Embed Size (px)
Citation preview

VasculitidesVasculitides
Premchand Anne, MD, MPHPremchand Anne, MD, MPH
PGY II (aka the class that PGY II (aka the class that rocks)rocks)
Internal Medicine/PediatricsInternal Medicine/Pediatrics
ObjectivesObjectives
basic principles of vasculitisbasic principles of vasculitis cases/discussion/didacticcases/discussion/didactic questionsquestions

VasculitisVasculitis
Inflammation of blood vessels and Inflammation of blood vessels and its consequencesits consequences
Classification Classification Pathology of vasculitisPathology of vasculitis
– Role of Immune complexes, Role of Immune complexes, complement, in vasculitiscomplement, in vasculitis
Presentation: purpura vs. nodulePresentation: purpura vs. nodule

Doctor, Doctor, my son Doctor, Doctor, my son has a rash for three days.has a rash for three days.
8 year old male who is very active in sports, presents with 8 year old male who is very active in sports, presents with complaints of rash and swelling of the feet and ankles. Pt’s complaints of rash and swelling of the feet and ankles. Pt’s mother noticed a progressive bumpy red rash and the mother noticed a progressive bumpy red rash and the swelling over the past three days. Rash is also present on swelling over the past three days. Rash is also present on buttocks bilaterally and onset similar to that of the feet. buttocks bilaterally and onset similar to that of the feet. Low grade fevers for a week, no nausea or vomiting but Low grade fevers for a week, no nausea or vomiting but reported frothy urine and intermittent abdominal pain over reported frothy urine and intermittent abdominal pain over the past few hours. History of a URI in the family, including the past few hours. History of a URI in the family, including the child, 2-3 weeks ago. No family history. No PMHx.the child, 2-3 weeks ago. No family history. No PMHx.
QUESTIONS?QUESTIONS? DIFFERENTIAL DIAGNOSES?DIFFERENTIAL DIAGNOSES? WORK UP?WORK UP?


Henoch Schonlein PurpuraHenoch Schonlein Purpura Self limitedSelf limited vasculitis of the small vessels vasculitis of the small vessels Occurrence 9/100000 with male predominanceOccurrence 9/100000 with male predominance 2-8 years of age, most common2-8 years of age, most common IgA and C3a mediated disease and can occur with IgA and C3a mediated disease and can occur with
other other Renal involvement leads to nephrotic syndromeRenal involvement leads to nephrotic syndrome Clinical diagnosisClinical diagnosis
– Arthritis in knees and anklesArthritis in knees and ankles– Angioedema in dependent areas with palpable lesionsAngioedema in dependent areas with palpable lesions– Intermittent abdominal pain with possibility of Intermittent abdominal pain with possibility of
intussusception (3%) with currant jelly stools.intussusception (3%) with currant jelly stools.
Henoch Schonlein Purpura Henoch Schonlein Purpura cont...cont...
Differential diagnosisDifferential diagnosis– PAN with neuro and cardiology involvementPAN with neuro and cardiology involvement– Meningococcemia for the rashMeningococcemia for the rash– Kawasaki disease-rash limited to LE, high feverKawasaki disease-rash limited to LE, high fever– JRA-salmon pink rash that is fleetingJRA-salmon pink rash that is fleeting– Flea and spider bitesFlea and spider bites
Labs: Def. Dx: bx of lesion shows leukoclastic angiitis, Bx Labs: Def. Dx: bx of lesion shows leukoclastic angiitis, Bx of renal shows IgA nephropathy and segmental GN with of renal shows IgA nephropathy and segmental GN with crescents, elevated ESR, and elevated serum IgM and IgGcrescents, elevated ESR, and elevated serum IgM and IgG
Therapy: symptomatic; high dose steroids if significant GI, Therapy: symptomatic; high dose steroids if significant GI, Neuro, and renal involvement and baby aspirin if Neuro, and renal involvement and baby aspirin if hypercoagublehypercoaguble
Doctor, Doctor, my child Doctor, Doctor, my child has a high fever and a red has a high fever and a red
tonguetongue 3 year old Asian girl is brought in for persistent fevers of 3 year old Asian girl is brought in for persistent fevers of
102-104102-104ooF for more than two weeks. Patient was taken F for more than two weeks. Patient was taken to primary pediatrician and was given antibiotics for a to primary pediatrician and was given antibiotics for a sorethroat 10days ago but no improvement in fevers, sorethroat 10days ago but no improvement in fevers, neck masses or the redness of the tongue and oral neck masses or the redness of the tongue and oral cavity. Fevers are improving but the girl has cavity. Fevers are improving but the girl has conjunctival injection and has periungual and perianal conjunctival injection and has periungual and perianal desquamation and incredibly irritable and poor appetite. desquamation and incredibly irritable and poor appetite. No N/V/D/myalgias but reporting joint pains. No N/V/D/myalgias but reporting joint pains.
QUESTIONS?QUESTIONS? DIFFERENTIAL DIAGNOSES?DIFFERENTIAL DIAGNOSES? WORK UP?WORK UP?

Kawasaki DiseaseKawasaki Disease Aka MUCOCUTANEOUS LYMPH NODE SYNDROMEAka MUCOCUTANEOUS LYMPH NODE SYNDROME febrile vasculitis of childhoodfebrile vasculitis of childhood cause is unknowncause is unknown unlikely in <4 months due to maternal Abunlikely in <4 months due to maternal Ab 80% are under 5 years of age80% are under 5 years of age
Path: severe inflammation of medium sized vessels, with strong Path: severe inflammation of medium sized vessels, with strong affinity for the coronary arteries, leading to destruction of the affinity for the coronary arteries, leading to destruction of the intimal layer (all 3 layers involved in severe cases)intimal layer (all 3 layers involved in severe cases)
Cardiac disease: MOST COMMON, decreased ventricular Cardiac disease: MOST COMMON, decreased ventricular function 2function 2oo myocarditis, pericarditis, and coronary aneurysms, myocarditis, pericarditis, and coronary aneurysms, thrombosis, stenosis, and sudden death.thrombosis, stenosis, and sudden death.

Kawasaki disease cont...Kawasaki disease cont... Clinical manifestationsClinical manifestations::
Acute phase: 1-2 weeks with fevers upto 104F and unresponsive to Acute phase: 1-2 weeks with fevers upto 104F and unresponsive to AntibioticsAntibiotics
Subacute phase: irritability, anorexia, conjuctival infection, Subacute phase: irritability, anorexia, conjuctival infection, desquamation of periungual and perineal regions and arthritisdesquamation of periungual and perineal regions and arthritis
Convalescent stage: 6-8 weeks post onset of diseaseConvalescent stage: 6-8 weeks post onset of disease
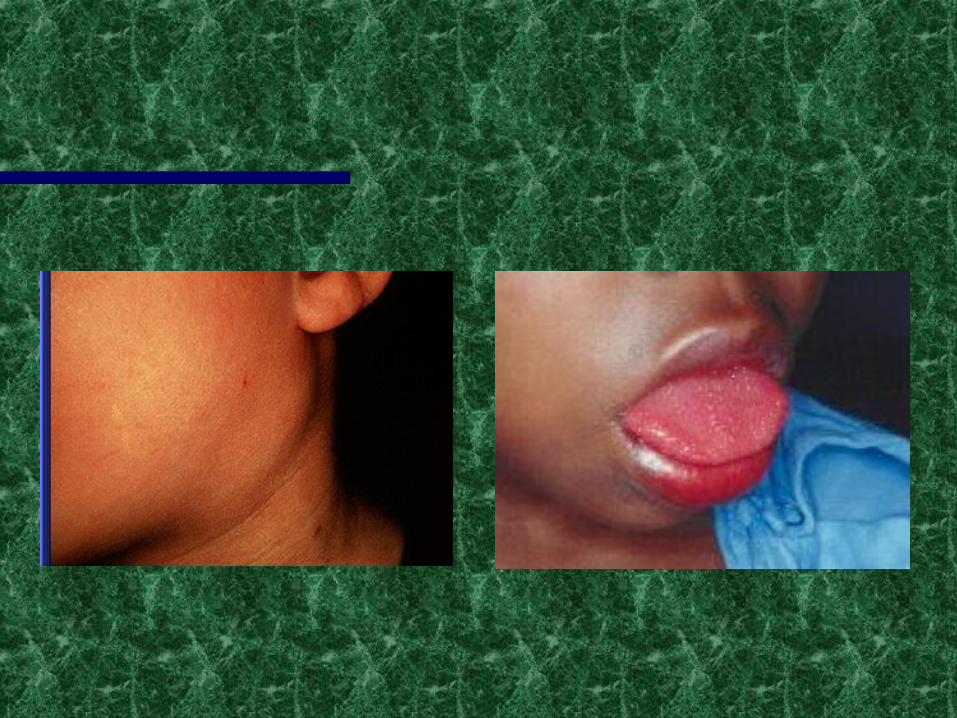
– bilateral bulbar conjunctival injection without exudatebilateral bulbar conjunctival injection without exudate– strawberry tongue and oral erythemastrawberry tongue and oral erythema– erythema and edema of arms and legserythema and edema of arms and legs– CERVICAL LYMPHADENOPATHY > 1.5 cmCERVICAL LYMPHADENOPATHY > 1.5 cm– RashRash
Differential Diagnoses:Differential Diagnoses:– Scarlet fever, TSSS, Measles, SJS, JRA, and RMSFScarlet fever, TSSS, Measles, SJS, JRA, and RMSF
Kawasaki disease cont...Kawasaki disease cont...
Labs: 2D-Echo absolutely pertinent due to Labs: 2D-Echo absolutely pertinent due to extensive coronary involvement; Ig profile due extensive coronary involvement; Ig profile due to elevations in subacute phase, coag studies. to elevations in subacute phase, coag studies. Follow up 2D absolutely recommendedFollow up 2D absolutely recommended
Therapy:Therapy:– IVIG: decreases CAD by 75% (2g/kg over 10 IVIG: decreases CAD by 75% (2g/kg over 10
hours)hours)– ASA for hypercoagulable state due to ASA for hypercoagulable state due to
thrombocytosisthrombocytosis

Doctor, Doctor, I have Doctor, Doctor, I have painful marks on my legspainful marks on my legs
25 y/o asian indian female presents with complaints of 25 y/o asian indian female presents with complaints of nightsweats, anorexia, weight loss, fatigue, and myalgias of few nightsweats, anorexia, weight loss, fatigue, and myalgias of few weeks duration. She reports coming to the US 3 months ago. In weeks duration. She reports coming to the US 3 months ago. In addition to the above symptoms, pt noticed severely painful addition to the above symptoms, pt noticed severely painful nodular lesions in the anterior aspects of her legs. Pain is nodular lesions in the anterior aspects of her legs. Pain is unremitting. Physical exam reveals a thin women in distress unremitting. Physical exam reveals a thin women in distress secondary pain, (+) carotid bruit on the right, widened and secondary pain, (+) carotid bruit on the right, widened and laterally displaced PMI, and Left chest pain relieved with leaning laterally displaced PMI, and Left chest pain relieved with leaning forward. AVSS. (+) splenomegaly. LE exam with nodular forward. AVSS. (+) splenomegaly. LE exam with nodular lesions resembling erythema nodosum and tender to touch. lesions resembling erythema nodosum and tender to touch.
QUESTIONS?QUESTIONS? DIFFERENTIAL DIAGNOSES?DIFFERENTIAL DIAGNOSES? WORKUP?WORKUP?


TAKAYASU ARTERITISTAKAYASU ARTERITIS Vasculitis affecting mostly large caliber vessels, mainly aortic Vasculitis affecting mostly large caliber vessels, mainly aortic
arch branchesarch branches predominant in Asian and Indian subcontinent peoples, women predominant in Asian and Indian subcontinent peoples, women
>>men predominance.>>men predominance. 1/3 before the age of 201/3 before the age of 20
Path: preference for aorta and major branches with significant Path: preference for aorta and major branches with significant renal disease (GN). Association with TB exposure and HLA-Brenal disease (GN). Association with TB exposure and HLA-B
Differential Diagnoses:Differential Diagnoses:– Cogan syndromeCogan syndrome– Behcet’s diseaseBehcet’s disease– Reiter syndromeReiter syndrome– SarcoidosisSarcoidosis
TAKAYASU ARTERITIS TAKAYASU ARTERITIS CONT...CONT...
Clinical manifestations:Clinical manifestations:– pre-pulselesspre-pulseless: :
nightsweatsnightsweats anorexiaanorexia weight lossweight loss fatiguefatigue myalgiamyalgia
– pulselesspulseless: : splenomegalysplenomegaly erythema nodosum, syncope, amaurosis fugaxerythema nodosum, syncope, amaurosis fugax dilated CM, myocarditis, and pericarditisdilated CM, myocarditis, and pericarditis (+) vascular bruit.(+) vascular bruit.
Labs: ESR>60, microcytic hypochromic anemiaLabs: ESR>60, microcytic hypochromic anemia Confirmation of Dx: angiography for occlusive and Confirmation of Dx: angiography for occlusive and
aneurysmal diseaseaneurysmal disease

TAKAYASU ARTERITIS TAKAYASU ARTERITIS CONT...CONT...
TherapyTherapy– surgical excision of stenotic lesions and surgical excision of stenotic lesions and
management of dilated aorta if indolent management of dilated aorta if indolent diseasedisease
– Immunosuppressives: Immunosuppressives: prednisone (1mg/kg/day) in early stage, prednisone (1mg/kg/day) in early stage, cyclophosphamide and methotrexate if refractory cyclophosphamide and methotrexate if refractory
to steroidsto steroids

Doctor, Doctor, my child Doctor, Doctor, my child needs your helpneeds your help
10 year old child presented with complaints of 10 year old child presented with complaints of persistent fevers with diagnosis of FUO, persistent fevers with diagnosis of FUO, diarrhea, skin lesions, numbness and tingling diarrhea, skin lesions, numbness and tingling with muscle weakness for the past few days. with muscle weakness for the past few days. Physical exam with temp of 101.1, Physical exam with temp of 101.1, erythematous and necrotic skin lesions on the erythematous and necrotic skin lesions on the leg and lateral aspect of the ankle, similar to leg and lateral aspect of the ankle, similar to stasis ulcers, and Left foot dropstasis ulcers, and Left foot drop
QUESTIONS?QUESTIONS? DIFFERENTIAL DIAGNOSES?DIFFERENTIAL DIAGNOSES? WORKUP?WORKUP?
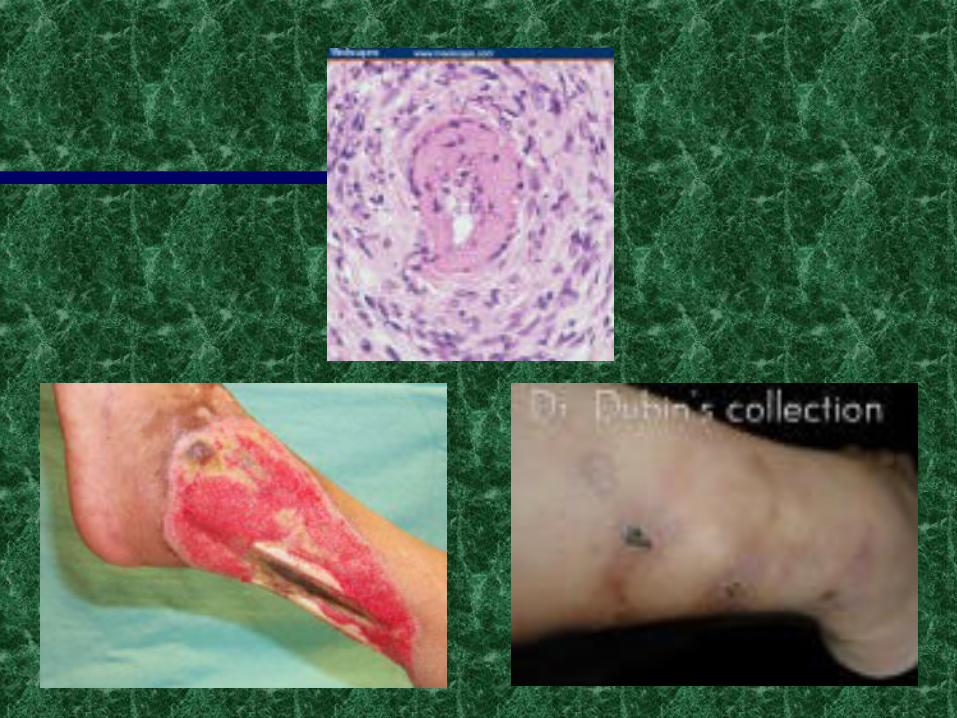
POLYARTERITIS NODOSAPOLYARTERITIS NODOSA Clinical manifestationsClinical manifestations
– FUO, mononeuritis multiplexFUO, mononeuritis multiplex– depends on variety of vessels involveddepends on variety of vessels involved– multiple systems affected, including peripheral nerves, mesenteric multiple systems affected, including peripheral nerves, mesenteric
vessels, heart and brainvessels, heart and brain– often associated with p-ANCA in adults but classis PAN is ANCA often associated with p-ANCA in adults but classis PAN is ANCA
negative.negative. Diagnosis: Biopsy of tissue in symptomatic sites is highly Diagnosis: Biopsy of tissue in symptomatic sites is highly
sensitive and specific and ANGIOGRAPHY for dilatation of arteries.sensitive and specific and ANGIOGRAPHY for dilatation of arteries. Differential diagnosisDifferential diagnosis
– HSPHSP– Wegener’s Wegener’s – good pasture’s good pasture’s – Churg straussChurg strauss
POLYARTERITIS NODOSA POLYARTERITIS NODOSA cont...cont...
LabsLabs: :
– ESRESR– abnormal urineabnormal urine– Hep B and C serology (cause 10-30%)Hep B and C serology (cause 10-30%)– increased B-cell lymphocytesincreased B-cell lymphocytes– hydralazine, allopurinol, penicillamine causeshydralazine, allopurinol, penicillamine causes
TherapyTherapy– SteroidsSteroids– cytoxancytoxan– prostacyclinprostacyclin
Doctor, Doctor, my Doctor, Doctor, my teenage son coughed up teenage son coughed up
bloodblood
15 y/o male with hx of chronic sinusitis 15 y/o male with hx of chronic sinusitis and congestion, here with complaints of and congestion, here with complaints of hemoptysis and dyspnea but stable hemoptysis and dyspnea but stable now.now.
QUESTIONS?QUESTIONS? DIFFERENTIAL DIAGNOSIS?DIFFERENTIAL DIAGNOSIS? WORKUPWORKUP

WEGENER’S WEGENER’S GRANULOMATOSISGRANULOMATOSIS
Differential diagnosisDifferential diagnosis– sarcoidsarcoid– TBTB– Churg StraussChurg Strauss
Epidemiology of WGNEpidemiology of WGN– mostly kidney and lung with granuolomasmostly kidney and lung with granuolomas– adults (4th and 5th decades) >>>kidsadults (4th and 5th decades) >>>kids– caucasians >>>noncaucasiancaucasians >>>noncaucasian– initially with respiratory symptoms and then renal initially with respiratory symptoms and then renal
insufficiencyinsufficiency
WEGENER’S WEGENER’S GRANULOMATOSISGRANULOMATOSIS
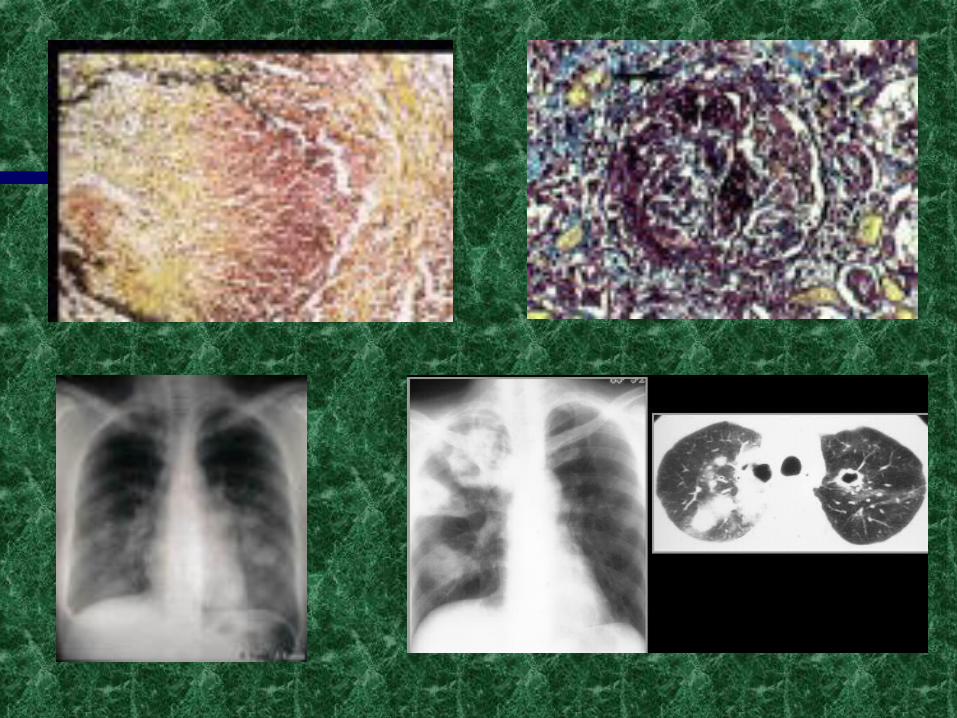
Diagnosis: Clinical findings of sinusitis and pulm Diagnosis: Clinical findings of sinusitis and pulm finding, order high resolution CT. Check ANCA: finding, order high resolution CT. Check ANCA: (90% of WGN have the marker) with 70% (90% of WGN have the marker) with 70% sensitivitysensitivity
Bx:Bx:– lung: granulomas lung: granulomas – renal: 10% with granulomas, segmental necrotizing renal: 10% with granulomas, segmental necrotizing
GN GN RX: rapid therapy neededRX: rapid therapy needed
– SteroidsSteroids– cyclophosphamidecyclophosphamide
OTHERSOTHERS
Behcet’s disease =>f/u CT scan of brain for Behcet’s disease =>f/u CT scan of brain for ocular involvement. ocular involvement.
Cogan syndrome: autoimmune hearing loss, Cogan syndrome: autoimmune hearing loss, aortitis and keratitisaortitis and keratitis
Buerger’s Disease in a male <40 yrs smoker Buerger’s Disease in a male <40 yrs smoker with claudication, rest painwith claudication, rest pain
SLE arteritisSLE arteritis Temporal arteritis with polymyalgia Temporal arteritis with polymyalgia
rheumaticarheumatica Churg-Strauss SyndromeChurg-Strauss Syndrome

Behcet’s
Cogan’s
References:References:
Nelson’s PediatricsNelson’s Pediatrics Harrison’s Internal MedicineHarrison’s Internal Medicine Google search for picturesGoogle search for pictures AAP Board PREPAAP Board PREP CMDT 2004CMDT 2004