Embed Size (px)
Citation preview

Validity of the AM-PAC “6-Clicks”Inpatient Daily Activity and BasicMobility Short FormsDiane U. Jette, Mary Stilphen, Vinoth K. Ranganathan, Sandra D. Passek,Frederick S. Frost, Alan M. Jette
Background. Standardized assessment of patients’ activity limitations in acutecare settings can provide valuable information. Existing measures have not beenwidely implemented.
Objectives. The aim of this study was to provide evidence for validity of scoreson Activity Measure for Post-Acute Care (AM-PAC) “6-Clicks” measures of basicmobility and daily activity in acute care.
Design. A retrospective measurement study was conducted.
Methods. The study used a database from one health system containing “6-Clicks”scores from first and last physical therapist and occupational therapist visits for84,446 patients. Validity was analyzed by examining differences in “6-Clicks” scoresacross categories of patient characteristics; the ability of “6-Clicks” scores to predictpatients’ having more than one therapy visit; correlation of “6-Clicks” scores withFunctional Independence Measure (FIM) scores; and internal responsiveness over theepisode of care. Internal consistency reliability also was determined.
Results. The “6-Clicks” scores differed across patients’ age, preadmission livingsituation, and number of therapy visits. The areas under receiver operating charac-teristic curves derived using “6-Clicks” scores at the first visit to predict patientsreceiving more than one visit were 0.703 and 0.652 using basic mobility and dailyactivity scores, respectively. The “6-Clicks” scores at the final visit were correlatedwith scores on subscales of the FIM completed on admission to inpatient rehabilita-tion facilities (r�.65 and .69). Standardized response means were 1.06 and 0.95 andminimal detectable changes with 90% confidence level (MDC90) were 4.72 and 5.49for basic mobility and daily activity scores, respectively. Internal consistency reliabil-ity of basic mobility and daily activity scores was .96 and .91, respectively.
Limitations. Using clinical databases for research purposes has limitations,including missing data, misclassifications, and selection bias. Rater reliability is notknown.
Conclusions. This study provides evidence for the validity of “6-Clicks” scores forassessing patients’ activity limitations in acute care settings.
D.U. Jette, PT, DSc, FAPTA,Department of Rehabilitation andMovement Sciences, Universityof Vermont, Rowell Building,106 Carrigan Rd, Burlington, VT05405 (USA). Address all corre-spondence to Dr Jette at:[email protected].
M. Stilphen, Rehabilitation andSports Therapy, Cleveland Clinic,Cleveland, Ohio.
V.K. Ranganathan, MSE, MBA,Physical Medicine and Rehabilita-tion, Cleveland Clinic.
S.D. Passek, PT, DPT, Rehabilita-tion and Sports Therapy, Cleve-land Clinic.
F.S. Frost, MD, Physical Medicineand Rehabilitation, ClevelandClinic.
A.M. Jette, PT, PhD, FAPTA,School of Public Health, Healthand Disability Research Institute,Boston University.
[Jette DU, Stilphen M, Rangana-than VK, et al. Validity of theAM-PAC “6-Clicks” inpatient dailyactivity and basic mobility shortforms. Phys Ther. 2014;94:379–391.]
© 2014 American Physical TherapyAssociation
Published Ahead of Print:November 14, 2013
Accepted: November 12, 2013Submitted: May 21, 2013
Research Report
Post a Rapid Response tothis article at:ptjournal.apta.org
March 2014 Volume 94 Number 3 Physical Therapy f 379Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

In the acute care setting, the casemix index of hospitals provides ameans to measure the medical
complexity and burden of illness forthe patients they serve and the needfor resources. No similar measureexists to measure the burden pre-sented by activity limitations in theacute care setting. Impairments inmobility and activities of daily living(ADL) are important drivers of healthcare resource utilization and costs.1
Therefore, the implementation of atool that provides a “footprint” foractivity limitations in hospitalizedpatients could be an important ele-ment for improving the value of hos-pital care. A relatively high propor-tion of patients with neurological,musculoskeletal, and cardiopulmo-nary problems in acute care hospi-tals have limitations in walking, self-care, and changing and maintainingbody positions,2 and these types oflimitations are the focus of care pro-vided by physical therapists andoccupational therapists in this set-ting.3,4 In an era of constrainedresources, there is a pressing need todetermine which patients in acutecare require skilled rehabilitation ser-vices so that personnel can bedeployed in an efficient and effectivemanner.
Studies have shown that the percent-age of patients scheduled for physi-cal therapy, yet not receiving theseservices, may be quite high5 and thatthe time spent by therapists whenpatients cannot be treated may besubstantial.4 Although some visitsthat result in nontreatment are dueto patients being medically unstable,some may be the result of patientsbeing referred who are sufficientlymobile and have sufficient capacityfor functional activity as to notrequire services.6 This problem hasled to exploration of potentialscreening instruments to identifyappropriate referrals and triagepatients in order to improve effi-ciency of rehabilitation services.6,7
Without standardized measurement,clinical recommendations andresource allocation may be subjectto excessive variability, error, andbias.
Although several instruments havebeen developed for measuringpatients’ activity limitations in theacute care setting,8–16 it appearsthey have not been widely imple-mented.17 Recently, Cleveland ClinicHealth System hospitals have pilotedthe use of new standardized instru-ments that allow physical therapistsand occupational therapists to mea-sure basic mobility and daily activityfunctions of patients in the acutecare setting. These tools, called“6-Clicks,” are short forms createdfrom the Activity Measure for Post-Acute Care (AM-PAC) instrument,developed by researchers at BostonUniversity.18 The AM-PAC measures3 functional domains: basic mobility,daily activities, and applied cogni-tion. It may be used for assessmentin adults with a wide range of diag-noses and levels of performance inthe 3 domains. The “6-Clicks” instru-ments may have advantages overthe instruments previously devel-oped for the acute care setting inthat they are simple and quick tocomplete, provide a transparentmeasure of patients’ capabilities infunctional areas important for prior-itization of therapy resources, anduse item response theory to derive acommon metric that can be linkedwith other short forms derived fromthe AM-PAC instrument.19 Thus far,implementation of the “6-Clicks”instruments in acute care at theCleveland Clinic Health System hasallowed clinicians and managers todetermine the feasibility of its imple-mentation in routine patient care;however, its psychometric proper-ties have not been tested. The overallpurpose of this study, therefore, wasto determine clinical validity of the“6-Clicks” basic mobility and dailyactivity short forms.
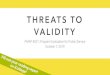
MethodData SourceA clinical database derived and col-lated from the MediLinks electronicmedical record system (EMR) usedby Cleveland Clinic Health Systemphysical therapy and occupationaltherapy departments was the sourceof data for analyses. It containedmore than 200,000 visit entries, withdata on 92,899 individual patientsseen in acute care by physical thera-pists or occupational therapists, orboth, from April 2011 to December2012. We identified 84,466 patientsfor whom we had data for first or lastphysical therapy or occupationaltherapy visits (Fig. 1). The dataincluded in the clinical dataset were“6-Clicks” basic mobility and dailyactivity scores; number of visits byphysical therapists and occupationaltherapists; patient demographicinformation, including age, primarymedical or surgical condition, andpreadmission living situation; lengthof hospital stay; and discharge dispo-sition if patients were dischargedhome with services or to anotherfacility. If patients were admitted toan inpatient rehabilitation facility(IRF) within the Cleveland ClinicHealth System, the admission scoreon the Functional IndependenceMeasure (FIM) was included.
Setting and ProcedureThe Cleveland Clinic Health Systemis a nonprofit system that includes3,700 beds in the main campus hos-pital and 8 regional hospitals. TheRehabilitation and Sports Therapyenterprise includes more than 700therapy professionals, with 90 phys-ical therapists and 45 occupationaltherapists assigned primarily toacute hospital care. These therapistsmanage more than 1,900 patientevaluations per week. The “6-Clicks”items and implementation processwere introduced to staff at a 1-hourin-service meeting that providedthem with the background, ratio-nale, and instructions for comple-
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
380 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

tion. The implementation was partof a broad institutional push for pro-viding uniform, high-quality services.Physical therapists were asked tocomplete the basic mobility shortform, and occupational therapistswere asked to complete the dailyactivity short form. The therapistswere instructed to determine scoresfor each item either by observingpatients’ performance or using theirclinical judgment. The therapistswere familiar with the EMR andentered their patients’ “6-Clicks”scores into the EMR as part of theirvisit documentation.
Patients were discharged to manysettings within the community,some to IRFs within the Cleveland
Clinic Health System. In the Cleve-land Clinic Health System IRFs, theFIM was administered by trained per-sonnel using the standard protocol.20
The dataset used for this studyincluded FIM data from those set-tings. Our dataset did not indicatethe date of this administration; how-ever, the regulations governing IRFsstipulate the assessment must bedone within the first 3 calendar daysfrom admission.20
The institutional review boards ofthe Cleveland Clinic Health Systemand the University of Vermont clas-sified this project as “nonhuman sub-jects” research. The dataset includedonly de-identified data.
InstrumentationThe “6-Clicks” short forms includeitems selected from the calibratedAM-PAC item banks. The AM-PAC is avalidated measure based on the activ-ity limitation domain of the WorldHealth Organization’s InternationalClassification of Functioning, Dis-ability and Health (ICF)21 and isdesigned to be used for patientsreceiving postacute care rehabilita-tion regardless of type of conditionor setting.18 One “6-Clicks” formassesses basic mobility function, andanother assesses daily activities func-tion. The items for each form wereselected for their relevance topatients’ capacity for functionalactivities in an acute care setting andrepresent types of activities that
Figure 1.Data selection flowchart. PT�physical therapist, OT�occupational therapist.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 381Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

physical therapists and occupationaltherapists commonly assess. Theyalso represent the functional activi-ties of most interest to postacuterehabilitation providers screeningpatients for admission to their facili-ties. Each item is scored on 1 of 4levels based on the amount of diffi-culty a patient has or how much helpis needed from another person incompleting the task. Because theitems in the “6-Clicks” forms weredrawn from the calibrated AM-PACitem bank, standardized scores onthe t-score scale (where the mean is50 and the standard deviation is 10)can be generated and used to assessthe level of patients’ activity limita-tions.19 Lower scores equate to agreater degree of limitation. The“6-Clicks” short forms and scoringare shown in Appendixes 1 and 2.Although intended for use in post-acute care settings, one study ofpatients with complex medical andpostsurgical conditions within 3days of discharge from acute careshowed that the AM-PAC might beuseful for assessment of the range offunctional activities in patients inacute care.22
The FIM is a standardized measurewith 18 items that assess patients’level of independence and depen-dence in ADL, mobility, bowel andbladder function, and cognitivefunction. The items are scored on ascale from 1 to 7, with 7 indicatingcomplete independence, based onobservations of patients’ actualperformance.20
Data AnalysisAll analyses were conducted usingIBM-SPSS Statistics version 20 (IBMCorp, Armonk, New York). Descrip-tive statistics were derived todescribe the patients for whom datawere collected at the first or lastphysical therapist or occupationaltherapist visit. All remaining analyseswere conducted separately for basicmobility and daily activities scores.
To determine possible ceiling andfloor effects, we examined the distri-bution of scores derived from thefirst and final visits. Internal consis-tency of initial visit scores for eachform was determined with the Cron-bach alpha.
To assess the validity of the“6-Clicks” scores, we developedreceiver operating characteristic(ROC) curves to determine whetherinitial scores could be used to deter-mine patients needing only one visitversus more than one visit. The ROCanalyses allowed us to determine thesensitivity and specificity for receiv-ing more than one visit for each pos-sible score cutpoint. Using these val-ues for sensitivity and specificity, wecalculated the positive and negativepredictive values assuming 50% ofthe sample received more than onevisit. Calculations were made basedon a standardized 50% prevalence toreduce the effect on predictive val-ues of the study-specific prevalenceof receiving more than one visit. Wealso examined the proportion ofpatients with the highest “6-Clicks”scores receiving more than one visit.Although we realized that physiciansand nurses might request consulta-tions for patients with relatively highlevels of functional activity and,therefore, that these patients wouldbe visited by physical therapists andoccupational therapists, we hypoth-esized that in an efficient system,those patients would not receivemore than one visit.
To determine the construct validityof “6-Clicks” scores, we used analy-ses of variance to examine differ-ences in mean first visit scores across4 age groups (18–40, 41–64, 65–85,and 86� years) and 5 types of pre-admission living situations (homealone, home with others, assistedor independent senior living, IRF orskilled nursing facility, and extendedcare). We also performed trend anal-yses. We used t tests to examine the
first visit score difference for thosewith one therapy visit comparedwith those with more than one visit.We hypothesized that youngerpatients would have higher scores,that patients living at home wouldhave higher scores than those livingin more restrictive settings, and thatpatients with lower scores wouldhave more than one therapy visit.
Construct validity also was examinedusing Pearson correlation coeffi-cients to determine the relationshipof “6-Clicks” basic mobility and dailyactivity scores at the last visit in theacute care setting to the mobility(bed/chair transfer, toilet transfer,shower/tub transfer, locomotion,stairs) and ADL (eating, grooming,bathing, dressing upper body, dress-ing lower body, toileting) compo-nent FIM scores, respectively, at thetime of admission to an IRF setting.
Internal responsiveness23 of thescores on each form was determinedby first estimating the minimaldetectable change with 90% confi-dence level (MDC90) in scores usingthe standard deviation of all initialscores and Cronbach alpha as thereliability coefficient. We then deter-mined the proportion of patientswho had improved, worsened, orstayed the same based on theMDC90. We also calculated the stan-dardized response mean (SRM) andits 95% confidence interval usingscores for patients for whom wehad both first and last visit data.Because patients’ activity limitationsin the acute care setting may worsenas well as improve due to medicalstatus, we calculated the SRM usingthe absolute value of change scores.We interpreted the magnitudes ofeffect statistics using an ordinal scaleproposed by Hopkins.24
ResultsTable 1 includes data describing thepatients in the sample. The meanage was 69.0 years (SD�15.6), and
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
382 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

the majority were women. Approxi-mately 88% of the patients had beenadmitted from their homes, and theyhad a wide variety of primary medi-cal and surgical conditions. Thenumber of physical therapist andoccupational therapist visits forpatients was highly skewed, withmedians of 1 (interquartile range�1–2).
The distributions of scores for the“6-Clicks” forms completed at thefirst visit demonstrated 2.7% and2.3% of responses at the lowest scorefor basic mobility and daily activityforms, respectively. The highest scorewas given for 15.5% of patients com-pleting the basic mobility form, andof all possible scores, this was themost frequent. For the daily activitiesform, the highest score was givenfor 10.1% of patients. The internalconsistency reliability of the basicmobility and daily activity scores was.957 (95% confidence interval [95%CI]�.956, .958) and .911 (95%CI�.909, .912), respectively.
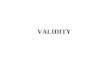
The areas under the ROC curvesderived using “6-Clicks” scores at thefirst visit to predict whether patientsrequired more than one visit com-pared with one visit only were 0.703(95% CI�0.699, 0.707) using basicmobility scores and 0.652 (95%CI�0.648, 0.657) using daily activityscores (Fig. 2). Interestingly, 3.0% ofthe patients with first visit scoresindicating no difficulty in perform-ing, or assistance needed, in basicmobility functions, and 4.9% of thepatients with no difficulty in dailyactivities had more than 1 visit froma physical therapist or occupationaltherapist.
Further evidence for validity of the“6-Clicks” forms is delineated inTable 2. Patients with more than onevisit had lower first visit scores onboth forms compared with thosewith only one visit (P�.001). Therewere also significant differences
(P�.001) in first visit scores for bothforms based on patients’ age, with asignificant trend of older patientsdemonstrating lower scores(P�.001). Scores at the first visit alsosignificantly differed by living situa-tion prior to admission (P�.001); thetrend was significant (P�.001).Those living at home alone or with
others had similar scores; however,scores differed for all other livingsituations, with those in extendedcare settings having the lowestscores (P�.001). Validity was furthersupported by the correlation of“6-Clicks” scores with FIM scores.We had FIM scores for 272 patientswho went to IRFs within the Cleve-
Table 1.Patient Characteristicsa
Characteristic Measurement
Age (y), n (%) (n�84,466)
18–40 4,140 (4.9)
41–64 26,969 (31.9)
65–85 40,988 (48.5)
86� 12,369 (14.6)
Sex, n (%) (n�83,904)
Female 47,464 (56.6)
Male 36,440 (43.4)
Primary diagnosis type, n (%) (n�82,894)
Cardiac disorder 9,723 (11.7)
Endocrine/metabolic disorder 748 (0.9)
GI/GU disorder 10,576 (12.8)
Infection 3,954 (4.8)
Integumetary disorder 1,060 (1.3)
Lymphatic disorder 54 (0.1)
Morbid obesity 132 (0.2)
Neoplasm/cancer 3,684 (4.4)
Neurological disorder 10,085 (12.2)
Obstetrical disorder 70 (0.1)
Orthopedic disorder 18,604 (22.4)
Pain disorder 212 (0.3)
Psychiatric disorder 841 (1.0)
Pulmonary disorder 8,182 (9.9)
Vascular disorder 3,560 (4.3)
Other condition 11,409 (13.8)
Living situation prior to admission, n (%) (n�74,619)
Home alone 17,422 (23.3)
Home with others 48,681 (65.2)
Assisted living or independent senior living 3,626 (4.9)
IRF/SNF 1,733 (2.3)
Long-term or extended care 2,633 (3.5)
Other 524 (0.7)
Length of stay, median (interquartile range) (n�84,272) 5.0 (3.1–8.6)
(Continued)
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 383Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

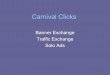
land Clinic hospital system. This sam-ple comprised 7.8% of patients dis-charged to IRFs. Of these patients,we had final visit basic mobilityscores for 170 patients and final visitdaily activity scores for 192 patients,1.2% and 3.1% of all patients forwhom we had final visit basic mobil-ity and daily activity scores, respec-tively. The correlation of the“6-Clicks” basic mobility score at thelast visit with the FIM motor sub-score was large24 (r�.69 [95%CI�.62, .75]), as was the correlationof the “6-Clicks” daily activities scorewith the FIM ADL subscore (r�.65[95% CI�.57, .72]) (Fig. 3).
Mean absolute differences betweenthe scores for first visit and last visitwere 5.71 (95% CI�5.61, 5.80) forbasic mobility and 4.61 (95% CI�4.49,4.73) for daily activity. The SRM was1.06 (95% CI�1.04, 1.08) for basicmobility scores and 0.95 (95%CI�0.95, 0.97) for daily activityscores. Thirty-five percent of thepatients improved in basic mobilityby at least the MDC90 (4.72), and10% worsened by at least the MDC90.
Approximately 27% of the patientsimproved in daily activities by atleast 1 MDC90 (5.49), and 4%worsened.
DiscussionOur findings support the validityof the “6-Clicks” basic mobility anddaily activities scores in assessing theactivity limitations of patients with awide variety of medical and surgicalconditions in an acute care setting.The “6-Clicks” forms were imple-mented by physical therapists andoccupational therapists with onlybrief instruction, and, using EMR,they accomplished data entry in lessthan a minute as part of routine doc-umentation of the patient encounter.Using EMR, in which scores can beautomatically and quickly calculatedfor the practitioner to view immedi-ately, enhances the feasibility of stan-dardized assessment of activity limi-tations and is more user-friendly thanpaper forms that require practitio-ners to carry out score calculations.Because therapists’ judgments canbe used to assess patients’ functionalcapabilities using “6-Clicks” forms,
patients are not required to performa specific task. This approach limitsmissing values and reduces theambiguity of total scores when itemscores for “not tested” are included,as in some other instruments.12,14
Using calibrated items drawn fromthe AM-PAC item pool, “6-Clicks”forms yield standardized scores in ametric common to all versions ofthe AM-PAC. The common scoringallows for direct comparison withAM-PAC assessments done over timeand across different care settings.Inclusion of only 6 items from theoverall AM-PAC, each with a simple,4-level scoring system, also facilitatesapplication of “6-Clicks.” Existingtools may have many items10 orlevels of scoring for eachitem,9,11,14,15,25 making it challengingfor clinicians to make such fine dis-tinctions in activity limitations inthe acute care setting. Additionally,application may be slow and inter-pretation difficult in tools thatinclude different scoring structuresfor different items.9,16
Internal consistency reliability forboth basic mobility and daily activi-ties forms was very high. Validity ofboth forms was supported by evi-dence for ceiling and floor effectsbelow 20% at first and last visits.Validity also was supported by differ-ences in scores across groups ofpatients who would be expected todiffer in levels of ability based onage, living situation, and number oftherapy visits provided to them.Large correlations24 of scores onboth forms at the last acute care visitwith admission FIM scores forpatients discharged to IRFs withinthe Cleveland Clinic hospital systemfurther support validity. Given thefact that the mobility subscore of theFIM does not include lower-levelactivities such as rolling in bed orcoming to a sitting position, as doesthe “6-Clicks” basic mobility form, agreater degree of correlation might
Table 1.Continued
Characteristic Measurement
No. of visits, median (interquartile range)
Physical therapist (n�57,943) 1 (1–2)
Occupational therapist (n�56,645) 1 (1–2)
Discharge destination, n (%) (n�53,393)
Home with services 21,460 (40.2)
Assisted living or independent senior living 315 (0.6)
Acute or subacute rehabilitation 27,924 (52.3)
Long-term or extended care 3,694 (6.9)
Basic mobility scale score, X (SD) (n�14,323)b
Admission 40.4 (7.3)
Discharge 43.7 (8.9)
Daily activity scale score, X (SD) (n�6,122)b
Admission 35.8 (5.6)
Discharge 38.9 (7.2)
a GI/GU�gastrointestinal/genitourinary, IRF�inpatient rehabilitation facility, SNF�skilled nursingfacility. Number of patients varies due to missing data.b Includes only patients with scores at both initial and final visits.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
384 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

not be expected. On the other hand,the items comprising the ADL sub-score of the FIM represent identicalactivities to the “6-Clicks” daily activ-ity form; therefore, a greater degreeof correlation might have beenexpected.
Internal responsiveness of the“6-Clicks” scores also was supportedby very large SRMs.24,26 The SRMswere higher than those found usingthe full AM-PAC measure withcomputerized adaptive testing forpatients with orthopedic problemsover a course of outpatient physicaltherapy27 and similar to the SRMsover a period of 12 months forpatients with a variety of conditionsdischarged from IRFs.28 The MDCsin our study were slightly higherthan those reported for patients withorthopedic problems seen in outpa-tient settings due to higher standarddeviation of basic mobility scores atbaseline and lower internal consis-tency of daily activity scores in ourstudy than in the previous study.27
Given the need for maximizing effi-ciency and productivity of rehabilita-tion professionals in the fast-pacedsetting of acute care, other studieshave proposed models for triagingpatients.6,7 Although these modelssuggest that decisions about needfor services rely on more thanpatients’ functional abilities, ourfindings demonstrate that initial visit“6-Clicks” scores have the potentialto be useful in predicting patients’requirement for more than one visitby a physical therapist or occupa-tional therapist.
The ROC curves and the dataincluded in Figure 2 illustrate theutility of “6-Clicks” scores for makingclinical decisions about patients’need for more than one physicaltherapist or occupational therapistvisit in the acute care setting. Thegreater the area under the curve andthe greater the distance from the ref-
erence line, the better the test is atclassifying patients. Using Table 3,which includes data derived fromthe ROC curves, one can determinethat 63% of patients with a scorebelow a basic mobility cutoff scoreof 43.7 would be correctly identifiedas needing more than one visit and73% of patients with a score above
43.7 would be correctly classified asnot needing more than one visit.Generally, the goal in determiningcutoff scores is to maximize correctdecisions. In making decisions, how-ever, one has to determine the con-sequences of inaccuracy and selectcutoff scores accordingly. Using theabove example, therapists would
Figure 2.Receiver operating characteristic (ROC) curves for “6-Clicks” scores in determiningmore than one physical therapist or occupational therapist visit.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 385Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

need to determine whether the con-sequences (eg, higher cost and inef-ficiency) of providing more than onevisit to those who might not needthem would have worse conse-quences than providing only onevisit to those who might requiremore (eg, lost opportunity to addresspatients’ activity limitations). At thesame time, the consequences mightbe weighed differently by therapistsdepending on what a patient’s dis-charge disposition might be. Forexample, for patients going to a reha-bilitation setting where limitations inmobility and daily activity will beaddressed, a lower cutoff scoremight be acceptable.
Our findings also suggest that“6-Clicks” scores might be used toaudit service efficiency. For exam-ple, finding that some patients havemore than one visit despite demon-strating no limitations based on“6-Clicks” scores could lead to fur-
ther examination of whether addi-tional visits were, indeed, necessaryor whether those patients requiredfurther skilled intervention. It maybe that issues other than patients’activity limitations, such as patients’or families’ needs for education con-cerning safety, self-care, or homemodifications, drive additional visits.The “6-Clicks” forms do not assesscognitive or communication func-tions, and these functions couldaffect physical therapists’ and occu-pational therapists’ decisions aboutthe number of visits required. It isalso possible that strength, range ofmotion, or endurance may not beadequate despite high “6-Clicks”scores, leading to additional visits toaddress those impairments. A recentstudy of patients receiving physicaltherapy in the intensive care unitshowed improvements in activitylimitations but not in strength forthose who received services com-pared with those who did not.11
Physical therapists and occupationaltherapists also could provide addi-tional visits with the goal of patients’achieving higher levels of mobilityand daily activities than determinedby “6-Clicks” (eg, walking longer dis-tances than that required in the hos-pital room). Another possible reasonfor additional treatment sessions inpatients with high levels of capabil-ity could be nurses’ perceived barri-ers in allowing patients independentmobility, leading to their requests foradditional therapy visits.29,30
We also found that a fairly high pro-portion of patients seen by physicaltherapists and occupational thera-pists had no limitations in basicmobility or daily activity based on“6-Clicks” scores. This finding sug-gests that some patients may havebeen referred who did not requireskilled services. This phenomenonwould not be inconsistent with theexperience of therapists in other
Table 2.Evidence for Construct Validitya
Variable
BasicMobility
Scale Score
95% ConfidenceInterval Basic
MobilityRaw ScoreEquivalent
DailyActivity
Scale Score
95% ConfidenceInterval Daily
ActivityRaw ScoreEquivalent
LowerBound
UpperBound
LowerBound
UpperBound
First visit scores by number of visitsb n�57,938 n�56,644
1 visit only 47.2 47.1 47.3 18.5 40.3 40.2 40.4 18.0
More than 1 visit 40.2 40.1 40.4 15.3 36.1 36.0 36.1 16.0
First visit scores by age (y)b n�57,938 n�56,644
18–40 49.5 49.2 49.9 19.6 41.8 41.5 42.2 18.8
41–64 47.3 47.1 47.4 18.6 40.2 40.1 40.3 18.1
65–85 44.4 44.3 44.5 17.2 38.0 37.9 38.1 16.9
�85 41.8 41.6 42.0 15.9 35.8 35.7 36.0 15.7
First visit scores by living situationprior to admissionc
n�51,835 n�50,343
Home alone 46.1 46.0 46.3 18.1 39.2 39.1 39.4 17.6
Home with other(s) 46.1 46.0 46.2 18.1 39.2 39.1 39.3 17.6
Assisted or independent senior living 42.4 42.0 42.7 16.3 36.5 36.2 36.7 16.1
IRF/SNF 35.8 35.4 36.2 12.6 32.5 32.2 32.9 13.8
Long-term care 34.8 34.4 35.2 12.0 30.1 29.7 30.4 12.4
a IRF�inpatient rehabilitation facility, SNF�skilled nursing facility. Number of patients varies due to missing data.b All values significantly different from other values in category at .05 level.c Home alone not significantly different from home with other(s); all other values significantly different at .05 level.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
386 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

acute care settings.31 Managerscould use information from“6-Clicks” scores to gain understand-ing of the referral practices in partic-ular clinical units or the practice ofparticular therapists to determinebest approaches to providing high-quality, efficient care. In combina-tion with efficiency audits using“6-Clicks” scores, educational effortscould be directed toward nursing orphysician house staff about criteriafor referral. Additionally, trials couldbe done using different “6-Clicks”cutoff scores for deciding whetherpatients receive more than one visitand then examining their outcomes.
It is not clear why measures of func-tional activity previously developedfor use in the acute care setting havenot been adopted; however, in orderto be useful to clinicians, measure-ment tools must be relevant to theirpatients’ conditions, provide infor-mation that will help them with theirdecision making, and be quick touse and easy to interpret.17 Reasonscited for developing new instru-ments for use in the acute care set-ting have included perceptions thatexisting instruments did not includerelevant items9,12,13,15; had compli-cated instructions, scoring, or admin-istration8,10,14; were not able to mea-sure patients’ improvement9,10,14;and were too lengthy.10 Althoughreports of the application of varioustools have suggested that they mightaddress some of these concerns,their usefulness in doing so hasnot been consistently documented.Our findings suggest that “6-Clicks”forms meet many of these criteria,particularly relevance and ease ofuse.
LimitationsThe limitations of this study includethe fact that data were collected bya large number of clinicians andwe did not assess rater reliability.Another limitation is use of a clinicaldatabase to provide data for analyses.
The limitations in using clinical data-bases for research have been welldocumented.32 The database weused was developed to enhanceoperations and allow quality assess-ment, not for research purposes.
Clinical databases also are designedto be helpful to clinicians in docu-menting patients’ status. Therefore,they may not include the type of datanecessary to address research ques-tions, nor the form of data useful
Figure 3.Correlation of final acute care visit “6-Clicks” scores with Functional IndependenceMeasure (FIM) scores on admission to the inpatient rehabilitation facility.ADL�activities of daily living.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 387Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

for analysis. Clinical databases thatinclude narrative information, suchas the database used in this study,can provide rich descriptions thatmay be helpful for patient care. Suchinformation, however, may be diffi-cult to code accurately when using itfor research purposes and may leadto misclassifications and missing datapoints.
We had FIM data for a small propor-tion of patients due to the fact thatmany patients were discharged toIRFs that were not part of the Cleve-land Clinic hospital system; there-fore, the data were not in our data-base. This sample could be biased inways that we cannot determine.Other biases also might exist that aredifficult to identify. For example, wedo not know whether implementa-
tion of “6-Clicks” forms influencedtherapists’ decisions about numberof visits. Another limitation is thatthis study took place within only onehealth care system, and it is unclearhow the “6-Clicks” instrumentswould perform in other settings. Onthe other hand, the health care sys-tem in which this study was donecomprises several facilities withinwhich data were collected by a largenumber of clinicians.
Further StudyRater reliability of “6-Clicks” formshas not been examined. Assessingintratester reliability may be difficultgiven the rapid changes in functionalabilities that patients in acute caremay undergo in a short period oftime; however, interrater reliabilityshould be assessed. Determining
rater reliability may be particularlyimportant given that “6-Clicks”scores may be based solely onobserving patients’ performance ofeach item. Clinicians’ judgments ofpatients’ functional capabilities maybe more variable than their ability toscore actual performance. Studiesalso could be undertaken to examinefurther the usefulness of “6-Clicks”scores in determining discharge set-ting. Finally, further investigation todefine cutoff scores for making deci-sions about need for interventionand the appropriate extent of inter-vention should be undertaken. Wesuggest studies in which the effi-ciency and effectiveness of rehabili-tation services are assessed whennurses use “6-Clicks” forms to deter-mine whether to seek referral torehabilitation services. In a recent
Table 3.Sensitivity, Specificity, and Predictive Values for Various Basic Mobility and Daily Activity Scores
BasicMobilityScorea
Sensitivity Specificity
PositivePredictiveValueb,d
NegativePredictiveValuec,d
DailyActivityScorea
Sensitivity Specificity
PositivePredictiveValueb,d
NegativePredictiveValuec,dScale Raw Scale Raw
25.0 6.5 0.03 0.98 0.56 0.50 18.6 6.5 0.02 0.98 0.52 0.50
27.5 7.5 0.04 0.97 0.58 0.50 21.5 7.5 0.03 0.97 0.52 0.50
29.6 8.5 0.09 0.94 0.61 0.51 24.1 8.5 0.04 0.96 0.53 0.50
31.4 9.5 0.11 0.93 0.61 0.51 26.3 9.5 0.05 0.95 0.54 0.50
33.1 10.5 0.16 0.90 0.62 0.52 28.2 10.5 0.07 0.94 0.55 0.50
34.6 11.5 0.23 0.87 0.64 0.53 29.8 11.5 0.10 0.93 0.56 0.51
36.0 12.5 0.30 0.84 0.65 0.54 31.3 12.5 0.14 0.90 0.57 0.51
37.4 13.5 0.34 0.82 0.65 0.55 32.7 13.5 0.19 0.86 0.58 0.52
38.8 14.5 0.39 0.80 0.65 0.57 34.0 14.5 0.27 0.81 0.59 0.53
40.1 15.5 0.44 0.77 0.66 0.58 35.3 15.5 0.39 0.73 0.59 0.54
41.5 16.5 0.51 0.73 0.66 0.60 36.6 16.5 0.53 0.66 0.61 0.58
42.9 17.5 0.62 0.67 0.65 0.64 38.0 17.5 0.64 0.60 0.61 0.62
44.5 18.5 0.80 0.54 0.63 0.73 39.4 18.5 0.77 0.49 0.60 0.68
46.6 19.5 0.85 0.49 0.63 0.77 41.1 19.5 0.88 0.37 0.58 0.75
49.0 20.5 0.90 0.42 0.61 0.81 43.2 20.5 0.93 0.30 0.57 0.82
51.8 21.5 0.93 0.37 0.60 0.84 45.7 21.5 0.97 0.23 0.56 0.88
55.1 22.5 0.96 0.29 0.58 0.89 49.1 22.5 0.98 0.19 0.55 0.92
59.0 23.5 0.98 0.21 0.56 0.93 52.8 23.5 0.99 0.16 0.54 0.93
a Cutoff scores are the averages of 2 consecutive scores.b Proportion of patients with this score or lower who had more than 1 visit.c Proportion of patients with this score or higher who had only 1 visit.d Predictive values are calculated with a standardized prevalence of more than one visit equal to 50%.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
388 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

study by Drolet et al,33 an algorithmwas developed that allowed nursesto assess patients’ mobility and makedecisions about appropriate physicaltherapist and occupational therapistreferrals. Such an approach mayimprove the efficiency of rehabilita-tion services and decrease the costs,and we believe nurses’ educationand experience would allow themto assess patients’ performance on“6-Clicks” items.
ConclusionThe “6-Clicks” basic mobility anddaily activities forms are new toolsthat are based on the AM-PAC anddesigned for measuring patients’activity limitations in the acute caresetting. This study provides evidencefor the validity of the measures’scores and their potential ability toaddress some of the concerns aboutinstruments previously designed andproposed for this purpose.
All authors provided concept/idea/researchdesign. Dr D. Jette, Mr Ranganathan, DrFrost, and Dr A. Jette provided writing. DrStilphen, Mr Ranganathan, Dr Passek, andDr Frost provided data collection. Dr Stil-phen, Mr Ranganathan, and Dr Passek pro-vided data analysis. Dr Stilphen, Dr Passek,and Dr Frost provided project management.Dr Frost provided fund procurement andclerical support. Dr Stilphen and Dr Frostprovided study participants and facilities/equipment. Mr Ranganathan and Dr Frostprovided institutional liaisons. Dr Stilphen,Dr Passek, Dr Frost, and Dr A. Jette providedconsultation (including review of manuscriptbefore submission).
DOI: 10.2522/ptj.20130199
References1 Carpenter I, Bobby J, Kulinskaya E, Sey-
mour G. People admitted to hospital withphysical disability have increased lengthof stay: implications for diagnosis relatedgroup re-imbursement in England. AgeAgeing. 2007;36:73–78.
2 Muller M, Grill E, Stier-Jamer M, et al. Val-idation of the comprehensive ICF coresets for patients receiving rehabilitationinterventions in the acute care setting.J Rehabil Med. 2011;43:92–101.
3 Griffin S. Occupational therapy practice inacute care neurology and orthopaedics.J Allied Health. 2002;31:35–42.
4 Jette DU, Brown R, Collette N, et al. Phys-ical therapists’ management of patientsin the acute care setting: an observationalstudy. Phys Ther. 2009;89:1158–1181.
5 Young DL, Arata R, Enerson M, Johnson C.Rates and reasons for patient non-treatment in physical therapy in an acutecare hospital. HPA Resource. 2011;11:10–18.
6 Hobbs JA, Boysen JF, McGarry KA, et al.Development of a unique triage system foracute care physical therapy and occupa-tional therapy services: an administrativecase report. Phys Ther. 2010;90:1519–1529.
7 Foster CB, Gorga D, Padial C, et al. Thedevelopment and validation of a screeninginstrument to identify hospitalized medi-cal patients in need of early functionalrehabilitation. Qual Life Res. 2004;13:1099–1108.
8 JHH Functional Acute Care Score GuideBooklet. Baltimore, MD: Johns HopkinsHospital; 1996.
9 DiCicco J, Whalen D. University of Roch-ester Acute Care Evaluation: developmentof a new functional outcome measure forthe acute care setting. J Acute Care PhysTher. 2010;1:14–20.
10 Roach KE, Van Dillen LR. Development ofan acute care index of functional status forpatients with neurological impairment.Phys Ther. 1988;68:1102–1108.
11 Schweickert WD, Pohlman MC, PohlmanAS, et al. Early physical and occupationaltherapy in machanically ventilated, criti-cally ill patients: a randomized controlledtrial. Lancet. 2009;373:1874–1882.
12 Shields RK, Leo KC, Miller B, et al. Anacute care physical therapy clinical prac-tice database for outcomes research. PhysTher. 1994;74:463–470.
13 Skinner EH, Berney S, Warrillow S, DenehyL. Development of a physical function out-come measure (PFIT) and a pilot exercisetraining protocol for use in intensive care.Crit Care Resusc. 2009;11:110–115.
14 Swafford BB. Validity of Kansas UniversityHospital physical therapy acute care func-tional outcomes tool. Acute Care Perspec-tives. 2008;17:14–17.
15 Zanni JM, Korupolu R, Fann E, et al. Reha-bilitation therapy and outcomes in acuterespiratory failure: an observational pilotproject. J Crit Care. 2010;25:254–262.
16 Mahoney FI, Barthel DW. Functional eval-uation: the Barthel Index. Md State Med J.1965;14:61–65.
17 Jette DU, Halbert J, Iverson C, et al. Use ofstandardized outcome measures in physi-cal therapist practice: perceptions andapplications. Phys Ther. 2009;89:125–135.
18 Haley SM, Coster WJ, Andres PL, et al.Activity outcome measurement for post-acute care. Med Care. 2004;42:I-49–I-61.
19 Haley SM, Coster WJ, Andres PL, et al.Score comparability of short forms andcomputerized adaptive testing: simulationstudy with the activity measure for post-acute care. Arch Phys Med Rehabil. 2004;85:661–666.
20 Centers for Medicare & Medicaid Services.The Inpatient Rehabilitation FacilityPatient Assessment Instrument (IRF-PAI)training manual. 2012. Available at:https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/Downloads/IRFPAI-manual-2012.pdf. Accessed August 20, 2013.
21 International Classification of Function-ing, Disability and Health. Geneva, Swit-zerland: World Health Organization; 2001.
22 Siebens H, Andres PL, Ni P, et al. Measur-ing physical function in patients with com-plex medical and postsurgical conditions:a computer adaptive approach. Am J PhysMed Rehabil. 2005;84:741–748.
23 Husted JA, Cook RJ, Farewell VT, GladmanDD. Methods for assessing responsiveness:a critical review and recommendations.J Clin Epidemiol. 2000;53:459–468.
24 Hopkins WG. A new view of statistics:effect magnitudes. 2002. Available at:http://www.sportsci.org/resource/stats/effectmag.html. Accessed September 5,2013.
25 Chiang L, Wang L, Wu C, et al. Effects ofphysical training on functional status inpatients with prolonged mechanical ven-tilation. Phys Ther. 2006;86:1271–1281.
26 Middel B, van Sonderen E. Statistical sig-nificant change versus relevant or impor-tant change in (quasi) experimentaldesign: some conceptual and methodolog-ical problems in estimating magnitude ofintervention-related change in health ser-vices research. Int J Integr Care. 2002;2:1–8. Available at: http://www.ijic.org/index.php/ijic/article/view/URN%3ANBN%3ANL%3AUI%3A10-1-100307. AccessedSeptember 5, 2013.
27 Jette AM, Haley SM, Tao W, et al. Prospec-tive evaluation of the AM-PAC CAT in out-patient rehabilitation settings. Phys Ther.2007;87:385–398.
28 Coster WJ, Haley SM, Jette AM. Measuringpatient-reported outcomes after dischargefrom inpatient rehabilitation settings.J Rehabil Med. 2006;38:237–242.
29 Brown CJ, Williams BR, Woodby LL, et al.Barriers to mobility during hospitalizationfrom the perspectives of older patientsand their nurses and physicians. J HospMed. 2007;2:305–313.
30 Doherty-King B, Bowers B. How nursesdecide to ambulate hospitalized olderadults: development of a conceptual mod-el. Gerontologist. 2011;51:786–797.
31 Masley PM, Havrilko C-L, MahnensmithMR, et al. Physical therapist practice in theacute care setting: a qualitative study. PhysTher. 2011;91:906–922; invited commen-tary 919–921; author response 921–922.
32 Pryor DB, Lee KL. Methods for the analysisand assessment of clinical databases: theclinician’s perspective. Stat Med. 1991;10:617–628.
33 Drolet A, DeJuilio P, Harkless S, et al.Move to Improve: the feasibility of usingan early mobility protocol to increaseambulation in the intensive and interme-diate care settings. Phys Ther. 2013;93:197–207.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 389Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

Appendix 1.“6-Clicks” Inpatient Basic Mobility Short Forma
Please check the box that reflects your (the patient’s) best answer to each question. Unable A Lot A Little None
How much difficulty does the patient currently have . . . .
1. Turning over in bed (including adjusting bedclothes, sheets, and blankets)? ▫1 ▫2 ▫3 ▫4
2. Sitting down on and standing up from a chair with arms (eg, wheelchair, bedside commode)? ▫1 ▫2 ▫3 ▫4
3. Moving from lying on back to sitting on the side of the bed? ▫1 ▫2 ▫3 ▫4
How much help from another person does the patient currently need . . .
4. Moving to and from a bed to a chair (including a wheelchair)? ▫1 ▫2 ▫3 ▫4
5. To walk in hospital room? ▫1 ▫2 ▫3 ▫4
6. Climbing 3–5 steps with a railing? ▫1 ▫2 ▫3 ▫4
Clinicians may find the following helpful in selecting responses:1. Total/Unable�Total/Dependent Assist2. A Lot�Maximum/Moderate Assist3. A Little�Minimum/Contact Guard Assist/Supervision4. None�Modified Independence/Independent
“6-Clicks” Inpatient Basic Mobility Short Form Scoring
Raw Score Scale ScoreScale Score
Standard ErrorApproximate Degree ofFunctional Impairment
6 23.55 4.57 100%
7 26.42 4.33 92%
8 28.58 4.04 87%
9 30.55 3.69 81%
10 32.29 3.42 77%
11 33.86 3.22 73%
12 35.33 3.08 69%
13 36.74 2.99 65%
14 38.10 2.95 61%
15 39.45 2.93 58%
16 40.78 2.95 54%
17 42.13 3.03 51%
18 43.63 3.20 47%
19 45.44 3.55 42%
20 47.67 4.06 36%
21 50.25 4.69 29%
22 53.28 5.43 21%
23 56.93 6.22 11%
24 61.14 6.94 0%
a The AM-PAC “6-Clicks” forms are copyright protected by The Trustees of Boston University.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
390 f Physical Therapy Volume 94 Number 3 March 2014Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017

Appendix 2.“6-Clicks” Inpatient Daily Activity Short Form
Please check the box that reflects your (the patient’s) best answer to each question. Unable A Lot A Little None
How much help from another person does the patient currently need . . .
1. Putting on and taking off regular lower body clothing? ▫1 ▫2 ▫3 ▫4
2. Bathing (including washing, rinsing, drying)? ▫1 ▫2 ▫3 ▫4
3. Toileting, which includes using toilet, bedpan, or urinal? ▫1 ▫2 ▫3 ▫4
4. Putting on and taking off regular upper body clothing? ▫1 ▫2 ▫3 ▫4
5. Taking care of personal grooming such as brushing teeth? ▫1 ▫2 ▫3 ▫4
6. Eating meals? ▫1 ▫2 ▫3 ▫4
Clinicians may find the following helpful in selecting responses:1. Unable�Total/Dependent Assist2. A Lot�Maximum/Moderate Assist3. A Little�Minimum/Contact Guard Assist/Supervision4. None�Modified Independence/Independent
“6-Clicks” Inpatient Daily Activity Short Form Scoring
Raw Score Scale ScoreScale Score
Standard ErrorApproximate Degree ofFunctional Impairment
6 17.07 3.74 100%
7 20.13 3.68 92%
8 22.86 3.43 86%
9 25.33 3.17 80%
10 27.31 2.96 75%
11 29.04 2.79 70%
12 30.60 2.68 67%
13 32.03 2.62 63%
14 33.39 2.61 60%
15 34.69 2.65 56%
16 35.96 2.71 53%
17 37.26 2.82 50%
18 38.66 2.97 47%
19 40.22 3.20 43%
20 42.03 3.55 38%
21 44.27 4.08 33%
22 47.10 4.81 26%
23 51.12 5.88 16%
24 57.54 7.36 0%
a The AM-PAC “6-Clicks” forms are copyright protected by The Trustees of Boston University.
AM-PAC “6-Clicks” Inpatient Daily Activity and Basic Mobility Short Forms
March 2014 Volume 94 Number 3 Physical Therapy f 391Downloaded from https://academic.oup.com/ptj/article-abstract/94/3/379/2735547/Validity-of-the-AM-PAC-6-Clicks-Inpatient-Dailyby gueston 21 September 2017