Embed Size (px)
Citation preview

Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.
Validation and adaptation of the Norwegian version of Hayes Ability Screening Index for intellectual diffi culties in a psychiatric sample
ERIK S Ø NDENAA , Ø YVIND NYG Å RD , JIM AAGE N Ø TTESTAD , OLAV MARTIN LINAKERS ø ndenaa E, Nyg å rd Ø , N ø ttestad JA, Linaker OM. Validation and adaptation of the Norwegian version of Hayes Ability Screening Index for intellectual diffi culties in a psychiatric sample. Nord J Psychiatry 2011;65:47–51.
© 2011 Informa H
Background: Intellectual disabilities (ID) among psychiatric patients have traditionally been neglected. A lack of convenient instruments and competency in ID may have worsened the conditions and treatment availability for these patients. Aims: Validation and adaptation of a screening instrument for ID (Hayes Ability Screening Index; HASI) in a psychiatric hospital setting. Methods: This is a cross-sectional study of 50 psychiatric patients in two Norwegian psychiatric hospitals comparing results of the HASI with the Wechsler Abbreviated Scale of Intelligence (WASI). Results: The HASI correlated well with the standard IQ test used ( r � 0.67, P � 0.001). At a stated cut-off score of 85, the HASI had a sensitivity of 100% and specifi city of 34%. Conclusions: The HASI is a valid and time-saving screening instrument for ID among psychiatric patients. The prescribed cut-off score, however, resulted in a large number of false positives.
• Intellectual disabilities, Psychiatric patients, Screening instrument.
Erik S ø ndenaa, Forensic Department Br ø set, Center for Research and Education in Forensic Psychiatry, P.O. 1803 Lade, 7440 Trondheim, Norway, E-mail: [email protected]; Accepted 14 April 2010.
International studies often discriminate between the
“administrative” and the “true” prevalence of intellec-
tual disability (ID) (1). Administrative prevalence usually
includes only people with the most severe disabilities
who are known because they receive services from the
administrations in the municipalities (2). The true preva-
lence also counts people having intellectual problems,
but without the need for health and care services adapted
for people with ID. A number of studies cited in
Roeleveld et al. (1), demonstrate a higher prevalence of
“true” ID compared with “administrative” ID. The
“administrative” prevalence was found between 0.23%
and 0.47% (3). The Norwegian administrative prevalence
is 0.45% (4). In contrast, Roeleveld et al. (1) found an
average “true” prevalence of ID in school children of
3%. The true prevalence in the Nordic countries is
slightly lower (5) as a consequence of the social and
welfare system, estimated at 1–2% of the population.
Hence, many people with ID are probably unknown to
the social and health authorities as well as to themselves,
and they may have undiscovered needs for services or
service adjustments.
ealthcare
There is an increased prevalence of psychiatric disor-
ders among people with ID. Several studies confi rm this
association: Richards et al. (6) found that depression,
anxiety and adjustment disorders are more prevalent
among people with ID than in the general population.
Greenwood et al. (7) noted a family association between
ID and schizophrenia. Among people with ID, the pooled
results of studies suggest rates of between 2% and 6%
for schizophrenia (7). These prevalence rates are about
four times higher than in the general population. Corbett
(8) found a 25% rate of personality disorders in a large
community sample of 402 persons with ID. People with
mild ID among psychiatric patients may not be identifi ed
and thus not treated in appropriately in the context of
their cognitive limitations (9).
No validated screening instruments for intellectual
capacity are available in Norwegian. The validated instru-
ments are time consuming, designed to be administered
by examiners who have psychological or psychometric
training, and in many cases designed to search for spe-
cifi c symptoms. For example, administration time for the
Kaufmann Brief Intelligence Test (K-BIT; 10) is 15–30
DOI: 10.3109/08039488.2010.486444

E S Ø NDENAA ET AL.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.
min (11, 12). The Mini Mental State Examination
(MMSE) is commonly used to estimate the severity of
cognitive impairment in dementia (13). The administra-
tion time for the Wechsler Abbreviated Scale of Intelli-
gence (WASI; 14) is roughly half an hour and the test
may be too time consuming to be used as a screening
tool. The Wechsler Adult Intelligence Scale (WAIS-III;
15) is even more time consuming.
The Hayes Ability Screening Index (HASI) was devel-
oped by Susan Hayes (16) to serve as a valid and user-
friendly instrument to screen for ID within the criminal
justice system. People with reduced intellectual abilities
are overrepresented among habitual criminals (17), peo-
ple with mental disorders (18) and people with general
social problems (19). The HASI can be administered
quickly. Each subtest has a raw score, which is scaled
differently, summarized and added to the constant score
of 26. The whole battery, including administration and
scoring, is intended to be completed within 10–15 min.
This study aimed to validate the HASI with the WASI
used as the criterion for validity. Findings from a previ-
ous study using these two instruments in a prison sample
(20), suggested that in this context the number of false
positives could be reduced if the HASI cut-off score were
set at a lower level. Changing the cut-off score would,
however, raise copyright concerns. A study of the concor-
dance between the two instruments among psychiatric
patients could give the HASI legitimacy as a screening
instrument in this population.
Method Sample In total, 50 participants in two psychiatric hospitals in
the Norwegian county of S ø r-Tr ø ndelag were included in
the study. All were inpatients. There were 24 male and
26 female participants; 96% were ethnic Norwegians. The
participants’ ages ranged from 18 to 72 years (mean � 41.9;
standard deviation, s � 13.6). Two of the participants did
not complete the WASI, and were therefore withdrawn
from the analysis.
Instruments The HASI asks participants to self-evaluate whether they
think they may have a learning disability or be a “slow
learner”, collects some facts about spelling and the alpha-
bet, immediate verbal attention, divided attention, visuo-
spatial and constructional knowledge, and knowledge
about important issues of everyday living. The HASI has
been shown to correlate signifi cantly with the K-BIT
( r � 0.627) (10) and the Vineland Adaptive Behavior
Scales ( r � 0.497) (21, 22).
The HASI consists of four subtests: Background Infor-
mation, Backwards Spelling, Puzzle (adaptation of the
Trail-Making Test B) and Clock Drawing. The background
48
information subtest consists of four questions that are
sensitive to school diffi culties, the subject’s self-aware-
ness concerning their learning diffi culties, and the sub-
ject’s economic and social status. This subtest is based
on self-report. The task in Backwards spelling is to spell
a fi ve-letter word backwards. The original word in the
English edition (16) was “WORLD”. In the Norwegian
edition, the word “NORGE” (NORWAY) is used. Back-
ward spelling is a well-known test from many screening
batteries, including the Mini Mental State Examination
(MMSE). This task requires the ability to mentally rotate
words and pay attention. Clearly, some degree of liter-
acy in the Norwegian language is essential for this sub-
test. In the subtest “Puzzle”, the examinee draws lines
between a pattern of numbers and letters. This is an
adaptation of a well-known neuropsychological test best
known as the Trail Making Test (23). A variant of the
B-part of this test is used in the HASI, and is intended
to assess visual–conceptual and visual–motor tracking.
The test is based on the ability to maintain divided
attention, and is sensitive to effects of brain injury (24).
The last subtest in the HASI is the Clock Drawing test
(25). This test is often used as a part of a neurological
screening procedure, and demands visual–spatial and
constructional abilities. It is also sensitive to dementia.
The subject is asked to draw a large clock face, and to
put the hands of the clock at 3:40. The Clock Drawing
test correlates with other tests of non-verbal visuo-con-
struction such as the Rey–Osterrieth test (26) and the
Block Design test in the WAIS (27), and only marginally
with a verbal factor (27). A study by Ishiai et al. (28)
showed that clock drawings correlated highly (Spearman’s
rank correlation r s � 0.745, P � 0.01) with the verbal
Wechsler IQ test.
The WASI (14) was used as a criterion of validity in
this study. The WASI consists of two verbal tests
(“Vocabulary” and “Similarities”) and two performance
tests (“Block Design” and “Matrix Reasoning”). A Nor-
wegian translation (29) was used, but with US norms. A
study of the psychometric properties of the Norwegian
WASI translation found that mean T -scores and IQ
results, as well as intercorrelations of subtests and IQ
values, closely resemble results published with regard to
the US population (30). The WASI subtests correlated
signifi cantly with the WAIS subtests ( r � 0.85–0.93,
P � 0.001) in a Norwegian sample (31).
The HASI cut-off score for people aged 13–18 years
is set at 90 and for those aged over 18 at 85 (16). In
contrast with the WASI, the scores are not age-adjusted
in the HASI. Subjects with scores below the cut-off
score should be referred for further assessment. The
HASI does not report an IQ score, but a score that indi-
cates whether a person should be referred for further
assessment. The scores of the HASI cover the range
from 48.7 to 96.4 (16).
NORD J PSYCHIATRY·VOL 65·NO 1·2011

INTELLECTUAL DIFFICULTIES IN PSYCHIATRIC PATIENTS
125,00100,0075,0050,00
WASI-IQ score
12
10
8
6
4
2
0
Fre
qu
en
cy
100,0095,0090,0085,0080,0075,0070,0065,0060,0055,00
HASI
130,00
120,00
110,00
100,00
90,00
80,00
70,00
60,00
50,00
WA
SI
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.
The Norwegian translation of the HASI included the
complete version (16). The translation was done by one
of the authors of this article. A preliminary trial was
conducted to detect problems in the structure of the
instrument, translation errors, diffi culties in understand-
ing, terms and expressions, which could cause cultural,
linguistic or ethical confl icts (32, 33). The fi nal Norwe-
gian version was retranslated into English by a profes-
sional translator and endorsed by the original author,
Susan Hayes, according to internationally accepted rules
for cross-cultural translation procedures (34).
Procedure Data collection took place during August 2007–April
2008. The data were collected by one psychologist and
one medical student. The psychologist administered the
WASI and the medical student administered the HASI.
All participants were tested with both the HASI and the
WASI. The instruments were administered in random
order. The participants were tested in a hospital setting.
After collection, all data were anonymized. Each sub-
ject gave written informed consent to participate. The
study was approved by the Regional Ethical Committee
for Medical Research.
Data analysis The data were analyzed using the SPSS software program,
version 14.0.
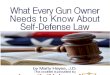
Results The average IQ in the sample as measured by WASI was
91.0 ( s � 18.3), with a minimum of 56 and maximum of
127. The distribution of the WASI IQ scores showed four
(8.3%) participants below 70, 12 (25%) between 70 and
80, 27 (56.3%) between 80 and 120, and fi ve (10.4%)
above 120 (Fig. 1). For male participants ( n � 23) the
average IQ score was 91.1 ( s � 19.0) and for the female
participants ( n � 25) it was 90.8 ( s � 17.9).
The average HASI score was 79.1 ( s � 8.1), with a
minimum of 59.3 and maximum of 96.4. The average
HASI scores for the male participants ( n � 24) was 78.2
( s � 8.1) and for the female participants ( n � 26) it was
79.9 ( s � 8.2).
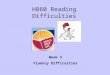
The Pearson two-tailed correlation coeffi cient between
the WASI and the HASI scores was signifi cant ( r � 0.67,
P � 0.001). The correlation between the scales increased
( r � 0.71) when the subtest “Background information”
was eliminated from the HASI.
The HASI and the WASI scores were plotted together.
Figure 2 illustrates the distribution of the scores.
The internal consistency of the HASI was equivalent
to a coeffi cient of α � 0.67. The correlations between the
HASI subtests and the WASI were as follows: Backward
NORD J PSYCHIATRY·VOL 65·NO 1·2011
spelling 0.48, Puzzle 0.44 and Clock drawing 0.60. For
Background information, the correlation was 0.08. For
all the subtests except the “Background information”, the
correlations were signifi cant.
The HASI is meant to be over-inclusive, and at the
cut-off of 85 the sensitivity is 100% (95% CI 64.6–100%)
and the specifi city is 35.4% (95% CI 23.0–50.8%). Con-
fi dence intervals for proportions were calculated using
the Wilson (score) method. This methods performs well
even with small counts as we have (35). Sensitivity is
the proportion, or percentage, of those tested with the
condition (IQ � 70) that the test (HASI) correctly identifi es
as having it. Specifi city is the proportion, or percentage,
Fig. 1 . Distribution of the Standard scores of the WASI ( n � 48).
Fig. 2. Scatter-plot and cut-off for HASI (vertical) and cut-off for
WASI (horizontal).
49

E S Ø NDENAA ET AL.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.
of those tested without the condition that the screening
test correctly identifi es as not having it.
Discussion This study attempted to ascertain whether the HASI could
serve as a useful and time-saving tool in a psychiatric
setting. An important purpose for a screening tool such
as the HASI is to reduce the number of individuals
referred unnecessarily for time-intensive, costly individual
assessments. In the copyrighted HASI, the cut-off is set
at 85. The authors of this article are not authorized to
recommend alterations to this cut-off, but the results from
the present sample propose that further research might
enable improvements in the utility of parts of the screening
instrument in a psychiatric setting.
The HASI was developed to indicate the possible
presence of ID, but not to be used for diagnostic pur-
poses (16). The HASI allows identifi cation of people
with a need for further assessment with full-scale neu-
ropsychological examinations. It is designed to be over-
inclusive, and may also identify individuals suffering
from a psychiatric illness or substance abuse disorder, or
who cannot speak the language properly (22). According
to Hayes (22), a cut-off score of 85 on the HASI was
originally found to be the optimum for discriminating
between participants with and without ID.
The possible correlation between the HASI and the
WASI is infl uenced by the fact that WASI measures IQ
throughout the range of scores, while the HASI has a
maximum score of 96.4. For participants with a WASI
IQ above 96.4, it will thus not be meaningful to deter-
mine the correlation with the HASI score. The HASI
was developed as a screening instrument for ID and it is
not sensitive to performance in the higher range of IQ
scores.
The HASI was sensitive to participants with an ID
and it was over-inclusive with many false positives. A
coeffi cient of α � 0.67 was obtained for internal consis-
tency, indicating that the scale measured a reasonably
consistent concept. According to Nunnally (36), a reli-
ability coeffi cient of 0.6 and more can be described as
moderate.
Concerning the subtest “Background information”,
several interesting results were found. In this part of the
test, patients are asked four questions concerning ID.
Several of the patients with ID denied or lacked insight
into their ID. Lyall et al. (37) found that the application
of questions related to ID was problematic because of
the negative connotations of ID. Several of the ID
patients in their study also denied their ID. In addition,
they did not report that they had attended a special-needs
school. Other studies have found that people may not
accept such labels as applicable to them and may defi ne
their own problems in different ways. This population
50
may have been in contact with professionals and may
have experienced that the information they gave could
have negative consequences. This might lead to evasive
answers. Other background items might possibly replace
the exciting items.
As a consequence of these issues, the subtest “Back-
ground information” did not correlate very well either
with the other HASI subtests, or with the WASI. Possi-
bly the subtest items should be studied and improved in
psychiatric populations.
The “Background information” subtest has demon-
strated signifi cant correlation with IQ in previous studies
(16, 20, 38), and the results based on the small sample
in the present study suggest the need for further research
on a larger sample. The limited sample also represents a
problem in measuring sensitivity and specifi city of the
screening instrument. Using the Wilson (score) method,
these calculations are meaningful even with small counts
as we have (35). The Wilson method is also generally
preferable when sensitivity or specifi city proportions are
close to or 100%, as found in the study (35). It is possi-
ble that inadequacies in the translation or differences in
the welfare system infl uenced the scores obtained using
the Norwegian version of the HASI. The HASI is copy-
righted and cannot be altered without specifi c permis-
sion. If such permission were granted, a modifi ed version
of the HASI should probably include a substitute for the
background information subtest.
As the HASI and the WASI correlate well, the HASI
may prove to be a useful and time-saving tool for psy-
chiatric services in identifying people with a need for
specially adapted treatment related to ID or other cogni-
tive defi ciencies. Employees in these services often lack
the competence as well as the tools and resources to
evaluate such problems properly. A further obstacle is
that most tests must be administered by certifi ed person-
nel. The HASI may be helpful in the process of identify-
ing people with cognitive defi ciencies, who should then
be referred for further assessment. It was designed to be
administered and scored by non-psychologists such as
correctional offi cers, police, probation and parole person-
nel, lawyers, welfare and mental health workers, drug
and alcohol workers, and medical practitioners, including
psychiatrists (16). This test may help to bridge the gap
between local services and the specialized health services,
and therefore make it easier for people with undetected
needs caused by ID to get appropriate help.
As a quick and highly available instrument, the HASI
can become an effective resource for detecting diffi cul-
ties. The fact that a large number of psychiatric patients
also have undetected ID (9) may diminish the value of
care and treatment decisions. A thorough prevalence
study of ID in specifi c psychiatric patient samples would
be valuable. Adaptation of the services offered to these
patients might stimulate progress in this fi eld.
NORD J PSYCHIATRY·VOL 65·NO 1·2011

INTELLECTUAL DIFFICULTIES IN PSYCHIATRIC PATIENTS
Erik S ø ndenaa, Ph.D., Norwegian University of Science and Technol-ogy and St. Olavs Hospital. Ø yvind Nyg å rd, M.D. student, Norwegian University of Science and Technology. Jim Aage N ø ttestad, Dr.philos., Associate Professor, Norwegian University of Science and Technology and St. Olavs Hospital. Olav Martin Linaker, M.D., Professor, Norwegian University of Science and Technology and St. Olavs Hospital.
Nor
d J
Psyc
hiat
ry D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y U
nive
rsity
of
Ade
laid
e on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.
Declaration of interest: The authors report no confl icts of
interest. The authors alone are responsible for the content
and writing of the paper.
References Roeleveld N, Zielhuis GA, Gabriels F. The prevalence of mental 1. retardation: A critical review of recent literature. Devel Med Child Neurol 1997;39:125–32. Leonard H, Wen X. The epidemiology of mental retardation: 2. Challenges and opportunities in the new millennium. Ment Retard Devel Disabil Res Rev 2002;8:117–34. Emerson E, Hatton C, Felce D, Murphy GH. Learning Disabili-3. ties. The fundamental facts. London: The Mental Health Founda-tion (Foundation for people with learning disabilities); 2001. Ministry of Local Government and Regional Development. Crite-4. ria for income in local communities. http://dep.no/fi larkiv/256170/vedlegg_2.pdf (accessed August 21, 2006). Gjærum B, Gr ø svik K. Psykisk utviklingshemming/ mental 5. retardasjon. In: Gjærum B, Ellertsen B, editors. Hjerne og atferd; utviklingsforstyrrelser hos barn og ungdom i et nevrobiologisk perspektiv, 2nd edition. Oslo: Gyldendal Akademisk; 2002. Richards M, Maughan B, Hardy R. Long-term Affective disorder 6. in people with mild learning disability. Br J Psychiatry 2001;179:523–7. Greenwood CMT, Husted J, Bomba MD, Hodgkinson KA, Bassett 7. AS. Elevated rates of schizophrenia in a familial sample with mental illness and intellectual disability. J Intellect Disabil Res 2004;48:531–9. Corbett JA. Psychiatric morbidity and mental retardation. In: 8. James FE, Snaith RP, eds. Psychotherapy in the mentally retarded. New York: Grune and Stratton; 1979. Linaker OM. 20.000 kan være “skjulte” utviklingshemmede 9. 20,000 people may have “hidden” intellectual disabilities. Dagens medisin; 2007. Kaufmann AS, Kaufmann NL. Kaufmann Brief Intelligence Test 10. Manual. Circle Pines, MN: American Guidance Service; 1990. Spreen O, Strauss E. A compendium of neuropsychological tests, 11. 2nd edition. New York: Oxford University Press; 1998. Walters SO, Weaver KA. Relationships between the Kaufmann Brief 12. Intelligence Test and the Wechsler Adult Intelligence Scale—Third edition. Psychol Rep 2003;92:1111–5. Folstein MF, Folstein SE, McHugh PR. Mini-Mental State: A practi-13. cal method of grading the cognitive state of patients for the clini-cian. J Psychiat Res 1975;12:189–98. Wechsler D. Wechsler abbreviated scale of intelligence manual. San 14. Antonio, TX: Harcourt Brace & Company; 1999. Wechsler D, Nyman H, Nordvik H. WAIS-III: Wechsler Adult Intel-15. ligence Scale: Manual (Norwegian edition). Stockholm: Psykologiförlaget; 2003. Hayes S. Hayes Ability Screening Index. Manual. Sydney: Faculty 16. of Medicine. University of Sydney; 2000. Cockram J. Careers of offenders with an intellectual disability: The 17. probabilities of rearrest. J Intellect Disabil Res 2005;49(Pt 7):525–36. Linaker OM. Mental retardation and psychiatry. Past and present. 18. Doctoral thesis, University of Trondheim, Tapir; 1994. Winter N, Holland AJ, Collins S. Factors predisposing to suspected 19. offending by adults with self-reported learning disabilities. Psychol Med 1997;27:595–607.
NORD J PSYCHIATRY·VOL 65·NO 1·2011
S ø ndenaa E, Rasmussen K, Palmstierna T, N ø ttestad JA. The preva-20. lence and nature of intellectual disability in Norwegian prisons. J Intellect Disabil Res. in press. Sparrow S, Balla D, Cicchetti D. Vineland Adaptive Behavior 21. Scales, Survey edition. MN: Circle Pines; 1984. Hayes S. Early intervention or early incarceration? Using a screen-22. ing test for intellectual disability in the criminal justice system. J Appl Res Intellect Disabil 2002;15:120–8. War Department. Army individual test: Manuals of directions and 23. scorings. Washington DC; 1944. Reitan RM. Validity of the Trail-Making Test as an indicator of 24. organic brain damage. Perceptual Motor Skills 1958;8:271–6. Brattersly WS, Bender MB, Pollack M, Kahn RL. Unilateral “spatial 25. agnosia” (“inattention”) in patient with cortical lesions. Brain 1956;79:68–93. Osterrieth PA. The Complex Figure Copy Test: Contributions to the 26. study of perception and memory. Arch Psychol 1944;30:206–356. Freedman M, Kaplan E, Delis D, Morris R. Clock drawing: A 27. neuropsychological analysis. New York: Oxford University Press; 1994. Ishiai S, Shuishita M, Ichikawa T, Gono S, Watabiki S. Clock 28. drawing tests and unilateral spatial neglect. Neurology 1993;43:106–10. Sundet K, Ø rbeck B, Brager-Larsen LM, Bang Nes R. Wechsler 29. Abbreviated Scale of Intelligence (Norwegian version). Oslo: Uni-versity of Oslo; 2000–2001. Brager-Larsen LM, Sundet K, Engvik H, Ø rbeck B, Bang Nes R. 30. Psychometric properties of a Norwegian research version of the Wechsler Abbreviated Scale of Intelligence (WASI). Bull Norwegian Neuropsychol Assoc 2001;4:70. Bosnes O. En sammenligning av Wechsler Adult Intelligence Scale/31. Wechsler Intelligence Scale for Children-Revised med Wechsler Abbreviated Scale of Intelligence i et norsk klinisk utvalg Tidsskrift for Norsk Psykologforening 2005;42:598–602. Merenda PF. An overview of adapting educational and psychological 32. assessment instruments: Past and present. Psychol Rep 2006;99:307–14. Sternberg RJ. Culture and intelligence. Am Psychol 2004;59:325–38. 33. Flaherty JA, Gaviria FM, Pathak D, Mitchell, T. , Wintrob R, 34. Richman JA, Birz S. Developing instruments for cross-cultural psychiatric research. J Nerv Mental Dis 1988;12:189–98. Altman D, Machin D, Bryant T, Gardner S. Statistics with confi -35. dence: Confi dence intervals and statistical guidelines, 2nd edition. London: BMJ Books; 2000. Nunnally JC. Psychometric theory. New York: McGraw-Hill; 1978. 36. Lyall I, Holland AJ, Collins S, Styles P. Incidence of persons with a 37. learning disability detained in police custody: A needs assessment for service development. Med Sci Law 1995;35:61–71. S ø ndenaa E, Bj ø rgen TG, N ø ttestad JA. Validation of the Norwegian 38. version of Hayes Ability Screening Index for mental retardation. Psychol Rep 2007;101:1023–30.
51