Embed Size (px)
Citation preview
Clinical Study Report
Clinical efficacy assessment of
Vcheck cPL and fPL
Requested by: Sun-Ae Kim, Managing Director, BioNote Inc.
Research institute: Haemaru Referral Animal Hospital Small Animal Clinical Research
Institute
Principal investigator: Sun-Young Hwang, Haemaru Referral Animal Hospital Small
Animal Clinical Research Institute
Product name: Vcheck cPL test
Vcheck fPL test
Study period: 3 months (1st March, 2018 ~ 30th June, 2018)
Managing Director, Haemaru Co. Ltd.
Hyun-Wook Kim (sealed)
I. Research background
Pancreatitis is one of the most common disorder associated with pancreatic endocrine dysfunction in
cats and dogs. Although pancreatitis is usually caused by inflammation of the pancreas, it can also be
caused by necrosis or fibrosis, resulting in a complex presentation that is not only related to
inflammation. Therefore, in order to make a proper diagnosis, the history taking, clinical symptoms,
and clinical pathological test results need to all be considered in combination.
Due to the difficulties in diagnosing pancreatitis, several tests are employed for more accurate, faster
diagnosis. The essential tests in patients suspected of having pancreatitis are complete blood count,
serum biochemistry profile, and urinalysis. However, this tests can also show abnormal values in other
diseases, and are lacking specificity for pancreatitis. A number of studies have been conducted to
explore biomarkers with high specificity, such as serum amylase and lipase activity, or trypsin-like
immunoreactivity (TLI) levels. But these methods still do not show sufficient specificity.
Recently, the pancreatitis biomarker with the highest specificity in cats and dogs is serum pancreatic
lipase (PL). Measuring PL and also performing abdominal ultrasonography is known to be useful for
excluding other diseases with similar clinical symptoms to pancreatitis. While abdominal
ultrasonography alone might have very high specificity for diagnosing pancreatitis, it has low sensitivity,
and interpretation of the results is also highly affected by the examiner’s experience. As a quantitative
indicator, PL measurement is a powerful method to make up for the limitations of abdominal
ultrasonography.
Ultimately, the gold standard diagnostic technique is pancreatic biopsy. However, the tissue sampling
procedure for biopsy is a major burden for both the examiner and the patient. Therefore, in a clinical
setting, the most realistic choice is close observation of clinical symptoms combined with PL
measurement and abdominal ultrasonography.
Currently, the most commonly used commercial PL measurement devices in veterinary medicine in
South Korea are IDEXX SPEC and SNAP. But recently, BioNote has developed a test kit that can be
applied to Vcheck series for rapid, quantitative measurement of PL immunoreactivity (PLI). In this
study, we measured PL using IDEXX SPEC and SNAP, and BioNote Vcheck in cats and dogs who
visited our hospital with suspected pancreatitis, and assessed the usefulness of Vcheck cPL and fPL test
in clinical veterinary medicine.
II. Methods
1. Objective
The objective of this study was to assess the clinical efficacy of the “Vcheck cPL, fPL test kit”,
which are diagnostic test kits using immunochromatography, that are developed and sold by
BioNote Inc. For the efficacy assessment, we analyzed the sensitivity, specificity, and reference
range, and compared the performance with products from competitors.
2. Control groups
(1) At least 20 dogs diagnosed as not having pancreatitis by a veterinarian (patients showing
no effect on peak serum cPL)
(2) At least 5 cats diagnosed as not having pancreatitis by a veterinarian (patients showing no
effect on peak serum fPL)
3. Test groups
(1) At least 20 dogs diagnosed with pancreatitis by a veterinarian
(2) At least 5 cats diagnosed with pancreatitis by a veterinarian
4. Test items
(1) CBC
(2) Serum chemistry (Amylase, Lipase)
(3) Ultrasonography
(4) Clinical symptoms (compulsory)
(5) Vcheck canine CRP or feline SAA (compulsory)
(6) Vcheck cPL or fPL (compulsory)
(7) IDEXX SNAP cPL or fPL (compulsory)
(8) IDEXX SPEC cPL or fPL (compulsory)
(9) In order to exclude or confirm pancreatitis, Items (4)~(8) were compulsory. The definitive
diagnosis for pancreatitis was made by a veterinarian after performing the necessary tests
from among CBC, serum chemistry, and ultrasonography.
III. Results
1. Correlation analysis of cPL and pancreatitis diagnosis/symptoms in dogs
(1) Correlation between BioNote Vcheck cPL measurements and IDEXX SPEC cPL
measurements
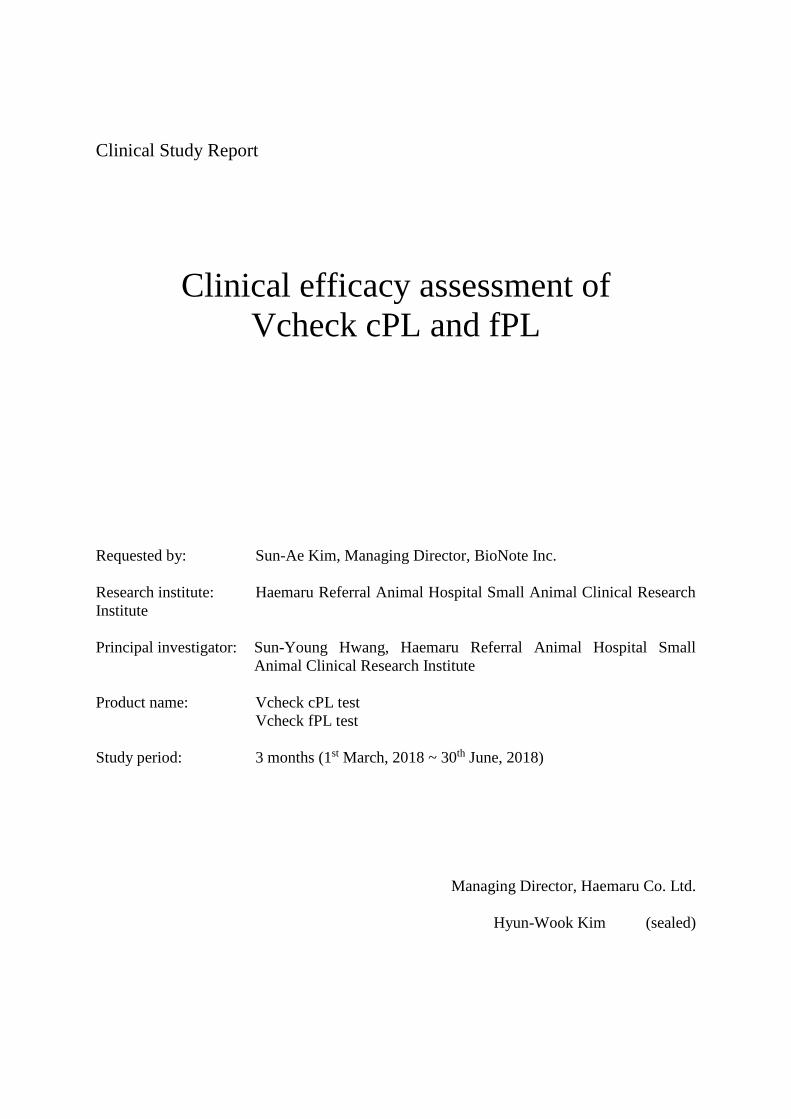
1) Among the total of 54 total dogs in which measurements were taken, 2 were excluded
due to missing SPEC cPL measurements, and paired measurements from the
remaining 52 were used to compare Vcheck cPL and SPEC cPL. In the graph, all
measurements < 50 ng/mL are displayed as 49.9 ng/mL and all measurements > 2000
ng/mL are displayed as 2000.1 ng/mL.
Figure 1. Comparison of BioNote Vcheck cPL measurements and IDEXX SPEC cPL measurements
in dogs
2) As shown in Fig. 1 above, Vcheck cPL and SPEC cPL showed a strong correlation,
with R2 > 0.95 (𝑦=0.98𝑥+13.76, R2=0.958). The correlation coefficient could increase
if the values outside of the equipment’s measurement range were shown as absolute
values.
3) In terms of the reference ranges, the normal range for both Vcheck cPL and SPEC cPL
is defined as 0 ~ 200 ng/mL, meaning that measurements > 200 ng/mL are defined as
elevated cPL (the sparse dotted line in Fig. 1). Meanwhile, both test methods defined
measurements > 400 ng/mL as consistent with pancreatitis (the dense dotted line in
Fig. 1).
4) Apart from one patient (‘a’ in Fig. 1), the interpretation of all results was the same with
respect the reference value of 200 ng/mL. For patient ‘a’, the result for Vcheck cPL
(228 ng/mL) was above the upper limit of the reference range, while the result for
SPEC cPL (138 ng/mL) was within the reference range. Patient ‘a’ (ID 201800368)
visited the hospital on 30th of March, presenting with a enterocutaneous fistula caused
by the products of inflammation in the caudal pole of the right kidney, as well as
inflammation in the pancreas and right ureter caused by adjacent granulomatous tissue
result from inflammation secondary to the fistula. In abdominal ultrasonography, the
margin of the pancreas was poorly defined, and the adjacent mesentery was
hyperechoic, indicating the possibility of mild pancreatitis. The IDEXX SNAP result
was also interpreted as abnormal (indicated by the green color in the graph). Therefore,
the elevated cPL result of Vcheck cPL is considered to have aided diagnosis in this
patient, while the SPEC cPL result was found to be detrimental to the diagnosis.
5) Meanwhile, based on the threshold value of 400 ng/mL for ‘consistent with
pancreatitis’, the result of patient ‘c’ was below the threshold when using Vcheck cPL
(292 ng/mL), but above the threshold when using SPEC cPL (655 ng/mL). This patient
(ID 200701136) visited the hospital on 14th of March, presenting with symptoms
caused by protein-losing enteropathy (PLE). The right lobe of the pancreas was
hyperechoic in abdominal ultrasonography, and the patient was diagnosed with
chronic pancreatitis. Although the results of the two tests cannot be considered
completely consistent with each other in this patient, they both showed values > 200
ng/mL, indicating elevated cPL, and so neither test was found to be detrimental to the
diagnosis.
6) In addition, there were two patients that showed different results for SPEC and SNAP
(‘b’ in Fig. 1). However, the interpretation of SNAP close to the limits of the reference
range is unclear, and the IDEXX user manual also recommends that, in such cases, the
SPEC test should also be performed. Therefore, we considered this a situation that
could arise commonly.
(2) Comparison of BioNote Vcheck cPL and IDEXX SPEC cPL measurements with
definitive diagnosis
1) Of all patients, for the 38 first-time patients, pairs of measurements were compared
with the definitive diagnosis considering of clinical symptoms and findings in
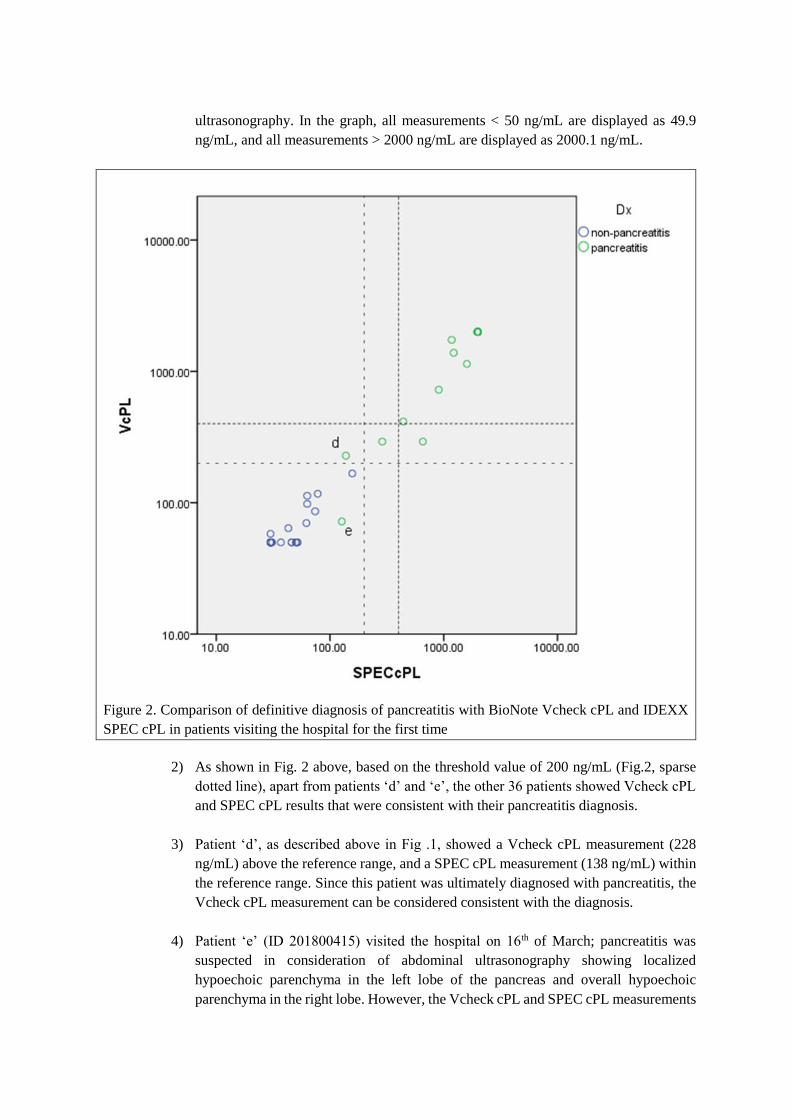
ultrasonography. In the graph, all measurements < 50 ng/mL are displayed as 49.9
ng/mL, and all measurements > 2000 ng/mL are displayed as 2000.1 ng/mL.
Figure 2. Comparison of definitive diagnosis of pancreatitis with BioNote Vcheck cPL and IDEXX
SPEC cPL in patients visiting the hospital for the first time
2) As shown in Fig. 2 above, based on the threshold value of 200 ng/mL (Fig.2, sparse
dotted line), apart from patients ‘d’ and ‘e’, the other 36 patients showed Vcheck cPL
and SPEC cPL results that were consistent with their pancreatitis diagnosis.
3) Patient ‘d’, as described above in Fig .1, showed a Vcheck cPL measurement (228
ng/mL) above the reference range, and a SPEC cPL measurement (138 ng/mL) within
the reference range. Since this patient was ultimately diagnosed with pancreatitis, the
Vcheck cPL measurement can be considered consistent with the diagnosis.
4) Patient ‘e’ (ID 201800415) visited the hospital on 16th of March; pancreatitis was
suspected in consideration of abdominal ultrasonography showing localized
hypoechoic parenchyma in the left lobe of the pancreas and overall hypoechoic
parenchyma in the right lobe. However, the Vcheck cPL and SPEC cPL measurements
were both < 200 ng/mL. This patient had previously been diagnosed with pancreatitis
at another clinic, and so we believe that, while the pancreatitis had not been completely
cured, cPL level has been improved by the fluid therapy provided at that clinic.
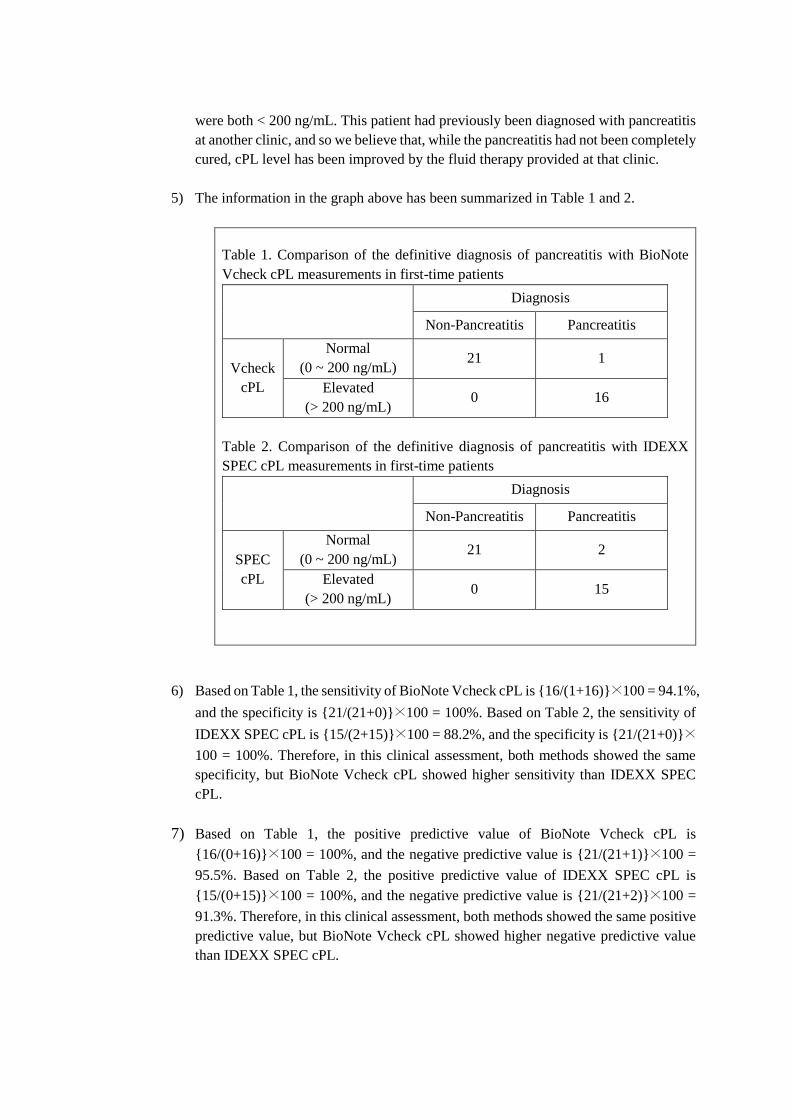
5) The information in the graph above has been summarized in Table 1 and 2.
Table 1. Comparison of the definitive diagnosis of pancreatitis with BioNote
Vcheck cPL measurements in first-time patients
Diagnosis
Non-Pancreatitis Pancreatitis
Vcheck
cPL
Normal
(0 ~ 200 ng/mL) 21 1
Elevated
(> 200 ng/mL) 0 16
Table 2. Comparison of the definitive diagnosis of pancreatitis with IDEXX
SPEC cPL measurements in first-time patients
Diagnosis
Non-Pancreatitis Pancreatitis
SPEC
cPL
Normal
(0 ~ 200 ng/mL) 21 2
Elevated
(> 200 ng/mL) 0 15
6) Based on Table 1, the sensitivity of BioNote Vcheck cPL is {16/(1+16)}×100 = 94.1%,
and the specificity is {21/(21+0)}×100 = 100%. Based on Table 2, the sensitivity of
IDEXX SPEC cPL is {15/(2+15)}×100 = 88.2%, and the specificity is {21/(21+0)}×
100 = 100%. Therefore, in this clinical assessment, both methods showed the same
specificity, but BioNote Vcheck cPL showed higher sensitivity than IDEXX SPEC
cPL.
7) Based on Table 1, the positive predictive value of BioNote Vcheck cPL is
{16/(0+16)}×100 = 100%, and the negative predictive value is {21/(21+1)}×100 =
95.5%. Based on Table 2, the positive predictive value of IDEXX SPEC cPL is
{15/(0+15)}×100 = 100%, and the negative predictive value is {21/(21+2)}×100 =
91.3%. Therefore, in this clinical assessment, both methods showed the same positive
predictive value, but BioNote Vcheck cPL showed higher negative predictive value
than IDEXX SPEC cPL.
(3) Correlation between cPL levels and improvement of clinical symptoms in patients
who visited multiple times
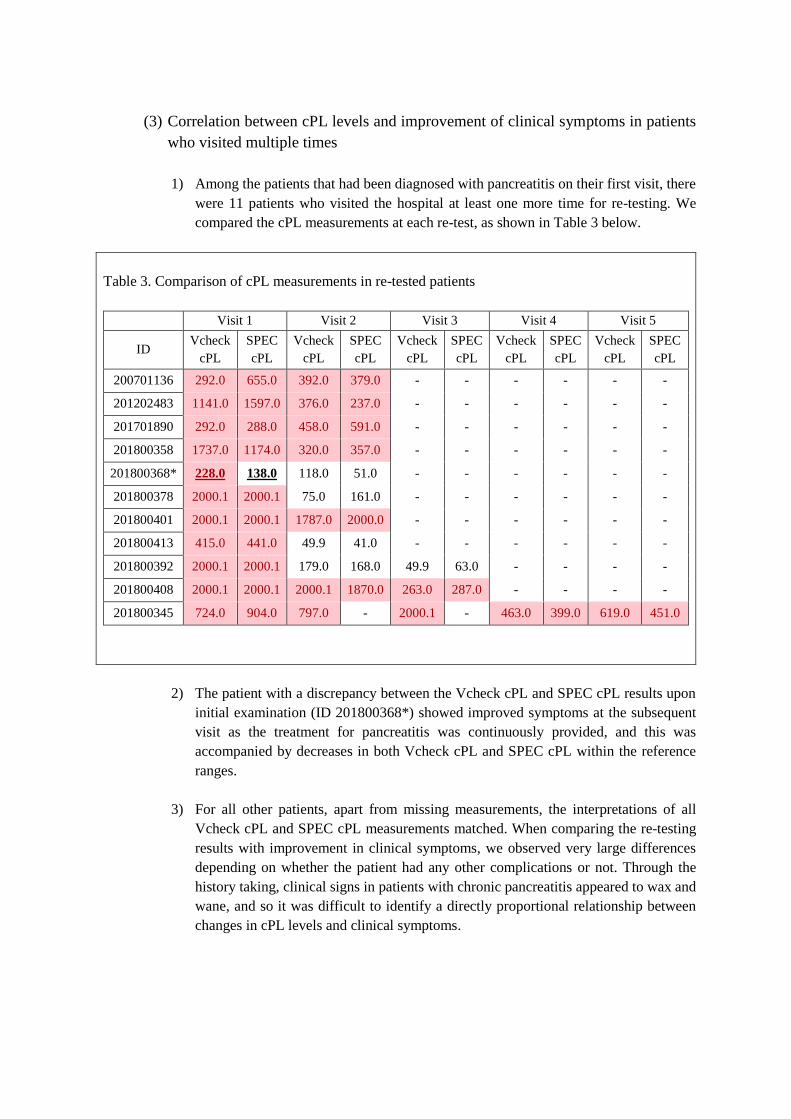
1) Among the patients that had been diagnosed with pancreatitis on their first visit, there
were 11 patients who visited the hospital at least one more time for re-testing. We
compared the cPL measurements at each re-test, as shown in Table 3 below.
Table 3. Comparison of cPL measurements in re-tested patients
Visit 1 Visit 2 Visit 3 Visit 4 Visit 5
ID Vcheck
cPL
SPEC
cPL
Vcheck
cPL
SPEC
cPL
Vcheck
cPL
SPEC
cPL
Vcheck
cPL
SPEC
cPL
Vcheck
cPL
SPEC
cPL
200701136 292.0 655.0 392.0 379.0 - - - - - -
201202483 1141.0 1597.0 376.0 237.0 - - - - - -
201701890 292.0 288.0 458.0 591.0 - - - - - -
201800358 1737.0 1174.0 320.0 357.0 - - - - - -
201800368* 228.0 138.0 118.0 51.0 - - - - - -
201800378 2000.1 2000.1 75.0 161.0 - - - - - -
201800401 2000.1 2000.1 1787.0 2000.0 - - - - - -
201800413 415.0 441.0 49.9 41.0 - - - - - -
201800392 2000.1 2000.1 179.0 168.0 49.9 63.0 - - - -
201800408 2000.1 2000.1 2000.1 1870.0 263.0 287.0 - - - -
201800345 724.0 904.0 797.0 - 2000.1 - 463.0 399.0 619.0 451.0
2) The patient with a discrepancy between the Vcheck cPL and SPEC cPL results upon
initial examination (ID 201800368*) showed improved symptoms at the subsequent
visit as the treatment for pancreatitis was continuously provided, and this was
accompanied by decreases in both Vcheck cPL and SPEC cPL within the reference
ranges.
3) For all other patients, apart from missing measurements, the interpretations of all
Vcheck cPL and SPEC cPL measurements matched. When comparing the re-testing
results with improvement in clinical symptoms, we observed very large differences
depending on whether the patient had any other complications or not. Through the
history taking, clinical signs in patients with chronic pancreatitis appeared to wax and
wane, and so it was difficult to identify a directly proportional relationship between
changes in cPL levels and clinical symptoms.
2. Correlation analysis of fPL and pancreatitis diagnosis/symptoms in cats
(1) Correlation between BioNote Vcheck fPL measurements and IDEXX SPEC fPL
measurements
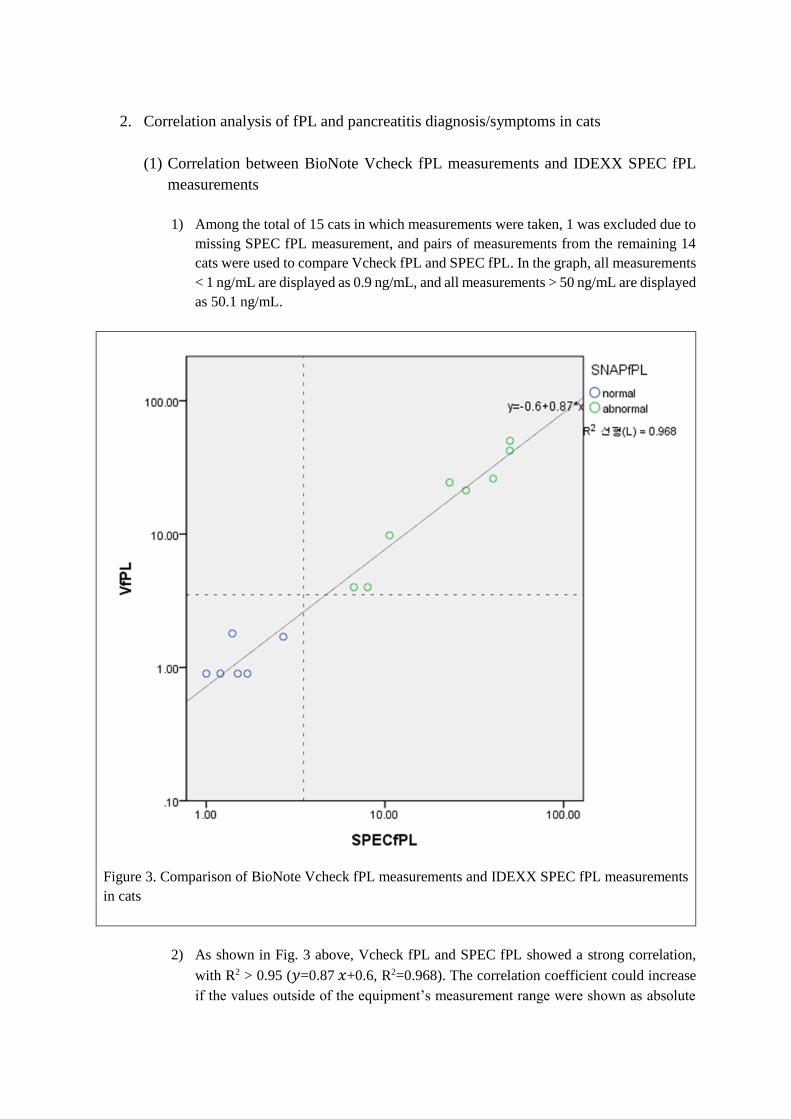
1) Among the total of 15 cats in which measurements were taken, 1 was excluded due to
missing SPEC fPL measurement, and pairs of measurements from the remaining 14
cats were used to compare Vcheck fPL and SPEC fPL. In the graph, all measurements
< 1 ng/mL are displayed as 0.9 ng/mL, and all measurements > 50 ng/mL are displayed
as 50.1 ng/mL.
Figure 3. Comparison of BioNote Vcheck fPL measurements and IDEXX SPEC fPL measurements
in cats
2) As shown in Fig. 3 above, Vcheck fPL and SPEC fPL showed a strong correlation,
with R2 > 0.95 (𝑦=0.87 𝑥+0.6, R2=0.968). The correlation coefficient could increase
if the values outside of the equipment’s measurement range were shown as absolute
values.
3) In terms of the reference ranges, the normal range for both Vcheck fPL and SPEC fPL
is defined as 0 ~ 3.5 ng/mL, meaning that measurements > 3.5 ng/mL are defined as
elevated fPL (the sparse dotted line in Fig. 3).
4) Using a threshold value of 3.5 ng/mL, the interpretations of both tests were the same
for all cats. The interpretations of SPEC and SNAP results were also all concordant.
(2) Comparison of BioNote Vcheck cPL and SPEC fPL measurements with definitive
diagnosis
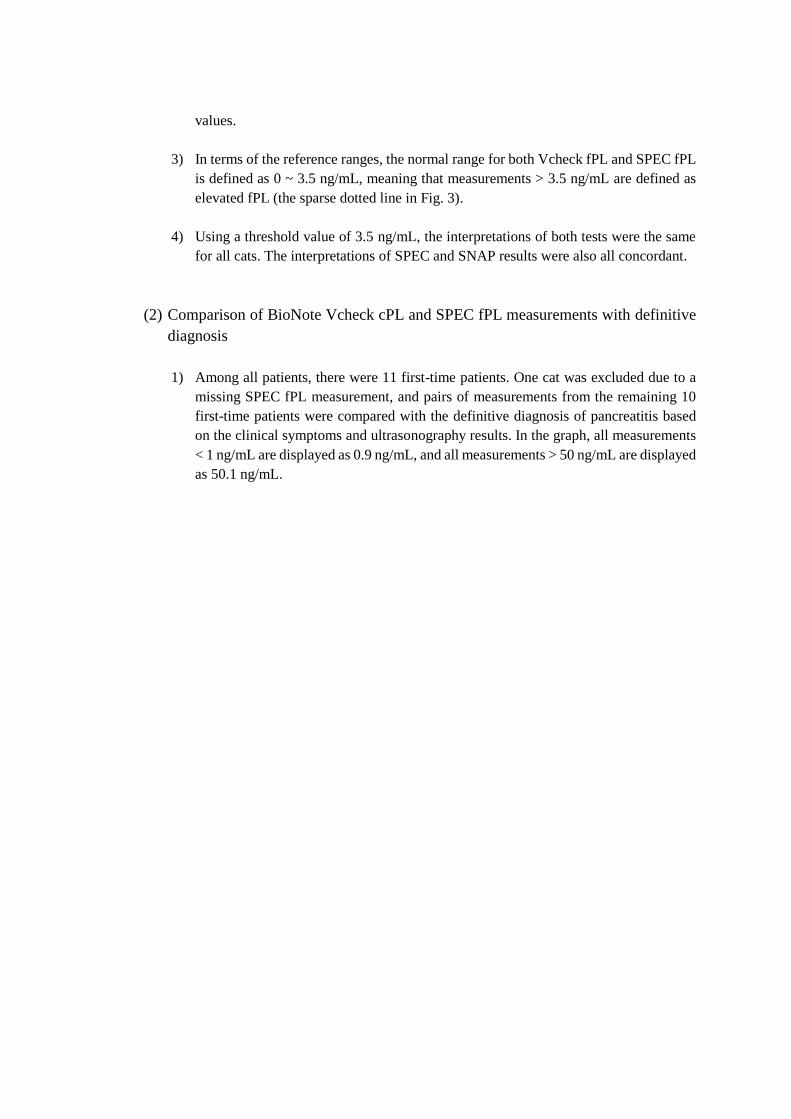
1) Among all patients, there were 11 first-time patients. One cat was excluded due to a
missing SPEC fPL measurement, and pairs of measurements from the remaining 10
first-time patients were compared with the definitive diagnosis of pancreatitis based
on the clinical symptoms and ultrasonography results. In the graph, all measurements
< 1 ng/mL are displayed as 0.9 ng/mL, and all measurements > 50 ng/mL are displayed
as 50.1 ng/mL.
Figure 4. Comparison of definitive diagnosis of pancreatitis with BioNote Vcheck fPL and IDEXX
SPEC fPL in patients visiting the hospital for the first time
2) As shown in Fig. 4 above, using a threshold value of 3.5 ng/mL (Fig. 4, sparse dotted
line), Vcheck fPL and SPEC fPL measurements were consistent with the pancreatitis
diagnosis in all 10 cases.
3) The information in the graph above is summarized in Table 4 and 5.
Table 4. Comparison of BioNote Vcheck fPL measurements and pancreatitis
diagnosis in first-time patients
Diagnosis
Non-Pancreatitis Pancreatitis
Vcheck
fPL
Normal
(0 ~ 3.5 ng/mL) 5 0
Elevated
(> 3.5 ng/mL) 0 5
Table 5. Comparison of IDEXX SPEC fPL measurements and pancreatitis
diagnosis in first-time patients
Diagnosis
Non-Pancreatitis Pancreatitis
SPEC
fPL
Normal
(0 ~ 3.5 ng/mL) 5 0
Elevated
(> 3.5 ng/mL) 0 5
4) Based on Tables 4 and 5, the sensitivity and specificity of BioNote Vcheck fPL and
IDEXX SPEC fPL were all 100%. In addition, the positive predictive value and
negative predictive value of both tests were also 100%. Although we cannot consider
these results to be reliable due to the low sample size, within this clinical assessment,
both BioNote Vcheck fPL and IDEXX SPEC fPL were shown to be helpful for
diagnosing pancreatitis in cats.
(3) Correlation between fPL levels and improvement of clinical symptoms in patients
who visited multiple times
1) Among the patients that had been diagnosed with pancreatitis on their first visit, there
were 4 patients who visited the hospital at least one more time for re-testing. We
compared the fPL measurements at each re-test, as shown in Table 6 below.
2) Excluding only the patient with a missing SPEC fPL measurement at the initial visit,
the interpretations of the Vcheck fPL and SPEC fPL measurements matched with each
other in re-tests.
3) When comparing the re-testing results with improvement in clinical symptoms, we
observed very large differences depending on whether the patient had any other
complications or not. Through the history taking, clinical signs in patients with chronic
pancreatitis appeared to wax and wane, and so it was difficult to identify a directly
proportional relationship between changes in fPL levels and clinical symptoms
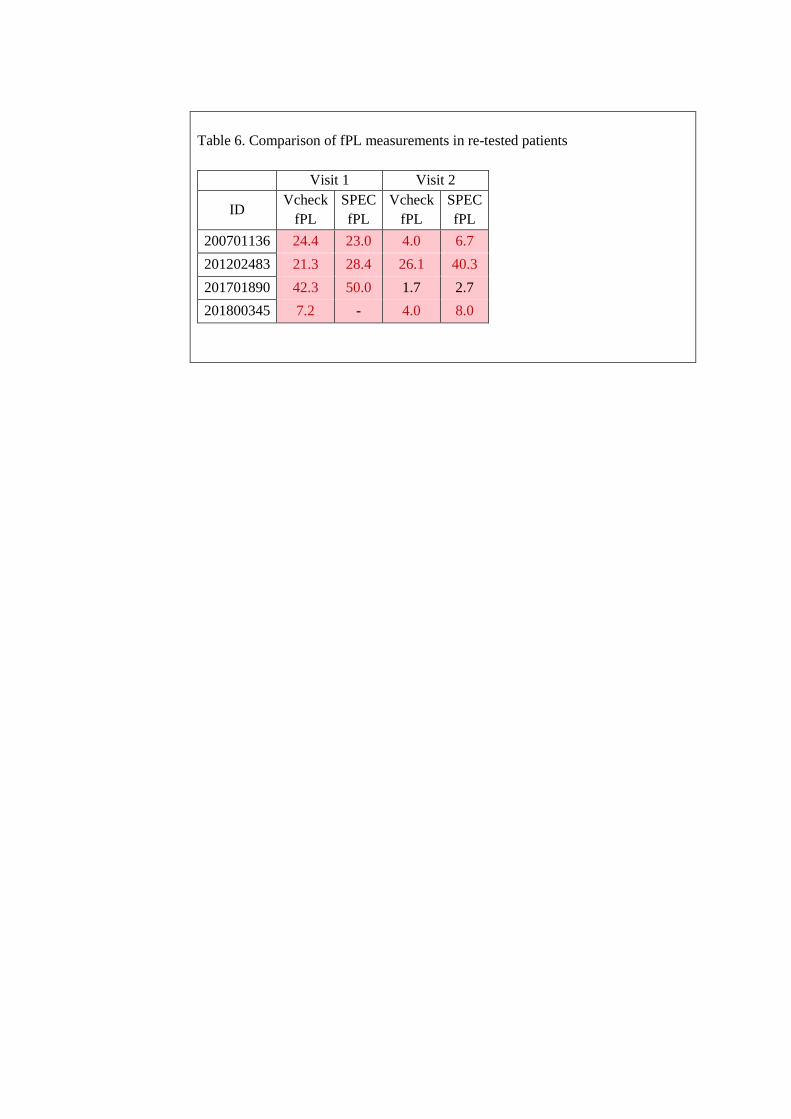
Table 6. Comparison of fPL measurements in re-tested patients
Visit 1 Visit 2
ID Vcheck
fPL
SPEC
fPL
Vcheck
fPL
SPEC
fPL
200701136 24.4 23.0 4.0 6.7
201202483 21.3 28.4 26.1 40.3
201701890 42.3 50.0 1.7 2.7
201800345 7.2 - 4.0 8.0

IV. Discussion
As observed in the results of the clinical trial above, Vcheck and SPEC measurements of cPL and fPL
showed strong correlations. The two tests use the same normal ranges, and in our study, excluding
patients with missing measurements, there were 84 patients for which the two tests could be compared
(52 dogs at initial visit, 14 dogs with multiple visits, 14 cats at initial visit, 4 cats with multiple visits);
apart from a single case, the other 83 patients all showed matched interpretations for the two tests.
In the one case which showed different interpretation results from Vcheck cPL and SPEC cPL, the
Vcheck cPL was above the threshold value and the SPEC cPL measurement was below the threshold
value. Since this patient was ultimately diagnosed with pancreatitis, the Vcheck cPL was considered to
have been beneficial to clinical diagnosis. However, given that the SPEC cPL result was close to the
upper limit of the normal range (200 ng/mL), the low SPEC measurement was considered to be a result
that could occur commonly in patients with pancreatitis. In no circumstances should a veterinarian
depend solely on any one test result, and patients should be diagnosed based on a comprehensive
assessment of various clinical tests and clinical symptoms.
In terms of convenience, the SPEC cPL test suffers from the two drawbacks of high cost and the long
time required to obtain results. To overcome these limitations, the SNAP cPL kit is provided to enable
immediate testing and verification of the results in hospitals. However, when the cPL concentration is
close to the upper limit of 200 ng/mL for the reference range (not ≥ 400 ng/mL, which is interpreted as
‘consistent with pancreatitis’), it is difficult to precisely read the results with the naked eye, and an
additional SPEC test may have to be requested. On the other hand, when using Vcheck, the results can
be checked immediately at the hospital, like SNAP, and since it provides a quantitative measurement,
it enables more objective results compared to those that are checked with the naked eye.
In conclusion, since Vcheck shows high sensitivity and specificity at a similar level to SPEC, it is
considered to be equally beneficial to diagnosis of pancreatitis in both dogs and cats. Since the rate of
agreement with SPEC is high, we expect that animal hospitals previously using SPEC and SNAP could
change to Vcheck, and there would be little difference in diagnoses. Moreover, the advantages of rapid
diagnosis and quantitative results would offer greater convenience when used in clinics. In the future,
we anticipate that outstanding domestic companies will continue to accelerate development of clinical
testing technology for veterinarian hospitals, and the commercial advances will be pursued within the
clinical veterinary medicine industry in South Korea.













![[홍보자료Œ] Vcheck D-dimer PPT EN](https://img.pdfslide.net/doc/110x75/61e11e2b440fb31d77387e5a/-vcheck-d-dimer-ppt.jpg)















