Embed Size (px)
Citation preview
Venlafaxine versus methylphenidate in pediatric outpatientswith attention deficit hyperactivity disorder: a randomized,double-blind comparison trial
Ali-Reza Zarinara1, Mohammad-Reza Mohammadi2, Nazanin Hazrati2, Mina Tabrizi3,Shams-Ali Rezazadeh4, Farzin Rezaie5 and Shahin Akhondzadeh2*
1IT Center, Deputy for Research, Tehran University of Medical Sciences, Tehran, Iran2Psychiatric Research Centre, Roozbeh Hospital, Tehran University of Medical Sciences, Tehran, Iran3Faculty of Medicine, Department of Medical Genetics, Tehran University of Medical Sciences, Tehran, Iran4Institute of Medicinal Plants (ACECR), Tehran, Iran5Depertment of Psychiatry, Kurdistan University of Medical Sciences, Sanandaj, Iran
Objective The present report aimed to investigate the efficacy and tolerability of venlafaxine compared to methylphenidate in children andadolescents with Attention Deficit/Hyperactivity Disorder (ADHD).Methods This was a 6-week, parallel group, randomized clinical trial. Thirty-eight patients (27 boys and 11 girls) with a DSM-IV-TRdiagnosis of ADHD were the study population of this trial. All study subjects were randomly assigned to receive treatment using capsules ofvenlafaxine at doses of 50–75mg/day depending on weight (50mg/day for<30 kg and 75mg/day for>30 kg (group 1) or methylphenidate ata dose of 20–30mg/day depending on weight (group 2) for a 6-week double blind, randomized clinical trial. The principal measure of outcomewas the Teacher and Parent Attention Deficit/Hyperactivity Disorder Rating Scale-IV.Results No significant differences were observed between the two groups on the Parent and Teacher Rating Scale scores (df¼ 1; F¼ 1.77;p¼ 0.19 and df¼ 1; F¼ 1.64; p¼ 0.20, respectively). Side effects of headaches and insomnia were observed more frequently in themethylphenidate group.Conclusions The results suggest that venlafaxine may be useful for the treatment of ADHD. In addition, a tolerable side-effect profile is oneof the advantages of venlafaxine in the treatment of ADHD. Copyright # 2010 John Wiley & Sons, Ltd.
key words—ADHD; RCT; venlafaxine
INTRODUCTION
Attention Deficit/Hyperactivity Disorder (ADHD) isa commonly diagnosed childhood disorder that affectsapproximately 3–7% of children. As a result, ADHDis one of the most common presenting problemsamong children referred to mental health professionals(Noorbala and Akhondzadeh, 2006).Pharmacotherapy is the most commonly recom-
mended intervention for ADHD and it has been shownto be the optimal treatment option in cases where noother comorbid conditions are present. Numerousresources document the efficacy of stimulants suchas methylphenidate and other stimulants (Rader et al.,
2000; Mohammadi and Akhondzadeh, 2007). Stimu-lant medications are likely to remain first-linetreatments for ADHD, yet other alternatives willincreasingly be of value for a variety of treatmentsituations. For example, findings suggest that nearly25% of affected youth will not respond to abovementioned medications, or that they will discontinueusage due to negative side effects, most notablyinsomnia and loss of appetite (Banaschewski et al.,2004; Curatolo et al., 2009). Therapy with antidepress-ant drugs has proved beneficial in heterogeneousgroups of children with disruptive behavioral symp-toms. The use of these drugs was further supportedby their inhibitory actions on dopamine and norepi-nephrine metabolism – findings consistent with thehypothesis of decreased catecholamine activity inADHD (Mohammadi and Akhondzadeh, 2007).Venlafaxine, an antidepressant with both serotonergicand noradrenergic properties, has been investigated
human psychopharmacology
Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.
Published online 22 September 2010 in Wiley Online Library
(wileyonlinelibrary.com) DOI: 10.1002/hup.1148
*Correspondence to: S. Akhondzadeh, Psychiatric Research Center, Rooz-beh Psychiatric Hospital, Tehran University of Medical Sciences, SouthKargar Street, Tehran 13337, Iran. Tel: þ98-21-88281866; Fax: þ98-21-55419113. E-mail: [email protected]
Copyright # 2010 John Wiley & Sons, Ltd.
Received 18 May 2010
Accepted 11 August 2010
as a possible treatment alternative in ADHD. It has nosignificant affinity for muscarinic, cholinergic, hista-minic, or alpha-1-adrenergic receptors and a relativeshort half-life, and is given in divided doses (Ninan,2000; Hardy et al., 2002; Gutierrez et al., 2003). Somesmall open-label studies suggest that venlafaxine maybe an effective medication in treating the coresymptoms of ADHD in children and adolescents(Mukaddes and Abali, 2004; Findling et al., 2007).There are only three open-label studies reporting
efficacy of venlafaxine in children and adolescentsand to the best of our knowledge there is no publishedplacebo or active agent controlled trial of venlafaxinein child and adolescent (Olvera et al., 1996; Mukaddesand Abali, 2004; Findling et al., 2007). Thepresent report aimed to investigate the efficacy andtolerability of venlafaxine compared to methylpheni-date in children and adolescents with ADHD.
METHODS
This was a 6-week, parallel group, randomized clinicaltrial undertaken in an outpatient child and adolescentclinic at Roozbeh Psychiatric Hospital in Tehran, Iranduring March 2009–February 2010.
Participants
Subjects included 38 outpatients (27 boys and 11 girls)between the ages of 6–13 who clearly met the DSM-IV-TR diagnostic criteria for ADHD. At screening,investigators conducted a psychiatric evaluationwith the DSM-IV-TR criteria for ADHD and theKiddie Schedule for Affective Disorders and Schizo-phrenia-Present and Lifetime diagnostic interviewand performed a complete medical history andphysical examination (American Psychiatric Associ-ation, 2000; Ghanizadeh et al., 2006). Additionalinclusion criteria included total and/or subscale scoreson Attention-Deficit/Hyperactivity Disorder RatingScale-IV (ADHD-RS-IV) School Version of at least1.5 standard deviations above norms for patient’s ageand gender (DuPaul et al., 1998). The patients wererecruited from the outpatient child and adolescentclinic at Roozbeh Psychiatric Hospital. The diagnosisof ADHD was confirmed by a child and adolescentpsychiatrist before participants were initiated intothe study. All patients had combined subtype of ADHDand were newly diagnosed. Parents were carefullyinterviewed and asked to rate the severity of the DSM-IV-TR ADHD symptoms that their children displayedat home. Children were excluded if they had a historyor current diagnosis of pervasive developmental
disorders, schizophrenia, or other psychiatric disorders(DSM-IVaxis I); or any current psychiatric comorbid-ity that required pharmacotherapy; any evidence ofsuicide risk and mental retardation (IQ< 70). Inaddition, patients were excluded if they had a clinicallysignificant chronic medical condition, includingorganic brain disorder, seizures, or current abuse ordependence on drugs the last 6 months. Additionalexclusion criteria were hypertension or hypotension.To participate, parents and children had to be willingto comply with all requirements of the study. After adescription of the purpose and the procedures of thestudy, written informed consent was obtained fromeach patient’s parent or guardian. Informed consentwas received before the administration of any studyprocedure or distribution of study medication inaccordance with the ethical standards of the investi-gative site’s Institutional Review Board (IRB) and withthe Helsinki declaration of 1975, as revised in 2000.The study was approved by the IRB of TehranUniversity of Medical Sciences (grant no: 6963).
Study design
Patients underwent a standard clinical assessmentcomprised of a psychiatric evaluation, a structureddiagnostic interview, a medical history, and anelectrocardiogram (ECG). Patients were randomizedto receive tablet of venlafaxine or methylphenidate ina 1:1 ratio using a computer-generated code. Bothtablets were encapsulated and were identical. Theassignments were kept in sealed, opaque envelopesuntil data analysis. The randomization and allocationprocess was done by the pharmacist at the RoozbehHospital. All study subjects were randomly assigned toreceive treatment using capsules of venlafaxine atdoses of 50–75mg/day depending on weight (50mg/day for <30 kg and 75mg/day for >30 kg (group 1) ormethylphenidate at doses of 20–30mg/day dependingon weight (20mg/day for <30 kg and 30mg/day for>30 kg (group 2) for a 6-week double blind,randomized clinical trial. Venlafaxine was titrated upduring the trial according to the following schedule:week 1: 25mg/day; week 2: 50mg/day (one capsule ofvenlafaxine in the morning and one capsule ofvenlafaxine at midday); and week 3: 75mg/day forchildren >30 kg (one capsule of venlafaxine in themorning, one capsule of venlafaxine at midday, andone capsule of venlafaxine at 16.00). Methylphenidatewas titrated up during the trial according to thefollowing schedule: week 1: 10mg/day (5mg in themorning and 5mg at midday); week 2: 20mg/day(10mg in the morning and 10mg at midday); and week
Copyright # 2010 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.DOI: 10.1002/hup
VENLAFAXINE IN THE TREATMENT OF adhd 531
3: 30mg/day for children >30 kg (10mg in themorning, 10mg at midday, and 10mg at 16.00). Inthis schedule, drugs were blindly administered duringtitration. Throughout the study, the person whoadministrated the medications, the rater, and thepatients along with their parents were blind to groupassignments. The principal measure of outcome wasthe Parent and Teacher ADHD-Rating Scale-IV thathas been used extensively in Iran in school-agechildren and provides valid measures of behavioralabnormality and attention (Akhondzadeh et al., 2003,2004; Amiri et al., 2008; Kahbazi et al., 2009; Salehiet al., 2010). ADHD-RS-IV is an instrument thatassesses the 18 symptoms of ADHD as defined in theDSM-IV-TR according to a 4-point Likert scale. Themean decrease in ADHD-RS-IV score from baselinewas used as the main outcome measure of response
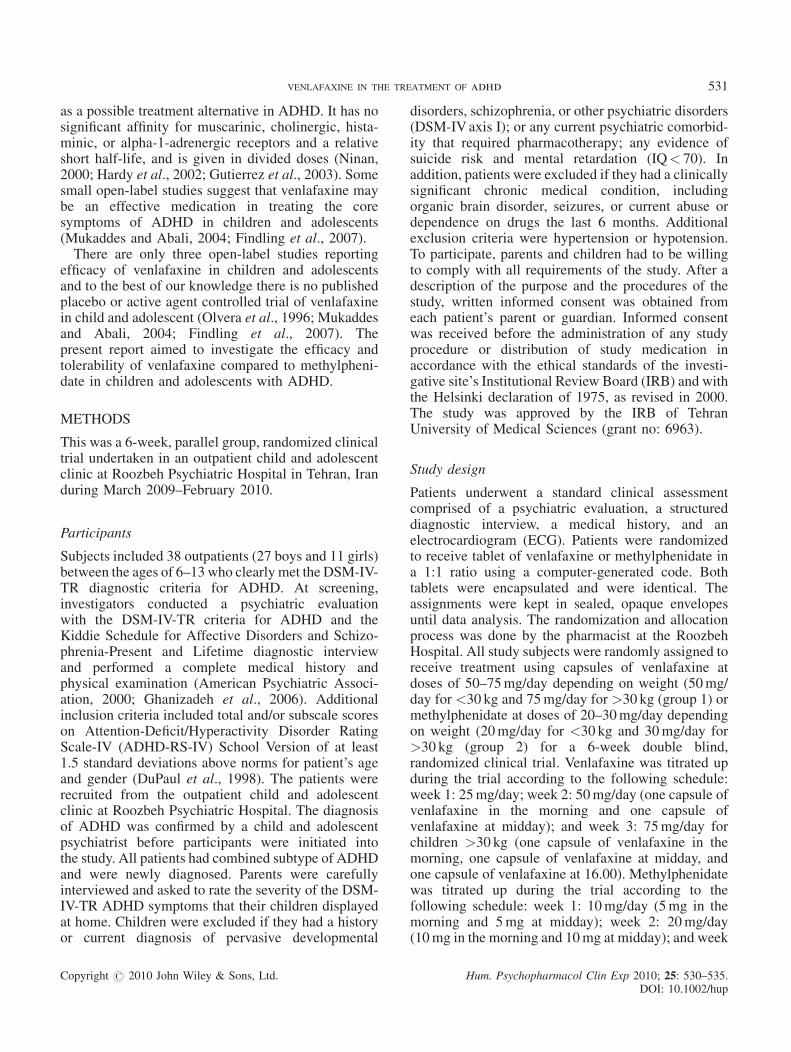
of ADHD treatment. Patients were assessed at baselineand 21 and 42 days after the medication was startedby a fellow of child psychiatry. Side effects weresystematically recorded throughout the study and wereassessed using a checklist that comprises 20 sideeffects including psychic, neurologic, autonomic, andother side effects, administered by a child psychiatriston days 7, 21, and 42. One patient dropped out fromeach group due to lack of follow-up (no parentcollaboration), leaving 36 patients who completedthe trial (Figure 1). Hematology tests were collectedat baseline and weeks 2, 4, and 6; serum chemistry andurinalysis were evaluated at baseline and week 6;body weight and vital signs were measured at baselineand weeks 1, 2, 4, and 6; and 12-lead ECG andphysical examinations were evaluated at baseline andweek 6.
Figure 1. Enrollment and outcome flowchart
Copyright # 2010 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.DOI: 10.1002/hup
532 a.-r. zarinara ET AL.
Statistical analysis
A two-way repeated measures analysis of variance(time-treatment interaction) was used. The two groups(venlafaxine and methylphenidate) as a between-subjects factor (group) and the three measurementsduring treatment as the within-subjects factor (time)were considered. This was done for Parent and TeacherADHD Rating Scale scores. Results are presented asmean� SD. Differences were considered significantwith p� 0.05. To compare the demographic data andfrequency of side effects between the protocols,Fisher’s exact test was performed. To consider thefinal difference between the two groups, at least ascore of 5 on the Teacher and Parent ADHD RatingScale, S¼ 5 and power¼ 0.8, the sample size wascalculated at least 15 patients in each group. Intentionto treat (ITT) analysis with the last observation carriedforward (LOCF) procedure was performed.
RESULTS
No significant difference was identified between patientsrandomly assigned to the group 1 or 2 conditions withregard to basic demographic data including age genderand weight (Table 1).
Parent ADHD rating scale
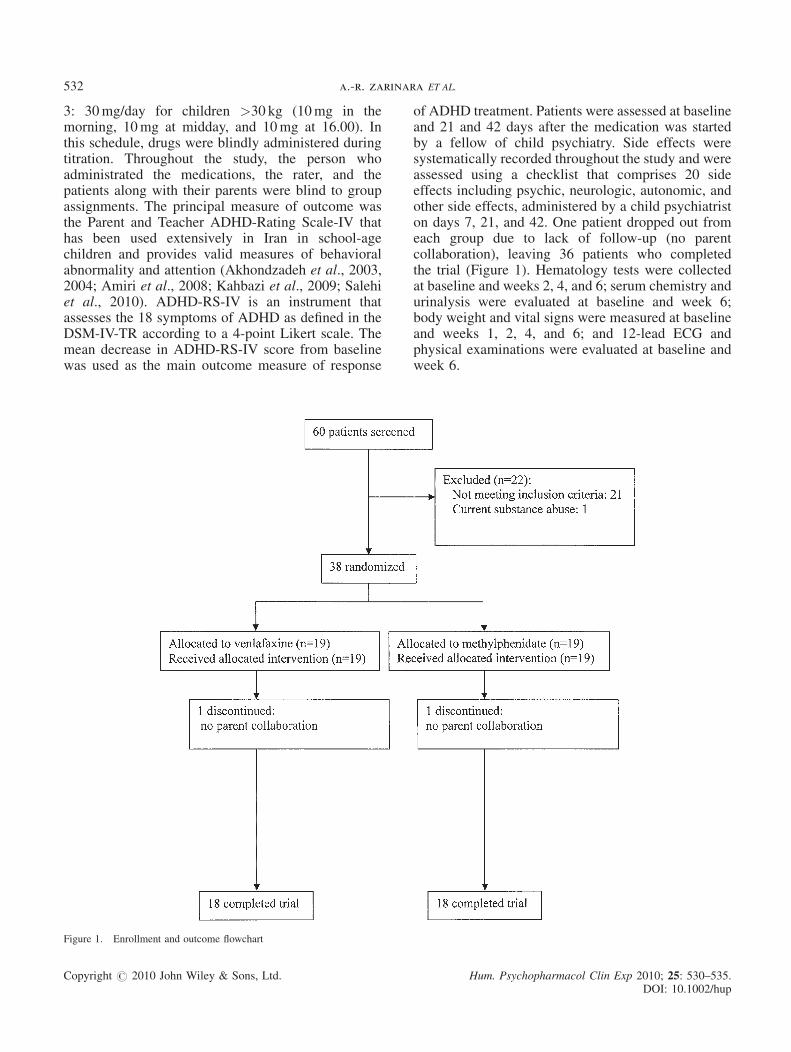
The mean� SD scores of the two groups are shown inFigure 2. There was no significant difference betweenthe two groups at day 0 (baseline) on the Parent ADHDRating Scale (t¼ 0.24; df¼ 36; p¼ 0.8). The differ-ence between the two groups was not significant asindicated by the effect of group, the between subjectsfactor (df¼ 1; F¼ 1.77; p¼ 0.19). The behavior of thetwo treatment groups was similar across time (groupsby time interaction, Greenhouse–Geisser, df¼ 2.21;F¼ 0.61; p¼ 0.55). In addition, a one-way repeatedmeasures analysis of variance showed a significanteffect of both protocols on the Parent ADHD RatingScale scores (p< 0.001). The differences between thetwo protocols were not significant at the endpoint(t¼ 1.39; df¼ 36; p¼ 0.17). The changes at endpoint
compared to baseline were:�14.15� 7.01 (mean� SD)and �16.63� 8.59 (mean� SD) for venlafaxine andmethyphenidate, respectively. No significant differencewas observed on the reduction of scores of the ParentADHD Rating Scale at week 6 compared to baseline inthe two groups (t¼ 0.97; df¼ 36; p¼ 0.33). There wereno significant differences between the two groups interms of percentage of responders (those with at leasta 40% decrease in Parent ADHD Rating Scale scorebetween baseline and treatment culmination) (venlafax-ine: 68.42%, 13 of 19, and methylphenidate: 73.68%, 14of 19).
Teacher ADHD rating scale
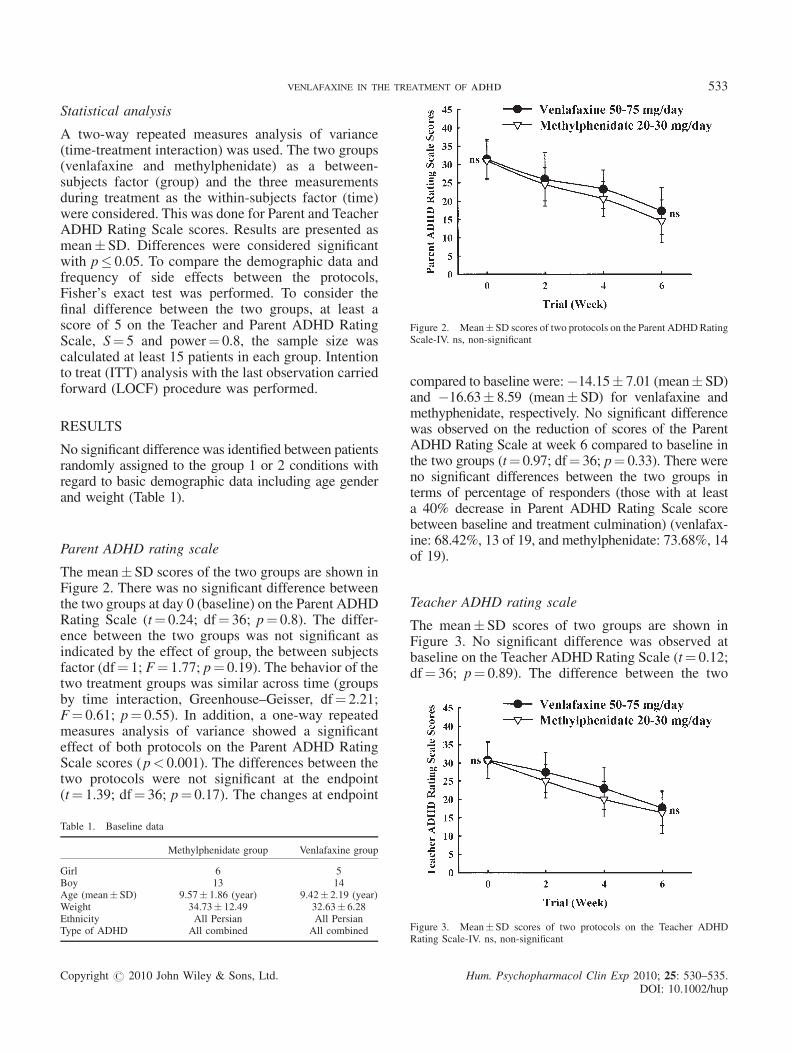
The mean� SD scores of two groups are shown inFigure 3. No significant difference was observed atbaseline on the Teacher ADHD Rating Scale (t¼ 0.12;df¼ 36; p¼ 0.89). The difference between the two
Table 1. Baseline data
Methylphenidate group Venlafaxine group
Girl 6 5Boy 13 14Age (mean�SD) 9.57� 1.86 (year) 9.42� 2.19 (year)Weight 34.73� 12.49 32.63� 6.28Ethnicity All Persian All PersianType of ADHD All combined All combined
Figure 2. Mean�SD scores of two protocols on the Parent ADHDRatingScale-IV. ns, non-significant
Figure 3. Mean�SD scores of two protocols on the Teacher ADHDRating Scale-IV. ns, non-significant
Copyright # 2010 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.DOI: 10.1002/hup
VENLAFAXINE IN THE TREATMENT OF adhd 533
protocols was not significant as indicated by the effectof group, the between subjects factor (df¼ 1; F¼ 1.64;p¼ 0.20). The behavior of the two treatment groupswas similar across time (groups by time interaction;Greenhouse–Geisser, df¼ 1.76; F¼ 1.11; p¼ 0.32).In addition, a one-way repeated measures analysis ofvariance showed a significant effect of both groupson the Teacher ADHDRating Scale scores (p< 0.001).The difference between the two groups was notsignificant at the endpoint (t¼ 0.76; df¼ 36; p¼ 0.45).The changes at the endpoint compared to baselinewere: �13.05� 4.77 (mean� SD) and �15.31� 8.13(mean� SD) for venlafaxine and methylphenidate,respectively. No significant difference was observedon the reduction of scores of the Teacher ADHDRatingScale at week 6 compared to baseline in the two groups(t¼ 1.04; df¼ 36; p¼ 0.30). There were no significantdifferences between the two groups in terms of thepercentage of responders (those with at least a 40%decrease in Teacher ADHD Rating Scale score betweenbaseline and treatment end) (venlafaxine: 63%, 12 of 19,and methylphenidate: 68.42%, 13 of 19).
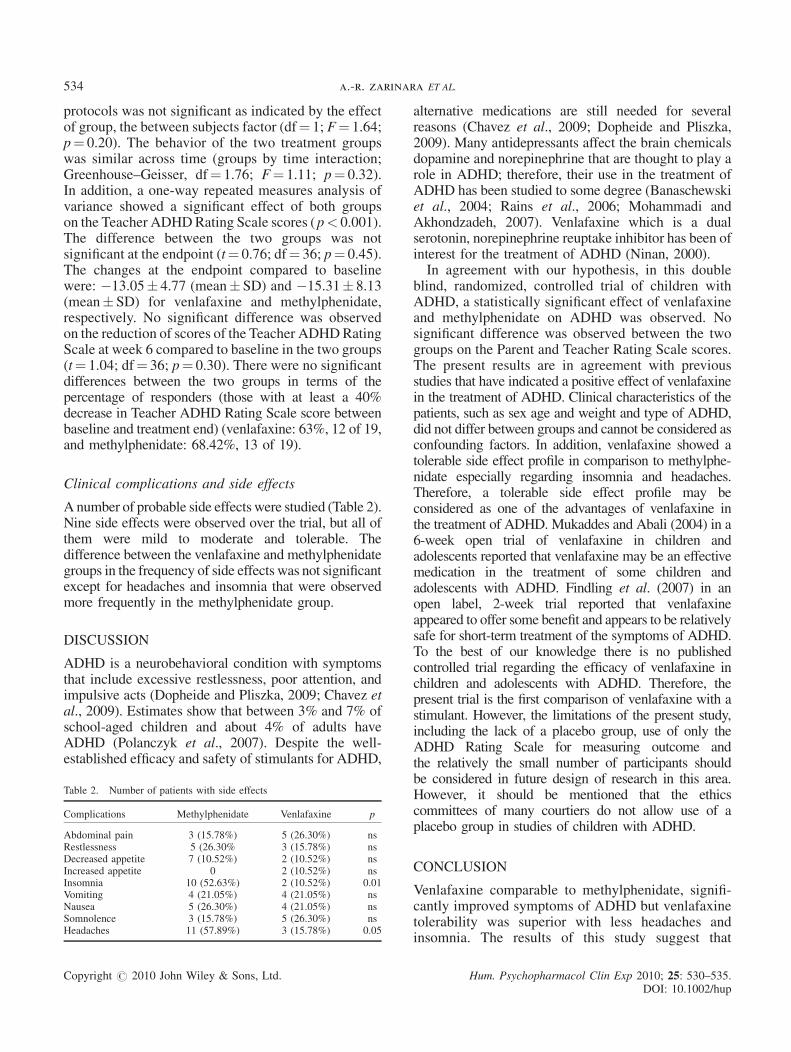
Clinical complications and side effects
Anumber of probable side effects were studied (Table 2).Nine side effects were observed over the trial, but all ofthem were mild to moderate and tolerable. Thedifference between the venlafaxine and methylphenidategroups in the frequency of side effects was not significantexcept for headaches and insomnia that were observedmore frequently in the methylphenidate group.
DISCUSSION
ADHD is a neurobehavioral condition with symptomsthat include excessive restlessness, poor attention, andimpulsive acts (Dopheide and Pliszka, 2009; Chavez etal., 2009). Estimates show that between 3% and 7% ofschool-aged children and about 4% of adults haveADHD (Polanczyk et al., 2007). Despite the well-established efficacy and safety of stimulants for ADHD,
alternative medications are still needed for severalreasons (Chavez et al., 2009; Dopheide and Pliszka,2009). Many antidepressants affect the brain chemicalsdopamine and norepinephrine that are thought to play arole in ADHD; therefore, their use in the treatment ofADHD has been studied to some degree (Banaschewskiet al., 2004; Rains et al., 2006; Mohammadi andAkhondzadeh, 2007). Venlafaxine which is a dualserotonin, norepinephrine reuptake inhibitor has been ofinterest for the treatment of ADHD (Ninan, 2000).In agreement with our hypothesis, in this double
blind, randomized, controlled trial of children withADHD, a statistically significant effect of venlafaxineand methylphenidate on ADHD was observed. Nosignificant difference was observed between the twogroups on the Parent and Teacher Rating Scale scores.The present results are in agreement with previousstudies that have indicated a positive effect of venlafaxinein the treatment of ADHD. Clinical characteristics of thepatients, such as sex age and weight and type of ADHD,did not differ between groups and cannot be considered asconfounding factors. In addition, venlafaxine showed atolerable side effect profile in comparison to methylphe-nidate especially regarding insomnia and headaches.Therefore, a tolerable side effect profile may beconsidered as one of the advantages of venlafaxine inthe treatment of ADHD. Mukaddes and Abali (2004) in a6-week open trial of venlafaxine in children andadolescents reported that venlafaxine may be an effectivemedication in the treatment of some children andadolescents with ADHD. Findling et al. (2007) in anopen label, 2-week trial reported that venlafaxineappeared to offer some benefit and appears to be relativelysafe for short-term treatment of the symptoms of ADHD.To the best of our knowledge there is no publishedcontrolled trial regarding the efficacy of venlafaxine inchildren and adolescents with ADHD. Therefore, thepresent trial is the first comparison of venlafaxine with astimulant. However, the limitations of the present study,including the lack of a placebo group, use of only theADHD Rating Scale for measuring outcome andthe relatively the small number of participants shouldbe considered in future design of research in this area.However, it should be mentioned that the ethicscommittees of many courtiers do not allow use of aplacebo group in studies of children with ADHD.
CONCLUSION
Venlafaxine comparable to methylphenidate, signifi-cantly improved symptoms of ADHD but venlafaxinetolerability was superior with less headaches andinsomnia. The results of this study suggest that
Table 2. Number of patients with side effects
Complications Methylphenidate Venlafaxine p
Abdominal pain 3 (15.78%) 5 (26.30%) nsRestlessness 5 (26.30% 3 (15.78%) nsDecreased appetite 7 (10.52%) 2 (10.52%) nsIncreased appetite 0 2 (10.52%) nsInsomnia 10 (52.63%) 2 (10.52%) 0.01Vomiting 4 (21.05%) 4 (21.05%) nsNausea 5 (26.30%) 4 (21.05%) nsSomnolence 3 (15.78%) 5 (26.30%) nsHeadaches 11 (57.89%) 3 (15.78%) 0.05
Copyright # 2010 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.DOI: 10.1002/hup
534 a.-r. zarinara ET AL.

venlafaxine may be considered as an alternativetreatment for children with ADHD.
CONFLICT OF INTEREST
All authors declare no conflict of interest.
ACKNOWLEDGEMENTS
This study was the postgraduate thesis of Dr. NazaninHazrati toward the Iranian board of psychiatry. This studywas supported by a grant from Tehran University of MedicalSciences (grant no: 6963) to Prof. Shahin Akhondzadeh.
REFERENCES
Akhondzadeh S, Tavakolian R, Davari-Ashtiani R, Arabgol F, Amini H.2003. Selegiline in the treatment of attention-deficit hyperactivity dis-order in children: a double-blind and randomized trial. Prog Neuropsy-chopharmacol Biol Psychiatry 27: 841–845.
Akhondzadeh S, Mohammadi MR, Khademi M. 2004. Zinc sulfate as anadjunct to methylphenidate for the treatment of attention deficit hyper-activity disorder in children: a double blind and randomized trial[ISRCTN64132371]. BMC Psychiatry 8(4): 9.
American Psychiatric Association. 2000. American Psychiatric AssociationDiagnostic and Statistical Manual for Mental Disorders DSM IV-TR, 4thedn (Text Revision) American Psychiatric Press: Washington DC.
Amiri S, Mohammadi MR, Mohammadi M, Nouroozinejad GH, KahbaziM, Akhondzadeh S. 2008. Modafinil as a treatment for Attention-Deficit/Hyperactivity Disorder in children and adolescents: a double blind,randomized clinical trial. Prog Neuropsychopharmacol Biol Psychiatry32: 145–149.
Banaschewski T, Roessner V, Dittmann RW, Santosh PJ, Rothenberger A.2004. Non-stimulant medications in the treatment of ADHD. Eur ChildAdol Psychiatry 13: 102–116.
Chavez B, Sopko MA, Jr., Ehret MJ, et al. 2009. An update on centralnervous system stimulant formulations in children and adolescents withattention-deficit/hyperactivity disorder. Ann Pharmacother 43: 1084–1095.
Curatolo P, Paloscia C, D’Agati E, Moavero R, Pasini A. 2009. Theneurobiology of attention deficit/hyperactivity disorder. Eur J PaediatrNeurol 13: 299–304.
Dopheide JA, Pliszka SR. 2009. Attention-deficit-hyperactivity disorder: anupdate. Pharmacotherapy 29: 656–679.
DuPaul G, Power T, Anastopoulos A, Reid R. 1998. ADHD Rating Scale-IV.Guilford: New York.
Findling RL, Greenhill LL, McNamara NK, et al. 2007. Venlafaxine inthe treatment of children and adolescents with attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol 17: 433–445.
Ghanizadeh A, Mohammadi MR, Yazdanshenas A. 2006. Psychometricproperties of the Farsi translation of the Kiddie schedule for affectivedisorders and schizophrenia – present and lifetime version. BMC Psy-chiatry 15(6): 10.
Gutierrez MA, Stimmel GL, Aiso JY. 2003. Venlafaxine: a 2003 update.Clin Ther 25: 2138–2154.
Hardy J, Argyropoulos S, Nutt DJ. 2002. Venlafaxine: a new class ofantidepressant. Hosp Med 63: 549–552.
Kahbazi M, Ghoreishi A, Rahiminejad F, Mohammadi MR, KamalipourA, Akhondzadeh S. 2009. A randomized, double-blind and placebo-controlled trial of modafinil in children and adolescents with attentiondeficit and hyperactivity disorder. Psychiatry Res 168: 234–237.
Mohammadi MR, Akhondzadeh S. 2007. Pharmacotherapy of attention-deficit/hyperactivity disorder: nonstimulant medication approaches. ExpRev Neurotrapeutics 7: 195–201.
Mukaddes NM, Abali O. 2004. Venlafaxine in children and adolescentswith attention deficit hyperactivity disorder. Psychiatry Clin Neurosci 58:92–95.
Ninan PT. 2000. Use of venlafaxine in other psychiatric disorders. DepressAnxiety 12(Suppl 1): 90–94.
Noorbala AA, Akhondzadeh S. 2006. Attention-deficit/hyperactivitydisorder: etiology and pharmacotherapy. Arch Iran Med 9: 374–380.
Olvera RL, Pliszka SR, Luh J, Tatum R. 1996. An open trial ofvenlafaxine in the treatment of attention-deficit/hyperactivity dis-order in children and adolescents. J Child Adolesc Psychopharmacol6: 241–250.
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA. 2007. Theworldwide prevalence of ADHD: a systematic review and metaregressionanalysis. Am J Psychiatry 164: 942–948.
Rader R, McCauley L, Callen EC. 2000. Current strategies in the diagnosisand treatment of childhood attention-deficit/hyperactivity disorder. AmFam Phys 79: 657–665.
Rains A, Scahill L, Hamrin V. 2006. Nonstimulant medications for thetreatment of ADHD. J Child Adolesc Psychiatr Nurs 19: 44–47.
Salehi B, Imani R, Mohammadi MR, et al. 2010. Ginkgo biloba forattention-deficit/hyperactivity disorder in children and adolescents: adouble blind, randomized controlled trial. Prog NeuropsychopharmacolBiol Psychiatry 34: 76–80.
Copyright # 2010 John Wiley & Sons, Ltd. Hum. Psychopharmacol Clin Exp 2010; 25: 530–535.DOI: 10.1002/hup
VENLAFAXINE IN THE TREATMENT OF adhd 535





























