Embed Size (px)
DESCRIPTION
Vulnerability and Capacity Assessment is a participatory investigative process designed to diagnose, assess, analyze and address risks that affect communities. It aims at determining people’s vulnerability to those risks and the capacity they possess to cope with hazards and recover from disasters.
Citation preview

Study Supported by Kenya Red Cross (KRCS) Mombasa Branch through Post Tsunami Rehab Project funded by the German Red Cross.
By Joram H. Oranga

Table of Content
Abstract………………………………………………………………………………………………………………...iii.
Acknowledgement…………………………………………………………………………………………………….iv.
List of Acronyms…………………………………………………………………………………………………........v.
List Figures and Tables………………………………………………………………………………………….. ….vi.
List of Appendices……………………………………………………………………………………………………vii.
1.0 Introduction…………………………………………………………………………………………………………1
2.0 Objectives of the Study……………………………………………………………………………………………2
3.0 Theoretical/Conceptual Framework……………………………………………………………………………..3
3.1 Theoretical Framework of the study……………………………………………………………………….........3
3.2 Conceptual framework of the study………………………………………………………………………..........4
4.0 Study Techniques, Methods and Materials …………………………………………………………………….6
4.1 VCA Study Sites……………………………………………………………………………………………….. …6
4.2 Data and Data Collection Instruments…………………………………………………………………………..7
5.0 Results and Findings of the VCA Process………………………………………………………………….. ..10
5.1 Susceptibility to Disasters……………………………………………………………………………………….10
5.1.1 Exposure to Hazards…………………………………………………………………………………………..11
5.2 Susceptibility to Health Consequences and Nutritional Conditions………………………………………...12
5.3 Vulnerability Demographically……………………………………………………………………………….....16
5.4 Community Vulnerability…………………………………………………………………………………………18
5.5 Disaster Preparedness Capacity…………………………………………………………………………….....21
6.0 Summary of the Findings………………………………………………………………………………………. 24
7.0 Conclusions and Recommendations…………………………………………………………………………..26
References…... ……………………………………………………………………………………………………....27
Appendices……………………………………………………………………………………………………………28
ii | P a g e

Abstract
The purpose of this Report is to present a tentative framework for Reducing Vulnerability and Building Community Resilience and determine variability, change, influence and transformation generally applicable to a wide range of contexts, systems and hazards and address the cause-effects of hazards on the local community studied. Social Vulnerability is distinguished from biophysical vulnerability, which is broadly equivalent to the natural hazards concept of risk. A concise typology of physically defined hazards is presented; the relationship between the vulnerability and adaptive capacity of a human system depends critically on the nature of the hazard faced. Adaptation by a system may be inhibited by process originating outside the system; it is therefore important to consider “external” obstacles to adaptation, and links across scales, when assessing adaptive capacity. When disasters occur, they do not affect everyone in the same way. In emergency planning, it is important to pay special attention to the needs of people who are deemed particularly at risk, or the “most vulnerable”. The common view is that “vulnerable populations” include the very young, the very old, women and people with disabilities, while partially accurate, this view of the “most vulnerable” is often misleading and could result in inappropriate response expectations or activities. Stated more specifically, not all seniors, youth or women are “vulnerable”. Some may in fact be more adept at responding to disaster than their general grouping or population category might first indicate.
Most importantly, the VCA model focuses on the population of a community with the objective of answering these three questions: who are the community’s “most vulnerable”; where do they generally reside; and, what is their capacity to respond or recover? The VCA model is intended to be applicable universally across diverse cultures, community sizes, geographic locations, or resource levels. However, to apply the model successfully, two key ingredients are required: a team effort by a broad group of people who reflect the community, as well as its key stakeholders; and a patient effort to continue to expand ones’ understanding of “vulnerability”, the “most vulnerable” and the reality of emergency situations.
iii | P a g e

Acknowledgement
My sincere gratitude goes to the staff of the Kenya Red Cross Society, Mombasa Branch for giving me an
opportunity to lead the VCA Process. Many Special thanks go to Anwar Said-Branch Coordinator, Tom
Omollo-Regional Disaster Management Officer, Abdalla Athmani-First Aid Training Officer, Team Leaders
and Volunteers/Enumerators for their inputs, cooperation and dedication throughout the entire exercise.
Much appreciation also goes to the respondents who set aside personal time from their normal schedule for
the sake and interest of this exercise during data collection. I also acknowledge the invaluable support
received from the Area Chiefs of the 11 Locations by mobilizing community members, Village Elders,
Opinion Leaders and the Community Disaster Management Committee (CDMC) Members. Much
appreciation also goes to the key informants for their active participation and insight.
May this Report provide the much needed impetus to support Disaster Risk Reduction (DRR) activities and
programmes.
List of Acronyms
AIDS Acquired Immune Deficiency Syndrome
ARI Acute Respiratory Infection
iv | P a g e

BMI Body Mass Index
CBD Central Business District
CBO Community Based Organization
CDF Constituency Development Fund
CDMC Community Disaster Management Committee
CPGH Coast Provincial General Hospital
CVCA Community-based Vulnerability Capacity Assessment
DC District Commissioner
DRR Disaster Risk Reduction
EWS Early Warning System
FBO Faith Based Organization
FGD Focus Group Discussion
Fig Figure
HIV Human Immuno-deficiency Virus
KMA Kenya Maritime Authority
KPA Kenya Port Authority
KRCS Kenya Red Cross Society
KWS Kenya Wildlife Service
LATF Local Authority Trust Fund
MCM Municipal Council Mombasa
MOWASCO Mombasa Water and Sewerage Company
MUAC Mid Upper Arm Circumference
PRA Participatory Rural Appraisal
PUA Participatory Urban Appraisal
RTA Road Traffic Accident
STD Sexual Transmitted Diseases
TB Tuberculosis
VCA Vulnerability and Capacity Assessment
WHZ Weight-for-height z scores
List of Figures and Tables
i. List of figures
Fig.1a………………..Vulnerability variables, 3
v | P a g e

Fig.1b………………..Base of vulnerability variables, 3
Fig. 2a………………..Conceptual framework, 4
Fig. 2b………………..An illustration of the conceptual framework (specific focus on vulnerability), 5
Fig. 3…………………A step by step approach to the VCA Process, 8
Fig. 5…………………Ranking of hazards/risks according to community impact, 10
Fig. 6………………....Diseases ranking on weighted basis (community projections), 12
Fig. 8b………………..Infant mortality rate, 14
Fig. 8c………………..An illustration of infant mortality rate, 15
Fig. 9………………....An illustration of the level of vulnerability demographically, 16
Fig. 10…………….....Community vulnerability on weighted basis, 19
ii. List of Tables
Table 4.1…………….Respondent groups and data collection techniques, 9
Table 4.2…………….Breakdown of respondents demographically, 10
Table 7………………Infant and maternal malnutrition rates, 14
Table 8a……………..Infant and mortality rate, 14
Table 8d……………..Summary of common illness in Mombasa, 16
Table 11……………..Analysis of organizations, 23
List of Appendices
Appendix 1. List of the locations under the study, 28
Appendix 2. List of respondents/informants/stakeholders, 29
vi | P a g e

Appendix 3. VCA Checklist and questionnaires, 30
Appendix 4. Graphical presentation of the study area, 32
vii | P a g e

1. Introduction
The main victims of disasters tend to be people who are already among the most vulnerable, with livelihoods that are under constant threat and living in areas that are already impoverished and degraded. These people live and work in places at risk because they cannot afford to be where it is safer. They lack the protection that others have, and the ability to influence everyday decision making process. They are often excluded from the discussions and studies that determine management policy, and live far from where health and power are concentrated. This distance increases the likelihood of socio-cultural problems that arise when efforts to assist these people are deployed, they are individuals merely controlled by their own need for survival and nothing else. With no will and know how to change their situations, any project introduced to them must first try to address their need for survival to enlist willingness to participate.
The global environmental change and sustainability situations increasingly recognize the need to address the consequences of changes taking place in the structure and function of the biosphere. These changes raise questions such as: Who and what are vulnerable to the multiple environmental changes underway, and where? Previous studies demonstrate that vulnerability is registered not by exposure to hazards (perturbations and stresses) alone but also resides in the sensitivity and resilience of the system experiencing such hazards. This recognition requires revisions and enlargements in the basic design of vulnerability assessments, including the capacity to treat coupled human–environment systems and those linkages within and without the systems that affect their vulnerability. A vulnerability framework for the assessment of coupled human–environment systems is presented in the theoretical/conceptual framework.
The disaster risk scenario for Mombasa County can be described as moderate. The county experience moderate risk conditions owing to a high vulnerability due to critical poverty conditions in most locations. A bigger number of people continue to be highly vulnerable to water and sanitation, water/air borne diseases, diarrhoea, flooding due to poor drainage, poor waste disposal and much of this vulnerability is chronic and as a result of high levels of poverty projected at 40% at urban levels. The increase in the price of staple and general impact of inflation on household expenditure means that very poor households will miss some of their food entitlements further plunging these families in to severe malnutrition. In the areas studied, most Sources of income for the ‘poor’ and ‘very poor’ are predominantly casual labour opportunities in the manufacturing plants, informal sector, Kilindini port, small kiosk businesses, food vending, water vending, car washing and clothes washing and other manual labours. Employment and remittances is the major source of income for the ‘middle and upper levels’. The difference in employment activities for the wealthier and the poorer households is that while the poorer households predominantly depend on casual labour, the ‘middle’ and ‘upper levels’ are engaged in skilled and semi – skilled labour activities.
The need to have safe and safer communities have pushed the local people to develop their own initiatives as the services from the responsible government ministries/agencies are never forth coming, and when they do, they are inadequate and substandard. The local population in the studied areas feel cheated and short changed by the responsible parties. Municipal Council of Mombasa (MCM) is only visible when checking for operating licences for small business and collecting rates and fees, when it comes to service provision it is almost nonexistent. In some local villages it was even much harder to define MCM which was more associated with councillors and politicians rather than organ of service for the locals.An evaluation of community capacity and resilience presents key information to aid better decision making when it comes to disaster situations. The effort to assess existing preparedness, response and recovery plans and missions would facilitate realignment of resources for better mitigation practices including
1 | P a g e

awareness and knowledge development. Stakeholders and partners analysis also provided a proactive approach towards resource management and consolidation.
Furthermore, this study finds that the level of exposure and vulnerability of the areas studied can actually be brought to manageable level as they mainly point towards, lack f essential services like water supply, sewerage system, housing, sanitation facilities, access roads, community security and by and large information materials and access to information n disaster management.
This exercise was carried out as part of the Kenya Red Cross, Disaster Preparedness Programme geared towards reducing disaster risk and promoting community safety and resilience.
2. Objectives of the Study
Vulnerability and Capacity Assessment is a participatory investigative process designed to diagnose, assess, analyze and address risks that affect communities. It aims at determining people’s vulnerability to those risks and the capacity they possess to cope with hazards and recover from disasters.
The objective(s) of the study were to;-
Help communities understand the hazards they face, assist them to improve the prevailing situation based on local skills, knowledge and initiatives and prevent hazards from turning into disasters and better understand the local environment including predication and pattern of risks and hazards.
Provide a wide range of information to support decision making, assist in monitoring and evaluation of disaster projects and support the communities to embark on viable livelihood efforts to reduce vulnerability.
Gather baseline information to serve as reference for emergency needs assessment to aid the development and designing of response, prevention and preparedness programmes that contribute towards building community resilience and promote increased community education, awareness and safety and disaster risk reduction.
To analyze the local capacity to cope with risks and hazards with patterns and local authorities to prevent or reduce the potential effects of disasters including mapping stakeholders and outlining their capacities, roles and responsibilities.
3. Theoretical/Conceptual Framework of the Study3.1 Theoretical Framework of the Study
The background of this study is a postulation of a cause-effect relationship between Vulnerability, Hazard Events and the Impacts of Disasters. Necessitating further the need to understand and recognize the
2 | P a g e

presence of Independent, Dependent and Moderating and Intervening Variables in the event of analyzing VCA process, see further illustration in fig 1(a) and (b) below.
Fig 1a: Vulnerability Variables
The illustration above in 1(a) explains the cause-effect relations between Vulnerability (Independent Variable), Hazard Event (Dependent Variable), Exposure (Dependent Variable) and Impacts (Dependent Variable) while Dose-response is the Moderating Variable.
Fig 1b: Base of Vulnerability Variables
When analyzing the risk factors surrounding the vulnerable population, it is important to understand what would be the probable intervention and at what levels. Fig. 1b illustrates a situation analysis in the event that there is a need to address the unstable systems that happen to a larger extent contribute towards the disasters experienced. Base Vulnerability Variables are the Independent Variables, Disaster and Hazard (perturbation) is the Dependent Variables.
3.2 Conceptual Framework of the Study
3 | P a g e

Fig 2a: Conceptual Framework
The conceptual framework illustrated on the table above fig 2a. shows the Relationship between variables at different levels, the contributors of community vulnerability and what cause of action the community is willing and would be willing to take and at what levels. The conceptual framework below fig 2b. illustrates the relationships and correlations between different attributes existent at the local levels and the vulnerability levels. Vulnerability rests largely within the condition and dynamics of the coupled human–environment and the system exposed to hazards. Vulnerability analysis must be comprehensive, treating not only the system in question but also its many and varied linkages, comprehensive vulnerability analysis ideally consider the totality of the system. Failure to consider this larger context could lead to the identification of ‘‘response opportunities,’’ which, if implemented, lead to significant unintended consequences or ‘‘surprise’’ the vulnerability framework presented here is guided by the need to provide a template suitable for ‘‘reduced-form’’ analysis yet inclusive of the larger systemic character of the problem. The framework is not explanatory but provides the broad classes of components and linkages that comprise a coupled system’s vulnerability to hazards. The basic architecture (Fig. 2a) consists of: ( i) linkages to the broader human and biophysical (environmental) conditions and processes operating on the coupled system in question; (ii) perturbations and stressors stress that emerge from these conditions and processes; and (iii) the coupled human–environment system of concern in which vulnerability resides, including exposure and responses (i.e., coping, impacts, adjustments).
4 | P a g e

Fig 2b: An illustration of the Conceptual Framework (Specific focus on Vulnerability)
These elements are interactive and scale dependent, such that analysis is affected by the way in which the coupled system is conceptualized and bounded for study. The full framework is illustrated in Fig. 2a by way of spatial scale, linking place (blue) to region (yellow) to globe (green), and various parts are elaborated in Fig. 2b. The coupled human–environment system, whatever its spatial dimensions, constitutes the place of analysis. The hazards acting on the system arise from influences outside and inside the system and place but, given their complexity and possible nonlinearity, their precise character is commonly specific to the place-based system. For these reasons, the hazards themselves are located both within and beyond the place of assessment. These hazards hold the potential to affect the coupled system, including the ways in which the system experiences perturbations and stressors. The human–environment conditions of the system determine its sensitivity to any set of exposures.
These conditions include both social and biophysical capital that influences the existing coping mechanisms, which take effect as the impacts of the exposure are experienced, as well as those coping mechanisms adjusted or created because of the experience. For the human subsystem, these mechanisms may be individual or autonomous action and or policy-directed changes. Importantly, the social and biophysical responses or coping mechanisms influence and feed back to affect each other, so that a response in the human subsystem could make the biophysical subsystem more or less able to cope, and vice versa. In some cases, coping mechanisms per se give way to adaptation, significant system-wide changes in the human–environment conditions. The responses, whether autonomous action or planned, public or private, individual or institutional, tactical or strategic, short- or long-term, anticipatory or reactive in kind, and their outcomes collectively determine the resilience of the coupled system and may transcend the system or location of analysis, affecting other scalar dimensions of the problem with potential feedback of the coupled system in question. The framework illustrates the complexity and interactions involved in vulnerability analysis, drawing attention to the array of factors and linkages that potentially affect the vulnerability of the coupled human–environment system in a place.
4. Study Techniques, Methods and Materials4.1 VCA Study Sites
5 | P a g e

Mombasa County is composed of four administrative districts namely Changamwe, Kisauni, Likoni and Mombasa curved from what was originally Mombasa then later Mombasa and Kilindini Districts as the government continues to reorganize its services with several divisions and locations spread out from Shika Adabu in the South Coast to Bamburi in the North Coast to Miritini in the West Coast.
Mombasa County lies between latitudes 30 8 and 40 10 south of equator and longitudes 390 41 and 390 80 east of Greenwich Meridian with an estimated population size of 945, 785. Mombasa is the main business and industrial hub of the Coast Region providing essential finished goods, processing raw materials and providing essential access to goods and services through the Kilindini Port and transportation further hinterland. Kilindini Harbour also provides docking facilities for both merchant and cruise ships. Availability of world class tourist hotels ensure continued free flow of tourist both domestic and foreigners visiting the County. Moi International Airport serves the county and links internationally providing vital connection for tourism and business travels.
The County lies within the coastal strip in the hot tropical region where the weather is influenced by monsoon winds. The total annual rainfall ranges between 1025-1270mm while the annual mean temperature is 27.90c with a minimum of 22.70c and a maximum of 33.10c. Average humidity at noon is about 65 per cent. The livelihood patterns are mainly characterized by small enterprises, small scale agriculture, fishing, construction related work, permanent and temporary employment. Population distribution and settlement patterns are mainly influenced by proximity to roads, water, electricity and other essential amenities.
The VCA was conducted in eleven locations in Mombasa County namely
Chaani Location Changamwe Location Ganjoni Location Majengo Location Mikindani Location Miritini Location
Mwembe Tayari Location Port Reitz Location Shika Adabu Location Shimanzi Location Tononoka Location
With Chaani, Changamwe, Mikindani, Miritini and Port Reitz Location being in what is now known as Changamwe District previously part of Kilindini District. Majengo, Mwembe Tayari, Shimanzi and Tononoka Locations are part of Mombasa District while Shika Adabu is in Likoni District.
4.2 Data and Data Collection Instruments
A step by step approach to conducting VCA through the CVCA Model was employed to address the objectives of this study. A checklist, questionnaire and tools for VCA were designed and developed through
6 | P a g e

extensive consultation. Having designed the process and tools, a list of data type, strategy that conforms to the universal VCA standard was followed. The analysis process of the VCA model is intentionally sequential. One should firm up knowledge at one level or step before moving on to the next. The intent of each step is to provide further meaning or greater context to the understanding that one has of the “most vulnerable” segment of the population. The CVCA model (see Diagram below) contains the following steps. (Each of the steps is explained separately below.)
1. Create the Planning Team2. Set planning parameters3. Gather relevant information4. Define and map the general population5. Define and map high-density areas6. Divide and map the Location into “Operational Sectors”7. Define and map “high-risk” areas8. Select applicable categories for the “most vulnerable” 9. Identify, categorize (as full or part-time), and map sites related or specific to the identified “most
vulnerable” groups (e.g., seniors’ homes, long-term care facilities, day-care facilities, social services access points, or clinics).
10. Identify and map other areas where each of the “most vulnerable” groups has significant numerical presence.
11. Estimate likely emergency needs of the “most vulnerable”(i.e., of each vulnerable group within each sector)
12. Identify realistic expectations regarding the capacity of each identified group (consider physical, cognitive, resources, linkages, support system)
13. Consider conditions that change the presence or vulnerability level of the identified groups (e.g., population shifts during the day)
14. Categorize sectors, facilities or community segments into relative levels of priority (1 or highest, 2, or 3).
15. Indentify issues or groups for further consideration or action.16. Review and update your information as appropriate.
7 | P a g e
Create planning team (1)
Set planning parameters (2)
Gather relevant info. (3)

No
Yes
No
Yes No
Yes
Review/update
Fig 3: A step by step approach to the VCA Process
The study area was delineated after careful considerations and interrogation of disaster trends in Mombasa. Deliberate attempts were made to include all key respondents who possess rich and vital information that can add value to the VCA Process. The desire to generate reliable and valid data was highly emphasized with respondents clustered in consultation with KRCS Mombasa Office.
The respondent groups were drawn from community organizations i.e. women groups, youth groups, village elders, opinion/religious leaders, chiefs, government ministries/agencies that have previously experienced impacts of disasters, intervened during disasters and or responded to disasters. Purposive Sampling Technique was used to narrow down and identify subjects because they are informative or possess the required characteristics that the VCA sets to study or understand. Random Sampling was
8 | P a g e
Define/map general population (4)
Identify/map high-density areas (5)
Divide/map Location into operational sectors (6)
Is Location well
Define/map high risk areas (7)
Selected MV categories (8)
Identify MV sites & categorize (9).
Vulnerability analysis
Identify MV presence (10)
Identify MV/High risk over lap (11) overlap (11)
Identify critical periods (12)
Identify expectations (14) Identify ‘changes’ (15)
Estimate MV needs (13)
Understand MV areas?
Under high-risk areas?
Prioritize (16)
Identify issues and take actions (17)

thereafter employed to get the respondents to participate in the exercise to reduce the level of bias from purposive sampling. Data was sorted and sieved by use of excel and analysis of quantitative data through Strata and SPSS software while qualitative data was analyzed through NCT Techniques (Notice Think Collect). The following data collection tools were picked from the toolbox
Direct Observation Vulnerability and Risk Mapping Capacities and Resource Mapping Seasonal Chart Community Organization Chart Livelihoods/Wealth Chart
Transect Walk Historical Chart Historical Profile Focus Groups Questionnaires Group/Individual Interview
The Community VCA Investigations were carried out by the VCA teams in the eleven communities and the information gathered presented here, for all the communities.
Table 4.1: Respondent groups and data collection technique employed
S/No. Key Informants Data Collection Tools
Sample Size Geographical Location
1. Individual Respondents InterviewQuestionnaire
71 11 locations (see appendix 1)
2. 2Private/Civil Society and FBO/CBO groups
InterviewQuestionnaire
22 Mombasa, Kilindini
3. Community Members strategically selected
PUA/PRAGroup InterviewsObservations Transect WalksRisk MappingResource Maps
342 11 locations (see appendix 1)
4. Government Agencies Interview Questionnaires
12 Mombasa, Kilindini
5. Public interest groups FGDsGroup Interviews
22 11 locations (see appendix 1)
6. Children 10 Changamwe, Chaani, Port Reitz Locations
Table 4.2: Breakdown of Respondents Demographically
S/No. Respondents No. in attendance % represented1. Women 139 29
2.
Men 201 42
3.
Youth 125 26
4.
Elderly (187) Crosscutting (men/women atleast 55%)
5.
Disabled persons and Children 14 3
Total 479 100
9 | P a g e

5. Results and Findings of the VCA Process5.1 Susceptibility to Disasters
The table below is an illustration of ranking of risks/hazards according to impact on the communities. The ranking is an analysis of the number of mentions a specific attribute received from the respondents and community social groups on weight-basis according to effects, frequency and impact either in the past or as currently projected. An investigation in to the nature of disaster trends and patterns elicited mixed reactions and very interesting debates as most disasters were mentioned according to occupation and or households, meaning that the respondents had firsthand knowledge of the disasters. The respondents then were allowed to draw a list of different disasters that affects and or has affected them in the past. An explanation was done to ensure the community understands disaster in the same context as the objectives of the study. A final list was drawn after a resolution was carried out as shown in the chart.
12%
13%
13%
5%4%12%
17%
6%
4%
4%4%
5% 2%Community Hazard and RisksFloods
FireDrugs/S.AW. ShortageRTAPoor DrainageDiseasesPollution (Wa-ter)Derilicts Build-ingProstitutionSexual ViolenceLandslidesInsecurity
Fig 5. Ranking of Hazards/Risks according to Impact on Community
The Ranking showed a particular pattern of the disasters/hazards/risks some closely related, for instance, where the community complained about poor drainage there was also a mention of flooding, pollution and disease outbreaks which strongly appeared in all the eleven locations studied. Where there were problems of drugs and substance abuse the cases of HIV/AIDS and sexual violence were also mentioned especially in Miritini, Shimanzi, Tononoka, Shika Adabu, Port Reitz and Chaani. Road Traffic Accident (RTA) was mainly attributed to the highway with cases in Changamwe, Mikindani, Miritini, Shika Adabu and Tononoka Locations. Water shortage was another teething problem extensively repetitive in most locations and closely related to diseases outbreak. Where the community complained of water shortage as a problem there were also cases of Typhoid, Cholera, Diarrhoea and Intestinal Parasites/Worms reported, mainly because of the levels of hygiene observed in the areas of Mikindani (Bangladesh Slums), Changamwe, Chaani, Port Reitz (Wayani/Bokole Slums), Shika Adabu and Miritini. However, community organizations and individual respondents mentioned disasters that directly affected their livelihoods and or would impact on their lives in the short run if not properly addressed. More interesting was the continued reference to
10 | P a g e

disasters that adversely affected communities in the past like Mtongwe Ferry Mishap, ‘Kaya Bombo’ Likoni Clashes, El Nino Floods and Gas Leakage at the Refinery. Meaning the ranking was based on personal understanding of the disasters affecting the community.
5.1.1 Exposure to Hazarda. Changamwe, Port Reitz and Chaani
Residents of Changamwe and Chaani are exposed to the following hazards; gas leakage, poor drainage, dust, sewerage, TB, respiratory problems, diarrhoea, skin conditions, petroleum fumes, oil tankers parked in residential areas, garbage disposal, overflowing sewerage, blocked drainage, fire, alcoholism, drugs, contaminated water, poor sanitation and lack of toilet facilities.
b. Mikindani and Miritini
Mikindani and Miritini is exposed to floods, landslides, fire, rampant local brew/alcohol trade, intestinal worms, cholera, poor human waste disposal, garbage, collapsed sewerage system, respiratory problem, skin conditions, dust, RTA, sexual violence and TB.
c. Shika Adabu
Shika Adabu is exposed to the following hazards; fire, garbage, RTA, drugs, contaminated water, sanitation and floods.
d. Majengo, Mwembe Tayari and Shimanzi
Hazards rampant in the 3 locations are fire, drugs, HIV/AIDS, TB, Cholera, contaminated water, poor sanitation, poor drainage, prostitution and derelict buildings.
e. Tononoka
Tononoka has the problem of drugs, derelict buildings, and lack of sanitation facilities in some areas, TB, HIV/AIDS and Diarrhoea.
f. Ganjoni
Ganjoni is mainly faced by insecurity cases but in the slums it is more of drugs, lack of water and sanitation facilities, diarrhoea, TB, HIV/AIDS and to some extent skin conditions.
5.2 Susceptibility to Health Consequences and Nutritional Conditions
Diseases on weighted-basis ranked highest accounting for 17 per cent of the disasters that the communities collectively are aware of and or directly affect their livelihoods. Relatively, disease based risks and hazards have strong correlations with the prevailing community conditions like Cholera weighed highly on communities with heavy presence of slums and or informal settlements, severe to frequent water shortages, poor drainage system and malfunctioning and or lack of sanitation facilities and problem of garbage and dumping sites in residential areas including medium to severe sanitation, waste and drainage problems. Strong cases reported in Ganahola, Bangladesh/Kisumu Ndogo slums in Mikindani, Chaani, Wayani and Bokole slums in Port Reitz. While areas like Shimanzi, Shika Adabu, Changamwe and upper Mikindani have garbage disposal problems. Mikindani and Miritini suffer severe air pollution that spreads
11 | P a g e

TB, Respiratory and Coughing and skin problems due to the levels of dust in most places within the residential areas. Below is an illustration of the diseases reported to be affecting the community.
14%
19%
16%7%
9%
2%
9%
12%
5%5% 2%
Disease Ranking according to Impact
HIV/AIDS
Cholera
Malaria
Malnutrition
Typhoid
STDs
Respiratory Prob-lem
TB/Coughing
Intestinal Parasites
Food Poisoning
others
Fig 6: Disease ranking on weighted-basis (community projections)
5.2.1 Child and Maternal Mortality and Nutritional Ratesa. Area of study Shika Adabu, Mikindani, Miritini, Chaani, Changamwe and Port
Reitz Locations
The most serious malnutrition happens in a child’s first year of life. It is caused by diseases such as malaria or worm infestation, poor sanitation and personal hygiene, which leads to diarrhoea and inadequate childcare practices such as early weaning and mixed feeding. The early years are critical to a child’s growth and development. The tragedy is that for so many children malnourished in the formative years their physical and mental development lags are irreversible and becomes permanent. Representing huge losses in human potential. Malnutrition is a direct cause of child mortality and diminishes intelligence, impairs learning and weakens human productivity. Adequate nutrition is critical to child development. The period from birth to two years of age is important for optimal growth, health, and development. Unfortunately, from the study it indicated this period is often marked by growth faltering, micronutrient deficiencies, and common childhood illnesses such as diarrhoea and acute respiratory infections (ARI). Feeding practices reported include early initiation of breastfeeding, exclusive breastfeeding during the first six months of life, continued breastfeeding for up to two years of age and beyond, timely introduction of complementary feeding at six months of age, frequency of feeding solid/semisolid foods, and the diversity of food groups fed to children 0-2 years.
12 | P a g e

A woman’s nutritional status has important implications for her health as well as the health of her children. Malnutrition in women results in reduced productivity, an increased susceptibility to infections, slow recovery from illness, and heightened risks of adverse pregnancy outcomes. For example, a woman who has poor nutritional status as indicated by a low body mass index (BMI), short stature, anemia, or other micronutrient deficiencies has a greater risk of obstructed labour, of having a baby with low birth weight, of producing lower quality breast milk, of mortality due to postpartum haemorrhage, and of morbidity of both herself and her baby.
Child nutrition rates were found to be alarming as per the analysis according to the District Public Health Officer for Kilindini District. Nutrition and other related basic care for children are at the lowest level this was attributed to failure by parents to attend follow medication and care. The data obtained from the District Health Information and Records Office at Port Reitz District Hospital showed that the health facilities handle only new cases of infants and children upto 1 year old. Children above 1 year old were the highest defaulters when it comes to basic care and nutrition. The highest and most common nutrition elements was found to be Vitamin A supplements where 61.9 percent of children were found to be compliant. While children under 5 years attending clinics were 60 percent clearly indicating the level of personal awareness among parents were high. However, the general health status of children were found to be unsatisfactory as the Mid Upper Arm Circumference (MUAC) with greater than 13.5cm was only 5.13 percent of the number of children attending clinics, with the biggest number not known as there are no follow up records 35 percent of children under five are stunted (low height-forage), while 7 percent of children are wasted (low weight-for-height) and 16 percent are underweight (low weight-for-age).
S/No. Nutritional Item Rate in %
Remarks
1ECD Children Supplemented with vitamin A in 2010 61.9
Confirmed after visiting nursery schools and diagnosis of the children.
2
Children under 5 receiving Vitamin A supplements in health facility
60
Confirmation from data of the patients seeking treatment at the facilities.
3Children Under 5 attending growth monitoring clinic new visits 31.3
These are mainly new cases. Old cases lack adherence as parents do not turn up for monitoring.
4
Children under 5 with MUAC less than 13.5cm
5.13
These are new cases. Old cases cannot confidently build assumptions as the follow up rates is negligible.
5
Lactating mothers with MUAC greater than 21.5cm
2.15
These are id upper arm circumference measurements taken at the facility for mothers seeking medical attention.
6
Pregnant mothers with MUAC greater than 21.5cm
2.57
These are id upper arm circumference measurements taken at the facility for mothers seeking medical attention.
Table 7: Infant and Maternal Malnutrition Rate
13 | P a g e

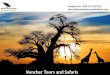
The chart below illustrates the level of deaths among infants and children under 1 year. In 1000 births recorded in the facility 80 deaths are reported while in 1000 births recorded outside the facility 60 deaths are reported.
S/No. Item Rate in %1 Infant Mortality Rate 62 Facility Infant Mortality Rate 83 Maternal Mortality Rate 0.634 Facility Based Maternal Mortality Rate 1.7
Table 8a: Infant and Maternal Mortality Rate
43%
57%
Infant Mortality Rate per 1000
Infant Mortality RateFacility Infant Mor-tality Rate
Fig 8b. An illustration of infant mortality rate
Maternal mortality rate was realized to be much higher in the health facilities as compared to outside. This was mainly due to the level of referrals carried out in the district as most facilities cannot offer the level of service and attention needed for pregnant and ailing mothers. Meaning that fewer deaths are likely to be reported at the community level as compared to the facilities, maternal health was another issue of concern as the safety and health of the children could directly be comparable to that of the mothers. The main contributor to the mortality rates of mothers apart from nutritional issues was realized to be the lack of enough capacity at the local community to handle such cases which is worsened by the poor roads network and accessibility. Patients from Shika Adabu suffer a lot as their referrals are to the Coast Provincial General Hospital which takes a long time due to the inconsistent and slow ferry services. Even though there exists emergency considerations there are always ineffective to be relied upon.
14 | P a g e

Fig 8c. An illustration of Maternal Mortality Rate
Clinical features of malnutrition were significantly more common among children with MUAC less than or equal to 11.5 cm than among those with weight-for-height z scores (WHZ) less than or equal to −3.
5.2.2(b.)Area of study Majengo, Mwembe Tayari, Tononoka and Shimanzi
Locations
Malnutrition rate according to the clinical data reviewed indicated low levels among infants and children under 5 years. The explanation for this can be in two folds (1.) being that the areas studied are within the island which is the CBD of the county or (2.) the levels of information, income and living standards are average or above average. Further analysis of the data showed a similar trend with the data collected in Changamwe indicating that a good number of the mothers seek and or are referred for further assistance in health facilities in Mombasa. However, feedback from informants indicates that the common ailments they suffer from were Malaria, Respiratory Ailments, Diarrhoea, occasional Cholera and STDs which were corroborated by the data from the District Health Office in Mombasa as indicated below. Infant mortality rate recorded at 59.3%, malnourished children at 10, 080 out of 66714 or 15.11%.
Rank Children Adults1 Malaria Diseases of the respiratory System
2Diseases of Respiratory System
Clinical Malaria 4 Diarrhoea Confirmed Malaria 5 Skin conditions Skin Conditions 6 Pneumonia Diarrhoea
Fig 8d. Summary of common diseases in Mombasa
Comparatively, susceptibility to health risks is more high in the west coast in the locations studied than within the island. More households are prone to illness with women and children under 5 years being the most vulnerable.
5.3 Vulnerability Demographically
Community vulnerability cannot directly be linked to specific households but more so on the general practices of an entire community. The common view is that “vulnerable populations” include the very young, the very old, women and people with disabilities, while partially accurate, this view of the “most vulnerable” is often misleading and could result in inappropriate response expectations or activities. Stated more
15 | P a g e
92%
8%Maternal Mortality Rate per 100, 000
Maternal Mortality RateFacility Based Ma-ternal Mortality Rate

specifically, not all seniors, youth or women are “vulnerable”. Some may in fact be more adept at responding to disaster than their general grouping or population category might first indicate. However, the feedback from the respondents provided a vital insight on why certain cadre of the community is vulnerable or dimmed to be more vulnerable than the others. The graph below indicates the most vulnerable in percentage.
0
5
10
15
20
25
30
35
Level of Vulnerability Demographically
Fig 7: an illustration of the Level of vulnerability demographically
Women are the most vulnerable in the 11 locations studied this can also be attributed to the cultural practices, community beliefs and attitude towards women and the unwillingness of men to let women participate in decision making at the household and community levels. Even though, direction observations and individual interviews intimated a few women taking leadership positions including political and organizational. The results strongly indicated a correlation between the level of women vulnerability and that of the children under 5 yrs and between 5yrs-14yrs. Because women are vulnerable they are more likely to rub and or impact the same on their children at all levels, this attribute is strongly repeated in the 11 locations with worse case in Miritini where women and children face sexual violence and exploitation in equal measure. In most of the households interviewed, Women are expected to take care of their families, look after their households and ensure the household properties are secured.
The top ranked risk factors are household related and this is where women and children are likely to be found most of the time. High cases are found in Bangladesh, Chaani, Port Reitz (Bokole, Wayani,), Shika Adabu, Changamwe (Kisumu Ndogo slums) and Tononoka (Moroto, CPGH slums). Another key element of concern is the household or domestic violence reportedly in the slums that further weakens women resolve in building their own resilience towards disasters. Youth Vulnerability is mainly attributed to lack of employments opportunities, costly higher education and lack of pass time/social recreational facilities that have made them susceptible to drugs and substance abuse. Youth vulnerability is correlated to drugs and substance abuse which is rampant and strongly repeated in the 11 locations with worse cases in Tononoka, Shimanzi, Port Reitz, Mwembe Tayari, Mikindani and Shika Adabu. The elderly vulnerability is attributed to neglect and lack of old aged care services with exception of Majengo and Shimanzi that have a closer proximity to such services. While men’s vulnerability is the lowest and strongly attributed to low
16 | P a g e

cadre employment and local brews/alcoholism. A trend that repeats itself in all the slums and low economic endowed households.
More surprising was the level of individual awareness on disasters, understanding of risk factors seemed to increase with the level of exposure and proximity, this is explained by the information levels of the people in slums and informal settlements on the dangers that surrounds them (Mikindani-Bangladesh slums, Miritini, Chaani slums and Port Reitz slums) unlike in the middle level settlement people are oblivious of the risks around them, there’s is a feeling of safety ‘Self fulfilling prophecy’ i.e. Ganjoni, Mwembe Tayari, Tononoka, Mikindani and Port Reitz (middle class settlements). Vulnerability to risk and disasters is pegged more to the levels of income a household generates rather than awareness and education levels. Resource endowment was particularly the main causal factor of the community living conditions. Most respondents expressed strong feelings of wanting to move out and or live somewhere else that is much better and safer.
5.4 Community Vulnerability
Community vulnerability is presented by developmental challenges that are neither regulated nor checked with some within the control of the locals while some quiet beyond their efforts exposing them to all manner of risks. The following attributes were noted from the respondents which further highlighted the in depth of the causes of vulnerability among the local people.
a. Water and Sanitation
Fresh water supply coverage is limited at 54 percent of the total demand according to the Mombasa Water and Sewerage Company (MOWASCO) however the picture on the ground is even much alarming. An average household which is 1 out of approximately 12 households receives tapped water once or twice a week indicating that the percentage coverage could be much lower approximately 25 percent of the demand. This deficit in the supply of tapped water has led to the mushrooming of water vendors and kiosks taking advantage of the problem to earn a living. However, it might be a coping mechanism but further analysis indicates that the water vendors observes no water transportation standards or water handling safety measures exposing the consumers to more water borne related diseases. Hygiene conditions are much lower in the locations studied characterized by informal settlements and collapsed system. On sanitation, only 17 percent of Mombasa County is connected by Sewerage system managed by Mombasa Municipal Council at Kipevu plant, the rest 83 percent are left to find their own means of disposing solid waste including human waste.
The Problem is more pronounced in Chaani, Changamwe, Port Reitz, Miritini and Shika Adabu where human waste is mainly collected in wells which act as septic tanks and most toilet facilities are mainly pit latrines. While the sewerage system in Mikindani has collapsed pouring effluent to Bangladesh slums all
17 | P a g e

the way to Changamwe then Chaani to the ocean at Kipevu exposing close to 150,000 people to various ailments from the overflow. The lack of proper waste disposal, sanitation facilities and systems have caused major pollution problem in the studied locations, with garbage lying everywhere, fresh water wells mixing with effluents as they are sunk closer to each other. Common ailments are malaria, cholera, typhoid, food poisoning, diarrhoea, skin conditions and intestinal parasites/warms in both adults and children all strongly related to hygiene conditions. Food handling and vending was pointed out by health specialists as one contributor to the ailments.
The water and sanitation bit pose more public health related concerns. As the water shortage continues the locals find an alternative means to bridge the gap to ensure their normal lives is not drastically affected. The same was also noted with the failure by the landlords and municipal council to connect houses to a functioning sewerage system, septic tanks are bit to act as holding area for human waste before it drains its content in to wells sunk to serve the purpose sewerage system would have served.
12%
8%
5%
8%
12%
12%
14%
6%
10%
14%
Community Vulnerability on Weighted Basis Water and Sanitation
Roads and Infrastruc-tureInsecurityInadequate Health Services Delivery PointLandlessness/Squat-tersSlums/Informal Set-tlementsHousing ProblemsUnemployementDrug Trafficking and AbusePoverty
Fig 10. Community vulnerability on weighted basis
b. Roads and Infrastructure
The locations studied being mostly urban, the main roads network is tarmac/macadam roads not prone to flooding. However, an analysis of the feedback on roads showed that the connecting and main roads were designed for low volumes of traffic to facilitate movement of vehicles from the mainland to the island, it was also realized that the roads are narrow and characterized by heavy traffic jams apparently an indication that the roads are overwhelmed, particularly by heavy commercial vehicles in Changamwe, Miritini, Mikindani and Port Reitz causing heavy snarl up of vehicles.
18 | P a g e

The roads serving the residential areas are mainly all weather and marrum roads. The transect walks and direct observation noted that most of the access routes have been blocked by barricades and tyres leaving only space passable by foot and not vehicles. An interview of the locals showed this as a mitigation measure against insecurity in the areas. However, in disaster risk reduction, it was noted that this pose more danger to the locals but they are unaware as in case of an emergency it would be difficult for the response teams to carry out any meaningful assistance especially when it is fire related. The access routes are characterized by individual footpaths rather than known and designated roads and leave-ways. The results also showed that the road networks existing in the eleven locations are overwhelmed and unable to handle the nature of traffic it currently experiences. Some of the interior roads are floods prone with bridges suffering the brunt of storm water during the rainy season especially in Shika Adabu, Chaani, Miritini and Mikindani. The sewerage pipe serving Mikindani collapsed after being washed away by storm water and has not been repaired, the effect is, the sewerage effluent drains into Changamwe to Chaani posing more serious health threat to close to 150,000 people.
c. Houses and Housing Type
The common house type in the area of study was evidently in two kinds, a.) Swahili Type and b). Block type houses found mostly in all the locations with exception to Ganjoni, Shimanzi and Tononoka that have flats and maisonette type while Majengo and Mwembe Tayari has a mixture of flats, swahili and block houses with iron sheet roofing.
In terms of vulnerability of the household to disasters, it was evident that the Swahili type is more prone to all manner of hazards and risk; this was after a careful assessment of the type of risks on a weighted scale pertaining to a specific area. High risk areas were found to be predominately Swahili type housing areas, this was also supported by the community through the number of mentions during hazard mapping exercise. This can also be seen by the number of cases reported outside Mombasa Island as compared to the island which is substantially built. The problem is more pronounced and worst case scenarios in Mikindani, Miritini Shika Adabu, Chaani, Port Reitz and Changamwe. In terms of Districts, Changamwe is far much worse.
Safety of the houses looking at age, construction type, alarm and the capability to withstand fire for sometime before the arrival of fire brigade was found to be zero, as the materials used and the type of housing are highly flammable. The results also indicated lack of supervision during construction to ascertain standards and quality after approval is granted, every builder constructs as pleased, and this is evident in how the houses are laid out in a particular area, facing no particular direction. More interesting was the government owned houses which were found to be very old, unsafe and dilapidated but still have people living in them especially in Changamwe, Shimanzi and Tononoka.
The study finds the residential areas under the VCA to be extremely dirty, polluted and water logged in most places with Ganjoni being average. This can also be attributed to the type of housing, the Swahili type of houses encourages communal utilization of facilities like water points, toilets and common areas which further makes it difficult to maintain and control sanitation and general hygiene. The houses also lack toilet facilities, the few that are lucky to have, are inadequate and not connected to a sewerage system. The houses are prone and susceptible to flooding and fire due to their construction, materials and closeness to each other.
19 | P a g e

d. Accessibility to health and health facilities
Health facilities are spread out all over Mombasa County with some privately owned and others government owned, yet lacking adequate services, delivery points and personnel. Most of the facilities are shells providing no more than first aid services upto 5 O’clock in the evening when they close for the day. This quickly translates to lack of emergency Medicare services that are affordable and within the reach of the locals. Any cases of emergency are referred to Port Reitz Hospital for those living in the West Coast and the Coast Provincial General Hospital for those living in Likoni and Mombasa sometimes being too late especially for women in labour characterizing the high number of facility maternal mortality rates. Likoni faces the worst scenario in terms of emergency preparedness and care, with only one public health facility and a dozen dispensaries and private clinics, all the cases are referred to Mombasa for more improved attention, there are no known bed capacity for other ailments apart from 12 beds that cater for maternity cases. The furthest point in Shika Adabu to the Health Centre in Likoni is averagely 12 Kms while to Coast Provincial General Hospital is averagely 25Kms. The results also showed that most people prefer to recuperate at home than use the busy and congested ferry services to seek treatment in Mombasa Island.
Ferry Services was identified as one of the biggest hurdle in accessing health care for people living in the South Coast, it is a tiring and painful process for ailing and sick people, by the time they get to the hospital their condition has worsen. More sad for pregnant mothers with complications and require emergency operations. Gender considerations indicate that women seek Medicare more than men, this is salient in the number of women being treated or seeking various outpatient treatment services in the health facilities, the number of women being much higher than that of men.
5.5 Disaster Preparedness Capacity
Capacity Assessment was categorized in three levels household, community and individual. The interpretation was at what point would any level intervene in the event of a disaster, how and by what means? More surprising was the lack of exhaustive ideas on the capacities individuals and households posses. At the community level capacities were more pronounced due to the local initiatives put in place, notably was the establishment of community disaster management committees to disseminate and create awareness and continuous knowledge development including monitoring of early warning system.
Floods, fire and disease outbreaks are the most common disasters but the preparedness level is lacking this is salient when looking at the number of functioning fire fighting engines and teams which can effectively deal with fire hazards. The fire engines operational in Mombasa were bought in 1976 and only 1 is functioning, the districts also lack water hydrants out of the 164 built only 2 are working indicating the lack of preparedness. Most of the disaster committees at the community lack basic knowledge on disaster management even though, they serve the community and have contributed to reduced cases especially in respect to fire. Floods were attributed to poor drainage facilities and the grabbing of public land by property developers who hardly consider issues of drainage. Those found to be functioning were either clogged or blocked at some point or incomplete draining their content in residential areas and roads this was seen as a challenge and the community has taken local level initiative to reinforce road reserves with sand bags, build drainage and water ways
The results also showed the availability of cash reserves in the Constituency Development Fund (CDF) and local government trust fund (LATF) that can be used to build capacity and or respond to emergencies.
20 | P a g e

Though the funds have not been properly utilized to respond to emergency the community is increasingly getting aware of its existence. Most importantly, there were strong indication of contingency planning by the District Steering Group on Disaster supported by Kenya Red Cross and the DCs Office, the contingency plans are mainly geared towards risks reduction. The existence of corporate organizations both private and public in the areas of disaster management boost the capacity of the county in handling small to medium level disasters. The assessment pointed out the following organizations and the area of interventions.
Table 11. Analysis of organizations and partners
S/No. Organization Area of Intervention1. Kenya Ports Authority (KPA) EWS sea related and fire fighting2. Kenya Maritime Authority (KMA) Search and Rescue-sea, EWS3. Kenya Red Cross Disaster Response-Search and Rescue
both land and sea, DRR4. Kenya Wildlife Service (KWS) EWS, Search and Rescue-sea5. Fire Brigade- Mombasa Municipal Council Fire fighting, search and rescue-land6. Kenya Navy Fire fighting, search and rescue-
sea/land, disaster response7. Kenya Airports Authority Fire fighting8. Kenya Petroleum Refineries Limited Fire fighting9. G4S Security Services Brigade Fire fighting10. St. John’s Ambulance Service First aid services, disaster response.11. Kenya Marine Police Security, search and rescue-sea12. Kenya Police Service (regular) Security 13. Ministry of Public Health and Sanitation Disease surveillance, disaster response,
EWS-health14. Ministry of Medical Services Disaster response
The above organizations have in earnest contributed collectively to the capacity of the local communities to disasters management, supporting the locals to respond to fire cases, disease outbreaks and phenomena that exceed the local capacity to cope.
Community capacity to reduce disaster risks has not been fully tapped, data from Municipal Council of Mombasa Fire Brigaded Department, shows that fire incidences have drastically reduced in the last two years can directly be attributed to the community disaster teams, increased personal awareness and continued surveillance of early warning system. Increased community awareness to disasters has also indicated increased potential at the local levels to reduce vulnerability and disaster risks.
21 | P a g e

6. Summary of the findings
The risks extensively repetitive in the 11 locations are strongly health related, meaning the community vulnerability is contributed by their exposure to health hazards and risks with Diarrhoea and Malaria being the lead causal factors. Skin conditions, intestinal parasites/worms, respiratory conditions and TB can highly be attributed to hygiene levels, pollution, garbage disposals and human/solid waste disposals in the locations studied. Even though, Cholera and Typhoid is repeatedly mentioned and recurrent, data from the specialist indicate isolated cases that are not rampant. Drugs and substance abuse and STDs were the key contributor to the levels of vulnerability among the youth which strongly correlates to the levels of criminal activities, recourse to violence and insecurity among the youth. This also corresponds to the levels of prostitution and HIV/AIDS.
The results also showed that women are more vulnerable to most of the disasters because they are largely presumed to be household or occupational based and they happen where women are likely to be found most of the time, it is an indication that women are likely to be exposed to most risks. The results show that exceptions are however, when it comes to skin diseases, intestinal worms, TB and cholera men are mostly affected, this can be attributed to the nature of work men do especially in Changamwe District that expose them to the hazards. Incidentally, children under 5 years share the same or near level of vulnerability with women, infant mortality and malnutrition rates also are at levels that can be considered as high in this time and era.
Roads and infrastructure poor maintenance have made them prone to flooding in Miritini, Mikindani, Shika Adabu and Port Reitz where bridges and feeder roads are sometimes completely cut off. Health facilities are not properly equipped with materials and personnel to handle the level of cases they do, most are merely first aid posts, holding and stabilizing patients before disposing to hospitals which averagely is about 25Kms or more to the furthest village which was part of the areas of the study. In Chaani, Port Reitz and Mikindani illegal houses are built below or near high voltage electricity lines, gasoline pipelines and petroleum pipelines being more catastrophic further, showing how people place themselves in the path of hazards in these areas.
Severe to acute water shortage levels in the 11 locations have exposed the communities to water contamination due to water vending and handling. This is a practice where water is sold in jerry cans in handcarts, the handling does not follow any universal recognizable or acceptable standards. The effects of this has been poor hygiene standards, diarrhoea, skin conditions, intestinal worms and to worse extents cholera outbreaks. Sanitation largely is another key concern, lack of toilet facilities especially in the slums, collapsed or nonfunctioning sewerage system and uncoordinated disposal of human solid waste is the largest single contributor of the increased levels of health hazards. In most households interviewed, the results indicate the use of septic tanks sunk as wells. Incidentally there are water wells and boreholes supplying the same households with water within the same area and not meeting the required 30m distance for safety of the water for domestic use. The effects corresponding to the situations are cholera, typhoid, diarrhoea, skin conditions which reportedly are rampant. The entire Mombasa County has no well functioning sewerage system, what is referred to as sewerage system serves only 17 percent of the total
22 | P a g e

population. An alarming percentage especially when Mombasa is considered to be the second largest town in the Country.
Landslides are hardly reported and have currently reached devastating levels in Mikindani especially affecting the informal settlements of Bangladesh, the same has also been experienced in Miritini where roads and other essential amenities like water points and toilets have been swept away during the rainy season. RTAs are mainly associated with the highways at Shika Adabu, Mikindani and Miritini. This is also due to narrow roads , heavy tracks and heavy traffic.
Disasters are not frequent in the areas studied, however, the prevailing conditions, living conditions and economic endowment force people to seek cheaper and less costly way of life. This was salient in what the local people call residential areas, very much pronounced in the nature and type of houses found in these places. The house type poses more danger to the locals than they would want to openly admit, prone to flooding, collapse and landslides as they are muddy and mainly thatched or iron sheet roofed or blocks but haphazardly done. Lack of effective services has left gaps in the community that is being exploited by other unscrupulous people. Lack of water and severe shortages has created unregulated water vending which increases water contamination due to the unsafe handling, food kiosks and vending have increased food poisoning and intestinal worms with resultant diarrhoea.
7. Conclusion and Recommendations
Disaster preparedness is generally low, with no clear and distinct authority despite the national disaster policy providing an outline in terms of coordination, response and recovery strategies. At the local level it is equally worse in most cases appealing to government and well wishers to support measures requiring substantial financial commitments. In the study areas it was presumed the DC to be incharge of all disaster operations in the district. The following are the pertinent recommendations made from the results of the VCA process.
1. Prioritize major programs for rigorous monitoring and evaluation. Many programs would benefit from systematic monitoring and evaluation, such as the Constituency Development Fund emergency kitty, disaster management committees, disaster response teams and disaster based organizations. Since strong technical skills in research design, management, analysis and reporting are required, collaboration with independent research institutions can help ensure the quality and credibility of results. This is mainly due to the lack of credible data on how disaster initiatives are carried out, involvement criteria and who are responsible for what and how at the local levels. Management of data is a key concern when it comes to building scenarios as what is available is inadequate with the exception of health records.
2. There is an urgent need to carry out extensive Hygiene and Sanitation awareness to build the capacity of the local people to handle risks and hazards pertaining to health, water and sanitation as these are found to be the key concern and most common on weighted-basis. Collectively they have largely affected community health and safety than any other single occurrence causing epidemics in some areas and increasing vulnerability to high proportions.
3. Community Disaster Committees require more specialized training to be able to monitor early warning system, create awareness and reduce risks to build enough capacity at the local levels for disaster risk reduction. In the 11 locations disaster committees exist but with no clear terms of reference, training
23 | P a g e

nor formal knowledge on managing or coordinating disaster situations, nevertheless disaster committees are underutilized and untapped local resource. The districts were also found to be lacking in disaster preparedness plans, it was also difficult to understand the operations of the existing committees at the district levels and the terms of reference that guide them. The contingency plans were evident and well spelt out, there is a need to share the contingency plans with the local communities, disseminate what is expected from the plans, enforcement terms and criteria and the expectations from the community.
4. Drugs and Substance Abuse especially hard drugs and alcohol contributes to the vulnerability of youth and men who are the majority of the working groups, this shows a trend that might affect and threaten the community livelihood in the long term due to reduced manpower capacity which again will affect household earnings and living standards. Advocacy, lobbying and increased awareness on substance abuse need to be scaled up including security surveillance and law enforcement to eradicate the practice.
5. Enforcement of environmental laws and regulations on solid and liquid waste disposal especially human waste. The areas studied are an eyesore, dirty and polluted in many parts with no sewerage system, poor sanitation, garbage collection and disposal problem and acute water shortage, there is urgent need to lobby jointly with stakeholders for better services to improve community safety.
6. Disaster response is skewed, despite corporate organizations’ presence and willingness to assist during disasters, the coordination is lacking, and this is evident in the manner in which disasters are managed. The local communities and stakeholders need to develop a system for coordination and management of disaster situations to improve efficiency and reduce the interface between disaster occurrence and the vulnerable community.
7. Concerted efforts to track and explore predictive mechanisms for various disasters have not been made, the efforts currently are reactive and preemptive rather than preventive. Historical profiles of disasters from the communities indicate a consistency of occurrence and impacts of the same disasters almost on a yearly basis and the local people would tell you the same things over and over. Stakeholders and partner’s consultation and collaborations need to be strengthened through more networking, joint/inter-agency planning and further research.
8. Public Health Department needs to be integrated in the enforcement of regulations and continued public education as the laws are largely violated in the 11 locations studied. This would bring about improvement of living conditions, personal hygiene and sanitation levels to reduce health hazards. More public education on child and maternal health to reduce the malnutrition among children under 5 years and their mothers.
9. Disaster Risks Reduction programmes in Mombasa need to focus more on community education, awareness and continued knowledge development, capacity building and training as a means to recruit and enlist local support and get the people to take action through their own initiatives to bring about much needed transformation.
References
24 | P a g e

1. Assessment of Severe Malnutrition Among Hospitalized Children in Rural Kenya Comparison of Weight for Height and Mid Upper Arm Circumference: http://motherchildnutrition.org/resources/pdf/mcn-comparison-of-weight-for-height-and-mid-upper-arm-circumference.pdf
2. Urban Slums Mass Screening Report, November 2010 GoK/FHI/UNICEF
3. Kilindini District Development Plan 2008-2012, Government Printers Nairobi June 2009, Office of the Prime Minister, Ministry of State for Planning, National Development and Vision 2030
4. FAO (1990), The Toolbox: the idea, methods and participatory assessment, monitoring, evaluation in community forestry. D’Arcy Davis Case: http://www.fao.org/documents/show_cdr.asp?url_file=/docrep/x5307e/x5307e00.htm
5. Development Association for Self-reliance, Communication and Health. Participatory Rural Appraisal on Health
6. VCA Toolbox International Federation of the Red Cross and Red Crescent Societies 2008
7. Mombasa District Development Plan 2008-2012, Government Printers Nairobi June 2009, Office of the Prime Minister, Ministry of State for Planning, National Development and Vision 2030
8. Ross, John(1999)Ways of Approaching Research: Quantitative Designs, http://www.fortunecity.com/greenfield/grizzly/432/rra2.htm
9. Interworks (2001), Disaster Management Community Baseline Data, Jim Good and Charles Dufresne; www.interworksmadison.com
10. A Guide to Library Research Methods: Thomas Mann, Oxford University Press, ISBN 0195049446.1987
11. BPI reference, International Federation of the Red Cross and Red Crescent Societies, (2003) Aid: Supporting or undermining recovery? Lessons from the BPI, international Federation, Geneva.
12. Catholic Relief Services (1999), Rapid Rural Appraisal and Participatory Rural Appraisal Manual, K. Freudenberger.
13. Institute of Economic Affairs 2008: Socio-economic impacts and political profile of Kenya
14. Kenya Poverty and Inequality Assessment Volume I: Synthesis Report June 2008. Report No. 44190-KE WORLD BANK
15. National Disaster Management Policy Sessional Paper, Office of the President, Ministry of State for Special Programme 2006.
Appendix 1:
25 | P a g e

List of the Locations under the Study Area alphabetically
1. Chaani2. Changamwe 3. Ganjoni 4. Majengo 5. Mikindani6. Miritini7. Mwembe Tayari 8. Port Reitz9. Shika Adabu10. Shimanzi 11. Tononoka
Appendix 2:
List of respondents/key informants/ stakeholders interviewed
Stakeholders/partners
1. Kenya Wildlife Services2. Kenya Maritime Authority3. Ministry of Public Health and Sanitation
26 | P a g e

4. Municipal Council of Mombasa-Fire Brigade5. Office of the President6. Ministry of Medical Services-District Health Records Department
Key informants
1. Chiefs: Miritini, Mikindani, Shika Adabu, Chaani, Majengo2. Village Elders (11 locations)3. Women Leaders4. Opinion Leaders5. Youth Leaders
Focus interest groups
1. Business people2. Vendors3. Local hawkers
Appendix 3: VCA Checklist
Community checklist baseline data collection questionnaires
a. Susceptibility to Disasters - What people are most at risk during disasters (age, gender, occupation, area)?- In what specific ways are they vulnerable?- What are the causes of their vulnerability?- How frequent are the disasters?- What items are valued most as the key contributors to the locals’ livelihoods?- What challenges ahs the community faced when it comes to disasters over space and time (probable time/recurrence)?- What makes the community so vulnerable to disasters?- What is the impact of the problem/challenges so far?- Who are the most vulnerable (children, women, men, youth)?
27 | P a g e

b. Susceptibility, Health and Nutritional Conditions- What rate is infant mortality in this community?- Most common illness among the general population (measles, HIV/AIDS, influenza, pneumonia, dengue, cholera, etc)?- Nutritional rate for children under 5 years?- Most common illness among children and youth (meningitis, pneumonia, measles, diarrhoea, intestinal parasites)?- Is there public education on health issues? yes/no- Public education received by whom and on what health issues i.e. malaria, pre-natal care, HIV/AIDS, disease, sanitation
c. Availability of Health Services- What types of clinics are available?- How far is the nearest health facility/clinic?- Where is the nearest health facility/clinic?- What health services can you get at the community levels?- How big in terms of bed capacity is the facility(s)?- What is the average number of beds available at any given time?- How many nurses are available as residents in the community?- How many resident physicians are available in the community?- What is the number of public health or maternal and child health are agents in the community?
d. Physical Community Susceptibility - Vegetation covering (trees, grasses, open agricultural areas, mainly open with occasional tree covering, heavily wooded)- Grade (construction of buildings; are they built on level ground (0-2%) or low slope (3-5%) or medium slope (5-10%) or high
slope (above 10%)- Situation of community on or near streams that do or may flood (river banks-not elevated structures, river banks- but
elevated structures, flood plain, high ground.- What are the important physical structures, buildings and infrastructure most vulnerable to disasters?- List what types of disasters they are vulnerable to?
e. Infrastructure and Access Infrastructure- What type of road is available to access the community? Concrete, Asphalt, Macadam/gravel/limestone, unpaved/dirt,
vulnerable to flooding, mudslides?- Bridges (are there any existing bridges leading to the community? Types of bridges, vulnerable to flooding?- Power (local overhead electricity distribution, local generator and network, individual only/generators, no electrification)- Communications (Radio, telephones, fax, email. which types, who, where)
f. Access to Food, Water, Housing and Shelter and Sanitation- Basic housing construction type- Other prominent types in the community- Average housing size- Availability of emergency shelter- Location of mass shelter- Condition and type of construction for emergency shelter
- What is the water source for the community?- Is there a Water source vulnerable to flooding?- Any water source dependant on electrical pumps?- Quality of the drinking water- Potable- Non potable, but not polluted?- Polluted source
28 | P a g e

- Describe typical sanitation in use by individuals.- What is the Sanitation arrangement in use for mass shelters? - Are sanitation arrangements adequate for the number of people to be housed in the shelter?
g. Disaster Preparedness/Planning Capacity/EWS- Is there any existing disaster preparedness and response plan in place?- Who is the primary contact, how long has it been in existence?- Does the community have community-based response teams?- What are the linkages between the community and other actors?- What is early warning system?- Is there an early warning system?- Are community members familiar with it and what it means?- If yes, do community members consider it to be a reliable system?- Has this early warning system been used successfully in the last five years?- Does the community recognize and respect those with the authority to announce an evacuation?- Has the evacuation plans been used successfully in the last five years? - What emergency response skills and resources exist in the community (e.g. public health, first aid, sanitation)?- Has the community participated in the emergency response, evacuation drills and simulations before?- Damage Assessment and Needs Assessment.
h. Community available Capacity for Response and Mitigation of Disasters- What are the existing social capitals?- Physical/material resources and capacities.- Technical skills/human resources in the community- Social/organizational capacities in the community- Critical safe facilities- Cash reserves
i. Economic Endowment- What nature of economic activities do the locals engage in?- Is there a diversified local economy?- What are the main sources of livelihoods for the local people?- How is the land tenure and ownership?
Semi-Structured Interviews and FGDs
- What are the problems caused by disasters in the community?- What are the overall coping strategies and the community motivation?- What do you think could be the solutions?- What are the coping strategies for each specific area addressed?- What are some of the constraints and pitfalls in managing disasters?- What are the roles of the different agencies in disaster mitigation?- What kind of assessment has the (local) government carried out, and did it involve the community?- What do most people do when affected/victims of disasters?- Are losses and damages incurred during disasters more/less frequent than in the past?- Do you have a community disaster response team/committee/management team?- Is there a disaster contingency/response/preparedness plans? When was it developed? Has it been operationalized? What
is the community and stakeholders response?- Who is responsible for disaster coordination?
29 | P a g e

Organizational Assessment/Appraising Partners
- What kind of an organization is it? Is it social, political or commercial?- When was it established, area of operations, what is its relations with the local community?- For what purpose was it formed?- How many members are there? Active/Passive. Is it on the increase or decrease?- How do you make your decisions? What is the attendance?- Do you have a community development plan? Is the organization functioning?- What contribution have you made to the community?- What resources does your organization have that can contribute towards disaster risk reduction (skilled personnel, financial
resource, equipment, materials, and facilities)? - Who has the highest level of authority in this community?- Who has the highest level of government affiliation or authority in the community?- Who has the highest authority; religious groups, CSOs?- What NGOs and local community-based organizations exist in the community? What are the areas of programming and
expertise?
a. Do the respondents understand disaster response mechanisms Yes No Not exactly/Not sure Don’t Know
b. Knowledge level among the community level on disaster Understand Don’t Understand Not Sure
c. Wealth Ranking Level of Income Earnings Economic Activities
Appendix 4. Photographs
1. Graphic presentation of the areas studied
30 | P a g e

31 | P a g e

32 | P a g e

33 | P a g e

34 | P a g e

35 | P a g e

36 | P a g e

37 | P a g e