to 24 weeks. The primaryclinical end-point was cessation of zoster-associ-ated pain, while secondary end-points includedtime to complete cessation of zoster-associated ab-normal sensations, and rash healing. These end-points were examined statistically in relation to themajor demographic and disease characteristics de-tailed above.
00 4 8 16 24
20
40
60
80
100
Pat
ient
s ex
perie
ncin
g pa
in (
%)
Weeks
Valaciclovir (n = 56)Aciclovir (n = 54)
Fig. 5. Time course of resolution of zoster-associated pain inpatients (n = 110) with herpes zoster ophthalmicus after treat-ment with valaciclovir 1000mg 3 times daily or aciclovir 800mg5 times daily for 7 days.[63]
Pat
ient
s w
ith s
peci
fic o
cula
rco
mpl
icat
ions
(%
)
0
10
20
30
40
50Valaciclovir (n = 56)Aciclovir (n = 54)
Conjun
ctivit
is
Puncta
te ke
retiti
s
Dendr
itic ke
retiti
s
Strom
al ke
retiti
s
Dendr
itic u
lcer
Uveitis
↑ Intra
ocula
r pre
ssur
e
Sclerit
is or
epis
clerit
is
Fig. 4. Ocular complications in patients with herpes zoster op-hthalmicus treated with valaciclovir 1000mg 3 times daily oraciclovir 800mg 5 times daily, both for 7 days.[63]
Valaciclovir in Herpes Zoster: A Review 1331
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

There was a strong association between the du-ration of zoster-associated pain and the age of thepatients, and pain resolved almost twice as rapidlyin patients aged between 18 and 49 years as in those≥50 years (HR = 1.91; CI = 1.71 to 2.12; p <0.0001).[61] 11% of patients in the older age groupstill had pain at the end of the study compared withonly 2% in the younger age group. Abnormal sen-sations also ceased significantly earlier in patientsyounger than 50 years: 16 vs 31 days (HR = 1.68;95% CI = 1.50 to 1.88; p < 0.0001).The time to resolution of pain in patients with
herpes zoster ophthalmicus was not significantlydifferent overall from that in patients with non-ophthalmic zoster. However, there was a tendencyfor pain resolution to slow down at the later time-points in patients with herpes zoster ophthalmicus;at 6 months zoster-associated pain was still presentin 12% of those with, versus 7% of those without,herpes zoster ophthalmicus. Also, there was a sta-tistically significant difference when the durationof abnormal sensations in patients with non-oph-thalmic zoster and ophthalmic zoster were com-pared, and these resolved ≈40%more rapidly in thenon-ophthalmic zoster group (HR = 1.4; 95% CI =1.16 to 1.69; p = 0.0004).[61]A multivariate analysis revealed that the inten-
sity of prodromal pain was a significant risk factorfor more prolonged zoster-associated pain. For noto mild versus moderate prodromal pain the HRwas 1.3 (95% CI = 1.12 to 1.52; p = 0.0008), whilefor no to mild versus severe to very severe prodro-mal pain the HR was 1.78 (95% CI = 1.53 to 2.07;p < 0.0001).[61] However, in contrast to the findingsof controlled double-blind studies by Beutner[7]and others,[75,76] the simple presence or absence ofprodromal pain was not specifically a risk factorfor more prolonged zoster-associated pain.[61] Whenthe risk of prolonged zoster-associated abnormalsensations was analysed in the same way the severityof prodromal pain was again found to be a signifi-cant prognostic factor. Interestingly, patients withpre-existing neurological disorders were also at agreater risk of prolonged zoster-associated abnor-
mal sensations (HR = 1.55; 95% CI = 1.26 to 1.91;p < 0.0001).[61]In terms of the therapeutic value of valaciclovir
in the treatment of zoster, an interesting finding ofthis study was that the time to cessation of pain andabnormal sensations was not significantly affectedwhen therapy was initiated more than 72 hours af-ter rash onset. The median time to cessation of painwas 16 and 15 days, respectively, in patients whosetreatment was initiated ≤72 hours and >72 hoursafter rash onset. The corresponding values for ces-sation of abnormal sensations were 24 and 22days.[61] It would be useful to know the maximumtime from rash onset to initiation of treatment, butthis information could not be derived from a trialof this design. Patients with ophthalmic and non-ophthalmic zoster were not analysed separately soit is not possible to say whether the finding appliedequally to both groups of patients. Also, patientsstarting therapy earlier may have been older andhad more significant symptoms earlier. These pa-tients would be more likely to seek medical careearly and be more prone to prolonged pain thanthose seeking treatment later.[61]Further analysis of the two pivotal valaciclovir
clinical trials[7,55,56] and 4 aciclovir trials have alsoexamined potential risk factors for persistent painin patients with herpes zoster.[65] In general the re-sults were consistent with those of the non-comparative study of Decroix et al.[61] Age againhad a strong influence on pain outcome and pa-tients ≥50 were significantly more likely to haveprolonged zoster-associated pain than younger pa-tients. Prodromal pain and moderate to severe painat presentation were also predictive for prolongedzoster-associated pain. The risk of persistent painwas increased by the presence of two or more riskfactors. Duration of pain was not influenced bytime to initiation of treatment after rash onset or thesex of the patient.[65]
4.4 Exploratory Dose Regimens
The thrice daily valaciclovir regimen used totreat zoster should confer a compliance advantageover the 5 times daily regimen employed when oral
1332 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

aciclovir is prescribed.[7] Twice daily administra-tion may be even more convenient for the patient,and Severson et al.[62] have examined the efficacyand tolerability of valaciclovir 1500mg twice dailyfor the treatment of acute herpes zoster in a non-comparative trial and have published the results inan abstract. 58 immunocompetent patients wereenrolled and all received valaciclovir 1500mgtwice daily, initiated within 72 hours of rash onsetand continued for 7 days. Duration of pain, the pri-mary end-point, was 43 days in patients ≥50 yearsand 36 days in those >18 but <50 years of age. Themedian time to the secondary end-point, loss ofcrusts (complete cutaneous healing), was 20 daysin both age groups.It is not possible from these limited data to say
whether a twice daily valaciclovir regimen of1500mg is as effective as the standard 1000mg 3times daily regimen. An appropriately poweredstudy comparing the 2 regimens, and utilising es-tablished end-points for rash healing (≥50%) andfollow-up to 6 months for postherpetic neuralgiawould be required.
4.5 Pharmacoeconomic Issues
Data from the pivotal trial comparing valacic-lovir and aciclovir treatment for 7 days were usedto model the costs and consequences of treatingherpes zoster.[64] The model used considered bothdirect medical costs (acquisition of antiherpesdrugs and pain relief medication, doctors’ visits,long term pain relief and cost of treating severeocular complications) and indirect medical costs;the latter were based on the loss of earnings forpatients in paid employment (27.5% of the studypopulation). Because herpes zoster is an acute dis-ease costs were not discounted, except for the cal-culation of lifetime costs of treating long term pain.The perspective of the study was US society as awhole and a baseline case to cost analysis modelwas used.The total direct costs per patient were $US298.38
and $US358.39 for valaciclovir and aciclovir, re-spectively. When indirect costs were included, thetotal costs were $US437.74 for valaciclovir and
US$544.29 for aciclovir. Therefore, compared withaciclovir, valaciclovir reduced direct medical costsby 17%, indirect costs by 25% and total direct andindirect costs by 20%.[64]It is important to note that since this study was
published generic aciclovir has become availableand these cost savings are likely to be affected[77](a 7-day course of generic aciclovir now costsaround US$70 compared with about US$130 forbranded aciclovir). According to sensitivity analy-sis, once the cost of aciclovir relative to baselinefalls below about 50% the overall cost advantageof valaciclovir is lost. However, cost effectivenessanalysis revealed that even if the cost of aciclovirfell to zero the additional direct medical cost ofmanaging a case of herpes zoster would be $US5.30for each additional day of pain.[64] Therefore, val-aciclovir would still be considered cost effective.
4.6 Quality of Life
Quality of life (QOL) is significantly affectedby herpes zoster, particularly in terms of pain, dis-ruption of sleep and loss of energy,[7] and the influ-ence of valaciclovir for 7 or 14 days and aciclovirfor 7 days on QOL has been reported.[7] QOL scoreswere generally improved for valaciclovir over aci-clovir. However, the power of the study was notsufficient for formal statistical testing of treatmentdifferences. At 30 days the pain scores (with standarderrors) were 19.2 (1.6), 15.5 (1.4) and 20.4 (1.6)for 7- and 14-day valaciclovir and aciclovir, re-spectively.
5. Tolerability
Oral valaciclovir is well tolerated with an ad-verse event profile similar to that of oral aciclo-vir.[25,78] The tolerability of short term (1 to 30 days)administration of valaciclovir has been investig-ated in healthy young[42] and elderly volunteers[47]and in patients with HIV infection,[48] genital HSVinfection,[79-82] or herpes zoster.[7] Valaciclovir isalso used as suppressive therapy for HSV infectionin immunocompetent patients and forHSVandCMVinfection in immunocompromised patients.[20] Thetolerability of both acute and long term (≥90 days)
Valaciclovir in Herpes Zoster: A Review 1333
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
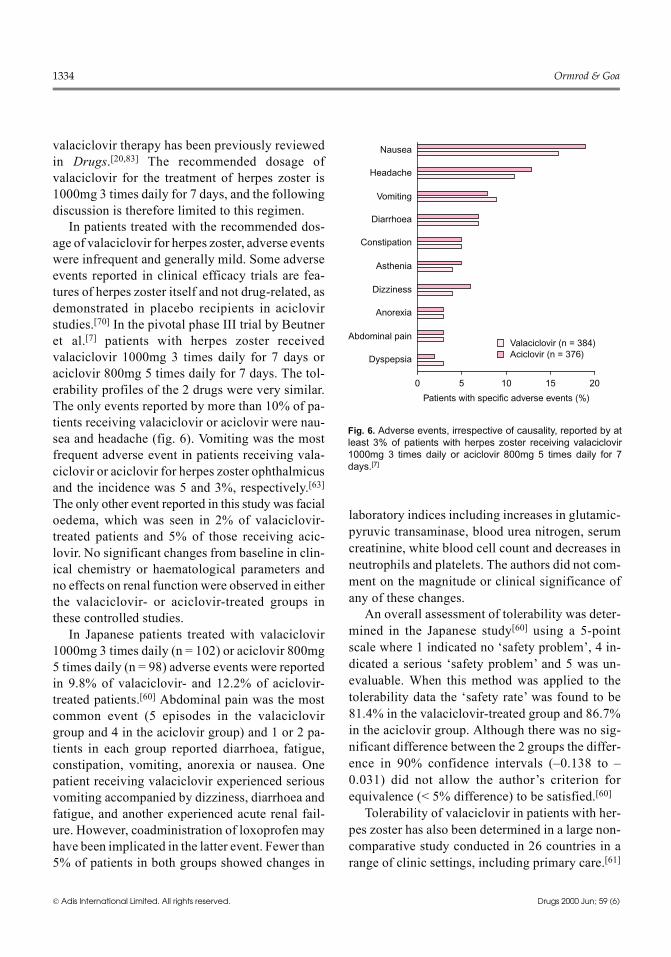
valaciclovir therapy has been previously reviewedin Drugs.[20,83] The recommended dosage ofvalaciclovir for the treatment of herpes zoster is1000mg 3 times daily for 7 days, and the followingdiscussion is therefore limited to this regimen.In patients treated with the recommended dos-
age of valaciclovir for herpes zoster, adverse eventswere infrequent and generally mild. Some adverseevents reported in clinical efficacy trials are fea-tures of herpes zoster itself and not drug-related, asdemonstrated in placebo recipients in aciclovirstudies.[70] In the pivotal phase III trial by Beutneret al.[7] patients with herpes zoster receivedvalaciclovir 1000mg 3 times daily for 7 days oraciclovir 800mg 5 times daily for 7 days. The tol-erability profiles of the 2 drugs were very similar.The only events reported by more than 10% of pa-tients receiving valaciclovir or aciclovir were nau-sea and headache (fig. 6). Vomiting was the mostfrequent adverse event in patients receiving vala-ciclovir or aciclovir for herpes zoster ophthalmicusand the incidence was 5 and 3%, respectively.[63]The only other event reported in this study was facialoedema, which was seen in 2% of valaciclovir-treated patients and 5% of those receiving acic-lovir. No significant changes from baseline in clin-ical chemistry or haematological parameters andno effects on renal function were observed in eitherthe valaciclovir- or aciclovir-treated groups inthese controlled studies.In Japanese patients treated with valaciclovir
1000mg 3 times daily (n = 102) or aciclovir 800mg5 times daily (n = 98) adverse events were reportedin 9.8% of valaciclovir- and 12.2% of aciclovir-treated patients.[60] Abdominal pain was the mostcommon event (5 episodes in the valaciclovirgroup and 4 in the aciclovir group) and 1 or 2 pa-tients in each group reported diarrhoea, fatigue,constipation, vomiting, anorexia or nausea. Onepatient receiving valaciclovir experienced seriousvomiting accompanied by dizziness, diarrhoea andfatigue, and another experienced acute renal fail-ure. However, coadministration of loxoprofen mayhave been implicated in the latter event. Fewer than5% of patients in both groups showed changes in
laboratory indices including increases in glutamic-pyruvic transaminase, blood urea nitrogen, serumcreatinine, white blood cell count and decreases inneutrophils and platelets. The authors did not com-ment on the magnitude or clinical significance ofany of these changes.An overall assessment of tolerability was deter-
mined in the Japanese study[60] using a 5-pointscale where 1 indicated no ‘safety problem’, 4 in-dicated a serious ‘safety problem’ and 5 was un-evaluable. When this method was applied to thetolerability data the ‘safety rate’ was found to be81.4% in the valaciclovir-treated group and 86.7%in the aciclovir group. Although there was no sig-nificant difference between the 2 groups the differ-ence in 90% confidence intervals (–0.138 to –0.031) did not allow the author’s criterion forequivalence (< 5% difference) to be satisfied.[60]Tolerability of valaciclovir in patients with her-
pes zoster has also been determined in a large non-comparative study conducted in 26 countries in arange of clinic settings, including primary care.[61]
Dyspepsia
Abdominal pain
Anorexia
Dizziness
Asthenia
Constipation
Diarrhoea
Vomiting
Headache
Nausea
0 5 10 15 20
Patients with specific adverse events (%)
Valaciclovir (n = 384)Aciclovir (n = 376)
Fig. 6. Adverse events, irrespective of causality, reported by atleast 3% of patients with herpes zoster receiving valaciclovir1000mg 3 times daily or aciclovir 800mg 5 times daily for 7days.[7]
1334 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

In this prospective study (n = 1897) adverse eventswere monitored during treatment and 6 months offollow-up. The overall incidence of adverse eventswas somewhat lower than that reported in the con-trolled studies in patients with herpes zoster. Head-ache was reported by 3% of patients in both the 18to 49- and ≥50-year age groups, while nausea andconstipation were slightly more common in pa-tients ≥50 years of age than in the younger group:4 versus 2% for nausea and 3 versus 1% for con-stipation. One or 2% of patients in each age groupreported asthenia, diarrhoea or abdominal pain.Adverse events were generally mild in both agegroups; however, 4 patients experienced eventsconsidered serious during or immediately aftertreatment that were possibly attributable to vala-ciclovir. There was 1 occurrence each of temporaryconfusion, reversible skin rash, vomiting, and ret-initis accompanied by dizziness.[61]The comparative tolerability profiles of vala-
ciclovir and famciclovir in patients with herpeszoster were reported in an abstract and found to besimilar, with headache and nausea being the mostcommon adverse events.[67]Valaciclovir is not generally approved for use in
immunocompromised patients for the treatment ofherpes zoster, but some physicians suggest valacic-lovir use may be appropriate in this group.[21,22]Therefore, it should be noted that thromboticmicroangiopathy (TMA)-like syndrome has beenreported in immunocompromised patients (mostlypatients with advanced HIV disease) receivinghigh doses of valaciclovir for extended periods (8g/day for at least 90 days).[21,22]
6. Dosage and Administration
The recommended oral dosage of valaciclovirfor the treatment of herpes zoster in immunocom-petent patients is 1000mg 3 times daily for 7 days.Treatment should be started promptly and ideallywithin 72 hours of onset of rash,[26,53] but recentdata suggest that treatment initiated later than 72hours may be efficacious.[61] The immediate im-pact of aciclovir from valaciclovir is to terminateVZV replication, for which the recognised surro-
gate is termination of new skin lesion formation.Therefore, treatment may be considered appropri-ate for any patient with herpes zoster presentingafter 72 hours who shows evidence of skin lesionsstill forming. The dosage of valaciclovir should bereduced in patients with moderate or severe renalimpairment. Recommended dosage reductions forvalaciclovir for patients with renal impairmentvary and local prescribing information should beconsulted.[26,53,54]Oral valaciclovir has not been prospectively
studied in the treatment of herpes zoster in im-munocompromised patients although some pa-tients with mild impairment of immunity were per-mitted in the Japanese studies of valaciclovir.Prescribing information in some countries restrictsits use to immunocompetent individuals. However,immunocompromised patients are at risk of seriousdisease following VZV infection, and cliniciansworking with immunocompromised patients havesuggested oral valaciclovir be used to treat VZVinfection in this population.[21,22] Since valacic-lovir (1000mg 3 times daily) is equivalent to intra-venous aciclovir (5 mg/kg 3 times daily) in im-munocompromised patients,[84] the use ofvalaciclovir in patients with mildly impaired im-munity may be considered.The tolerability and efficacy of oral valaciclovir
for the treatment of herpes zoster in children or inpregnant women have not been evaluated.[26,53]Therefore, use of valaciclovir for herpes zoster inthese groups is not recommended unless potentialbenefit outweighs risk.
7. Place of Valaciclovir in theManagement of Herpesvirus Infections
Herpes zoster results from VZV reactivation andthe risk of developing the disease increases withage:[85] from approximately 0.7 per 1000 individ-uals aged 20 to 30 years to 10 per 1000 individualsaged >80 years.[83] There is therefore a striking re-lationship between herpes zoster and aging, and inthe 1980s in the US the number of patients whodeveloped this infection was estimated to be 300 000to 600 000 per year.[3] Since these figures were com-
Valaciclovir in Herpes Zoster: A Review 1335
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

piled the population has aged considerably, HIVhas become endemic and drug-induced immuno-suppression (as a result of cancer therapy or anti-rejection therapy in organ transplantation) hasincreased. These factors will have combined to in-crease the prevalence of herpes zoster and The Var-icella Zoster Virus Research Foundation estimatesthe current incidence to be in excess of 850 000cases each year.[86] Between 10 and 20% of immu-nocompetent adults will experience an episode ofherpes zoster during their lifetime, and up to 2% ofthese may have a second episode.[83,85] UK figuresare very similar, and it is estimated that more than50% of individuals in the UK who reach 85 yearsof age will have experienced herpes zoster, and 1%will have had more than 1 attack.[87] The acute rashis self-limiting, but the pain that accompanies therash is the most troublesome feature and can persistfor months or even years after rash healing. In about15% of patients herpes zoster involves the eye (her-pes zoster ophthalmicus), most commonly with con-junctivitis, episcleritis, keratitis, iritis and neuralgia,both acute and chronic.[9,10] Rare complications aremotor nerve palsies, effects on the autonomic ner-vous system (urinary retention, ileus), meningio-encephalomyelitis, and disseminated zoster.[83]Disseminated zoster is rare in immunocompetentpatients but common in immunocompromised pa-tients and can be fatal in this group.[83]About 10% of all patients (all age groups) de-
velop postherpetic neuralgia after the dermal le-sions have resolved, and in about 3% of patientsthe pain persists for a year or more.[12] The inci-dence of postherpetic neuralgia increases with ageand can affect 60 to 70% of those older than 60years.[3] In 1 of the trials detailed here (section4.2.1) 79 to 85% of patients experienced pain afterrash healing.[7] Relief of this painful and debilitat-ing condition and reduction of its duration are pri-mary goals of the treatment of herpes zoster, alongwith preventing ocular complications of herpeszoster ophthalmicus. Secondary aims are to shortenthe duration of rash, prevent secondary bacterialinfection and stop virus replication.[5] The adventof antiviral drugs such as aciclovir has enabled
some of these goals to be partially attained. Newerdrugs such as valaciclovir and famciclovir have ex-tended the physician’s ability to effectively treatherpes zoster.[38,88]Once established, postherpetic neuralgia is no-
toriously difficult to treat and conventional analge-sics are generally ineffective.[89] In patients withherpes zoster and mild pain who are <50 years ofage symptomatic care is usually recommended.Those with severe pain, herpes zoster ophthalmi-cus or who are ≥50 years of age should be treatedwith oral antiviral therapy for 7 days.[90-92] Allmildly immunocompromised patients are alsotreated with oral antiviral drugs, while the moreseriously immunocompromised patients generallyreceive intravenous aciclovir.[21,22,90]As discussed in section 1, aciclovir has been
widely used for the treatment of herpes zoster andeffectively reduces the pain and duration of rash inthe acute phase of the disease. However, it is lesseffective in the prevention of postherpetic neural-gia, most likely as a result of low oral bioavailabil-ity. Valaciclovir was developed to overcome thislimitation and is at least equivalent to, and better incertain parameters than, aciclovir in the manage-ment of herpesvirus diseases.[19,20,25] In herpes zos-ter, valaciclovir 1000mg 3 times daily for 7 dayshas been shown to be as effective as aciclovir800mg 5 times daily for 7 days for the treatment ofthe symptoms of acute zoster and more effective inthe resolution of zoster-associated pain, a measurethat includes the pain experienced during the acutestage and postherpetic neuralgia (section 4.2.1).[7]A smaller trial in Japanese patients confirmed thesimilarity of valaciclovir and aciclovir for the treat-ment of acute herpes zoster, but did not formallyassess postherpetic neuralgia.[60] Valaciclovir andaciclovir have also demonstrated comparable effi-cacy for the treatment of herpes zoster ophthalmi-cus.[63]Valaciclovir has been approved for use in herpes
zoster since the mid 1990s in more than 50 coun-tries and clinical researchers have gathered pro-spective data from patients treated with valacic-lovir in a range of settings including primary care.
1336 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

In the largest of these trials, 1897 patients treatedwith valaciclovir 1000mg daily for 7 days weremonitored for 24 weeks.[61] The key findings ofthis study were that pain resolved almost twice asrapidly in patients aged <50 years of age than inthose ≥50 years, and the intensity of prodromalpain or the presence of pre-existing neurologicaldisorders predicted more prolonged postherpeticneuralgia. Interestingly, the duration of zoster-associated pain in those patients whose treatmentwas initiated before 72 hours after rash onset wasnot statistically different from that experienced bypatients who started treatment more than 72 hoursafter rash onset. However, further analysis of thesedata is required to rule out bias which may havearisen because older patients with more severesymptoms might have started therapy earlier. Aretrospective analysis[63] of the pivotal study byBeutner et al.[7] revealed that starting therapy early(within 48 hours of rash onset compared with 48to 72 hours) did not affect outcome in terms ofresolution of pain. However, the current recom-mendation is that valaciclovir therapy should bestarted within 72 hours of the appearance of symp-toms of herpes zoster and this should still be theaim.[22,72-74]Famciclovir, an antiviral drug with a qualita-
tively similar mode of action to valaciclovir, hasalso shown efficacy in the management of herpeszoster.[8,93] Like valaciclovir, famciclovir is a pro-drug which improves the bioavailablity of the ac-tive antiviral compound, in this case penciclovir.In a comparative study famciclovir appeared to beas effective as aciclovir in herpes zoster.[94] Thereis a similar potential compliance advantage forvalaciclovir and famciclovir, as they are both ef-fective taken 3 times daily compared with 5 timesdaily for aciclovir. Preliminary results (reported asan abstract) of a double-blind study indicate com-parable efficacy of valaciclovir (1000mg 3 timesdaily) and famciclovir (500mg 3 times daily) inaccelerating skin healing in herpes zoster andspeeding resolution of pain, including postherpeticneuralgia.[67]
At the dosage recommended for the treatmentof herpes zoster (1000mg 3 times daily for 7 days)valaciclovir was well tolerated with an adverseevent profile similar to that of aciclovir and fam-ciclovir.[7,25,60,67,93] Headache and events relatingto the gastrointestinal tract were most commonlyreported and were generally mild. In Japanese pa-tients the ‘safety rate’ was reported as 81.4 and86.7% for valaciclovir and aciclovir, respectively.In a noncomparative trial carried out in differentinternational clinical settings the tolerability ofvalaciclovir was also good,[61] and the overall in-cidence of adverse events was somewhat lowerthan that reported in the controlled clinical trials.Herpes zoster can have a significant effect on
QOL,[7] but as yet there is only limited evidencethat valaciclovir can improve QOL in herpes zos-ter.[7] Further studies evaluating the effects ofvalaciclovir on QOL in patients with herpes zosterare required. Herpes zoster occurs frequently inimmunocompromised patients[38] and prospectivestudies of valaciclovir in this group are alsoneeded.In conclusion, the earlier data which demon-
strated the efficacy of valaciclovir for the treatmentof herpes zoster have been confirmed and extendedby follow-up studies in herpes zoster ophthalmi-cus, in Japanese patients and in a wider range ofclinical settings including primary care. The differ-ences between the therapeutic benefits of vala-ciclovir and aciclovir are modest but significant; inparticular valaciclovir leads to a faster resolutionof zoster-associated pain, which includes posther-petic neuralgia. In addition, there is a potentialcompliance advantage engendered by the 3 timesdaily regimen for valaciclovir compared with the5 times daily administration schedule for oralaciclovir; this may be particularly important in el-derly patients, who constitute the largest group ofindividuals with herpes zoster and may find it dif-ficult to follow the latter regimen. Therefore, vala-ciclovir is a well tolerated first-line therapy withan established place in the treatment of immuno-competent patients with herpes zoster.
Valaciclovir in Herpes Zoster: A Review 1337
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
References1. McCrary ML, Severson J, Tyring SK. Varicella zoster virus. J
Am Acad Dermatol 1999 Jul; 41: 1-142. Lee BW. Review of varicella zoster seroepidemiology in India
and Southeast Asia. TropMed Int Health 1998; 3 (11): 886-903. Schmader K. Management of herpes zoster in elderly patients.
Infect Dis Clin Pract 1995; 4 (4): 293-94. Gilden DH, Vafai A, ShtramY, et al. Varicella-zoster virus DNA
in human sensory ganglia. Nature 1983; 306: 478-805. Nikkels AF, Piérard GE. Recognition and treatment of shingles.
Drugs 1994 Oct; 48: 528-486. Rogers RS, Tindall JP. Herpes zoster in the elderly. Postgrad
Med 1971 Dec; 50 (6): 153-77. Beutner KR, Friedman DJ, Forszpaniak C, et al. Valaciclovir
compared with acyclovir for improved therapy for herpes zos-ter in immunocompetent adults. Antimicrob Agents Chemo-ther 1995 Jul; 39: 1546-53
8. Dworkin RH, Boon RJ, Griffin DRG, et al. Postherpetic neural-gia: impact of famciclovir, age, rash severity, and acute painin herpes zoster patients. J Infect Dis 1998; 178 Suppl. 1:S76-80
9. Liesegang TJ. Corneal complications from herpes zoster op-hthalmicus. Ophthalmology 1985; 92 (3): 316-24
10. Liesegang TJ. Varicella-zoster virus eye disease. Cornea 1999;18 (5): 511-31
11. Johnson RW. Herpes zoster and postherpetic neuralgia: optimaltreatment. Drugs Aging 1997 Feb; 10: 80-94
12. Hanania MM, Brietstein D. Postherpetic neuralgia: a review.Cancer Invest 1997; 15 (2): 165-76
13. Bean B, Braun C, Balfour Jr HH. Acyclovir for acute herpeszoster. Lancet 1982; 2: 118-21
14. van den Broek PJ, van derMeer JWM,Mulder JD, et al. Limitedvalue of acyclovir in the treatment of uncomplicated herpeszoster: a placebo-controlled study. Infection 1984; 12: 338-41
15. Crooks RJ, Jones DA, Fiddian AP. Zoster-associated chronicpain: an overview of clinical trials with acyclovir. Scand JInfect Dis 1991 Suppl. 78: 62-88
16. Wood MJ, Kay R, Dworkin RH, et al. Oral acyclovir therapyaccelerates pain resolution in patients with herpes zoster: ameta-anamysis of placebo-controlled trials. Clin Infect Dis1996; 22: 341-7
17. Jackson JL, Gibbons R, Meyer G, et al. The effect of treatingherpes zoster with oral acyclovir in preventing postherpeticneuralgia - a meta-analysis. Arch Intern Med 1997 Apr 28;157: 909-12
18. Looke DFM. Revisiting herpes zoster – updating management.Mod Med Aust 1999; 42 (4): 67-78
19. Perry CM, Faulds D. Valaciclovir: a review of its antiviral ac-tivity, pharmacokinetic properties and therapeutic efficacy inherpesvirus infections. Drugs 1996 Nov; 52: 754-72
20. Ormrod DJ, Scott LJ, Perry CM. Valaciclovir: a review of itslong term utility in the management of genital herpes simplexvirus and cytomegalovirus infections. Drugs 2000; 59 (4):839-63
21. Griffiths P. Update on herpesvirus infections. J R Coll Physi-cians Lond 1998; 32 (3): 199-202
22. Cohen JI, Brunell PA, Straus SE, et al. Recent advances in var-icella-zoster virus infection. Ann Intern Med 1999; 130 (11):922-32
23. Beutner KR. Valacyclovir: a review of its antiviral activity,pharmacokinetic properties, and clinical efficacy. AntiviralRes 1995; 28 (4): 281-90
24. Wagstaff AJ, Faulds D, Goa KL. Aciclovir: a reappraisal of itsantiviral activity, pharmacokinetic properties and therapeuticefficacy. Drugs 1994; 47 (1): 153-205
25. Patel R. Valaciclovir: development, clinical utility and poten-tial. Expert Opin Invest Drugs 1997; 6 (2): 173-89
26. Glaxo Wellcome. Valtrex (valacyclovir hydrochloride) caplets.Product information. 1999, Research Triangle Park (NC)
27. Takahashi K, Suzuki M, Iwata Y, et al. Selective activity ofvarious nucleoside and nucleotide analogues against humanherpesvirus 6 and 7. Antiviral Chem Chemother 1997; 8 (1):24-31
28. Kedes DH, Ganem D. Sensitivity of Kaposi’s sarcoma-associatedherpesvirus replication to antiviral drugs: implications for po-tential therapy. J Clin Invest 1997; 99 (9): 2082-6
29. MedveczkyMM,Horvath E, LundT, et al. In vitro antiviral drugsensitivity of the Kaposi’s sarcoma-associated herpesvirus.AIDS 1997; 11: 1327-32
30. Neyts J, de Clercq E. Antiviral drug susceptibility of humanherpesvirus 8. Antimicrob Agents Chemother 1997; 41 (12):2754-6
31. Ertl P, Snowden W, Lowe D, et al. A comparative study of thein vitro and in vivo antiviral activities of acyclovir and pen-ciclovir. Antiviral Chem Chemother 1995; 6 (2): 89-97
32. Champness JN, Bennett MS, Wein F, et al. Exploring the activesite of herpes simplex virus type-1 thymidine kinase by X-raycrystallography of complexes with aciclovir and other lig-ands. Proteins 1998; 32 (3): 350-61
33. Reusser P. Herpesvirus resistance to antiviral drugs: a review ofthe mechanisms, clinical importance and therapeutic options.J Hosp Infect 1996 Aug; 33: 235-48
34. Boivin G, Edelman K, Pedneault L, et al. Phenotypic and geno-typic characterization of acyclovir-resistant varicella-zostervirus isolates from persons with AIDS. J Infect Dis 1994; 170:68-95
35. Morfin F, Thouvenot D, de Tourenne-Tessier M, et al. Pheno-typic and genetic characterization of thymidine kinase fromclinical strains of varicella-zoster virus resistant to acyclovir.Antimicrob Agents Chemother 1999; 43 (10): 2412-6
36. Reusser P, Cordonnier C, Einsele H, et al. European survey ofherpesvirus resistance to antiviral drugs in bonemarrow trans-plant recipients. Bone Marrow Transplant 1996; 17: 813-7
37. Ida M, Kageyama S, Sato H, et al. Emergence of resistance toacyclovir and penciclovir in varicella-zoster virus and geneticanalysis of acyclovir-resistant variants. Antiviral Res 1999;40: 155-66
38. Snoeck R, Andrei G, De Clercq E. Current pharmacologicalapproaches to the therapy of varicella zoster virus infections:a guide to treatment. Drugs 1999 Feb; 57: 187-206
39. Wetherall NT, Hodges-Savola CA, Reyes M, et al. Acyclovir-resistant herpes simplex virus: characterization of virus iso-lates from a nationwide surveillance system [abstract no. 17].Antiviral Res 1998; 37 (3): A44
40. Soul-Lawton J, Weller S, On N, et al. Oral valaciclovir - in-creased acyclovir bioavailability in different patient popula-tions [abstract no. P59]. AIDS 1994 Nov; 8 Suppl. 4: S33
41. Azuma J, Yamamoto I, Aoki T, et al. A phase I study of a newantiviral drug, valaciclovir hydrochloride (256U87), in healthymale volunteers [in Japanese]. Rinsho Iyaku 1998; 14 (15):2683-700
42. Weller S, BlumMR, Doucette M, et al. Pharmacokinetics of theacyclovir pro-drug valaciclovir after escalating single- andmultiple-dose administration to normal volunteers. Clin Phar-macol Ther 1993 Dec; 54: 595-605
1338 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)
43. Soul-Lawton J, Seaber E, On N, et al. Absolute bioavailabilityand metabolic disposition of valaciclovir, the l-valyl ester ofacyclovir, following oral administration to humans. Anti-microb Agents Chemother 1995 Dec; 39: 2759-64
44. de Miranda P, Blum MR. Pharmacokinetics of acyclovir afterintravenous and oral administration. J Antimicrob Chemother1983; 12 Suppl. B: 29-37
45. Crooks RJ. Valaciclovir - a review of its potential in the man-agement of genital herpes. Antiviral Chem Chemother 1995;6 Suppl. 1: 39-44
46. First MR, BlumMR, Brennan P, et al. Pharmacokinetics (PK)of 256U87, an acyclovir (ACV) prodrug in renal transplant(RTX) patients [abstract]. Clin Pharmacol Ther 1993 Feb;53: 238
47. Wang LH, Schultz M, Weller S, et al. Pharmacokinetics andsafety of multiple-dose valaciclovir in geriatric volunteerswith and without concomitant diuretic therapy. AntimicrobAgents Chemother 1996 Jan; 40: 80-5
48. Jacobson MA, Gallant J, Wang LH, et al. Phase I trial ofvalaciclovir, the l-valyl ester of acyclovir, in patients withadvanced human immunodeficiency virus disease. Anti-microb Agents Chemother 1994 Jul; 38: 1534-40
49. Conant MA, Murphy R, Thompson S, et al. Valaciclovir for themanagement of recurrent herpes simplex virus infection inHIV-infected individuals - two double-blind controlled trials.London: Glaxo Wellcome, 1999 (Data on file)
50. On NT, Ehninger G, Gluckman E, et al. Acyclovir pharmaco-kinetics following oral multiple-dose of valaciclovir (Valtrex)in allogeneic BMT patients [abstract]. Bone Marrow Trans-plant 1995 Mar; 15 Suppl. 2: S122
51. Burnette TC, Harrington JA, Reardon JE, et al. Purification andcharacterization of a rat liver enzyme that hydrolyzesvalaciclovir, the l-valyl ester prodrug of acyclovir. J BiolChem 1995; 270 (26): 15827-31
52. De Bony F, Bidault R, Tod M, et al. Interaction of cimetidine andprobenecid with valaciclovir and its metabolite acyclovir [ab-stract]. 36th ICAAC 1996 Sep: New Orleans, LA 15: 6
53. Glaxo Wellcome. Valtrex. Summary of product characteristics.Greenford: Glaxo Wellcome, 1999
54. Glaxo Wellcome K.K. Antiviral chemotherapeutic agent.Valtrex Tablets 500. Tokyo: Glaxo Wellcome, 2000
55. SmileyML, The International Valaciclovir Zoster StudyGroup.The efficacy and safety of valaciclovir for the treatment ofherpes zoster. 33rd International Conference on Antimicro-bial Agents andChemotherapy. 1993Oct 17-20;NewOrleans(LA), 340
56. Johnson RW, Crooks RJ, International Valaciclovir ZosterStudy Group. The clinical efficacy of valaciclovir in the treat-ment of herpes zoster [abstract]. J Eur AcadDermatol Venerol1995 Oct; 5 Suppl. 1: S75
57. NiimuraM, HondaM, KawashimaM, et al. Early phase II studyof valaciclovir hydrochloride tablet in patients with herpeszoster [in Japanese]. Rinsho Iyaku 1998; 14 (15): 2701-15
58. Niimura M, Honda M, Nishikawa T, et al. Late phase II studyof valaciclovir hydrochloride tablet in patients with herpeszoster: optimal dose finding by double-blind comparativestudy [in Japanese]. Rinsho Iyaku 1998; 14 (16): 2833-66
59. Tagami H, Okuyama R, Funayama M, et al. Clinical efficacyof valaciclovir hydrochloride tablet in patients with herpeszoster: open study [in Japanese]. Rinsho Iyaku 1998; 14 (16):2903-20
60. Niimura M, Honda M, Nishikawa T, et al. Phase III study ofvalaciclovir hydrochloride tablets in patients with herpes zos-
ter: double-blind comparative study with aciclovir tablets [inJapanese]. Rinsho Iyaku 1998; 14 (16): 2867-902
61. Decroix J, Partsch H, Gonzalez R, et al. Factors influencingpain outcomes in herpes zoster - an observational study withvalaciclovir. J EurAcadDermatolVenerol 2000; 14 (1): 23-33
62. Severson J, Tyring S, Evans T, et al. Efficacy and safety of oralvalacyclovir (VACV) 1.5MG [1.5g in text] BID in the treat-ment of acute herpes zoster [abstract]. 57th Annual Meetingof the Americal Acadamy of Dermatology; 1999 Mar 19-24;New Orleans (LA), 36
63. Colin J, Prisant O, Cochener B, et al. A double-blind random-ized trial to compare the efficacy and safety of valaciclovirand aciclovir for the treatment of herpes zoster ophthalmicus.Ophthalmology. In press
64. Grant DM, Mauskopf JA, Bell L, et al. Comparison ofvalaciclovir and acyclovir for the treatment of herpes zosterin immunocompetent patients over 50 years of age: a cost-consequence model. Pharmacotherapy 1997 Mar-Apr; 17:333-41
65. Whitley RJ, Shukla S, Crooks RJ, et al. The identification ofrisk factors associated with persistent pain following herpeszoster. J Infect Dis 1998; 178 Suppl. 1: S71-5
66. WoodMJ, Shukla S, FiddianAP, et al. Treatment of acute herpeszoster: effect of early (<48 h) versus late (48-72 h) therapywith acyclovir and valaciclovir on prolonged pain. J InfectDis 1998 Nov; 178 Suppl. 1: S81-4
67. Van der Straten M, Carrasco D, Lee P, et al. Comparison ofvalacyclovir and famciclovir for treatment of acute herpeszoster [abstract no. 374]. Poster Book, American Academy ofDermatology, 58th Annual Meeting: 2000 Mar 10-15, SanFrancisco (CA)
68. Wood MJ, Herpes Zoster CTCG. How should zoster trials beconducted? J Antimicrob Chemother 1995Dec; 36: 1089-101
69. Dworkin RH, Carrington D, Cunningham A, et al. Assessmentof pain in herpes zoster: lessons learned from antiviral trials.Antiviral Res 1997; 33: 73-85
70. Wood MJ, Ogan PH, McKendrick MW, et al. Efficacy of oralacyclovir in the treatment of herpes zoster. Am J Med 1988;85 Suppl. 2A: 79-83
71. Mahalingam R, Wellish M, Wolf W, et al. Latent varicella-zos-ter viral DNA in human trigeminal and thoracic ganglia. NEngl J Med 1990; 323 (10): 627-31
72. Cobo LM, Foulks GN, Liesegang T, et al. Oral acyclovir in thetreatment of acute herpes zoster ophthalmicus. Ophthalmol-ogy 1996; 93 (6): 763-70
73. Hoang-Xuan T, Büchi ER, Herbort CP, et al. Oral acyclovir forherpes zoster ophthalmicus. Ophthalmology 1992; 99 (7):1062-71
74. Harding SP, Porter SM. Oral acyclovir in herpes zoster op-hthalmicus. Curr Eye Res 1991; 10 Supp.: 177-82
75. Choo PW, Galil K, Donahue JG, et al. Risk factors for post-herpetic neuralgia. Arch InternMed 1997 Jun 9; 157: 1217-24
76. Meister W, Neiβ A, Gross G, et al. A prognostic score for post-herpetic neuralgia in ambulatory patients. Infection 1998; 26(6): 359-63
77. Grose C, Wiedeman J. Generic acyclovir vs. famciclovir andvalacyclovir. Pediatr Infect Dis J 1997; 16 (9): 838-41
78. Tilson HH, Engle CR, Andrews EB. Safety of acyclovir: a sum-mary of the first 10 years experience. J Med Virol 1993; 41Suppl. 1: 67-73
79. Bodsworth NJ, Crooks RJ, Borelli S, et al. Valaciclovir versusaciclovir in patient initiated treatment of recurrent genital her-pes: a randomised, double blind clinical trial. GenitourinMed1997; 73: 110-6
Valaciclovir in Herpes Zoster: A Review 1339
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)

80. Spruance SL, Tyring SK, DeGregorio B, et al. A large-scaleplacebo-controlled, dose-ranging trial of peroral valaciclovirfor episodic treatment of recurrent herpes genitalis. Arch In-tern Med 1996 12/26 Aug; 156: 1729-35
81. Tyring SK, Douglas Jr JM, Corey L, et al. Arandomized, placebo-controlled comparison of oral valacyclovir and acyclovir inimmunocompetent patients with recurrent genital herpes in-fections. Arch Dermatol 1998 Feb; 134: 185-91
82. Fife KH, Barbarash RA, Rudolph T, et al. Valaciclovir versusacyclovir in the treatment of first-episode genital herpes in-fection: results of an international, multicenter, double-blind,randomized clinical trial. Sex TransmDis 1997 Sep; 24: 481-6
83. Conlon CP. Herpes zoster. Prescr J 1995; 35 (2): 46-5284. HöglundM, Ljungman P, Larsson R, et al. Comparable aciclovir
exposures produced by oral valaciclovir and intravenousaciclovir in immunocompromised cancer patients [abstractno. P7]. J Antimicrob Chemother 1999; 44 Suppl. A: 42
85. Donahue JG, Choo PW, Manson JE, et al. The incidence ofherpes zoster. Arch Intern Med 1995 7/12 Aug; 155: 1605-9
86. VZV Research Foundation. The Varicella-Zoster Virus & VZVInfections. Available from: http://www.vzvfoundation.org/templates/VaricellaZosterVirus.cfm [Accessed 2 May 2000]
87. Wood MJ. Herpes zoster in immunocompetent patients. ResClin Forum 1986; 8 (6): 61-8
88. Stein GE. Pharmacology of new antiherpes agents: famciclovirand valacyclovir. Both of these prodrugs produce higherplasma concentrations of active antiviral agent than is ob-served with oral acyclovir. J Am Pharm Assoc 1997; 37 (2):157-63
89. Hong W, Cousins M. Postherpetic neuralgia: is it preventableand treatable? Mod Med Aust 1996; 39 (3): 84-7
90. Johnson R, Mandal B, Bowsher D, et al. Guidelines for themanagement of shingles: report of a Working Group of theBritish Society for the Study of Infection. J Infect 1995; 30:193-200
91. Wood MJ, Kroon S, editors. Management strategies in herpes:reducing the burden of zoster-associated pain – update. 2nded. Worthing: PPS Europe, 1997
92. Wood MJ, Kroon S, on behalf of the International Herpes Man-agement Forum. Reducing the burden of zoster-associatedpain – update. Available from: URL: http://www.ihmf.com/li-brary/libpost.asp [Accessed 20 May 2000]
93. Tyring S, Barbarash RA, Nahlik JE, et al. Famciclovir for thetreatment of acute herpes zoster: effects on acute disease andpostherpetic neuralgia: a randomised, double blind placebo-controlled trial. Ann Intern Med 1995; 123: 89-96
94. Degreef H, Famciclovir Herpes Zoster Clinical Study Group.Famiciclovir, a new oral antiherpes drug: results of the firstcontrolled clinical study demonstrating its efficacy and safetyin the treatment of uncomplicated herpes zoster in immuno-competent patients. Int J Antimicrob Agents 1994; 4: 241-6
Correspondence: Douglas Ormrod, Adis International Lim-ited, 41 Centorion Drive, Private Bag 65901, Mairangi Bay,Auckland 10, New Zealand. E-mail: [email protected]
1340 Ormrod & Goa
© Adis International Limited. All rights reserved. Drugs 2000 Jun; 59 (6)