Embed Size (px)
Citation preview
Academiejaar 2015 – 2016
VALIDATION OF THE FINNISH DIABETES RISK SCORE (FINDRISC)
FOR DIABETES SCREENING IN THE BELGIAN POPULATION
Dr. Jeroen DE COCKER
Promotor: Prof. dr. E. Rietzschel
Masterproef voorgedragen in de master in de specialistische geneeskunde CARDIOLOGIE

2
! !

3
Academiejaar 2015 – 2016
VALIDATION OF THE FINNISH DIABETES RISK SCORE (FINDRISC)
FOR DIABETES SCREENING IN THE BELGIAN POPULATION
Dr. Jeroen DE COCKER
Promotor: Prof. dr. E. Rietzschel
Masterproef voorgedragen in de master in de specialistische geneeskunde CARDIOLOGIE

4
Table of contents
1. Abstract
2. Introduction
3. Materials and methods
a. Patient population
b. FINDRISC score
c. Statistical analysis
4. Results
a. Patient characteristics
b. Validation of FINDRISC
5. Discussion
6. References
7. Nederlandstalige samenvatting

5
Abstract
Background:
Late detection of type-2 diabetes mellitus significantly increases the risk of major
(cardio)vascular complications. Screening tools such as the Finnish Diabetes Risk Score
(FINDRISC) are important to detect asymptomatic individuals in an early stage of the disease.
The aim of this study is to evaluate the performance of the FINDRISC in predicting type-2
diabetes mellitus in the Belgian population.
Methods:
As part of the Asklepios population study, a total of 1898 healthy individuals aged 35-55
years (coming from one Belgian community) were investigated during a follow-up period of
10 years. Data was collected on all the risk factors in the FINDRISC score and the incidence
of type-2 diabetes mellitus was monitored. Logistic regression was used to evaluate the
predictive ability of every risk factor in the FINDRISC score. The discriminative ability of
FINDRISC to predict the development of type-2 diabetes was investigated using the area
under the receiver-operating curve (AUC-ROC).
Results:
New onset type-2 diabetes mellitus developed in 95 individuals (5.0 % of the population). The
most important independent risk factors in the logistic regression were obesity (OR 9.950;
2.737 – 36.168), high waist circumference (male > 102 cm and female > 88 cm) (OR 4.215;
1.353 – 13.133), history of high blood glucose (OR 3.784; 2.360 – 6.068), first-degree rela-
tives with diabetes (OR 2.805; 1.714 – 4.589) and antihypertensive treatment (OR 1.899;
1.117 – 3.229). Age, physical activity and daily intake of fruit or vegetables were not identi-
fied as significant predictors. At FINDRISC ! 12 the model showed a sensitivity of 0.81 (0.72
- 0.88), a specificity of 0.83 (0.81 - 0.84) and a positive predictive value of 0.20 (0.16 - 0.24).
The FINDRISC showed excellent discriminative ability in predicting development of type-2
diabetes mellitus (AUC 0.88). These findings are consistent with previous studies.
Conclusions:
The FINDRISC score was validated in our study as a tool with high performance and
excellent discriminative ability to predict the development of type-2 diabetes mellitus in the
Belgian community.
6
Introduction
In recent years, the prevalence of type-2 diabetes mellitus is rapidly increasing worldwide (1).
As reported by the World Health Organisation, without effective prevention strategies, the
prevalence of type-2 diabetes will likely continue to increase globally (2). Type-2 diabetes
frequently leads to major (cardio)vascular complications, which in their turn impose a
significant impact on patient life quality and life expentancy (3). Since the disease goes
mostly undetected in the early stages, effective screening tools have gained much importance
over the last years to detect asymptomatic patients with early stages of type-2 diabetes
mellitus (4). One such screening tool that was developed over recent years is the Finnish
Diabetes Risk Score (FINDRISC) (5) (Tables 1 and 2), which since then has been widely
validated and used (6-10). However, to this date the FINDRISC score hasn’t been validated in
the Belgian community. As a result, it remains unclear whether this FINDRISC score can
accurately identify individuals at risk for developing type-2 diabetes mellitus in the Belgian
population. If this is the case, the FINDRISC could be used as a primary screening tool where
individuals with a high FINDRISC score are referred for additional tests to detect type-2
diabetes mellitus, such as measurements of glycated hemoglobin (HbA1c) levels.
In this study, our aim is to test whether the FINDRISC score is valid in the Belgian
community to predict the probability of developing type-2 diabetes mellitus.

7
Table 1. The Finnish Diabetes Risk Score (FINDRISC).
Risk factor Score
1. Age Under 45 years 0 45 – 54 years 2 55 – 64 years 3 Over 64 years 4
2. Body mass index Lower than 25 kg/m2 0 25 – 30 kg/m2 1 Higher than 30 kg/m2 3
3. Waist circumference measured below the ribs MEN WOMEN
Less than 94 cm Less than 80 cm 0 94 – 102 cm 80 – 88 cm 3 More than 102 cm More than 88 cm 4
4. Physical activity ! 30 minutes/day (work, leisure time) Yes 0 No 2
5. Consumption of vegetables, fruit and/or berries Every day 0 Not every day 1
6. Use of antihypertensive medication (past or present) No 0 Yes 2
7. History of high blood glucose (e.g. illness, pregnancy) No 0 Yes 5
8. Family history of of diabetes (type 1 of type 2) No 0 Yes: grandparent, aunt, uncle, or first cousin 3 Yes: parent, brother, sister or own child 5
Table 2. Ten-year risk of developing type-2 diabetes mellitus according to FINDRISC.
Score Risk Interpretation
< 7 Low Estimated 1 in 100 will develop disease
7- 11 Slightly elevated Estimated 1 in 25 will develop disease
12 – 14 Moderate Estimated 1 in 6 will develop disease
15 – 20 High Estimated 1 in 3 will develop disease
> 20 Very high Estimated 1 in 2 will develop disease
8
Materials and methods
Study population
In this study we made use of the Asklepios study population, which is a representative cross-
sectional cohort of 2524 healthy volunteers aged 35-to-55 years old, free from overt cardio-
vascular disease at study initiation, randomly sampled from the twinned Belgian communities
of Erpe-Mere and Nieuwerkerken (11). These individuals underwent a comprehensive cardio-
vascular examination (by means of questionnaires, risk factor assessment, extensive bio-
chemistry panel, electrocardiography, echocardiography and duplex of carotid and femoral
arteries) by a single observer (one study nurse, one physician) at a single study center within a
single 2-year consecutive timeframe. These measurements were performed at baseline (at
study initiation, between October 2002 and September 2004) and were repeated after a time
frame of 10 to 12 years (from 2012 to 2016). Inclusion criteria were male or female volun-
teers aged 35–55 years at study initiation; living in the communities of Erpe-Mere or
Nieuwerkerken. Exclusion criteria were presence of overt cardiovascular disease (clinical
atherosclerosis, atrial fibrillation, heart failure, significant valvular disease), diabetes mellitus,
major co-morbidity, pregnancy, and inability to give informed consent. The primary objective
of the original Asklepios study was to explore the interplay between ageing, diet,
cardiovascular hemodynamics and inflammation. The full details and design of this study is
described elsewhere (11).
In this substudy, we made use of the data of Asklepios participants in whom full 10-year
longitudinal follow-up data were available at the time of analysis (n = 1898). New-onset
diabetes was defined as the presence of drug-treated type-2 diabetes mellitus at the conclusion
of the 10-year follow-up period, in individuals free of type-2 diabetes at baseline examination.
FINDRISC score
The Finnish Diabetes Risk Score (FINDRISC) is a risk stratification tool developed by
Finnish authors Lindström and Tuomilehto and was first published in 2003 (5). They investi-
gated the incidence of type-2 diabetes in a random population sample of 4435 healthy
individuals aged 25–64 years over a follow-up period of 10 years (from January 1987 to

9
December 1997). Eight risk factors for new-onset type-2 diabetes were identified through
multivariate logistic regression and were assigned a score according to their weight (Table 1).
Summation of these individual scores gives result to a comprehensive diabetes risk score
ranging 0 to 26, where a score < 12 indicates a low risk, a score ranging 12-20 indicates a
high risk and a score > 20 indicates a very high risk for development of type-2 diabetes
mellitus (Table 2).
In the Asklepios study database, data on all the risk factors included in the FINDRISC score is
readily available. Age, body-mass index (BMI) and waist circumference were recorded as
continuous variables and were subsequently categorized according to the prespecified risk
categories in the FINDRISC score. An extensive diary of food intake made it possible to
identify subjects eating vegetables or fruit on a daily basis. Drug use was recorded for all
patients throughout the study, which made it possible to identify those patients on antihyper-
tensive treatment. A history of high blood glucose was defined as either a reported history of
pregnancy diabetes, or a high fasting blood glucose (FBG > 100 mg/dl) as documented on
biochemistry screening at baseline examination. An extensive familial history was obtained
throughout the study, which made it possible to identify subjects with positive familial history
for diabetes mellitus (type 1 and 2, first and second degree relatives). Finally, the presence of
moderate to vigorous physical activity > 30 minutes daily was derived from the self-reported
questionnaire data on work-related and leisure-time physical activity.
Statistical analysis
Statistical analyses were performed using the IBM Statistical Package for the Social Sciences
(SPSS) software for MacIntosh version 23.0 (International Business Machines Corporation,
Armonk, New York, U.S.A.).
Baseline characteristics were computed for the total population and according to FINDRISC
class. For continuous variables, means were compared between categories using the one-way
ANOVA test. For categorical variables, the "2 test was used to compare frequencies between
FINDRISC categories. Values were assessed as missing at random (though not ‘missing
completely at random’ as Little’s test demonstrated a P-value < 0.05). A multiple imputation
strategy (12) was used to deal with the missing values (50 iterations were used).

10
Multivariate binary logistic regression analysis was performed to assess the impact of the
FINDRISC risk factors on the incidence of type-2 diabetes mellitus in the Asklepios
population. The Hosmer-Lemeshow test and Brier score were used to evaluate the calibration
of the model (13-14).
Finally, the performance of the FINDRISC score was assessed by computing the sensitivity
and specificity, as well as the positive/negative predictive values and positive/negative likeli-
hood ratios for every stratum of the FINDRISC score. A receiver operating characteristic
curve (ROC) was drawn based on this data and an area under the curve (AUC) was calculated
to assess the discriminative power of the FINDRISC score in the Asklepios population (15).

11
Results
Baseline characteristics
Descriptive statistics at baseline examination (study period 2002 – 2004) were obtained for all
variables and are summarized in Table 3. Mean age in the total population was 45.7 years
with a slight female predominance of 51.4 %. A body mass index (BMI) > 30 kg/m2 was
observed in 13.7 % of subjects and a waist circumference > 102 cm for men and > 88 cm for
women was observed in 18.8 % of subjects. Fifty-eight per cent of subjects reported a daily
moderate to vigorous physical activity of more than 30 minutes. Only 9.8 % of subjects were
on antihypertensive treatment, whereas 13.9 % had a history of raised fasting blood glucose.
Finally, twenty-five per cent of individuals reported a positive family history for diabetes
mellitus in a first-degree family member. Significant differences were demonstrated for all
variables across FINDRISC categories, with a greater incidence of each risk factor in the high
and very-high risk categories, except for gender (P = 0.2) and daily intake of fruit and vegeta-
bles (P = 0.1). Missing values were infrequent: BMI (1 case), waist circumference (25 cases),
physical activity (3 cases), dietary intake (26 cases) and familial history (9 cases).
The FINDRISC ranged from 0 to 24 and had a symmetrical distribution (Figure 1), with
skewness lower than one (0.71) and kurtosis near zero (0.02). The mean FINDRISC score was
7.45 ± 4.85. There was a median FINDRISC score of 7, with an interquartile range (IQR) of 7
(Q1 = 3; Q3 = 10). A moderate risk for developing diabetes (FINDRISC 12 – 14) was present
in 10.3 % of cases, whereas a high to very high risk (FINDRISC > 14) was present in 10.4 %
of cases. New-onset type-2 diabetes mellitus occured in 95 individuals (5.0 %), of which 55
are male.
Validation of FINDRISC
Results of the binary logistic regression analysis are shown in Table 4. The !-coefficients are
shown with their significance level and odds ratios are calculated. The strongest independent
predictive factor for development of type-2 diabetes mellitus is obesity (body mass index > 30
kg/m2) with an odds ratio of 9.950 (95% C.I. 2.737 – 36.168). Next is high waist circumfer-
ence (male > 102 cm and female > 88 cm) with an odds ratio of 4.215 (95% C.I 1.353 –
13.133). Other significant predictors are history of high blood glucose (odds ratio 3.784; 95%

12
C.I. 2.360 – 6.068), first-degree relatives with diabetes (odds ratio 2.805; 95% C.I. 1.714 –
4.589) and antihypertensive treatment (odds ratio 1.899; 95% C.I. 1.117 – 3.229).
Age, physical activity and daily intake of fruit or vegetables are not significant in this study.
The Hosmer-Lemeshow test (P > 0.2) and Brier score (0.039) showed good calibration.
Figure 1. Distribution of FINDRISC score in the Asklepios population. Histogram
depicting the FINDRISC score on the X-axis and the frequency on the Y-axis. The full
line represents the normal distribution.
13
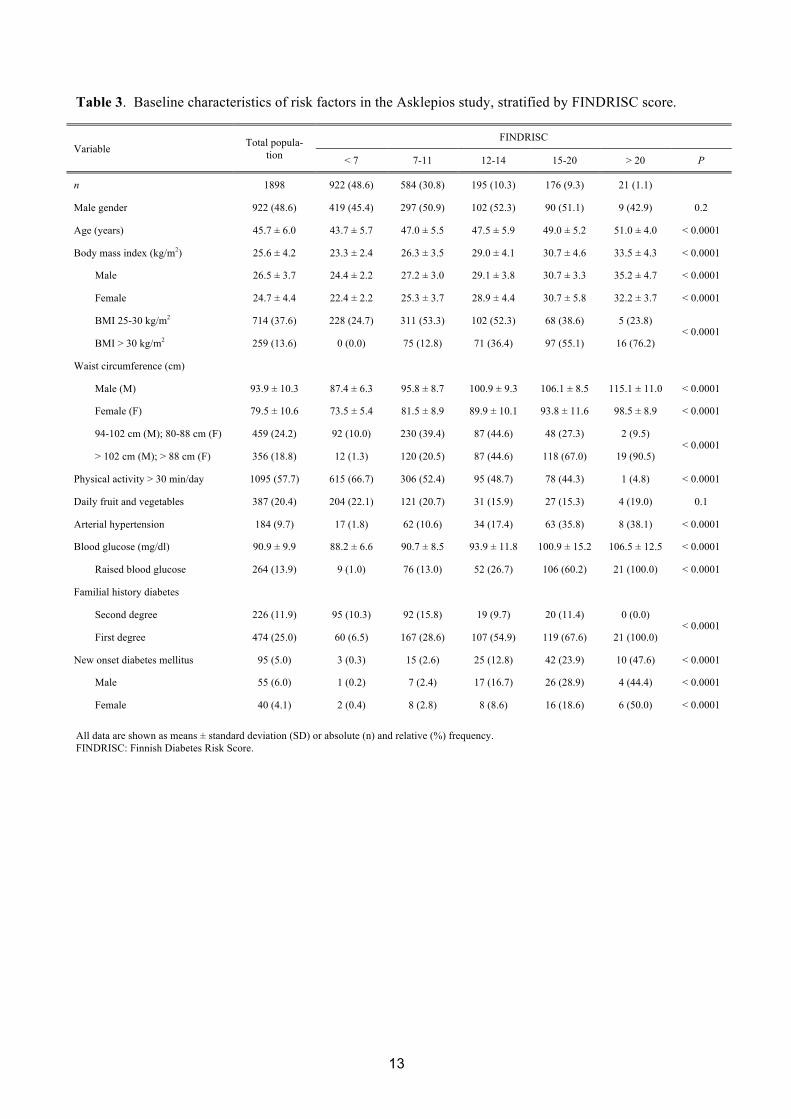
Table 3. Baseline characteristics of risk factors in the Asklepios study, stratified by FINDRISC score.
Variable Total popula-tion
FINDRISC
< 7 7-11 12-14 15-20 > 20 P
n 1898 922 (48.6) 584 (30.8) 195 (10.3) 176 (9.3) 21 (1.1)
Male gender 922 (48.6) 419 (45.4) 297 (50.9) 102 (52.3) 90 (51.1) 9 (42.9) 0.2
Age (years) 45.7 ± 6.0 43.7 ± 5.7 47.0 ± 5.5 47.5 ± 5.9 49.0 ± 5.2 51.0 ± 4.0 < 0.0001
Body mass index (kg/m2) 25.6 ± 4.2 23.3 ± 2.4 26.3 ± 3.5 29.0 ± 4.1 30.7 ± 4.6 33.5 ± 4.3 < 0.0001
Male 26.5 ± 3.7 24.4 ± 2.2 27.2 ± 3.0 29.1 ± 3.8 30.7 ± 3.3 35.2 ± 4.7 < 0.0001
Female 24.7 ± 4.4 22.4 ± 2.2 25.3 ± 3.7 28.9 ± 4.4 30.7 ± 5.8 32.2 ± 3.7 < 0.0001
BMI 25-30 kg/m2 714 (37.6) 228 (24.7) 311 (53.3) 102 (52.3) 68 (38.6) 5 (23.8) < 0.0001
BMI > 30 kg/m2 259 (13.6) 0 (0.0) 75 (12.8) 71 (36.4) 97 (55.1) 16 (76.2)
Waist circumference (cm)
Male (M) 93.9 ± 10.3 87.4 ± 6.3 95.8 ± 8.7 100.9 ± 9.3 106.1 ± 8.5 115.1 ± 11.0 < 0.0001
Female (F) 79.5 ± 10.6 73.5 ± 5.4 81.5 ± 8.9 89.9 ± 10.1 93.8 ± 11.6 98.5 ± 8.9 < 0.0001
94-102 cm (M); 80-88 cm (F) 459 (24.2) 92 (10.0) 230 (39.4) 87 (44.6) 48 (27.3) 2 (9.5) < 0.0001
> 102 cm (M); > 88 cm (F) 356 (18.8) 12 (1.3) 120 (20.5) 87 (44.6) 118 (67.0) 19 (90.5)
Physical activity > 30 min/day 1095 (57.7) 615 (66.7) 306 (52.4) 95 (48.7) 78 (44.3) 1 (4.8) < 0.0001
Daily fruit and vegetables 387 (20.4) 204 (22.1) 121 (20.7) 31 (15.9) 27 (15.3) 4 (19.0) 0.1
Arterial hypertension 184 (9.7) 17 (1.8) 62 (10.6) 34 (17.4) 63 (35.8) 8 (38.1) < 0.0001
Blood glucose (mg/dl) 90.9 ± 9.9 88.2 ± 6.6 90.7 ± 8.5 93.9 ± 11.8 100.9 ± 15.2 106.5 ± 12.5 < 0.0001
Raised blood glucose 264 (13.9) 9 (1.0) 76 (13.0) 52 (26.7) 106 (60.2) 21 (100.0) < 0.0001
Familial history diabetes
Second degree 226 (11.9) 95 (10.3) 92 (15.8) 19 (9.7) 20 (11.4) 0 (0.0) < 0.0001
First degree 474 (25.0) 60 (6.5) 167 (28.6) 107 (54.9) 119 (67.6) 21 (100.0)
New onset diabetes mellitus 95 (5.0) 3 (0.3) 15 (2.6) 25 (12.8) 42 (23.9) 10 (47.6) < 0.0001
Male 55 (6.0) 1 (0.2) 7 (2.4) 17 (16.7) 26 (28.9) 4 (44.4) < 0.0001
Female 40 (4.1) 2 (0.4) 8 (2.8) 8 (8.6) 16 (18.6) 6 (50.0) < 0.0001
All data are shown as means ± standard deviation (SD) or absolute (n) and relative (%) frequency. FINDRISC: Finnish Diabetes Risk Score.

14
Table 4. Logistic regression of FINDRISC covariates with new onset diabetes mellitus as dependent variable.
Hosmer-Lemeshow goodness of fit: P = 0.230. Brier score: 0.039. Hosmer-Lemeshow goodness of fit: P = 0.611. Brier score: 0.039.
C.I.: confidence interval.
Full FINDRISC model Concise FINDRISC model
Predictor Odds ratio (with 95% C.I.) !-coefficient P-value Odds ratio (with 95% C.I.) !-coefficient P-value
Intercept - 6.186 - 6.110
Age ! 45 years 1.428 (0.854 – 2.387) 0.356 0.2 –––– –––– ––––
Body mass index
25 – 30 kg/m2 2.759 (0.942 – 8.081) 1.015 0.08 2.721 (1.036 – 7.144) 1.001 0.08
> 30 kg/m2 9.884 (2.728 – 35.811) 2.291 0.0005 9.320 (2.604 – 33.362) 2.232 0.0006
Waist circumference
Men 94 - 102 cm; women 80 - 88 cm 3.020 (1,109 – 8,220) 1.105 0.03 3.205 (1,184 – 8,673) 1.165 0.02
Men > 102 cm; women > 88 cm 4.238 (1.363 – 13.173) 1.444 0.01 4.761 (1.557 – 14.560) 1.560 0.006
Physical activity > 30 minutes /day 0.815 (0.511 – 1.298) - 0.205 0.4 –––– –––– ––––
Daily intake of vegetables or fruit 1.059 (0.603 – 1.861) 0.057 0.8 –––– –––– ––––
Use of blood pressure medication 1.900 (1.120 – 3.224) 0.642 0.02 1.987 (1.179 – 3.349) 0.686 0.01
History of high blood glucose 3.800 (2.372 – 6.068) 1.335 < 0.0001 3.962 (2.485 – 6.317) 1.377 < 0.0001
Positive family history for diabetes mellitus
Second degree relatives 1.672 (0.738 – 3.785) 0.514 0.2 1.534 (0.682 – 3.449) 0.428 0.3
First degree relatives 2.818 (1.726 – 4.601) 1.036 < 0.0001 2.774 (1.706 – 4.513) 1.020 < 0.0001

15
The sensitivity, specificity and predictive values of the FINDRISC score were calculated for
each level (Table 5). The best compromise between sensitivity and specificity was observed at
FINDRISC cut-offs ! 10 (sensitivity 0.87 [0.79 - 0.93]); specificity 0.73 [0.71 - 0.75]), ! 11
(sensitivity 0.82 [0.73 - 0.89]; specificity 0.79 [0.77 - 0.81]) and ! 12 (sensitivity 0.81 [0.72 -
0.88]; specificity 0.83 [0.81 - 0.84]). The positive predictive values (PPV) at these levels are
0.15 (0.12 - 0.18), 0.17 (0.14 - 0.21) and 0.20 (0.16 - 0.24) respectively.
Furthermore, a receiver operating curve was plotted (Figure 1), to assess the ability of the
model to discriminate between individuals who will develop type-2 diabetes mellitus and
those who won’t. The area under the curve (AUC; also known as C-statistic) is 0.88 (95% C.I.
0.85 – 0.91; P < 0.0001), which implicates an excellent discriminitive ability of the
FINDRISC score in this study.
Figure 2. Receiver operating characteric curve of FINDRISC score.

16
Table 5. Performance of FINDRISC in predicting drug-treated type 2 diabetes mellitus in the Asklepios population.
FINDRISC: Finnish Diabetes Risk Score. C.I.: confidence interval.
FINDRISC Sensitivity (95% C.I.) Specificity (95% C.I.) Predictive values (PV) Likelihood ratios (LR)
Positive PV (95% C.I.) Negative PV (95% C.I.) Positive LR (95% C.I.) Negative LR (95% C.I.)
0 1.00 (0.96 - 1.00) 0.00 (0.00 - 0.00) 0.05 (0.04 - 0.06) 0.00 (-) 1.00 (1.00 - 1.00) 0.00 (-)
! 1 1.00 (0.96 - 1.00) 0.02 (0.01 - 0.03) 0.05 (0.04 - 0.06) 1.00 (0.91 - 1.00) 1.02 (1.01 - 1.03) 0.00 (-)
! 2 1.00 (0.96 - 1.00) 0.10 (0.09 - 0.12) 0.06 (0.05 - 0.07) 1.00 (0.98 - 1.00) 1.11 (1.09 - 1.13) 0.00 (-)
! 3 1.00 (0.96 - 1.00) 0.15 (0.13 - 0.16) 0.06 (0.05 - 0.07) 1.00 (0.99 - 1.00) 1.17 (1.15 - 1.19) 0.00 (-)
! 4 1.00 (0.96 - 1.00) 0.27 (0.25 - 0.29) 0.07 (0.05 - 0.08) 1.00 (0.99 - 1.00) 1.36 (1.32 - 1.40) 0.00 (-)
! 5 1.00 (0.96 - 1.00) 0.34 (0.32 - 0.36) 0.07 (0.06 - 0.09) 1.00 (0.99 - 1.00) 1.52 (1.47 - 1.57) 0.00 (-)
! 6 0.98 (0.93 - 1.00) 0.42 (0.40 - 0.44) 0.08 (0.07 - 0.10) 1.00 (0.99 - 1.00) 1.68 (1.60 - 1.77) 0.05 (0.01 - 0.20)
! 7 0.97 (0.91 - 0.99) 0.51 (0.49 - 0.53) 0.09 (0.08 - 0.11) 1.00 (0.99 - 1.00) 1.98 (1.86 - 2.10) 0.06 (0.02 - 0.19)
! 8 0.94 (0.87 - 0.98) 0.58 (0.56 - 0.61) 0.11 (0.09 - 0.13) 0.99 (0.99 - 1.00) 2.25 (2.09 - 2.43) 0.11 (0.05 - 0.24)
! 9 0.93 (0.85 - 0.97) 0.66 (0.64 - 0.69) 0.13 (0.10 - 0.15) 0.99 (0.99 - 1.00) 2.76 (2.53 - 3.00) 0.11 (0.05 - 0.23)
! 10 0.87 (0.79 - 0.93) 0.73 (0.71 - 0.75) 0.15 (0.12 - 0.18) 0.99 (0.98 - 1.00) 3.23 (2.90 - 3.59) 0.17 (0.10 - 0.29)
! 11 0.82 (0.73 - 0.89) 0.79 (0.77 - 0.81) 0.17 (0.14 - 0.21) 0.99 (0.98 - 0.99) 3.85 (3.38 - 4.37) 0.23 (0.15 - 0.35)
! 12 0.81 (0.72 - 0.88) 0.83 (0.81 - 0.84) 0.20 (0.16 - 0.24) 0.99 (0.98 - 0.99) 4.64 (4.03 - 5.33) 0.23 (0.15 - 0.35)
! 13 0.67 (0.57 - 0.77) 0.87 (0.86 - 0.89) 0.22 (0.17 - 0.27) 0.98 (0.97 - 0.99) 5.35 (4.45 - 6.44) 0.37 (0.28 - 0.50)
! 14 0.61 (0.51 - 0.71) 0.90 (0.89 - 0.92) 0.25 (0.19 - 0.31) 0.98 (0.97 - 0.98) 6.29 (5.08 - 7.79) 0.43 (0.34 - 0.56)
! 15 0.55 (0.44 - 0.65) 0.92 (0.91 - 0.93) 0.26 (0.20 - 0.33) 0.97 (0.97 - 0.98) 6.81 (5.35 - 8.66) 0.49 (0.39 - 0.61)
! 16 0.42 (0.32 - 0.53) 0.95 (0.94 - 0.96) 0.29 (0.22 - 0.38) 0.97 (0.96 - 0.98) 7.91 (5.82 - 10.74) 0.61 (0.51 - 0.73)
! 17 0.38 (0.28 - 0.48) 0.96 (0.95 - 0.97) 0.33 (0.24 - 0.43) 0.97 (0.96 - 0.97) 9.36 (6.65 - 13.17) 0.65 (0.55 - 0.76)
! 18 0.28 (0.20 - 0.39) 0.98 (0.97 - 0.99) 0.42 (0.30 - 0.55) 0.96 (0.95 - 0.97) 13.85 (8.82 - 21.75) 0.73 (0.64 - 0.83)
! 19 0.23 (0.15 - 0.33) 0.99 (0.98 - 0.99) 0.45 (0.31 - 0.60) 0.96 (0.95 - 0.97) 15.46 (9.16 - 26.11) 0.78 (0.70 - 0.87)
! 20 0.15 (0.08 - 0.23) 0.99 (0.98 - 0.99) 0.45 (0.27 - 0.64) 0.96 (0.95 - 0.97) 15.63 (7.95 - 30.75) 0.86 (0.79 - 0.94)
! 21 0.11 (0.05 - 0.19) 0.99 (0.99 - 1.00) 0.48 (0.26 - 0.70) 0.95 (0.94 - 0.96) 17.25 (7.51 - 39.61) 0.90 (0.84 - 0.96)
! 22 0.09 (0.04 - 0.17) 1.00 (0.99 - 1.00) 0.56 (0.30 - 0.80) 0.95 (0.94 - 0.96) 24.40 (9.29 - 64.11) 0.91 (0.85 - 0.97)
! 23 0.02 (0.00 - 0.07) 1.00 (1.00 - 1.00) 0.50 (0.07 - 0.93) 0.95 (0.94 - 0.96) 18.98 (2.70 - 133.28) 0.98 (0.95 - 1.01)
! 24 0.01 (0.00 - 0.06) 1.00 (1.00 - 1.00) 0.50 (0.01 - 0.99) 0.95 (0.94 - 0.96) 18.98 (1.20 - 301.12) 0.99 (0.97 - 1.01)
! 25 0.00 (0.00 - 0.04) 1.00 (1.00 - 1.00) 0.00 (-) 0.95 (0.94 - 0.96) 0.00 (-) 1.00 (1.00 - 1.00)
17
Discussion
Previous studies have shown that early detection of type-2 diabetes mellitus improves patient
outcome in terms of preventing (cardio)vascular complications and improving quality of life
as well as life expectancy. However, evidence for screening the entire population for incident
type-2 diabetes mellitus remains scarse (16). It has been demonstrated that lifestyle
modifications (such as increased physical activity, weight loss) and pharmacotherapy can alter
the risk of developing type-2 diabetes in patients with increased risk (17-18). Targeting
patients at risk can be done by means of biochemical analyses such as fasting blood glucose
or glucose tolerance testing. However, as useful as these screening tools are, they remain
rather unpractical in use for general practitioners (19). Other screening tools such as
hemoglobin A1c are relatively expensive to consider for population screening. In contrast,
risk scores that combine a handful well-known and easy to obtain risk factors have proven to
be both effective and easy to calculate (20). Furthermore, they are cheap and easily
implementable at population level. One such risk score model is the Finnish Diabetes Risk
score (FINDRISC) (5), which has been well-validated and used in many countries worldwide
since its publication in 2003 (6-10). However, since population characteristics can differ from
region to region, risk score models may not be blindly adopted from one region to another and
need to be externally validated in the target population first. In this study, we aimed to
validate the FINDRISC score in a representative cohort of healthy Belgian inhabitants. If
valid, the FINDRISC can be used to help identify individuals at risk of developing type-2
diabetes mellitus, in whom additional biochemical testing (hemoglobin A1c, fasting blood
glucose, glucose tolerance test) should be strongly considered.
In this study, we made use of the data available in the Asklepios longitudinal population
study, which is a large prospective cohort study that was originally set up in 2002 to
investigate the interplay between ageing, cardiovascular haemodynamics and inflammation in
preclinical cardiovascular disease (11). As part of this study, a substantial mass of information
was gathered in a prospective manner, including extensive biometrical and biochemical data,
as well as information on drug therapy and a wide array of data coming from questionnaires.
As a result, all the information needed to calculate a FINDRISC score was readily available in
the Asklepios dataset. Albeit new-onset type-2 diabetes mellitus was not defined as a primary
endpoint in the Asklepios study, information on the incidence of type-2 diabetes mellitus was
prospectively gathered during the course of the study. Furthermore, the design of the study

18
and the studied population is quite similar to that of the original FINDRISC study, in that a
similar number of healthy adult individuals (without diabetes mellitus or known
cardiovascular disease), from a certain region or community, were longitudinally followed up
for a period of 10 years. Both studies started with a questionnaire, followed by a clinical visit.
Main difference is the studied age category, ranging from 25 to 65 years in the Finnish study,
as compared to 35 to 55 years in our study.
External validation of a risk score model encompasses four distinct features (21): (a) model
fit, (b) calibration, (c) discrimination and (d) generalisability. Model fit relates to the amount
and combination of predictors needed to obtain maximal model accuracy, meaning that
adding or subtracting any predictor will only worsen model accuracy. To avoid problems of
under- or overfitting, the presence of at least 10 outcome events per predictor in the model is
required. A good calibration implies that the predictions based on the score closely match
what is observed. On the contrary, a good discrimination means that the risk model can
reliably distuingish people with a high risk of developing type-2 diabetes from those with a
low risk. Finally, the study sample should be representative for the population in which it will
be used (generalisability).
In our study, 95 outcome events were observed in total. When the 8 predictors from the
FINDRISC score are included in the model, the fit of the model is good (12 outcome events
per predictor). Both the Hosmer-Lemeshow test and Brier score compare the observed
outcome versus the predicted probability. A Hosmer-Lemeshow significance level below 0.05
signifies a bad model calibration; in our analysis the significance level was well above 0.05 (P
= 0.230). A Brier score (BS) of zero signifies a perfect calibration and a Brier score of 0.25
signifies a useless prediction model (22); in our analysis the Brier score was close to zero (BS
= 0.039). Furthermore, the FINDRISC score showed an excellent discrimination evidenced by
an area under the curve (AUC) of 0.88 (AUC > 0.75 indicates very good discrimination; AUC
> 0.80 indicates excellent discrimination). These findings are similar to those of previous
validation studies (6-10). Based on the above findings, we can conclude that we were
successfully able to validate the FINDRISC score in the Belgian population.
Comparison of the results of the logistic regression between our dataset (Table 4) and the
original FINDRISC study (5) shows similar trends. The most important risk factors in both
analyses are history of high blood glucose, obesity and increased waist circumference;
although there is variation in the !-coefficients between both studies. Next is presence of a

19
positive family history for diabetes in the first degree and use of antihypertensive medication.
Age seems to play a lesser role. In our study, we only investigated subjects between 35 and 55
years old. As a result, there is nobody to investigate in the age categories > 55 years. When
comparing age below and above 45 years, we are unable to find a significant difference
between the 2 groups. Similar to the results in the original FINDRISC study, regular physical
activity (> 30 minutes/day) and intake of vegetables/fruit seem to have no significant effect on
the development of type-2 diabetes mellitus. The authors of the FINDRISC study included
these variables in the definitive FINDRISC model to stress their importance in lifestyle
modification therapies (5). When performing a stepwise logistic regression protocol (instead
of entering all the FINDRISC covariates at once in the model), these last 2 covariates are
omitted from the final model together with age (Table 4). However, this has only a limited
effect on the weight of the other risk factors.
The FINDRISC score has good sensitivity and specificity for detecting type-2 diabetes
mellitus (Table 5). At cut-off value ! 10 there is a sensitivity of 87% (79 – 93%), a specificity
of 73% (71 – 75 %), a positive predictive value of 0.15 (0.12 – 0.18) and a negative predictive
value of 0.99 (0.98 – 1.00). The higher the cut-off, the lower the sensitivity and the higher the
specificity and positive predictive value. At cut-off value ! 12 there is a good trade-off
between sensitivity (81%; 72 – 88%) and specificity (83%; 81 – 84 %), with a positive
predictive value of 0.20 (0.16 - 0.24). Furthermore, this cut-off represents the demarcation
line between a low to slightly elevated risk versus a moderate to (very) high risk of
developing type-2 diabetes mellitus in the FINDRISC score. Of all subjects in our study with
a FINDRISC score ! 12, every 1 out of 8 individuals (12.8 %) developed type-2 diabetes
mellitus after 10 years of follow-up. At a FINDRISC score ! 15 (high to very high risk),
every 1 out of 4 individuals (23.9 %) developed type-2 diabetes (Table 6).
The incidence rates in our study are globally a bit lower than in the original FINDRISC study
(5), but the risk increase per FINDRISC category is similar. A possible explanation for the
slightly lower incidence rates of type-2 diabetes mellitus in our study is that full 10-year
follow-up data was only available for about 3 out of 4 individuals (1898/2524; 75.2 %) at the
time of the analysis. It seems plausible that healthy individuals have more incentive to return
for their follow-up visit (since they are still at risk and feel well) than individuals who have
already been diagnosed with type-2 diabetes mellitus, with or without major complications.
However, when comparing the baseline characteristics of the studied and the full Asklepios
20
population (11), no major differences are noted. There only seems to be a slightly higher
prevalence of obesity in the full Asklepios population (15.4 vs. 13.6 %). These findings are
summarized in Table 7. Furthermore, when comparing the 10-year incidence of type-2 diabe-
tes with other population studies in North America and Europe, similar findings are noted (23-
24).
In this study we only investigated healthy individuals aged 35 to 55 years, which is a rather
limited age category when compared to other population studies such as the FINDRISC study
itself where people aged 25 to 64 years were enrolled. Because of this limitation,
we were not able to investigate the effect of elderly age (> 55 years) on the incidence of type-
2 diabetes mellitus in the Belgian population. As a result, the results of this study can only be
extrapolated to the 35 to 55 year-old segment of the population, although age above 55 years
scores only 1 extra point in the FINDRISC score (out of maximal 26 points) when compared
to age category 45 tot 54 years.
In Canada, the FINDRISC score is used to provide recommendations on the use of
hemoglobin A1c in detection of type-2 diabetes mellitus (25). They warrant further screening
with hemoglobin A1c in individuals with a high pre-test probability (FINDRISC score ! 15).
If the hemoglobin A1c is negative, re-screening is recommended every 3 tot 5 years. In
patients with a very high pre-test probability (FINDRISC score ! 21), annual hemoglobin A1c
screening is recommended (25). Based on the findings in this study, the Belgian government
can adapt similar recommendations on hemoglobin A1c screening to the Belgian population.
The main issue here will be to decide at what FINDRISC cut-off you decide to refer
individuals for additional (hemoglobin A1c) testing. An ‘ideal’ primary screening test has a
sensitivity close to 100 %, whereas secondary ‘confirmation’ tests need to possess high speci-
ficity to distinguish the true positives from the false positives. In this case, moving the
FINDRISC cut-off from ! 12 points (sensitivity 81 %) to ! 10 points (sensitivity 87 %)
results in a 9.1 % total (and 59 % relative) increase in individuals referred for further testing.
Lowering the FINDRISC cut-off further to ! 7 points (to obtain a high sensitivity of 97 %),
results in an even more dramatic increase of individuals to be screened (29% total and 190 %
relative increase), which of course has its implications on the health care budget.
21
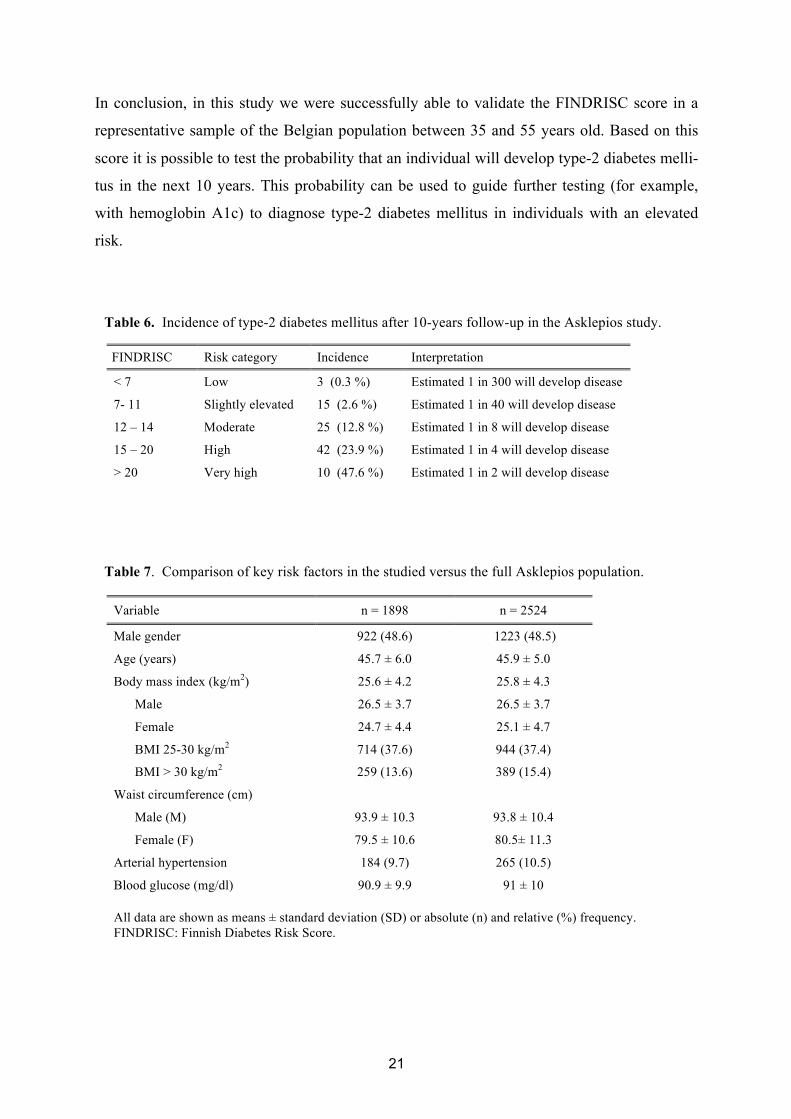
In conclusion, in this study we were successfully able to validate the FINDRISC score in a
representative sample of the Belgian population between 35 and 55 years old. Based on this
score it is possible to test the probability that an individual will develop type-2 diabetes melli-
tus in the next 10 years. This probability can be used to guide further testing (for example,
with hemoglobin A1c) to diagnose type-2 diabetes mellitus in individuals with an elevated
risk.
Table 6. Incidence of type-2 diabetes mellitus after 10-years follow-up in the Asklepios study.
FINDRISC Risk category Incidence Interpretation
< 7 Low 3 (0.3 %) Estimated 1 in 300 will develop disease
7- 11 Slightly elevated 15 (2.6 %) Estimated 1 in 40 will develop disease
12 – 14 Moderate 25 (12.8 %) Estimated 1 in 8 will develop disease
15 – 20 High 42 (23.9 %) Estimated 1 in 4 will develop disease
> 20 Very high 10 (47.6 %) Estimated 1 in 2 will develop disease
Table 7. Comparison of key risk factors in the studied versus the full Asklepios population.
Variable n = 1898 n = 2524
Male gender 922 (48.6) 1223 (48.5)
Age (years) 45.7 ± 6.0 45.9 ± 5.0
Body mass index (kg/m2) 25.6 ± 4.2 25.8 ± 4.3
Male 26.5 ± 3.7 26.5 ± 3.7
Female 24.7 ± 4.4 25.1 ± 4.7
BMI 25-30 kg/m2 714 (37.6) 944 (37.4)
BMI > 30 kg/m2 259 (13.6) 389 (15.4)
Waist circumference (cm)
Male (M) 93.9 ± 10.3 93.8 ± 10.4
Female (F) 79.5 ± 10.6 80.5± 11.3
Arterial hypertension 184 (9.7) 265 (10.5)
Blood glucose (mg/dl) 90.9 ± 9.9 91 ± 10
All data are shown as means ± standard deviation (SD) or absolute (n) and relative (%) frequency. FINDRISC: Finnish Diabetes Risk Score.
22
References
(1) Shaw J, Sicree R, Zimmet P. Global estimates of the prevalence of diabetes for 2010
and 2030. Diabetes Research and Clinical Practice. 2010;87(1):4-14.
(2) Global report on diabetes. World Health Organization; Geneva; 2016. ISBN 978 92
4 156525 7.
(3) Narayan K. Lifetime risk for diabetes mellitus in the United States. JAMA.
2003;290(14):1884.
(4) Noble D, Mathur R, Dent T, Meads C, Greenhalgh T. Risk models and scores for
type 2 diabetes: systematic review. BMJ. 2011;343(1):d7163-d7163.
(5) Lindstrom J, Tuomilehto J. The diabetes risk score: a practical tool to predict type 2
diabetes risk. Diabetes Care. 2003;26(3):725-731.
(6) Franciosi M, De Berardis G, Rossi M, Sacco M, Belfiglio M, Pellegrini F et al. Use
of the diabetes risk score for opportunistic screening of undiagnosed diabetes and
impaired glucose tolerance: the IGLOO (Impaired Glucose Tolerance and Long-
Term Outcomes Observational) study. Diabetes Care. 2005;28(5):1187-1194.
(7) Bergmann A, Li J, Wang L, Schulze J, Bornstein S, Schwarz P. A simplified Finnish
diabetes risk score to predict type 2 diabetes risk and disease evolution in a German
population. Hormone and Metabolic Research. 2007;39(9):677-682.
(8) Makrilakis K, Liatis S, Grammatikou S, Perrea D, Stathi C, Tsiligros P et al.
Validation of the Finnish diabetes risk score (FINDRISC) questionnaire for
screening for undiagnosed type 2 diabetes, dysglycaemia and the metabolic
syndrome in Greece. Diabetes & Metabolism. 2011;37(2):144-151.
(9) Robinson C, Agarwal G, Nerenberg K. Validating the CANRISK prognostic model
for assessing diabetes risk in Canada's multi-ethnic population. Chronic diseases and
injuries in Canada. 2011;32(1):19-31.
(10) Soriguer F, Valdés S, Tapia M, Esteva I, Ruiz de Adana M, Almaraz M et al.
Validation of the FINDRISC (FINnish Diabetes RIsk SCore) for prediction of the
risk of type 2 diabetes in a population of southern Spain. Pizarra Study. Medicina
Clínica. 2012;138(9):371-376.
(11) Rietzschel E, De Buyzere M, Bekaert S, Segers P, De Bacquer D, Cooman L et al.
Rationale, design, methods and baseline characteristics of the Asklepios Study.
European Journal of Cardiovascular Prevention & Rehabilitation. 2007;14(2):179-
191.
23
(12) Gladitz J, Rubin, D. Multiple Imputation for Nonresponse in Surveys. Biom J.
1989;31(1):131-132.
(13) Hosmer D, Lemeshow S. Confidence interval estimates of an index of quality
performance based on logistic regression models. Statist Med. 1995;14(19):2161-
2172.
(14) Dawid A. Probability forecasting. In: Encyclopedia of statistical sciences. John
Wiley & Sons, 1986.
(15) Hanley J, McNeil B. The meaning and use of the area under a receiver operating
characteristic (ROC) curve. Radiology. 1982;143(1):29-36.
(16) Simmons R, Echouffo-Tcheugui J, Griffin S. Screening for type 2 diabetes: an
update of the evidence. Diabetes, Obesity and Metabolism. 2010;12(10):838-844.
(17) Tuomilehto J, Lindström J, Eriksson J, Valle T, Hämäläinen H, Ilanne-Parikka P et
al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with
impaired glucose tolerance. New England Journal of Medicine. 2001;344(18):1343-
1350.
(18) Diabetes Prevention Program Research Group: Reduction in the incidence of type 2
diabetes with lifestyle intervention or metformin. New England Journal of Medicine.
2002;346(6):393-403.
(19) Gillies C, Lambert P, Abrams K, Sutton A, Cooper N, Hsu R et al. Different
strategies for screening and prevention of type 2 diabetes in adults: cost effectiveness
analysis. BMJ. 2008;336(7654):1180-1185.
(20) Mann D, Bertoni A, Shimbo D, Carnethon M, Chen H, Jenny N, et al. Comparative
validity of 3 diabetes mellitus risk prediction scoring models in a multiethnic US
cohort: the Multi-Ethnic Study of Atherosclerosis. American Journal of
Epidemiology. 2010;171(9):980-988.
(21) Harrell F Jr, Lee K, Mark D. Multivariable prognostic models: issues in developing
models, evaluating assumptions and adequacy, and measuring and reducing errors.
Stat Med 1996;15(4):361-368.
(22) Arkes H, Dawson N, Speroff T, Harrell F, Alzola C, Philips R et al. The covariance
decomposition of the probability score and its use in evaluating prognostic estimates.
Med Decis Making. 1995;15(2):120–131.
(23) Diabetes Prevention Program Research Group. 10-year follow-up of diabetes
incidence and weight loss in the Diabetes Prevention Program Outcomes Study.
Lancet 2009;374:1677–1686.

24
(24) Lindström J, Ilanne-Parikka P, Peltonen M, Aunola S, Eriksson J, Hemiö K et al.
Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: fol-
low-up of the Finnish Diabetes Prevention Study. Lancet 2006;368:1673–1679.
(25) Canadian Task Force on Preventive Health Care. Recommendations on screening for
type 2 diabetes in adults. Canadian Medical Association Journal. 2012;184(15):1687-
1696.

25
Nederlandstalige samenvatting
Achtergrond:
Late diagnose van type-2 diabetes mellitus leidt tot een significante toename in de incidentie
van majeure (cardio)vasculaire complicaties. Risico scores zoals de Finnish Diabetes Risk
Score (FINDRISC) kunnen een belangrijke rol spelen in de vroegdetectie van asympto-
matische individuen. Het doel van deze studie is om de performantie van de FINDRISC score
in de Belgische populatie te evalueren.
Methoden:
In het kader van de Asklepios populatie studie werden 1898 gezonde vrijwilligers met leeftijd
35 tot 55 jaar (komende vanuit één gemeenschap in België) onderzocht gedurende een periode
van 10 jaar. Data werd verzameld met betrekking tot alle risico factoren in de FINDRISC
score en de incidentie van type-2 diabetes mellitus werd opgevolgd. Logistische regressie
werd gebruikt om de predictieve waarde van elke risico factor in de FINDRISC score te
evalueren. Het discriminerende vermogen van de FINDRISC score werd onderzocht door het
berekenen van de ruimte onder de receiver-operating curve (AUC-ROC).
Resultaten:
Type-2 diabetes mellitus ontstond in 95 individuen (5.0 % van de populatie). De belangrijkste
risico factoren in de logistische regressie waren obesitas (OR 9.950; 2.737 – 36.168),
buikomtrek > 102 cm bij mannen en > 88 cm bij vrouwen (OR 4.215; 1.353 – 13.133),
voorgeschiedenis van verhoogde glycemie (OR 3.784; 2.360 – 6.068), eerstegraads verwanten
met diabetes (OR 2.805; 1.714 – 4.589) en antihypertensieve behandeling (OR 1.899; 1.117 –
3.229). Leeftijd, fysieke activiteit en dagelijkse inname van fruit of groenten waren geen
significante predictoren. Bij een FINDRISC score ! 12 punten bedraagt de sensitiviteit 0.81
(0.72 - 0.88), de specificiteit 0.83 (0.81 - 0.84) en de positieve predictieve waarde 0.20 (0.16 -
0.24). De FINDRISC score toont verder een excellent disciminerend vermogen getuige een
AUC van 0.88. Deze bevindingen zijn consistent met voorgaande studies.
Conclusies:
De FINDRISC score werd in deze studie gevalideerd als een instrument met een hoge
performantie en een excellent disciminerend vermogen om het ontstaan van type-2 diabetes
mellitus in de Belgische gemeenschap te voorspellen.