Embed Size (px)
Citation preview

ARTICLE IN PRESS
0277-9536/$ - se
doi:10.1016/j.so
�CorrespondE-mail addr
igraham@ohri.
(C. Dornan), a
phebert@ottaw
Social Science & Medicine 64 (2007) 174–185
www.elsevier.com/locate/socscimed
Variant Creutzfeldt–Jakob disease and the Canadian bloodsystem after the tainted blood tragedy
Kumanan Wilsona,�, Ian Grahamb, Maura Rickettsc, Christopher Dornanc,Andreas Laupacisa, Paul Hebertb
aUniversity of Toronto, Toronto, Ont., Canada M5G 2C4bUniversity of Ottawa, CanadacCarleton University, Canada
Available online 2 October 2006
Abstract
The transfusion transmission of hepatitis C and HIV to thousands of Canadian blood recipients was one of this
country’s largest public health catastrophes. In response to this crisis, and in an effort to prevent such a tragedy from
occurring again, the Canadian blood system has undergone substantial reform. Variant Creutzfeldt–Jakob (vCJD) disease
was the first infectious threat faced by the blood system since undergoing reform. The response at the time to this risk
provides insights into the Canadian blood system’s new approach to infectious threats. Our analysis of the decision-
making concerning vCJD identifies two dominant themes characterizing the new blood system’s approach to safety:
(1)
the adoption of a precautionary approach to new risks which involves taking action in advance of definitive evidence,and
(2)
risk aversion amongst policy makers, which has contributed to the adoption of safety measures with comparativelyhigh cost-effectiveness ratios.
Overall the principles governing the new blood system have contributed to the system both providing protection against
emerging infectious risks and regaining the confidence of the public and recipients. However, the current set of policy
factors will likely contribute to increasingly risk-averse policy making that will contribute to continued increases in the cost
of the blood system. The challenge the blood system now faces is to find the appropriate balance between maximizing
safety and ensuring the system remains affordable.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Creutzfeldt–Jakob disease; Blood safety; Policy analysis; Risk decision-making; Precautionary principle; Cost-effectiveness;
Canada
e front matter r 2006 Elsevier Ltd. All rights reserved
cscimed.2006.08.023
ing author. Tel.: +1 416 340 3662.
esses: [email protected] (K. Wilson),
ca (I. Graham), [email protected]
[email protected] (A. Laupacis),
ahospital.on.ca (P. Hebert).
Introduction
The transfusion of individuals with productsinfected with HIV and hepatitis C was, arguably,the largest public health catastrophe in Canada’s
.

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 175
history. Estimates suggest that infected transfusionsled to more than one thousand individuals acquiringHIV and up to 30 000 individuals acquiring hepatitisC (Krever, 1997a). A national inquiry into thefunctioning of the blood system and how it couldhave led to the tragedy, headed by Justice HoraceKrever, precipitated a transformation of the deliv-ery of transfusion services in this country. Thistransformation involved the replacement of theCanadian Red Cross as the operator of the bloodsystem and the creation of new financial arrange-ments and operating principles (Krever, 1997b). Ithas now been 8 years since Canada’s blood systemhas undergone reform and the opportunity exists toreflect on how successful the transition to a newsystem has been. From the perspective of managinginfectious threats, the new blood system would haveto be viewed as a major success. Canada has actedaggressively to protect the blood supply from realand theoretical risks such as variant CJD, West Nilevirus and Severe Acute Respiratory Syndrome(Canadian Blood Services, 2004). In this regard,the post-Krever blood system has received highmarks, including from hemophiliacs who were oneof the primary groups affected by the tainted bloodtragedy (Canadian Hemophilia Society, 2005).However, the blood system has not been withoutcriticism, which has primarily been directed at theintroduction of safety measures with prohibitivecost-effectiveness ratios that have contributed toescalating blood costs.
There are several opportunities to learn from theCanadian blood system’s reform efforts and in manyways the blood system provides an important modelfor other public health sectors which are addressingnew and emerging risks in an increasingly risk averseenvironment. To better understand how decision-making has been transformed in the post-Krever erawe provide a detailed examination of the Canadianblood system’s management of variant Creutzfeldt–-Jakob disease, its first infectious threat since under-going transition. While many faults could be foundwith how blood officials managed affairs leading tothe tainted blood tragedy, one of the areas ofparticular concern was how scientific evidence wasutilized to formulate policy. Our analysis is thereforeassisted by the use of a descriptive policy analysisframework that focuses on the role of information inthe policy process. We review our findings in thecontext of subsequent blood policy decisions toarrive at general principles governing policy makingin the post-Krever environment.
The vCJD policy problem
In the late 1990s, the Canadian blood system andhealth officials were confronted with a true policydilemma: how to manage the theoretical risk ofblood transmission of CJD. This challenge emergedjust as Justice Krever was releasing his final reportand federal/provincial/territorial officials werecreating a new blood system in line with many ofthe recommendations of this report. The challengealso presented itself as the United Kingdom wasaddressing the outbreak of Bovine SpongiformEncephalopathy, which eventually led to the emer-gence of vCJD in humans, and dealing withcriticism of their response to this crisis. Thus, thepotential transfusion transmission of CJD com-bined aspects of two of the highest profile publichealth controversies at the time.
Further contributing to the challenge of mana-ging the infections risk posed by CJD to the bloodsupply was the unusual nature of the disease itself.CJD is a rare infectious condition that is believed tobe caused by a new form of infectious agent, aninfectious protein, known as a prion (Prusiner,1982). The infection is devastating and affectedpatients suffer progressive neurological deteriora-tion and dementia due to spongiform changes in thebrains of the victims. Patients inevitably die fromthe infection, usually within a year of the diagnosis.While extremely rare (o1% of all cases), there havealso been several documented cases of iatrogenictransmission of CJD. The documented iatrogenictransmission of CJD via human growth hormone, inparticular, raised concerns in the United States andCanada about whether the condition may also betransmissible via blood products. This concernarose in the Canadian blood system, as it wasrecovering from the tragedy of hepatitis C and HIVblood transmission. As a consequence, the potentialtransfusion transmission of CJD was viewed as thefirst major test for the blood system after theseinfectious threats (Vaughan, 1996).
The challenge of managing the potential trans-mission of CJD via blood products was furthercomplicated by the discovery, in 1996, of a variantform of CJD in the United Kingdom (Will et al.,1996). The condition was believed to have arisenfrom Bovine Spongiform Encephalopathy (BSE).While there was no epidemiological evidence ofblood transmission of vCJD, the theoretical riskwas considered higher than classical CJD for avariety of reasons (Cashman, 1999). Policy makers

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185176
in the United Kingdom decided to reject donationsfrom their citizens and import their plasma require-ments due to concerns over the potential bloodtransmission of vCJD. This prompted decision-makers in the United States and Canada to evaluatewhether they should accept donations from indivi-duals who had traveled to the United Kingdom.However, this would potentially reduce the bloodsupply and cause shortages. Ultimately Canadianpolicy makers decided to defer donations fromindividuals who had spent 6 months in the UnitedKingdom between the years 1980 and 1996 (thepeak period of the BSE epidemic). It was antici-pated that this policy would reduce the risk of vCJDto the blood supply and ensure that the bloodsupply remained adequate (Wilson et al., 2001).These policies have been modified as furtherevidence has accumulated of the prevalence ofBSE and donor deferral policies have been insti-tuted for individuals who have resided in Franceand all of Western Europe. Most significantly,scientific evidence has accumulated which validatesthe institution of the precautionary policies, bothfrom animal models demonstrating transfusiontransmission and from case reports of transfusiontransmission in humans (Wilson & Ricketts, 2004).
A framework for understanding decision-making on
health risks
To understand decision-making on issues of riskpertaining to the blood system, analytical tools thatprovide a comprehensive understanding of themultiplicity of factors that influence policy arerequired. Descriptive policy analyses are well suitedto analyzing policy making concerning risks byidentifying the critical factors influencing decision-making as well as providing insights on wheredecision-making breaks down and, equally impor-tant, where it works effectively (Hogwood & Gunn,1984). Descriptive policy analyses in health, how-ever, have often been based on the assumption thatrational decisions are made on the basis of completeinformation (Pal, 1992). Given the uncertainty ofscientific information on potential health risks, theseinformation-based models may not be adequate.Alternative models to evaluate decision-makinghave focused on the role of value systems orinstitutions. However, to be truly comprehensive,approaches to policy analysis integrating the impactof information, values and institutions are needed toensure that both the policy makers and the public
understand how decisions are made concerninghealth risks.
Paul Sabatier has compiled some of the availableframeworks for conducting descriptive policy ana-lyses (Sabatier, 1993a). One of the criteria used forselecting frameworks is that they address the roles ofconflicting values and interests, information flows,institutional arrangements and variations in socio-economic environment on the policy process. Thefollowing frameworks were identified as useful fordescribing decision-making within a given politicalsystem or set of institutional arrangements: thestages heuristic, institutional rational choice, multi-ple-streams framework, punctuated equilibriumframework and the advocacy coalition framework.The last framework, the advocacy coalition frame-work (ACF), was proposed by Sabatier and suggeststhat decision making occurs in a policy subsysteminvolving individuals from a variety of public andprivate organizations who are actively concernedwith a policy problem. Within this subsystem,individuals aggregate into advocacy coalitions basedon shared ideologies and beliefs. The success of thecoalitions in translating their beliefs into policy isdependent upon their resources (money, expertise,legal authority and size). Policy brokers attempt tomediate the conflict between the various advocacycoalitions. This process of conflict and mediationeventually results in policy outputs by the governingstructures in the subsystem (Sabatier, 1987; Sabatier,1993b). The ACF model has been identified as beingeffective in describing decision-making in a varietyof policy sectors (Jenkins-Smith & Sabatier, 1994).
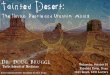
A modification of the ACF model has been putforward by Jonathan Lomas (Fig. 1) (Lomas, 2000).In this model individuals make policy in an‘‘institutional structure for decision-making’’. Thisstructure consists of ‘‘formal’’ actors, who actuallyparticipate directly in the decision-making process,and ‘‘informal’’ actors, who influence decision-making through other means. Values in this modelare divided into ideologies (views on how thingsought to be), beliefs (causal assumptions on howthings are), and interests (responses to incentivesand rewards). In addition, this model pays greaterattention to the role of information producers andpurveyors. It specifically examines how informationis produced and spread and how the value systemsof those involved in the policy subsystem influencethe interpretation and use of this information.
Our choice of the Lomas framework was basedon face and content validity parameters; i.e. the

ARTICLE IN PRESS
Power Relationships
Persuasion
Information
InstitutionalStructure for
Decision-Making
ProducersResearchers
InstitutesPollsters
PurveyorsMedia
AdvocatesNetworks
Knowledge
Formal StructureExecutiveLegislative
Bureaucracy
Informal StructurePolicy Brokers
CoalitionsStakeholders
Citizens
Values
IdeologiesViews aboutwhat ought to
be
BeliefsCausal
assumptionsabout what is
InterestsResponses to
incentivesand rewards
Policies
Epistemology,
Fig. 1. Lomas policy analysis framework. A schematic of the contextual influences on the decision-making process.
K. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 177
domains we felt would be important are appro-priately captured in the framework. The vCJDdecision was primarily characterized by how policymakers utilized scientific information. In this sense,the Lomas framework is well suited to conductingthe analysis given its focus on knowledge develop-ment and knowledge transfer. The framework’shypothesis that policy makers resolve conflictsbetween their various value systems through aprocess of cognitive dissonance reduction is alsowell suited to analyzing a policy problem whereinformation is uncertain and value systems wouldnecessarily play a particularly prominent role.
Understanding the Canadian blood systems vCJD
donor deferral policy
The objective of our overall study was to under-stand and compare the decision-making processes
concerning two Creutzfeldt–Jakob disease-relateddecisions: a 1995 withdrawal of blood productsfrom a classical CJD donor and a 1999 decision todefer donations from individuals who had traveledto the United Kingdom for 6 months during thepeak of the BSE outbreak (1980–1996). We present,here, the full analysis of the second decision, withthe first decision acting as important historicalcontext.
Our study consisted of a literature review andsemi-structured interviews. The literature reviewincluded a systematic review of the risk of transmis-sion of CJD via blood products, a content analysisof newspaper reporting as well as a review ofimportant policy documents. In total we conducted31 semi-structured interviews with key informantsof all major decision-making organizations. Indivi-duals were asked to describe decision-makingleading to the 1995 and 1999 decisions as well as

ARTICLE IN PRESS
Table 1
Factors influencing decision-making on the CJD donor deferral
decision
Information 1. Risk of transfusion transmission of vCJD
2. Impact of deferral policy on blood supply
3. Degree of reduction of blood supply that
system can sustain
Information
purveyors
1. Think-tank
2. Scientists
3. Media
Values Beliefs: theoretical risk of transfusion
transmission of vCJD
Ideologies: evidence-based decision-making vs.
precautionary principle
Interests: protection of supply vs. safety of
supply, legal, re-establishing confidence
Institutions 1. Existence of two operators
2. Separation of regulatory and financial
responsibilities
3. Decisions in other policy subsystems (UK,
US)
4. Legacy of the Krever Inquiry
K. Wilson et al. / Social Science & Medicine 64 (2007) 174–185178
other relevant decisions. Individuals were also askedabout the role of information, information pur-veyors, decision-making organizations and externalfactors in the decision-making process. All informa-tion from the interviews was coded using QSRNudist, a qualitative software program. Findings ofthe study were fed back to decision-makers throughmember check sessions with key stakeholder orga-nizations. Our findings have been presented in aseries of papers, initially focusing on information(Wilson, Code, & Ricketts, 2000) and informationpurveyors (Wilson et al., 2004), then institutions(Wilson et al., 2001; Wilson, McCrea-Logie, &Lazar, 2004) and finally the role of values andchanges in ideology (Wilson, Wilson, Hebert, &Graham, 2003). We synthesized the results of thesestudies using the Lomas framework. Based on thissynthesis we isolate the key policy factors that aredriving current decision-making in the Canadianblood system. We then propose mechanisms bywhich acting on these policy factors could influencefuture decisions.
Factors influencing decision-making (Table 1)
Information
In Canada three pieces of information played animportant role in influencing the decision-makingprocess leading to the donor deferral decision: (1)the risk of transmission of vCJD via bloodproducts, (2) the impact of donor deferral on theblood supply, and (3) the degree of reduction in theblood supply the blood system could sustain. All ofthese pieces of information had substantial levels ofuncertainty associated with them. There were noepidemiological studies on risk of blood transmis-sion of vCJD and an estimation of the risk wasbased primarily on biological models. Based onthese models the theoretical risk possibility of bloodtransmission of vCJD was considered for thefollowing reasons: vCJD had been demonstratedto be transmissible through a peripheral route (GItract) and thus peripheral transmission via bloodproducts was believed to be possible, the prionconcentration in affected tissues was high in vCJDand prions are found in the lymphoreticular systemin vCJD which is intimately linked to the bloodsupply (Cashman, 1999). Scientists argued that thisevidence of risk based on biological models wassubstantial enough to warrant government action toprotect the blood supply.
Given the uncertainty of information on risk ofblood transmission of vCJD the impact of a policyon the blood supply needed to be considered beforeproceeding. This information was obtained from asurvey that suggested that a 3% reduction in theblood supply would occur with a 6-month deferralpolicy. Previous experience in the blood systemindicated that a 3% reduction was sustainable,although there was considerable uncertainty overthis estimate. In an attempt to integrate all of thisinformation, as well as the likelihood of developingvCJD over different residency periods in the UnitedKingdom, a risk modeling exercise was performed.This analysis also suggested that the risk ofcontracting vCJD increased after 6 months resi-dence in the United Kingdom. However, this modelwas based on infectivity rates of BSE that, to thisdate, remain unclear (ElSaadany & Giulivi, 2000).
Information purveyors
Three major information purveyors influencedthe policy process leading to the donor deferraldecision: scientists, the media and think tanks. Themedia’s primary role was to disseminate the releaseof a report by a think tank advisory committee onbioethics, which advocated that the Canadian blood

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 179
system should adopt a donor deferral policy (BayerAdvisory Council on Bioethics, 1998). In combina-tion, this report and the media coverage it receivedplayed an important agenda setting function bybringing the emerging issue to the public’s attention(Wilson et al., 2004). Scientists also played animportant role in communicating information onrisk to policy makers. In particular, due to the lackof scientific expertise on the subject, one scientistcame to play a prominent role in the decision-making process. This individual was a consultant onthree separate sources of information that weresupplied to the decision-makers. All of theserecommended that the government take action toprotect the blood supply from vCJD (BayerAdvisory Council on Bioethics, 1998; Cashman,1999; Expert Advisory Committee on Blood Reg-ulation, 1998).
Institutions
We had a unique opportunity to assess the impactof institutions on decision-making by being able tocompare the vCJD donor deferral decision toanother CJD related decision that took place priorto institutional change in the blood system; the 1995recall of blood from a classical CJD donor. Themajor structural changes to the blood system thattook place over this time period was the replace-ment of the Canadian Red Cross as sole operator ofthe blood system by two separate operators, Hema-Quebec in the province of Quebec, and CanadianBlood Services in the rest of Canada. We observedthat the movement to a two-operator system had animportant impact on the decision-making process.The presence of a second operator introduced aform of ‘‘check and balance’’ on the decision-making processes of the larger operator by propos-ing competing policy options to address the vCJDproblem. However, it also increased the complexityof the decision-making process and initially pro-duced some inter-institutional conflict (Wilsonet al., 2001).
Distribution of regulatory authority and fundingalso played an important role in the decision-making process, specifically the separation of thesetwo functions. In Canada regulatory authority forblood products exists at a federal level. Financing ofthe blood system is the responsibility of theprovinces. In this system, the incentive exists forthe regulator to introduce policies that maximize thesafety of the blood supply, and the financial
considerations of the decision play a secondary role(Wilson, McCrea-Logie et al., 2004).
Other institutional effects include decisions madeby institutions in parallel subsystems, in particularother countries’ blood systems. The UK decision toban plasma donation from its own citizens played alarge role in initiating the decision-making processin both Canada and the United States as to how tohandle donations from individuals who had traveledto the United Kingdom. Of particular importance,Canadian policy makers attempted to coordinateCanada’s donor deferral policy with that of theUnited States. This was largely a consequence of thefact that Canada imports a substantial portion of itsplasma requirements from the United States. Ingeneral, Canadian policy makers are expected tomeet international standards in protecting the bloodsupply (Canadian Blood Services, 2003).
Value systems
We observed that most individuals shared acommon belief, defined as a ‘‘causal assumption ofwhat is’’, on the risk of transmission of CJD; thattransfusion transmission was a theoretical risk withno known documented cases of transmission.However, while the risk was viewed as theoretical,the type of risk which was presented is one to whichthe public and policy makers would be particularlyaverse. The factors contributing to this perceptionof risk include the potentially catastrophic, invo-luntary nature of the risk, the lack of knowledge ofthe risk and the lack of trust in the system’s abilityto manage the risk (Slovic, 1987).
Ideologies, defined as ‘‘causal assumptions ofhow things ought to be’’, played an important rolein determining how information was interpretedand utilized to develop policy. Two dominantideologies on how decision-making should takeplace on issues of risk were at play: evidence-baseddecision-making and the precautionary principle.The precautionary principle came to play a parti-cularly prominent role largely as a consequence ofthe Krever Inquiry into the blood system use.However, we observed a clear tension in whichdecision-makers struggled with the idea of introdu-cing a policy that could create a health risk (bloodshortages) to protect against a risk for which noepidemiological evidence existed (Wilson, Wilsonet al., 2003).
At the institutional level, we found competinginterest systems at work. The regulator’s primary

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185180
responsibility was to protect the safety of the bloodsystem. The operators, in contrast, were interestedin balancing safety with adequacy of supply.However, all players in the blood system recognizedthe crucial need to reestablish public confidence inthe blood system and their responsibility to protectthe blood supply on behalf of the public. At the levelof the policy-maker, the lasting effects of theKrever Inquiry played an important role in influen-cing individuals’ actions. The spotlight that wasplaced on previous decision-makers in the bloodsystem and the legal consequences of the subsequentcriminal probe created a climate that encouragedimplementation of a risk-averse policy (Picard,2002).
Synthesis
Reconstructing the policy process from thefactors we have analyzed presents us with thefollowing explanation of why events unfolded asthey did. Agenda setting in Canada primarilyoccurred due to policy decisions made in othercountries (e.g. the UK blood system). Publicawareness was raised by the release of a think-tankreport and the dissemination of the informationfrom this report via the print media. The decision tointroduce a partial measure to protect against thetheoretical risk, in the absence of definitive evidenceof the risk, was largely influenced by the knowledgethat the United States would proceed with a similardecision. The Canadian decision-making processwas also shaped by the emergence of the precau-tionary principle as a dominant ideology in publichealth. However, perhaps the most importantdriving factors in the decision-making process werethe past experience of the blood supply withhepatitis C and HIV, the general shadow cast bythe recent Krever Inquiry, policy maker fiduciaryduty to the pubic and their need to re-establishpublic trust by being seen to be acting pro-actively.
Blood policy making after the tainted blood tragedy:
precaution and risk aversion
The vCJD policy decision deserves closer exam-ination for several reasons. It demonstrated howpolicy was made to address an, at the time,theoretical risk. The Canadian vCJD donor deferraldecision was also emblematic of how other nationsaddressed the vCJD threat. In addition to with-drawing blood products derived from individuals
subsequently diagnosed with vCJD and importingfractionated products from abroad, the UK hasrecently decided to ban donations from individualswho had previously received a transfusion. Francealso has instituted precautionary policies includingthe introduction of leukoreduction, which theoreti-cally would remove infectious material from do-nated blood (Lee, 2001). The US policy regardingvCJD was similar to Canada’s, choosing to intro-duce donor deferral policies for individuals who hadtraveled to countries in which BSE was endemic(FDA, January 2002). The vCJD decision-makingprocess in all of these countries reflected a paradigmshift in how to manage emerging risks. This newparadigm involved the institution of protectivemeasures at an early stage of the risk identificationprocess and reflected a conscious decision by policymakers to act in advance of complete scientificinformation.
Important lessons can be learned from theCanadian vCJD policy-making process and thedecision-making process stands in stark contrastto the decisions concerning hepatitis C and HIV inthe pre-Krever blood system. In particular, two keythemes that have come to dominate decision-making in the post Krever era deserve furtheranalysis—the application of the precautionaryprinciple to blood policy and the challenge of risingcosts in a risk-averse blood system.
Precautionary decision-making
Blood policy makers, in addressing the potentialthreat of vCJD, ultimately embarked upon astrategy that they believed balanced the reductionin blood supply with reducing the risk of exposureof Canadians to potentially infected blood products.This decision explicitly acknowledged the possibilityof risk in the absence of epidemiological studies andrepresented a critical shift from the previousmechanism of policy making. Many criticisms existof blood policy making in several countries leadingto the transfusion transmission of hepatitis C andHIV. Particularly, in the instance of HIV, thecriticisms surround unacceptable delays implement-ing policies recognized as providing some protectionto blood recipients (Gilmore & Somerville, 1999;Picard, 1998; Weinberg et al., 2002). However, oneof the primary limitations of pre-Krever decision-making in Canada was the manner in whichscientific information was utilized in the formula-tion of policy. This was perhaps most glaringly

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 181
demonstrated when considering the decision-mak-ing process concerning the adoption of surrogatetesting for hepatitis C. The details of the Canadiandecision regarding surrogate testing has been welldescribed elsewhere (Krever, 1997c). In summary,blood officials in the 1980s were confronted with thethreat of a new form of hepatitis referred to asnonA-nonB hepatitis, later discovered to be hepa-titis C. This form of hepatitis was known to betransfusion transmissible, however, the virus hadnot been identified and thus no specific test existedto identify contaminated blood. Consideration wastherefore given to the use of surrogate tests whichcould not only identify some infected donations butalso would result in the discarding of somedonations that were not infected (Aach et al.,1981; Alter, Purcell, Holland, Alling, & Koziol,1981). Canadian officials awaited the results of aprospective trial that compared the rates of posttransfusion hepatitis from individuals who receivedblood from donors who had surrogate testingcompared to those who received blood from donorswho had not undergone surrogate testing. Unfortu-nately, by the time evidence demonstrating theefficacy of the surrogate testing strategy becomeavailable, thousands of individuals had becomeinfected by hepatitis C through blood transfusions,many of which could potentially have been pre-vented (Blajchman, Bull, & Feinman, 1995).
On reflection, it becomes apparent that a funda-mental failing of the Canadian blood system’smanagement of hepatitis C was the adoption orperhaps misapplication of the evidence-based para-digm when developing policy concerning safety. Theevidence-based paradigm is dominated with thebelief in a hierarchy of evidence that asserts thatrandomized trials are the highest level of evidence(Upshur, 2003). In the tainted blood tragedy suchan approach was found to be wanting in manyrespects, primarily related to the consequences ofwaiting for high quality evidence when the health ofpopulations, as opposed to the health of individuals,is at risk. Reflecting this recognition, the ‘‘precau-tionary principle’’ has emerged as a new paradigmgoverning the use of scientific information. Theprecautionary principle essentially states that com-plete evidence of risk does not have to exist beforeaction is taken to protect against the risk, particu-larly when the risk is potentially catastrophic(Wingspread conference participants, 1998).Although there are numerous interpretations ofthe principle, applications generally advocate an-
ticipatory action to protect against harm, prioritizeprotection of public health and the environment andpromote public participation in decision-making(Stoto, 2002). While the principle has become highlyinfluential in risk decision-making in the environ-ment and in health, it also has been heavilycriticized. Opponents of the principle point to itslack of clarity, potential to create unnecessary fearand potentially denying the public the benefits ofnew technology (Morris, 2000).
In addressing the theoretical risk of vCJD, theCanadian blood system, and blood systems aroundthe world, was guided by the precautionaryprinciple. However, at the same time they alsointegrated components of evidence-based policymaking in an attempt to find a middle groundbetween these potentially conflicting paradigms.Specifically, they chose to introduce a measuredresponse that would not cripple the blood supply.This response was then calibrated as new evidenceemerged on risk of transmission. In doing so theysucceeded in accomplishing several policy objectivesincluding reestablishing confidence in the bloodsystem and demonstrating to the public that policymakers were acting proactively to protect thepublic. Most importantly, as evidence accumulatedto demonstrate the probable transfusion transmis-sibility of vCJD, the policy decisions made byCanada and other countries appear to have beenwarranted and likely prevented further spread ofvCJD through transfusion (Llewelyn et al., 2004;Peden, Head, Ritchie, Bell, & Ironside, 2004).In hindsight, the integration of precautionary policymaking in the new blood system would have to beconsidered a major success (Wilson & Ricketts,2004).
Risk aversion and increasing costs
While the new blood system’s precautionaryapproach to blood safety has received praise it alsohas not been without some criticism. In Canada,over a three-year period since the blood systemunderwent structural reform, expenditures in theblood system have increased by 50% (Wilson &Hebert, 2003). These rising blood system costs havebeen attributed to several factors including theincrease in use of blood products, and the increasein cost of specific blood products such as intrave-nous immunoglobulin (Wilson, MacDougall et al.,2003). However, attention has particularly beenfocused on the introduction of new safety measures

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185182
that have only marginally improved the safety of theblood supply. Some transfusion policy analysts havedescribed the introduction of these safety measuresas ‘‘irrational’’. These individuals point to thenormally prohibitive cost-effectiveness ratios ofmany of theses measures (Bayer & Feldman,1999). The cost-effectiveness ratios associated withseveral of the post–Krever safety measures has farexceeded the generally accepted cost-effectivenessratios of $50 000 to $100 000 per QALY (Laupacis,Feeny, Detsky, & Tugwell, 1992). For example, thecost/quality adjusted life year of nucleic acidamplification testing for hepatitis C is $4 million/QALY and for solvent detergent plasma $8 million/QALY (AuBuchon & Petz, 2001). These tests havealso impacted upon the cost of blood. Nucleic acidamplification testing for both hepatitis C and HIVhas been estimated to contribute 13–20% of the costof a unit of blood in the United States (Weinberg etal., 2002). Blood systems are also being confrontedwith the decision of adopting several expensive newsafety measures, such as pathogen inactivationtechnologies (Council of Europe, 2001). In theUnited States (US) the Medicare Payment AdvisoryCommittee identified that blood-related costs havebeen increasing more rapidly than other hospitalcosts placing strains on the current DiagnosisRelated Group (DRG) payment system (MedicarePayment Advisory Committee, 2001). In Canada,provinces, which are responsible for funding theblood system, have expressed unease about risingblood costs and asked for a reconsideration of howpolicy decisions concerning the introduction ofsafety measures are being made (IBM Consulting,2002).
The decision to introduce highly risk aversepolicies (i.e. the choice of policies with a highcertainty of eliminating remote risks) does notappear to be driven by ‘‘public hysteria’’ but ratherby incentive systems that act directly on the policy-makers. Evidence for the lack of public demanddriving the policy process is provided by theintroduction of other similar protective policies.For example leukoreduction, a process by whichwhite blood cells are removed, was introduced toprotect against transfusion reactions and potentiallyother immune mediated effects. The policy metsome controversy over its necessity and could not beexpected to have been a high agenda issue for thepublic who would have little understanding of theprocess and for whom transfusion reactions wouldnot be a major health concern (Goodnough, 2000).
The other explanation for the lack of publicinfluence on blood policy is the absence of well-defined advocacy coalitions representing the publicand the interests of consumers of blood products(Orsini, 2002). The majority of recipients of bloodproducts are members of the general populationwho cannot necessarily be identified in advance. TheCanadian blood system has also explicitly involvedrepresentatives of various consumer groups in theirpolicy making process which has reduced the needfor public lobbying by these individuals.
In contrast to the relative lack of risk aversionamongst the public, our analyses suggest that riskaversion on the part of policy makers is likelyresponsible for the introduction of several of thesafety policies. Canadian officials are eminentlyaware of the public health consequences of thetransfusion transmission of hepatitis C and HIV.They also cannot help but be aware of the legalconsequences of those who were involved in thedecision-making processes at the time. The currentincentive structure does little to protect againstliability because the recommendation of the JusticeKrever to introduce a no-fault compensation systemfor transfusion related injury was not implemented.Such systems have been found to be effective incontrolling litigation in pediatric vaccination, ananalogous policy area (Plotkin, 2001). Furthercontributing to risk-averse policy making is theseparation of funding from decision-making in theblood system, with the federal government havingthe authority of introducing safety measures but notthe responsibility for paying for them. The impactof this structural factor on blood system costs couldhave been mitigated if Justice Krever’s recommen-dation to have hospitals pay for blood products hadbeen introduced since the budget restrictions of thehospitals would have limited their ability to pay forexpensive products.
Policy making concerning blood safety—looking
forward
Despite the growing cost pressures on the bloodsystem, we would expect the Canadian blood system’sproactive response to threats to blood safety tocontinue, given the current set of operating principlesand policy factors at play. Consequently, so will thetrend towards the adoption of risk-averse safetymeasures with marginal cost-effectiveness ratios. Ifindividuals in the blood system are interested incontinuing the current practice of ensuring a safe

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 183
blood supply with cost being a secondary concern,little change needs to occur in the decision-makingprocess. On the other hand, if blood system decision-makers or provincial officials responsible for fundingthe blood system desire a change to this approach, itis unlikely that additional studies demonstrating thecomparatively poor cost-effectiveness of safety mea-sures alone will have much impact. The current set ofinstitutional arrangements, in which the regulator canintroduce safety regulations and not be held directlyresponsible for the costs of these regulations, willcontinue to encourage the implementation of safetymeasures to ensure a high level of blood safety. This isalso encouraged by the arms length relationshipbetween the blood system operator and the provincialfunders that permits the operator to independentlyintroduce safety measures. To combat the impact ofthese factors provincial governments will have tomake efforts to regain control of the policy makingprocess in the blood system, or perhaps requirefederal regulators to pay a component of the costsassociated with their safety regulations. The scenarioof such federal unfunded mandates imposing costburdens on other orders of government has beenobserved in the US where it was partially addressedthrough legislative means (Conlan, Riggle, &Schwartz, 1995). A risk-averse approach to bloodsafety is further encouraged as long as decision-makers are aware of their potential legal and publicaccountability and a no-fault compensation programfor transfusion injured recipients that limits legalliability may help address this issue. Our analysis alsosuggests that as long as the Canadian blood supply isreliant upon importing plasma from the UnitedStates, Canadian blood policy will be heavilyinfluenced by US blood policy. The continued goalof the Canadian blood system to achieve self-sufficiency may address this concern. Nevertheless,in an increasingly integrated world, decisions made inparallel policy subsystems of other nations’ will play acrucial role in determining policy. Standard of caremay be defined as the international response to athreat and a decision-maker who disagrees with thisresponse may still be left with little option but to meetthe international standard.
Despite the presence of these factors, the adop-tion of highly risk averse policies cannot continueendlessly and the opportunity costs of these policieswill become increasingly evident. Eventually, policy-makers will have to decide at what level ofuncertainty of risk or at what level of cost/QALYsafety measures will not be introduced. The decision
of whether to adopt pathogen inactivation technol-ogies, which offer the promise to remove bothknown and unknown pathogens from transfusionsalthough at a substantial cost, will present aninteresting challenge to the continued adoption ofnew safety measures.
Conclusion
In many ways, the Canadian blood system servesas a model for a transformed system emerging froma crisis of confidence. vCJD represents the firstinfectious threat to this transformed system andimportant lessons can be learned from how thisthreat was managed. Decision-making related tovCJD is representative of the new blood system’sapproach of aggressively addressing risk in aproactive manner and introducing policies inadvance of clear evidence of risk. While thisapproach was essential in the first stages of reform,and has reestablished the confidence of the Cana-dian public, it has contributed to rising costs. Thechallenge the blood system now faces is to find theappropriate balance between maximizing safety andensuring the system remains affordable.
Acknowledgments
This study was supported by a grant from theCanadian Institutes of Health Research. Thanksalso to Cathy Code and Nadya Ahmad.
References
Aach, R. D., Szmuness, W., Mosley, J. W., Hollinger, F. B.,
Kahn, R. A., Stevens, C. E., et al. (1981). Serum alanine
aminotransferase of donors in relation to the risk of non-A,
non-B hepatitis in recipients: The transfusion-transmitted
viruses study. New England Journal of Medicine, 304(17),
989–994.
Alter, H. J., Purcell, R. H., Holland, P. V., Alling, D. W., &
Koziol, D. E. (1981). Donor transaminase and recipient
hepatitis. Impact on blood transfusion services. Journal of The
American Medical Association, 246(6), 630–634.
AuBuchon, J. P., & Petz, L. D. (2001). Making decisions to
improve transfusion safety. In J. AuBuchon, L. Petz, & A.
Fink (Eds.), Policy alternatives in transfusion medicine.
Bethesda, MD: AABB Press.
Bayer Advisory Council on Bioethics. (1998). Creutzfeldt– Jakob
disease, blood and blood products: A bioethics framework.
Ottawa: Bayer Advisory Council on Bioethics.
Bayer, R., & Feldman, E.A. (1999). Understanding the blood
feuds. In F. E. A., B. R. (Eds.), Blood feuds. Aids, blood,
and the politics of medical disaster. Oxford: Oxford
University Press.

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185184
Blajchman, M. A., Bull, S. B., & Feinman, S. V. (1995). Post-
transfusion hepatitis: Impact of non-A, non-B hepatitis
surrogate tests. Canadian Post-Transfusion Hepatitis Preven-
tion Study Group. Lancet, 345(8941), 21–25.
Canadian Blood Services. (2003). CBS response and action
plan—summary. In Performance review of Canadian blood
services. Canadian Blood Services.
Canadian Blood Services. (2004). Safety of products. In Rising to
the challenge. A report to Canadians 2003/4. Canadian Blood
Services Operations Division.
Canadian Hemophilia Society. (2005). Report card on Canada’s
blood system 7 years after the Commission of Inquiry on the
blood system in Canada. Blood Safety Committee of the
Canadian Hemophilia Society.
Cashman, N. R. (1999). New variant Creutzfeldt– Jakob disease
and the Canadian blood supply: Scientific basis of risk.
Laboratory Centre for Disease Control.
Conlan, T. J., Riggle, J. D., & Schwartz, D. E. (1995).
Deregulating federalism? The politics of mandate reform in
the 104th Congress. Publius, 25(3), 23–40.
Council of Europe, Expert Committee in Blood Transfusion
Study Group on Pathogen Inactivation of Labile Blood
Components. (2001). Pathogen inactivation of labile blood
products. Transfusion Medicine Reviews, 11(3), 149–175.
ElSaadany, S., & Giulivi, A. (2000). Comprehensive risk assess-
ment for vCJD in France and other countries for Canadians and
the Canadian blood supply. Ottawa: Division of Blood Borne
Pathogens, Health Canada.
Expert Advisory Committee on Blood Regulation. (1998).
Minutes. Item 2. Ottawa: Health Protection Branch, Health
Canada.
FDA. (January 2002). Guidance for industry. In F. a. D. A (Ed.),
Revised preventive measures to reduce the possible risk of
transmission of Creutzfeldt– Jakob disease (CJD) and variant
Creutzfeldt– Jakob disease (vCJD) by blood and blood
products. US Department of Health and Human Services,
Center for Biologics Evaluation and Research (CBER).
Gilmore, N., & Somerville, M.A. (1999). From trust to tragedy:
HIV/AIDS and the Canadian blood system. In B. R.
Feldman, E. A. (Ed.), Blood feuds. Aids, blood and the politics
of medical disaster. Oxford: Oxford University Press.
Goodnough, L. T. (2000). The case against universal WBC
reduction (and for the practice of evidence-based medicine).
Transfusion, 40(12), 1522–1527.
Hogwood, B. W., & Gunn, L. A. (1984). Models of policy
making. In Policy analysis for the real world. Oxford: Oxford
University Press.
IBM Consulting. (2002). Executive summary. In performance
review of Canadian blood services. Final Report.
Jenkins-Smith, H. C., & Sabatier, P. A. (1994). Evaluating the
advocacy coalition framework. Journal of Public Policy, 14,
175–203.
Krever, H. (1997a). The Consequences of the Contamination of
the blood Supply. Chapter 26. In Commission of inquiry on the
blood system in Canada. Final Report. Ottawa: Canadian
Government Publishing.
Krever, H. (1997b). The blood system for the future. Chapter 40.
In Commission of inquiry on the blood system in Canada. Final
Report. Ottawa: Canadian Government Publishing.
Krever, H. (1997c). Canada’s rejection of surrogate testing. In
Commission of inquiry on the blood system in Canada. Final
Report. Ottawa: Canadian Government Publishing.
Laupacis, A., Feeny, D., Detsky, A. S., & Tugwell, P. X. (1992).
How attractive does a new technology have to be to warrant
adoption and utilization? Tentative guidelines for using
clinical and economic evaluations. Canadian Medical Associa-
tion Journal, 146(4), 473–481.
Lee, K. (2001). France acts on threat of BSE transmission by
blood. The French blood transfusion authorities are banning
donors who might have become exposed to BSE in the UK.
The Scientist January 23.
Llewelyn, C. A., Hewitt, P. E., Knight, R. S., Amar, K., Cousens,
S., Mackenzie, J., et al. (2004). Possible transmission of
variant Creutzfeldt–Jakob disease by blood transfusion.
Lancet, 363(9407), 417–421.
Lomas, J. (2000). Connecting research and policy. Canadian
Journal of Policy Research, 140–144.
Medicare Payment Advisory Committee. (2001). Blood safety in
hospitals and medicare inpatient payment. Report to the
Congress.
Morris, J. (2000). Defining the precautionary principle. In J.
Morris (Ed.), Rethinking risk and the precautionary principle.
Oxford: Butterworth-Heinemann.
Orsini, M. (2002). The politics of naming, blaming and claiming:
HIV, Hepatitis C, and the Emergence of Blood Activism in
Canada. Canadian Journal of Political Science, 35(3),
475–491.
Pal, L. A. (1992). Public policy analysis. Scarborough, ON:
Nelson Canada.
Peden, A. H., Head, M. W., Ritchie, D. L., Bell, J. E., & Ironside,
J. W. (2004). Preclinical vCJD after blood transfusion in a
PRNP codon 129 heterozygous patient. Lancet, 364(9433),
527–529.
Picard, A. (1998). The gift of death. Confronting Canada’s tainted-
blood tragedy. Canada: Harper Collins.
Picard, A. (2002). RCMP Lay 32 charges in tainted-blood case.
Globe and Mail November 21, 2002.
Plotkin, S. A. (2001). Lessons learned concerning vaccine safety.
Vaccine, 20(Suppl. 1), S16–S19 discussion S1.
Prusiner, S. B. (1982). Novel proteinaceous infectious particles
cause Scrapie. Science, 216(4542), 136–144.
Sabatier, P. A. (1987). Knowledge, policy-oriented learning, and
policy change. An advocacy coalition framework. Knowledge:
Creation, Diffusion, Utilization, 8, 649–692.
Sabatier, P. A. (1993a). The need for better theories. In Theories
of the policy process. Boulder, CO: Westview Press.
Sabatier, P. A. (1993b). Policy change over a decade or more. In
Policy change and learning. An advocacy coalition approach.
Boulder, CO: Westview Press.
Slovic, P. (1987). Perception of risk. Science, 236(4799), 280–285.
Stoto, M. A. (2002). The precautionary principle and emerging
biological risks: Lessons from swine flu and HIV in blood
products. Public Health Report, 117(6), 546–552.
Upshur, R. E. (2003). Are all evidence-based practices alike?
Problems in the ranking of evidence. Canadian Medical
Association Journal, 169(7), 672–673.
Vaughan, P. (1996). Creutzfeldt–Jakob disease latest unknown in
struggle to restore faith in blood supply. Canadian Medical
Association Journal, 155(5), 565–568.
Weinberg, P. D., Hounshell, J., Sherman, L. A., Godwin, J., Ali,
S., Tomori, C., et al. (2002). Legal, financial, and public
health consequences of HIV contamination of blood and
blood products in the 1980s and 1990s. Annals of Internal
Medicine, 136(4), 312–319.

ARTICLE IN PRESSK. Wilson et al. / Social Science & Medicine 64 (2007) 174–185 185
Will, R. G., Ironside, J. W., Zeidler, M., Cousens, S. N., Estibeiro,
K., Alperovitch, A., et al. (1996). A new variant of Creutz-
feldt–Jakob disease in the UK. Lancet, 347(9006), 921–925.
Wilson, K., Code, C., Dornan, C., Ahmad, N., Hebert, P., &
Graham, I. (2004). The reporting of theoretical health risks by
the media: Canadian newspaper reporting of potential blood
transmission of Creutzfeldt–Jakob disease. BMC Public
Health, 4(1), 1.
Wilson, K., Code, C., & Ricketts, M. N. (2000). Risk of acquiring
Creutzfeldt–Jakob disease from blood transfusions: Systema-
tic review of case-control studies. British Medical Journal j,
321(7252), 17–19.
Wilson, K., & Hebert, P. C. (2003). The challenge of an
increasingly expensive blood system. Canadian Medical
Association Journal, 168(9), 1149–1150.
Wilson, K., Hebert, P. C., Laupacis, A., Dornan, C., Ricketts,
M., Ahmad, N., et al. (2001). A policy analysis of major
decisions relating to Creutzfeldt–Jakob disease and the blood
supply. Canadian Medical Association JournalCmaj, 165(1),
59–65.
Wilson, K., MacDougall, L., Pinard, B., Amin, M. A.,
Fergusson, D., Graham, I., et al. (2003). How should Canada
fund the blood system? An evaluation of the chargeback
proposal. Hospital Quarterly, 6(3), 44–47.
Wilson, K., McCrea-Logie, J., & Lazar, H. (2004). Under-
standing the impact of intergovernmental relations on
public health: Lessons form reform initiatives in the blood
system and health surveillance. Canadian Public Policy, 30,
177–194.
Wilson, K., & Ricketts, M. N. (2004). The success of precaution?
Managing the risk of transfusion transmission of
variant Creutzfeldt–Jakob disease. Transfusion, 44(10),
1475–1478.
Wilson, K., Wilson, M., Hebert, P. C., & Graham, I. (2003). The
application of the precautionary principle to the blood
system: The Canadian blood system’s vCJD donor deferral
policy. Transfusion Medicine Review, 17(2), 89–94.
Wingspread conference participants. (1998). Wingspread state-
ment on the precautionary principle. Paper read at Wingspread
Conference, January 23–25 1998, at Racine, Wisconsin.