Embed Size (px)
Citation preview

Vanderbilt Student Research Training Program
• Diabetes & Endocrinology▫ http://vanderbiltsrtp.org/
• NIDDK▫ http://medicalstudentdiabetes
reseach.org/• Nephrology & Hypertension • National Symposium at
Vanderbilt

Absence of PAI-1 results in direct podocyte protection in vivo
Amanda Morden (Florida State University College of Medicine), Haichun Yang, and Agnes B. Fogo
Vanderbilt University School of Medicine, Nashville, Tennessee

Background
• PAI-1

Background
Hypothesis
• Previous data in vitro and in the 5/6 nephrectomy model: supports that PAI-1 deficiency could directly protect podocytes from injury.
• The previously studied 5/6 nephrectomy model does not injure podocytes directly. The Nep 25 transgenic mice can be used for this purpose.
We hypothesize that the absence of PAI-1 will improve protection against direct injury of the podocyte, and that this will allow decreased ECM accumulation in the Nep 25 podocyte injury model

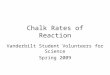
Animal Model: Nep 25/PAI-1 (-/-) Transgenic Mouse
Group NControl 8
PAI-1 Knockout 10
Nep 25/ PAI-1 (-/-) Transgenic Mouse
PAI-1 (-/-) Transgenic Mouse
Assessments Every 3rd
Day
Body WeightUrinalysisBlood Pressure
Mice sacrificed on day 10
Nep 25 Transgenic Mouse
Dose = 11 ng/g BW

ResultsBody Weight
Blood Pressure
Urine Albumin/Creatinine Ratio (ACR)

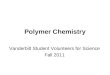
Results
Wild Type WT-1 Staining PAI-1 (-/-) WT-1 Staining
Real Time PCR; WT1

Results
Real Time PCR; B7, GLEPP-1 & synaptopodin
Glomerulosclerosis Index
Real Time PCR; Col I and TGF β

Conclusion
Absence of the PAI-1 gene provides protection to podocytes by preserving podocyte number and differentiation markers after toxic injury which leads to improved outcomes in kidney disease progression.

Is the POLST model desirable for Florida? Brittany Lamb, MS2Sarah Catherine Spillers, JD Candidate 2012

Special thanks goes to Dr. Charles Matthews and the Department of Geriatrics for funding
this research.

What is POLST?
• Physician Orders for Life-Sustaining Treatment
• A form of advance directive • Includes various medical treatments
and turns patient preferences into physician orders

Our goal and methods
• We wanted to make a recommendation for or against the use of POLST in the state of Florida
• Conducted an extensive literature review• Held interviews with family members of
deceased patients, heath care professionals and administrators, lawyers etc
• Finally, we combined this information into a paper

Why did we choose this research project?
• Personal interest/Experiences• Interest in health care policy and
intersections with the law• Relevance- the population of
persons 65 and older is expected to more than double in the U.S. by 2040

History of the form
• Developed in Oregon in the early 90’s• Doctors, nurses, emergency personnel and
ethics committee members were concerned over the shortfalls of existing advanced directives
• They saw problems with unclear language, transferability, and patient preferences not being honored
• The POLST form was born out of these concerns


What type of patient would benefit from POLST?
• Patients who are critically ill/have an end stage disease
• Nursing home/hospice patients

What is wrong with current forms of advance directives ?
1) People don’t use them.2) Even when patients do fill out a form
challenges arise3) The forms are often not transferrable 4) It is very common for patients to have a
DNR order as their only form of advance directive

5) Health care providers often fail to discuss end-of-life issues
I interviewed the sister of Ms. B, a 71 year old who suffered from a stroke leaving her unable to speak or swallow, but retained her mental faculties.
Her sister recalled the following:“She could answer yes or no questions by shaking her head. The hardest part was that I knew she was suffering. She was always thirsty. She would fight people to get to a sink and constantly motioned for water. She was resuscitated several times and I never understood why. When I asked the [hospital] staff, they said they had to do everything they possibly could to keep her alive. It was hard for me to watch. I knew she was suffering and I felt powerless to stop it.”
Ms. B had no advance directive and was subject to this treatment for a year before she passed away.

Does POLST provide a solution for the problems with current advance directives?
• The following findings from studies done in Oregon say yes:
• Hospice staff say POLST helps initiate difficult conversations about end of life treatment goals and successfully prevents unwanted medical treatment
• Nursing home residents’ treatment preferences are being honored with use of the POLST
• EMTs like the form, wish more patients would use it, and say it has changed method of treatment in close to have of their cases

Why would POLST be beneficial for Florida?
• 17% of Florida’s population is 65 years or older -this is the highest percentage in the nation-tied with West Virgina. (Kaiser Family Foundation, 2009)
• We have the 6th highest hospital care intensity index in the country (Commonwealth Fund, 2009)
• We have the 2nd highest percentage of decedents spending a week or more in an ICU during the last 6 months of life at 23.1% (Dartmouth Atlas, 2007)

What is, in our opinion, the best way to implement the use of POLST in Florida?
• Avoid the legislative route- it takes too long • Start with educational efforts to encourage voluntary use
of POLST statewide• Analyze the data from the ongoing pilot study in south
Florida• Implement regulations which recognize the validity of the
form and insure immunity from liability for good faith compliance

Is it legal to use the POLST form now?
• Yes! There is nothing in current Florida law that poses any significant barrier to the use of the POLST Form
§ 765, Fla. Stat. (2011)(“Health Care Advance Directives”)§ 401, Fla. Stat. (2011)(“Medical Telecommunications and Transportation”)

Any Questions?

Thanks again to Dr. Charles Matthews and the Department of Geriatrics

References
• United States Department of Health and Human Services, Administration on Aging, (2010). Aging statistics: Projected future growth of older population [Data file]. Retrieved from http://www.aoa.gov/AoARoot/Aging_Statistics/future_growth/docs/By_Age_65_and_over.xls
• Beach, M., & Morrison, R. (2002). The effect of do-not-resuscitate orders on physician decision-making. Journal of the American Geriatrics Society, 50, 2057-2061.• Cadogan, M. (2010). CPR Decision making and older adults: Clinical implications. Journal of Gerontological Nursing, 36(12), 10-15.• Campbell, Paul R. (2010). State Population Projections. Retrieved from http://www.census.gov/population/www/pop-profile/stproj.html• Dartmouth Atlas. (2007). Percent of Decedents Spending 7 or More Days in ICU/CCU During Last 6 Months of Life, by Gender. Retrieved from
http://www.dartmouthatlas.org/data/table.aspx?ind=129&ch=32&loc=2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52&loct=2&tf=10&fmt=154&sortcol=1&sort=desc
• Ehlenbach, W., Barnato, A., Curtis, J., & Kreuter, W. (2009). Epidemiologic study of in-hospital cardiopulmonary resuscitation in the elderly. The New England Journal of Medicine, 361(1), 22-31.• Fagerlin, A., & Schneider, C. (2004). Enough: The failure of the living will. Hastings Center Report, 34, 30-42.• H.B. 1017, 2006 Leg., Reg. Sess. (Fla. 2006).• Hickman, S., Tolle, S., Brummel-Smith, K., & Carley, M. (2004). Use of the physician orders for life-sustaining treatment program in Oregon nursing facilities: Beyond resuscitation status. Journal
of the American Geriatrics Society, 52, 1424-1429.• Hickman, S., Nelson, C., Moss, A., Hammes, B., Terwilliger, A., Jackson, A., & Tolle, S. (2009). Use of the physician orders for life-sustaining treatment (POLST) paradigm program in the hospice
setting,” Journal of Palliative Medicine, 12: 133-41.• Hickman, S., Nelson, C., Perrin, N., Moss, A., Hammes, B., & Tolle, S. (2010). A comparison of methods to communicate treatment preferences in nursing facilities: Traditional practices versus the
physician orders for life-sustaining treatment program. Journal of the American Geriatrics Society, 2955, 1241-1248.• The Commonwealth Fund. (2009). Hospital care intensity index, based on inpatient days and inpatient physician visits among chronically ill Medicare beneficiaries in the last two years of life.
Retrieved from http://www.commonwealthfund.org/Maps-and-Data/State-Data-Center/State-Scorecard/DataByDimension/Bar-Chart.aspx?ind=32&ch=4&tf=1&sortch=4&sorttf=1• Kirschner, K. (2005). When written advance directives are not enough. Clinics in Geriatric Medicine, 21(1), 193–209.• Kush v. Lloyd, 616 So.2d 415 (Fla. 1992).• Marco, C., & Schears, R. (2002). Prehospital resuscitation practices: A survey of prehospital providers. The Journal of Emergency Medicine, 24(1), 101-106.• Patient Self-Determination Act of 1990, 42 U.S.C. §§ 1395cc, 1396a (1990)).• POLST Paradigm Program Contact List by State. (2011). Retrieved from http://www.ohsu.edu/polst/programs/state+programs.htm• Kaiser Family Foundation. (2009). Population distribution by age, states (2008-2009), U.S. (2009). Retrieved from
http://www.statehealthfacts.org/comparebar.jsp?typ=2&ind=2&cat=1&sub=1&cha=3&o=d• S. 2572, 2006 Leg., Reg. Sess. (Fla. 2006).• Sabatino, C. (2007). Advance directives and advance care planning: Legal and policy issues. Retrieved from http://aspe.hhs.gov/daltcp/reports/2008/ADCongRpt-C.pdf• Sabatino, C., & Karp, N. (2011). Improving advanced illness care: The evolution of state POLST programs. AARP Public Policy Institute. Retrieved from http://assets.aarp.org/rgcenter/ppi/cons-
prot/POLST-Report-04-11.pdf• Scheible v. Joseph L. Morse Geriatric Center, Inc., 988 So. 2d 1130 (Fla. 4th DCA 2008).• Schmidt, T., Hickman, S., Tolle, S., & Brooks, H. (2004). The physician orders for life-sustaining treatment program: Oregon emergency medical technicians’ practical experiences and
attitudes. Journal of the American Geriatrics Society, 52, 1430-1434.• Spann, J. (1999). Implementing end-of-life treatment preferences across clinical settings. State Initiatives in End-of-Life Care, 3. Retrieved from
http://www.rwjf.org/files/publications/other/State_Initiatives_EOL3.pdf• Teno, J., Branco, K., Mor, V., Phillips, C., Hawes, C., Morris, J., & Fries, B. (1997). Changes in advance care planning in nursing homes before and after the Patient Self-Determination Act: Report
of a 10-state survey. Journal of the American Geriatrics Society, 45(8), 940-945.• Teno, J. (2004). Facts on dying: Policy relevant data on care at the end of life. Retrieved from http://www.chcr.brown.edu/dying/factsondying.htm• Tolle, S., Tilden, V., Nelson, C., & Dunn, P. (1998). A prospective study of the efficacy of the physician order form for life-sustaining treatment. Journal of the American Geriatrics Society, 46(9),
1098-1102.• Zewig, S., Kruse, R., Binder, E, Szafara, K., & Mehr, D. (2004). Effect of do-not-resuscitate orders on hospitalization of nursing home residents evaluated for lower respiratory infections. Journal of
the American Geriatrics Society, 52, 51-58.

Preclinical Determination of Large Artery Stiffness
Charles Clark, M2

Outline
• Arterial stiffness and end organ damage• Pulse wave velocity as a measure of arterial stiffness
• Development of our preclinical model• Future directions

Arterial Stiffness and Aging
• Increased arterial stiffness causes isolated systolic hypertension with aging• Aortic stiffness increases independent of blood pressure
O’Rourke et al; J. Am. Coll. Cardiol. Vol 50, No. 1, 2005

Arterial Stiffness is a risk factor for CVD
Chu et al; Heart 96:817-23, 2010

Measurement of Arterial Stiffness
Pulse wave velocity is the primary clinical measure of arterial stiffness.
McEniery et al; J. Am. Coll. Cardiol. 46:1753-1760, 2005

Clinical Technique

Clinical Technique

Preclinical Model to assess PWV
• Previously, pulse wave velocity procedures were done under anesthesia as a terminal procedure
• This method would allow for long‐term, conscious recording
Cosson et al; Am J Phys:207:H2506-12, 2007

Methods
• Subjects: Male Sprague‐Dawley rats, 300 g• Surgery: anesthetized with isoflurane and 2 transmitter device inserted
• Post‐op recovery: 10 days before treatment• Treatments: atenolol (p.o. 25 mg/kg) , LNAME (p.o. 40 mg/kg), temperature (4°C), isoflurane (inhaled, 2%)
• Data Collection: 30‐60 minutes during light phase in home cage

Data Collection

16 ms
Pulse Wave Velocity Measurement
Carotid BP (mmHg)
Aortic BP (mmHg)
200
50
50200

Data
Treatment SBP (mmHg) DBP (mmHg) SBP (mmHg) DBP (mmHg) HR (bpm)H2O 130 ± 6 101 ± 6 139 ± 6 93 ± 6 338 ± 17
LNAME 165 ± 6 134 ± 5 170 ± 5 129 ± 5 312 ± 104 C 144 ± 6 113 ± 6 150 ± 5 105 ± 5 452 ± 22
Atenolol 114 ± 5 87 ± 4 120 ± 4 81 ± 4 280 ± 12Isoflurane 115 ± 5 84 ± 5 122 ± 5 78 ± 5 329 ± 8
AorticCarotid

Measurement of Arterial Stiffness
Pulse wave velocity is the primary clinical measure of arterial stiffness.

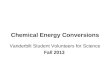
Data
5
5.5
6
6.5
7
7.5
75 95 115 135 155 175
Pulse Wave Ve
locity (m
/s)
Systolic Blood Pressure (mmHg)
PWV vs SBP
LNAME
4 C
H2O
Isoflurane
Atenolol

This new method will advance attempts to understand mechanisms of and potential
treatments for arterial stiffness
Chu et al; Heart 96:817-23, 2010

Acknowledgments
• Postdoctoral Fellow: Rohit Seth, PhD• PI: J Michael Overton, PhD
• FSU College of Medicine Research Fellowship• FSU College of Medicine Seed Grant