Embed Size (px)
Citation preview

The Peripheral Vascular System
C H A P T E R
The Peripheral Vascular System 1414
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 441
Brachial artery
Ulnar artery
Arterial arches
Radial artery
ANATOMY AND PHYSIOLOGY
This chapter focuses on circulationto the arms and legs. It includes thearteries, the veins, the capillary bedthat connects them, and the lym-phatic system with its lymph nodes.
Arteries
Arterial pulses are palpable when anartery lies close to the body surface.In the arms, there are two or some-times three such locations. Pulsa-tions of the brachial artery can befelt in and above the bend of theelbow, just medial to the biceps ten-don and muscle. The brachial arterydivides into the radial and ulnar ar-teries. Radial artery pulsations canbe felt on the flexor surface of thewrist laterally. Medially, pulsationsof the ulnar artery may be palpable,but overlying tissues frequently ob-scure them.
The radial and ulnar arteries are in-terconnected by two vascular archeswithin the hand. Circulation to thehand and fingers is thereby doublyprotected against possible arterialocclusion.

In the legs, arterial pulsations canusually be felt in four places. Thoseof the femoral artery are palpablebelow the inguinal ligament, mid-way between the anterior superioriliac spine and the symphysis pubis.The femoral artery travels down-ward deep within the thigh, passesmedially behind the femur, and be-comes the popliteal artery. Poplitealpulsations can be felt in the tissuesbehind the knee. Below the knee,the popliteal artery divides into twobranches, both of which continueto the foot. There the anterior branchbecomes the dorsalis pedis artery. Itspulsations are palpable on the dor-sum of the foot just lateral to theextensor tendon of the big toe. Theposterior branch, the posterior tib-ial artery, can be felt as it passes be-hind the medial malleolus of theankle.
Like the hand, the foot is protectedby an interconnecting arch betweenits two chief arterial branches.
Veins
The veins from the arms, together with those from the upper trunk and thehead and neck, drain into the superior vena cava and on into the rightatrium. Veins from the legs and the lower trunk drain upward into the in-ferior vena cava. Because the leg veins are especially susceptible to dysfunc-tion, they warrant special attention.
The deep veins of the legs carry about 90% of the venous return from thelower extremities. They are well supported by surrounding tissues.
ANATOMY AND PHYSIOLOGY
442 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Anterior superioriliac spine
Inguinal ligament
Femoral artery
Symphysis pubis
Popliteal artery
Arterial arch
Posterior tibial artery
Dorsalis pedis artery

In contrast, the superficial veins are located subcutaneously, and are sup-ported relatively poorly. The superficial veins include (1) the great saphe-nous vein, which originates on the dorsum of the foot, passes just in frontof the medial malleolus, and then continues up the medial aspect of the legto join the deep venous system (the femoral vein) below the inguinal lig-ament; and (2) the small saphenous vein, which begins at the side of thefoot and passes upward along the back of the leg to join the deep systemin the popliteal space. Anastomotic veins connect the two saphenous veinssuperficially and, when dilated, are readily visible. In addition, communi-cating (or perforating) veins connect the saphenous system with the deepvenous system.
Deep, superficial, and communicating veins all have one-way valves. Theseallow venous blood to flow from the superficial to the deep system and to-ward the heart, but not in the opposite directions. Muscular activity con-tributes importantly to venous blood flow. As calf muscles contract in walk-ing, for example, blood is squeezed upward against gravity, and competentvalves keep it from falling back again.
ANATOMY AND PHYSIOLOGY
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 443
Femoral vein
Great saphenousvein
Small saphenousvein
Femoral vein
Communicatingvein
Small saphenousvein
Great saphenousvein

The Lymphatic System and Lymph Nodes
The lymphatic system comprises an extensive vascular network that drainsfluid, called lymph, from bodily tissues and returns it to the venous circu-lation. The system starts peripherally as blind lymphatic capillaries, andcontinues centrally as thin vascular vessels and then collecting ducts thatfinally empty into major veins at the root of the neck. The lymph trans-ported in these channels is filtered through lymph nodes that are inter-posed along the way.
Lymph nodes are round, oval, or bean-shaped structures that vary in sizeaccording to their location. Some lymph nodes, such as the preauriculars,if palpable at all, are typically very small. The inguinal nodes, in contrast,are relatively larger—often 1 cm in diameter and occasionally even 2 cm inan adult.
In addition to its vascular functions, the lymphatic system plays an impor-tant role in the body’s immune system. Cells within the lymph nodes engulfcellular debris and bacteria and produce antibodies.
Only the superficial lymph nodes are accessible to physical examination.These include the cervical nodes (p. 133), the axillary nodes (p. 300), andnodes in the arms and legs.
ANATOMY AND PHYSIOLOGY
444 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Infraclavicularnode
Centralaxillary nodes
Lateralaxillarynodes
Epitrochlearnodes

ANATOMY AND PHYSIOLOGY
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 445
Femoralvein
Greatsaphenousvein
Verticalgroup
Femoralartery
Horizontalgroup
Recall that the axillary lymph nodes drain most of the arm. Lymphaticsfrom the ulnar surface of the forearm and hand, the little and ring fingers,and the adjacent surface of the middle finger, however, drain first into theepitrochlear nodes. These are located on the medial surface of the arm about3 cm above the elbow. Lymphatics from the rest of the arm drain mostlyinto the axillary nodes. A few may go directly to the infraclaviculars.
The lymphatics of the lower limb,following the venous supply, consistof both deep and superficial systems.Only the superficial nodes are pal-pable. The superficial inguinal nodesinclude two groups. The horizontalgroup lies in a chain high in the ante-rior thigh below the inguinal liga-ment. It drains the superficial portionsof the lower abdomen and buttock,the external genitalia (but not thetestes), the anal canal and perianalarea, and the lower vagina.
The vertical group clusters near theupper part of the saphenous vein anddrains a corresponding region of theleg. In contrast, lymphatics from theportion of leg drained by the smallsaphenous vein (the heel and outeraspect of the foot) join the deep sys-tem at the level of the popliteal space.Lesions in this area, therefore, arenot usually associated with palpableinguinal lymph nodes.
Fluid Exchange and the Capillary Bed
Blood circulates from arteries to veins through the capillary bed. Here fluidsdiffuse across the capillary membrane, maintaining a dynamic equilibrium be-tween the vascular and interstitial spaces. Blood pressure (hydrostatic pressure)within the capillary bed, especially near the arteriolar end, forces fluid out intothe tissue spaces. In effecting this movement, it is aided by the relatively weakosmotic attraction of proteins within the tissues (interstitial colloid oncoticpressure) and is opposed by the hydrostatic pressure of the tissues.
As blood continues through the capillary bed toward the venous end itshydrostatic pressure falls, and another force gains dominance. This is the col-loid oncotic pressure of plasma proteins, which pulls fluid back into the vasculartree. Net flow of fluid, which was directed outward on the arteriolar side ofthe capillary bed, reverses itself and turns inward on the venous side. Lym-phatic capillaries, which also play an important role in this equilibrium, removeexcessive fluid, including protein, from the interstitial space.

THE HEALTH HISTORY
446 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
See Table 14-1, Painful PeripheralVascular Disorders and Their Mimics, pp. 460–461.
Lymphatic dysfunction or disturbances in hydrostatic or osmotic forces canall disrupt this equilibrium. The most common clinical result is the increasedinterstitial fluid known as edema (see Table 14-4, Some Peripheral Causesof Edema, p. 464).
Changes With Aging
Aging itself brings relatively few clinically important changes to the peripheralvascular system. Although arterial and venous disorders, especially athero-sclerosis, do afflict older people more frequently, they probably cannot beconsidered part of the aging process. Age lengthens the arteries, makes themtortuous, and typically stiffens their walls, but these changes develop with orwithout atherosclerosis and therefore lack diagnostic specificity. Loss of arte-rial pulsations is not a part of normal aging, however, and demands carefulevaluation. Skin may get thin and dry with age, nails may grow more slowly,and hair on the legs often becomes scant. Because these changes are com-mon, they are not specific for arterial insufficiency, although they are classi-cally associated with it.
Common or Concerning Symptoms
! Pain in the arms or legs! Intermittent claudication! Cold, numbness, pallor in the legs, hair loss! Color change in fingertips or toes in cold weather! Swelling in calves, legs, or feet! Swelling with redness or tenderness
THE HEALTH HISTORY
To assess possible peripheral vascular disease, begin by asking patients aboutany pain in the arms and legs. Be aware that pain in the extremities may arisefrom the skin, the peripheral vascular system, the musculoskeletal system, orthe nervous system. In addition, visceral pain may be referred to the ex-
Interstitial space
Artery
Capillary bed
Lymphatic vessel
Vein
EXAMPLES OF ABNORMALITIES

tremities, like the pain of myocardial infarction that radiates to the left armor cervical arthritis that radiates to the shoulder.
To elicit symptoms of arterial peripheral vascular disease in the legs, in-quire about intermittent claudication, which is exercise-induced pain thatis absent at rest, makes the patient stop exertion, and remits within about10 minutes. Ask “Have you ever had any pain or cramping in your legs whenyou walk or exercise?” and “How far can you walk without stopping to rest?”Also, “Does the pain get better with rest?” These questions clarify whatmakes the patient stop and how quickly the pain is relieved. Ask also aboutcoldness, numbness, or pallor in the legs or feet or loss of hair over the ante-rior tibial surfaces.
Many patients with arterial peripheral vascular disease have few symptoms,so it is important to identify background risk factors. Assess the patient’s his-tory of tobacco abuse. Ask if the patient has had hypertension, diabetes, orhyperlipidemia. Further, is there any history of myocardial infarction orstroke? Such patients warrant further evaluation, even if without symptomsin the extremities (see p. 448).
To elicit symptoms of arterial spasm in the fingers or toes, ask “Do yourfingertips ever change color in cold weather or when you handle cold ob-jects?” . . . “What color changes do you notice?” . . . “What about your toes?”
There may be symptoms of venous peripheral vascular disease, such asswelling of the feet and legs. Ask about any ulcers on the lower legs, often thenear ankles.
The redness, swelling, and tenderness of local inflammation are seen insome vascular disorders and in other conditions that mimic them. In con-trast, relatively brief leg cramps that commonly occur at night in other-wise healthy people do not indicate a circulatory problem, and cold handsand feet are so common in healthy people that they have relatively littlepredictive value.
THE HEALTH HISTORY
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 447
Atherosclerosis can cause sympto-matic limb ischemia with exertion;distinguish this from spinal stenosis,which produces leg pain with exertion that may be reduced byleaning forward (stretching thespinal cord in the narrowed verte-bral canal) and less readily relievedby rest.
Hair loss over the anterior tibiae indecreased arterial perfusion. “Dry”or brown-black ulcers from gan-grene may ensue.
Only about 10% of affected pa-tients have the classic symptoms ofexertional calf pain relieved by rest.
Digital ischemic changes ofblanching, followed by cyanosis,then rubor with cold exposure and rewarming in Raynaud’s phenomenon or disease
Hyperpigmentation, edema, andpossible cyanosis, especially whenlegs are dependent, in venous stasisulcers
Inflammation in cellulitis, superficialthrombophlebitis, and erythema nodosum
Etiology of common leg crampsand “restless legs” not well under-stood. Leg cramps sometimes fromdiuretic use with hypokalemia
EXAMPLES OF ABNORMALITIES

HEALTH PROMOTION AND COUNSELING
448 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
*Hirsh AT, Criqui MH, Treat-Jacobson D, et al: Peripheral Arterial Disease: Detection, Awareness,and Treatment in Primary Care. JAMA 286 (11):1317–1324, 2001; Hiatt WR: Medical Treatment of Peripheral Arterial Disease and Claudication. NEJM 344 (21):1608–1620, 2001.
HEALTH PROMOTION AND COUNSELING
Important Topics for Health Promotion and Counseling
! Detection of peripheral arterial disease (PAD)! Risk factors for PAD! Screening for PAD: the ankle–brachial index (ABI)
Peripheral arterial disease (PAD) generally refers to atherosclerotic occlusionof arteries in the lower extremities. The femoral and popliteal arteries are in-volved most commonly, followed by the tibial and peroneal arteries. PADaffects from 12% to 25% of community populations; however, recent stud-ies* have shown that despite significant associations with cardiovascular andcerebrovascular disease, PAD often is underdiagnosed in office practices.Most patients with PAD have either no symptoms or a range of nonspecificleg symptoms, such as aching, cramping, numbness, or fatigue. The classictriad for vascular claudication, exercise-induced calf pain that causes stop-ping of exercise and results in relief of pain in 10 minutes or less, may bepresent in only about 10% of affected patients.*
Patients with current or past tobacco use, diabetes, hypertension, hyper-lipidemia, or cardiovascular or cerebrovascular disease are at increased riskof atherosclerotic PAD. Such patients should be screened for subclinical PADand targeted for aggressive risk factor intervention. For screening, cliniciansshould consider use of the ankle–brachial index (ABI), a highly accurate testfor detecting 50% or greater stenoses of 50% or more in major vessels of thelegs. The ABI is readily performed by clinicians or office staff, and consists ofmeasuring the systolic blood pressure with Doppler ultrasonography in eacharm and in the dorsalis pedis and posterior tibial pulses. The ABI is calcu-lated on both the right and left by dividing the higher right ankle pressureby the higher right arm pressure, and the higher left ankle pressure by thehigher left arm pressure. ABI values are as follows: 0.90–1.30 is considerednormal; 0.41–0.90—mild to moderate peripheral arterial disease, usuallywith symptoms of claudication; and 0.00–0.40—severe peripheral vasculardisease with critical leg ischemia.
The severity of peripheral vascular disease closely parallels the risk of myo-cardial infarction, ischemic stroke, and death from vascular causes. Patientswith ABIs in the lowest category have a 20% to 25% annual risk of death.*A wide range of interventions is available to reduce both onset and progres-

HEALTH PROMOTION AND COUNSELING
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 449
Suggests atherosclerotic peripheralarterial disease
Preview: Recording the Physical Examination—The Peripheral Vascular System
Note that initially you may use sentences to describe your findings; lateryou will use phrases. The style below contains phrases appropriate formost write-ups. Unfamiliar terms are explained in the next section, Techniques of Examination. Recall that the written description of lymphnodes appears after the Head and Neck section (see p.143). Likewise, assessment of the carotid pulse is recorded in the Cardiovascular section(see p. 265).
“Extremities are warm and without edema. No varicosities or stasischanges. Calves are supple and nontender. No femoral or abdominalbruits. Brachial, radial, femoral, popliteal, dorsalis pedis (DP), and posterior tibial (PT) pulses are 2+ and symmetric.”
OR
“Extremities are pale below the midcalf, with notable hair loss. Rubornoted when legs dependent but no edema or ulceration. Bilateral femoralbruits; no abdominal bruits heard. Brachial and radial pulses 2+; femoral,popliteal, DP and PT pulses 1+.” (Alternatively, pulses can be recorded asbelow.)
Dorsalis PosteriorRadial Brachial Femoral Popliteal Pedis Tibial
RT 2+ 2+ 1+ 1+ 1+ 1+LT 2+ 2+ 1+ 1+ 1+ 1+
sion of subclinical PAD, including meticulous foot care and well-fittingshoes, tobacco cessation, treatment of hyperlipidemia, optimal control andtreatment of diabetes and hypertension, use of antiplatelet agents, and, ifneeded, surgical revascularization.
(Students should consult specialty texts for less common forms of vascularocclusion from arterial or venous thrombosis or endarteritis from infection,inflammation, or autoimmune disease.)
EXAMPLES OF ABNORMALITIES

TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
450 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Lymphedema of arm and handmay follow axillary node dissectionand radiation therapy.
Prominent veins in an edematousarm suggest venous obstruction.
(Source of photo above: Marks R: SkinDisease in Old Age. Philadelphia, JBLippincott, 1987)
In Raynaud’s disease, wrist pulsesare typically normal but spasm ofmore distal arteries causes episodes
Important Areas of Examination
The Arms! Size, symmetry, skin color! Radial pulse, brachial pulse! Epitrochlear lymph nodes
TECHNIQUES OF EXAMINATION
Assessment of the peripheral vascular system relies primarily on inspection ofthe arms and legs, palpation of the pulses, and a search for edema. See Chap-ter 3 for a method of integrating these techniques into your examination of thelimbs. Additional techniques may be useful when you suspect an abnormality.
Arms
Inspect both arms from the fingertips to the shoulders. Note:
! Their size, symmetry, and any swelling
! The venous pattern
! The color of the skin and nail beds and the texture of the skin
Palpate the radial pulse with the padsof your fingers on the flexor surfaceof the wrist laterally. Partially flexingthe patient’s wrist may help you feelthis pulse. Compare the pulses inboth arms.
The Legs! Size, symmetry, skin color! Femoral pulse and inguinal
lymph nodes! Popliteal, dorsalis pedis, and
posterior tibial pulses! Peripheral edema

EXAMPLES OF ABNORMALITIES
There are several systems for grading the amplitude of the arterial pulses.One system is to use a scale of 0 to 4, as below; however, you should checkto see what scale is used in your institution.
TECHNIQUES OF EXAMINATION
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 451
of sharply demarcated pallor of thefingers (see Table 14-1, Painful Peripheral Vascular Disorders andTheir Mimics, pp. 460–461).
Note that if an artery is widely di-lated, it is aneurysmal.
Bounding carotid, radial, andfemoral pulses in aortic insuffi-ciency; asymmetric diminishedpulses in arterial occlusion fromatherosclerosis or embolism
An enlarged epitrochlear nodemay be secondary to a lesion in its drainage area or may be associated with generalized lymphadenopathy.
4+ Bounding3+ Increased2+ Brisk, expected1+ Diminished, weaker than expected0 Absent, unable to palpate
If you suspect arterial insufficiency,feel for the brachial pulse. Flex thepatient’s elbow slightly, and with thethumb of your opposite hand palpatethe artery just medial to the bicepstendon at the antecubital crease. Thebrachial artery can also be felt higherin the arm in the groove between thebiceps and triceps muscles.
Feel for one or more epitrochlearnodes. With the patient’s elbow flexedto about 90° and the forearm sup-ported by your hand, reach aroundbehind the arm and feel in the groovebetween the biceps and triceps mus-cles, about 3 cm above the medialepicondyle. If a node is present, noteits size, consistency, and tenderness.
Epitrochlear nodes are difficult orimpossible to identify in most nor-mal people.
Legs
The patient should be lying down and draped so that the external genitaliaare covered and the legs fully exposed. A good examination is impossiblethrough stockings or socks!
Medial aspect of left arm
Right hand of examinerMedial epicondyle of humerus

Inspect both legs from the groin and buttocks to the feet. Note:
! Their size, symmetry, and anyswelling
! The venous pattern and anyvenous enlargement
! Any pigmentation, rashes,scars, or ulcers
! The color and texture of theskin, the color of the nailbeds, and the distribution ofhair on the lower legs, feet,and toes.
Palpate the superficial inguinalnodes, including both the hori-zontal and the vertical groups.Note their size, consistency, anddiscreteness, and note any ten-derness. Nontender, discrete in-guinal nodes up to 1 cm or even2 cm in diameter are frequentlypalpable in normal people.
Palpate the pulses in order to assess the arterial circulation.
! The femoral pulse. Press deeply, below the inguinal ligament and aboutmidway between the anterior superior iliac spine and the symphysis pubis.As in deep abdominal palpation, the use of two hands, one on top of theother, may facilitate this examination, especially in obese patients.
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
452 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Verticalgroup
Greatsaphenousvein
Femoral vein
Femoral arteryHorizontalgroup
See Table 14-2, Chronic Insuffi-ciency of Arteries and Veins (p. 462).
See Table 14-3, Common Ulcers ofthe Feet and Ankles (p. 463).
Lymphadenopathy refers to enlarge-ment of the nodes, with or withouttenderness. Try to distinguish be-tween local and generalized lym-phadenopathy, respectively, byfinding either (1) a causative lesionin the drainage area, or (2) enlargednodes in at least two other non-contiguous lymph node regions.
A diminished or absent pulse indi-cates partial or complete occlusionproximally; for example, at theaortic or iliac level, all pulses distalto the occlusion are typically affected. Chronic arterial occlusion,usually from atherosclerosis,causes intermittent claudication,(pp. 460–461), postural colorchanges (p. 458), and trophicchanges in the skin (p. 462)
An exaggerated, widened femoralpulse suggests a femoral aneurysm,a pathologic dilatation of the artery.

EXAMPLES OF ABNORMALITIES
! The popliteal pulse. The patient’s knee should be somewhat flexed, the legrelaxed. Place the fingertips of both hands so that they just meet in themidline behind the knee and press them deeply into the popliteal fossa.The popliteal pulse is often more difficult to find than other pulses. It isdeeper and feels more diffuse.
TECHNIQUES OF EXAMINATION
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 453
An exaggerated, widened poplitealpulse suggests an aneurysm of thepopliteal artery. Neither poplitealnor femoral aneurysms are com-mon. They are usually due to atherosclerosis, and occur primarilyin men over age 50.
Atherosclerosis (arteriosclerosisobliterans) most commonly ob-structs arterial circulation in thethigh. The femoral pulse is thennormal, the popliteal decreased or absent.
If you cannot feel the popliteal pulse with this approach, try with the patientprone. Flex the patient’s knee to about 90°, let the lower leg relax againstyour shoulder or upper arm, and press your two thumbs deeply into thepopliteal fossa.

! The dorsalis pedis pulse. Feel thedorsum of the foot (not the ankle)just lateral to the extensor tendonof the great toe. If you cannot feela pulse, explore the dorsum of thefoot more laterally.
! The posterior tibial pulse. Curveyour fingers behind and slightlybelow the medial malleolus of theankle. (This pulse may be hard tofeel in a fat or edematous ankle.)
Tips on feeling difficult pulses: (1) Position your own body and examininghand comfortably; awkward positions decrease your tactile sensitivity. (2) Place your hand properly and linger there, varying the pressure of yourfingers to pick up a weak pulsation. If unsuccessful, then explore the area de-liberately. (3) Do not confuse the patient’s pulse with your own pulsatingfingertips. If you are unsure, count your own heart rate and compare it withthe patient’s. The rates are usually different. Your carotid pulse is convenientfor this comparison.
Note the temperature of the feet and legs with the backs of your fingers. Com-pare one side with the other. Bilateral coldness is most often due to a coldenvironment or anxiety.
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
454 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
The dorsalis pedis artery may becongenitally absent or may branchhigher in the ankle. Search for apulse more laterally.
Decreased or absent foot pulses (assuming a warm environ-ment) with normal femoral and popliteal pulses suggest occlusive disease in the lowerpopliteal artery or its branches—a pattern often associated with diabetes mellitus.
Sudden arterial occlusion, as by em-bolism or thrombosis, causes painand numbness or tingling. The limbdistal to the occlusion becomescold, pale, and pulseless. Emergencytreatment is required. If collateralcirculation is good, only numbnessand coolness may result.
Coldness, especially when uni-lateral or associated with othersigns, suggests arterial insuffi-ciency from inadequate arterialcirculation.
EXAMPLES OF ABNORMALITIESTECHNIQUES OF EXAMINATION
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 455
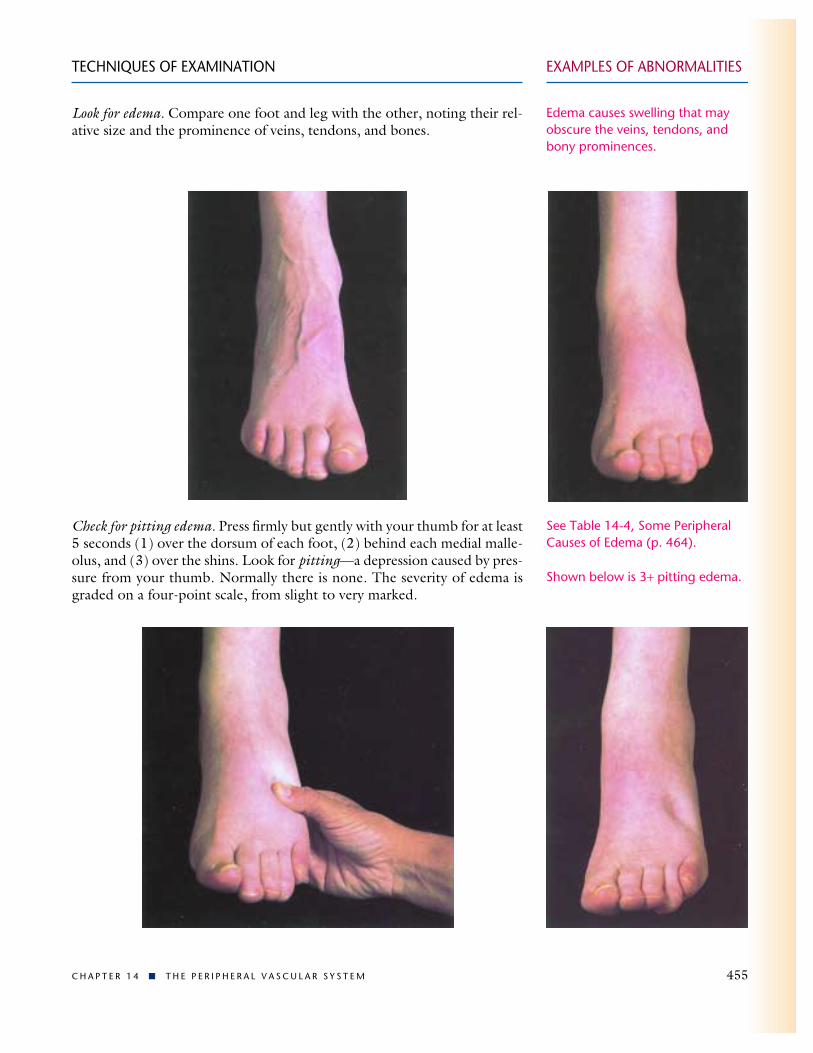
Look for edema. Compare one foot and leg with the other, noting their rel-ative size and the prominence of veins, tendons, and bones.
Check for pitting edema. Press firmly but gently with your thumb for at least5 seconds (1) over the dorsum of each foot, (2) behind each medial malle-olus, and (3) over the shins. Look for pitting—a depression caused by pres-sure from your thumb. Normally there is none. The severity of edema isgraded on a four-point scale, from slight to very marked.
Edema causes swelling that mayobscure the veins, tendons, andbony prominences.
See Table 14-4, Some PeripheralCauses of Edema (p. 464).
Shown below is 3+ pitting edema.
If you suspect edema, measurement of the legs may help you to identify it andto follow its course. With a flexible tape, measure (1) the forefoot, (2) thesmallest possible circumference above the ankle, (3) the largest circumfer-ence at the calf, and (4) the midthigh a measured distance above the patellawith the knee extended. Compare one side with the other. A difference ofmore than 1 cm just above the ankle or 2 cm at the calf is unusual in normalpeople and suggests edema.
If edema is present, look for possible causes in the peripheral vascular sys-tem. These include (1) recent deep venous thrombosis, (2) chronic venousinsufficiency due to previous deep venous thrombosis or to incompetenceof the venous valves, and (3) lymphedema. Note the extent of the swelling.How far up the leg does it go?
Is the swelling unilateral or bilateral? Are the veins unusually prominent?
Try to identify any venous tenderness that may accompany deep venousthrombosis. Palpate the groin just medial to the femoral pulse for tender-ness of the femoral vein. Next, with the patient’s leg flexed at the knee andrelaxed, palpate the calf. With your fingerpads, gently compress the calf mus-cles against the tibia, and search for any tenderness or cords. Deep venousthrombosis, however, may have no demonstrable signs, and diagnosis oftendepends on high clinical suspicion and other testing.
Note the color of the skin.
! Is there a local area of redness? If so, note its temperature, and gently tryto feel the firm cord of a thrombosed vein in the area. The calf is mostoften involved.
! Are there brownish areas near the ankles?
! Note any ulcers in the skin. Where are they?
! Feel the thickness of the skin.
Ask the patient to stand, and inspect the saphenous system for varicosities. Thestanding posture allows any varicosities to fill with blood and makes themvisible. You can easily miss them when the patient is in a supine position.Feel for any varicosities, noting any signs of thrombophlebitis.
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
456 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
Conditions such as muscular atrophy can also cause differentcircumferences in the legs.
In deep venous thrombosis, the extent of edema suggests the location of the occlusion: the calfwhen the lower leg or the ankle isswollen, the iliofemoral veins whenthe entire leg is swollen.
Venous distention suggests a venouscause of edema.
A painful, pale swollen leg, togetherwith tenderness in the groin overthe femoral vein, suggests deepiliofemoral thrombosis. Approxi-mately half of patients with deepvenous thrombosis in the calf havetenderness and cords deep in thecalf. Calf tenderness is nonspecific,however, and may be presentwithout thrombosis.
Local swelling, redness, warmth,and a subcutaneous cord suggestsuperficial thrombophlebitis.
A brownish color or ulcers justabove the ankle suggest chronicvenous insufficiency.
Thickened brawny skin occurs in lymphedema and advanced venous insufficiency.
Varicose veins are dilated and tor-tuous. Their walls may feel some-what thickened. Many varicoseveins can be seen in the leg on p. 459.

Release your pressure over the ulnar artery. If the ulnar artery is patent, thepalm flushes within about 3 to 5 seconds.
Patency of the radial artery may betested by releasing the radial arterywhile still compressing the ulnar.
EXAMPLES OF ABNORMALITIES
Special Techniques
Evaluating the Arterial Supplyto the Hand. If you suspect arte-rial insufficiency in the arm or hand,try to feel the ulnar pulse as well asthe radial and brachial pulses. Feelfor it deeply on the flexor surface ofthe wrist medially. Partially flexingthe patient’s wrist may help you. Thepulse of a normal ulnar artery, how-ever, may not be palpable.
The Allen test gives further information. This test is also useful to assure thepatency of the ulnar artery before puncturing the radial artery for blood sam-ples. The patient should rest with hands in lap, palms up.
Ask the patient to make a tight fist with one hand; then compress both ra-dial and ulnar arteries firmly between your thumbs and fingers. Next, askthe patient to open the hand into a relaxed, slightly flexed position. Thepalm is pale.
TECHNIQUES OF EXAMINATION
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 457
Arterial occlusive disease is muchless common in the arms than inthe legs. Absent or diminishedpulses at the wrist in acute embolicocclusion and in Buerger’s disease,or thromboangiitis obliterans.
Extending the hand fully maycause pallor and a falsely positivetest.
Persisting pallor indicates occlusionof the ulnar artery or its distalbranches.

Postural Color Changes ofChronic Arterial Insufficiency.If pain or diminished pulses suggestarterial insufficiency, look for pos-tural color changes. Raise both legs,as shown at the right, to about 60° until maximal pallor of the feet develops—usually within a minute.In light-skinned persons, either main-tenance of normal color, as seen inthis right foot, or slight pallor isnormal.
Then ask the patient to sit up withlegs dangling down. Compare bothfeet, noting the time required for:
! Return of pinkness to the skin, nor-mally about 10 seconds or less
! Filling of the veins of the feet andankles, normally about 15 seconds.
This right foot has normal color andthe veins on the foot have filled.These normal responses suggest anadequate circulation.
Look for any unusual rubor (dusky redness) to replace the pallor of the de-pendent foot. Rubor may take a minute or more to appear.
Normal responses accompanied by diminished arterial pulses suggest that agood collateral circulation has developed around an arterial occlusion.
Color changes may be difficult to see in darker-skinned persons. Inspectthe soles of the feet for these changes, and use tangential lighting to seethe veins.
TECHNIQUES OF EXAMINATION EXAMPLES OF ABNORMALITIES
458 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
The foot below is still pale and theveins are just starting to fill—signsof arterial insufficiency.
Persisting rubor on dependencysuggests arterial insufficiency (seep. 462). When veins are incompe-tent, dependent rubor and thetiming of color return and venousfilling are not reliable tests of arte-rial insufficiency.
Marked pallor on elevation sug-gests arterial insufficiency.
(Source of foot photos: Kappert A, Winsor T: Diagnosis of Peripheral Vascular Disease. Philadelphia, FADavis, 1972).

EXAMPLES OF ABNORMALITIES
Mapping Varicose Veins. Youcan map out the course and connec-tions of varicose veins by transmit-ting pressure waves along the blood-filled veins. With the patient standing,place your palpating fingers gentlyon a vein and, with your other handbelow it, compress the vein sharply.Feel for a pressure wave transmittedto the fingers of your upper hand.A palpable pressure wave indicatesthat the two parts of the vein areconnected.
A wave may also be transmitteddownward, but not as easily.
Evaluating the Competency of Venous Valves. By the retrogradefilling (Trendelenburg) test, you can assess the valvular competency in boththe communicating veins and the saphenous system. Start with the patientsupine. Elevate one leg to about 90° to empty it of venous blood.
Next, occlude the great saphenous vein in the upper thigh by manual com-pression, using enough pressure to occlude this vein but not the deeper ves-sels. Ask the patient to stand. While you keep the vein occluded, watch forvenous filling in the leg. Normally the saphenous vein fills from below,taking about 35 seconds as blood flows through the capillary bed into thevenous system.
After the patient has stood for 20 seconds, release the compression and lookfor any sudden additional venous filling. Normally there is none: competentvalves in the saphenous vein block retrograde flow. Slow venous filling continues.
When both steps of this test are normal, the response is termed negative–negative. Negative–positive and positive–negative responses may also occur.
TECHNIQUES OF EXAMINATION
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 459
Rapid filling of the superficialveins while the saphenous vein isoccluded indicates incompetentvalves in the communicating veins.Blood flows quickly in a retrogradedirection from the deep to thesaphenous system.
Sudden additional filling of super-ficial veins after release of compres-sion indicates incompetent valvesin the saphenous vein.
When both steps are abnormal,the test is positive–positive.
Feel for apressure wave
Compress sharply

TABLE 14-1 ! Painful Peripheral Vascular Disorders and Their Mimics
460 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABLE 14-1 ! Painful Peripheral Vascular Disorders and Their Mimics
Problem Process Location of Pain
Arterial DisordersAtherosclerosis(arteriosclerosis obliterans)! Intermittent claudication
! Rest pain
Acute Arterial Occlusion
Raynaud’s Disease and Phenomenon
Venous DisordersSuperficial Thrombophlebitis
Deep Venous Thrombosis
Chronic Venous Insufficiency (deep)ThromboangiitisObliterans (Buerger’sdisease)
Acute Lymphangitis
Mimics*Acute Cellulitis
Erythema Nodosum
Episodic muscular ischemia induced by exercise,due to obstruction of large or middle-sized arteriesby atherosclerosis
Ischemia even at rest
Embolism or thrombosis, possibly superimposedon arteriosclerosis obliterans
Raynaud’s disease: Episodic spasm of the smallarteries and arterioles; no vascular occlusion.Raynaud’s phenomenon: Syndrome is secondary toother conditions such as collagen vascular disease,arterial occlusion, trauma, drugs
Clot formation and acute inflammation in asuperficial vein
Clot formation in a deep vein
Chronic venous engorgement secondary to venousocclusion or incompetency of venous valves
Inflammatory and thrombotic occlusions of smallarteries and also of veins, occurring in smokers
Acute bacterial infection (usually streptococcal)spreading up the lymphatic channels from a portalof entry such as an injured area or an ulcer
Acute bacterial infection of the skin andsubcutaneous tissues
Subcutaneous inflammatory lesions associated witha variety of systemic conditions such as pregnancy,sarcoidosis, tuberculosis, and streptococcal infections
Usually the calf, but also may be in thebuttock, hip, thigh, or foot, depending onthe level of obstruction
Distal pain, in the toes or forefoot
Distal pain, usually involving the foot and leg
Distal portions of one or more fingers.Pain is usually not prominent unlessfingertip ulcers develop. Numbness andtingling are common.
Pain in a local area along the course of asuperficial vein, most often in thesaphenous system
Pain, if present, is usually in the calf, butthe process more often is painless.
Diffuse aching of the leg(s)
! Intermittent claudication, particularly inthe arch of the foot
! Rest pain in the fingers or toes
An arm or a leg
Arms, legs, or elsewhere
Anterior surfaces of both lower legs
* Mistaken primarily for acute superficial thrombophlebitis.

TABLE 14-1 ! Painful Peripheral Vascular Disorders and Their Mimics
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 461
Factors ThatTiming Aggravate Factors That Relieve Associated Manifestations
Fairly brief; pain usuallyforces the patient to rest.
Persistent, often worse atnight
Sudden onset; associatedsymptoms may occurwithout pain.
Relatively brief (minutes)but recurrent
An acute episode lastingdays or longer
Often hard to determinebecause of lack ofsymptoms
Chronic, increasing as theday wears on! Fairly brief but recurrent! Chronic, persistent, may
be worse at night
An acute episode lastingdays or longer
An acute episode lastingdays or longer
Pain associated with a seriesof lesions over several weeks
Exercise such as walking
Elevation of the feet, as in bed
Exposure to cold,emotional upset
Prolonged standing
! Exercise
Rest usually stops the painin 1–3 min.
Sitting with legs dependent
Warm environment
Elevation of the leg(s)
! Rest! Permanent cessation of
smoking helps both kindsof pain (but patientsseldom stop)
Local fatigue, numbness, diminishedpulses, often signs of arterialinsufficiency (see p. 462)
Numbness, tingling, trophic signs andcolor changes of arterial insufficiency(see p. 462)
Coldness, numbness, weakness,absent distal pulses
Color changes in the distal fingers:severe pallor (essential for thediagnosis) followed by cyanosis andthen redness
Local redness, swelling, tenderness, a palpable cord, possibly fever
Possibly swelling of the foot and calfand local calf tenderness; oftennothing
Chronic edema, pigmentation,possibly ulceration (see pp. 462, 463)
Distal coldness, sweating, numbness,and cyanosis; ulceration and gangreneat the tips of fingers or toes;migratory thrombophlebitis
Red streak(s) on the skin, withtenderness, enlarged, tender lymphnodes, and fever
A local area of diffuse swelling,redness, and tenderness withenlarged, tender lymph nodes andfever; no palpable cord
Raised, red, tender swellings recurringin crops; often malaise, joint pains,and fever
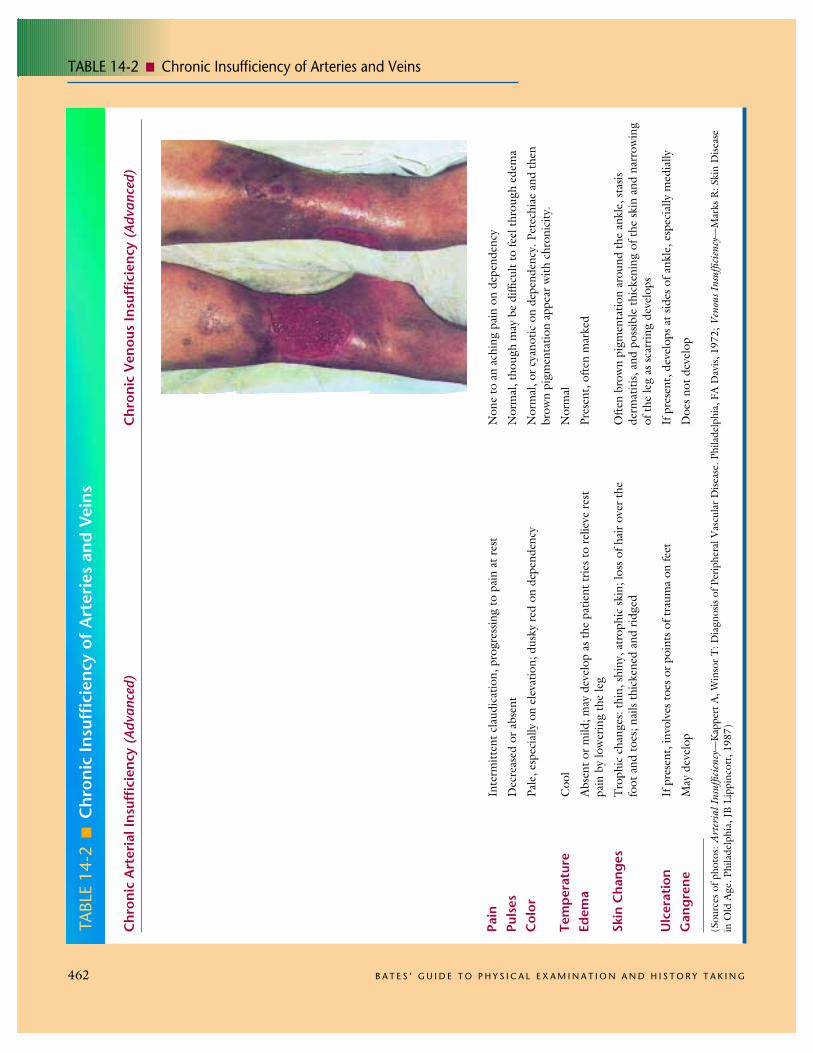
TABLE 14-2 ! Chronic Insufficiency of Arteries and Veins
462 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABL
E 14
-2!
Chr
onic
Insu
ffici
ency
of
Art
erie
s an
d Ve
ins
Chr
onic
Art
eria
l Ins
uffic
ienc
y (A
dvan
ced)
Chr
onic
Ven
ous
Insu
ffici
ency
(Ad
vanc
ed)
Pain
Puls
esC
olor
Tem
pera
ture
Edem
a
Skin
Cha
nges
Ulc
erat
ion
Gan
gren
e
Inte
rmitt
ent c
laud
icat
ion,
pro
gres
sing
to p
ain
at re
st
Dec
reas
ed o
r abs
ent
Pale
, esp
ecia
lly o
n el
evat
ion;
dus
ky re
d on
dep
ende
ncy
Coo
l
Abs
ent o
r mild
; may
dev
elop
as t
he p
atie
nt tr
ies t
o re
lieve
rest
pain
by
low
erin
g th
e le
g
Tro
phic
cha
nges
: thi
n, sh
iny,
atr
ophi
c sk
in; l
oss o
f hai
r ove
r the
foot
and
toes
; nai
ls th
icke
ned
and
ridge
d
If p
rese
nt, i
nvol
ves t
oes o
r poi
nts o
f tra
uma
on fe
et
May
dev
elop
Non
e to
an
achi
ng p
ain
on d
epen
denc
y
Nor
mal
, tho
ugh
may
be
diffi
cult
to fe
el th
roug
h ed
ema
Nor
mal
, or c
yano
tic o
n de
pend
ency
. Pet
echi
ae a
nd th
enbr
own
pigm
enta
tion
appe
ar w
ith c
hron
icity
.
Nor
mal
Pres
ent,
ofte
n m
arke
d
Ofte
n br
own
pigm
enta
tion
arou
nd th
e an
kle,
stas
isde
rmat
itis,
and
poss
ible
thic
keni
ng o
f the
skin
and
nar
row
ing
of th
e le
g as
scar
ring
deve
lops
If p
rese
nt, d
evel
ops a
t sid
es o
f ank
le, e
spec
ially
med
ially
Doe
s not
dev
elop
(Sou
rces
of p
hoto
s: A
rter
ial I
nsuf
ficie
ncy—
Kap
pert
A, W
inso
r T: D
iagn
osis
of P
erip
hera
l Vas
cula
r Dise
ase.
Phi
lade
lphi
a, F
A D
avis,
197
2; V
enou
s Ins
uffic
ienc
y—M
arks
R: S
kin
Dise
ase
in O
ld A
ge. P
hila
delp
hia,
JB
Lip
pinc
ott,
1987
)

TABLE 14-3 ! Common Ulcers of the Feet and Ankles
C H A P T E R 1 4 ! T H E P E R I P H E R A L V A S C U L A R S Y S T E M 463
TABL
E 14
-3!
Com
mon
Ulc
ers
of t
he F
eet
and
Ank
les
Art
eria
l Ins
uffic
ienc
yC
hron
ic V
enou
s In
suffi
cien
cyN
euro
path
ic U
lcer
Loca
tion
Skin
Aro
und
the
Ulc
erPa
in
Ass
ocia
ted
Gan
gren
eA
ssoc
iate
dSi
gns
Toe
s, fe
et, o
r pos
sibly
in a
reas
of
trau
ma
(e.g
., th
e sh
in)
No
callu
s or e
xces
s of p
igm
ent;
may
be a
trop
hic
Ofte
n se
vere
, unl
ess n
euro
path
ym
asks
it
May
be
pres
ent
Dec
reas
ed p
ulse
s, tr
ophi
c ch
ange
s,pa
llor o
f the
foot
on
elev
atio
n, d
usky
rubo
r on
depe
nden
cy
Inne
r or s
omet
imes
out
er a
nkle
Pigm
ente
d, so
met
imes
fibr
otic
Not
seve
re
Abs
ent
Ede
ma,
pig
men
tatio
n, st
asis
derm
atiti
s, an
d po
ssib
ly c
yano
sis o
fth
e fo
ot o
n de
pend
ency
Pres
sure
poi
nts i
n ar
eas w
ithdi
min
ished
sens
atio
n, a
s in
diab
etic
poly
neur
opat
hy
Cal
lous
ed
Abs
ent (
and
ther
efor
e th
e ul
cer m
aygo
unn
otic
ed)
In u
ncom
plic
ated
neu
ropa
thic
ulc
er,
abse
nt
Dec
reas
ed se
nsat
ion,
abs
ent a
nkle
jerk
s
(Sou
rce
of p
hoto
s: M
arks
R: S
kin
Dise
ase
in O
ld A
ge. P
hila
delp
hia,
JB
Lip
pinc
ott,
1987
)

TABLE 14-4 ! Some Peripheral Causes of Edema
464 B A T E S ’ G U I D E T O P H Y S I C A L E X A M I N A T I O N A N D H I S T O R Y T A K I N G
TABL
E 14
-4!
Som
e Pe
riph
eral
Cau
ses
of E
dem
a
Abo
ut o
ne t
hird
of t
otal
bod
y w
ater
is e
xtra
cellu
lar,
or o
utsid
e th
e bo
dy’s
cel
ls.A
bout
25%
of e
xtra
cellu
lar fl
uid
is pl
asm
a an
d th
e re
mai
nder
is in
ters
titia
l flui
d. A
tth
e ar
terio
lar e
nd o
f the
cap
illar
ies,
hydr
osta
tic p
ressu
rein
the
bloo
d ve
ssel
s and
the
collo
id o
ncot
ic p
ressu
rein
the
inte
rstit
ium
cau
se fl
uid
to m
ove
into
the
tiss
ues;
atth
e ve
nous
end
of t
he c
apill
arie
s and
in th
e ly
mph
atic
s, hy
dros
tatic
pre
ssur
e in
the
inte
rstit
ium
and
the
collo
id o
ncot
ic p
ress
ure
of p
lasm
a pr
otei
ns c
ause
flui
d to
re-
turn
to th
e va
scul
ar c
ompa
rtm
ent.
A n
umbe
r of c
linic
al c
ondi
tions
disr
upt t
his b
al-
ance
, res
ultin
g in
ede
ma,
or a
clin
ical
ly e
vide
nt a
ccum
ulat
ion
of in
ters
titia
l flui
d.N
ot d
epic
ted
belo
w is
cap
illar
y le
ak sy
ndro
me,
whe
re p
rote
in le
aks i
nto
the
inte
r-st
itial
spac
e, se
en in
bur
ns, a
ngio
edem
a, sn
ake
bite
s, an
d al
lerg
ic re
actio
ns.
Chr
onic
Ven
ous
Pitt
ing
Edem
aIn
suffi
cien
cyLy
mph
edem
a
Nat
ure
of E
dem
a
Skin
Thi
cken
ing
Ulc
erat
ion
Pigm
enta
tion
Edem
a of
Foo
tBi
late
ralit
yEx
ampl
es/
Mec
hani
sms
Soft,
pits
on
pres
sure
Abs
ent
Abs
ent
Abs
ent
Pres
ent
Alw
ays
!In
ters
titia
l flui
d fro
m: l
egs d
epen
dent
from
pro
long
ed st
andi
ng o
r sitt
ing
"!
hydr
osta
tic p
ress
ure
in v
eins
, cap
illar
ies;
cong
estiv
e he
art f
ailu
re "
#ca
rdia
cou
tput
, !hy
dros
tatic
pre
ssur
e in
vei
ns,
capi
llarie
s; ne
phro
tic sy
ndro
me,
cirr
hosis
,m
alnu
triti
on "
low
alb
umin
, #in
tra-
vasc
ular
col
loid
onc
otic
pre
ssur
e; d
rugs
Soft,
pits
on
pres
sure
; lat
er m
ay b
ecom
ebr
awny
(ha
rd)
May
be
pres
ent,
espe
cial
ly n
ear a
nkle
Com
mon
Com
mon
Ofte
n pr
esen
t
Occ
asio
nally
Chr
onic
obs
truc
tion
or v
alvu
lar
inco
mpe
tenc
e of
the
deep
vei
ns
Soft
in e
arly
stag
es, t
hen
beco
mes
indu
rate
d, h
ard,
non
pitt
ing
Bec
omes
mar
ked
Rar
e
Abs
ent
Pres
ent,
incl
udin
g to
es
Ofte
n
Lym
ph c
hann
els o
bstr
ucte
d by
tum
or,
fibro
sis, i
nflam
mat
ion;
also
from
axi
llary
node
diss
ectio
n, ra
diat
ion
Pitt
ing
Sw
olle
n fo
otA
dvan
ced
Pitt
ing
Pig
men
t
Ulc
er
No
pitti
ng
Ski
n th
ick F
oot s
wol
len