-
8/2/2019 Validity Oral
1/9
206 Journalof Public Health Dentistry
Validity of Two Methods for Assessing Oral Health Statusof
PopulationsEugenio D. Beltran, DMD, MPH, MS, DrPH; Dolores M.
Malvitz, RDH, MPH, DrPH;Stephen A. Eklund, DDS, MHSA, DrPH
_ _ - _ _ ~ -bstractObjective: This investigation assessed two
methods for estimatingepidemiologic indicators of oral health
status among children: (1 ) a visual-onlyscreening,performed
independently by a dental hygienist and a registered nurse;and (2)
a parent- or guardian-completed questionnaire. The indicators
includeddichotomous variables measuring dental caries and treatment
needs, presenceof sealants, njuries to the anterior teeth, and
dental fluorosis.Methods:Followingtraining and calibration, data
were collected over an eight-day period in April 1994among 632
elementary schoolchildren (aged5 to 1Pyears) n Monticello,
Georgia.Both screening and questionnaire findings were compared
pairwise with resultsfrom visual-tactile examinations done by a
dentist. Validity, represented bysensitivity, specificity, and
predictive values, was assessed for screening resultsfrom the
dental hygienist, the nurse, and the parent-completed
questionnaire.Results: Validity was high for screening for caries
and treatment needs (>go%for sensitivity, specificity, and
predictive values in a sample having 30% to 40%prevalence). Less
valid data -mainly an effect of false negatives- ereobtained for
fluorosis, njuries, and presence of sealants. No significant
differencein validity was observed between the nurse and the dental
hygienist. One-third ofrespondents to the questionnaire did not
know if their children needed fillings (aproxy for untreated decay)
or had received sealants; only knowledge of restora-tions was
comparable to results from screening. lntraexaminer reliability for
thetwo screeners ranged from 85 to 100 for percent agreement and
0.70 to 0.93 forkappa scores. Conclusions: Screening by dental
hygienists or nurses canprovide valid data for surveillance of
dental caries and treatment needs. Trainingfor visual assessment of
fluorosis and injuries must be improved to diminish theproportion
of false negatives. A parent-completed questionnaire is less
effectivethan visual screening for evaluating oral health status in
children. [J Public HealthDent 1997;57(4):206-2141
~ ~
Key Words: validity, reliability, visual-tactile examination,
screenings, question-naire, oral health assessment,
surveillance.
Surveillance in public health is de-fined as the ongoing
systematic collec-tion, analysis, and interpretation
ofoutcome-specific data for use in theplanning, implementation, and
evalu-ation of public health practice (1).Sev-eral approaches and
sources of dataare used in public health surveillance:vital
statistics, notifiable disease data,registries, sample surveys,
adminis-trative data, and sentinel surveillancedata (2) .An
important element of any
surveillance system is the use of thedata to advance public
health.No true surveillance systems fororal conditions exist. The
prevalenceand trends of oral diseases have beenmonitored through
oral health sur-veys at the national and sometimesstate and local
levels. These surveyshave used some sort of clinical exami-nation
and questionnaire. A dentalprofessional generally performs a
vis-ual-tactile assessment of the mouth in
a sample of the population. Many ofthese surveys have used the
Radikediagnostic criteria and examinationprotocol (3),
modifications of theRadike criteria such as those by theNational
Institute of Dental Research(4),or those of the World Health
Or-ganization (5).Some differences exist between thediagnostic
criteria used in these sur-veys and those used by clinicians
intheir practices. In clinical examina-tions practitioners make
complexmeasurements, stressing the precisionof the process, i.e.,
the detection of themost incipient signs of disease. Thegreater the
complexity, however, thegreater the likelihood of unreliable
re-sults. Research shows that cliniciansapply different criteria
(6,7)and differsignificantly in their diagnoses andtreatmentplans
(8-11).Oral health sur-veys have emphasized the reliabilityof
measurements. Experience sug-gests that visual-tactile
examinationscan be used to estimate the oral healthsta tus of
populations, provided the as-sessment is performed in
well-definedsamples by trained examiners whousevalid indices with
known reliability. Inoral epidemiology these surveys areconsidered
the standard, even thoughsome underdiagnosis is expected dueto the
lack of procedures and tech-niques that are feasibleor practical
forfield examinations (e.g., x-rays, opticaltransillumination).
Still, oral healthsurveys are complex and demand ex-tensive
resources, which might ex-plain why many programs lack dataon oral
health status (12).Screeningsare defined in the medi-cal model as
procedures that can sortout persons who may have a conditionfrom
those who may not (13). Thosewho appear to have the condition
are
- _ __ _ ~ - _ _ ____-__. - . -Send correspondence and reprint
requests to Dr. eltran, Divisio n of Oral Health, Centers for
Disease Control and Pre vention, NCC DPH P, 4770Buford Highway , MS
F-10, Chamblee, GA 30341. E-mail: edM@ cdc.gov.Dr. Malvitz is
chief, Surveillance, Investigations, a nd Kesearch Branch,Bv i s i
on of Oral H ealth, CDC. Dr. Eklund is associate professor, School
of Public Health, University of Michigan, AM Arbor. llus manusaipt
waspresented as a poster a t the annual meeting of the American
Association for Dental Research in San Francisco, April 1996. Man
uscript recvived:8/26/96; returned to authors for revision:
10/29/96; accepted for publication: 4/18/97.
-
8/2/2019 Validity Oral
2/9
Vol. 37, No.4, Fall 1997 207followed up to obtain a final
diagnosis(13).Because screenings are applied topopulations, their
methods must besimple, inexpensive, and require mini-mal training
for application and inter-pretation, e.g., the PPD tuberculin
test.Screenings must be evaluated againstsome standard procedure
for valid-ity-that is, their sensitivity, specific-ity, and
predictive value. In this evalu-ation, the proportion of false
positivesand false negatives are important topatient follow-up and
cost (14).Frankenburg (15) has provided thefollowing 10 criteria
for selecting dis-eases or conditions for screening pro-grams: ( I
) the condition has to be seri-ous or potentially so, (2) i t
should bepossible to differentiate those with thecondition from
those at borderline orwithout it, (3) the prognosis should
beimproved if the condition is detectedand treated early, (4) there
should beadequat e lead and screening time, (5)the condition should
be treatable orcontrollable, (6) the condition shouldbe prevalent,
(7) there should be noharm caused to the individual beingscreened,
(8) here should b e a follow-u p for those found positive, (9)
theprocedure should be cost effective,and (10) the program should
be ac-ceptable to the public.Screening protocols for oral canceror
precancerous lesions reported inthe literature (16-19) involve the
sys-tematic and consistent visual-tactileexamination of all
anatomical sites ofthe oral and pharyngeal cavity andneck (20). Few
oral conditions, otherthan oral cancer, have been the subjectof
screening programs and activities(21-23). For den tal caries,
screeningdenotes a fast and simple process bywhich an examiner
visually inspectsthe oral cavity to detect the presenceor absence
of specific oral conditions(24),as has been done in health
fairs(25). Based on Frankenburgs criteria,dental caries, dental
fluorosis, anddental injuries screening protocolscould be developed
as alternatives tovisual-tactile examinations.Few studies have
tested the visualand visual-tactile abilities of dentaland
nondental personnel other thandentists. Only in a few large-scale
sur-veys have dental hygienists been ex-aminers (26-30). These
studies re-ported interexaminer reliability tocompare the
examinations made byhygienists and dentists. None of thesestudies
evaluated validity. Two stud-
ies from the s ame research team(29,301 reported measures of
validity;however, these measures were on theability of their
research instrument (amultivariable statistical model) to pre-dict
future caries patterns. Basedmostly on reliability values,
thesestud ies concluded that dental hygien-ists could be used to
collect oral healthstatus data. A few studies (2531) havefocused on
the use of other person-nel-such as denta l auxiliaries,
dentalstuden ts, or teachers-for examina-tions or screenings;
however, none ofthese studies have assessed validity.Oral health
status and behaviorsalso have been assessed by question-naires, for
example those of the Na-t ional Health In terview Survey(NHIS) (32)
and the Behavioral RiskFactor Surveillance System (BRFSS)(33).
These data a re self-reported andsubject to error, particularly
selectionand information biases (34,35). Severalstudies have
compared data obtainedfrom clinical examinations with
thoseself-administered questionnaires (36-411 phone interviews
(421, and parent-responded questionnaires (43). De-spite the
different methodologies,populations, oral conditions assessed,and
the fact that many studies evalu-ated reliability instead of
validity, re-searchers concluded that question-naires appear to be
useful tools forobtaining oral health data.
The objective of this investigationwas to test the validity of
visualscreening (protocol 1) and parent- orguardian-completed
questionnaire(protocol 2) for assessing the oralhealth sta tus of
schoolchildren, withthe goal of using these protocols astools in a
surveillance system for oralconditions. The visual-tactile
exami-nation was used as the standard pro-tocol.Methods
Children in kindergarten throughfifth grade (N=838;ged 5 to 12
years)in a rural school in Monticello, Geor-gia, were invited to
participate in thisinvestigation. This school had askedthe Georgia
Department of HumanResources to evaluate the childrensdental
status. One week before exami-nation, children were given a
packagethat included a letter of invitation, aconsent form, and a
multiple-choicequestionnaire for their parents. Allchildren who
returned questionnairespart icipated in the examination
(n=632; 75% response rate). Followingexamination, a form with
recommen-dations regarding the childs need fordental treatment was
sent to the par-ents.All clinical procedures followedguidelines for
infection control in den-tal settings (44,45). A protocol for
in-jury exposure control consistent withCDC guidelines and the
OccupationalSafety and Health Administrationstandards was followed.
Institutionalreview board approval was obtainedfrom both CDC and
the University ofMichigan.
Measurement Protocols. Th estandard examination protocol was
avisual-tactile examination of all toothsurfaces in each child. All
childrenwere examined by a dentist who hadbeen calibrated using
NIDR diagnos-tic criteria for dental caries and pres-ence of
sealants (4), Deans index fordental fluorosis (41, and Bhats
criteriafo rdental injuries (46).A portable den-tal chair and
light, dental explorers,and plane-surface mirrors were used;no
radiographs were exposed. Fromthese examinations, each child
wasclassified into one of the followinggroups based on dental
caries in theirprimary and permanent teeth: (1)car-ies free; (2) at
least one tooth restored,but no untreated decay; or (3) at leastone
untreated carious lesion, whetherrestorations were present or not.
Inaddition, each child was classified ashaving (yes/no): (1) at
least one per-manent molar with pit and fissuresealants, (2) at
least one anterior toothwith injury or sequelae, and (3)
dentalfluorosis. Finally, each child was clas-sified into a
three-level variable ac-cording to urgency of treatmentneeded (no
need, nonurgent, and ur-gent). Need for urgent treatment wasdefined
a s having one or more teethwith extensive tissue
destruction,probably involving the pulp, or his-tory of pain or
signs of infection.Nonurgent needs included presenceof untreated
carious lesions or calcu-lus.Two measurement protocols weretested.
Protocol 1 was a visual-onlyscreening of the childsmouth done bya
dental hygienist or a registerednurse, each of whom screened
aboutone-half of each class in sequential or-der. The dental
hygienist had not per-formed oral assessments or providedtreatment
for more than five years.The nurse had no previous clinical
-
8/2/2019 Validity Oral
3/9
208 Journal of Public Health Dentistrydental experience. Both
screeners re-ceived written material on the proce-dures and
diagnostic criteria for eachcondition to be evaluated.The protocol
allowed the dental hy-gienist to perform oral screenings
afterreview of this material and withoutfurther training. A
five-hour trainingsession, which used both slides andpatients,
familiarized the nurse withdental nomenclature and clinical
fea-tures of each condition. The protocolrequired the screener to
inspect allfour quadrants of the mouth sequen-tially and to code
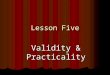
the results accordingto fivealgorithms. Figure 1depicts
thealgorithm used to code dental caries (afull set of these
algorithms is availableupon request). In the particular case
ofcoding for dental caries, some childrenwith restorations were
coded as 2because they also had untreated cari-ous lesions.
Screenings were carriedout using a portable chair, a flashlightfor
intraoral i l lumination, and atongue blade to facilitate visual
accessduring inspection. Visual screening al-ways preceded the
visual-tactile ex-amination for each child. Approxi-mately 5
percent of the children werereexamined by the dentist and the
twoscreeners to estimate intraexaminerreliability. Most replicate
assessmentswere performed 2C-25 minutes after
the initial dental screenings and 45-60minutes after the initial
visual-tactileexaminations.Protocol 2 was a 17-item,
multiple-choice questionnaire completed by aparent or guardian when
permissionto participate wa s granted. The q u e s
tionnaire asked about conditions pre-sent in the childs mouth,
demo-graphic characteristics, and family so-cioeconomic status.
Questions aboutdental fluorosis and need for dentaltreatment were
not included; dontknow options were available. The
FIGURE 1Visual Screening Algorithm for Coding Dental Caries
Do a cycle through the four quadrants, then answer:IEeIs here
any dk ay ed ooth?]--+ N OatDo another cycle and answer:t
I 1IThen code caries [2] I Then code caries [l] LThen code
caries [O]TABLE 1
Validity of Visual Screening Versus Visual-tactile Examination
in Evaluating Presence of Selected Oral Conditions,Both Screeners
Combined
Condition N* Sensitivity (%)Caries3Restorations present
Untreated decayCaries experiences
FluorosisInjuriesSealantsTreatment7Nonurgent
UrgentAny treatmentneeded
421434632632632632554482632
94.093.694.378.680.059.173.398.483.4
Predictive Value (%)Specificity(%) Positive Negative
99.6 99.4 %.296.9 95.3 95.896.6 97.5 92.395.9 90.9 89.798.2 85.7
97.399.7 92.9 97.095.7 81.7 93.199.8 98.4 99.795.4 89.0 92.9
Prevalence (%)t
39.739.958.534.011.97.020.912.930.5
Total samplesize available (includingthe reference group) o
assess validity for each condition.+A s determmed by the
msual-tactile examination.6Caries experiencewas detined a s having
treated or unaeated cariouslesions. N o need for treatment was used
as the reference.Caries free was used as the reference.
-
8/2/2019 Validity Oral
4/9
Vol. 57, No.4, Fall 1997 209TABLE 2
Validity of Visual Screening by Dental Hygienist Versus
Visual-tactile Examination in Evaluating Presenceof SelectedOral
ConditionsPredictive Value (% )
ConditionCaries$
_ _
Restorations presentUntreated decayCaries experiences
Fluorosis1n juriesSeaIan tsTreatmen 91Nonurgen
UrgentA ny treatmentneeded
w~
188215309309309309266221309
Sensitivity(%)
98.094.893.788.280.659.179.497.186.7
Specificity (%)-~~.100.0
94.194.195.598.999.791.699.591.2
Positive
100.092.996.288.290.692.974.697.183.5
Negative_ _94.195.790.395.597.597.093.599.593.0
Prevalence(70)t~
40.444.761.527.511.77.1
23.715.434.0
Total sample size available (including the reference group) to
assess validity for each condition.tA s determined by the
visual-tactile examination.fCaries experience was defined a s
having treated or untreated carious lesions. N o need for treatment
was used a s t h e reference.
Caries free was used as th e reference.
questionnaire was reviewed andtested by persons with expertise
inquestionnaire development and by aconvenience sample of paren ts
andschool eachers.Data Management and StatisticalMethods. Data were
entered directlyinto computer files using customizeddata entry
programs in the Epi Infosoftware (47). Following dat a cleaningand
editing, epidemiologic indicatorswere calculated using SAS
software.Later, the screening and the question-naire data sets were
matched withdata from the standard protocol usingall eligible
records to maximize sam-ple size. Pairwise matching of thescreening
data with the standard pro-tocol produced 3x3 contingency tablesfo
r dental caries and treatment ur-gency and 2x 2 tables for all
other con-ditions. Pairwise matching of ques-tionnaire data with
the standard pro-tocol produced 2x2 tables. To assessthe validity
of each alternative proto-col in each condition, a 2x2 table
wasprepared; for dental caries and treat-ment urgency in the
screening proto-col, only the appropria te cells from the3x3 table
were included.All measures of validity- ensitiv-ity, specificity,
positive predictivevalue, and negative predictive value-and the
prevalence of the condition inthe sample were calculated using
standard procedures (48). When ap-propriate, standard errors and
confi-dence intervals were estimated usingbinomial approximation.
Data werestratified to control for sociode-mographic variables.
Data from dupl i-cate examinations and screeningswere used to check
for intraexaminerreliability tested by percent agreementand kappa
statistics (49).Results .Validity of Visual Screenings andType of
Screener.Summaries of valid-ity results for screening are
includedin Tables 1-3. In each table two addi-tional comparisons
grouped thosewith a ny caries experience (treatedoruntre ated ) and
those needing anytreatment. Tables 1 4 isplay the totalnumber of
subjects (N) used in the sta-tistical procedures to assess
validityfor each condition, including those inthe reference gro up
(those not havingthe condition).
Specificity for both screeners com-bined (Table 1) was greater
than 95percent across all oral conditions; the95 percent confidence
intervals variedfrom 94 to 100 percent (data not dis-played). The
sensitivity for caries wasaround 94 percent (95%CI=91%,96%).The
lowest sensitivity was found inscreening for sealants (59%;
95%CI=55%, 63%), followed by nonurgent
treatment needed (73%), fluorosis(79%), and injuries (80%).A
positivepredictive value of 89 percent orhigher was found for most
oral condi-tions; exceptions were nonurgenttreatment needed (82%)
and injuries(86%). Negative predictive valueswere 90 percent or
higher across allconditions, and many values wereover 95
percent.The dental hygienist (Table 2 )screened 309 children with
moreprevalent untreated decay than in the323children screened by
thenurse; thesample screened by the nurse had ahigher prevalence of
fluorosis (Table3). Results obtained by the dental hy-gienist and
nurse were comparable tothose obtained by the dentist (confi-dence
intervals overlapped); never-theless, some minor differences
werefound. For example, the dental hy-gienist performed slightly
better thanthe nurse in assessing fluorosis anddetermining the need
for nonurgentand any treatment (Tables 2 and 3).These differences
could be explained,in part, by the differences in preva-lence in
some of these conditions. Theoverall lower sensitivity for
nonurgenttreatment needs may be a conse-quence of the lower
prevalence ofthese conditions in children screenedby the nurse. The
lack of a tactile com-ponent in the assessments made by
-
8/2/2019 Validity Oral
5/9
210 Journal of Public Health DentistryTABLE3
Validity of Visual Screening by Nurse Versus Visual-tactile
Examinationin Evaluating Presence of Selected OralConditions
ConditionCaries$~- ~~ ~ -Restorations presentUntreated
decayCaries experiences
FluorosisInjuriesSealan tsTreatment
NonurgentUrgentA n y treatmentneeded
w_ _233219323323323323288261323
Sensitivity (% ) Specificity(9%)~ ~ -~ -~ -
96.7 99.392.2 99.395.0 98.672.3 96.479.5 97.559.1 99.766.0
99.2
100.0 100.079.6 99.2
Predictive Value (5%)Positive-~ ~-
98.998.698.893.181.692.994.6
100.097.2
Negative__ -97.995.994.083.897.297.192.8
100.092.8
39.135.255.740.312.16.8
18.410.727.2
Total samplesize available (including the reference group) to
assess validity for each condition.t As determined by th e
visual-tactile examin ation.iCaries experiencewas defined as having
treated or untreated carious lesions. N o need for treatment was
used as the reference.Caries free was used as the reference.
TABLE4Validity of ParenVGuardian-completed Questionnaire Versus
Visual-tactile Examination in Evaluating Presence
of Selected Oral ConditionsPredictive Value ( 7 0 )Excluded n
Sensitivity Specificity Prevalence
N ( 7 c ) (?GI (5%) Positive Negative (70)_ _ _ _ _ ~ _ _ ~ ~ _
_ _ _ ~ _ _ _ _~~ ~~~ . ___ ~~~N o caries vs restorations 401 60
(10) 93.3 89.1 84.5 95.1 40.7N o caries vs untreated 305 214 (34)
68.8 88.3 80.4 80.3 40.9Injuries 611 17 (3) 20.0 87.3 16.9 89.4
11.5Sealants 423 205 (33) 56.7 89.3 28.8 93.4 7.1
prescntdecay
As determined by visual-tactileexamination
both screeners may be the cause of thelower sensitivity for
sealants.
Validity of Questionnaires. Aboutone-third of respondents did
notknow or did not indicate whether theirchildren had received
sealants orneeded restorative treatment. A lowerproportion (10%)did
not know if theirchildren had restored teeth. To
avoidclassification bias, these observationswere not included in
the assessment ofthe questionnaires validity (Table 4).The best
results were obtained inevaluating the presence of
restorations(93%sensitivity and95%negative pre-dictive value).
Although these values
were similar to those obtained byscreening (Table 11,
specificity andpositive predictive value were lowerin the
questionnaire (89% and 85%,respectively) than in the
screening.Measures of validity were lower forthe other three
conditions (untreateddecay, injuries, and presence of seal-ants),
as well.To evaluate any potential differ-ences among respondents
ability tocorrectly assess the presence of resto-rations, responses
were stratified byfamily income (2$30,000/year vsother),
eligibility for free or reduced-price lunch, number of children in
the
family (23vs other), and respondentslevel of education (>high
school vsother). Respondents with greater fam-il y income or having
children not eli-gible for free or reduced-price lunchassessed
presence of restorations intheir children with higher
sensitivity(data not shown).
Reliability of Measurements. Per-cent agreement and kappa
estimatesfor each condition were calculatedseparately for the
dentist, the dentalhygienist, and the nurse (Table5).Thedentist
evaluated caries status andpresence of sealants on each surface
byusing 14 mutually exclusive diagnos-
-
8/2/2019 Validity Oral
6/9
Vol. 57 , No.4, Fall 1997 211TABLE 5Intraexaminer Reliability
for Examiner and Screeners
Caries+ Sealantst Treatment Urgency$ Fluorosis ~njuriesy% Agree.
Kappa % Agree. Kappa ?& Agree. Kappa YoAgree. Kappa YOAgree.
Kappa
Dentist 99 0.97 100 1 o 98 0.92 99 0.92Hygienist 85 0.77 100
1.00 89 0.77 96 0.92 96 0.70Nurse 96 0.93 100 1 oo 100 1 .o 91 0.81
96 0.83The dentist evaluated canes status on each surface by using
14 mutually exclusive diagnostic categories; both sue ene rs
evaluated caries in theentire mouth by using three possible
diagnostic categories.tThe dentist evaluated presence of sealants
as part of the magnosis of canes.iBased on two diagnostic
categories.YThe denhst evaluated injuries by using four
&agnostic categories for each of the upper front teeth; both
screene rs evaluated injuries in the upperanterior teeth by using
two &agnostic categories
Based on three &agnostic categories.
tic categories; therefore, presence ofsealants was not analyzed
a s an inde-pendent item for the dentist. The den -tists
reliability was evaluated over 14diagnostic categories for caries
andpresence of sealants, seven for pres-ence of injuries (46),
three for treat-ment urgency, and two for dentalfluorosis. Both the
dental hygienistand nurse were evaluated using three-level
variables for caries and treatmenturgency and two-level variables
forpresence of sealants, dental fluorosis,and dental injuries. All
examinersshowed high reliability: agreementswere greater than 85%,
and kappa sta-tistics were greater than 0.70, a sub-stantial and
almost perfect score ac-cording to the scale proposed by Lan-dis
and Koch (50).Discussion
Validity of Visual Screening andType of Screener. Visual
screeningscan produce data highly comparableto those obtained from
visual-tactileexaminations. The highest validitywas found in the
screening for canesand urgent treatment (Table 1) in asample for
which the prevalence ofdental caries was comparable to theentire
population of Georgia (51)andthe United States (4). The protocol
forscreening did not discriminate be-tween dental caries of the
primary andpermanent dentitions because its ob-jective was to
obtain epidemiologic in-formation on the overall caries experi-ence
of the subject. If necessary, theprotocol could be modified to
measureeach dentition separately.With the exception of negative
pre-dictive values for caries experience,predictive values were
greater than 95
percent, which indicates that if the vis-ual screening protocol
were applied toa sample having a similar caries preva-lence, at
least 95 ou t of every 100posi-tive and negative cases would be
truepositives and true negatives. These re-sults suggest that the
visual screeningprotocol could provide valid epide-miologic
information for dental cariesand restorations.The lower validity of
screening fortreatment needs in this investigationmay indicate
uncertainty in translat-ing the diagnosis of untreated decayinto
the category of nonurgent treat-ment. A solution would be the use
ofa computer algorithm incorporatedinto the data entry program
thatwould automatically assign a code fortreatment urgency by
taking into ac-count the information entered for car-ies and
responses to yes or no ques-tions about other oral health
variables.
Lower validity also was found forother oral conditions
(fluorosis, inju-ries, and presence of sealants). Injuriesand
presence of sealants were not asprevalent a s dental canes in the
sam-ple, which might explain some of theseresults. The low
sensitivity for pres-ence of sealants (59%)was probably aneffect of
the lack of tactile reference.Although fluorosis wasas prevalent
ascaries in the sample, a significantnumber of false negatives (46
out of215) were responsible for the lowersensitivity (79%)and
negative predic-tive value (90%).
Some researchers have suggestedthat validity could be enhanced
by im-proving the diagnostic criteria, re-training, and follow-up
of training(16,521. Diagnostic criteria and codingin this
investigation were designed to
be simple to understand and apply.The validity of screening for
injuriesand fluorosis could be improved byincreasing the length and
quality oftraining and allowing exposure to awider variety of
clinical cases. How-ever, improved training may not affectthe
validity of screening for dentalsealants d ue to the lack of
tactile refer-ence.Few screening protocols for oralconditions have
been proposed andtested; only screening programs fororal mucosal
lesions have been testedfor validity (16,17,19).Some investiga-tors
used findings from these screen-ing protocols to estimate
epidemi-olo g~c arameters (53-55).Screeningprograms for other oral
conditions, es-pecially dental caries, have been im-plemented
without testing their valid-ity (25). Anecdotal information
sug-gests that screening protocols, such asthe one in the
Association of State andTerritorial Dental Directors seven-step
model (24), are being increas-ingly used, in part because of the
fi-nancial and logistic difficulties associ-ated with
visual-tactile examinations.The current investigation also fo-cused
on potential differences in thevalidity of measurements obtained
bya registered nurseand a dental hygien-ist. Except for sensitivity
for fluorosisand nonurgent treatment, the nurseprovided information
as valid as thatprovided by the dental hygienist. Inboth cases,
this finding could be ex-plained in part by differences in
preva-lence. The hygienists higher sensitiv-ity and lower
specificity values for un-treated decay (95% and 94%,respectively)
could be explained alsoby a higher prevalence in her sample
-
8/2/2019 Validity Oral
7/9
212 Journal of Public Health Dentistry
(45%). However, the hygienist had asubstantially larger
proportion of falsepositives, with a direct effect on herpositive
predictive value (93%).Possi-bly, t h e hygienist's previous
clinicaltraining, focused on evaluating incipi-ent signs of
disease, is responsible forthe large proportion of false
positives,a tendency that could have been ag-gravated by the
absence of a confirma-tory tactile reference.Few studies have
reported on thequality of the data collected by person-nel other
than dentists in performingvisual or visual-tactile intraoral
exami-nations (26,29). Direct comparisonwith their results is not
possible be-cause of their focus on reliability or useof different
methodologies. However,we agree that personnel other thandentists
can be trained to perform oralhealth status assessments.
Primaryhealth care workers have been used inSri Lanka and India to
perform screen-ings to detect oral mucosal lesions(1656).
Observations by nondentistscan be highly valid if the criteria
areclear and appropriate training is pro-vided. In this
investigation we chose aregistered nurse because of her
avail-ability. Her normal duties include thehealth assessment of
children in Mon-ticello, and we foresee theseepidemiologic
assessments as part ofroutine health examinations. What
isparticularly remarkable from the pre-sent findings is that a
nurse, who hadlittle formal dental training, was ableto use the
screening criteria and ade-quately apply them.
Validity of Questionnaires. Ques-tionnaires completed by parents
orguardians were tested for their valid-it y in obtaining status
information ona selected group of oral conditions, i.e.,presence of
restorations, untreated de-cay, sealants, and injuries to the
ante-rior teeth. The instrument included a"don't know" option in
all questionsto avoid forcing the parent to "guess"the status of
their children. A fairlyhigh proportion of respondents didnot know
the oral health sta tus of theirchildren. Validity was modest for
allfour indicators except for restorations(Table 41, suggesting
limitations fortheir use in surveillance.
Many studies have reported on t h equality of self-reported
information ondifferent aspects of oral health. A se-ries of
studies published in the 197Os,1980s, and early 1990s in
Scandinavia(36-41 , England and Ireland (43,57),
and the United States (42) nvestigatedthe quality of data
collected throughquestionnaires. Data collected in
theseinvestigations included the respond-ers' number of teeth and
use of den-tures, presence of caries and gingivaldiseases, and
personal medical his-tory. These investigations comparedthe
self-appraised oral health statuswith results from a clinical
examina-tion. These studies tested reliability(sometimes labeled as
"agreement" or"validity") by using various statistics,including
percent agreement, kappa,statistical mean, and Pearson's prod-uct
moment correlation. Some studiesdescribed overreporting, e.g.,
havingmore tee th than those present(36,41,43), others
underreporting(38,40),or both (37). This inconclusiveevidence
suggests that the reliabilityof self- or proxy-reported oral
healthdata is limited.In this investigation, analysis by
so-ciodemographic variables showed noclear or consistent difference
from theoverall results. This finding may beexplained, in part, by
the sociode-mographic homogeneity of the chil-dren in the
sample.
How "Good" is a "Valid" Proce-dure? A review of publications in
thedental literature reveals subjective as-sessments by
investigators on howgood they view the quality of theirresults
based on values for validity.For example, for O'Sullivan and
Ti-nanoff (58),a positive predictive valueof 87 percent for canes
in the maxillaryteeth a s an indicator of caries risk inthe pits
and fissures of posterior teethin the primary dentition one year
laterwas acceptable. Bretz and co-workers(59) concluded that
PERIOSCANTM,which showed 91 percent sensitivityand 89 percent
specificity, was a validinstrument for detecting
bacterfalcolonization of root surfaces. Pietilaand associates
(22)accepted specificityvalues between 72 percent and 92 per-cent
as valid. Ikeda and associates (17)concluded that a positive
predictivevalue of 71 percent was fairly good.Warnakulasuriya and
Pindborg (16)concluded that a positive predictivevalue of 58
percent was successful. Ina recent publication, Brunette
(60)pre-sented a sample of sensitivity andspecificity values for
diagnostic testsused in dentistry taken from the litera-ture.
Sensitivity for dental can es wasas low as 13percent and as high as
93percent. Clearly, a wide range of ac-
ceptance levels exists. In fact, few stud-ies have concluded
that the proce-dures being tested were not valid. Thisconclusion
can mislead potential userswho might apply a procedure
withborderline validity in a low prevalencesample and reach
incorrect conclu-sions (61).The problem of defining how"good" a
procedure is based on a va-lidity result depe nds on many
aspects,including the nature and quality of thestandard used, the
prevalence of thecondition being assessed (maximizingpositive
predictive value with mini-mum effect on negative predictivevalue),
and the proportion of falsepositives and false negatives the userof
the procedure is willing to accept.These arguments reduce the
problemfrom how "valid" a procedure is to"how practical" it is for
its intendedpurpose. In fact, oral epidemiologiststrade off val
idity for reliability inmany indices and procedures. Giventhis
circumstance, the screening pro-cedure tested in this investigation
ap-pears useful for estimating dental car-ies in samples having a
similar preva-lence to this study.Surveillance systems for oral
condi-tions are so underdeveloped that al-most every aspect of
these systems re-quires empirical support. The need fororal health
status and treatment needsdata is increasing because dental pub-lic
health programs must support theirneed for and use of resources.
Thisinvestigation has tested a visualscreening protocol suitable as
a sur -veillance tool for collecting oral healthstatus data.
Parent- or guardian com-pleted questionnaires seem to be oflimited
us e mainly because a high pro-portion of parents did not know
theirchildren's oral health status, otherthan the presence of one
or more res-torations. Because questionnaires areunlikely to be
designed to addressonly one topic, if necessary, this ques-tion on
restorations could be includedin ongoing structured
questionnaireswith a wider range of topics.References
1. ThackerSB,Berkelman RL. Public healthsurveillance in the
United States.Epidemiol Rev 1988;1016490.2.Stroup NE, Zack MM,
Wharton M.Sources of routinely collected data forsurveillance. In:
Teutxh SM , ChurchillRE, eds. Principles and practice of
publichealth surveillance. New York: OxfordUniversity Press,
1994:31-85.3. Radlke AW. Criteria for diagnosisof den-
-
8/2/2019 Validity Oral
8/9
Vol. 57, No.4, Fall 1997tal caries. Proceedings of the
conferenceon the c l in ical tes t ing of cariostaticagen ts.
Chicago: American Dental Ass@aat ion , 1968.4. National Institute
of Dental Research.O r a l health of United Sta tes
children.Washington, DC: U S Public Health Serv-ice, 1989; pu b n o
(NIH) 89-2247.5. World I lealth Organization. Oral he althsurvey s
basic methods. 3rd ed. Geneva:WllO, 1987.6. Riordan PJ, Espelid I,
Tveit AB. Radio-graphic interpretation an d treatment de-as io ns
among den tal therap is ts and den-tists in Western Australia.
CommunityDent Oral E pidem iol 1991;19:268-71.7. Knutsson K,
Brehmer B, Lysell L, RohlinM. General dental
practitionersevalu-ation of the need for extraction of a s y m
ptomahc mandb u lar th i rd molars . Com-munity Dent Oral Epidemiol
1992;20:347-50.8. Rytomaa I, Jarvinen V, Jarvinen J. Vari-a ti on
in c a n e r eco rd n g an d r e sto ra t iv etreatment plan am ong
university teach-ers. Community Den t Oral Ep idemio
l1979;7335-9.9. Mileman P, Purdell-Lewis D, van derWeek LT.
Variation in treatment dea-s ions and rad ograp h ic car ies d
iagnosisamong un ivers ity teachers . CommunityDent Oral
Epidemiol1982;10329-34.10. Bader JD , Shugars DA. Unders tand
ingdentists restorative treatment decisions.J Public I lealth Dent
1992;52:102-10.11. B a d e r JD , S h u g a r s D A . A g r e e m e
n tamong den t is ts recommendat ions fo rrestorative treatment. J
Dent Res 1993;72:
12. Centers for Disease Control and Preven-tion. Core public
health functions andstate efforts to improve oral health-United
States, 1993. MMW R Mo rb Mor-tal Wkly Rep 1994;43:201,207-9.13 .
Commission on Ch ronicIllness.Chronicillness in the Unite d States
. Vol. 1. Pre-vention of chronic Illness. Cam bridge,MA : f farvard
University Press, 95745 .14. Morrison AS. Screening in chronic d
isease . N ew Y o rk : O x fo rd U n iv e r s i t yPress, 1985.15.
Frankenburg WK. Pnnciples in selectingd i s e a s e s f o r s c r e
e n i n g - c r it e r i a i nscreening test selection.
ln:FrankenburgWK, Cam p BW, eds . Pediatric screening
891-6.
tests. Sprhgf ie ld , IL : Char les C . Thom ag1975:9-37.16 .
WarnakulasuriyaS, PlndborgJJ. Reliabil-it y of oral precancer
screening by pri-mary health care workers in Sri Lanka.Com mun ity
Dent H ealth 1990;772-9.17. Ikeda N, lshii T, Iida S, Kawai T.
Epide-mio log ical s tudy of o ra l l eu k o p lak iabased on m ass
screening for oral mucosaldseases in a selected Japanese
popula-tion. Community Dent Oral Epidemiol1991;19:1M)-3.18. B a n k
z y 1, Rgo 0.Prevalence stu dy oforal precancerous lesions within a
com-plex screening system in Hu ngary . Com-munity Dent Oral
Epidemiol 1991;19:265-7.19. Downer MC, Evans AW, Hug hes HalletCM,
Jullien JA, Speig ht PM, Zakrzew skaJM. Evaluation of screening for
oral can-ce r and precancer in a company head-quarters. Community
Dent Oral Epide-
mi011995;23:84-8.20. Pindborg JJ. Scree ning for oral cancer.
In:Proro k PC, Miller AB, eds . Screen ing forcancer. Technical
Report Series, 78 . Ge -neva: lntemational Union Against Can-cer,
1985.21. Bruck TL. Dental screening. In: Franker-b u rg W K , C am
p B W , ed s . P ed ia t r i cscreening tests. Springfield, IL:
CharlesC. Thomas, 1975:270-84.22. Piehla T, Retila I, Vaataja P.
Early screen-in g for orthodontic treatment. Differ-ences in
assessments mad e by a consult-ant orthodontist and three public
healthden t ists . Community I k n t Oral Ep ide-miol
1992;20208-13.23. Gerstn er GE, Clark GT, Goulet J-P.Valid-ity of a
brief questionnaire in screeningasymptomat ic sub jects f rom sub
jectswith tension-type headachesor te mp or ema ndb u lar d iso
rders . Commun ity Den tOral E pidem iol 1994;22:235-42.24.
Association of State and Territorial Den-tal Directors, Maternal an
d Child Hea lthBureau . Assess ing o ral heal th needs .ASTDD
seven-s tep model . Co lumbus,OH: ASTDD, 1995.25. Heine CS, Jo ngA,
Casamassimo PS,0sterbrock N, Call RL. Oral health statusand behav
io rs of the elderly and otherad u l t s : r e su l t s of a heal
th screen ing .Geriatr Dent 19833:217-21.26. Hu gh es JT, Rozier
RG, Ramsey DL.Natu ral h is to ry of den tal d iseases inNorth
Carolina 19761977. Durham, NC:Carolina Academ ic Press, 1982.27.
Maine Departme nt of Human Services.Survey of the oral health of
Maines hfth-grade public schoolchildren. Augusta,ME: Maine D
epartment of 1 luman Serv-ices, 1985.28. South C arolma D epartm
ent of Healthand Environmental Control. The SouthCaro l ina Den tal
I leal th and Pehatr icBlood Pressure Survey 1982-1983. C elumbia,
SC:South Carolina Depa rtmentof Heal th and Env ironmental Con tro
l.29. Mau riello SM, Bader JD , Disney JA,Graves RC. Examiner ag
reement be-tween hygenists and dentists for cariesprevalence
examinations. J Public t lealthDent 1990;5032-7.30. Disney JA, A
berna thy JK , Graves RC,Mauriello SM, Bohannan I IM, Zack
DD.Comparative effectiveness of visual/tac-tile and simplified
screening examina-tions in caries risk assessment. Com mu-nity Dent
Oral Epidemiol1992;20:32&32.31. Bovonsantijid Y. Factors asso
aa ted withthe reliability of oral examination byteachers in Phuket
primary school orald w a s e w e l l l a n c e p ro g ra m ( d is
se rt a-tion). Bangkok, Thailand: Mahidol Uni-versity, 1990.32 .
Wagener DK, Nou ja h P, I Iorowitz AM.Trends in cluldhood use of
dental carep ro d u c t s co n ta in in g f lu o n d e : U n i t
edStates, 198S89. Advance d ata from Vitaland Hea lth Statistics;
no 219.1 lyattsville,M D Nat ional Cen ter fo r Health S ta t
istics,1992.33.Cleveland J, Holm K, Malvitz D, i Iines B.Recent
dental exams am ong adults inWashington State-Behavioral Risk
Fac-tor Surveillance System, 1993-1994 [ A bstract]. J Dent Res
1996;75(Speclss):231.3 4 . K l e i n b a u m D G , K u p p e r L L,
M o r -
213g en s t e rn H. Epidemio log ic research .Pr incip les and
quan t i ta t ive methods.New York : Van Nostrand Reinho ld
,1986.35 . Ro th man KJ. Mod ern ep idemio logy .Boston, MA:
Little, Brown and Com-pany, 1986.36. Heloe LA. Comparison of dental
healthdata ob tained from questionnaires, inter-view s and clinical
examinations. Scand JDent Res 1972;80495-9.37. Wid strom E, Nilsson
B. Dental healthand p erceived treatement need s of Finn-ish
immigrants in Sweden. %and J SocMed 1984;12:129-36.38. Kononen M ,
Lipasti J, Murtomaa 11 .Comparison of dental informahon o btained
from self-examination and c hi ca lexamination. Com mun ity Dent
Oral Epi-demiol1986;14:258-60.39. Tervonen T, Knuuttila M .
Awareness ofd en ta l d i so rd e r s an d d i screp an cy b ctween
objective and subjective den-tal treatment needs. Community
DentOral Epidemiol1988;16:3458.40.Lahti S, Tuutti H, Honkala E. C o
m p an -son of numb ers of remaining teeth fromquestionnaires a nd
clinical examination.Proc Fin Dent SOC 1989;85217-23.41. Palmqvist
S, Sbderfeldt B, Arnbjerg D.Self-assessment of dental condtions:
va-lidity of a questionnaire. CommunityDent Oral
Epidemiol1991;19:249-51.42. Douglass CW, Berlin J, Tennstedt S.
Thevalidity of self-reported oral health statu sin the e lder ly .
J Publ ic Heal th Den t1991 51:220-2.43. Beal JF, Dickson
S.Parental aw areness ofthe dental needs of 5-year-old children
inthe West Midlands, England. Commu-nity Dent O ral Epidemiol
1974;2:914.
44. enters for Disease Control and Preven-t ion . Recommended in
fect ion -con tro lpractices in den tistr y , 1993. MMWRMorb Mortal
W kly Rep 1993;42(RR-8).45. Summ ers CJ, Gooch BF, Marianos
DW,Malvitz DM , Bond WW . Practical infec-tion control in oral
health surveys andscreenings. J Am Dent Assoc
1994;125:1213.17.46.Kaste LM, Gift HC, Bhat M, Sw ang o
PA.Prevalence of incisor trauma in persons 6to 50 years of age:
United States, 198%1991. J Dent Res 1996;75(Spec Iss):696705.47.
Dean AG, Dean JA, Burton Afl, UlckerRC. Epi Info, Version 6.
Atlanta: Ce ntersfor Dse ase Control an d Prevention, 1994.48.
Gordis L. Epidemiology. Philadelphia:WB S u n d e r s , 1 99 6.49 .
FleissJL.Statisticalmethodsforratesandproportions. New York: John
Wiley &Sons, 1981.50. Landis JR, Koch GG. The measurementof
observer agreement for categoricalda ta. Biometrics
1977;33:159-74.51. Alderman EJ, White SL, Johnson WT.Georga dental
disease prevalence SUT-vey. Georgia Dent Assoc Action 1994:17-19 .5
2. C a m p BW. h c i p l e s of screening. In:Frankerburg WK, Camp
BW, eds. Pedi-at r ic screen ing tests. Springfield, IL:Char les C.
Thomas, 19755-8.53. Gupta PC, Mehta FS,Daftary DK, et al.Incidence
rates of oral cancer and naturalhistory of oral precancerou s
lesions in a
-
8/2/2019 Validity Oral
9/9
214 Journa l of Public Health Dentistry10-year follow-up study
of Indian mllag-ers. Community Dent Oral
Epiderniol1980;8:283-33.
54 . Bouquot JE , Gorlin RJ. Leukoplakia, li-chen planus, and
other oral keratoses in23,616 white Americans over the age of35
years. Oral Surg 1986;61:373-81.55.Axd l T. Occurrence of leuk
oplaha andsome other oral white lesions among20,333 adult Swemsh
people. Commu-nity Dent Oral Epidemiol 1987;13:46-51.
oral cancer using basic health workers inan area of h g h oral
cancer inadence inIndia. Cancer Detect Prev 1986;9218-25.57. Fenlon
MR, McCartan BE. Validty of apatient self-completed health
question-naire in a primary care dental practice.Community Dent
Oral Epidemiol 1992;20:130-2.58. CYSullivan DM, Tinanoff N .
Maxillaryanterior caries associated with increasedcaries risk in
other primary teeth. J Dent
The use of rapid enzymatic assay in thefield for the detection
of infections as=aa ted with adult periodontitis. J PublicHealth
Dent 1993;53:2354.60. Brunette DM. Critical thinlung.
Under-standing and evaluating dental research.Chicago, IL:
Qluntessence, 1996.61. Shapiro MF, Lehrnan AF. he dagnosisof
depression in different clinical set-tings. An analysis of
thelitera ture on thedexamethasone suppression test. J Nerv56.
Mihta FS, Cupti PC, Bhonsle RB, MurtiPR, Daftary DK, Pindborg JJ .
Detection of Res 1993;72:1577-86. Ment Dis 1983;171:7i4-20.59.
Bretz WA, Eklund SA , Radicchi R, et al.
ALAMANCE COUNTYHEALTH DEPARTMEN TNORTH CAROLINADentist position
available with the Alamance CountyHealth Department, Burlington,
NC. Duties include:acting as director for Dental Clinic;
determining den-ta l needs; treatment plans; providing restorative,
sur-gical, and preventive care for children enrolled in theDental
Clinic; serving as consultant for public healthdentistry in
Alamance County, working closely withschools, area dentists, and
community agencies; beingresponsible for the opera tion and fiscal
control of theDental Program, including supervision of 3-5
staffmembers.Salary commensurate with experience. Paid em-ployee
medical/life/dental/liability insurance; de-pendent insurance
available at group rates; paid sickand annual leave; 11-12 paid
holidays; state retire-ment plan; 401K (employee contribution
only).Requirements: graduation from an accredited schoolof
dentistry with a license to practice dentistry in NC.Send completed
county application to Becky Perkins,Alamance County Health
Department, 319 N. Gra-ham-Hopedale Road, Burlington, N C 27217.
Tel.:(910) 513-5517 for more information.
FUTURE AAPHDANNUAL MEETINGDATESOctobe r 21-23/1998. . . . .San
Francisco, CAOctober 6-8,1999. . . . . . . . . . .Honolulu,
HIOctober 25-27/2000 . . . . . . . . . . .Chicago, IL
COLUMBIA UNIVERSITYSYMPOSIUM TARGETS MED ICAIDMAN AGED
CARE"Medicaid Managed Care and its Rela tionship to Den-tistry"
will be the topic of the 13th Dunning MemorialSympsium held at
Columbia University School ofDental and Oral Surgery on March
27,1998. Initiatedin 1981 by James Dunning, dean emeritus at
HarvardSchool of Dental Medicine, the symposium is dedi-cated to
the memory of William and Henry Sage Dun-ning, cofounders of the
Columbia University School ofDental and Oral Surgery.Focusing on
dentistry in the era of managed care, thesymposium will include
opening remarks by the Hon-orable Barbara A. DeBuono, commissioner
of health ofthe New York Department of Health, as well as
pres-entations from both the private and public sectorsgiven by Dr.
Robert Isman, dental program consultantwith the California
Department of Health Servicesandproject director of the Children's
Dental Health Initia-tive of the Dental Health Foundation, and Dr.
Alex B.White, current president of the AAPHD and seniorinvestigator
and associate program director of healthservices and social and
economic studies at the KaiserPermanente Center for Health
Research. The after-noon will involve presentations by three New
YorkState Provider Grant Recipients: DentNY IPA, Inc.,Neighborhood
Health Providers, and Syracuse Com-munity Health Center, Inc. These
will reflect analysesof experiences with populations being served
by themanaged care plans. Professor Emeritus Irwin D.Mandel will
then lead a panel discussion that willinclude the program
participants and Dr. JamesSpencer, a member of the ADA Council on
DentalBenefit Programs.The symposium is sponsored by the School of
Dentaland Oral Surgery of Columbia University, the Dun-ning
Memorial Fund, and the New York Council ofDental Deans. Continuing
education credits will beawarded. For further information, please
contact:Melissa Welsh at Columbia University: (212)305-6881.